Embed Size (px)
Citation preview

Sindrome da anticorpi antifosfolipidi: la moderna gestione del paziente
Angela Tincani Dpt. of Clinical and Experimental Sciences
University of Brescia- Italy

THE IDENTIFICATION of THEANTIPHOSPHOLIPID SYNDROME
Avortments à repetition, thromboses et anticoagulant
circulant antithromboplastinSoulier, J.P., Boffa, M.C.
Nouv. Presse Med. 1980; 9:859-864.
Thrombosis,abortion, cerebral disease, and the lupus anticoagulant
Hughes, G.R.V.Br. Med. J. 1983,287: 1088-1089
PRIMARY
WITHIN OTHER AUTOIMMUNE DISEASES (OFTEN SLE)
PERIPHERAL VASCULAR SYNDROMES ASSOCIATED WITH SYSTEMIC LUPUS ERYTHEMATOSUS
ALARCON SEGOVIA D, OSMUNDSON PJ. L. Ann Intern Med. 1965 May;62:907-19

International consensus statement on an update of the preliminary classification criteria of the antiphospholipid syndrome November 2004
Miyakis S, Lockshin MD, Atsumi T, Branch DW, Brey RL, Cervera R, Derksen RHWM, de Groot PG, Koike T, Meroni PL, Reber G, Shoenfeld Y, Tincani A, Vlachoyiannopoulos PG, Krilis SA. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost 2005; DOI: 10.1111/j.1538-7836.2005.01753.

APS: gestione moderna del paziente
1-Diagnosi precoce: 2-Terapia:
• Interpretare gli anticorpi • Riconoscere le manifestazioni
cliniche
• Profilassi primaria • Profilassi recidive

Andreoli L, Tincani A. Beyond the “Syndrome”: Antiphospholipid antibodies as risk factors. Arthritis Rheum 2012; 64:342-5.
Non all the patients wth aPL have thrombosis or pregnancy losses
Many patients with thrombosis or miscariaged do not have aPL
Risk profile, needed to quantitatethe risk

INTERNATIONAL CONSENSUS ON THE CONCEPT OF MULTIPLE POSITIVITY
2006
2009

Antiphospholipid antibodies are associated to thrombosis and pregnancy losses in clinical studies. Soulier, J.P., Boffa, M.C. Nouv. Presse Med. 1 980; 9:859- 864 Hughes, G.R.V.Br. Med. J. 1 983, 287: 1 088- 1 089
In experimental animals, the presence of antiphospholipid antibodies can enhance the thrombus formation and cause pregnancy failure Shoenfeld Y and Blank M 1992; Pierangeli S, Harris N, 1994-98
In prospective studies, aPL predict thrombosis occurrence and pregnancy problems both in SLE patients and in healthy women. Shulman S, et al. Am J Med 1998; 104: 332-338 Galli M et al. Blood 2003;5:1827-32 Lockshin MD,et al. N Engl J Med 1985; 313: 152-6 Lockwood CJ, Am J Obstet Gynecol 1989; 161:369-73
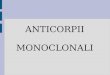
Patients affected by systemic autoimmune diseases, without thrombotic events. Healthy adult individuals. Healthy pre-school children. Avcin T et al, Rheum 2001; 40: 565-573
..BUT anti-β2GPI are detected in:

Anti β2GPI in healthy subjects n= 100 adults n= 13 1-3 yrs old children
n= 17 >3 yrs old children
n= 10 <1 yr old children
IgG
ant
i β2g
lyco
prot
ein
I
>3yrs old (n=17)
1-3yrs old (n=13)
<1yr old (n=10)
25° perc min median max 75° perc
Children

Anti β2GPI antibodies …are always the same?
Andreoli L et al. Ann Rheum Dis 2011; 70:380-383

Anti β2GPI antibodies and autoimmunity
Andreoli L, Chighizola C et al. Arthritis & Rheumatology 2015; 2196-2204

Anti-cardiolipin antibody
Anti-B2GPI Antibody
Anti-Domain Antibody
Lupus Anticoagulant
Isotype IgG, IgM (IgA) IgG, IgM (IgA)
Domain I/ Domain IV-V /
Titre >40 GPL/MPL low,
medium, high
low, medium, high ?+/-
Iterpretation of isolated positivity + ++ ?? +++
Other autoantibodies (ANA, anti Ro/SS-A, Coomb’s pos, etc) These data can complete the patient risk profile Complement levels
ANTIPHOSPHOLIPID ANTIBODY PROFILE

Averse pregnancy outcome occurred in 33 (15%) pregnancies: 14 (42%) in triple positive, 5 (15%) in double positive, 14 (42%) in single positive patients.
217 prospectively followed pregnancies in patients with aPL
N.B.: 15 (45%) occurred in LA negative pregnancies.
CLINICALLY SIGNIFICANT PROFILE in OAPS
M G Lazzaroni Unpublished obs.

Low-titre aCL/aβ(2)GPI positivity (>95(th )< 99(th) percentile) was considered positive for obstetric but not for thrombotic APS. Twenty-six women with purely obstetric APS had persistent low-titre aCL and/or aβ(2)GPI. Our data suggest that....low-titre antibodies should be included in the diagnosis of obstetric APS.
The clinical significance of low aPL titres
Gardiner C, Hills J, Machin SJ, Cohen H. Diagnosis of antiphospholipid syndrome in routine clinical practice. Lupus. 2013 Jan;22(1):18-25.

Main and associated Clinical Features
Recurrent arterial/venous thombosis Recurrent pregnancy loss Throbocytopenia Livaedo reticularis Leg ulcers Headache Chorea, epilepsy Cognitive disorders Heart valve lesions Haemolytic anemia Pulmunary hypertension
GRV Hughes BMJ 1988 GRV Hughes Lancet 1993
Clinical features associated to aPL in SLE Recurrent fetal loss Venous thrombosis Arterial thrombosis Leg ulcers Livaedo reticularis Haemolytic anemia Throbocytopenia
D. Alarcon-Segovia et al, Seminars Arthritis Rheum 1992.
MUCH MORE THAN THROMBOSIS AND PREGNANCY LOSS

Antiphospholipid Syndrome Clinical and Immunologic Manifestations and Patterns of Disease
Expression in a Cohort of 1,000 Patients
Clinical features at disease onset No. (%) of patients
Deep vein thrombosis 317 (31.7) Thrombocytopenia (<100,000 plts/µl) 219 (21.9) Livedo reticularis 204 (20.4) Stroke 131 (13.1) Superficial thrombophlebitis 91 (9.1) Pulmonary embolism 90 (9.0) Fetal loss 83 (8.3) Transient ischemic attack 70 (7.0) Hemolytic anemia 66 (6.6) Skin ulcers 39 (3.9) Epilepsy 34 (3.4) Pseudovasculitic skin lesions 26 (2.6) Myocardial infarction 28 (2.8) Amaurosis fugax 28 (2.8) Digital gangrene 19 (1.9).
Cervera R et al. ARTHRITIS & RHEUMATISM Vol. 46, No. 4, April 2002, pp 1019–1027
The Euro-Phospholipid Project

The relevance of “non-criteria” clinical manifestations of antiphospholipid syndrome: 14th International Congress on Antiphospholipid Antibodies Technical Task Force Report on Antiphospholipid Syndrome Clinical Features. Autoimmunity Reviews 14 (2015) 401–414
«Non-criteria» clinical features of APS
Recommendation for future classification

Standard of care of well defines APS (prophilaxis of recurrence) Venour thombosis: long term oral anticoagulation with target INR 2-3. Arterial thombosis: longterm anticoagulation with target INR 3-4; antiplatelet alone; long term anticoagulation with target INR 2-3; long term anticoagulation with target INR 2-3 + antplatelet. Obstetric APS: LDA + LMWH
aPL Carriers Primary prophilaxis of thrombosis Primary profilaxis of pregnany loss
Absence of aPL Seronegative APS Classical APS that become aPL negative after time and treatments
Refractory APS Thrombosis recurrence in standard treatment Pregnancy loss in standard treatment
APS treatment
Espinosa G &Cervera R. Nature review Rheumatolgy, 2015
?

Reports on Thrombosis Recurrence
95 patients with primary APS Mean follow-up time 4.5 years (0.3-26)
Breslow test 4.7, p=0.02 Log-rank test (p < 0.001).
177 patients( 56% primary) with vascular APS Median follow-up time 6.5 years (1-27)
Hernández-Molina G, Espericueta-Arriola G, Cabral AR. The role of lupus anticoagulant and triple marker positivity as risk factors for rethrombosis in patients with primary antiphospholipid syndrome. Clin Exp Rheumatol. 2013 May-Jun;31(3):382-8.
Bazzan M, Vaccarino A, Stella S, Sciascia S, Montaruli B, Bertero MT, Carignola R, Roccatello D; Piedmont APS Consortium. Patients with antiphosholipid syndrome and thrombotic recurrences: A real world observation (the Piedmont cohort study). Lupus. 2016 Apr;25(5):479-85.
OAT or A : oral aticoagulant alone or with antiplatelet therapy No OA or B: anti-platelet treatment or no treatment

Longterm Outcome of Patients with Primary Antiphospholipid Syndrome
Long rank (Mantel Cox test) Chi sqare 1.28, p 0.26 Grehan Breslow Wilcoxon test Chi square 0,93, p 0.33
OA: oral aticoagulant alone or with antiplatelet therapy NOA: 21 antiplatelet treatment, 1 HCQ, 1LMWH and 6 no treatment
84 PAPS patients with thrombotic history, median follow-up time: 17.66 yrs (range 15-30)
Taraborelli M, Reggia R, Dall’Ara F, Fredi M, Andreoli L, Gerosa M, Hoxha A, Massaro L, Tonello M, Costedoat-Chalumeau C, Cacoub P, Franceschini F, Meroni PL, Piette JC, Ruffatti A, Valesini G, Harris EN, Tincani A. J Rheumatol. 2017 in press
24 severe bleeding episodes were observed in 18 patients, all treated with oral AC (23%), 4 having more than 1 bleeding episode. Genital tract (metrorrhagia) was the most frequent affected site (29%), followed by cerebral (23%), gastro -intestinal (GI; 17%), ENT (14%), etc.
Median free time from events: • in oral anticoagulant (OA) 221 months • no oral anticoagulant (NO) 198 months

The new oral anticoagulants
-Cowell RPW. Direct oral anticoagulants: integration into clinical practice. Postgraduate Medical Journal. 2014;90(1067):529-539. -Urbanus R. Rivaroxaban to treat thrombotic antiphospholipid syndrome. Lancet Haematology 2016; 3 September
The reported safety of oral anticoagulants combined with an increase in patients’ wellbeing (reduced need of monitoring) are important arguments in favour od these drugs in the secondary prevention of venous thromboembolism

The new oral anticoagulants: clinical studies in APS
Schaefer JK, McBane RD, Black DF, et al. Failure of dabigatran and rivaroxaban to prevent thromboembolism in antiphospholipid syndrome: a case series of three patients. Thromb Haemost. 2014;112:947–50. Noel N, Dutasta F, Costedoat-Chalumeau N, et al. Safety and efficacy of oral direct inhibitors of thrombin and factor Xa in antiphospholipid syndrome. Autoimmun Rev. 2015;14:680–5. Win K, Rodgers GM. New oral anticoagulants may not be effective to prevent venous thromboembolism in patients with antiphospholipid syndrome. Am J Hematol. 2014;89:1017. Signorelli F, Nogueira F, Domingues V, Mariz HA, Levy RA. Thrombotic events in patients with antiphospholipid syndrome treated with rivaroxaban: a series of eight cases. Clin Rheumatol. 2015 Jul 30. Maksim Son et al. The use of rivaroxaban in patients with antiphospholipid syndrome: A series of 12 cases. Thrombosis Research 135 (2015) 1035–1036
26 pts with thrombotic APS (11 primary ); 11 with arterial events. 11 pts in dabigatran 15 pts in rivaroxaban
Discontinuation of the treatment in 4 pts (15%) after a median follow-up of 19 months; one patient had relapse of arterial thrombosis, two developed bleeding events, and one recurrent migraine.

Rivaroxaban v.s. warfarin in pts. with thrombotic APS, with or without SLE: a randomised, controlled, open-label, phase 2/3, non-inferiority trial. Available data: 56 pts in warfarin (INR 2.5) and 54 patients rivaroxaban (20 mg daily). At day 42: thrombin generation (assessment of the anticoagulant effects of warfarin and rivaroxaban). The overall thrombogram indicated no increase in thrombotic risk with rivaroxaban. At day 210: clinical evaluation. Absence of new thrombotic events during 6 months of treatment. No major bleeding episodes were noted, and rivaroxaban was significantly associated with improved quality of life.
Rivaroxaban and APS The RAPS trial
-Cohen H et al. Rivaroxaban versus warfarin to treat patients with thrombotic antiphospholipid syndrome, with or without systemic lupus erythematosus (RAPS): a randomised, controlled, open-label, phase 2/3, non-inferiority trial.Lancet Haematology 2016; Vol. 3 September. -Urbanus R. Rivaroxaban to treat thrombotic antiphospholipid syndrome. Lancet Haematology 2016; Vol.3, September.
Study limitations: -small number of pts included - <20% triple-positive aPL -excluded pts with arterial thrombosis or recurrence in warfarin -too short clinical follow-up

(1)Rivaroxaban in APS Pilot Trial—A Multicenter Feasibility Study of Rivaroxaban for Patients with APS and Prior Arterial or Venous Thrombosis (ClinicalTrials.gov Identifier: NCT02116036);
(2)TRAPS— Rivaroxaban in Thrombotic APS Trial Update—A Prospective, Randomized Clinical Trial Comparing Rivaroxaban vs Warfarin in High Risk Patients With APS (ClinicalTrials.gov Identifier: NCT02157272);
(3) ASTRO APS—Apixaban for the Secondary Prevention of Thromboembolism: A Prospective Randomized Outcome Pilot Study Among Patients with APS (ClinicalTrials.gov Identifier: NCT02295475).
The new oral anticoagulants: Ongoing clinical trials in APS

Treatment of «non-criteria» clinical manifestations of APS
Treatment Evidence Hematological manifestations -throbocytopenia -haemolytic anemia
Steroids, IVIG, immunosuppressant, rituximab, splenectomy. Primary thomboprophilaxis (HCQ, LDA) in case of significant serology.
Case series and 1 open label study
Neurologic manifestations -Chorea -mielytis -muntiple sclerosis like disease
Steroids and immunosuppressive agents (>in SLE-APS) +anticoagulat (>in patients with multiple sclerosis like disease and mielytis). Antidopaminergic drugs or dopamine-depleting agents in chorea.
Case series
Heat valve disease Oral anticoagulant for symtomatic patients Careful monitoring of anticoagulation for heart valve surgery
Case series
aPL-associated nephropathy
-SLE nephritis HCQ and/or antiplatelet/anticoagulant Non randomized controlled studies
-isolated aPL-nephropathy antiplatelet/anticoagulant Case series
-all the patients Angitensin-converting enzyme inhibitors and angitensin-receptor blockers
Clinical judgement

HYDROXYCHLOROQUINE (HCQ) and APS Synthetic antimalarial drug with immunosuppressive properties in systemic autoimmune diseases
• Antiplatelet • Hypoglycemic • Cholesterol metabolism
Block TNF-α ↓ Circulating immune complexes
↓ binding of anti-β2GPI to phospholipid bilayers
Rand JH, Blood 2008
• Thrombosis • Survival
↓ Activation TLR 3, 7 e 9 ↓ Proinflammatory cytokines
Bertrand et al. Med Trop. 1990; Espinola RG et al. Thromb.haemost. 2002; Emami J et al. J Physiol. Pharmacol 1999;
Berman J et al. J Immunol. 2005; Ziegler HK et al. Proc Natl Sci USA, 1982
Kyburz D et al. Rheumatol, 2006; Raschi E at al. Lupus, 2008
↓ aPL titres
Broder A, J Rheumatol 2013
What do we see in patients with primary APS?
Petri M, Lupus 1998; Broder A e Putterman C. J Rheumatol 2013; Ruiz-Irastorza et al. Lupus 2006
EFFECTS ON aPL IN PATIENTS WITH SLE

- APS classification according to the 2006 criteria by Miyakis et al. - Treatment with HCQ for at least 12 consecutive months
Inclusion criteria
114 patients (from Brescia, Milan and Padua) Retrospective, propensity score-matched cohort study from 1992 to 2016 with mean follow-up of 76 months (±48 SD).
- Treatment with other immunosuppressive drugs - Concomitant systemic autoimmune disease
Exclusion criteria
HYDROXYCHLOROQUINE in PRIMARY APS
57 pts. 57 pts.
Nuri E et al. Immunol Res 2016

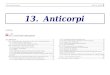
aPL TITERS: START vs. END OF FOLLOW-UP HCQ EXPOSED
Nuri E et al. Immunol Res 2016
HCQ NOT EXPOSED
Level of aPL positivity -negative: blank or white, low: -gray, medium–high titer: dark gray or black) at the beginning and at the end of the follow-up.

THROMBOTIC EVENTS DURING THE FOLLOW-UP
HCQ exposed
7 events
HCQ not
Exposed
7 events
Nuri E et al. Immunol Res 2016

Annual incidence of arterial recurrence
THROMBOTIC EVENTS DURING THE FOLLOW-UP
HCQ exposed HCQ not exposed
Annual incidence thrombotic recurrence
3,19-4,4%
1-3%
Medha B, Erkan D. Curr Rheumatol Rep 2011. Pengo V, Ruffatti A et al, J Thromb Haemost 2010. Cervera R, Serrano R et al, Annals of the Rheumatic Diseases 2015
Nuri E et al. Immunol Res 2016

Rituximab and APS
Pons I, Espinosa G, Cervera R. Efficacy and safety of rituximab in the treatment of primary antiphospholipid syndrome: analysis of 24 cases from the bibliography review. Med Clin. 2015;144:97–104. Ramos-Casals M, Brito-Zerón P, Muñoz S, BIOGEAS study group, et al. A systematic review of the off-label use of biological therapies in systemic autoimmune diseases. Medicine. 2008;87:345–64. Ioannou Y, Lambrianides A, Cambridge G, et al. B cell depletion therapy for patients with systemic lupus erythematosus results in a significant drop in anticardiolipin antibody titres. Ann Rheum Dis. 2008;67:425–6. Erre GL, Pardini S, Faedda R, et al. Effect of rituximab on clinical and laboratory features of antiphospholipid syndrome: a case report and a review of literature. Lupus. 2008;17:50–5. Erkan D, Vega J, Ramón G, et al. A pilot open-label phase II trial of rituximab for non-criteria manifestations of antiphospholipid syndrome. Arthritis Rheum. 2013;65:464–71.
B cell inhibition may have a role in difficult-to-treat APS patients, possibly in those with hematologic and microthrombotic/microangiopathic manifestations Erkan D, Aguiar CL, Andrade D, et al. 14th International Congress on Antiphospholipid Antibodies: task force report on antiphospholipid syndrome treatment trends. Autoimmun Rev. 2014;13:685–9.

Combine treatment that includes anticoagulation with: • heparin, • high dose steroids, • plasma exchange and/or intra-venous immunoglobulins
Management of the catastrophic APS and
aPL-associated microangiopathies
In refractory patients: rituximab and eculizumab are good alternatives.
Eculizumab, a humanized monoclonal antibody against complement protein C5, is currently approved for the treatment of paroxysmal nocturnal hemoglobinuria. It is able to reduce intravascular hemolysis and control complement mediated damage
J.A. Gómez-Puerta, R. Cervera / Journal of Autoimmunity 48-49 (2014) 20-25

FUTURE TREATMENTS
Novel therapeutic targets Antibodies against D1 of β2GPI have been shown to be pathogenic in animal models and have been found associated with obstetrical APS in humans Tolerogenic dendritic cells specific for β2GPI D1, lowerig antibody titre, were able to lower the rate of fetal loss
Agostinis C., et al.Blood 2014 Andreoli L. et al Arthritis Rheum. 2015 Zandman-Goddard G., et al. J Auoimmunity 2014
Synthetic peptide TIFI, that mimic the phospholipid bindng site of β2GPI (domain 5) was shown able to abrogate the aPL mediated angiogenesis inhibition at endometrial level. Di Simone N., et al., Am. J. Reprod. Immunol. 2013
Toll like receptor 4 was shown able to mediate the aPL impairment of trophoblast fusion and differentiation. HCQ could to reduce Toll lik receptor 4 mRNA and proten expression and to restore trophoblast function. Marchetti T. et al., J Thromb Haemost. 2014
Revised in: Ostensen M. Autoimmunity Reviews 2015

APS: gestione moderna del paziente
1-Diagnosi precoce: 2-Terapia:
• Stratificazione del rischio ! • Riconoscere non soltanto trombosi e patologia della gravidanza!
• Non solo anticoagulanti !

acknowledgments
Brescia Rheumatology Unit
Grazie a tutti per la attenzione !!!