Embed Size (px)
Citation preview

ARTICLE IN PRESS
Current Diagnostic Pathology (2006) 12, 40–53
0968-6053/$ - sdoi:10.1016/j.c
�Tel.: +1 818E-mail addr
www.elsevier.com/locate/cdip
MINI-SYMPOSIUM: HEAD AND NECK PATHOLOGY
Sinonasal carcinomas
Lester D.R. Thompson�
Southern California Permanente Medical Group, Woodland Hills Medical Center, Department of Pathology,5601 De Soto Avenue, Woodland Hills, CA 91367, USA
KEYWORDSSinonasal;Squamous cellcarcinoma;Nasal;Neuroendocrinecarcinoma;Basaloid squamouscell carcinoma;Lymphoepithelialcarcinoma;Olfactoryneuroblastoma;Sinonasalundifferentiatedcarcinoma
ee front matter & 2005dip.2005.10.009
719 2613; fax: +1 818 71ess: lester.d.thompson@
Summary Malignant neoplasms of the sinonasal tract encompass a wide variety ofepithelial, lymphoid and mesenchymal tumours. The separation and classification ofepithelial or neuroepithelial tumours is sometimes challenging, especially whentreatment and prognosis are different. Squamous cell carcinoma, keratinizing ornon-keratinizing and, usually, the poorly differentiated type need to be separatedfrom sinonasal undifferentiated carcinoma, lymphoepithelial carcinoma, neuroen-docrine carcinoma and olfactory neuroblastoma. Whereas melanoma and lymphomaare also included in the broad differential, along with primitive neuroectodermaltumours and rhabdomyosarcomas, the focus of this commentary will be to presentthe major clinical, radiographical, histological, immunohistochemical, ultrastruc-tural and molecular features which allow for separation of the principle mucosalepithelial neoplasms of the sinonasal tract.& 2005 Elsevier Ltd. All rights reserved.
Introduction
Malignant sinonasal tract tumours comprise o1% ofall neoplasms and about 3% of those of the upperaerodigestive tract.1 Squamous cell carcinoma(SCC) and adenocarcinoma are strongly associatedwith environmental factors, including tobacco,alcohol and occupational exposure (e.g. to heavymetal particles such as nickel and chromium) andwith workers in the leather, textile, furniture andwood industries.1–5
Sinonasal tract malignancies most commonlyaffect the maxillary sinus (about 60%), followed by
Elsevier Ltd. All rights reserve
9 2309.kp.org.
the nasal cavity (about 22%), ethmoid sinus (about15%) and frontal and sphenoid sinuses (o3%).Sinonasal tract tumours are diverse, with themajority being SCC and its variants (55%), followedby non-epithelial neoplasms (20%), glandular tu-mours (15%), undifferentiated carcinoma (7%) andmiscellaneous tumours (3%).1,3–5 Carcinoma of thenasopharynx differs in many aspects from that ofthe nasal cavity and paranasal sinuses and will notbe discussed herein. Furthermore adenocarcinomasincluding salivary gland-type carcinomas and non-epithelial tumours will not be discussed.
The clinical presentations, radiological featuresand pattern of tumour spread for SCC, adenocarci-noma and most of the other malignant neoplasms ofthe sinonasal tract are similar. Gross appearance of
d.
ARTICLE IN PRESS
Sinonasal carcinomas 41
the sinonasal tract and nasopharyngeal malignan-cies has limited value in aiding diagnosis, becausethe initial diagnosis depends on the tissue obtainedby endoscopy or polypectomy. The treatment ofchoice for most sinonasal tract carcinomas issurgical resection with clear margins.1,3–5 Thefollowing discussion will focus on the specificclinical, radiographical and diagnostic criteria usedin the separation of selected carcinomas of thesinonasal tract, specifically sinonasal undifferen-tiated carcinoma (SNUC), small cell carcinoma,lymphoepithelial carcinoma (nasopharyngeal-type)and neuroendocrine carcinoma (Table 1). In thiscontext, a brief discussion about SCC is necessary
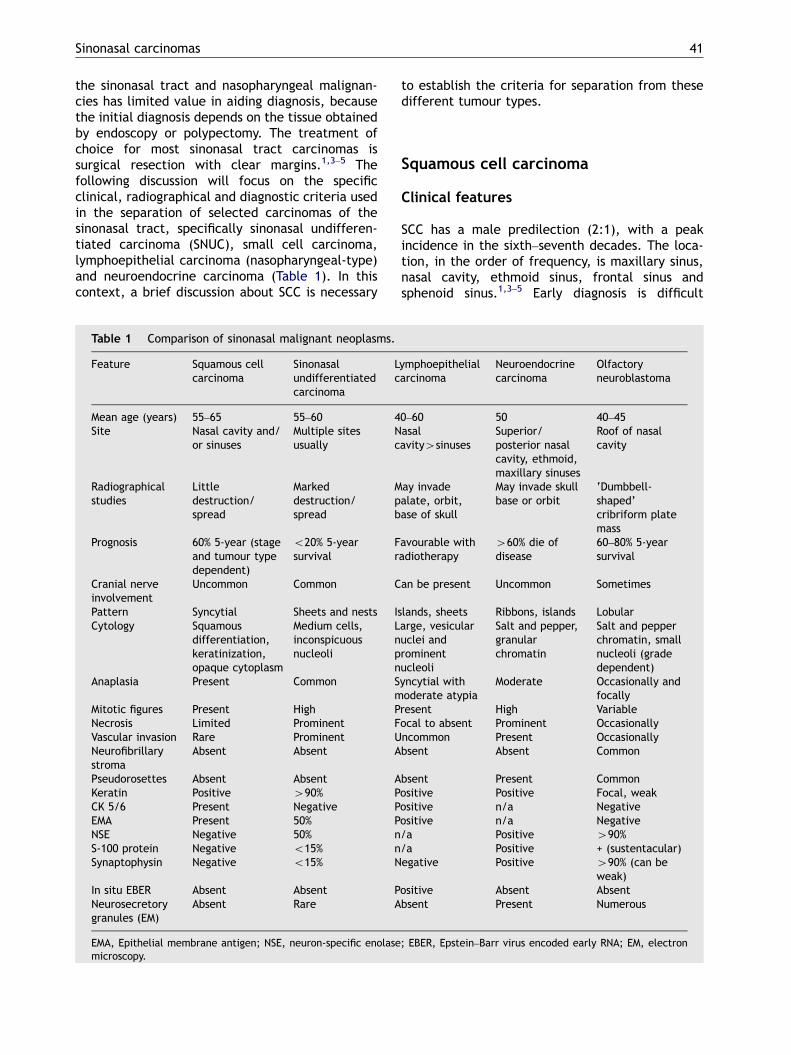
Table 1 Comparison of sinonasal malignant neoplasms.
Feature Squamous cellcarcinoma
Sinonasalundifferentiatedcarcinoma
Lc
Mean age (years) 55–65 55–60 4Site Nasal cavity and/
or sinusesMultiple sitesusually
Nc
Radiographicalstudies
Littledestruction/spread
Markeddestruction/spread
Mpb
Prognosis 60% 5-year (stageand tumour typedependent)
o20% 5-yearsurvival
Fr
Cranial nerveinvolvement
Uncommon Common C
Pattern Syncytial Sheets and nests IsCytology Squamous
differentiation,keratinization,opaque cytoplasm
Medium cells,inconspicuousnucleoli
Lnpn
Anaplasia Present Common Sm
Mitotic figures Present High PNecrosis Limited Prominent FVascular invasion Rare Prominent UNeurofibrillarystroma
Absent Absent A
Pseudorosettes Absent Absent AKeratin Positive 490% PCK 5/6 Present Negative PEMA Present 50% PNSE Negative 50% nS-100 protein Negative o15% nSynaptophysin Negative o15% N
In situ EBER Absent Absent PNeurosecretorygranules (EM)
Absent Rare A
EMA, Epithelial membrane antigen; NSE, neuron-specific enolasemicroscopy.
to establish the criteria for separation from thesedifferent tumour types.
Squamous cell carcinoma
Clinical features
SCC has a male predilection (2:1), with a peakincidence in the sixth–seventh decades. The loca-tion, in the order of frequency, is maxillary sinus,nasal cavity, ethmoid sinus, frontal sinus andsphenoid sinus.1,3–5 Early diagnosis is difficult
ymphoepithelialarcinoma
Neuroendocrinecarcinoma
Olfactoryneuroblastoma
0–60 50 40–45asalavity4sinuses
Superior/posterior nasalcavity, ethmoid,maxillary sinuses
Roof of nasalcavity
ay invadealate, orbit,ase of skull
May invade skullbase or orbit
‘Dumbbell-shaped’cribriform platemass
avourable withadiotherapy
460% die ofdisease
60–80% 5-yearsurvival
an be present Uncommon Sometimes
lands, sheets Ribbons, islands Lobulararge, vesicularuclei androminentucleoli
Salt and pepper,granularchromatin
Salt and pepperchromatin, smallnucleoli (gradedependent)
yncytial withoderate atypia
Moderate Occasionally andfocally
resent High Variableocal to absent Prominent Occasionallyncommon Present Occasionallybsent Absent Common
bsent Present Commonositive Positive Focal, weakositive n/a Negativeositive n/a Negative/a Positive 490%/a Positive + (sustentacular)egative Positive 490% (can be
weak)ositive Absent Absentbsent Present Numerous
; EBER, Epstein–Barr virus encoded early RNA; EM, electron
ARTICLE IN PRESS
L.D.R. Thompson42
because symptoms and signs are non-specific andclosely resemble those of chronic sinusitis, allergicreaction and nasal polyposis. Initial symptoms arerelated to the effects of the mass causing unilateralnasal obstruction. Secondary infection is common,giving rise to a mucoid or purulent discharge.Epistaxis develops when the mucosa is ulcerated ortumour extends into the sinus wall. Tumours invol-ving the ethmoid, maxillary, or frontal sinuses maycause proptosis, restriction of eye motility, diplopiaor loss of vision. Epiphora results from lacrimal sacor duct obstruction by the tumour. Compression ofthe nerve at the primary site or perineural spaceinvasion can compromise the functions of cranialnerves.1,5 A mass or discoloured lesion may bevisualized endoscopically and biopsied.
Late manifestations include facial swelling andcheek paraesthesia resulting from anterior max-illary extension into the soft tissue and infraorbitalnerve involvement, respectively. Inferior extensioninto the oral cavity forms a visible mass in thepalate or alveolar ridge. Posterior extension cancause trismus from pterygoid muscle invasion. Earsymptoms suggest possible involvement of thenasopharynx, eustachian tube and pterygoidplates. Upward extension into the skull base maylead to cranial nerve involvement and dura inva-sion. In the initial work-up, it is rare to find cervicallymph node metastasis.1,3–5
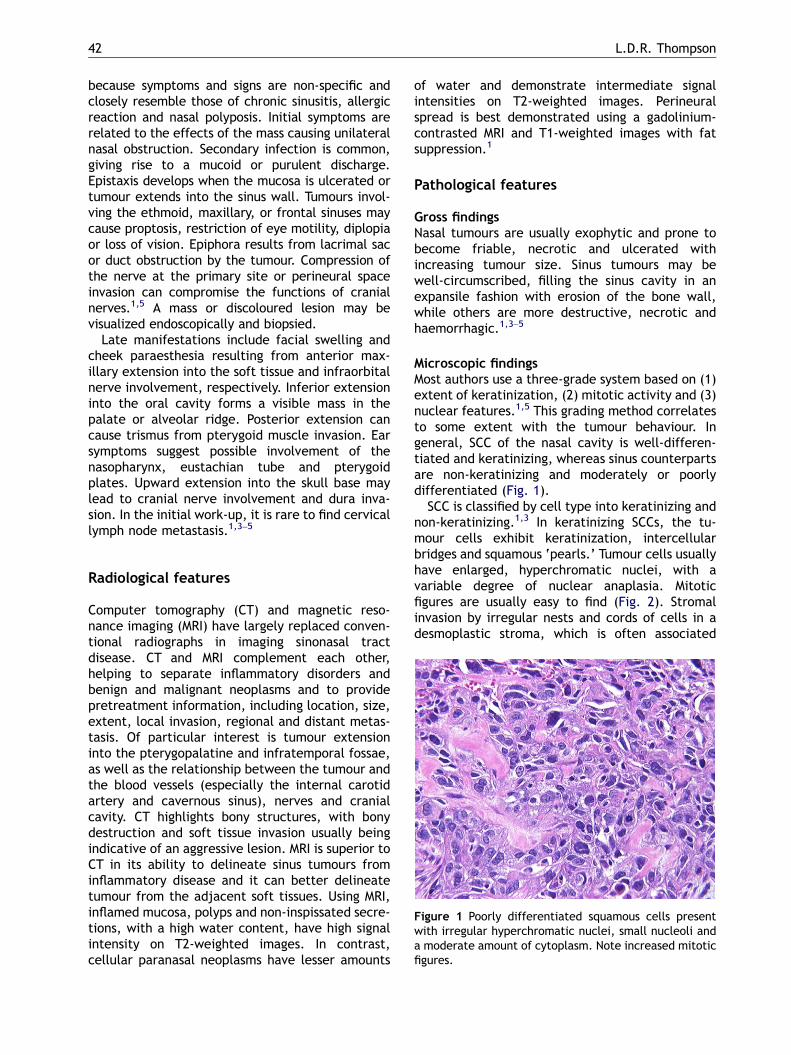
Figure 1 Poorly differentiated squamous cells presentwith irregular hyperchromatic nuclei, small nucleoli anda moderate amount of cytoplasm. Note increased mitoticfigures.
Radiological features
Computer tomography (CT) and magnetic reso-nance imaging (MRI) have largely replaced conven-tional radiographs in imaging sinonasal tractdisease. CT and MRI complement each other,helping to separate inflammatory disorders andbenign and malignant neoplasms and to providepretreatment information, including location, size,extent, local invasion, regional and distant metas-tasis. Of particular interest is tumour extensioninto the pterygopalatine and infratemporal fossae,as well as the relationship between the tumour andthe blood vessels (especially the internal carotidartery and cavernous sinus), nerves and cranialcavity. CT highlights bony structures, with bonydestruction and soft tissue invasion usually beingindicative of an aggressive lesion. MRI is superior toCT in its ability to delineate sinus tumours frominflammatory disease and it can better delineatetumour from the adjacent soft tissues. Using MRI,inflamed mucosa, polyps and non-inspissated secre-tions, with a high water content, have high signalintensity on T2-weighted images. In contrast,cellular paranasal neoplasms have lesser amounts
of water and demonstrate intermediate signalintensities on T2-weighted images. Perineuralspread is best demonstrated using a gadolinium-contrasted MRI and T1-weighted images with fatsuppression.1
Pathological features
Gross findingsNasal tumours are usually exophytic and prone tobecome friable, necrotic and ulcerated withincreasing tumour size. Sinus tumours may bewell-circumscribed, filling the sinus cavity in anexpansile fashion with erosion of the bone wall,while others are more destructive, necrotic andhaemorrhagic.1,3–5
Microscopic findingsMost authors use a three-grade system based on (1)extent of keratinization, (2) mitotic activity and (3)nuclear features.1,5 This grading method correlatesto some extent with the tumour behaviour. Ingeneral, SCC of the nasal cavity is well-differen-tiated and keratinizing, whereas sinus counterpartsare non-keratinizing and moderately or poorlydifferentiated (Fig. 1).
SCC is classified by cell type into keratinizing andnon-keratinizing.1,3 In keratinizing SCCs, the tu-mour cells exhibit keratinization, intercellularbridges and squamous ‘pearls.’ Tumour cells usuallyhave enlarged, hyperchromatic nuclei, with avariable degree of nuclear anaplasia. Mitoticfigures are usually easy to find (Fig. 2). Stromalinvasion by irregular nests and cords of cells in adesmoplastic stroma, which is often associated
ARTICLE IN PRESS
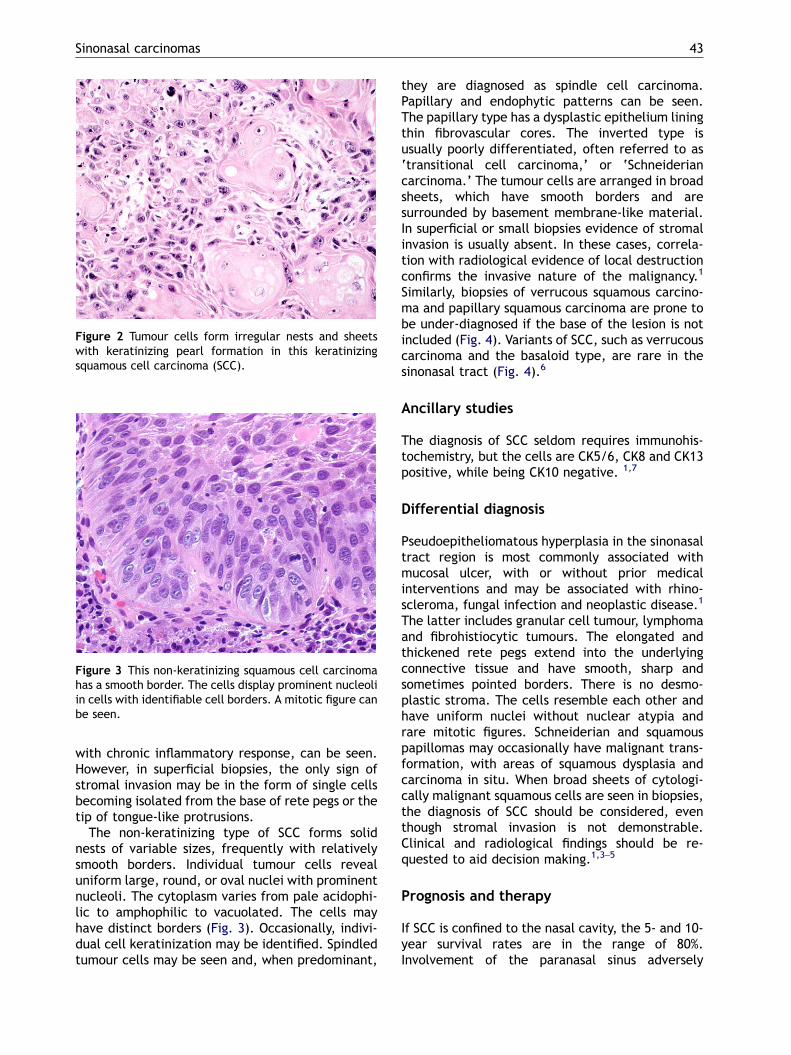
Figure 3 This non-keratinizing squamous cell carcinomahas a smooth border. The cells display prominent nucleoliin cells with identifiable cell borders. A mitotic figure canbe seen.
Figure 2 Tumour cells form irregular nests and sheetswith keratinizing pearl formation in this keratinizingsquamous cell carcinoma (SCC).
Sinonasal carcinomas 43
with chronic inflammatory response, can be seen.However, in superficial biopsies, the only sign ofstromal invasion may be in the form of single cellsbecoming isolated from the base of rete pegs or thetip of tongue-like protrusions.
The non-keratinizing type of SCC forms solidnests of variable sizes, frequently with relativelysmooth borders. Individual tumour cells revealuniform large, round, or oval nuclei with prominentnucleoli. The cytoplasm varies from pale acidophi-lic to amphophilic to vacuolated. The cells mayhave distinct borders (Fig. 3). Occasionally, indivi-dual cell keratinization may be identified. Spindledtumour cells may be seen and, when predominant,
they are diagnosed as spindle cell carcinoma.Papillary and endophytic patterns can be seen.The papillary type has a dysplastic epithelium liningthin fibrovascular cores. The inverted type isusually poorly differentiated, often referred to as‘transitional cell carcinoma,’ or ‘Schneideriancarcinoma.’ The tumour cells are arranged in broadsheets, which have smooth borders and aresurrounded by basement membrane-like material.In superficial or small biopsies evidence of stromalinvasion is usually absent. In these cases, correla-tion with radiological evidence of local destructionconfirms the invasive nature of the malignancy.1
Similarly, biopsies of verrucous squamous carcino-ma and papillary squamous carcinoma are prone tobe under-diagnosed if the base of the lesion is notincluded (Fig. 4). Variants of SCC, such as verrucouscarcinoma and the basaloid type, are rare in thesinonasal tract (Fig. 4).6
Ancillary studies
The diagnosis of SCC seldom requires immunohis-tochemistry, but the cells are CK5/6, CK8 and CK13positive, while being CK10 negative. 1,7
Differential diagnosis
Pseudoepitheliomatous hyperplasia in the sinonasaltract region is most commonly associated withmucosal ulcer, with or without prior medicalinterventions and may be associated with rhino-scleroma, fungal infection and neoplastic disease.1
The latter includes granular cell tumour, lymphomaand fibrohistiocytic tumours. The elongated andthickened rete pegs extend into the underlyingconnective tissue and have smooth, sharp andsometimes pointed borders. There is no desmo-plastic stroma. The cells resemble each other andhave uniform nuclei without nuclear atypia andrare mitotic figures. Schneiderian and squamouspapillomas may occasionally have malignant trans-formation, with areas of squamous dysplasia andcarcinoma in situ. When broad sheets of cytologi-cally malignant squamous cells are seen in biopsies,the diagnosis of SCC should be considered, eventhough stromal invasion is not demonstrable.Clinical and radiological findings should be re-quested to aid decision making.1,3–5
Prognosis and therapy
If SCC is confined to the nasal cavity, the 5- and 10-year survival rates are in the range of 80%.Involvement of the paranasal sinus adversely
ARTICLE IN PRESS
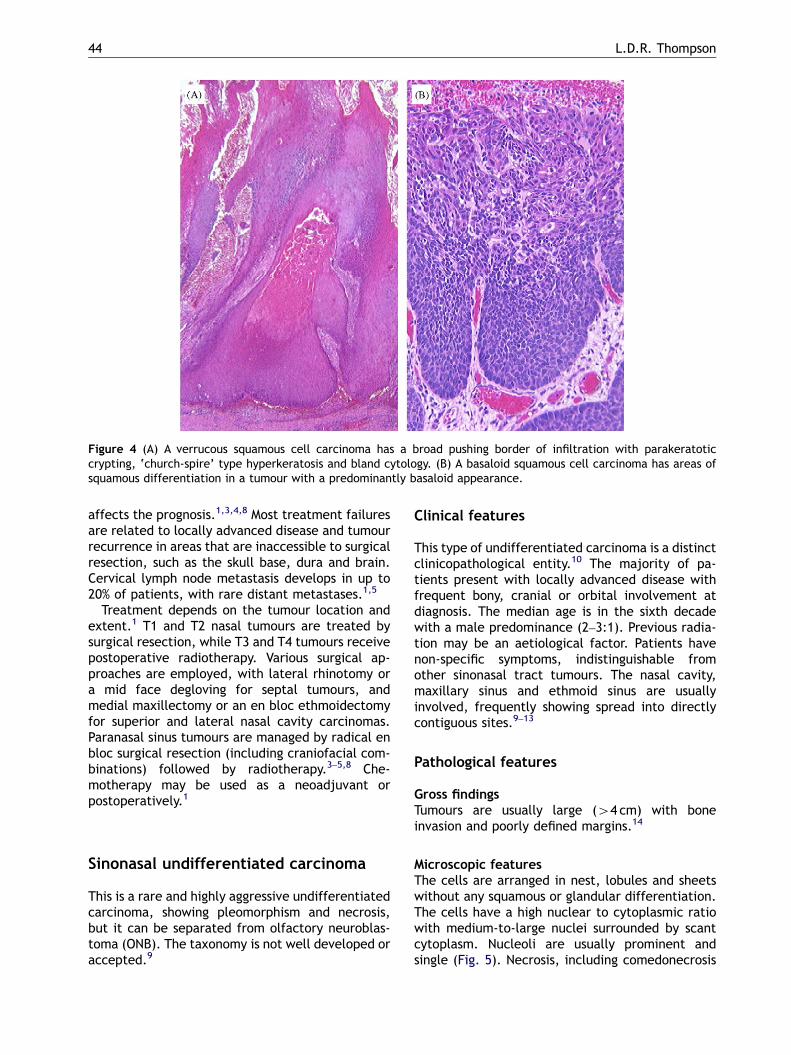
Figure 4 (A) A verrucous squamous cell carcinoma has a broad pushing border of infiltration with parakeratoticcrypting, ‘church-spire’ type hyperkeratosis and bland cytology. (B) A basaloid squamous cell carcinoma has areas ofsquamous differentiation in a tumour with a predominantly basaloid appearance.
L.D.R. Thompson44
affects the prognosis.1,3,4,8 Most treatment failuresare related to locally advanced disease and tumourrecurrence in areas that are inaccessible to surgicalresection, such as the skull base, dura and brain.Cervical lymph node metastasis develops in up to20% of patients, with rare distant metastases.1,5
Treatment depends on the tumour location andextent.1 T1 and T2 nasal tumours are treated bysurgical resection, while T3 and T4 tumours receivepostoperative radiotherapy. Various surgical ap-proaches are employed, with lateral rhinotomy ora mid face degloving for septal tumours, andmedial maxillectomy or an en bloc ethmoidectomyfor superior and lateral nasal cavity carcinomas.Paranasal sinus tumours are managed by radical enbloc surgical resection (including craniofacial com-binations) followed by radiotherapy.3–5,8 Che-motherapy may be used as a neoadjuvant orpostoperatively.1
Sinonasal undifferentiated carcinoma
This is a rare and highly aggressive undifferentiatedcarcinoma, showing pleomorphism and necrosis,but it can be separated from olfactory neuroblas-toma (ONB). The taxonomy is not well developed oraccepted.9
Clinical features
This type of undifferentiated carcinoma is a distinctclinicopathological entity.10 The majority of pa-tients present with locally advanced disease withfrequent bony, cranial or orbital involvement atdiagnosis. The median age is in the sixth decadewith a male predominance (2–3:1). Previous radia-tion may be an aetiological factor. Patients havenon-specific symptoms, indistinguishable fromother sinonasal tract tumours. The nasal cavity,maxillary sinus and ethmoid sinus are usuallyinvolved, frequently showing spread into directlycontiguous sites.9–13
Pathological features
Gross findingsTumours are usually large (44 cm) with boneinvasion and poorly defined margins.14
Microscopic featuresThe cells are arranged in nest, lobules and sheetswithout any squamous or glandular differentiation.The cells have a high nuclear to cytoplasmic ratiowith medium-to-large nuclei surrounded by scantcytoplasm. Nucleoli are usually prominent andsingle (Fig. 5). Necrosis, including comedonecrosis
ARTICLE IN PRESS
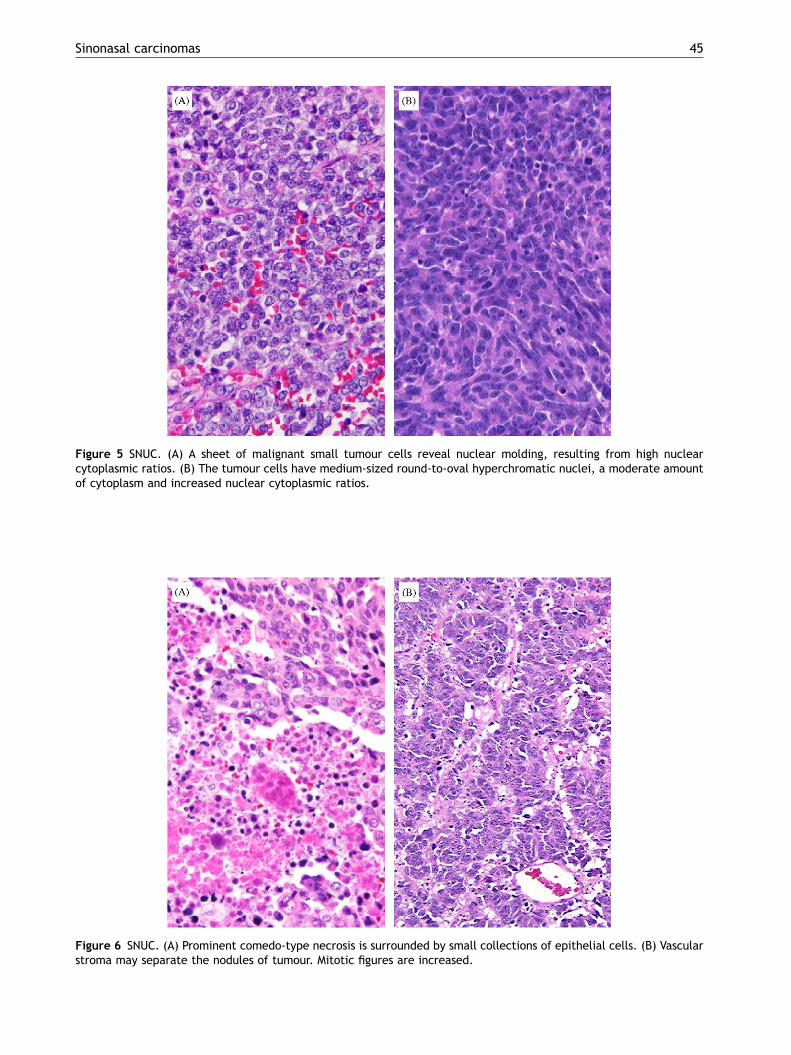
Figure 5 SNUC. (A) A sheet of malignant small tumour cells reveal nuclear molding, resulting from high nuclearcytoplasmic ratios. (B) The tumour cells have medium-sized round-to-oval hyperchromatic nuclei, a moderate amountof cytoplasm and increased nuclear cytoplasmic ratios.
Figure 6 SNUC. (A) Prominent comedo-type necrosis is surrounded by small collections of epithelial cells. (B) Vascularstroma may separate the nodules of tumour. Mitotic figures are increased.
Sinonasal carcinomas 45
ARTICLE IN PRESS
L.D.R. Thompson46
is common (Figs. 6 and 7). Mitotic figures areincreased. Lymph–vascular invasion is a commonfinding.9,10,12,15–17
Immunohistochemical features
The majority of tumours react with keratins(especially simple keratins especially (Fig. 8),
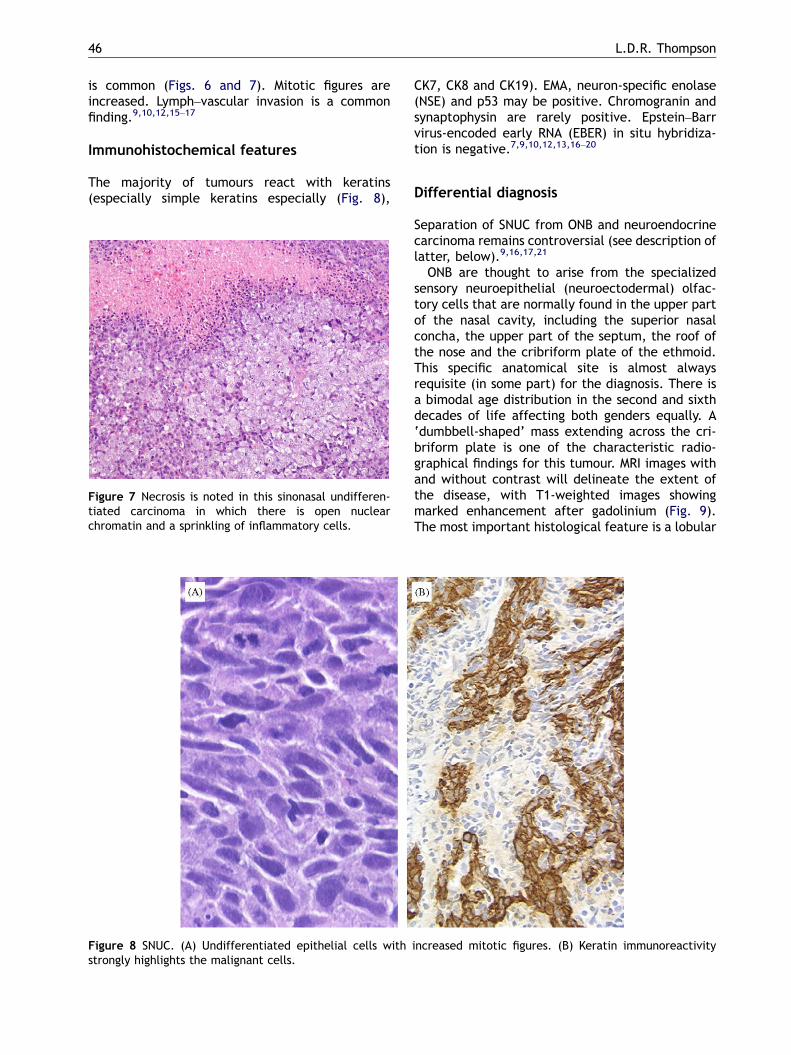
Figure 8 SNUC. (A) Undifferentiated epithelial cells withstrongly highlights the malignant cells.
Figure 7 Necrosis is noted in this sinonasal undifferen-tiated carcinoma in which there is open nuclearchromatin and a sprinkling of inflammatory cells.
CK7, CK8 and CK19). EMA, neuron-specific enolase(NSE) and p53 may be positive. Chromogranin andsynaptophysin are rarely positive. Epstein–Barrvirus-encoded early RNA (EBER) in situ hybridiza-tion is negative.7,9,10,12,13,16–20
Differential diagnosis
Separation of SNUC from ONB and neuroendocrinecarcinoma remains controversial (see description oflatter, below).9,16,17,21
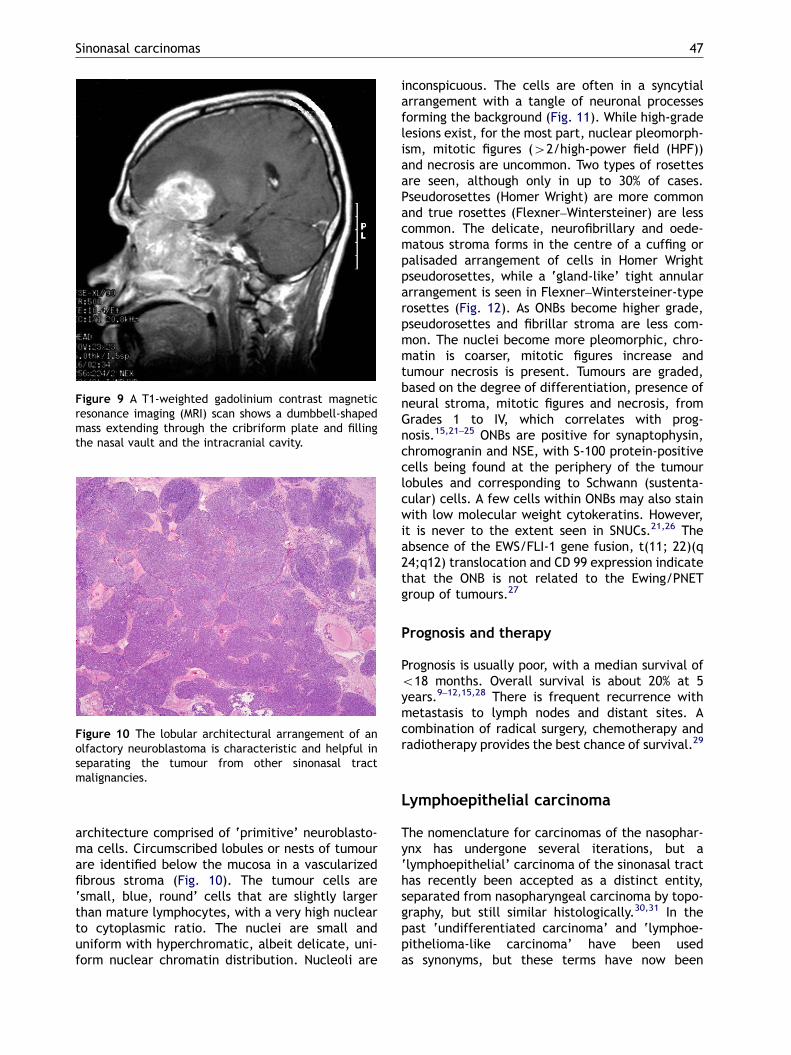
ONB are thought to arise from the specializedsensory neuroepithelial (neuroectodermal) olfac-tory cells that are normally found in the upper partof the nasal cavity, including the superior nasalconcha, the upper part of the septum, the roof ofthe nose and the cribriform plate of the ethmoid.This specific anatomical site is almost alwaysrequisite (in some part) for the diagnosis. There isa bimodal age distribution in the second and sixthdecades of life affecting both genders equally. A‘dumbbell-shaped’ mass extending across the cri-briform plate is one of the characteristic radio-graphical findings for this tumour. MRI images withand without contrast will delineate the extent ofthe disease, with T1-weighted images showingmarked enhancement after gadolinium (Fig. 9).The most important histological feature is a lobular
increased mitotic figures. (B) Keratin immunoreactivity
ARTICLE IN PRESS
Figure 9 A T1-weighted gadolinium contrast magneticresonance imaging (MRI) scan shows a dumbbell-shapedmass extending through the cribriform plate and fillingthe nasal vault and the intracranial cavity.
Figure 10 The lobular architectural arrangement of anolfactory neuroblastoma is characteristic and helpful inseparating the tumour from other sinonasal tractmalignancies.
Sinonasal carcinomas 47
architecture comprised of ‘primitive’ neuroblasto-ma cells. Circumscribed lobules or nests of tumourare identified below the mucosa in a vascularizedfibrous stroma (Fig. 10). The tumour cells are‘small, blue, round’ cells that are slightly largerthan mature lymphocytes, with a very high nuclearto cytoplasmic ratio. The nuclei are small anduniform with hyperchromatic, albeit delicate, uni-form nuclear chromatin distribution. Nucleoli are
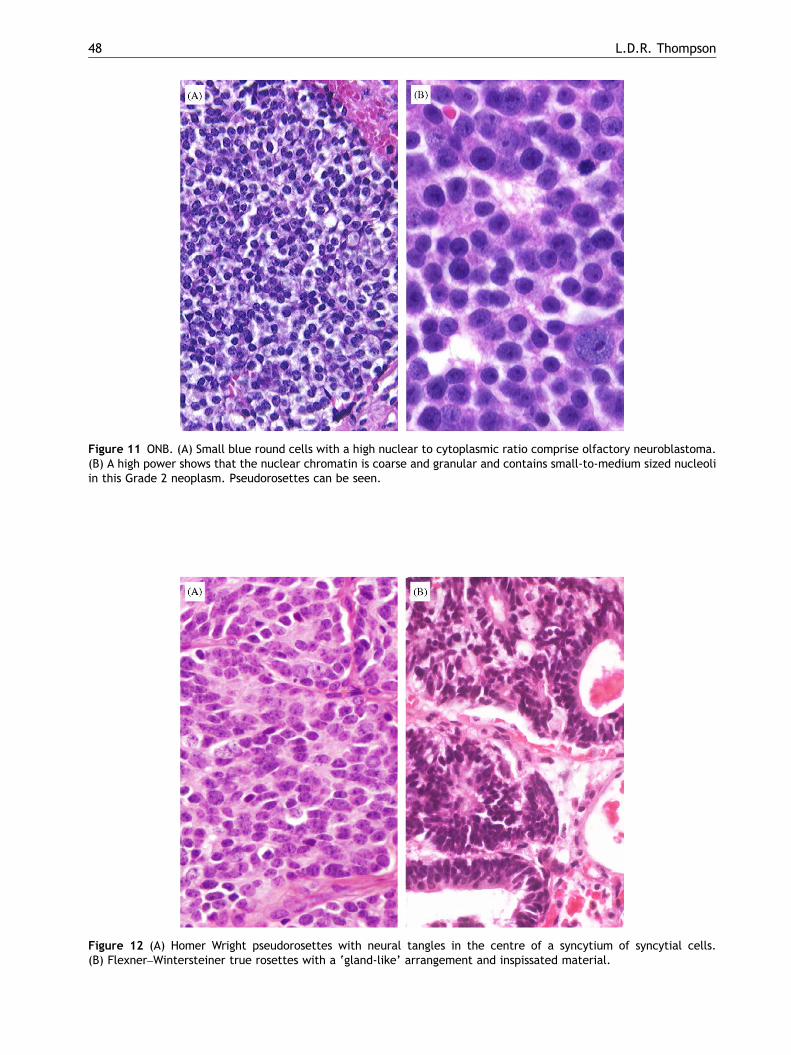
inconspicuous. The cells are often in a syncytialarrangement with a tangle of neuronal processesforming the background (Fig. 11). While high-gradelesions exist, for the most part, nuclear pleomorph-ism, mitotic figures (42/high-power field (HPF))and necrosis are uncommon. Two types of rosettesare seen, although only in up to 30% of cases.Pseudorosettes (Homer Wright) are more commonand true rosettes (Flexner–Wintersteiner) are lesscommon. The delicate, neurofibrillary and oede-matous stroma forms in the centre of a cuffing orpalisaded arrangement of cells in Homer Wrightpseudorosettes, while a ‘gland-like’ tight annulararrangement is seen in Flexner–Wintersteiner-typerosettes (Fig. 12). As ONBs become higher grade,pseudorosettes and fibrillar stroma are less com-mon. The nuclei become more pleomorphic, chro-matin is coarser, mitotic figures increase andtumour necrosis is present. Tumours are graded,based on the degree of differentiation, presence ofneural stroma, mitotic figures and necrosis, fromGrades 1 to IV, which correlates with prog-nosis.15,21–25 ONBs are positive for synaptophysin,chromogranin and NSE, with S-100 protein-positivecells being found at the periphery of the tumourlobules and corresponding to Schwann (sustenta-cular) cells. A few cells within ONBs may also stainwith low molecular weight cytokeratins. However,it is never to the extent seen in SNUCs.21,26 Theabsence of the EWS/FLI-1 gene fusion, t(11; 22)(q24;q12) translocation and CD 99 expression indicatethat the ONB is not related to the Ewing/PNETgroup of tumours.27
Prognosis and therapy
Prognosis is usually poor, with a median survival ofo18 months. Overall survival is about 20% at 5years.9–12,15,28 There is frequent recurrence withmetastasis to lymph nodes and distant sites. Acombination of radical surgery, chemotherapy andradiotherapy provides the best chance of survival.29
Lymphoepithelial carcinoma
The nomenclature for carcinomas of the nasophar-ynx has undergone several iterations, but a‘lymphoepithelial’ carcinoma of the sinonasal tracthas recently been accepted as a distinct entity,separated from nasopharyngeal carcinoma by topo-graphy, but still similar histologically.30,31 In thepast ‘undifferentiated carcinoma’ and ‘lymphoe-pithelioma-like carcinoma’ have been usedas synonyms, but these terms have now been
ARTICLE IN PRESS
Figure 11 ONB. (A) Small blue round cells with a high nuclear to cytoplasmic ratio comprise olfactory neuroblastoma.(B) A high power shows that the nuclear chromatin is coarse and granular and contains small-to-medium sized nucleoliin this Grade 2 neoplasm. Pseudorosettes can be seen.
Figure 12 (A) Homer Wright pseudorosettes with neural tangles in the centre of a syncytium of syncytial cells.(B) Flexner–Wintersteiner true rosettes with a ‘gland-like’ arrangement and inspissated material.
L.D.R. Thompson48
ARTICLE IN PRESS
Sinonasal carcinomas 49
abandoned in favour of lymphoepithelial carcinomafor this type, in order to separate it from SNUC.
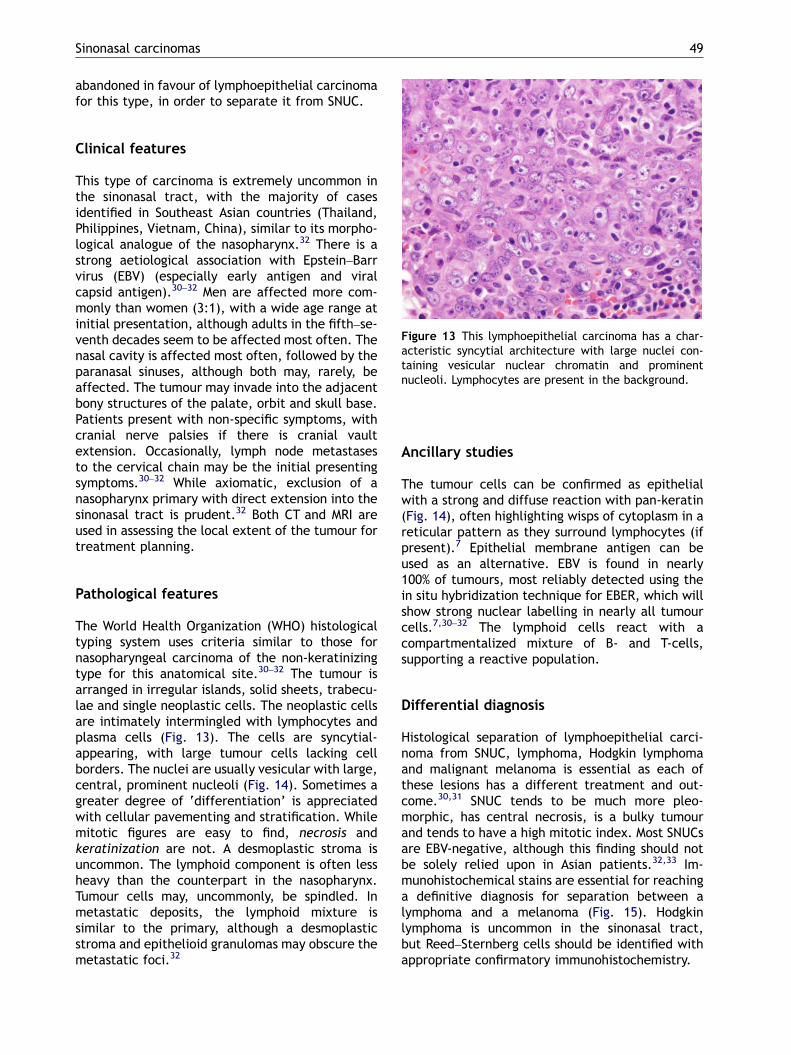
Figure 13 This lymphoepithelial carcinoma has a char-acteristic syncytial architecture with large nuclei con-taining vesicular nuclear chromatin and prominentnucleoli. Lymphocytes are present in the background.
Clinical features
This type of carcinoma is extremely uncommon inthe sinonasal tract, with the majority of casesidentified in Southeast Asian countries (Thailand,Philippines, Vietnam, China), similar to its morpho-logical analogue of the nasopharynx.32 There is astrong aetiological association with Epstein–Barrvirus (EBV) (especially early antigen and viralcapsid antigen).30–32 Men are affected more com-monly than women (3:1), with a wide age range atinitial presentation, although adults in the fifth–se-venth decades seem to be affected most often. Thenasal cavity is affected most often, followed by theparanasal sinuses, although both may, rarely, beaffected. The tumour may invade into the adjacentbony structures of the palate, orbit and skull base.Patients present with non-specific symptoms, withcranial nerve palsies if there is cranial vaultextension. Occasionally, lymph node metastasesto the cervical chain may be the initial presentingsymptoms.30–32 While axiomatic, exclusion of anasopharynx primary with direct extension into thesinonasal tract is prudent.32 Both CT and MRI areused in assessing the local extent of the tumour fortreatment planning.
Pathological features
The World Health Organization (WHO) histologicaltyping system uses criteria similar to those fornasopharyngeal carcinoma of the non-keratinizingtype for this anatomical site.30–32 The tumour isarranged in irregular islands, solid sheets, trabecu-lae and single neoplastic cells. The neoplastic cellsare intimately intermingled with lymphocytes andplasma cells (Fig. 13). The cells are syncytial-appearing, with large tumour cells lacking cellborders. The nuclei are usually vesicular with large,central, prominent nucleoli (Fig. 14). Sometimes agreater degree of ‘differentiation’ is appreciatedwith cellular pavementing and stratification. Whilemitotic figures are easy to find, necrosis andkeratinization are not. A desmoplastic stroma isuncommon. The lymphoid component is often lessheavy than the counterpart in the nasopharynx.Tumour cells may, uncommonly, be spindled. Inmetastatic deposits, the lymphoid mixture issimilar to the primary, although a desmoplasticstroma and epithelioid granulomas may obscure themetastatic foci.32
Ancillary studies
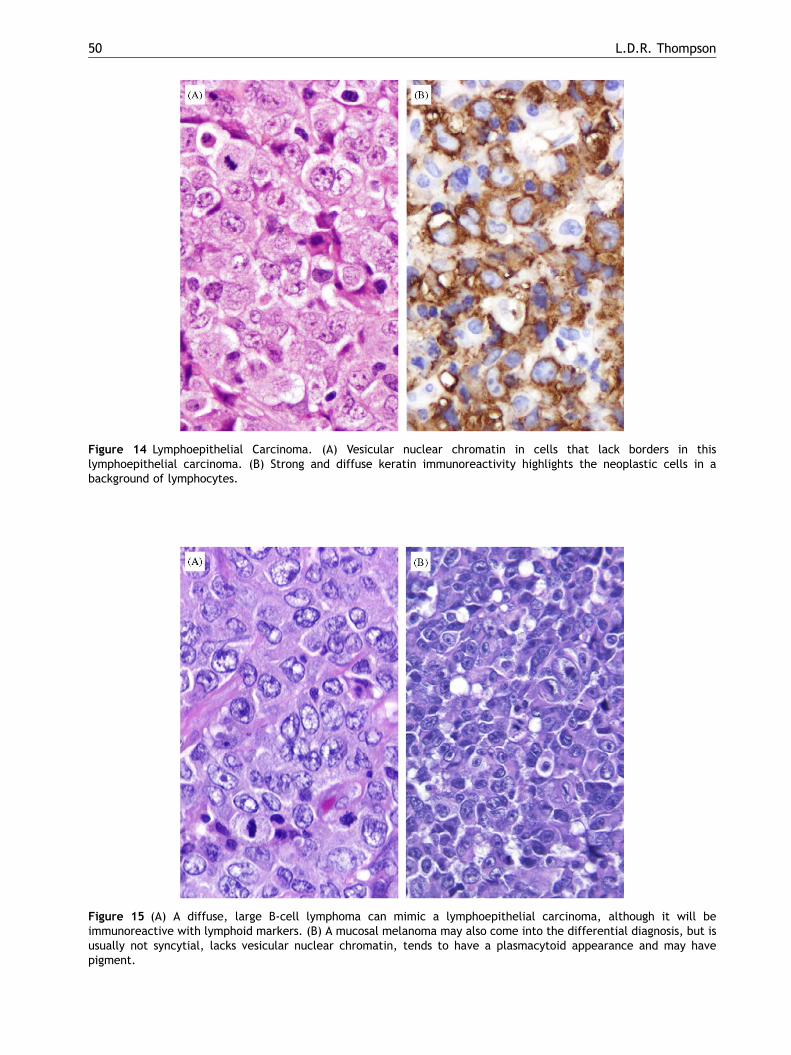
The tumour cells can be confirmed as epithelialwith a strong and diffuse reaction with pan-keratin(Fig. 14), often highlighting wisps of cytoplasm in areticular pattern as they surround lymphocytes (ifpresent).7 Epithelial membrane antigen can beused as an alternative. EBV is found in nearly100% of tumours, most reliably detected using thein situ hybridization technique for EBER, which willshow strong nuclear labelling in nearly all tumourcells.7,30–32 The lymphoid cells react with acompartmentalized mixture of B- and T-cells,supporting a reactive population.
Differential diagnosis
Histological separation of lymphoepithelial carci-noma from SNUC, lymphoma, Hodgkin lymphomaand malignant melanoma is essential as each ofthese lesions has a different treatment and out-come.30,31 SNUC tends to be much more pleo-morphic, has central necrosis, is a bulky tumourand tends to have a high mitotic index. Most SNUCsare EBV-negative, although this finding should notbe solely relied upon in Asian patients.32,33 Im-munohistochemical stains are essential for reachinga definitive diagnosis for separation between alymphoma and a melanoma (Fig. 15). Hodgkinlymphoma is uncommon in the sinonasal tract,but Reed–Sternberg cells should be identified withappropriate confirmatory immunohistochemistry.
ARTICLE IN PRESS
Figure 14 Lymphoepithelial Carcinoma. (A) Vesicular nuclear chromatin in cells that lack borders in thislymphoepithelial carcinoma. (B) Strong and diffuse keratin immunoreactivity highlights the neoplastic cells in abackground of lymphocytes.
Figure 15 (A) A diffuse, large B-cell lymphoma can mimic a lymphoepithelial carcinoma, although it will beimmunoreactive with lymphoid markers. (B) A mucosal melanoma may also come into the differential diagnosis, but isusually not syncytial, lacks vesicular nuclear chromatin, tends to have a plasmacytoid appearance and may havepigment.
L.D.R. Thompson50
ARTICLE IN PRESS
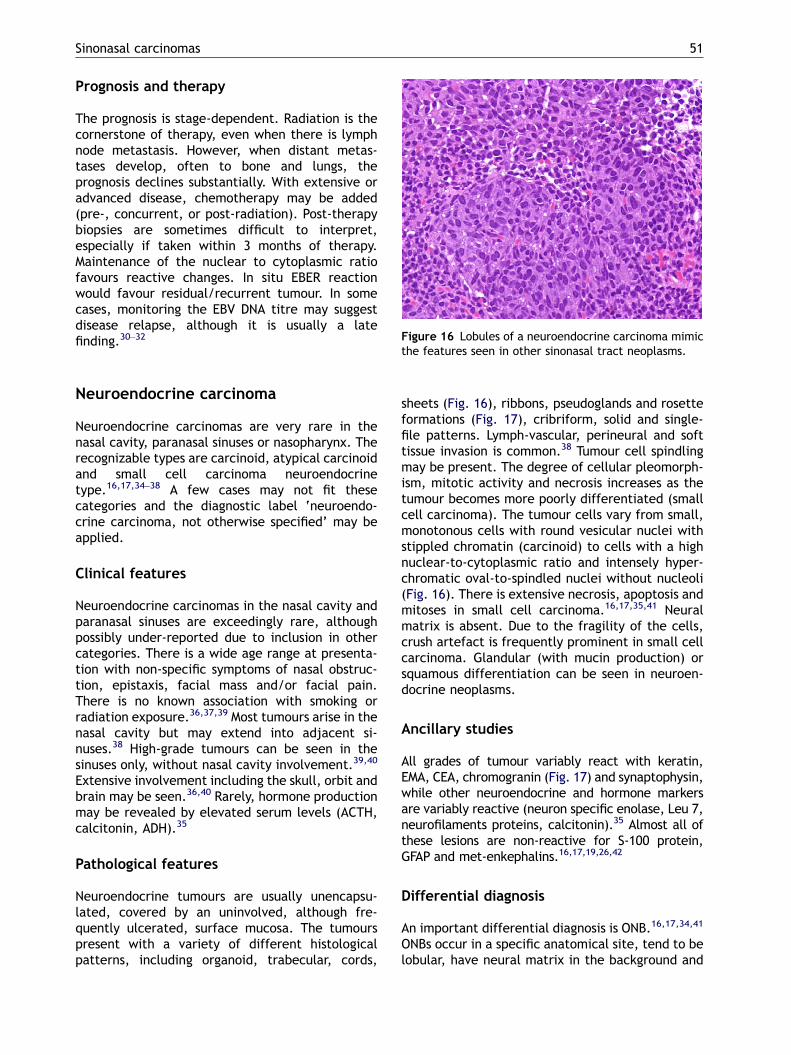
Figure 16 Lobules of a neuroendocrine carcinoma mimic
Sinonasal carcinomas 51
Prognosis and therapy
The prognosis is stage-dependent. Radiation is thecornerstone of therapy, even when there is lymphnode metastasis. However, when distant metas-tases develop, often to bone and lungs, theprognosis declines substantially. With extensive oradvanced disease, chemotherapy may be added(pre-, concurrent, or post-radiation). Post-therapybiopsies are sometimes difficult to interpret,especially if taken within 3 months of therapy.Maintenance of the nuclear to cytoplasmic ratiofavours reactive changes. In situ EBER reactionwould favour residual/recurrent tumour. In somecases, monitoring the EBV DNA titre may suggestdisease relapse, although it is usually a latefinding.30–32
the features seen in other sinonasal tract neoplasms.
Neuroendocrine carcinoma
Neuroendocrine carcinomas are very rare in thenasal cavity, paranasal sinuses or nasopharynx. Therecognizable types are carcinoid, atypical carcinoidand small cell carcinoma neuroendocrinetype.16,17,34–38 A few cases may not fit thesecategories and the diagnostic label ‘neuroendo-crine carcinoma, not otherwise specified’ may beapplied.
Clinical features
Neuroendocrine carcinomas in the nasal cavity andparanasal sinuses are exceedingly rare, althoughpossibly under-reported due to inclusion in othercategories. There is a wide age range at presenta-tion with non-specific symptoms of nasal obstruc-tion, epistaxis, facial mass and/or facial pain.There is no known association with smoking orradiation exposure.36,37,39 Most tumours arise in thenasal cavity but may extend into adjacent si-nuses.38 High-grade tumours can be seen in thesinuses only, without nasal cavity involvement.39,40
Extensive involvement including the skull, orbit andbrain may be seen.36,40 Rarely, hormone productionmay be revealed by elevated serum levels (ACTH,calcitonin, ADH).35
Pathological features
Neuroendocrine tumours are usually unencapsu-lated, covered by an uninvolved, although fre-quently ulcerated, surface mucosa. The tumourspresent with a variety of different histologicalpatterns, including organoid, trabecular, cords,
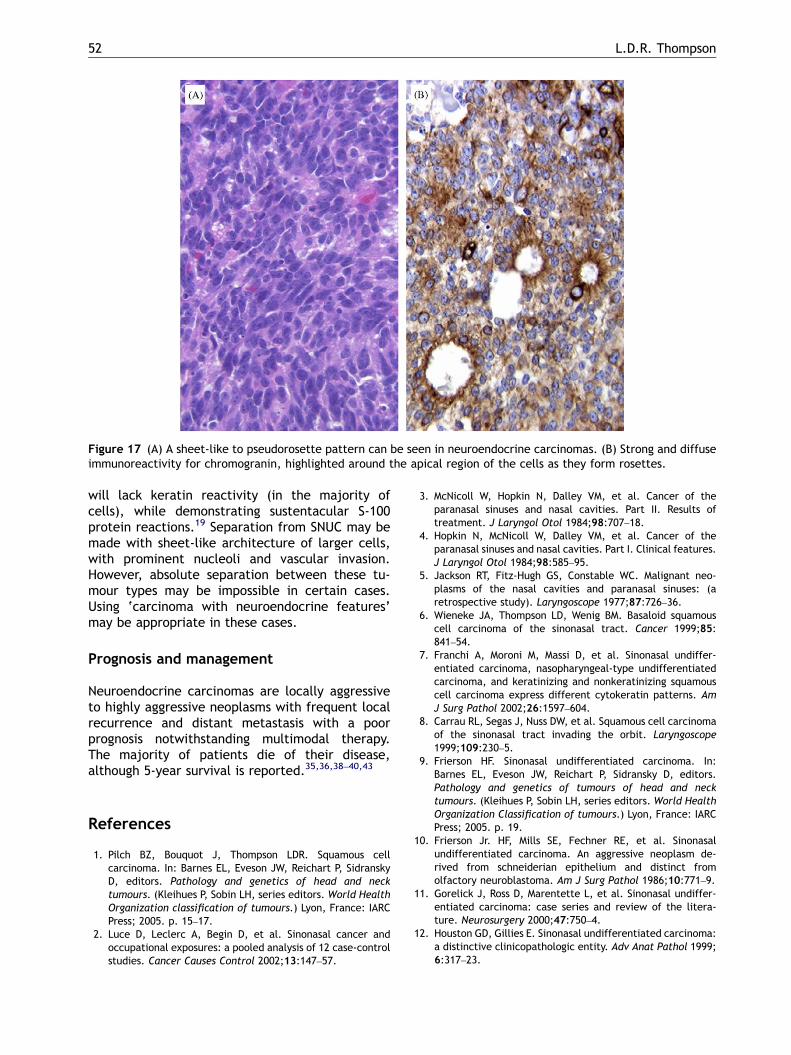
sheets (Fig. 16), ribbons, pseudoglands and rosetteformations (Fig. 17), cribriform, solid and single-file patterns. Lymph-vascular, perineural and softtissue invasion is common.38 Tumour cell spindlingmay be present. The degree of cellular pleomorph-ism, mitotic activity and necrosis increases as thetumour becomes more poorly differentiated (smallcell carcinoma). The tumour cells vary from small,monotonous cells with round vesicular nuclei withstippled chromatin (carcinoid) to cells with a highnuclear-to-cytoplasmic ratio and intensely hyper-chromatic oval-to-spindled nuclei without nucleoli(Fig. 16). There is extensive necrosis, apoptosis andmitoses in small cell carcinoma.16,17,35,41 Neuralmatrix is absent. Due to the fragility of the cells,crush artefact is frequently prominent in small cellcarcinoma. Glandular (with mucin production) orsquamous differentiation can be seen in neuroen-docrine neoplasms.
Ancillary studies
All grades of tumour variably react with keratin,EMA, CEA, chromogranin (Fig. 17) and synaptophysin,while other neuroendocrine and hormone markersare variably reactive (neuron specific enolase, Leu 7,neurofilaments proteins, calcitonin).35 Almost all ofthese lesions are non-reactive for S-100 protein,GFAP and met-enkephalins.16,17,19,26,42
Differential diagnosis
An important differential diagnosis is ONB.16,17,34,41
ONBs occur in a specific anatomical site, tend to belobular, have neural matrix in the background and
ARTICLE IN PRESS
Figure 17 (A) A sheet-like to pseudorosette pattern can be seen in neuroendocrine carcinomas. (B) Strong and diffuseimmunoreactivity for chromogranin, highlighted around the apical region of the cells as they form rosettes.
L.D.R. Thompson52
will lack keratin reactivity (in the majority ofcells), while demonstrating sustentacular S-100protein reactions.19 Separation from SNUC may bemade with sheet-like architecture of larger cells,with prominent nucleoli and vascular invasion.However, absolute separation between these tu-mour types may be impossible in certain cases.Using ‘carcinoma with neuroendocrine features’may be appropriate in these cases.
Prognosis and management
Neuroendocrine carcinomas are locally aggressiveto highly aggressive neoplasms with frequent localrecurrence and distant metastasis with a poorprognosis notwithstanding multimodal therapy.The majority of patients die of their disease,although 5-year survival is reported.35,36,38–40,43
References
1. Pilch BZ, Bouquot J, Thompson LDR. Squamous cellcarcinoma. In: Barnes EL, Eveson JW, Reichart P, SidranskyD, editors. Pathology and genetics of head and necktumours. (Kleihues P, Sobin LH, series editors. World HealthOrganization classification of tumours.) Lyon, France: IARCPress; 2005. p. 15–17.
2. Luce D, Leclerc A, Begin D, et al. Sinonasal cancer andoccupational exposures: a pooled analysis of 12 case-controlstudies. Cancer Causes Control 2002;13:147–57.
3. McNicoll W, Hopkin N, Dalley VM, et al. Cancer of theparanasal sinuses and nasal cavities. Part II. Results oftreatment. J Laryngol Otol 1984;98:707–18.
4. Hopkin N, McNicoll W, Dalley VM, et al. Cancer of theparanasal sinuses and nasal cavities. Part I. Clinical features.J Laryngol Otol 1984;98:585–95.
5. Jackson RT, Fitz-Hugh GS, Constable WC. Malignant neo-plasms of the nasal cavities and paranasal sinuses: (aretrospective study). Laryngoscope 1977;87:726–36.
6. Wieneke JA, Thompson LD, Wenig BM. Basaloid squamouscell carcinoma of the sinonasal tract. Cancer 1999;85:841–54.
7. Franchi A, Moroni M, Massi D, et al. Sinonasal undiffer-entiated carcinoma, nasopharyngeal-type undifferentiatedcarcinoma, and keratinizing and nonkeratinizing squamouscell carcinoma express different cytokeratin patterns. AmJ Surg Pathol 2002;26:1597–604.
8. Carrau RL, Segas J, Nuss DW, et al. Squamous cell carcinomaof the sinonasal tract invading the orbit. Laryngoscope1999;109:230–5.
9. Frierson HF. Sinonasal undifferentiated carcinoma. In:Barnes EL, Eveson JW, Reichart P, Sidransky D, editors.Pathology and genetics of tumours of head and necktumours. (Kleihues P, Sobin LH, series editors. World HealthOrganization Classification of tumours.) Lyon, France: IARCPress; 2005. p. 19.
10. Frierson Jr. HF, Mills SE, Fechner RE, et al. Sinonasalundifferentiated carcinoma. An aggressive neoplasm de-rived from schneiderian epithelium and distinct fromolfactory neuroblastoma. Am J Surg Pathol 1986;10:771–9.
11. Gorelick J, Ross D, Marentette L, et al. Sinonasal undiffer-entiated carcinoma: case series and review of the litera-ture. Neurosurgery 2000;47:750–4.
12. Houston GD, Gillies E. Sinonasal undifferentiated carcinoma:a distinctive clinicopathologic entity. Adv Anat Pathol 1999;6:317–23.
ARTICLE IN PRESS
Sinonasal carcinomas 53
13. Gallo O, Graziani P, Fini-Storchi O. Undifferentiated carci-noma of the nose and paranasal sinuses. An immunohisto-chemical and clinical study. Ear Nose Throat J 1993;72588–95.
14. Phillips CD, Futterer SF, Lipper MH, et al. Sinonasalundifferentiated carcinoma: CT and MR imaging of anuncommon neoplasm of the nasal cavity. Radiology 1997;202:477–80.
15. Miyamoto RC, Gleich LL, Biddinger PW, et al. Esthesioneur-oblastoma and sinonasal undifferentiated carcinoma: im-pact of histological grading and clinical staging on survivaland prognosis. Laryngoscope 2000;110:1262–5.
16. Mills SE, Fechner RE. ‘Undifferentiated’ neoplasms of thesinonasal region: differential diagnosis based on clinical,light microscopic, immunohistochemical, and ultrastructur-al features. Semin Diagn Pathol 1989;6:316–28.
17. Ordonez NG, Mackay B. Neuroendocrine tumors of the nasalcavity. Pathol Annu 1993;28:77–111.
18. Cerilli LA, Holst VA, Brandwein MS, et al. Sinonasal undiffer-entiated carcinoma: immunohistochemical profile and lack ofEBV association. Am J Surg Pathol 2001;25:156–63.
19. Smith SR, Som P, Fahmy A, et al. A clinicopathological studyof sinonasal neuroendocrine carcinoma and sinonasal un-differentiated carcinoma. Laryngoscope 2000;110:1617–22.
20. Hwang TZ, Jin YT, Tsai ST. EBER in situ hybridizationdifferentiates carcinomas originating from the sinonasalregion and the nasopharynx. Anticancer Res 1998;18:4581–4.
21. Wenig BM, Dulguerow P, Kapadia SB, Prasad ML, Fanburg-Smith JC, Thompson LDR. Neuroectodermal tumours. In:Barnes EL, Eveson JW, Reichart P, Sidransky D, editors.Pathology and genetics of tumours of head and necktumours. (Kleihues P, Sobin LH, series editors. World HealthOrganization classification of tumours.) Lyon, France: IARCPress; 2005. p. 66–76.
22. Mills SE, Frierson Jr. HF. Olfactory neuroblastoma. Aclinicopathologic study of 21 cases. Am J Surg Pathol 1985;9:317–27.
23. Dulguerov P, Allal AS, Calcaterra TC. Esthesioneuroblastoma: ameta-analysis and review. Lancet Oncol 2001;2:683–90.
24. Lund VJ, Howard D, Wei W, et al. Olfactory neuroblastoma:past, present, and future? Laryngoscope 2003;113:502–7.
25. Devaney K, Wenig BM, Abbondanzo SL. Olfactory neuroblas-toma and other round cell lesions of the sinonasal region.Mod Pathol 1996;9:658–63.
26. Devoe K, Weidner N. Immunohistochemistry of small round-cell tumors. Semin Diagn Pathol 2000;17:216–24.
27. Argani P, Perez-Ordonez B, Xiao H, et al. Olfactoryneuroblastoma is not related to the Ewing family of tumors:absence of EWS/FLI1 gene fusion and MIC2 expression. Am JSurg Pathol 1998;22:391–8.
28. Righi PD, Francis F, Aron BS, et al. Sinonasal undifferentiatedcarcinoma: a 10-year experience. Am J Otolaryngol 1996;17:167–71.
29. Rischin D, Porceddu S, Peters L, et al. Promising results withchemoradiation in patients with sinonasal undifferentiatedcarcinoma. Head Neck 2004;26:435–41.
30. Zong Y, Liu K, Zhong B, et al. Epstein–Barr virus infection ofsinonasal lymphoepithelial carcinoma in Guangzhou. ChinMed J (Engl) 2001;114:132–6.
31. Tsang WYW, Chan JKC. Lymphoepithelial carcinoma. In:Barnes EL, Eveson JW, Reichart P, Sidransky D, editors.Pathology and genetics of tumours of head and necktumours. (Kleihues P, Sobin LH, series editors. World HealthOrganization classification of tumours.) Lyon, France: IARCPress; 2005. p. 18.
32. Jeng YM, Sung MT, Fang CL, et al. Sinonasal undifferentiatedcarcinoma and nasopharyngeal-type undifferentiated carci-noma: two clinically, biologically, and histopathologicallydistinct entities. Am J Surg Pathol 2002;26:371–6.
33. Lopategui JR, Gaffey MJ, Frierson Jr. HF, et al. Detection ofEpstein–Barr viral RNA in sinonasal undifferentiated carci-noma from Western and Asian patients. Am J Surg Pathol1994;18:391–8.
34. Mills SE. Neuroectodermal neoplasms of the head and neckwith emphasis on neuroendocrine carcinomas. Mod Pathol2002;15:264–78.
35. Vasan NR, Medina JE, Canfield VA, et al. Sinonasalneuroendocrine carcinoma in association with SIADH. HeadNeck 2004;26:89–93.
36. Rosenthal DI, Barker Jr. JL, el Naggar AK, et al. Sinonasalmalignancies with neuroendocrine differentiation: patternsof failure according to histologic phenotype. Cancer2004;101:2567–73.
37. Noguchi K, Urade M, Kishimoto H, et al. Establishment of anew cell line with neuronal differentiation derived fromsmall cell neuroendocrine carcinoma of the maxillary sinus.Oncology 2004;66:234–43.
38. Perez-Ordonez B, Caruana SM, Huvos AG, et al. Small cellneuroendocrine carcinoma of the nasal cavity and paranasalsinuses. Hum Pathol 1998;29:826–32.
39. Georgiou AF, Walker DM, Collins AP, et al. Primary small cellundifferentiated (neuroendocrine) carcinoma of the max-illary sinus. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2004;98:572–8.
40. Galanis E, Frytak S, Lloyd RV. Extrapulmonary small cellcarcinoma. Cancer 1997;79:1729–36.
41. Watanabe K, Ogura G, Suzuki T. Intra-epithelial neuroendo-crine carcinoma of the nasal cavity. Pathol Int 2003;53:396–400.
42. Ordonez NG. Value of thyroid transcription factor-1 im-munostaining in distinguishing small cell lung carcinomasfrom other small cell carcinomas. Am J Surg Pathol2000;24:1217–23.
43. Galera-Ruiz H, Villar-Rodriguez JL, Sanchez-Calzado JA, etal. Sinonasal neuroendocrine carcinoma presenting as anasopharyngeal mass. Otolaryngol Head Neck Surg 2001;124:475–6.