Embed Size (px)
Citation preview
Respiratory Medicine (2012) 106, 1671e1679
Available online at www.sciencedirect.com
journal homepage: www.elsevier .com/locate/rmed
Short term and long term effects of pulmonaryrehabilitation on physical activity in COPD
Claire Egan a,b,e, Brenda M. Deering a,b,e, Catherine Blake c,Brona M. Fullen c, Niamh M. McCormack a,b, Martijn A. Spruit d,Richard W. Costello a,b,*
aDepartment of Respiratory Medicine, Royal College of Surgeons in Ireland, Beaumont Hospital, Dublin, IrelandbThe Education and Research Centre, Smurfit Building, Royal College of Surgeons in Ireland, Beaumont Hospital,Dublin, Irelandc School of Public Health, Physiotherapy, and Population Science, University College Dublin, Irelandd Program Development Centre, CIROþ, A Centre of Expertise for Chronic Organ Failure, Horn, The Netherlands
Received 15 March 2012; accepted 21 August 2012Available online 12 October 2012
KEYWORDSCOPD;Rehabilitation;Free-living exercise
* Corresponding author. Smurfit BuilE-mail address: [email protected] (
e Joint first authors.
0954-6111/$ - see front matter ª 201http://dx.doi.org/10.1016/j.rmed.201
Summary
The central purpose of pulmonary rehabilitation is to reduce morbidity by improving functionalcapacity through exercise. It is still unknown if improvements in functional capacity are main-tained in the long-term and if this leads to increased physical activity levels as measured bya free-living activity monitor. The hypothesis of this study was that pulmonary rehabilitationwould lead to a sustained increase in standard outcome measures and in daily physical activity.Methods: A prospective study of 47 subjects with COPD was performed, registered at Clinical-Trials.gov (Clinical Trial Number NCT 0112943). The primary outcome was a maintainedimprovement in standard outcome measures with a secondary aim of an increase in daily phys-ical activity. A convenient sample of the cohort (n Z 17) was re-evaluated at a third time pointat 1 year.Results: A seven week hospital based outpatient pulmonary rehabilitation program led toa significant reduction in total energy expenditure (p < 0.044) and breathlessness (Borg,p < 0.011) and improved exercise capacity (ISWT, p > 0.001, 6MWT, p > 0.002) PiMax(p > 0.007) and quality of life scores (SGRQ, p > 0.001, EQ5D, 0.025). However, pulmonaryrehabilitation did not significantly change the average number of daily steps taken, time spentsedentary activity, METs consumed or daily physical activity. Indeed, all of the standard andfreeliving values had returned towards the baseline value at 1 year.
ding, Beaumont Hospital, Dublin 9, Ireland. Tel.: þ353 1 8093762.R.W. Costello).
2 Elsevier Ltd. All rights reserved.2.08.016

1672 C. Egan et al.
Discussion: These findings show that while pulmonary rehabilitation increased exercisecapacity this was not transmitted into increased daily physical activity. Hence, alternativemethods to alter/affect behavioural change need to be addressed.ª 2012 Elsevier Ltd. All rights reserved.
Background
In 2011, the World Health Organisation estimated that 31%of the world’s population was inactive and that this physicalinactivity was the fourth leading risk factor for all globaldeaths.1 In patients with Chronic Obstructive PulmonaryDisease (COPD), activity levels are low compared to healthycontrols and other chronic conditions such as arthritis anddiabetes2,3 and decrease according to the clinical stage ofthe disease and age4-7. Conversely, the more physicallyactive a person with COPD is the better their functionalstatus in terms of exercise capacity.8 Deconditioning asa result of low levels of activities is detrimental to thehealth of this already compromised patient population.9
The primary goal of pulmonary rehabilitation (PR) pro-grammes has been to break the cycle of breathlessness anddeconditioning through prescribed exercise. The exercisetraining component of PR significantly improves functionalcapacity, quality of life, and symptoms of dyspnoea, evenfor those patients in the moderate to severe category,10,11
and this is now considered to be an essential aspect oftreatment of patients with COPD. Short-term programmeshave shown immediate benefit and some have arresteddeterioration over time.12 However, a dose-effect responsehas been suggested for long-term benefits.13e16
Physical inactivity and COPD are a product of lifestylechoice and lack of knowledge. Combined these lead toskeletal muscle abnormalities, deconditioning and loss offunction17,18 this loss of function is especially evident duringan exacerbation.19 Physical inactivity has been highlightedas component in a global strategy that can be targeted tohelp reduce the global burden of non-communicatediseases.20 The evidence that increased physical activity isachieved through participation in a pulmonary rehabilitationare inconclusive but suggest that these two goals are tooincongruent for the present programme design.21,22 A twotiered approach with functional capacity for secondary careand physical activity for primary care may be the wayforward with both embracing the educational componentand creating a supportive environment, imparting knowl-edge to the patient on the nature of the condition, teachingcoping mechanisms and by providing the patient with usefultools by the way of ‘Action Plans’.23
Physical activity monitors are a useful tool for measuringactivity levels in the community. They are an objective,accurate, non-invasive, and effective way of measuringfree-living activities.5,6,24 One such performance-basedmotion sensor is the SenseWear accelerometer. TheSenseWear has previously been used in patients with COPDand has been shown to be a reliable measure of physicalactivity in this population.25 To-date, only a six monthprogramme has been shown to improve free-living activitiesas measured by activity monitors.26 Given the paucity oflong-term follow up free-living physical activity outcomes
following standard PR programmes, further examination oflasting effect is warranted. The hypothesis of this study wasthat pulmonary rehabilitation leads to short term and sus-tained improvement in functional capacity along with free-living physical activity in patients with COPD in the settingof a standard 7 week pulmonary rehabilitation program.
Methods
Study design
This two-phased longitudinal study followed a group ofpatients with COPD (n Z 47) from baseline before pulmo-nary rehabilitation, immediately after completion and atthree months, to examine the short term effects on stan-dard measures and free-living physical activity. A conve-nient sample of 17 of these subjects were re-recruited fora follow up at 1 year, to evaluate if any sustained changesoccurred (Fig. 1). Exacerbations were reviewed at 1yearpre and 1yr post rehabilitation.
Criteria for selection of subjects was as recommended intheGOLDGuidelines for pulmonary rehabilitation27 (Table 1).All consecutive patients referred for pulmonary rehabilita-tion over a ninemonth periodwereenrolled in the study afterinformed consent was obtained. The study was approved bythe Beaumont Hospital Ethics committee, reference number07/10. Some of these subjects also participated in a secondstudy per Ethical approval (07/48.) The primary outcomewasto determine if participation in a supervised, outpatienthospital based, seven-week pulmonary rehabilitation pro-gramme resulted in sustained improvements in functionalcapacity and altered free-living activities including percentof time spent in sedentary activity, total TEE, physicalactivity duration (PAD), percentage of 450MET-Minutesa week (using 3METS as moderate activity,6 and the averagedaily number of steps, sleep efficiency (SE) and sleep time(ST) measured over 5 days. Secondary outcome measureswere measures of lung function, quality of life, and thenumber of exacerbations for oneyearprior to PRandoneyearpost PR. The trialwas registered at ClinicalTrials.gov (ClinicalTrial Number NCT 01530412).
Intervention
Patients completed fourteen rehabilitation classes overa seven week period on an outpatient basis.
Pulmonary rehabilitationPulmonary rehabilitation was held twice a week for sevenweeks with a recommended three further days of 30 min ofmoderate intensity of activity. The first hour consisted ofa warm-up and cool-down component made up of balanceandflexibility exercises, alongwith an individually prescribed
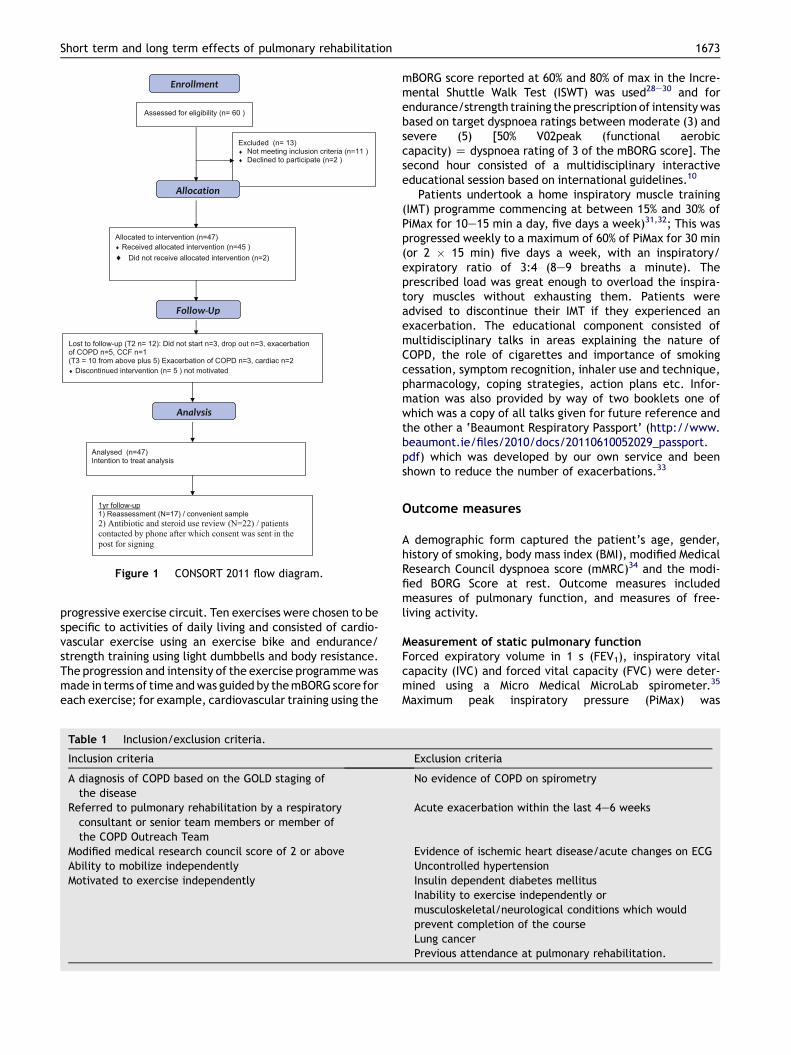
Figure 1 CONSORT 2011 flow diagram.
Short term and long term effects of pulmonary rehabilitation 1673
progressive exercise circuit. Ten exercises were chosen to bespecific to activities of daily living and consisted of cardio-vascular exercise using an exercise bike and endurance/strength training using light dumbbells and body resistance.The progression and intensity of the exercise programmewasmade in terms of time andwas guided by themBORG score foreach exercise; for example, cardiovascular training using the
Table 1 Inclusion/exclusion criteria.
Inclusion criteria
A diagnosis of COPD based on the GOLD staging ofthe disease
Referred to pulmonary rehabilitation by a respiratoryconsultant or senior team members or member ofthe COPD Outreach Team
Modified medical research council score of 2 or aboveAbility to mobilize independentlyMotivated to exercise independently
mBORG score reported at 60% and 80% of max in the Incre-mental Shuttle Walk Test (ISWT) was used28e30 and forendurance/strength training the prescription of intensitywasbased on target dyspnoea ratings between moderate (3) andsevere (5) [50% V02peak (functional aerobiccapacity) Z dyspnoea rating of 3 of the mBORG score]. Thesecond hour consisted of a multidisciplinary interactiveeducational session based on international guidelines.10
Patients undertook a home inspiratory muscle training(IMT) programme commencing at between 15% and 30% ofPiMax for 10e15 min a day, five days a week)31,32; This wasprogressed weekly to a maximum of 60% of PiMax for 30 min(or 2 � 15 min) five days a week, with an inspiratory/expiratory ratio of 3:4 (8e9 breaths a minute). Theprescribed load was great enough to overload the inspira-tory muscles without exhausting them. Patients wereadvised to discontinue their IMT if they experienced anexacerbation. The educational component consisted ofmultidisciplinary talks in areas explaining the nature ofCOPD, the role of cigarettes and importance of smokingcessation, symptom recognition, inhaler use and technique,pharmacology, coping strategies, action plans etc. Infor-mation was also provided by way of two booklets one ofwhich was a copy of all talks given for future reference andthe other a ‘Beaumont Respiratory Passport’ (http://www.beaumont.ie/files/2010/docs/20110610052029_passport.pdf) which was developed by our own service and beenshown to reduce the number of exacerbations.33
Outcome measures
A demographic form captured the patient’s age, gender,history of smoking, body mass index (BMI), modified MedicalResearch Council dyspnoea score (mMRC)34 and the modi-fied BORG Score at rest. Outcome measures includedmeasures of pulmonary function, and measures of free-living activity.
Measurement of static pulmonary functionForced expiratory volume in 1 s (FEV1), inspiratory vitalcapacity (IVC) and forced vital capacity (FVC) were deter-mined using a Micro Medical MicroLab spirometer.35
Maximum peak inspiratory pressure (PiMax) was
Exclusion criteria
No evidence of COPD on spirometry
Acute exacerbation within the last 4e6 weeks
Evidence of ischemic heart disease/acute changes on ECGUncontrolled hypertensionInsulin dependent diabetes mellitusInability to exercise independently ormusculoskeletal/neurological conditions which wouldprevent completion of the courseLung cancerPrevious attendance at pulmonary rehabilitation.

1674 C. Egan et al.
determined using a Micro Medical Respiratory PressureMeter. The best of five reproducible measurements witha maximal variability of 10% was used.32
Measurement of free-living physical activityThe SenseWear Pro Armbands were used to measure phys-ical activity (SenseWear Pro Armbands; BodyMedia, IncPittsburgh, PA). This activity armband is a biaxial acceler-ometer that records physiological parameters includingphysical activity duration (PAD) (set at �3METs/minute formoderate intensity as per Watz et al., 20096). To determinetime spend in moderate activity the percentage of MET/minwas calculated and for the purpose of this study, moderateintensity of 3METS over 150 min per week was the equiva-lent of 450MET/minutes per week.36 Total energy expen-diture (TEE), metabolic equivalent (METs), steps per day,and sleep time (ST)/efficiency (SE) were also measured.The validated SenseWear� activity monitor was worn overthe right triceps for five consecutive days for approximately23 h a day by all groups5 as armbands were removed forbathing. Patients were provided with written instructionsfor care. Data collected were downloaded using the soft-ware (INNERVIEW professional version 6.0.0; BodyMedia,Pittsburgh, PA). METs were set as follows 0e3 sedentary,3e6 Moderate, �6 vigorous. In order to standardise physicalactivity for each participant, only those data defined ashaving collected �85% over the five days of prescribed timewere included for each time set (5days). The average sumover the times was used for data analysis.
Measurement of exercise capacityThe Incremental Shuttle Walk test (ISWT) was performed inaccordancewith standard recommendations aswas the 6minwalk test (6MWT).37,38 Minimal clinical important difference(MCID) for the 6MWT is 26m39 and the ISWT is 47.5m.40
Quality of lifeTwo quality of life measurements were recorded at eachtime point: The St George’s Respiratory Questionnaire(SGRQ) and the EuroQol (EQ-5D).41,42
Healthcare usePharmacy records from the year prior to the study and at thecompletionof theyear followupwereobtained forall subjectsand a record of the number of antibiotics and steroid coursesadministered for respiratory complaints were recorded. Thiswas interpreted as the number of exacerbations in that timeperiod, as defined by requiring a change in medication.
Statistical analysis
Data on 47 patients were entered and analysed using SPSS(PASW) version 18 for normal distribution using parametricand non-parametric tests with a statistical differencemeasured as a p-value of less than 0.05. The hypothesis thata significant change would occur in PA following PR wastested, where data were normally distributed, witha repeated measures ANOVA with Bonferroni adjusted pair-wise comparisons between (i) pre and post pulmonaryrehabilitation (week 0e7) and (ii) pre to short term followup (week 0 to week 20) for the total group. This was also
performed for the pre to 1 year follow up (week 0 to week52) in a subset (n Z 17). For non-normal data, Friedman’stest was used to compare median scores over the repeatedtime points. Wilcoxon Sign Rank tests with Bonferroniadjusted critical values were used for the pairwisecomparisons. It was not possible to power the study based onarmband data due to the large number of patients required;therefore, this study should be taken in the context of beinginvestigative in a real clinical Irish hospital setting.
Results
Of the 60 subjects who fulfilled in the inclusion/exclusioncriteria, 47 were recruited for pulmonary rehabilitation and45 received pulmonary rehabilitation; Data for 47 patientswere retained for intention to treat purposes. Thirteenpatients did not complete the course (w28% drop-out rate).Four patients did not attend for follow-up at threemonths. Aconvenient sample of 17 patients was re-assessed at 1 year.
Baseline characteristics
Baseline characteristics for patients at week 0, week 7 andweek 20 are presented in Table 2. Participants were olderadults who smoked approximately 340,000 cigarettes intheir lifetime. Slightly less than half were male with a meanFEV1 indicating severe obstruction. Subjects generally hadan overweight BMI, a poor exercise performance, andweakened inspiratory muscles at baseline. Moreover,quality of life was impaired, in particular the SGRQ domains‘Symptom’ and ‘Activity’. Subjects were sedentary,spending only 9% in activities equal or above the recom-mended 500MET/mins a day43 and only 36% of the 10,000recommended steps a day. A 98% compliance rate wasrecorded for wearing the armband over the averagedrecorded 5 days. Table 3 gives a breakdown of 17 patientswho were contacted at one year for reassessment.
Short term effects (Wk0-Wk7)
Short-term effects (N Z 30) (Table 2): Functional exerciseperformance increased significantly immediately after the7-week PR programme [Incremental Shuttle Walk test:32.8 � 42.3m, p < 0.001; 6MWT: 37.1 � 51.6m, p < 0.002]as well as inspiratory muscle strength [PiMax: �9.2 � 13.4cmH2O, p < 0.007]. There was a significant fall (improve-ment) in symptoms of breathlessness [mBorg score(�0.6 � 1.5, pZ 0.011) and in health-related quality of life[SGRQ total score: �8.1 � 10.6 points, p < 0.001; the EQ5D(p < 0.025)]. There was a significant decrease in TEE(�143 � 273 kcal, p Z 0.016). There was no change in theaverage number of daily steps, time spent sedentary ortime spent in active exercise at either time point afterrehabilitation compared to the baseline values.
Medium term effects (Wk 0eWk 20)
Medium term effects (NZ 30) (Table 2): PiMax was the onlyvariable to maintain a significant difference at theWk0eWk20 (p Z 0.003). All other variable appeared to
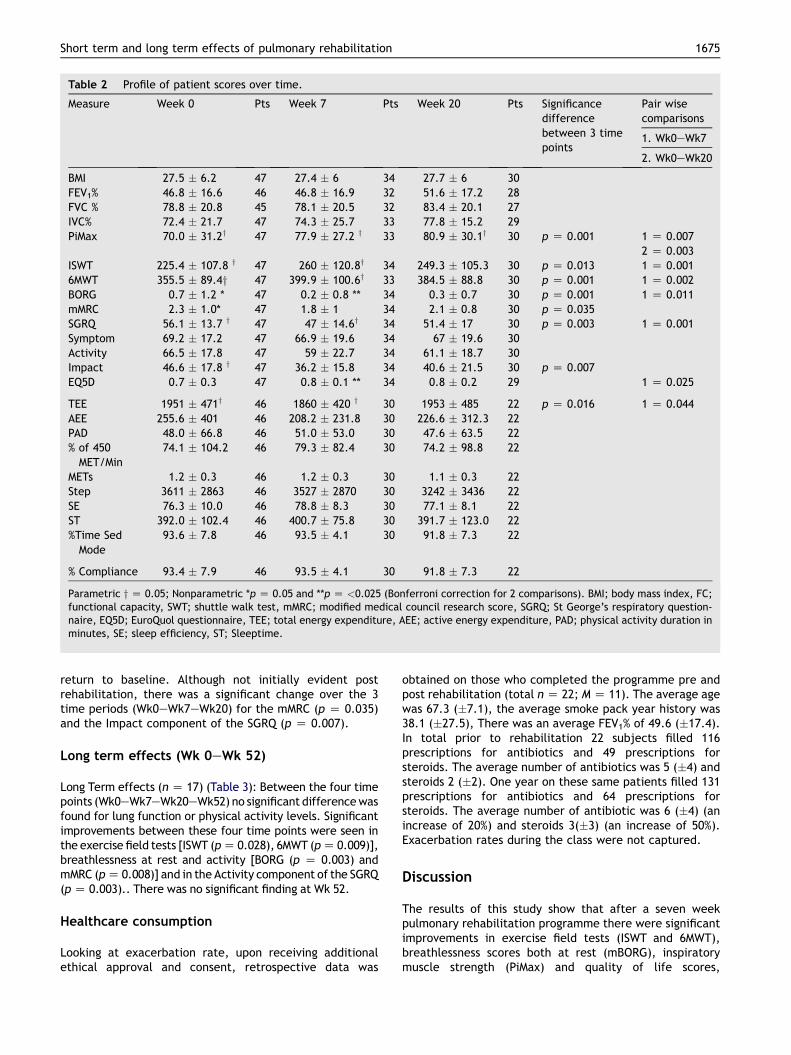
Table 2 Profile of patient scores over time.
Measure Week 0 Pts Week 7 Pts Week 20 Pts Significancedifferencebetween 3 timepoints
Pair wisecomparisons
1. Wk0eWk7
2. Wk0eWk20
BMI 27.5 � 6.2 47 27.4 � 6 34 27.7 � 6 30FEV1% 46.8 � 16.6 46 46.8 � 16.9 32 51.6 � 17.2 28FVC % 78.8 � 20.8 45 78.1 � 20.5 32 83.4 � 20.1 27IVC% 72.4 � 21.7 47 74.3 � 25.7 33 77.8 � 15.2 29PiMax 70.0 � 31.2y 47 77.9 � 27.2 y 33 80.9 � 30.1y 30 p Z 0.001 1 Z 0.007
2 Z 0.003ISWT 225.4 � 107.8 y 47 260 � 120.8y 34 249.3 � 105.3 30 p Z 0.013 1 Z 0.0016MWT 355.5 � 89.4y 47 399.9 � 100.6y 33 384.5 � 88.8 30 p Z 0.001 1 Z 0.002BORG 0.7 � 1.2 * 47 0.2 � 0.8 ** 34 0.3 � 0.7 30 p Z 0.001 1 Z 0.011mMRC 2.3 � 1.0* 47 1.8 � 1 34 2.1 � 0.8 30 p Z 0.035SGRQ 56.1 � 13.7 y 47 47 � 14.6y 34 51.4 � 17 30 p Z 0.003 1 Z 0.001Symptom 69.2 � 17.2 47 66.9 � 19.6 34 67 � 19.6 30Activity 66.5 � 17.8 47 59 � 22.7 34 61.1 � 18.7 30Impact 46.6 � 17.8 y 47 36.2 � 15.8 34 40.6 � 21.5 30 p Z 0.007EQ5D 0.7 � 0.3 47 0.8 � 0.1 ** 34 0.8 � 0.2 29 1 Z 0.025
TEE 1951 � 471y 46 1860 � 420 y 30 1953 � 485 22 p Z 0.016 1 Z 0.044AEE 255.6 � 401 46 208.2 � 231.8 30 226.6 � 312.3 22PAD 48.0 � 66.8 46 51.0 � 53.0 30 47.6 � 63.5 22% of 450MET/Min
74.1 � 104.2 46 79.3 � 82.4 30 74.2 � 98.8 22
METs 1.2 � 0.3 46 1.2 � 0.3 30 1.1 � 0.3 22Step 3611 � 2863 46 3527 � 2870 30 3242 � 3436 22SE 76.3 � 10.0 46 78.8 � 8.3 30 77.1 � 8.1 22ST 392.0 � 102.4 46 400.7 � 75.8 30 391.7 � 123.0 22%Time SedMode
93.6 � 7.8 46 93.5 � 4.1 30 91.8 � 7.3 22
% Compliance 93.4 � 7.9 46 93.5 � 4.1 30 91.8 � 7.3 22
Parametric y Z 0.05; Nonparametric *p Z 0.05 and **p Z <0.025 (Bonferroni correction for 2 comparisons). BMI; body mass index, FC;functional capacity, SWT; shuttle walk test, mMRC; modified medical council research score, SGRQ; St George’s respiratory question-naire, EQ5D; EuroQuol questionnaire, TEE; total energy expenditure, AEE; active energy expenditure, PAD; physical activity duration inminutes, SE; sleep efficiency, ST; Sleeptime.
Short term and long term effects of pulmonary rehabilitation 1675
return to baseline. Although not initially evident postrehabilitation, there was a significant change over the 3time periods (Wk0eWk7eWk20) for the mMRC (p Z 0.035)and the Impact component of the SGRQ (p Z 0.007).
Long term effects (Wk 0eWk 52)
Long Term effects (n Z 17) (Table 3): Between the four timepoints (Wk0eWk7eWk20eWk52) no significant differencewasfound for lung function or physical activity levels. Significantimprovements between these four time points were seen inthe exercise field tests [ISWT (pZ 0.028), 6MWT (pZ 0.009)],breathlessness at rest and activity [BORG (p Z 0.003) andmMRC (pZ 0.008)] and in the Activity component of the SGRQ(pZ 0.003).. There was no significant finding at Wk 52.
Healthcare consumption
Looking at exacerbation rate, upon receiving additionalethical approval and consent, retrospective data was
obtained on those who completed the programme pre andpost rehabilitation (total n Z 22; M Z 11). The average agewas 67.3 (�7.1), the average smoke pack year history was38.1 (�27.5), There was an average FEV1% of 49.6 (�17.4).In total prior to rehabilitation 22 subjects filled 116prescriptions for antibiotics and 49 prescriptions forsteroids. The average number of antibiotics was 5 (�4) andsteroids 2 (�2). One year on these same patients filled 131prescriptions for antibiotics and 64 prescriptions forsteroids. The average number of antibiotic was 6 (�4) (anincrease of 20%) and steroids 3(�3) (an increase of 50%).Exacerbation rates during the class were not captured.
Discussion
The results of this study show that after a seven weekpulmonary rehabilitation programme there were significantimprovements in exercise field tests (ISWT and 6MWT),breathlessness scores both at rest (mBORG), inspiratorymuscle strength (PiMax) and quality of life scores,
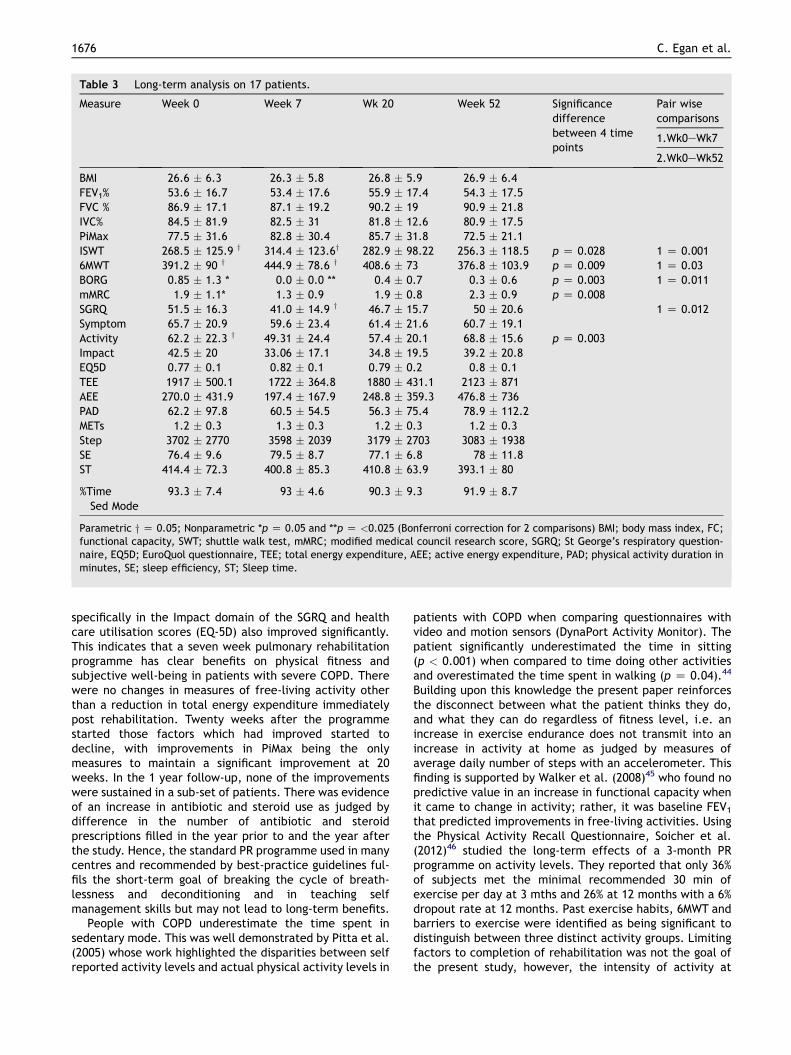
Table 3 Long-term analysis on 17 patients.
Measure Week 0 Week 7 Wk 20 Week 52 Significancedifferencebetween 4 timepoints
Pair wisecomparisons
1.Wk0eWk7
2.Wk0eWk52
BMI 26.6 � 6.3 26.3 � 5.8 26.8 � 5.9 26.9 � 6.4FEV1% 53.6 � 16.7 53.4 � 17.6 55.9 � 17.4 54.3 � 17.5FVC % 86.9 � 17.1 87.1 � 19.2 90.2 � 19 90.9 � 21.8IVC% 84.5 � 81.9 82.5 � 31 81.8 � 12.6 80.9 � 17.5PiMax 77.5 � 31.6 82.8 � 30.4 85.7 � 31.8 72.5 � 21.1ISWT 268.5 � 125.9 y 314.4 � 123.6y 282.9 � 98.22 256.3 � 118.5 p Z 0.028 1 Z 0.0016MWT 391.2 � 90 y 444.9 � 78.6 y 408.6 � 73 376.8 � 103.9 p Z 0.009 1 Z 0.03BORG 0.85 � 1.3 * 0.0 � 0.0 ** 0.4 � 0.7 0.3 � 0.6 p Z 0.003 1 Z 0.011mMRC 1.9 � 1.1* 1.3 � 0.9 1.9 � 0.8 2.3 � 0.9 p Z 0.008SGRQ 51.5 � 16.3 41.0 � 14.9 y 46.7 � 15.7 50 � 20.6 1 Z 0.012Symptom 65.7 � 20.9 59.6 � 23.4 61.4 � 21.6 60.7 � 19.1Activity 62.2 � 22.3 y 49.31 � 24.4 57.4 � 20.1 68.8 � 15.6 p Z 0.003Impact 42.5 � 20 33.06 � 17.1 34.8 � 19.5 39.2 � 20.8EQ5D 0.77 � 0.1 0.82 � 0.1 0.79 � 0.2 0.8 � 0.1TEE 1917 � 500.1 1722 � 364.8 1880 � 431.1 2123 � 871AEE 270.0 � 431.9 197.4 � 167.9 248.8 � 359.3 476.8 � 736PAD 62.2 � 97.8 60.5 � 54.5 56.3 � 75.4 78.9 � 112.2METs 1.2 � 0.3 1.3 � 0.3 1.2 � 0.3 1.2 � 0.3Step 3702 � 2770 3598 � 2039 3179 � 2703 3083 � 1938SE 76.4 � 9.6 79.5 � 8.7 77.1 � 6.8 78 � 11.8ST 414.4 � 72.3 400.8 � 85.3 410.8 � 63.9 393.1 � 80
%TimeSed Mode
93.3 � 7.4 93 � 4.6 90.3 � 9.3 91.9 � 8.7
Parametric y Z 0.05; Nonparametric *p Z 0.05 and **p Z <0.025 (Bonferroni correction for 2 comparisons) BMI; body mass index, FC;functional capacity, SWT; shuttle walk test, mMRC; modified medical council research score, SGRQ; St George’s respiratory question-naire, EQ5D; EuroQuol questionnaire, TEE; total energy expenditure, AEE; active energy expenditure, PAD; physical activity duration inminutes, SE; sleep efficiency, ST; Sleep time.
1676 C. Egan et al.
specifically in the Impact domain of the SGRQ and healthcare utilisation scores (EQ-5D) also improved significantly.This indicates that a seven week pulmonary rehabilitationprogramme has clear benefits on physical fitness andsubjective well-being in patients with severe COPD. Therewere no changes in measures of free-living activity otherthan a reduction in total energy expenditure immediatelypost rehabilitation. Twenty weeks after the programmestarted those factors which had improved started todecline, with improvements in PiMax being the onlymeasures to maintain a significant improvement at 20weeks. In the 1 year follow-up, none of the improvementswere sustained in a sub-set of patients. There was evidenceof an increase in antibiotic and steroid use as judged bydifference in the number of antibiotic and steroidprescriptions filled in the year prior to and the year afterthe study. Hence, the standard PR programme used in manycentres and recommended by best-practice guidelines ful-fils the short-term goal of breaking the cycle of breath-lessness and deconditioning and in teaching selfmanagement skills but may not lead to long-term benefits.
People with COPD underestimate the time spent insedentary mode. This was well demonstrated by Pitta et al.(2005) whose work highlighted the disparities between selfreported activity levels and actual physical activity levels in
patients with COPD when comparing questionnaires withvideo and motion sensors (DynaPort Activity Monitor). Thepatient significantly underestimated the time in sitting(p < 0.001) when compared to time doing other activitiesand overestimated the time spent in walking (p Z 0.04).44
Building upon this knowledge the present paper reinforcesthe disconnect between what the patient thinks they do,and what they can do regardless of fitness level, i.e. anincrease in exercise endurance does not transmit into anincrease in activity at home as judged by measures ofaverage daily number of steps with an accelerometer. Thisfinding is supported by Walker et al. (2008)45 who found nopredictive value in an increase in functional capacity whenit came to change in activity; rather, it was baseline FEV1
that predicted improvements in free-living activities. Usingthe Physical Activity Recall Questionnaire, Soicher et al.(2012)46 studied the long-term effects of a 3-month PRprogramme on activity levels. They reported that only 36%of subjects met the minimal recommended 30 min ofexercise per day at 3 mths and 26% at 12 months with a 6%dropout rate at 12 months. Past exercise habits, 6MWT andbarriers to exercise were identified as being significant todistinguish between three distinct activity groups. Limitingfactors to completion of rehabilitation was not the goal ofthe present study, however, the intensity of activity at

Short term and long term effects of pulmonary rehabilitation 1677
home was clearly not increased in those reassessed at oneyear in a group of 17 patients with an average FEV1pred �50%: i.e. baseline physical activity duration (PAD) at 3 METswas consistent wk0 (45%), wk20 (41%) and wk52 (44%).
Overall, the current study adds to a literature, moststudies present non-significant data on activity promotion,as reviewed by Casaburi and Ng.21,22
One possible explanation for a decrease in energyexpenditure after PR would be as a direct result of physi-ological changes resulting in less effort required for thesame activity. A reduction in breathlessness may be asa result of decreased effort and also perhaps through thedistraction from sensations of dyspnoea which occur duringexercise within a group or through the mood enhancingeffects of social interaction and exercise. We do notbelieve that the results of this study represent a sampleerror, firstly because there were improvements in theparameters that normally reflect a successful PR, andsecondly, there was a marked consistency of the activity inthe three follow up periods. The accelerometer used in thestudy has been widely used and validated in prospectivestudies of patients with COPD.5,47,48 Similar protocols wereused in these prior studies, including an extended durationof monitoring, avoiding holiday periods when socialbehaviour is different and by avoiding seasonal variations.49
Only data that was consistent with 85% of time worn wereincluded to exclude bias from inconsistent wearing of thedevice, which may underestimate activity. Hence, while weonly have one technique of identifying free-living activitythe technology is robust and reproducible.
The St.George’s Respiratory questionnaire41 is a diseasespecific questionnaire with three domains(Symptom,Activity and Impact) combining to give an overall QoL score.In the present study a significant improvement in thecomposite score was identified pre and post rehabiliationalong with a significant change in the Impact componentover a 3month period. Clinically relevant was that thecommon effect size exceeded the minimal clinical impor-tant difference (4) in both the Impact and Activitycomponents pre and post rehabilitation. These results areconsistent with the findings from a systematic reviewundertaken by Puhan50 who showed that Impact followedby Activity components improved over Symptoms aftera course of pulmonary rehabilitation. These two compo-nents could go some way to explain the increase in func-tional capacity and decreased effort (TEE) during dailyactivities in our small cohort of patients. The duration ofthe class (7Wks) and small number of patients may belimiting factors to larger improvements; however, wereenough to affect the cost of care as demonstrated by theimproved Utility Score in the EuroQol.
The breathlessness on activity scale (mMRC) did notdemonstrate an immediate effect post rehabilitationwhich isconsistent with the Activity Component of the SGRQ. Againthe short duration of class and small numbers may havecontributed to this finding. Also due to the absence ofa treadmill or walking track, the specificity of the trainingmay have been insufficient to meet the patients’ needs. Thishas since been addressed. In a separate study we havedemonstrated an improvement in this domain immediatelypost rehabilitationwith theadditionof acupuncture in a smallcohort of patients when compared to rehabilitation alone.
The combination of exercise, education and self-management strategies are the cornerstone of the successof pulmonary rehabilitation although the mechanismsinvolved in this improvement are still poorly under-stood.51,52 The indications are that while patients obtainbenefits in functional capacity compared to no interven-tion53 this is not sustained and does not carry over to theirhome life. Maintaining benefits after PR has proven to bea difficult undertaking and this study shows that withoutintervention benefits fade at 3months. Other studies thathave included strategies that include bimonthly phone callsto subjects did not prevent people from returning to theirold behaviour patterns.46 Identifying barriers and previousexercise behaviour patterns may be key to successfullyincreasing activity and functional levels in the long termbut any improvement may be limited to a subgroup ofpatients with better lung function and decreased exacer-bations rates.26,46 As evident by this study it would beerroneous to translate measures of physical activity intoestimates of physical fitness, capacity or actual function.Physical activity levels should instead be viewed in thecontext of lifestyle choice and behaviour patterns in orderto affect change.
It is possible that the study was underpowered, and thesubject number was small. Nonetheless, the standardmeasures of improvement seen in a clinical evaluation ofpulmonary rehabilitation were evident. It has been previ-ously demonstrated that a six month programme is requiredto alter patients freeliving activity levels26; therefore, theadditional goal for pulmonary rehabilitation to increaseactivity levels maybe unrealistic in their present format. Afurther limitation of the study is that the accelerometerdoes not inform as to possible changes in the subjectsability to undertake their activities of daily living. Activitiesof daily (ADL) living were not measured therefore it is notpossible to correlate ADLs with free-living activities or theother functional measures that improved.
Conclusion
In summary a traditional 7 week pulmonary rehabilitationprogramme increased physical capacity which in itself isvery worthwhile; however, these benefits were not sus-tained after one year. There was no increase in free-livingactivity.
Abbreviations
6MWT six minute walk testADL activity of daily livingBMI body mass indexCOPD chronic obstructive pulmonary diseaseEQ5D EuroQolFEV1 forced expiratory pressure in 1 sFVC forced vital capacityISWT incremental shuttle walk testIVC inspiratory vital capacitymBORG modified BORG

1678 C. Egan et al.
MCID minimal clinical importance differenceMETs metabolic equivalentmMRC modified medical research council scorePAD physical activity durationPiMax peak inspiratory muscle pressurePR pulmonary rehabilitationSE sleep efficiencySGRQ St. Georges Respiratory QuestionnaireST sleep timeTEE total energy expenditure
Conflict of interest statement
The pulmonary rehabilitation programme was supported bydonations of equipment provided to the COPD Outreachservice by Beaumont Foundation, Boehringer Ingleheim. Inparticular, this study was supported by the donation of theSenseWear armbands by SwordMedical Ltd. Without thisequipment the rehabilitation programme and study wouldnot be possible. The source of the donations had no role inthe study design, collection, analysis or interpretation ofthe data or in the decision to submit this paper to publi-cation. The authors Clare Egan reports no other conflicts ofinterest Brona Fullen reports no other conflicts of interestBrenda Deering reports no other conflicts of interest Mar-tijin Spruit reports no other conflicts of interest NiamhMcCormack reports no other conflicts of interest CatherineBlake reports no other conflicts of interest Richard Costelloreports no other conflicts of interest.
Richard Costello is the guarantor of the data in thispaper.
BD, CE conceived, designed and performed the analysisof the subjects and they were both involved in writing themanuscript. NMcC was involved in the design of the studyand in the collection of data. BF, CB and RC were involvedin the initial design, the data analysis interpretation of thedata and in the writing of the manuscript. MAS was involvedin revising and critically appraising it. All authors read andapproved of the final manuscript.
Competing interests
The pulmonary rehabilitation programme was supported bydonations of equipment provided to the COPD Outreachservice by Beaumont Foundation, Boehringer Ingleheim. Inparticular, this study was supported by the donation of theSenseWear armbands by SwordMedical Ltd. Without thisequipment the rehabilitation programme and study wouldnot be possible. The source of the donations had no role inthe study design, collection, analysis or interpretation ofthe data or in the decision to submit this paper topublication.
Richard Costello is the guarantor of the data in thispaper.
BD, CE conceived, designed and performed the analysisof the subjects and they were both involved in writing themanuscript. NMcC was involved in the design of the studyand in the collection of data. BF, CB and RC were involvedin the initial design, the data analysis interpretation of the
data and in the writing of the manuscript. MAS was involvedin revising and critically appraising it. All authors read andapproved of the final manuscript.
References
1. New Physical Activity guidance can help reduce risk of breast,colon cancers (www.who.int/mediacentre/new/notes/2011/world_cancer_da).
2. Arne M, Janson C, Janson S, Boman G, Lindqvist U, Berne C,Emtner M. Physical activity and quality of life in subjects withchronic disease: chronic obstructive pulmonary diseasecompared with rheumatoid arthritis and diabetes mellitus.Scand J Prim Health Care 2009;27(3):141e7.
3. Vorrink S, Kort H, Troosters T, Lammers JM. Level of dailyphysical activity in individuals with COPD compared withhealthy controls. Respir Res 2011;12(33):12e33.
4. Bohannon RW. Number of pedometer-assessed steps taken perday by adults: a descriptive meta-analysis. Phys Ther 2007;87(12):1642e50.
5. Watz H, Waschki B, Boehme C, Claussen M, Meyer T,Magnussen H. Extrapulmonary effects of chronic obstructivepulmonary disease on physical activity: a cross-sectional study.Am J Respir Crit Care Med 2008;177(7):743e51.
6. Watz H, Waschki B, Meyer T, Magnussen H. Physical activity inpatients with COPD. Eur Respir J 2009;33(2):262e72.
7. Troosters T, Sciurba F, Battaglia S, Langer D, Valluri SR,Martino L, Benzo R, Andre D, Weisman I, Decramer M. Physicalinactivity in patients with COPD, a controlled multi-centerpilot-study. Respir Med 2010;104(7):1005e11.
8. Garcia-Aymerich J, Serra I, Gomez FP, Farrero E, Balcells E,Rodriguez DA, de Batlle J, Gimeno E, Donaire-Gonzalez D,Orozco-Levi M, et al. Physical activity and clinical and func-tional status in COPD. Chest 2009;136(1):62e70.
9. Waschki B, Kirsten A, Holz O, Muller KC, Meyer T, Watz H,Magnussen H. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: a prospective cohortstudy. Chest 2011;140(2):331e42.
10. Nici L, Donner C, Wouters E, Zuwallack R, Ambrosino N,Bourbeau J, Carone M, Celli B, Engelen M, Fahy B, et al.American Thoracic Society/European respiratory SocietyStatement on pulmonary rehabilitation. Am J Respir Crit CareMed 2006;173(12):1390e413.
11. Ries AL, Kaplan RM, Limberg TM, Prewitt LM. Effects ofpulmonary rehabilitation on physiologic and psychosocialoutcomes in patients with chronic obstructive pulmonarydisease. Ann Intern Med 1995;122(11):823e32.
12. Singh SJ, Smith DL, Hyland ME, Morgan MD. A short outpatientpulmonary rehabilitation programme: immediate and longer-term effects on exercise performance and quality of life.Respir Med 1998;92(9):1146e54.
13. Maltais F, LeBlanc P, Simard C, Jobin J, Berube C, Bruneau J,Carrier L, Belleau R. Skeletal muscle adaptation to endurancetraining in patients with chronic obstructive pulmonarydisease. Am J Respir Crit Care Med 1996;154(2):442e7.
14. Troosters T, Gosselink R, Decramer M. Short- and long-termeffects of outpatient rehabilitation in patients with chronicobstructive pulmonary disease: a randomized trial. Am J Med2000;109(3):207e12.
15. Rossi G, Florini F, Romagnoli M, Bellantone T, Lucic S, Lugli D,Clini E. Length and clinical effectiveness of pulmonary reha-bilitation in outpatients with chronic airway obstruction. Chest2005;127(1):105e9.
16. Beauchamp MK, Janaudis-Ferreira T, Goldstein RS, Brooks D.Optimal duration of pulmonary rehabilitation for individualswith chronic obstructive pulmonary disease e a systematicreview. Chronic Respir Dis 2011;8(2):129e40.
Short term and long term effects of pulmonary rehabilitation 1679
17. Bernard S, LeBlanc P, Whittom F, Carrier G, Jobin J, Belleau R,Maltais F. Peripheral muscle weakness in patients with chronicobstructive pulmonary disease. Am J Respir Crit Care Med1998;158(2):629e34.
18. Seymour JM, Spruit MA, Hopkinson NS, Natanek SA, Man WD,Jackson A, Gosker HR, Schols AM, Moxham J, Polkey MI, et al.The prevalence of quadriceps weakness in COPD and the rela-tionship with disease severity. Eur Respir J 2010;36(1):81e8.
19. Crul T, Spruit MA, Gayan-Ramirez G, Quarck R, Gosselink R,Troosters T, Pitta F, Decramer M. Markers of inflammation anddisuse in vastus lateralis of chronic obstructive pulmonarydisease patients. Eur J Clin Invest 2007;37(11):897e904.
20. Bauman A, Craig CL. The place of physical activity in the WHOglobal strategy on Diet and physical activity. Int J Behav NutrPhys Act 2005;2:10.
21. Casaburi R. Activity promotion: a paradigm shift for chronicobstructive pulmonary disease therapeutics. Proc Am ThoracSoc 2012;8(4):334e7.
22. Cindy Ng LW, Mackney J, Jenkins S, Hill K. Does exercisetraining change physical activity in people with COPD? Asystematic review and meta-analysis. Chronic Respir Dis 2012;9(1):17e26.
23. Sedeno MF, Nault D, Hamd DH, Bourbeau J. A self-managementeducation program including an action plan for acute COPDexacerbations. COPD J Chronic Obstruct Pulm Dis 2009;6(5):352e8.
24. Pitta F, Troosters T, Probst VS, Spruit MA, Decramer M,Gosselink R. Quantifying physical activity in daily life withquestionnaires and motion sensors in COPD. Eur Respir J 2006;27(5):1040e55.
25. Moy ML, Matthess K, Stolzmann K, Reilly J, Garshick E. Free-living physical activity in COPD: assessment with accelerom-eter and activity checklist. J Rehabil Res Dev 2009;46(2):277e86.
26. Pitta F, Troosters T, Probst VS, Langer D, Decramer M,Gosselink R. Are patients with COPD more active afterpulmonary rehabilitation? Chest 2008;134(2):273e80.
27. Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P,Fukuchi Y, Jenkins C, Rodriguez-Roisin R, van Weel C, et al.Global strategy for the diagnosis, management, and preventionof chronic obstructive pulmonary disease: GOLD executivesummary. Am J Respir Crit Care Med 2007;176(6):532e55.
28. Singh SJ, Morgan MD, Hardman AE, Rowe C, Bardsley PA.Comparison of oxygen uptake during a conventional treadmilltest and the shuttle walking test in chronic airflow limitation.Eur Respir J 1994;7(11):2016e20.
29. Revill SM, Morgan MD, Singh SJ, Williams J, Hardman AE. Theendurance shuttle walk: a new field test for the assessment ofendurance capacity in chronic obstructive pulmonary disease.Thorax 1999;54(3):213e22.
30. Mejia R, Ward J, Lentine T, Mahler DA. Target dyspnea ratingspredict expected oxygen consumption as well as target heartrate values. J Cardiopulmonary Rehabil Prev 2000;20(2):133.
31. Wilson SH, Cooke NT, Edwards RH, Spiro SG. Predicted normalvalues for maximal respiratory pressures in caucasian adultsand children. Thorax 1984;39(7):535e8.
32. Heijdra Y, Dekhuijzen P, van Herwaarden C, Folgering H.Nocturnal saturation improves by target-flow inspiratorymuscle training in patients with COPD. Am J Respir Crit CareMed 1996;153(1):260e5.
33. McCormack N, Deering B, Costello R,GG. Assessment of theimpact of a ‘Respiratory passport’ for patients with chronicobstructive pulmonary disease (COPD). Irish J Med Sci 2009;178(11 Supp):S436.
34. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW,Wedzicha JA. Usefulness of the Medical Research Council(MRC) dyspnoea scale as a measure of disability in patients
with chronic obstructive pulmonary disease. Thorax 1999;54(7):581e6.
35. Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R,Yernault JC. Lung volumes and forced ventilatory flows. Reportworking Party Standardization of lung function tests, EuropeanCommunity for Steel and Coal. Official Statement of theEuropean respiratory Society. Eur Respir J Suppl 1993;16:5e40.
36. Esteghamati A, Khalilzadeh O, Rashidi A, Meysamie A,Haghazali M, Asgari F, Abbasi M, Rastad S, Gouya MM. Associ-ation between physical activity and insulin resistance in Iranianadults: National Surveillance of risk factors of non-Communicable diseases (SuRFNCD-2007). Prev Med 2009;49(5):402e6.
37. Singh SJ, Morgan MD, Scott S, Walters D, Hardman AE. Devel-opment of a shuttle walking test of disability in patients withchronic airways obstruction. Thorax 1992;47(12):1019e24.
38. ATS: ATS Statement. Guidelines for the six-minute walk test.Am J Respir Crit Care Med 2002;166(1):111e7.
39. Puhan MA, Chandra D, Mosenifar Z, Ries A, Make B, Hansel NN,Wise RA, Sciurba F. The minimal important difference ofexercise tests in severe COPD. Eur Respir J 2011;37(4):784e90.
40. Singh SJ, Jones PW, Evans R, Morgan MDL. Minimum clinicallyimportant improvement for the incremental shuttle walkingtest. Thorax 2008;63(9):775e7.
41. Jones PW. St. George’s respiratory questionnaire: MCID. COPD2005;2(1):75e9.
42. Rabin R, de Charro F. EQ-5D: a measure of health status fromthe EuroQol Group. Ann Med 2001;33(5):337e43.
43. Physical Activity Guidelines for Americans. http://wwwhealthgov/paguidelines/guidelines/chapter5aspx.
44. Pitta F, Troosters T, Spruit MA, Probst VS, Decramer M,Gosselink R. Characteristics of physical activities in daily life inchronic obstructive pulmonary disease. Am J Respir Crit CareMed 2005;171(9):972e7.
45. Walker PP, Burnett A, Flavahan PW, Calverley PMA. Lower Limbactivity and its determinants in chronic obstructive pulmonarydisease. Thorax 2008.
46. Soicher JE, Mayo NE, Gauvin L, Hanley JA, Bernard S, Maltais F,Bourbeau J. Trajectories of endurance activity followingpulmonary rehabilitation in COPD patients. Eur Respir J 2012;39(2):272e8.
47. St-Onge M, Mignault D, Allison DB, Rabasa-Lhoret Rm. Evalua-tion of a portable device to measure daily energy expenditurein free-living adults. Am J Clin Nutr 2007;85(3):742e9.
48. Waschki B, Spruit MA, Watz H, Albert PS, Shrikrishna D,Groenen M, Smith C, Man WD, Tal-Singer R, Edwards LD, et al.Physical activity monitoring in COPD: compliance and associ-ations with clinical characteristics in a multicenter study.Respir Med 2011;106(4):522e30.
49. Sewell L, Singh SJ, Williams JE, Morgan MD. Seasonal variationsaffect physical activity and pulmonary rehabilitationoutcomes. J Cardiopulm Rehabil Prev 2010;30(5):329e33.
50. Puhan M, Scharplatz M Torrsters, Steurer. Respiratory rehabil-itation after acute exacerbation of COPD may reduce risk forreadmission and mortality e a systematic review. Respir Res2005;6(54), http://respiratory-research.com/content/6/1/54.
51. Casaburi R, ZuWallack R. Pulmonary rehabilitation formanagement of chronic obstructive pulmonary disease. N EnglJ Med 2009;360(13):1329e35.
52. Nici L, Raskin J, Rochester CL, Bourbeau JC, Carlin BW,Casaburi R, Celli BR, Cote C, Crouch RH, Diez-Morales LF, et al.Pulmonary rehabilitation: what we know and what we need toknow. J Cardiopulm Rehabil Prev 2009;29(3):141e51.
53. Deering BM, Fullen B, Egan C, McCormack N, Kelly E, Pender M,Costello RW. Acupuncture as an adjunct to pulmonary reha-bilitation. J Cardiopulmonary Rehabil Prev 2011;31(6):392e9.