-
8/13/2019 Sindroame renale
1/25
Approach to the patient with renal
disease
Dr. Silvia Spnu
-
8/13/2019 Sindroame renale
2/25
Reminder
Syndrome= an association of signs and symptomswhich form
together a characteristic morbid frame,
which can be observed in different diseases.
Disease= a morbid entitycharacterized usually by
at least twoof these criteria:
recognized etiologic agent!s"
identifiable group of signs and symptoms
consistent pathological alterations.
-
8/13/2019 Sindroame renale
3/25
Identification of renal disease
#enourinary signs$symptoms
%rinary or blood abnormalities identified occasionally or by
screening
&bnormal renourinary imaging studies !%S, '(, etc."
First stage renal investigations (routine)
'linical e)amination: anamnesis, physical e)amination
%rinalysis, *uantitative determinations !eg. proteinuria$+ h"
Serum creatinine and urea !creatinine clearance
calculation"-
electrolytes- acidbase balance
maging: %S, intravenous urography
Recognizing the renal syndromes argeted renal investigations
Diagnosis of the renal disease
-
8/13/2019 Sindroame renale
4/25
Renal syndromes
Renal failure (acute! rapidly progressive! chronic) "ephritic
syndrome
"ephrotic syndrome
#acroscopic hematuria
Asymptomatic urinary a$normalities %rinary tract infection
Renal tu$ule defects
&ypertension
"ephrolithiasis %rinary tract o$struction
-
8/13/2019 Sindroame renale
5/25
Acute renal failure
Definition= abrupt / of 01# !hours or days" with
consecutive azotemia
D' criteria
rapid increase of s% and s'r
oliguria !D233 ml$+h" or anuria
signs and symptoms of uremia
hyper 45emia, metabolic acidosis
*tiologyprerenal, renal, postrenal
-
8/13/2019 Sindroame renale
6/25
Rapidly progressive renal failure
Definition= progressive / of 01# in the course ofwee6swith
consecutive doubling of serum
creatinine in less than 7 months.
*tiology
primary e)tracapillary !rapidly progressive" 08
and secondary 08 !vasculitis, 0oodpasturesyndrome".
other: thrombotic microangiopathies !9%S",
tubulointerstitial nephritis.
-
8/13/2019 Sindroame renale
7/25
+hronic renal failure
Definition= comple) of clinical and biochemical
abnormalities resulting from a progressive
and ireversibledamage of the nephrons.
D' criteria
/01# with consecutive azotemia documented
for 7 months
%S: decreased 6idney size
anemia
*tiologythe ma;ority of chronic nephropathies
-
8/13/2019 Sindroame renale
8/25
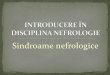
he structure of the glomerular capillary wall
-
8/13/2019 Sindroame renale
9/25
he role ,function of the glomerular capillary wall
Role= to assure the selective passage ofsubstances into
urine.
-ermselectivity assured by all 7 components of
the barrier:
. size selectivity and,or
. electrical charge selectivity
Damage to any of the 7 components = proteinuria
-
8/13/2019 Sindroame renale
10/25
he nephritic syndrome (Acute /")
-athophysiology
Definition= the result of acute inflamationin therenal
glomeruli.
acute 0 of /FR damage of the glomerularcapillary wall (/+1)
9ydrosaline retention 0lomerular macro$microscopic
hematuria!dysmorphic erythrocytes, erythrocyte casts"
1acial and peripheral edema 0lomerular proteinuria
-
8/13/2019 Sindroame renale
11/25
he nephritic syndrome
D' criteria 9ematuria !glomerular"
>dema
9ypertension ?roteinuria !glomerular"
&cute / of 01#
*tiologyprimary and secondary glomerular
diseases
-
8/13/2019 Sindroame renale
12/25
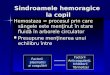
Types of hematuria
nonglomerular glomerular
-
8/13/2019 Sindroame renale
13/25
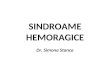
Erythrocyte casts
-
8/13/2019 Sindroame renale
14/25
-roteinuria
-hysiological proteinuria up to @A3 mg$+h
globulins 5 albumin !B++3 mg$+h"
#icroal$uminuria
= urinary loss of albumin between 73733 mg$+h
pathologicalC
mar6er of early glomerular in;ury !eg. diabeticnephropathy"
mar6er of vascular endothelial dysfunction
assessment of cardiovascular ris6
-
8/13/2019 Sindroame renale
15/25
ypes of proteinuria
/lomerular
proteins with intermediate E !mostly albumin"
'ause: defective glomerular barrier
u$ular
?roteins with low E !F+microglobulin, retinol
bindingprotein"normally filtered in the glomerulus and reabsorbed
inthe pro)imal tubule.
'ause: tubulointerstitial nephritis!/reabsorbtion"
-rerenal (overflow proteinuria)
proteins with low E !G$H light chains" I production
thatovercomes tubular reabsorbtion capacity
'ause: plasma cell dyscrasias !eg. myeloma"
-
8/13/2019 Sindroame renale
16/25
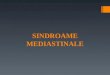
Types of proteinuria (urine protein
electrophoresis): glomerular (G), prerenal (PR)
and tubular (T)
-
8/13/2019 Sindroame renale
17/25
he nephrotic syndrome
Definition= glomerular proteinuria 7,A g$+ h J edema,
hypoproteinemia,
hypoalbuminemia, hyperlipidemia.
-athogenesisdamage of the 0'E as an
electric$mechanic barrier.
*tiologyprimary and secondary glomerular
diseases.
-
8/13/2019 Sindroame renale
18/25
he nephrotic syndrome . -athophysiology
Damage of the /+1 as an electric,mechanic $arrier
glomerular proteinuria 7,Ag$+h
+onse2uences of nephrotic range proteinuria
hypoproteinemia, hypoalbuminemia, malnutrition
hydrosaline retention !edema", hypotension, acute 6idney failure
thromboembolic complications !urinary loss of anticoagulant
proteins:
&(, plasminogen"
hyperlipidemia, lipiduria !reactive hepatic lipoprotein
synthesis"
increased ris6 for infections !urinary g losses"
deficient binding and transport of some drugs
ionic and hormonal disbalances !urinary losses of binding
proteins"
increased tubular reabsorbtion of filtered
proteinstubulointerstitial
to)icity
-
8/13/2019 Sindroame renale
19/25
he nephrotic syndrome . reatment
Specific treatment= treatment of the underlying glomerular
disease
"on.specific treatment
reduction of proteinuriadietary protein restriction,
&'>$K,
8S&D, nephrectomy
reduction of edemadietary salt restriction, diuretics,
albumin,hemofiltration
in case of hypovolemia and acute 3idney failurealbumin
treatment ,prophyla'is of throm$osisfractioned heparin
reduction of hyperlipidemia 90'o& reductase inhibitors
!statins"
prophyla'is of infectionsvaccines !eg. antipneumococcal
vaccine"
-
8/13/2019 Sindroame renale
20/25
Differentiation $etween nephrotic syndrome
and nephritic syndrome
ypical Features "ephrotic "epritic
4nset Insidious A$rupt
*dema 5555 55
6lood pressure "ormal Raised
7ugular venouspressure
"ormal,low Raised
-roteinuria 5555 55
&ematuria #ay,may not occur 555
Red.cell casts A$sent -resent
Serum al$umin 8ow "ormal,slightly reduced
-
8/13/2019 Sindroame renale
21/25
#acroscopic hematuria
#ecurrent $ single episode
0lomerular $ non glomerular
*tiology
uropathies:stones, tumours, infections
nephropathies:g& nephropathy, thin basement
membrane nephropathy
-
8/13/2019 Sindroame renale
22/25
Asymptomatic urinary a$normalities
-roteinuria 9:!;g,
-
8/13/2019 Sindroame renale
23/25
%rinary tract infection (%I)
Def.= colonization of the urine and urinary tract tissues
from
the bladder to the renal parenchima, with pathogenic
microorganisms.
*tiologynonspecific bacteria !>.coli, etc"
. tuberculosis, fungi !'andida", viruses
D' criteria isolation of the pathogenic agent from urine
symptoms and clinical signs of %(
radiological modifications
-
8/13/2019 Sindroame renale
24/25
Renal tu$ule defects
anatomic:autosomal dominant polycystic 6idney disease
!&D?4D"
functional!deficient tubular transport"
&ypertension renovascular!renal artery stenosis"
renal parenchymal!glomerular diseases"
"ephrolithiasiseliminated 6idney stones, stones removed by
urology procedures or identified by imaging !%S, i.v
urography"
%rinary tract o$structionobstacle 5 retrograde dilatation
-
8/13/2019 Sindroame renale
25/25
+lassification of the medical
nephropathies
0lomerular diseases
(ubulointerstitial diseases
Lascular diseases