Embed Size (px)
Citation preview

Sleep in Herniorrhaphy Patients
Neil 8. Kavey, MD,* New York, New York Kenneth Z. Altshuler, MD,t Dallas, Texas
This report is the first in a series of studies aimed at defining the effects of surgical trauma on sleep and the bearing these effects may have on patients’ re- covery or deterioration.
The last two decades have witnessed a burgeoning interest in sleep research, and the traditional notion of sleep as a quiet state devoid of stress has been re- placed by a more comprehensive understanding of it as a complex, physiologically active state with changes that may even be potentially stressful. The flow from one stage to another that typifies a night of sleep in normal adults is illustrated in Figure 1. Stage I is a period of drowsiness rather than true sleep. Stages II, III, and IV are associated with a progressive deepening of sleep and a lowering of au- tonomic activity such as heart rate, respiratory rate, and blood pressure. Stage II occurs intermittently throughout the night, while stages III and IV (also called delta or slow-wave sleep) normally occur largely within the first 3 or 4 hours of sleep. Rapid eye movement (REM) sleep is the stage during which visual dreaming occurs. In contrast to stages II, III, and IV (non-REM sleep), REM sleep is characterized by autonomic excitement, physiologically similar to active wakefulness. Heart rate, cardiac output, res- piratory rate, and blood pressure are highly variable and can undergo dramatic changes within seconds or minutes, making REM sleep potentially stressful as well as restful.
Other physiologic phenomena associated with the various stages of sleep may also be significant.
From the Department of Clinical Psychiatry, College of Physicians and Surgeons of Columbia University and the Presbyterian Hospital.’ New York, New York; and the Department of Psychiatry, University of Texas, South- western Medical School, the Presbyterian Hospital, and the Children’s Medical Center.’ Dallas, Texas. This research was supported by Grants GM 22515 and RR 00645 from the National Institutes of Health, Bethesda, Maryland.
Reprint requests should be addressed to Neil B. Kavey, MD, Department of Psychiatry, College of Physicians 8 Surgeons of Columbia University, 722 West 168th Street, New York, New York 10032.
Growth hormone, for example, is normally secreted in nocturnal bursts soon after the onset of sleep when stages III and IV appear [I]. The lowered metabolic rate of stages III and IV further favors anabolic processes [2,3]. Taken together, these findings suggest that tissue healing may be accelerated during the deeper stages of sleep. At the same time, medi- cations in common use affect sleep selectively, some blocking REM sleep (barbiturates, alcohol, and morphine) and some blocking stages III and IV (barbiturates, alcohol, and the benzodiazepines). Withdrawal of an REM blocking agent may be as- sociated with “REM rebound,” an increase to above normal amounts of REM sleep, and exacerbations of autonomic activity that may carry with them an unpleasant subjective experience. Rebounds of stages III and IV are also common, though not uncomfort- able; indeed, when such stages are lost, they may be made up even before REM sleep. Nowlin et al [4] and others [5,6] have suggested that REM sleep, with its rapid cardiovascular alterations, is a time of in- creased risk for angina or coronary ischemic changes in patients with coronary impairment.
Johns et al [7] and Orr and Stahl [8], studying the effect of surgery on sleep, found minor alterations in the preoperative sleep of patients scheduled for open heart surgery and severe disruptions of their sleep postoperatively. Stages III, IV, and REM were markedly reduced or absent for at least 2 to 4 days, and the time awake was increased; normal sleep gradually returned. The work with noncardiac sur- gical patients is sparse. Johns et al [7] noted post- operative REM suppression in a patient who un- derwent a colectomy; however, the patient’s alco- holism complicated the results. Ellis and Dudley [9], studying a mixed group of 12 herniorrhaphy, gas- trectomy, and vagotomy patients for varying lengths of time, cited three main changes in postoperative sleep: reduced slow-wave sleep, reduced REM sleep,
682 The American Journal of Surgery
Sleep in Herniorrhaphy Patients
TABLE I Mean Sleep Parameters by Day of Hospitalization
Age-Matched
Normal Patients Mean SD
Preop Mean SD
Postop Postop Postop Day 1 Day 2 Day 3
Mean SD Mean SD Mean SD
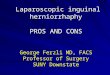
Total sleep time (min) 404.8 21.7 367.6 78.9 383.2 25.7 320.0 83.2 374.7 47.5 Sleep period time (min) 423.1 13.4 405.5 48.8 429.3 73.4 412.1 43.0 419.9 41.2 No. of awakenings 3.9 1.1 4.9 3.2 12.5 6.6 9.6 5.0 8.5 5.8 Sleep period time (%)
Stages awake and I 11.1 3.6 23.1 15.3 41.8 14.5 41.7 23.5 27.3 16.8 Stage REM 23.0 0.4 20.4 5.6 4.2 6.1 12.0 9.7 20.0 11.3 Stage II 54.9 2.3 42.3 13.7 52.7 13.1 39.1 13.0 43.2 10.5 Stages III and IV 11.1 4.6 13.3 11.3 1.2 3.5 6.6 9.5 8.6 9.0
Preop = preoperative; Postop = postoperative; SD = standard deviation.
and loss of sleep’s inherent rhythmicity. Febrile states may contribute to these alterations [IO]. We are studying more comprehensively the impact of surgery and its associated phenomena on sleep by tracing sleep throughout the entire hospital stay and comparing sleep disruptions in patients grouped according to level of surgical trauma. Herniorrhaphy, cholecystectomy, gastrectomy, and total hip re- placement patients and patients so severely trau- matized as to require special surgical intensive care are being studied. The aim is to provide information of clinical importance to physicians about the quantity, quality, and significance of sleep in the postoperative course of illness. The focus of this paper is the sleep of herniorrhaphy patients.
AWAKE
I
REM
STAGE I
STAGE GP STAGE2
SLEEP
STAGE 3
STAGE 4
I I 2 3 4 5 6 7
HOURS OF SLEEP
Figure 1. Normal pattern and stages of nighttime sleep.
Material and Methods
Ten male patients aged 17 to 49 years with hernias but no complicating illness were admitted to a typical new single-bedded hospital room and studied in their rooms from the day of admission, 1 or 2 nights preoperatively, to discharge 4 or 5 days after herniorrhaphy.
Six patients received general anesthesia (short-acting agents with rapid washouts), and the other four, spinal anesthesia. Meperidine (Demerol”), with dose and route of administration determined by the individual physician, was dispensed every 3 to 4 hours if requested by the pa- tient. No patient received hypnotics during the course of the study.
Continuous polygraphic recordings [I 1) including elec- troencephalograms (EEG), electrooculograms (EOG), electromyograms (EMG), respiratory rate recordings, and electrocardiograms (EKG) monitored the patients from the time they felt ready to go to sleep (about 11:00 P.M.) until morning awakening (6:30 to 7:OO A.M.). In addition, daytime sleep studies were conducted the afternoon after surgery in four patients. The polygraph and the technician were located outside the subject’s room and a log was maintained detailing the events of the study period. Re- cordings were scored and results formulated for the fol- lowing parameters: total sleep time (TST), total minutes asleep in the night; awake time (A), the time awake after initial sleep onset; sleep period time (SPT), the minutes from initial sleep onset to final morning awakening (TST plus A); stages I, II, III, IV, and REM, the length of time spent in each measured both in minutes and as a per cent of SPT; and sleep rhythmicity, the sequential flow from stage to stage visually evaluated from an analogue printout.
Each morning patients were interviewed and a ques- tionnaire was completed to evaluate the subjective aspects of the night. As part of the questionnaire, subjects rated the overall quality of their sleep on a scale of 1 to 5 (1 = very poor, 5 = excellent). In addition, the authors devised a quality-of-sleep scale to objectify the quality of a patient’s night of sleep with a numerical index comparing the pro- portions of stages in a given night of sleep with those in a normal population.*
Results are presented in terms of total sleep time, sleep rhythmicity, and the percentage of sleep period time spent awake or in the specific sleep stages. Since sleep time gradually increases after the first 2 postoperative nights,
l The quality-of-sleep scale is calculated as follows: 3 X number of minutes in stage IV + 2 X number of minutes in stage Ill i- 0.5 X number of minutes in stage II + 1 X number of minutes in stage REM. The scale at- tributes particular importance to the amount of time spent in stages Ill. IV. and REM so that changas in these stages will be clearly reflected. In a normal population the scale yields tha following values: ages 16 to 19 = 502.9: 20 to 29 = 453.8: 30 to 39 = 358.6: and 40 to 49 = 293.4. Notable deviations suggest a departure from normal values but do not specify which stages are disrupted.
Volume 138, November 1979 683
Kavey and Altshuler
50(
40(
MINUTES OF
SLEEP
30(
2oc
PT 1 \
PT 2
PT 3
I I 2 3 4
‘db’ PET ‘ET 7;’ ‘$6
DAY OF HOSPITALIZATION
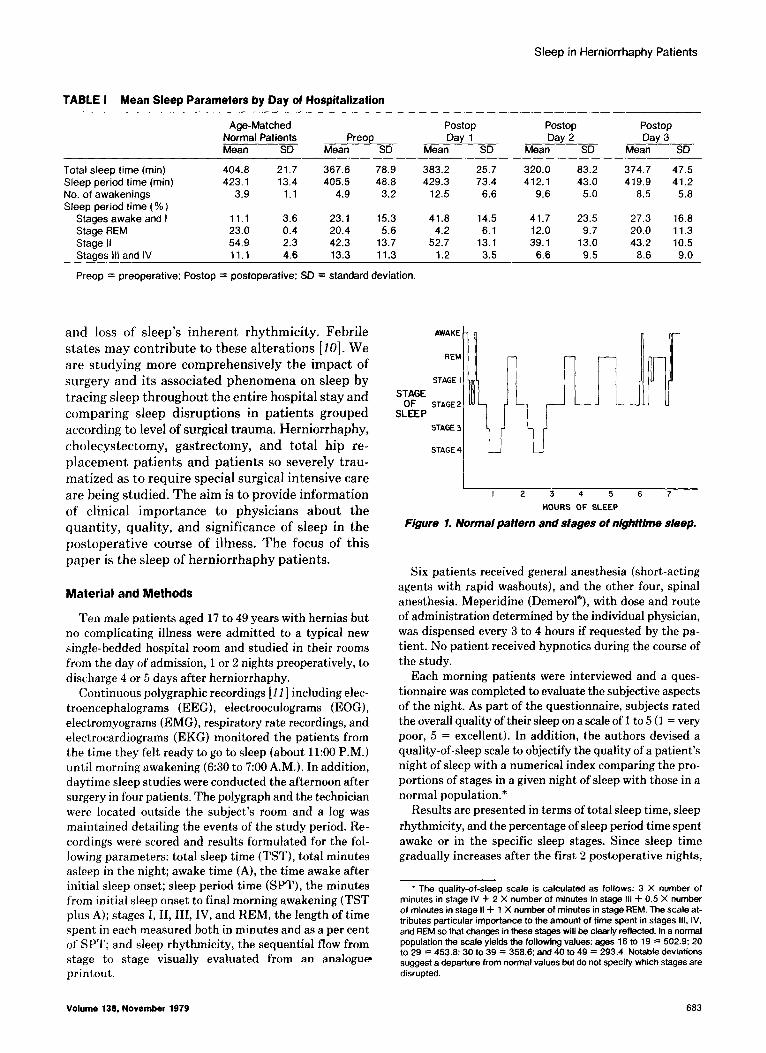
Figure 2. Total sleep time on pre- and postoperative nights for three patients.
percentage of sleep period time can be used as a near ac- curate reflection of changes in real time (minutes) in each stage. Awake time and stage I are combined as awake- drowsy time and stages III and IV as delta or deep sleep. The data were subjected to the F test for analysis of the significance of trends.
Results
Table I shows the sleep parameter means for all subjects by day of hospitalization.
Total Sleep Time (TST). Preoperative TST for the patient group averaged 6 hours and 8 minutes, 37 minutes less than the expected mean for men of the same age distribution [12]. Individual variation was considerable. Six patients acquired a below average sleep time, ranging from 3 hours and 35 minutes to 5 hours and 49 minutes, and four patients reached above average levels ranging from 6 hours and 41 minutes to 7 hours and 51 minutes. More noteworthy, however, is the fact that even the patients with low- ered sleep time retained a normal pattern of sleep stages, with deep sleep early in the night and REM sleep more concentrated toward morning. Mean percentages of TST spent in the various stages were all within normal range: stage II, 42.3 per cent; stages III and IV, 13.3 per cent; and stage REM, 20.4 per cent.
Postoperative TST was markedly decreased in all patients on at least 1 of the first 2 postoperative nights. It then gradually returned toward normal levels. Figure 2 illustrates the course of TST in three patients typifying these results and demonstrating their variability.
While TST measures the quantity of sleep, it does not reveal the quality of sleep or the number, relative duration, or sequence of the various stages or time
. . . ..YC
STAGE ( ! STAGE 2
STAGE 3
STAGE 4
AWAKE
REM
SfAGE STAGE I
s ;LEp STAGE 2
STAGE 3
STAGE 4
l-
AWAKE
REM
STAGE I
STAGE 2
STAGE 3
STAGE 4 LJ C: POST-OPERATIVE NIGHT 3
I I 2 3 4 5 6 7
HOURS OF SLEEP
A: POST-OPERATIVE NIGHT 1
B: POST-OPERATIVE NIGHT 2
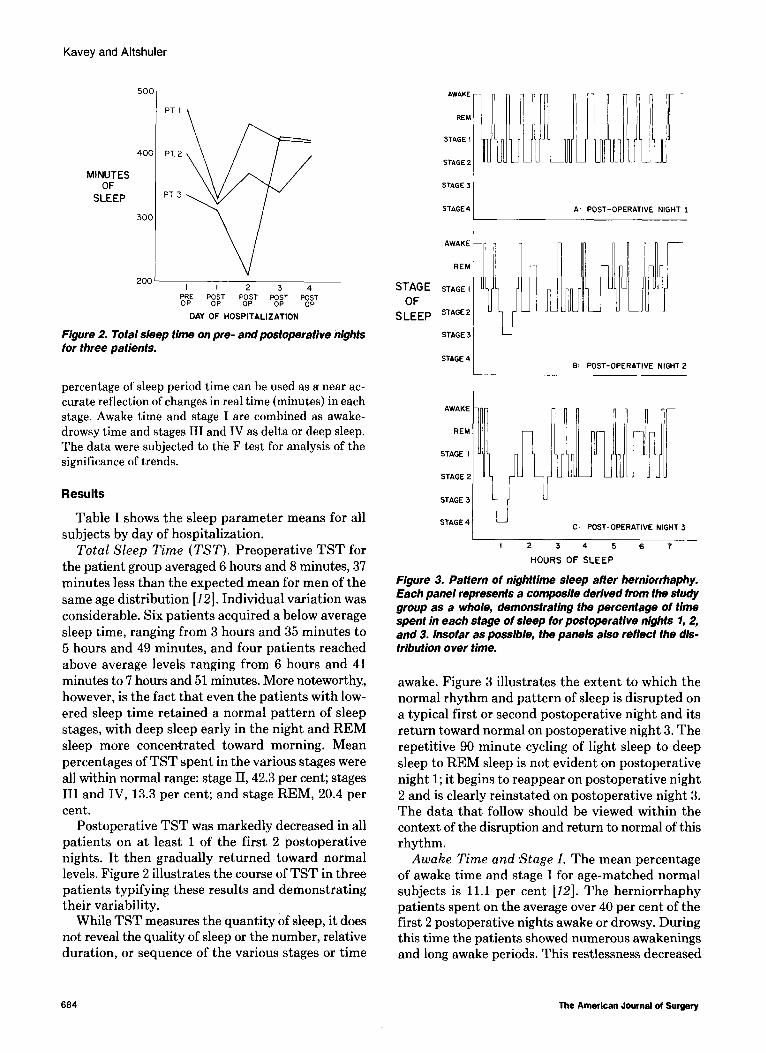
Figure 3. Pattern of nighttime sleep after herniorrhaphy. Each panel represents a composite derived from the study group as a whole, demonstrattng the percentage of time spent in each stage of sleep for postoperative nights 1,2, and 3. Insofar as possible, the panels also reflect the dis- tribution over time.
awake. Figure 3 illustrates the extent to which the normal rhythm and pattern of sleep is disrupted on a typical first or second postoperative night and its return toward normal on postoperative night 3. The repetitive 90 minute cycling of light sleep to deep sleep to REM sleep is not evident on postoperative night 1; it begins to reappear on postoperative night 2 and is clearly reinstated on postoperative night 3. The data that follow should be viewed within the context of the disruption and return to normal of this rhythm.
Awake Time and *Stage I. The mean percentage of awake time and stage I for age-matched normal subjects is 11.1 per cent [12]. The herniorrhaphy patients spent on the average over 40 per cent of the first 2 postoperative nights awake or drowsy. During this time the patients showed numerous awakenings and long awake periods. This restlessness decreased
664 The American Journal of Surgery
Sleep in Herniorrhaphy Patients
linearly over the postoperative nights (p <O.Ol) but was, even on postoperative night 4, twice as great (22.7 per cent) as would be expected in nonsurgical, age-matched normal subjects.
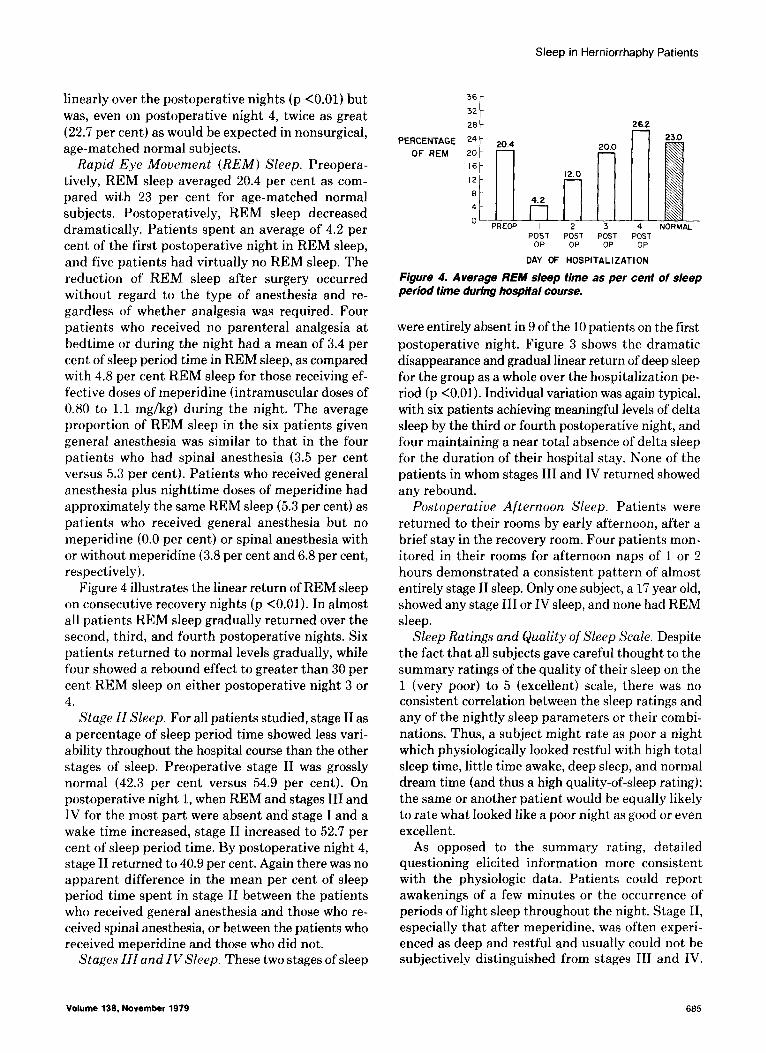
Rapid Eye Movement (REM) Sleep. Preopera- tively, REM sleep averaged 20.4 per cent as com- pared with 23 per cent for age-matched normal subjects. Postoperatively, REM sleep decreased dramatically. Patients spent an average of 4.2 per cent of the first postoperative night in REM sleep, and five patients had virtually no REM sleep. The reduction of REM sleep after surgery occurred without regard to the type of anesthesia and re- gardless of whether analgesia was required. Four patients who received no parenteral analgesia at bedtime or during the night had a mean of 3.4 per cent of sleep period time in REM sleep, as compared with 4.8 per cent REM sleep for those receiving ef- fective doses of meperidine (intramuscular doses of 0.80 to 1.1 mg/kg) during the night. The average proportion of REM sleep in the six patients given general anesthesia was similar to that in the four patients who had spinal anesthesia (3.5 per cent versus 5.3 per cent). Patients who received general anesthesia plus nighttime doses of meperidine had approximately the same REM sleep (5.3 per cent) as patients who received general anesthesia but no meperidine (0.0 per cent) or spinal anesthesia with or without meperidine (3.8 per cent and 6.8 per cent, respectively).
Figure 4 illustrates the linear return of REM sleep on consecutive recovery nights (p <O.Ol). In almost all patients REM sleep gradually returned over the second, third, and fourth postoperative nights. Six patients returned to normal levels gradually, while four showed a rebound effect to greater than 30 per cent REM sleep on either postoperative night 3 or 4.
Stage II Sleep. For all patients studied, stage II as a percentage of sleep period time showed less vari- ability throughout the hospital course than the other stages of sleep. Preoperative stage II was grossly normal (42.3 per cent versus 54.9 per cent). On postoperative night 1, when REM and stages III and IV for the most part were absent and stage I and a wake time increased, stage II increased to 52.7 per cent of sleep period time. By postoperative night 4, stage II returned to 40.9 per cent. Again there was no apparent difference in the mean per cent of sleep period time spent in stage II between the patients who received general anesthesia and those who re- ceived spinal anesthesia, or between the patients who received meperidine and those who did not.
Stages III and IV Sleep. These two stages of sleep
Volume 139, November 1979
36
32
28
PERCENTAGE 24 1
20.4
OF REM 20
‘6t 12 8 4
0 -n,
4.2
PRECP I
20.0
d 12.0 l-l
2 3 4
26 .2
i
23x)
NORMAL POST POST POST POST
OP OP OP OP
DAY Cf HOSPITALIZATION
Figure 4. Average REM sleep time as per cent of sleep period time during hospital course.
were entirely absent in 9 of the 10 patients on the first postoperative night. Figure 3 shows the dramatic disappearance and gradual linear return of deep sleep for the group as a whole over the hospitalization pe- riod (p <O.Ol). Individual variation was again typical, with six patients achieving meaningful levels of delta sleep by the third or fourth postoperative night, and four maintaining a near total absence of delta sleep for the duration of their hospital stay. None of the patients in whom stages III and IV returned showed any rebound.
Postoperative Afternoon Sleep. Patients were returned to their rooms by early afternoon, after a brief stay in the recovery room. Four patients mon- itored in their rooms for afternoon naps of 1 or 2 hours demonstrated a consistent pattern of almost entirely stage II sleep. Only one subject, a 17 year old, showed any stage III or IV sleep, and none had REM sleep.
Sleep Ratings and Quality of Sleep Scale. Despite the fact that all subjects gave careful thought to the summary ratings of the quality of their sleep on the 1 (very poor) to 5 (excellent) scale, there was no consistent correlation between the sleep ratings and any of the nightly sleep parameters or their combi- nations. Thus, a subject might rate as poor a night which physiologically looked restful with high total sleep time, little time awake, deep sleep, and normal dream time (and thus a high quality-of-sleep rating); the same or another patient would be equally likely to rate what looked like a poor night as good or even excellent.
As opposed to the summary rating, detailed questioning elicited information more consistent with the physiologic data. Patients could report awakenings of a few minutes or the occurrence of periods of light sleep throughout the night. Stage II, especially that after meperidine, was often experi- enced as deep and restful and usually could not be subjectively distinguished from stages III and IV.
665
Kavey and Altshuler
Since the quality of sleep scale was based on elec- troencephalographic criteria, it correlated with the patterns of sleep observed and reflected the linear progression toward better sleep.
Comments and Conclusions
The results demonstrate that even a relatively minor surgical procedure can cause major, although temporary, disruptions of nighttime sleep in other- wise healthy adults. While individual variations are wide-ranging, all patients showed major alterations in their postoperative sleep in comparison with their preoperative sleep or with sleep in normal, nonsur- gical subjects.
Preoperative sleep showed the relatively minor alterations one might expect to be caused by anxiety due to a new environment and concern about surgery and hospital procedures, including the sleep study: slightly decreased sleep time, more time awake, and slight reductions in REM time and deep sleep. Sur- prisingly, several subjects slept quite well the night before surgery. Immediate, postoperative afternoon naps are typically quiet stage II sleep. The freshness of the surgical trauma, morning medications, anes- thesia, and postoperative analgesia (meperidine) all contribute to the quality of this sleep.
the use of analgesia. Patients who had general anes- thesia and nighttime meperidine, general anesthesia and no meperidine during the night, or spinal anes- thesia with or without nighttime meperidine all had very little REM or stages III or IV. Although medi- cation used early in the day, or its metabolites, might be a contributing factor, the consistency of the findings strongly suggests that physical trauma and its correlates are the proximate causes. The absence of any rebound of delta sleep suggests that deep sleep lost after surgical trauma is done without and not recovered. Patients did take occasional daytime naps other than in the immediate postoperative hours, but these were not monitored. One would expect the factors suppressing nocturnal REM and delta sleep to be operant during the day and for naps to include these stages as recovery proceeds; it is unlikely that the naps significantly contributed to or caused the nocturnal aberrancies.
Postoperative sleep for the first night or two is characterized by restlessness, light sleep, and the almost complete absence of REM and delta sleep. The nights are spent going from awake to stage I to stage II, and back to stage I or awake. Pain, incisional or gas, and the nursing staff performing the necessary routine procedures are the major causes of awak- enings. Neither of these can be fully eliminated, but disruption of sleep might be reduced considerably if hospital personnel were able to take into account whether or not patients are sleeping when it is time for routine postoperative checks and procedures.
The six patients who received meperidine did not sleep differently, considering the night overall, from the four who did not. Yet meperidine might well have some effect on sleep. Three of the four patients showing an REM rebound had received the analgesia 1 or 2 nights before, perhaps indicating an REM suppressant effect of meperidine that is masked by the greater REM suppression of other features as- sociated with the surgery. Moreover, since relief of discomfort probably promotes sleep, it is likely that patients in pain require analgesia to get even the re- duced amount and disturbed quality of sleep that less uncomfortable patients obtain without analgesia.
The consequences of overall sleep loss and more specifically, the selective loss of certain stages of sleep, are uncertain. Metabolic rate is significantly lower in sleep than in wakeful rest and lower in slow wave sleep than in stage II [2]. Adam and Oswald [3] emphasized the importance for tissue restoration of this lowered metabolic state and presented evidence that degradative processes are stimulated during the awake state and restorative, synthetic processes are favored during sleep. Similarly, slow wave sleep, having the lowest metabolic rate, a high net protein synthesis, and being possibly accompanied by growth hormone secretion, may be a time of particular im- portance for wound healing. In addition, during REM sleep skeletal muscles are in the lowest tonic state of the day, and it is likely that then’ also net protein synthesis is high and healing maximized. Early con- clusions that prolonged selective REM deprivation led to serious emotional disturbance have been overturned. But REM sleep is probably a time of enhanced brain protein synthesis and possible psy- chologic integration of the day’s events, and its loss in a hospital setting could conceivably contribute to feelings of distress or depression. The presence of normal healing in the hernia patients (as grossly observed) and the absence of overt psychiatric problems suggest that in this group the synthetic processes promoted by waking rest and stage II sleep are sufficient. In cases of more extensive damage, the promotion of sleep and especially-if possible-the promotion of stages REM, III, and IV could possibly have a stabilizing effect on the psychologic state and an accelerating effect on wound healing.
The absence or low levels of REM and stages III It is noteworthy that the patients’ summary and IV on the first 2 postoperative nights are unre- stat,ements on the quality of a night’s sleep correlate lated to the type of anesthesia (general or spinal) or poorly with the electrophysiologic data as reflected
686 The American Journal of Surgery

Sleep in Herniorrhaphy Patients
DrOCeSSf?sS.
in the quality-of-sleep scale. A number of issues de-
crease the value of the subjective reports: although
stages III and IV are commonly considered periods of deep sleep because of their high arousal threshold,
patients commonly report deep sleep during a period that was stage II or REM; the stage II sleep after an
injection of meperidine was often experienced as
deep; and a patient’s selective recall of his most re-
cent sleep, the quality, timing, and causes of his awakenings, or even the type of mentation during
non-REM sleep might all contribute to a feeling of
sleep having been either restless or restful despite
contrary electrophysiologic evidence. In any event,
these data suggest that while asking how a patient slept is perhaps politic, it is unlikely to elicit a
meaningful answer unless followed by a more de-
tailed inquiry.
Since REM and stages III and IV are suppressed
by even minor surgical procedures, medical wisdom
would appear to dictate the avoidance, if possible, of
drugs that further interfere with these stages of sleep. More prolonged deprivation of REM sleep or en-
hanced REM rebound might interfere with psy-
chologic stability, and an enduring absence of REM
and deep sleep could conceivably delay healing. At
the same time one should consider that the promo-
tion of sleep, regardless of stage, will probably be
accompanied by an enhancement of net synthetic
Summary
The nocturnal sleep patterns of 10 elective her- niorrhaphy patients were documented by continuous,
8 hour polygraphic recordings from night 1 of hos- pitalization until discharge on day 4 or 5. Subjects
showed a dramatic loss of REM sleep and stages III
and IV and major increases in time awake and drowsy
for the first 2 postoperative nights, with a gradual
return toward normal sleep over the hospitalization
period. The significance for healing of the loss of
stages REM, III, and IV is discussed, especially with regard to hospital procedures and the use of medi- cat,ions. --__-__-
Acknowledgement: The authors express their gratitude to the surgeons of Presbyterian Hospital and the Columbia University College of Physicians and Surgeons who coop- erated in this interdisciplinary project. We also thank Dr. Alan C. Woodward, Ann Sellew, Louisa Peterson, and Angela Stio-McKenna for their assistance in the collection and analysis of the data.
References
1. Takahashi Y, Kipnis DM, Daughaday WH: Growth hormone secretion during sleep. J C/in Invest 47: 2079, 1968.
2. Brebbia DR. Altshuler KZ: Stage related patterns and nightly
sicians Lond 11: 376, 1977.
trends of energy exchange during sleep. Computers and Electronic Devices in Psychiatry (Kline NS, Laska E, eds). New York, Grune 8 Stratton, 1968, p 319.
3. Adam K, Oswald I: Sleep is for tissue restoration. J Co// Phy-
I----------
It is beyond the scope of this paper to attempt to
set guidelines for use of analgesics or hypnotics to
promote sleep in patients comparable to those
studied. The effects of these medications need fur-
ther evaluation in the actual clinical setting. At this
point sound clinical judgment should be used in
balancing their somewhat contradictory effects on subjects’ recovery from surgery. The medications
could interfere with the appearance of important
stages of sleep that have already been seriously
compromised by the physical trauma; yet overall,
they will encourage sleep in a patient population in
which that is a most desirable effect. Interference
with sleep for the performance of clock-bound hos-
pita1 procedures should certainly be minimized. Further studies will explore whether the aberrations
observed in the herniorrhaphy group will persist
longer or the sleep patterns show still greater dis- tortion after more severe general surgical proce-
4. Nowlin JB, Troyer WG Jr, Collins WS, Silverman G, Nichols CR, McIntosh HD, Estes EH Jr, Bogdonoff MD: The association of nocturnal angina pectoris with dreaming. Ann lntem Med 63: 1049, 1965.
5. Murao S, Harumi K, Katayana S, Machima S, Shimomura K, Murayama M, Matsuo H, Yamamoto H, Kato R, Chen C: All- night polygraphic studies of nocturnal angina pectoris. Jpn Hear-l J 13: 295, 1972.
6. Rosenblatt G, Zwilling G, Hartmann E: Electrocardiographic changes during sleep in patients with cardiac abnormalities. Psychophysiology 6: 233, 1969.
7. Johns MW, Laye AA, Masterton JP, Dudley HA: Sleep and de- lirium after open heart surgery. Br J Surg 61: 377, 1974.
8. Orr WC, Stahl ML; Sleep disturbance after open heart surgery. Am J Cardiol39: 196. 1977.
9. Ellis BW. Dudley HAF: Some aspects of sleep research in surgical stress. J Psychosom Res 20: 303, 1976.
10. Karacan I, Wolff SM, Williams RL, Hursch CJ, Webb WB: The effects of fever on sleep and dream patterns. Psychoso- matics 9: 331, 1968.
11. Rechtschaffen A, Kales A (ed): A Manual of Standardized Terminology, Techniques, and Scoring System for Sleep Stages of Human Subjects. NIH Publication No. 204, 1968.
12. Williams RL, Karacan I, Hursch CJ: Electroencephalography (EEG) of Human Sleep: Clinical Applications. New York, John
dures. Wiley & Sons, 1974.
Volume 139, November 1979 667