Embed Size (px)
Citation preview

Resuscitation (2007) 74, 83—89
CLINICAL PAPER
Significant factors in predicting sustained ROSC inpaediatric patients with traumatic out-of-hospitalcardiac arrest admitted to the emergencydepartment�
Yan-Ren Lina, Han-Ping Wua,b,e,∗, Chin-Yi Huangc, Yu-Jun Changd,Ching-Yuang Linb,e, Chu-Chung Choua
a Department of Emergency Medicine, Changhua Christian Hospital, 135 Nanshsiao Street,Changhua 500, Taiwanb Division of Paediatric Emergency and Critical Care Medicine, Department of Paediatrics,Changhua Christian Hospital, Changhua, Taiwanc Evidence Base Medicine Center, Changhua Christian Hospital, Changhua, Taiwand Laboratory of Epidemiology and Biostatistics, Changhua Christian Hospital, Changhua, Taiwane Institute of Medical Research, Chang Jung Christian University, Changhua, Taiwan
Received 4 August 2006; received in revised form 5 November 2006; accepted 10 November 2006
KEYWORDSOut-of-hospital cardiacarrest;Predict;Paediatric;Sustained ROSC
SummaryBackground: Paediatric patients with out-of-hospital cardiac arrest (OHCA) due totrauma pose difficult challenges in resuscitation. Trauma is a major cause of OHCAin children. The aim of this study was to determine which factors were related topredicting a sustained return of spontaneous circulation (ROSC) in paediatric OHCApatients with trauma.Method: This retrospective study comprised 115 paediatric patients (56 traumaticand 59 non-traumatic OHCA patients) aged younger than 18 years who had beenadmitted to the emergency department (ED) from January 2000 to December 2004.We analysed the demographic data and the factors that may have influenced sus-tained ROSC in the group of OHCA paediatric patients with trauma. The non-trauma
group was established as a control group. Survival analysis was used to compare dif-ferences in survival rate between trauma and non-trauma OHCA patients. Receiveroperating characteristic (ROC) analysis was used to determine the significant in-hospital CPR duration related to sustained ROSC.� A Spanish translated version of the summary of this article appears as Appendix in the final online version at10.1016/j.resuscitation.2006.11.022.
∗ Corresponding author at: Department of Emergency Medicine, Changhua Christian Hospital, 135 Nanshsiao Street, Changhua500, Taiwan. Tel.: +886 4 7238595x1034; fax: +886 4 7289233.
E-mail address: [email protected] (H.-P. Wu).
0300-9572/$ — see front matter © 2006 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.resuscitation.2006.11.022

84
Results: Initial cardiac rhythCPR (P < 0.001) were significsustained ROSC than those wanalysis, OHCA children withchildren as the interval fromROC analysis, the cut-off vapaediatric patients with trauConclusion: Several significain the OHCA paediatric patihospital CPR may have to be
td.
cTaOoiafinnhslia(
M
Ppattt(fcaupicatcs
circulation to return.© 2006 Elsevier Ireland L
Introduction
Adult patients who suffer from out-of-hospital car-diac arrest have a low chance of survival.1—7
In addition, out-of-hospital cardiac arrest (OHCA)patients pose difficult challenges in children foremergency department (ED) doctors because of thehigh mortality rate.8—12 Predictors of an increasedchance of sustained return of spontaneous cir-culation (ROSC) in adults include initial cardiacrhythm, bystander BLS, a short interval from sceneto hospital and early defibrillation.2,13—19 However,predictors for sustained ROSC in children remainunclear.
Patients with OHCA have different aetiolo-gies and require different management strategies.Analysing the factors related to sustained ROSC willhelp ED primary clinicians to evaluate the condi-tion and prognosis of OHCA paediatric patients withtrauma. It is unclear which factors are related topredicting sustained ROSC in children. In the ED,children with OHCA can be initially categorised intotrauma and non-trauma groups. Trauma is a majorcause of death.20 In this study, we aimed to deter-mine which significant factors can predict sustainedROSC in OHCA paediatric patients with trauma inthe ED.
Materials and methods
Patient population
This retrospective study was conducted from Jan-uary 2000 to December 2004. We reviewed thehospital records of 115 OHCA paediatric patients(56 traumatic and 59 non-traumatic OHCA patients)aged younger than 18 years, who had been admit-
ted to the emergency department at the ChanghuaChristian Hospital, a 1800-bed medical centre inTaiwan. The condition of OHCA patients was clas-sified as either trauma or non-trauma, based onlsf
Y.-R. Lin et al.
m on arrival (P = 0.005) and the duration of in-hospitalant factors. Patients with PEA or VF had higher rate ofith asystole (PEA: P = 0.003, VF: P = 0.03). In the survivaltrauma had a lower chance of survival than non-traumathe scene to the ER increased (P = 0.008). Based on thelues of in-hospital CPR duration were 25 min in OHCAma.nt factors relating to sustained ROSC were determined
ents with trauma; most importantly, we found that in-performed for at least 25 min to enable a spontaneous
All rights reserved.
linical assessment and bystander information.rauma OHCA in our study was defined as cardiacrrest which occurred after trauma; non-traumaHCA was defined as cardiac arrest due to causesther than trauma. The causes of trauma OHCAn this study were due to traffic accidents, fallsnd child abuse. Trauma OHCA patients wereurther divided into four main groups accord-ng to the main site of trauma: (1) head andeck injury (intracranial haemorrhage, subarach-oid haemorrhage, epidural haemorrhage, subduralaemorrhage, skull bone fracture and cervical-pine injury, etc.). (2) Abdominal injury (spleen,iver and pancreas or other intra abdominal organnjury, etc.), (3) thoracic injury (haemothoraxnd/or pneumothorax, etc.), (4) multiple traumatwo or more injuries).
ethods
re-hospital information was obtained from theublic emergency medical services (EMS) recordsnd included the time the call was received, theime of arrival and departure from the scene,he time the patient arrived at the ED, andhe duration of pre-hospital basic life supportBLS). In the study, we defined the ‘‘the periodrom scene to hospital’’ as the time from theall was received to the time the ambulancerrived at the ED. Patients presenting to EDnderwent resuscitation according to the advancedaediatric life support (APLS) protocols: trachealntubation, external chest compression, fluid resus-itation, vasopressors, direct-current cardioversionnd antiarrhythmic medications. In our study, sus-ained ROSC was deemed to have occurred whenhest compressions were not required for 20 con-ecutive minutes and signs of a circulation persist.3
In the trauma OHCA group, we analysed the fol-owing factors to determine if they had influencedustained ROSC: (1) demographic data gatheredrom the ED sheets including initial vital signs, age,

S aed
afBotttpoCvg
wmiepmlpapabtoaaraacIRg
S
DFaawmumavcubcOht
bP
R
Dw
Dc(sSbtEtwppim(Tltwtpo((
Rp
OrSrfiorrttCa(
ignificant factors in predicting sustained ROSC in p
nd sex, (2) mode of transportation, (3) the periodrom scene to hospital, (4) whether pre-hospitalLS had been performed, (5) initial cardiac rhythmn presentation to the ED, (6) the main site ofrauma, (7) type of trauma (blunt or penetratingrauma) and (8) the duration of in-hospital CPR. Inhe non-trauma OHCA group, we also recorded theeriod from scene to hospital and whether patientsbtained sustained ROSC or not after in-hospitalPR from the ED sheets. The data was used for sur-ival analysis between the trauma and non-traumaroups.
Initial cardiac rhythm on presentation to the EDas obtained from the electrocardiographic (ECG)onitor immediately after arrival. The rhythms
ncluded ventricular fibrillation (VF), pulselesslectrical activity (PEA) and asystole. VF includesatients with pulseless ventricular tachycardia. Theode of transportation to our ED included ambu-
ances and private vehicles. All OHCA paediatricatients were divided into five groups according toge: infant (1 month—1 year), toddler (1—3 years),reschool (4—5 years), school age (6—12 years), anddolescent (13—18 years). After sustained ROSC hadeen obtained, trauma patients were admitted tohe surgical intensive care unit (SICU). The outcomef patients who were resuscitated successfully werenalysed for significant prognostic factors. Survivalnalysis was done to compare the different survivalates between the trauma and non-trauma groupsccording to the period from scene to hospital. Inddition, receiver operating characteristic (ROC)urve for the duration of in-hospital CPR was drawn.n-hospital CPR duration related to sustainedOSC was determined statistically in the traumaroup.
tatistical methods
ata were analysed by the, Pearson Chi-square,isher’s exact test, stepwise logistic regressionnalysis, Log Rank test and receiver operating char-cteristic (ROC) curve. Distribution of variablesere reported as percentages, mean ± S.D., andedian. A stepwise logistic regression analysis was
sed to select independent predictors to dichoto-ous dependent variables between sustained ROSC
nd non-sustained ROSC patients. Results of sur-ival analysis were expressed by Log Rank and 95%onfidence interval (CI). The Log Rank test wassed in survival analysis to compare the differenceetween trauma and non-trauma groups. The ROC
urve for the duration of in-hospital CPR was drawn.n the basis of sensitivity, specificity, positive like-ood ratio (LR+), and negative likehood ratio (LR−),he best duration of in-hospital CPR was determined1t(r
iatric patients 85
y the cut-off points and LRs from ROC curve. A-value < 0.05 was regarded as significant.
esults
emographics of OHCA paediatric patientsith trauma
uring the 5-year study period, a total of 56 OHCAhildren with trauma aged younger than 18 yearsmean, 11.26 ± 6.46 years) were enrolled in thetudy. Among them, 22 were girls and 34 were boys.ustained ROSC was obtained in 20 OHCA patients,ut only one was eventually discharged from hospi-al. After implementation of APLS protocols in theD, the percentage of sustained ROSC was 35.7% inrauma patients; however, the total mortality rateas 98.2%. The mean period from scene to hos-ital was 18.41 ± 8.31 min; the mean duration ofre-hospital BLS was 3.48 ± 4.10 min; and the meann-hospital CPR duration was 27.75 ± 15.58 min. Theost common initial cardiac rhythm was asystole
60.7%), followed by PEA (26.8%) and VF (12.5%).he percentage of patients transported by ambu-
ance crew (two EMTs) was 82.1% while 17.9% wereransported by family members. Pre-hospital BLSas performed in 41 patients (73.2%). The trauma
ype included blunt trauma occurred in 94.6% andenetrating trauma in 5.4%. The injuries consistedf head and neck injury (51.8%), abdominal trauma19.6%), thoracic injury (19.6%), multiple trauma8.9%) (Table 1).
elated factors of sustained ROSC in OHCAaediatric patients with trauma
f the 56 traumatic patients, 20 (35.7%) wereevived by initial in-hospital CPR (ROSC ≥ 20 min).ustained ROSC was related to initial cardiachythm (P = 0.005) (Table 2). Patients who suf-ered from thoracic injury and head and necknjury had a lower survival rate than patients withther injuries. Furthermore, multivariate logisticegression analysis revealed that initial cardiachythm and the duration of in-hospital CPR werehe most significant factors associated with sus-ained ROSC (P < 0.001). The success rate of initialPR was higher in patients with PEA (P = 0.003)nd VF (P = 0.03) than in patients with asystoleTable 3).
The interval from scene to hospital was
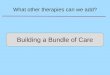
5.00 ± 8.62 min in sustained ROSC in children withrauma versus 20.36 ± 7.77 min in the remainderP = 0.15). As shown in Figure 1, survival analysisevealed a significant difference in the inter-
86 Y.-R. Lin et al.
Table 1 Demography of the traumatic OHCA paedi-atric patients
Traumatic OHCAchildren (N = 56)
No. %
GenderFemale 22 39.3Male 34 60.7
Age (y/o) 11.26 ± 6.46
Sustained ROSCa
Yes 20 35.7No 36 64.3
Initial cardiac rhythmAsystole 34 60.7PEA 15 26.8VFb 7 12.5
Mode of transportationFamily 10 17.9EMTs 46 82.1
Pre-hospital BLSYes 41 73.2No 15 26.8
Main site of traumaHead and neck injury 29 51.8Abdominal trauma 11 19.6Thoracic injury 11 19.6Multiple trauma 5 8.9
Type of traumaBlunt trauma 53 94.6Penetrating trauma 3 5.4
The period from scene to hospital 18.41 ± 8.31 min (5)c
The duration of pre-hospital BLS 3.48 ± 4.10 min (4)c
EMTs: emergency medical technicians, BLS: basic lifesupport.
Table 2 Related factors associated with sustainedROSC in traumatic OHCA paediatric patients (N = 56)
Sustained ROSCa
Success Failure P-value
GenderFemale 9 13 0.514Male 11 23
Initial cardiac rhythmAsystole 7 27 0.005PEA 10 5VF 3 4
Mode of transportationFamily 5 5 0.468EMTs 15 31
Pre-hospital BLSYes 15 26 0.822No 5 10
AgeInfant 2 1 0.257Toddler 3 8Preschool 0 1School age 2 10Adolescence 13 16
Main site of traumaHead and neck injury 11 18 0.582Abdominal trauma 5 6Thoracic injury 2 9Multiple trauma 2 3
Type of traumaBlunt trauma 19 34 1.000Penetrating trauma 1 2a Sustained ROSC: ROSC� 20 min.
oa
a Sustained ROSC: ROSC� 20 min.b VF includes patients with pulse less VT.c Number of patients with missing information.
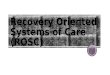
val from scene to hospital between the traumaand non-trauma groups (P = 0.008). The dura-tion of in-hospital CPR was analysed by ROCcurves (Figure 2). In the trauma group, the cut-
t207
Table 3 Multivariate logistic regression analysis of the rpaediatric patients
S.E.
Initial cardiac rhythmPEA 0.83VF 1.13Duration of in-hospital CPR 0.04
S.E., standard error; CI, confidence interval, OR: Odds ratio.a P-value = 0.003 for the comparison between asystole and PEA.b P-value = 0.03 for the comparison between asystole and VF.
ff values of in-hospital CPR duration by ROCnalysis had AUCs significantly greater than 0.5;he best cut-off duration of in-hospital CPR was5 min (AUC = 0.883 (95% CI 0.769—0.953), Sens
.90 (95% CI 68.3—98.5), Spec. 0.86 (95% CI0.5—95.3)).elated factors for sustained ROSC in traumatic OHCA
OR 95% CI P-value
0.0275.91 1.16—30.12 0.003a
11.54 1.27—105.13 0.03b
0.89 0.83—0.95 0.001

Significant factors in predicting sustained ROSC in paediatric patients 87
Figure 1 Survival rate analysis for the period from scene to h
Prognosis of OHCA patients with traumawho survived more than 7 days
Only one patient survived more than 7 days. He hada spleen laceration and massive internal bleeding,and underwent emergency splenectomy. After criti-cal care in our SICU, this child was discharged homeon day 19.
Discussion
Initial CPR performed on OHCA paediatric patientswith trauma is seldom successful.8,9,12,21—23 Sev-eral studies have revealed that children who suffer
Figure 2 Receiver operating characteristic curves for in-hospital CPR duration in the traumatic OHCA paediatricpatients.
Otdthpts
wA((rsdpat(la
tp(Rnttdpicctdp
ospital (P = 0.008). Survival event means ROSC� 20 min.
HCA due to trauma have a low chance of reachinghe hospital alive and an even lower chance of beingischarged from hospital (2—8%).8,9,12,21—23 Predic-ors for ROSC in adult OHCA have been defined;owever predictors for sustained ROSC in OHCAaediatric patients with trauma are not known. Inhis study, we determined the factors related toustained ROSC in these patients.
The first factor associated with sustained ROSCas the initial cardiac rhythm in the ED (P = 0.005).systole was the predominant initial cardiac rhythm60.7%), followed by PEA (26.8%) and then VF12.5%). Multivariate logistic regression analysisevealed that PEA and VF were better predictors ofuccessful CPR outcome than asystole. Primary EDoctors should keep in mind that paediatric traumaatients with VF or PEA have higher survival ratesfter CPR; therefore, accuracy and speed in readinghe ECG and providing the appropriate managementfor example, CPR in asystole or PEA; early defibril-ation in VF or pulseless VT) are important beforend during resuscitation.
In our study, blunt trauma was the most type ofrauma. Patients with head and neck injury com-rised the majority of those in the trauma group51.8%), and none survived to discharge. SustainedOSC can be obtained in patients with head andeck injury after performing in-hospital CPR, buthe prognosis is still very poor. Our findings supporthose reported in several previous studies whichemonstrated that the survival rate of paediatricatients with cardiac arrest secondary to traumas poor, especially in patients with head and spinalord injury.8,21 For example, Fisher et al. studied 65
hildren who suffered cardiac arrest following bluntrauma, and noted that all but one of these patientsied despite attempts at resuscitation. Ninety-fourercent died within the first 24 h; the only survivor
t2
C
SRwht
C
T
R
1
1
88
was discharged in a vegetative state. Further-more, severe head injury resulting in brain deathwas a leading cause of mortality.9 In our study,although the survival rate was very low, sustainedROSC was obtained in 35.7% head and neck injurypatients. This indicates that after primary survey(primary A.B.C.D.E.: airway, breathing, circulation,disability, exposure) of OHCA children with trauma,a thorough head-to-toe secondary survey shouldbe performed rapidly. In addition, patients shouldreceive X ray or computed tomography scan foraccurate diagnosis of head and neck injury withoutdelay after a brief neurological examination. Fur-thermore, sustained ROSC may serve as a bridgeto possible organ donation.9 If organ donation isexpected, sustained ROSC is necessary to preventorgan failure before surgical intervention.
Time-related factors influenced the outcome ofCPR in OHCA paediatric patients in our study. Theperiod from scene to hospital was shorter for CPRpatients who survived than for those who died(14.17 ± 7.42 min versus 20.06 ± 7.48 min). Survivalanalysis revealed that the sustained ROSC rate were80% in the traumatic group and 92% in the non-traumatic group on the 15th min. However, thesustained ROSC rate decreased to 8% in traumaticand 60% in non-traumatic groups on the 30th min.This analysis indicates that the two survival curvesfell once the period was prolonged, especially inthe trauma group (P = 0.008). We believe that theperiod from scene to hospital did influence sur-vival in both groups. Decreasing the period fromscene to hospital may improve the sustained ROSCrate in the ED, especially in OHCA children withtrauma.
In-hospital CPR must be performed on paediatricOHCA patients by primary clinicians in the ED. Pre-vious studies reporting on children with apnoea orno palpable pulse (or both) who presented to ED,concluded that a shorter duration of CPR in ED indi-cated a higher survival rate.10 However, they didnot mention the duration of CPR which resultedin sustained ROSC in OHCA children. In our study,we analysed the correlation between in-hospitalCPR duration and sustained ROSC rate. ROC analysisrevealed that the cut-off point of in-hospital CPRfor sustained ROSC was 25 min. The cut-off pointof 25 min had a sensitivity of 90% and a specificityof 86%. This indicates that in 90% of patients withsustained ROSC, CPR was performed in-hospital forless than 25 min. It also shows that 86.1% of patientswithout sustained ROSC do not return to achieve
ROSC even after more than 25 min of in-hospitalCPR. However, clinically, some patients in our studyreceived more than 25 min of in-hospital CPR andregained sustained ROSC. Therefore, we suggest1
Y.-R. Lin et al.
hat in-hospital CPR should be done for at least5 min in traumatic OHCA children.
onclusion
everal significant factors related to sustainedOSC were determined in OHCA paediatric patientsith trauma; most importantly, we found that in-ospital CPR should be performed for at least 25 mino allow for a spontaneous circulation to return.
onflict of interest
here is no conflict of interest related to this study.
eferences
1. Herlitz J, Engdahl J, Svensson L, et al. Factors associatedwith an increased chance of survival among patients suf-fering from an out-of-hospital cardiac arrest in a nationalperspective in Sweden. Am Heart J 2005;149:61—6.
2. Lin JN, Lin TJ, Kuo MC, et al. Analysis of factorsassociated with successful cardiopulmonary resuscitationin non-traumatic dead-on-arrival patients in emergencydepartment. Kaohsiung J Med Sci 2002;18:84—90.
3. Jacobs I, Nadkarni V, Bahr J, et al. Cardiac arrest and car-diopulmonary resuscitation outcome reports: update andsimplification of the Utstein templates for resuscitationregistries. A statement for healthcare professionals froma task force of the International Liaison Committee onResuscitation (American Heart Association, European Resus-citation Council, Australian Resuscitation Council, NewZealand Resuscitation Council, Heart and Stroke Foundationof Canada, Inter American Heart Foundation, ResuscitationCouncil of Southern Africa). Resuscitation 2004;63:233—49.
4. Holmberg M, Holmberg S, Herlitz J, et al. Survival aftercardiac arrest outside hospital in Sweden. Resuscitation1998;36:29—36.
5. Soo LH, Gray D, Young T, et al. Resuscitation from out-of-hospital cardiac arrest: is survival dependent on who isavailable at the scene? Heart 1999;81:47—52.
6. Bunch TJ, Hammill SC, White RD. Outcomes after ventricu-lar fibrillation out-of-hospital cardiac arrest: expanding thechain of survival. Mayo Clin Proc 2005;80:774—82.
7. Herlitz J, Bahr J, Fischer M, et al. Resuscitation in Europe: atale of five European regions. Resuscitation 1999;41:121—31.
8. Suominen P, Rasanen J, Kivioja A. Efficacy of cardiopul-monary resuscitation in pulseless paediatric traumaticpatients. Resuscitation 1998;36:9—13.
9. Fisher B, Worthen M. Cardiac arrest induced by blunt traumain children. Pediatr Emerg Care 1999;15:274—6.
0. Kuisma M, Suominen P, Korpela R. Paediatric out-of-hospitalcardiac arrests—–epidemiology and outcome. Resuscitation1995;30:141—50.
1. Herlitz J, Engdahl J, Svensson L, et al. Characteristics and
outcome among children suffering from out-of-hospital car-diac arrest in Sweden. Resuscitation 2005;64:37—40.2. Hazinski MF, Chahine AA, Holcomb GW, et al. Outcome ofcardiovascular collapse in pediatric blunt trauma. Ann EmergMed 1994 Jun;23:1229—35.

S aed
1
1
1
1
1
1
1
2
2
2
ignificant factors in predicting sustained ROSC in p
3. Bunch TJ, West CP, Packer DL, et al. Admission predictorsof in-hospital mortality and subsequent long-term outcomein survivors of ventricular fibrillation out-of-hospital cardiacarrest: a population-based study. Cardiology 2004;102:41—7.
4. Jacobs IG, Finn JC, Oxer HF, et al. CPR before defibrillationin out-of-hospital cardiac arrest: a randomized trial. EmergMed Australas 2005;17:39—45.
5. Bunch TJ, White RD, Friedman PA, et al. Trends in treatedventricular fibrillation out-of-hospital cardiac arrest: a 17-year population-based study. Heart Rhythm 2004;1:255—9.
6. Weaver WD, Cobb LA, Hallstrom AP, et al. Factors influenc-ing survival after out-of-hospital cardiac arrest. J Am CollCardiol 1986;7:752—7.
7. Herlitz J, Eek M, Engdahl J, et al. Factors at resuscitation andoutcome among patients suffering from out-of-hospital car-diac arrest in relation to age. Resuscitation 2003;58:309—17.
8. Herlitz J, Svensson L, Engdahl J, et al. Association betweeninterval between call for ambulance and return of spon-
2
iatric patients 89
taneous circulation and survival in out-of-hospital cardiacarrest. Resuscitation 2006;71:40—6.
9. Gray WA, Capone RJ, Most AS, et al. Unsuccessful emer-gency medical resuscitation-are continued efforts in theemergency department justified? N Engl J Med 1991;325:1393—8.
0. Hickey RW, Cohen DM, Strausbaugh S, et al. Pediatricpatients requiring CPR in the prehospital setting. Ann EmergMed 1995;25:495—501.
1. Calkins CM, Bensard DD, Partrick DA, et al. A critical analysisof outcome for children sustaining cardiac arrest after blunttrauma. J Pediatr Surg 2002;37:180—4.
2. Schindler MB, Bohn D, Cox PN, et al. Out come of out-
of-cardiac or respiratory arrest in children. N Engl J Med1996;335:1473—9.3. Pitetti R, Glustein JZ, Bhende MS. Prehospital care and out-come of pediatric out-of-hospital cardiac arrest. PrehospEmerg Care 2002;6:283—90.