Embed Size (px)
Citation preview

Welcome Applicants!
Friday, January 16, 2015
Prep QuestionA 5-year-old boy is brought to the office 4 hours after falling off his bicycle. His mother reports that he was not wearing a helmet, and bystanders said that he did not lose consciousness. When his friends brought him home, he was tearful and sleepy but was answering questions appropriately. His mother noted an abrasion on the left side of his head and applied ice to a small area of swelling on the left temple. Over the last several hours, however, he has become increasingly confused and has had multiple episodes of vomiting. On physical examination, he is difficult to arouse, and his right pupil is larger than his left.
Of the following, a TRUE statement regarding the patient’s likely diagnosis is that
A. Improved survival is associated with prompt neurosurgical intervention in symptomatic patients
B. Intracranial injury is unlikely because there was no loss of consciousness
C. Mannitol is the initial treatment of choice
D. The gradual onset of symptoms is most consistent with a concussion
E. The injury is caused by laceration of the veins that bridge the dural sinuses and the brain
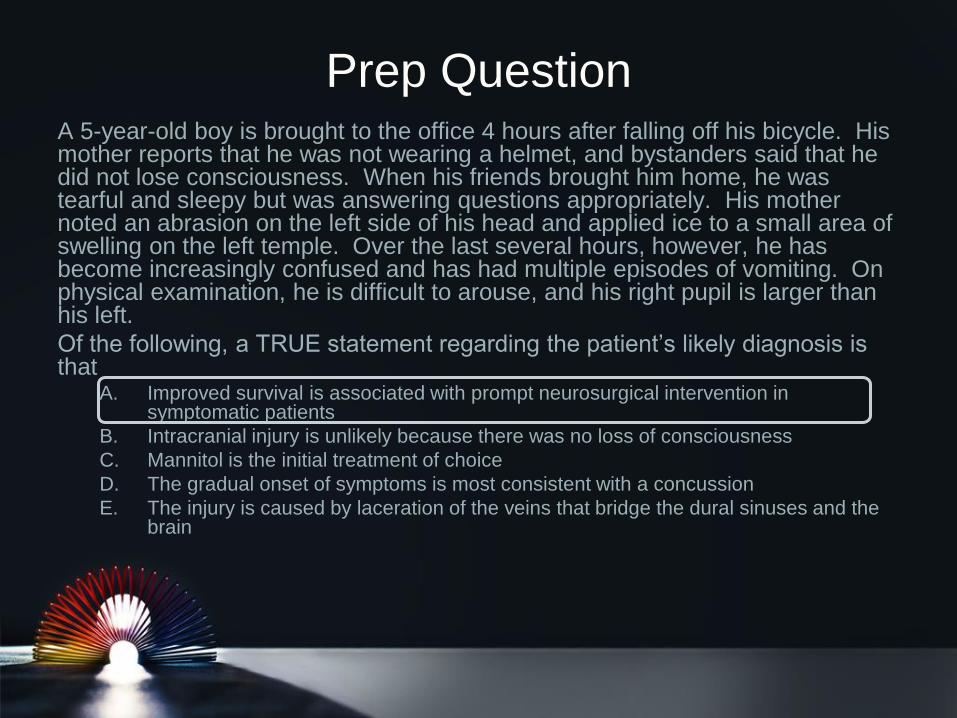
What are your first thoughts** in terms
of treatment/stabilization
Let’s meet our patient….
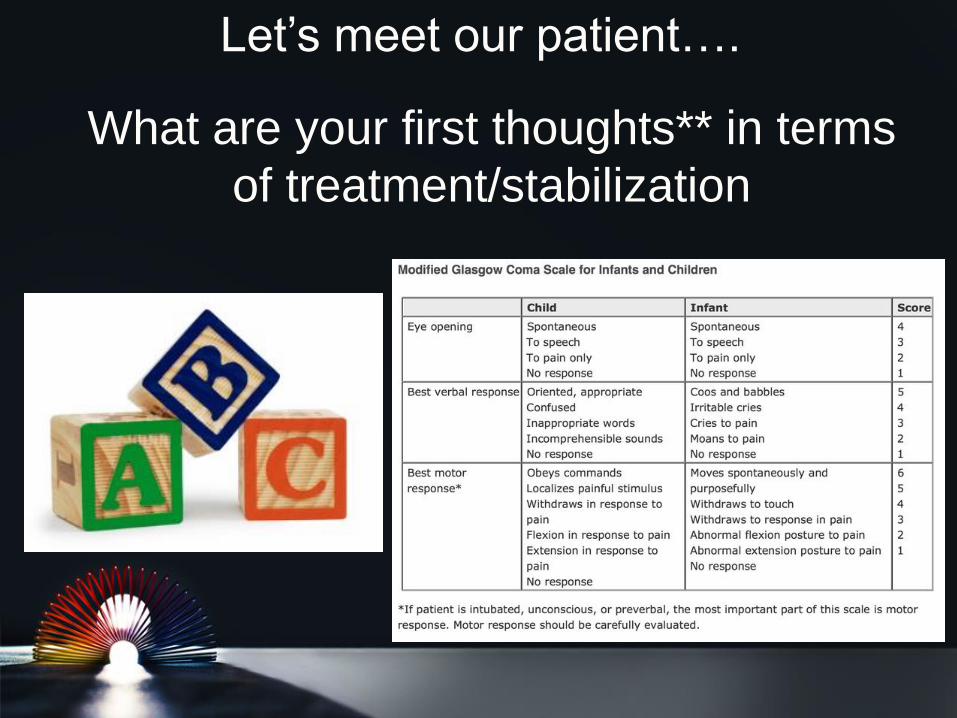
Qualifying our patient’s level of
consciousness
Level of Consciousness Description
Normal Awake, easy to arouse and
maintain alertness
Lethargic Difficult to maintain
alertness
Obtunded Decreased alertness,
responsive to pain, other
stimuli
Stuporous Decreased alertness,
responsive only to pain
Comatose Unresponsive, even to pain
Let’s go to the thinking chair….
Why is our patient stuporous?**
• Metabolic derangement
• Toxin or overdose
• Seizure
• Increased ICP
• Vascular
• Trauma
Let’s talk with mom
Finishing the exam….
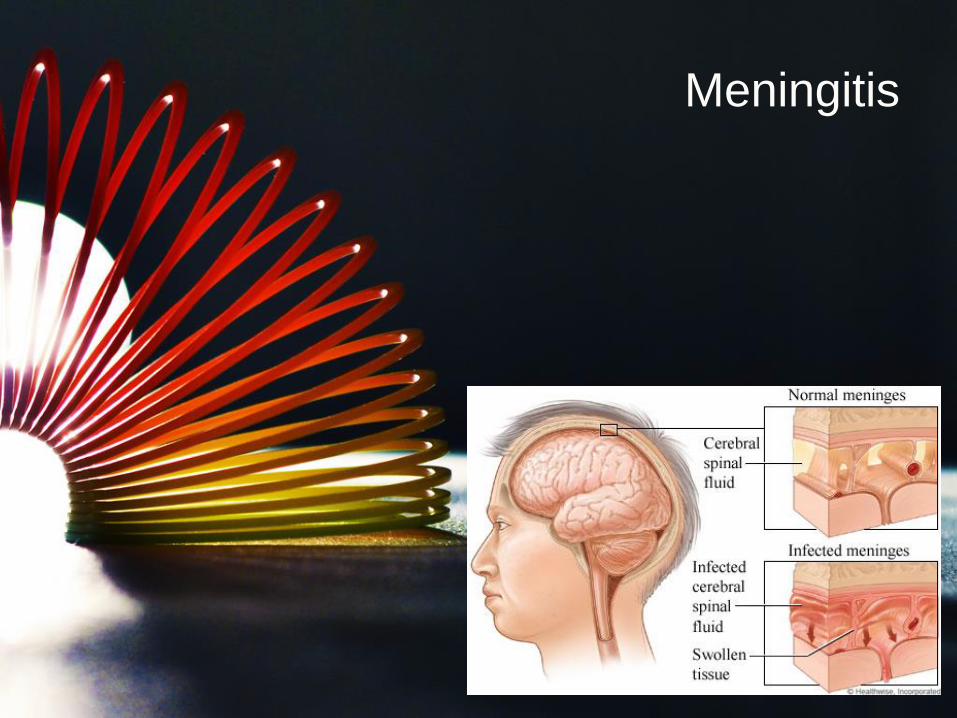
Meningitis
Epidemiology & Pathophysiology
• Bacteria/viruses gain entry into bloodstream through
mucosal surfaces, invade the meninges and
replicate, which induces an inflammatory response
• Bacterial vs Aseptic*
– 1 in 4 aseptic cases will have definitive cause found
• Who gets what bug?
– Well it depends
Etiology
Viruses
Fungi
Bacteria
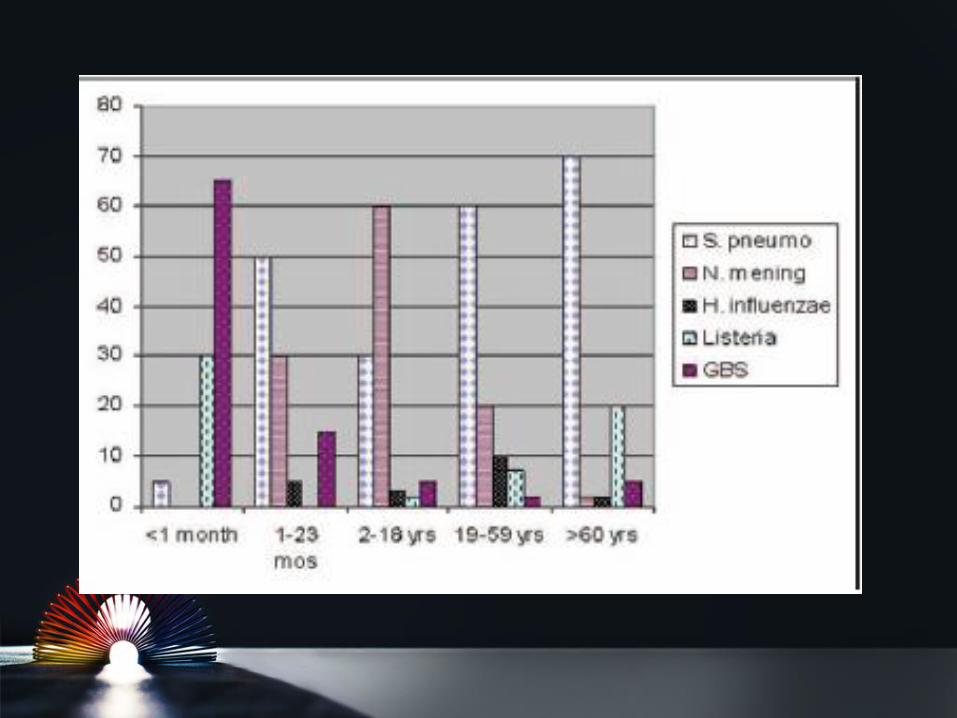
What are the 3 most common
causes of bacterial meningitis
in neonates?**
GBS, E coli, Listeria
What are the two most common
bacterial pathogens that cause
meningitis in children >1
month?**
Strep pneumoniae
Neisseria meningitidis
You are taking care of a very ill-appearing
baby who you suspect is septic. An LP is
suspicious for meningitis. Mom reports
AGE sxs prior to delivery and also received
imported cheese from France as a gift.
What organism are you worried about?
Listeria
Which bacteria should you also consider in
a patient adopted from a foreign country or
a patient whose mom has withheld
vaccinations due to fears of
complications?
Hib
Predisposing problems….
1) Your patient has a history of multiple infections and
now has Neisseria meningitis. What disorder
should you test this patient for?
• Terminal complement deficiency (C5-9)
2) You are taking care of a HgbSS patient with
suspected bacterial meningitis based on CSF
studies. What 3 organisms are you worried about?
• Neisseria, Strep pneumo, Hib
3) Other:
• Neurosurgery or head trauma within past month, CSF
leak, presence of neurosurgical devices, cochlear
implants, recent illness
It’s in the history**
Infants
• Fever
• Lethargy
• Irritability
• Especially with exam
• Prefer to be motionless
• AMS
• Vomiting
• Seizures
Older Children
• Malaise
• Myalgia
• HA
• Photophobia
• Neck stiffness
• Anorexia
• Nausea
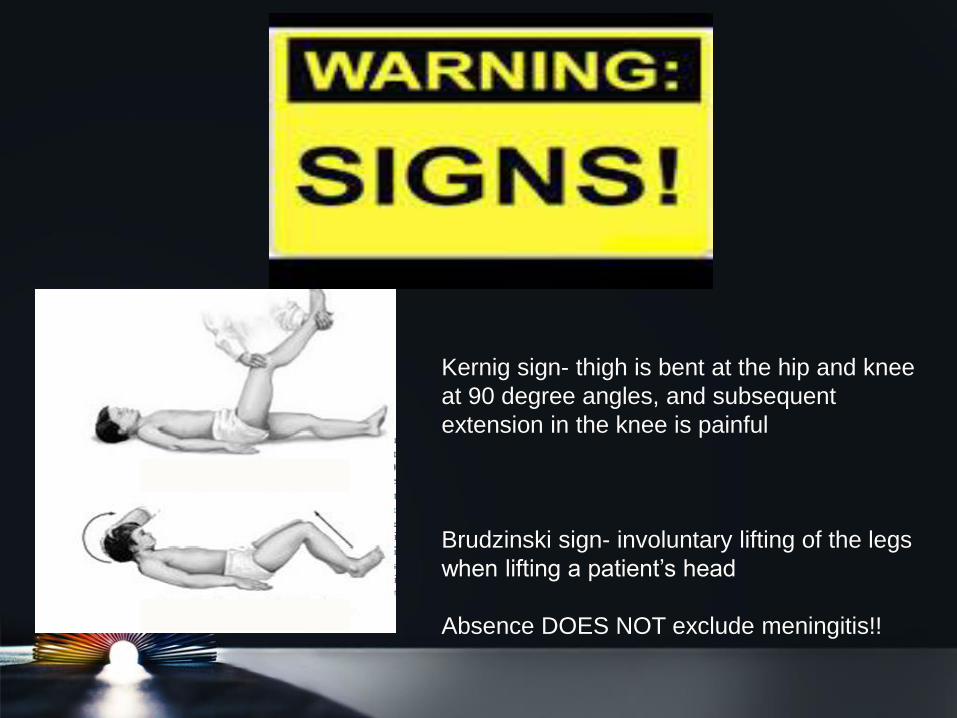
Kernig sign- thigh is bent at the hip and knee
at 90 degree angles, and subsequent
extension in the knee is painful
Brudzinski sign- involuntary lifting of the legs
when lifting a patient’s head
Absence DOES NOT exclude meningitis!!

Clinical Manifestations**• What is this physical exam finding?
• What organism do you suspect?
• Other than an LP, what diagnostic test can you do in an unstable patient to detect the organism?– Purpura fulminans
– N. meningitidis**
– Skin biopsy
• Remember the fontanelle
• Neurologic findings– AMS
– Papilledema
– Cranial nerve palsies (Lyme disease)**
– Focal deficits
Diagnostically speaking
• Labs: BCx, CBC/diff, chemistry panel, LFTs
(especially if suspecting HSV)
• CSF Studies
• Radiology
What kind of imaging?**
A CT of the head is necessary before LP in patients with signs or
symptoms of increased ICP and should be considered for…
– Altered mental status (GCS <12 or drop in GCS of ≥2)
– Immune deficiency
– Papilledema
– Focal neurologic deficit [excluding isolated CN VI or VII palsy]
– CSF shunt
– Hydrocephalus
– CNS trauma
– History of neurosurgery or a space-occupying lesions
– Signs or symptoms of parameningeal infection or tumor
Order of tubes
1. Gram stain, culture,
sensitivity
2. Glucose, protein
3. Cell count and differential
4. Miscellaneous studies
(fungal/viral/chemistry)
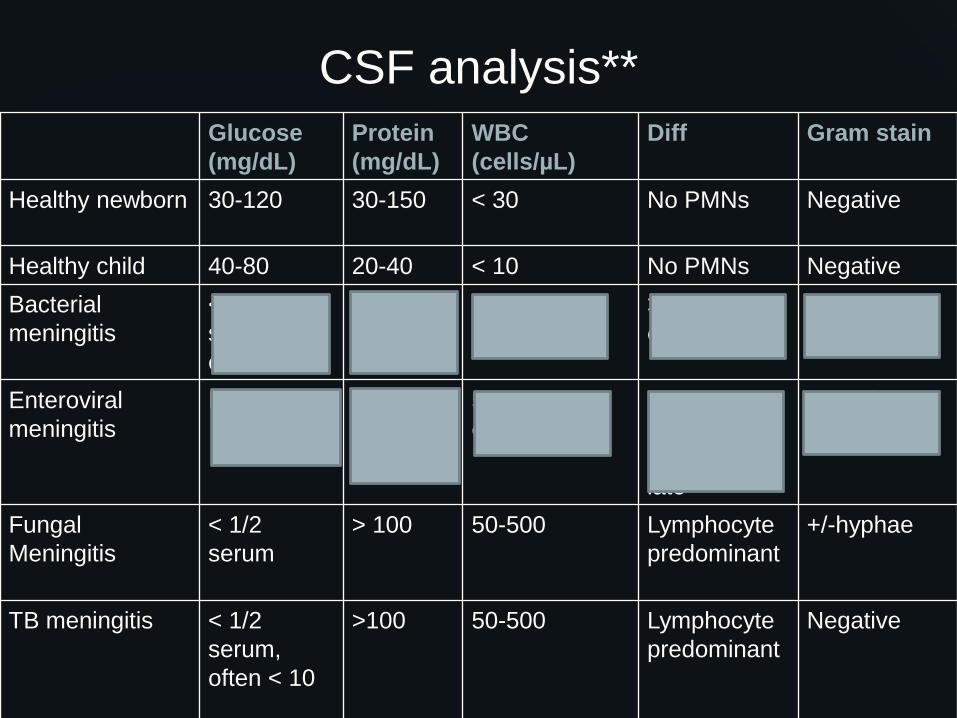
CSF analysis**
Glucose
(mg/dL)
Protein
(mg/dL)
WBC
(cells/µL)
Diff Gram stain
Healthy newborn 30-120 30-150 < 30 No PMNs Negative
Healthy child 40-80 20-40 < 10 No PMNs Negative
Bacterial
meningitis
< 1/2
serum,
often < 10
> 100 > 1000 >50% PMNs,
often >90%
Positive in
60-80%
Enteroviral
meningitis
Normal 40-60 50-500,
often < 100
>50%PMNs
early
<50%PMNs
late
Negative
Fungal
Meningitis
< 1/2
serum
> 100 50-500 Lymphocyte
predominant
+/-hyphae
TB meningitis < 1/2
serum,
often < 10
>100 50-500 Lymphocyte
predominant
Negative
Management
• Bacterial meningitis**
– Neonate: Ampicillin, Gentamicin/Claforen, consider
Acyclovir!!Supportive Care!!
– > 2 months: Vancomycin and Ceftriaxone/Claforen
– *Tailor antibiotic therapy once culture results obtained!
• Aseptic meningitis
– Supportive care
– Acyclovir for HSV meningitis
– Empiric therapy if suspect/cannot rule out bacterial
meningitis until cultures are negative
Complications**
• Shock
• Seizures
• Increased ICP
• Subdural effusions**
• Focal neurologic deficits
• Cerebral edema
• SIADH**…close monitoring of I/Os and electrolytes
is very important, especially for bacterial meningitis
cases!
In the long run…**
– Mortality - 5-10% for bacterial meningitis
– Intellectual deficits**
– Hydrocephalus
– Spasticity
– Blindness
– Hearing loss**
• Caused by infection +/- antibiotics
Have a great day!
Noon Conference: Feedback Sessions (Students Off!!)
Our patient’s course…