Embed Size (px)
Citation preview
ava i l ab l e a t www.sc i enced i rec t . com
www.e l sev i e r. com/ l oca te / ea r l humdev
Early Human Development (2008) 84, 577–585
Sleep fragmentation and evidence for sleep debt inalcohol-exposed infantsMarcia Troese a, Michio Fukumizua,b, Bethany J. Sallinena,Allyson A. Gilles a, Joseph D. Wellman a, Jonathan A. Paul c,Eric R. Brownd, Marie J. Hayes a,c,d,e,⁎
a Department of Psychology, University of Maine, Orono, ME, United Statesb Department of Child Neurology, National Institute of Neuroscience, National Center of Neurology and Psychiatry,Kodaira, Tokyo, Japanc Graduate School of Biomedical Sciences, University of Maine, Orono, ME, United Statesd Eastern Maine Medical Center, Bangor, Maine, United Statese Maine Institute of Human Genetics and Health, Brewer, ME, United States
Received 28 September 2007; received in revised form 5 February 2008; accepted 11 February 2008
⁎ Corresponding author. University ofStates. Tel.: +1 207 973 4963; fax: +1
E-mail address: [email protected]
0378-3782/$ - see front matter © 200doi:10.1016/j.earlhumdev.2008.02.001
KEYWORDSPrenatal alcohol exposure;Sleep fragmentation;Arousal;Movements;SIDS
Abstract
Background: Infants exposed prenatally to alcohol are at increased risk for poor neurodevelop-mental outcome including Sudden Infant Death Syndrome.Aim: To examine the relationship between prenatal alcohol exposure, sleep, arousal and sleep-related spontaneous motor movements in early infancy.Study design: Low-income women (N=13) were interviewed regarding pre- and pregnancy rates
of alcohol, cigarette smoking and other substance use in the perinatal period. Infants wereexamined in a laboratory nap study using EEG, videography and actigraphy at 6–8 weeks of age.Estimates of maternal pre- and pregnancy alcohol use were used to divide infants into high vs.low maternal alcohol use groups.Subjects: Mother–infant dyads recruited from a family practice clinic.Outcome measures: Sleep-related spontaneous movements, behavioral state, and maternalassessments of infant alertness and irritability.Results: Pre-pregnancy rates of alcohol consumption including binge drinking correlated withmaternal report of poor infant alertness, and increased irritability. High maternal exposuregroups showed increased sleep fragmentation, e.g. frequency and duration of wakefulnessfollowing sleep onset and decreased active sleep. Bout analysis of the temporal structure ofsleep-related spontaneous movements showed significantly reduced bout duration associatedwith high maternal alcohol use.Maine & Maine Institute of Human Genetics and Health, 43 Whiting Hill Rd., Brewer, ME 04412, United207 973 5640.u (M.J. Hayes).
8 Published by Elsevier Ireland Ltd.

578 M. Troese et al.
Conclusion: These results present evidence that prenatal alcohol exposure disrupts postnatalsleep organization and suppresses spontaneous movements during sleep, and increased sleepfragmentation promotes sleep deprivation. Results are consistent with the SIDS model of chronicsleep debt and suggest that attenuated sleep-related movements should be examined as animportant modulator of cardiorespiratory functions during sleep in high-risk groups.© 2008 Published by Elsevier Ireland Ltd.
1. Introduction
It is well known that prenatal alcohol exposure is teratogenicto the developing fetal brain [1–4]. Low levels of prenatalalcohol reported by using quantity-frequency-variabilitymethods of maternal interview correlate to pre-pregnancyreported rates [5–8]. Heavy episodic alcohol exposureprenatally (e.g. binge drinking) has been determined to bea critical determinant of functional impairment in humansand dose-dependent apoptotic neurodegeneration in animals[9] at all prenatal stages affecting rapidly developing neuralcircuitry at the time of the insult [10,11].
Homeostatic and circadian control of sleep and arousalsystems in alcohol-exposed infants has been little studied todate, although the effects in adults are characterized byrapid sleep onset but within sleep arousal disturbances after2–3 h [12]. Developmental animal work has found permanenteffects of prenatal alcohol exposure on biological rhythmtiming systems [13], suggesting that prenatal alcohol maydisrupt sleep and arousal systems in a fundamental way. Inthe first investigation of neonatal sleep and alcoholexposure, Rosett et al. reported that neonates had morefrequent arousals and large body movements when motherswere heavy drinkers [14]. Scher et al. reported poorer sleepparticularly in infants exposed to alcohol after the firsttrimester [15]. More recently, this group has reported thatprenatal alcohol, as well as marijuana and tobacco use,disrupts sleep state cycle length and EEG periodicity in thealpha range indicative of developmental delay [16]. In awell-controlled recent study, Mulder et al. found thatexposure to maternal alcohol during fetal life disruptedbehavioral state organization, particularly active sleep, andsuppressed breathing movements [17]. Consistent with thisfinding, Mennella found that infants slept less and had morearousals and less active sleep after exposure to alcohol inexpressed breast milk [18].
The links between prenatal risk factors for Sudden InfantDeath Syndrome (SIDS) are well established, and includeprenatal exposure to alcohol, although the mechanisms arenot known. Epidemiological risk-ratios that are 2–9 timeshigher are found in association with prematurity [19], historyof apnea [20], prenatal exposures including tobacco [21] andalcohol [22]. Adverse prenatal and/or perinatal conditionsrelated to maternal substance abuse, infant medical condi-tions such as apnea, etc. are hypothesized to promotedamage and/or developmental delay to brainstem neurocir-cuitry involved in the integrated arousal regulatory system,including the medulla oblongata [15]. Recent reports haveshown serotonergic deficiencies in the medulla oblongata inSIDS cases derived from a Plains Indian sample with high ratesof prenatal alcohol exposure [23,24].
Spontaneous movements as a potential state independentdevelopmental protectivemechanismhave not been examinedfor SIDS [25–28]. When spontaneous movements occur periodi-cally, the effect on motor activation is to: 1.) restore airwaypatency through increasedmotor tone [29–31]; 2.) reset respi-ratory cycles through somatic stimulation of the parabrachialand other medullary neural circuits [32]. Brain stem circuitscontrolling autonomic function and sleep and arousal organiza-tion develop rapidly in the first few months of life; however,high-risk infantswith prenatal exposures, e.g. tobacco, alcoholand other substances, often show evidence of poor regulationand sleep deprivation [33–36].
In the present study, we applied the translational methodswe have developed for studying spontaneous movements inthe human infant, with the goal of examining the frequency,duration and temporal patterning of spontaneous move-ments within the sleep period independent of waking per se[25,26]. We propose that the activational effect of periodicmovements may be protective in maintaining cardiorespira-tory tone during sleep period when infants are mostvulnerable to prolonged apnea and autonomic instability.Using this method allowed us to study the relationship ofsleep and movement patterns to maternal alcohol use in adisadvantaged, Caucasian cohort that had been character-ized as high use previously [37]. We examined the relation-ship of various measures of alcohol use to infant sleep,arousal and sleep-related spontaneous movements in thehigh-risk SIDS age of circa 2 months. We hypothesized thatinfants with mothers showing evidence of alcohol abusewould have poor sleep-wake organization and atypicaltemporal organization cyclic spontaneous movements duringsleep that were independent of movement associated witharousals and awakenings.
2. Methods
2.1. Subjects
Participants were mother–infant dyads (N=13) recruited froma prenatal clinic serving primarily disadvantaged families inNortheastern Maine. Previously, we established that womenfrom this cohort were primarily Caucasian, had high alcoholand tobacco use, but less use of other intoxicating substances[37]. All pregnancies were N36 GA, and participant dyads wereexcluded for congenital abnormalities, obstetrical complica-tions leading to admission to the NICU, or infants who weresmall for gestational age. This study was approved by theInstitutional Review Boards of the University of Maine andEastern Maine Medical Center, and informed consent wasobtained from each participant.

579Infant sleep and prenatal alcohol exposure
2.2. Maternal assessments
2.2.1. Peabody Picture Vocabulary Test—Third Edition(PPVT-III)Peabody Picture Vocabulary Test—Third Edition (PPVT-III)measures an individual's receptive vocabulary attainment forstandard English and is a screening test of verbal ability andintellectual functioning [38].
2.2.2. Four-Factor Index of Social StatusFour-Factor Index of Social Status [39]. The four factorsinclude education, occupation, marital status, and sex. Theeducational factor and occupational status of the motherswere used to obtain scores estimating socioeconomic status.
2.2.3. Alcohol and drug use: quantity-frequency-variability methodAlcohol and drug use: quantity–frequency–variability method[40]. Recent and retrospective patterns of use were assessedduring a confidential structured interview during a typicalweek retrospectively for the quantity, frequency, and varia-bility of alcohol and other substance use. Absolute alcoholamounts were estimated by comparing type of alcohol, size ofcontainer, and number of drinks of each type. Several derivedmeasures of relative alcohol consumption were used in theanalyses: average absolute alcohol per day (AA/day), averageAAper drinking day (AA/DD), and number of daysmother drankN2.5 oz of AA during the pregnancy.
2.2.4. Michigan Alcohol Screening Test (MAST)Michigan Alcohol Screening Test (MAST) [41] is a structuredinterview consisting of 25 questions that emphasize a historyof problems associated with alcohol.
2.2.5. T-ACET-ACE [42] is used as a screening tool to determine toleranceplus three questions from the CAGE [43] for alcoholaddiction.
2.2.6. TWEAKTWEAK [44] is a 6 question screening tool used to identifywomen who are risk drinkers. The TWEAK is more sensitivebut less specific than the T-ACE in detecting pregnancy riskdrinking [43].
2.2.7. Beck Depression Inventory—Second Edition (BDI-II)Beck Depression Inventory—Second Edition (BDI-II) [45] is a21-item self-report questionnaire that assesses an indivi-dual's symptoms of depression during the past 2 weeks on a 4-point scale.
2.3. Infant assessments
2.3.1. Mother and Baby Scales (MABS)Mother and Baby Scales (MABS) [46] is a 43-item self-reportquestionnaire that includes 5 subscales: Unsettled–Irregular,Alertness–Responsiveness, Easiness, Parental Lack of Con-fidence in Caretaking, and Global Parental Confidence.
2.3.2. Sleep recordingsInfant sleep state organization was measured using electro-encephalography (EEG), electro-oculogram (EOG), actigra-
phy (using a 10 mm×10 mm piezoelectric sensor placedunder the infants head and torso), and infrared time-synchronized videography. Hardware consisted of a Grass15Rxi-15A54 AC/DC amplifier with a compatible EEG boardand a piezoelectric sensor for measuring movementsincluding respiration. The hardware was interfaced to alaptop computer where the data were fed into recordingsoftware at a sampling rate of 64 samples/s. The GrassLink15 amplifier calibration software and Grass PolyViewdata acquisition software allowed the monitoring of eightchannels of input: bipolar EEG (Fp1-C3, C3-O1, Fp2-C4, C4-O2), a mastoid ground, bilateral EOG, and the piezoelec-tric sensor. These phase-locked signals had calibration set-tings of 50 uV, a sampling rate of 100/s, low and high filtersettings at 0.3 and 100 Hz respectively. The piezoelectricmattress used an internal electrical field to determinedifferences in pressure and to measure bouts of movement.The amplifier provided the internal electrical field that thepiezoelectric mattress used to calibrate these differencesin pressure. The sensitivity gains of the sensor was set torecord respirations in a still infant up to and including fullbody activity.
2.3.3. Behavioral statesBehavioral categories for coding sleep states are shown inTable 1 and were based on an adaptation of the criteria fromThoman et al. [47], in 1 min samples with a 3 min smoothingmethod as described by Anders et al. [48]. Criteria for eachstate must be met consecutively for a minimum of 1.5 min ofeach 3-min bin or no state change was recorded. A 3-minwindow with the criterion of 1.5 min of a single state forcoding allows for transient states to be smoothed whileretaining ongoing stable states [49,50]. Arousals were codedwhen a minimum of 1 min to b1.5 min behavioral criteriaweremet; durations above 1.5minwere coded aswake state.
2.3.4. ActigraphyThe temporal structure of movement bouts was examined bythree methods using the same algorithm to reflect bothmicro- and macrostructural features of sleep movements andquiescence periods during the sleep period. For theseanalyses, wake epochs were removed from the actigraphydata by comparison of actigraphy and phase-locked video-graphy to examine movements during sleep separately fromwake periods.
The absolute value of the digitized output was used todetermine the average movement for each record sepa-rately to establish a referent value representative of therange of movement velocity expressed by each infantacross the sleep period. Next, the data stream was binnedinto 6 s, 12 s, or 1 min epochs. The average movementscore was determined for each bin and was compared tothe overall session mean. Each bin was assigned a value of0 or 1 depending on whether the average value for that binwas above or below the average session referent. Thismethod corrected for individual differences in infantweight that influence the velocity of the piezoelectriccircuit. The bout structure analysis yielded a measure ofthe temporal distribution of movement bouts that quanti-fied the number, average duration, and maximum durationduring the nap recording. Quiescence was analyzed in amirror fashion.

Table 1 Behavioral state coding criteria
Wake: The infant's eyes are open, focused, and scanning the environment, and at times may appear tobe crying or fussing. Motor activity of the infant, if any, is usually oriented towards theenvironment, and respiration is even.
Brief arousal: The infant's eyes are open, focused, and scanning the environment. Motor activity, if present,is oriented towards the surroundings.
Drowse: The infant's eyes open and close slowly or may be open but dazed with a “heavy-lidded”appearance. Characteristics of both sleep and wake states are present, and respiration is even.
Active sleep: The infant's eyes are closed with periodic REMs occurring. Motor activity is sporadic withmuscle tone remaining low between movements. Typically respiration is uneven and costal innature.
Quiet sleep: The infant's eyes are shut. Motor activity is low, but muscle tone is maintained. Occasionalmouthing behaviors may or may not occur. The infant's respiration is even and abdominal innature.
Indeterminate sleep: Characteristics of two or more states are present, with the exception of active sleep features.State transitions: Changes in sleep states that occur during videotaping.State-changing interventions: Any touching or physical contact from the parent or research assistant that changes the infant's
behavioral state.
580 M. Troese et al.
2.4. Procedure
Maternal assessment of alcohol and substance use andcurrent psychological functioning measures were collectedat the third trimester intake or 1-month post birth. Atintake, the PPVT-III, Hollingshead Index and depressionmeasures were administered. Mothers were interviewedregarding their current and retrospective substance useusing the MAST, the TWEAK, and the T-ACE. Ten of 13mothers were interviewed in the early perinatal period andestimated their third trimester pregnancy drinking in atypical week.
2.4.1. Sleep studyBetween 6 and 8 weeks of age the mother–infant dyadsreturned to the hospital laboratory for a scheduled sleepstudy during a typical, post-feed, daytime nap. During thefeed, 10–20 calculations were made for standard bipolarelectrodes attached to ocular, frontal, central and occipitalsites bilaterally. To measure spontaneous movementsduring sleep, infants were placed on their backs in acommercial portable crib in which a piezoelectric acti-graphic mattress (10 mm×10 mm) was centered at thescapulae and reached from the lower head to the buttocks[25,26]. A real-time video recorder with infrared capacitywas positioned 2 m from the crib and documented arousalsand behavioral state from sleep onset until spontaneousawakening.
After the infant fell asleep at the breast or bottle, theinfant was placed in the crib, the room was darkenedand the sleep study commenced. In the Universitylaboratory, behavioral state was coded for sleep andwaking states by trained student research coding assis-tants blind to the hypotheses of the study. Total sleeptime (TST), state parameters (percent, epoch frequencyand duration) of wake (W), quiet sleep (QS), active sleep(AS), drowse (D) and state transitions were coded. Tapeswere recoded for reliability (Kappa coefficients rangedfrom 0.65–0.94).
2.5. Statistical analysis
All analyses were conducted using SPSS for Windows 14.0Standard Version (SPSS Inc.). Pair-wise Pearson's product-moment correlations were used to examine some of therelationships between infant developmental measures andpregnancy, pre-pregnancy and perinatal estimates of alco-hol use. Post-hoc group analyses were conducted forsome alcohol measures using median split to divide thesample into low vs. high maternal alcohol use groups. MAST,pre-pregnancy AA/DD and binge AA/occasion were logtransformed to correct for skewness (X=logX+1), and Stu-dent's t-tests were used to compare groups on various infantoutcome measures.
3. Results
3.1. Maternal demographics
Maternal mean age was 24.5±3.62 years range=19–29.Obtained scores on the PPVT-III were within the averagerange (mean=99.6; range=87–110). Unemployed women(n=7) were not calculated in the score because the Hollings-head estimates social status for individuals gainfully em-ployed at the time of assessment. Mothers had scores rangingfrom 15.5 to 39.0 on the Hollingshead Four-Factor Index, withan average of 26.5±7.5 consistent with the category of Semi-skilled Workers on the Occupational Scale [39].
Average BDI-II scores during pregnancy were 11.4±6.9,(range=5.0–24.0) and after pregnancy was statisticallyunchanged at 11.7±8.9, (range 3.0–31.0); both are withinthe normal range (BDI-II: t(7)=−0.86, p=0.42). Depressionmeasures were not significantly correlated with maternalalcohol consumption estimates.
Table 2 shows the means and standard deviations formaternal pre- and postnatal alcohol and substance use. Withregard to alcohol use history, average MAST and TWEAKscores were 6.7 (range=2.0–21.0) and 3.0 (range=0–6.0)
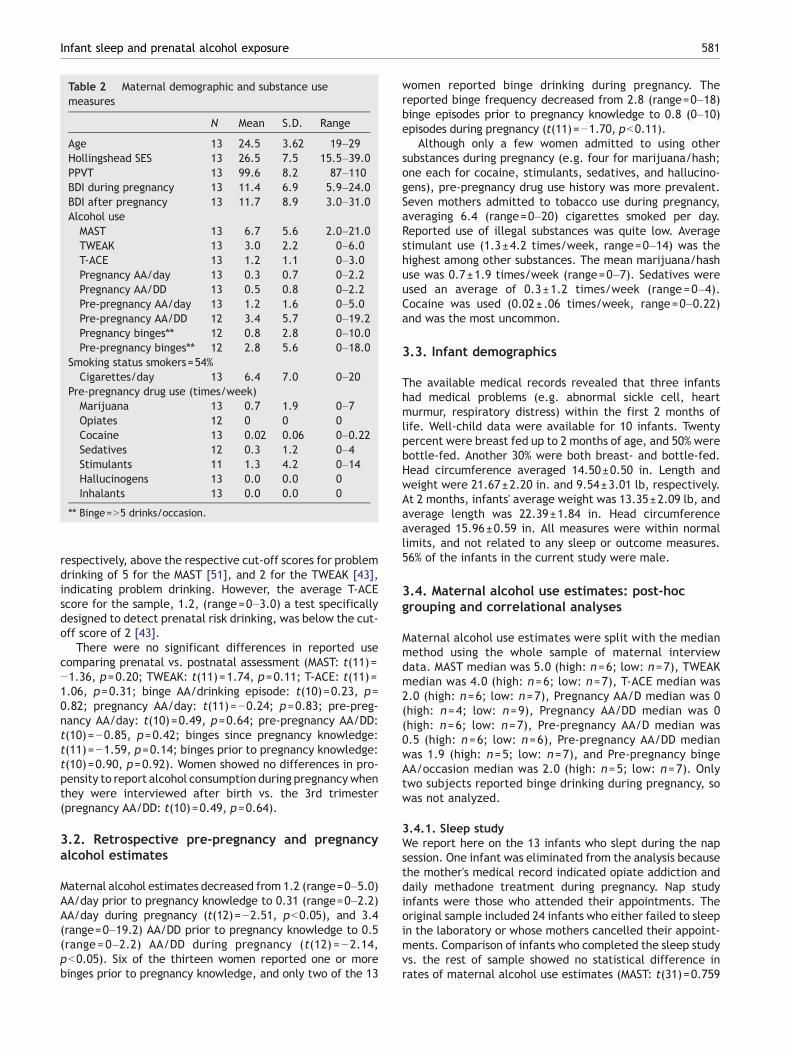
Table 2 Maternal demographic and substance usemeasures
N Mean S.D. Range
Age 13 24.5 3.62 19–29Hollingshead SES 13 26.5 7.5 15.5–39.0PPVT 13 99.6 8.2 87–110BDI during pregnancy 13 11.4 6.9 5.9–24.0BDI after pregnancy 13 11.7 8.9 3.0–31.0Alcohol use
MAST 13 6.7 5.6 2.0–21.0TWEAK 13 3.0 2.2 0–6.0T-ACE 13 1.2 1.1 0–3.0Pregnancy AA/day 13 0.3 0.7 0–2.2Pregnancy AA/DD 13 0.5 0.8 0–2.2Pre-pregnancy AA/day 13 1.2 1.6 0–5.0Pre-pregnancy AA/DD 12 3.4 5.7 0–19.2Pregnancy binges⁎⁎ 12 0.8 2.8 0–10.0Pre-pregnancy binges⁎⁎ 12 2.8 5.6 0–18.0
Smoking status smokers=54%Cigarettes/day 13 6.4 7.0 0–20
Pre-pregnancy drug use (times/week)Marijuana 13 0.7 1.9 0–7Opiates 12 0 0 0Cocaine 13 0.02 0.06 0–0.22Sedatives 12 0.3 1.2 0–4Stimulants 11 1.3 4.2 0–14Hallucinogens 13 0.0 0.0 0Inhalants 13 0.0 0.0 0
⁎⁎ Binge=N5 drinks/occasion.
581Infant sleep and prenatal alcohol exposure
respectively, above the respective cut-off scores for problemdrinking of 5 for the MAST [51], and 2 for the TWEAK [43],indicating problem drinking. However, the average T-ACEscore for the sample, 1.2, (range=0–3.0) a test specificallydesigned to detect prenatal risk drinking, was below the cut-off score of 2 [43].
There were no significant differences in reported usecomparing prenatal vs. postnatal assessment (MAST: t(11)=−1.36, p=0.20; TWEAK: t(11)=1.74, p=0.11; T-ACE: t(11)=1.06, p=0.31; binge AA/drinking episode: t(10)=0.23, p=0.82; pregnancy AA/day: t(11)=−0.24; p=0.83; pre-preg-nancy AA/day: t(10)=0.49, p=0.64; pre-pregnancy AA/DD:t(10)=−0.85, p=0.42; binges since pregnancy knowledge:t(11)=−1.59, p=0.14; binges prior to pregnancy knowledge:t(10)=0.90, p=0.92). Women showed no differences in pro-pensity to report alcohol consumption during pregnancywhenthey were interviewed after birth vs. the 3rd trimester(pregnancy AA/DD: t(10)=0.49, p=0.64).
3.2. Retrospective pre-pregnancy and pregnancyalcohol estimates
Maternal alcohol estimates decreased from 1.2 (range=0–5.0)AA/day prior to pregnancy knowledge to 0.31 (range=0–2.2)AA/day during pregnancy (t(12)=−2.51, pb0.05), and 3.4(range=0–19.2) AA/DD prior to pregnancy knowledge to 0.5(range=0–2.2) AA/DD during pregnancy (t(12) =−2.14,pb0.05). Six of the thirteen women reported one or morebinges prior to pregnancy knowledge, and only two of the 13
women reported binge drinking during pregnancy. Thereported binge frequency decreased from 2.8 (range=0–18)binge episodes prior to pregnancy knowledge to 0.8 (0–10)episodes during pregnancy (t(11)=−1.70, pb0.11).
Although only a few women admitted to using othersubstances during pregnancy (e.g. four for marijuana/hash;one each for cocaine, stimulants, sedatives, and hallucino-gens), pre-pregnancy drug use history was more prevalent.Seven mothers admitted to tobacco use during pregnancy,averaging 6.4 (range=0–20) cigarettes smoked per day.Reported use of illegal substances was quite low. Averagestimulant use (1.3±4.2 times/week, range=0–14) was thehighest among other substances. The mean marijuana/hashuse was 0.7±1.9 times/week (range=0–7). Sedatives wereused an average of 0.3±1.2 times/week (range=0–4).Cocaine was used (0.02±.06 times/week, range=0–0.22)and was the most uncommon.
3.3. Infant demographics
The available medical records revealed that three infantshad medical problems (e.g. abnormal sickle cell, heartmurmur, respiratory distress) within the first 2 months oflife. Well-child data were available for 10 infants. Twentypercent were breast fed up to 2 months of age, and 50% werebottle-fed. Another 30% were both breast- and bottle-fed.Head circumference averaged 14.50±0.50 in. Length andweight were 21.67±2.20 in. and 9.54±3.01 lb, respectively.At 2 months, infants' average weight was 13.35±2.09 lb, andaverage length was 22.39±1.84 in. Head circumferenceaveraged 15.96±0.59 in. All measures were within normallimits, and not related to any sleep or outcome measures.56% of the infants in the current study were male.
3.4. Maternal alcohol use estimates: post-hocgrouping and correlational analyses
Maternal alcohol use estimates were split with the medianmethod using the whole sample of maternal interviewdata. MAST median was 5.0 (high: n=6; low: n=7), TWEAKmedian was 4.0 (high: n=6; low: n=7), T-ACE median was2.0 (high: n=6; low: n=7), Pregnancy AA/D median was 0(high: n=4; low: n=9), Pregnancy AA/DD median was 0(high: n=6; low: n=7), Pre-pregnancy AA/D median was0.5 (high: n=6; low: n=6), Pre-pregnancy AA/DD medianwas 1.9 (high: n=5; low: n=7), and Pre-pregnancy bingeAA/occasion median was 2.0 (high: n=5; low: n=7). Onlytwo subjects reported binge drinking during pregnancy, sowas not analyzed.
3.4.1. Sleep studyWe report here on the 13 infants who slept during the napsession. One infant was eliminated from the analysis becausethe mother's medical record indicated opiate addiction anddaily methadone treatment during pregnancy. Nap studyinfants were those who attended their appointments. Theoriginal sample included 24 infants who either failed to sleepin the laboratory or whose mothers cancelled their appoint-ments. Comparison of infants who completed the sleep studyvs. the rest of sample showed no statistical difference inrates of maternal alcohol use estimates (MAST: t(31)=0.759
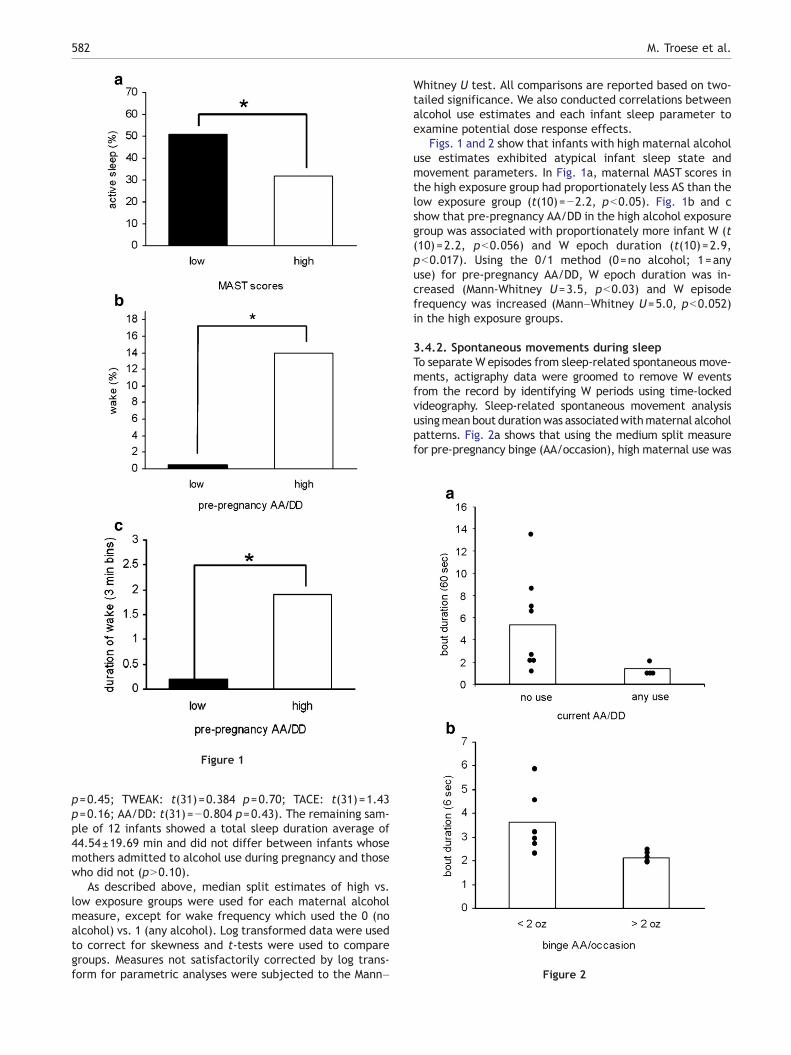
Figure 1
Figure 2
582 M. Troese et al.
p=0.45; TWEAK: t(31)=0.384 p=0.70; TACE: t(31)=1.43p=0.16; AA/DD: t(31)=−0.804 p=0.43). The remaining sam-ple of 12 infants showed a total sleep duration average of44.54±19.69 min and did not differ between infants whosemothers admitted to alcohol use during pregnancy and thosewho did not (pN0.10).
As described above, median split estimates of high vs.low exposure groups were used for each maternal alcoholmeasure, except for wake frequency which used the 0 (noalcohol) vs. 1 (any alcohol). Log transformed data were usedto correct for skewness and t-tests were used to comparegroups. Measures not satisfactorily corrected by log trans-form for parametric analyses were subjected to the Mann–
Whitney U test. All comparisons are reported based on two-tailed significance. We also conducted correlations betweenalcohol use estimates and each infant sleep parameter toexamine potential dose response effects.
Figs. 1 and 2 show that infants with high maternal alcoholuse estimates exhibited atypical infant sleep state andmovement parameters. In Fig. 1a, maternal MAST scores inthe high exposure group had proportionately less AS than thelow exposure group (t(10)=−2.2, pb0.05). Fig. 1b and cshow that pre-pregnancy AA/DD in the high alcohol exposuregroup was associated with proportionately more infant W (t(10)=2.2, pb0.056) and W epoch duration (t(10)=2.9,pb0.017). Using the 0/1 method (0=no alcohol; 1=anyuse) for pre-pregnancy AA/DD, W epoch duration was in-creased (Mann-Whitney U=3.5, pb0.03) and W episodefrequency was increased (Mann–Whitney U=5.0, pb0.052)in the high exposure groups.
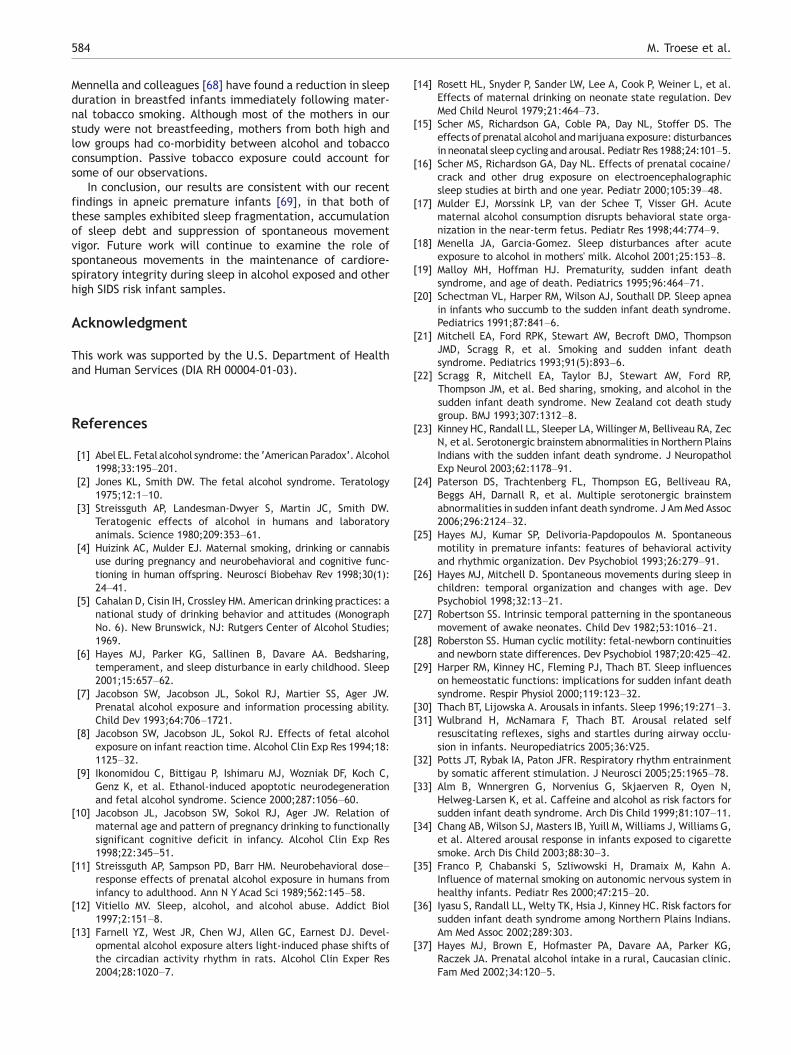
3.4.2. Spontaneous movements during sleepTo separate W episodes from sleep-related spontaneous move-ments, actigraphy data were groomed to remove W eventsfrom the record by identifying W periods using time-lockedvideography. Sleep-related spontaneous movement analysisusingmean bout durationwas associatedwithmaternal alcoholpatterns. Fig. 2a shows that using the medium split measurefor pre-pregnancy binge (AA/occasion), high maternal use was

Table 3 Matrix of significant correlations ofmother and babyscales sub-domain scores and maternal alcohol measures
Alertness Unsettled/irregular
AA/Binge −0.57⁎⁎ 0.50⁎AA/DD 0.47⁎Frequency of binge −0.76⁎⁎
⁎pb0.05, ⁎⁎pb0.01; binge=N5 drinks per occasion; AA=absolutealcohol; DD=drinking day. All alcohol measures are based on pre-pregnancy estimates from 21 participants.
583Infant sleep and prenatal alcohol exposure
associated with significantly shorter spontaneous movementbout duration (6 s epochs: t(9)=−2.5, pb0.037; r=−0.611,pb0.046). Similarly, in Fig. 2b, groups determined by currentAA/DD revealed that the high alcohol group had significantlyshorter movement bout duration (60 s epochs: t(8)=−2.5,pb0.036; r=−0.61, pb0.037).
In the final temporal pattern analysis of the actigraphydata reflecting sleep fragmentation through movementintrusion, quiescence bouts were determined based onsustained activity below the average. Quiescence duration(60 s epochs) was shorter with either TWEAK or T-ACE mediansplit estimates of maternal alcohol use (Mann–WhitneyU=2.5, pb0.03).
3.4.2.1. Post-hoc correlational analyses. The small samplesize precluded a more complex analysis of variance for otherfactors. However, we did examine maternal tobacco use inrelation to sleep and movement parameters. Daily estimatesof number of cigarettes was positively associated with aver-age drowse state duration (r=0.65, p=0.02), but not withother sleep or movement parameter. Feeding mode wasexamined using a conversion of the breastfeeding para-meters as follows: 3=full time breast feeding; 2=breast andbottle and 3=bottle only. No significant correlations withsleep or movements were found. Only one mother wasexclusively breastfeeding in the high alcohol use group.
3.4.3. Mother and baby scalesTable 3 shows the correlation between maternal alcoholestimates and infant behavior as rated by the mother. TheInfant Alertness subscale of the MABS correlated negativelywith pre-pregnancy AA/Binge (r=−.57, p≤0.01); and fre-quency of binge prior to the knowledge of pregnancy (r=−0.76, pb0.01). Both pre-pregnancy AA/DD (r=0.47,p≤0.05) and AA/binge (r=0.50, p≤0.05) were significantlycorrelated with the subscale Infant Unsettled–Irregular,which is an indicator of infant fussiness and irritability.
4. Discussion
Our results confirm and extend the few earlier reports thatinfant sleep regulatory mechanisms are significantly dis-rupted by prenatal alcohol exposure [14,16]; are consistentwith recent findings for acute alcohol effects in infants in alaboratory sleep study [18]; and for infants of substanceabusing women in the first year [52]. In the present study, wefound that prenatal alcohol exposure resulted in brief sleepepisodes that were interrupted after sleep onset by wakeful-ness, as well as important reductions in the duration of (non-
wake) sleep-related spontaneous movements. State regula-tion, age-appropriate state stability and smooth transitionsbetween states in early infancy are indices of the integrity ofthe developing central nervous system [53–56].
Our estimates of prenatal alcohol exposure were based onstandard clinical interview methods. Self-reported maternalalcohol use was assessed for a typical week and during bingedrinking occasions. Estimates of “current” drinking werebased on the late pregnancy period, and retrospectiveestimates were based on the time immediately prior toknowledge of pregnancy. As has been found previously[37,57], maternal retrospective, pre-pregnancy estimatesof alcohol consumption were generally greater than self-reported alcohol consumption during pregnancy.
Maternal alcohol use estimates predicted sleep fragmen-tation. In adults, sleep fragmentation is characterized byfrequent arousals after sleep onset which leads to sleepdeprivation reflected in impaired arousal threshold tohypoxic conditions [58]. Infants respond similarly [59], andcoupled with the immaturity of the hypoxic ventilatoryresponse [60], risk of failure to arouse may increase inthe presence of chronic sleep deprivation. We found thatmaternal reports of high alcohol use prior to and duringpregnancy, as well as based on alcohol use history (MAST),were associated with increased frequency and duration ofwake events, proportion of wake time, and concomitantreduction of AS. Consistent with developing sleep debt, AA/DD and binge measures were correlated with MABS mater-nal reports of decreased infant alertness and increasedirritability.
A second finding was that the typical profile of infantsleep-related spontaneous movement was suppressed in thepresence of prenatal alcohol exposure. In the present studysleep-related spontaneous movements were less vigorous,i.e. showed reductions in duration but not frequency. Wepropose that sleep-related movements may be part of aprimitive arousal response that is protective of cardior-espiratory function by upregulation stimulated by sponta-neous movements; a coupling that is mature by the thirdtrimester [32,61,62]. This system may overlap with, buthave unique features from, subcortical arousals [63], andbecome impaired by chronic sleep deprivation. Kahn andcolleagues have reported that short-term and long-termsleep deprivation in infants is associated with reduction inbody movements, increases in obstructive sleep apnea anda higher arousal threshold to sound [35,64]. Reduced bodymovements and reduced arousals have been reportedprospectively for SIDS infants [65,66]. Infants who latersuccumbed to SIDS were found to have fewer subcorticalarousals and less spontaneous movements without corticalactivation during REM sleep in the later part (0100–0500 AM)of the nocturnal sleep epoch, a particularly vulnerable periodfor SIDS death in the circadian day [67].
For alcohol-exposed infants, risk may be compounded byconditions in the postnatal environment, e.g. cosleeping,continued substance use, a chaotic home environment, poorcare, etc. and may further compromise alcohol-exposedinfants who may have premorbid brainstem respiratory andautonomic dysfunction. Importantly, tobacco was present in54% of the sample, and was associated with increased drowsestate during the nap, reminiscent of infant reductions inalertness on the MABS in association with higher alcohol use.
584 M. Troese et al.
Mennella and colleagues [68] have found a reduction in sleepduration in breastfed infants immediately following mater-nal tobacco smoking. Although most of the mothers in ourstudy were not breastfeeding, mothers from both high andlow groups had co-morbidity between alcohol and tobaccoconsumption. Passive tobacco exposure could account forsome of our observations.
In conclusion, our results are consistent with our recentfindings in apneic premature infants [69], in that both ofthese samples exhibited sleep fragmentation, accumulationof sleep debt and suppression of spontaneous movementvigor. Future work will continue to examine the role ofspontaneous movements in the maintenance of cardiore-spiratory integrity during sleep in alcohol exposed and otherhigh SIDS risk infant samples.
Acknowledgment
This work was supported by the U.S. Department of Healthand Human Services (DIA RH 00004-01-03).
References
[1] Abel EL. Fetal alcohol syndrome: the ‘American Paradox’. Alcohol1998;33:195–201.
[2] Jones KL, Smith DW. The fetal alcohol syndrome. Teratology1975;12:1–10.
[3] Streissguth AP, Landesman-Dwyer S, Martin JC, Smith DW.Teratogenic effects of alcohol in humans and laboratoryanimals. Science 1980;209:353–61.
[4] Huizink AC, Mulder EJ. Maternal smoking, drinking or cannabisuse during pregnancy and neurobehavioral and cognitive func-tioning in human offspring. Neurosci Biobehav Rev 1998;30(1):24–41.
[5] Cahalan D, Cisin IH, Crossley HM. American drinking practices: anational study of drinking behavior and attitudes (MonographNo. 6). New Brunswick, NJ: Rutgers Center of Alcohol Studies;1969.
[6] Hayes MJ, Parker KG, Sallinen B, Davare AA. Bedsharing,temperament, and sleep disturbance in early childhood. Sleep2001;15:657–62.
[7] Jacobson SW, Jacobson JL, Sokol RJ, Martier SS, Ager JW.Prenatal alcohol exposure and information processing ability.Child Dev 1993;64:706–1721.
[8] Jacobson SW, Jacobson JL, Sokol RJ. Effects of fetal alcoholexposure on infant reaction time. Alcohol Clin Exp Res 1994;18:1125–32.
[9] Ikonomidou C, Bittigau P, Ishimaru MJ, Wozniak DF, Koch C,Genz K, et al. Ethanol-induced apoptotic neurodegenerationand fetal alcohol syndrome. Science 2000;287:1056–60.
[10] Jacobson JL, Jacobson SW, Sokol RJ, Ager JW. Relation ofmaternal age and pattern of pregnancy drinking to functionallysignificant cognitive deficit in infancy. Alcohol Clin Exp Res1998;22:345–51.
[11] Streissguth AP, Sampson PD, Barr HM. Neurobehavioral dose–response effects of prenatal alcohol exposure in humans frominfancy to adulthood. Ann N Y Acad Sci 1989;562:145–58.
[12] Vitiello MV. Sleep, alcohol, and alcohol abuse. Addict Biol1997;2:151–8.
[13] Farnell YZ, West JR, Chen WJ, Allen GC, Earnest DJ. Devel-opmental alcohol exposure alters light-induced phase shifts ofthe circadian activity rhythm in rats. Alcohol Clin Exper Res2004;28:1020–7.
[14] Rosett HL, Snyder P, Sander LW, Lee A, Cook P, Weiner L, et al.Effects of maternal drinking on neonate state regulation. DevMed Child Neurol 1979;21:464–73.
[15] Scher MS, Richardson GA, Coble PA, Day NL, Stoffer DS. Theeffects of prenatal alcohol andmarijuana exposure: disturbancesin neonatal sleep cycling and arousal. Pediatr Res 1988;24:101–5.
[16] Scher MS, Richardson GA, Day NL. Effects of prenatal cocaine/crack and other drug exposure on electroencephalographicsleep studies at birth and one year. Pediatr 2000;105:39–48.
[17] Mulder EJ, Morssink LP, van der Schee T, Visser GH. Acutematernal alcohol consumption disrupts behavioral state orga-nization in the near-term fetus. Pediatr Res 1998;44:774–9.
[18] Menella JA, Garcia-Gomez. Sleep disturbances after acuteexposure to alcohol in mothers' milk. Alcohol 2001;25:153–8.
[19] Malloy MH, Hoffman HJ. Prematurity, sudden infant deathsyndrome, and age of death. Pediatrics 1995;96:464–71.
[20] Schectman VL, Harper RM, Wilson AJ, Southall DP. Sleep apneain infants who succumb to the sudden infant death syndrome.Pediatrics 1991;87:841–6.
[21] Mitchell EA, Ford RPK, Stewart AW, Becroft DMO, ThompsonJMD, Scragg R, et al. Smoking and sudden infant deathsyndrome. Pediatrics 1993;91(5):893–6.
[22] Scragg R, Mitchell EA, Taylor BJ, Stewart AW, Ford RP,Thompson JM, et al. Bed sharing, smoking, and alcohol in thesudden infant death syndrome. New Zealand cot death studygroup. BMJ 1993;307:1312–8.
[23] Kinney HC, Randall LL, Sleeper LA, Willinger M, Belliveau RA, ZecN, et al. Serotonergic brainstem abnormalities in Northern PlainsIndians with the sudden infant death syndrome. J NeuropatholExp Neurol 2003;62:1178–91.
[24] Paterson DS, Trachtenberg FL, Thompson EG, Belliveau RA,Beggs AH, Darnall R, et al. Multiple serotonergic brainstemabnormalities in sudden infant death syndrome. J AmMed Assoc2006;296:2124–32.
[25] Hayes MJ, Kumar SP, Delivoria-Papdopoulos M. Spontaneousmotility in premature infants: features of behavioral activityand rhythmic organization. Dev Psychobiol 1993;26:279–91.
[26] Hayes MJ, Mitchell D. Spontaneous movements during sleep inchildren: temporal organization and changes with age. DevPsychobiol 1998;32:13–21.
[27] Robertson SS. Intrinsic temporal patterning in the spontaneousmovement of awake neonates. Child Dev 1982;53:1016–21.
[28] Roberston SS. Human cyclic motility: fetal-newborn continuitiesand newborn state differences. Dev Psychobiol 1987;20:425–42.
[29] Harper RM, Kinney HC, Fleming PJ, Thach BT. Sleep influenceson hemeostatic functions: implications for sudden infant deathsyndrome. Respir Physiol 2000;119:123–32.
[30] Thach BT, Lijowska A. Arousals in infants. Sleep 1996;19:271–3.[31] Wulbrand H, McNamara F, Thach BT. Arousal related self
resuscitating reflexes, sighs and startles during airway occlu-sion in infants. Neuropediatrics 2005;36:V25.
[32] Potts JT, Rybak IA, Paton JFR. Respiratory rhythm entrainmentby somatic afferent stimulation. J Neurosci 2005;25:1965–78.
[33] Alm B, Wnnergren G, Norvenius G, Skjaerven R, Oyen N,Helweg-Larsen K, et al. Caffeine and alcohol as risk factors forsudden infant death syndrome. Arch Dis Child 1999;81:107–11.
[34] Chang AB, Wilson SJ, Masters IB, Yuill M, Williams J, Williams G,et al. Altered arousal response in infants exposed to cigarettesmoke. Arch Dis Child 2003;88:30–3.
[35] Franco P, Chabanski S, Szliwowski H, Dramaix M, Kahn A.Influence of maternal smoking on autonomic nervous system inhealthy infants. Pediatr Res 2000;47:215–20.
[36] Iyasu S, Randall LL, Welty TK, Hsia J, Kinney HC. Risk factors forsudden infant death syndrome among Northern Plains Indians.Am Med Assoc 2002;289:303.
[37] Hayes MJ, Brown E, Hofmaster PA, Davare AA, Parker KG,Raczek JA. Prenatal alcohol intake in a rural, Caucasian clinic.Fam Med 2002;34:120–5.
585Infant sleep and prenatal alcohol exposure
[38] Dunn LM, Dunn LM. Examiner's manual for the Peabody PictureVocabulary Test. 3rd ed.Circle Pines: AmericanGuidance Service;1997.
[39] Hollingshead AB. The four-factor index of social status. YaleUniversity, New Haven. (manuscript) in press.
[40] Cahalan D, Cisin IH, Crossley HM. American drinking practices: anational study of drinking behavior and attitudes (MonographNo. 6). New Brunswick, NJ: Rutgers Center of Alcohol Studies;1969.
[41] Selzer ML. The Michigan alcoholism screening test: the quest fora new diagnostic instrument. Am J Psychiatry 1971;127:1653–8.
[42] Sokol RJ, Martier SS, Ager JW. The T-ACE questions: practicalprenatal detection of risk-drinking. Am J Obstet Gynecol1989;160:863–70.
[43] RussellM.Newassessment tools for riskdrinkingduringpregnancy:T-ACE, TWEAK, and others. Alcohol Health Res World 1994;18:55–61.
[44] Chan AW, Pristach EA, Welte JW, Russell M. Use of the TWEAKtest in screening for alcoholism/heavy drinking in threepopulations. Alcohol Clin Exp Res 1993;17:1188–92.
[45] Beck AT, Steer RA, Brown GK. Beck Depression Inventory manual.2nd ed. San Antonio: The Psychological Corporation; 1996.
[46] Wolke D, St James-Roberts I. Multi-method measurement ofthe early parent–infant system with easy and difficult new-borns. In: Rauh H, Steinhausen HC, editors. Psychobiology andearly development. Amsterdam: North-Holland/Elsevier; 1987.p. 49–70.
[47] Thoman EB, Holditch-Davis D, Ray JR, Phillips AF, Rowe JC,Denenberg VH. Theophylline affects sleep-wake state devel-opment in premature infants. Neuropediatrics 1985;16:13–8.
[48] Anders T, Emde R, Parmelee A. A manual of standardizedterminology, techniques, and criteria for scoring of states ofsleep and wakefulness in newborn infants. Los Angeles: UCLABrain Information Service; 1971.
[49] Carskadon MA, Dement WC, Mitler MM, Roth T, Westbrook PR,Keenan S. Guidelines for the multiple sleep latency test (MSLT):a standard measure of sleepiness. Sleep 1986;9:519–24.
[50] Curzi-Dascalova I, Peirano P, Silvestri I, Korn G. Sleep organiza-tion in normal premature newborn infants. Polygraphic study.Rev Electroencephalogr Neurophysiol Clin 1985;15:237–42.
[51] Selzer ML, Vinokur A, Rooijen L. A self-administered ShortMichigan Alcoholism Screening Test (SMAST). J Stud Alcohol1975;36:117–26.
[52] Hanft A, Burnham M, Goodlin-Jones B, Anders TF. Sleeparchitecture in infants of substance abusing mothers. InfantMent Health J 2006;27:141–51.
[53] Ficca G, Fagioli P, Salzarulo P. Sleep organization in the firstyear of life: developmental trends in quiet sleep-paradoxicalsleep cycle. J Sleep Res 2000;9:1–4.
[54] Scher MS. A developmental marker of central nervous systemmaturation: Part I. Pediatr Neurol 1988;4:265–73.
[55] Scher MS. A developmental marker of central nervous systemmaturation: Part II. Pediatr Neurol 1988;4:329–36.
[56] Thoman EB. Sleeping and waking states in infants: a functionalperspective. Neurosci Biobehav Rev 1990;14:93–107.
[57] Jacobson SW, Jacobson JL, Sokol RJ, Martier SS, Ager JW,Kaplan MG. Maternal recall of alcohol, cocaine, and marijuanause during pregnancy. Neurotoxicol Teratol 1991;13:535–40.
[58] Chugh DK, Weaver TE, Dinges DF. Neurobehavioral conse-quences of arousals. Sleep 1996;19:S198–201.
[59] Franco P, Seret N, Van Hees JN, Scaillet S, Vermeulen F,Groswasser J, et al. Decreased arousals among healthy infantsafter short-term sleep deprivation. Pediatrics 2004;114: 192–7.
[60] Gaultier C. Cardiorespiratory adaptation during sleep in infantsand children. Pediatr Pulmonol 1995;19:105–17.
[61] Hayes MJ. Methodological issues in the study of arousal andawakening in infants. In: Salzarulo P, Ficca G, editors. Awakeningand sleep–wake cycle across development. Advances in Con-sciousness Research. New York: Elsevier; 2002. p. 23–45.
[62] DiPietro JA, Irizarry RA, Hawkins M, Constigan KA, Pressman EK.Cross-correlation of fetal cardiac and somatic activity as anindicator of antinatal neural development. Am J ObstetGynecol 2001;25:1421–8.
[63] McNamara F, Wulbrand H, Thach BT. Characteristics of theinfant arousal response. J Appl Physiol 1998;85:2314–21.
[64] Kato I, Scaillet S, Groswasser J, Montemitro E, Togari H, Lin JS,et al. Spontaneous arousability in prone and supine position inhealthy infants. Sleep 2006;29:785–90.
[65] Schectman VL, Harper RM, Wilson AJ, Southall DP. Sleep stateorganization in normal infants and victims of the sudden infantdeath syndrome. Pediatrics 1992;89(5):865–70.
[66] Kahn A, Groswasser J, Rebuffat E, Sottiaux M, Blum D, FoersterM. Sleep and cardiorespiratory characteristics of infant victimsof sudden death: a prospective case-control study. Sleep1992;15:287–92.
[67] Kato I, Franco P, Groswasser J, Scaillet S, Kelmanson I, Togari H,et al. Incomplete arousal processes in infants who were victimsof sudden death. Am J Respir Crit Care Med 2003;168: 1298–303.
[68] Mennella JA, Yourshaw LM, Morgan LK. Breastfeeding andsmoking: short-term effects on infant feeding and sleep.Pediatrics 2007;120:497–502.
[69] Hayes MJ, Akilesh MR, Fukumizu M, Gilles AA, Sallinen BJ,Troese M. Apneic preterms and methylxanthines: arousaldeficits, sleep fragmentation and suppressed spontaneousmovements. J Perinatol 2007;27:782–9.