Embed Size (px)
Citation preview

International Dental Journal (2001) 51, 463-467
Smoking and health: opinions andawareness among general dentistsin JordanSamar Z. BurganAmman, Jordan
Aim: To examine dentists' awareness on major health risks associatedwith smoking and their opinions on factors that influence tobacco use.Design: A pre-tested postal questionnaire survey. Participants: Arandomly selected sample of 849 licensed general dentists who werepracticing dentistry in Jordan. Results: A response rate of 72.2% (613/849)was obtained. The majority of respondents (91.8%) related lung cancer tosmoking, however, associations with other cancers (cancer of oesophagus,pancreas and urinary bladder) were the least reported (33.6%). Only 39%agreed that smoking is the most important cause of premature death,non-smokers were significantly more likely to believe in this than currentsmokers. Most dentists associated tobacco use with staining of teeth(97.2%), whereas fewer dentists reported that smokers have increasedrisks of oral cancer (83.7%) and potentially malignant oral lesions (76.7%).Friends and stress were the most frequently implicated factors in thehabit of smoking. Conclusion: This study revealed a significant lack ofawareness among Jordanian dentists with respect to serious health consequences of smoking. An educational programme targeted towards generaldentists in Jordan is needed, focusing attention on tobacco related morbidity and mortality.
Key words: Oral health, general health, tobacco use, smoking, dentists,Jordan
Correspondence to: Dr Samar Z. Burgan, University of Jordan, P. O. Box 13182, Amman11942, Jordan. E-mail: [email protected]
© 2001 FDllWorld Dental Press0020-6539/01/06463-05
Smoking is a health behaviour thatcontributes to various diseases andadverse conditions. Diseases attributable to cigarette smoking causesan estimated 430,000 deaths inthe United States', and 120,000deaths each year in Great Britain".Tobacco use is the most importantcause of lung cancer and severalother cancers, in addition tocardiovascular diseases and chronicrespiratory tract disease', Althoughthe impact of nicotine dependenceon oral health has long beenrecognised, only recently has themagnitude ofits serious sequel beenestimated. The most significant isdeaths related to oral cancers", assmoking is a primary risk factorfor potentially malignant red andwhite lesions, as well as severe periodontal diseases, tooth loss, anddelayed wound healingr". Dentistsare trained to detect oral changesthat are associated with smoking",Therefore, they have the responsibility to educate their patients onthe profound health effects ofsmoking".
Tobacco smoking is a widespread habit among Jordanians.Results from a recent nationalsurvey showed that 26.8 per centof the adult population in Jordanwere current smokers and themajority began smoking early inlife (15 years oldj":", Most smokers use cigarettes, whereas theremainder use either a pipe orHubbly Bubbly!". It is worth

Table 1 Regional distribution of working general dentists in Jordan
All Sample Response rate
Northern region 309 (18.2%) 155 (18.2%) 97 (15.8%)Central region 1297 (76.6%) 651 (76.7%) 496 (80.9%)Southern region 87 (5.1%) 43 (5.1%) 20 (3.3%)Total 1693 849 613
464
mentioning that data is lacking inJordan on the association ofsmoking with various diseases andpremature death. However, canceris the second cause of death inJordan after cardio-vasculardiseases, as was reported recentlyby the National Cancer Registry".
The purpose of this baselinesurvey was to determine dentists'awareness in Jordan with respectto the impact of smoking ongeneral and oral health and theiropinions on factors contributing totobacco use.
Methods
Setting
The Hashemite Kingdom ofJordanis a South-Western Asian countryand is bounded on the north bySyria, on the south by Saudi Arabiaand the Gulf of Aqaba, on the eastby Iraq and on the west by theWest Bank. The offices of theJordan Dental Association ODA)are situated in the Capital Ammanand its membership is restricted todentists of Jordanian nationality.In May 1999, the updated lists ofnames provided by the register atthe JDA showed that although thetotal number of dentists of theworking age was 3,362, the actualnumber of those practicing dentistryin Jordan was 1,856. The remainder were either outside the country(992) or unemployed (514). Of1,856 working dentists, 91.2 percent were general practitioners and8.8 per cent were specialists. Therefore, only 1,693 working generaldentists aged 65 years and underwere included in the study population as those more than 65 yearsold were retired.
Studysample
The distribution of 1,693 generaldental professionals among thethree regions ofJordan, of whicheach compromises four governorates (Ministry ofInterior, 1999)is as follows: 18.2 per cent (309)were distributed in the northern
International Dental Journal (2001) Vol. 51/No.6
region; 76.6 per cent (1,297) in thecentral region, and 5.1 per cent (87)were practicing in the southernregion. This was taken into consideration when designing the samplesize (Table 1).The first name on thelist for each region was selected bysimple random procedure, whichthen continued with a systematicrandom sample. A representativesample of general dentists wasselected (which compromised 50per cent of the eligible study population in Jordan). The questionnairesurvey conducted in July 1999 waspiloted on 50 dentists who wereexcluded from the study sampleprior to it being posted to theselected random sample. Each questionnaire was accompanied by anexplanatory letter and a stampedaddressed, and coded return envelope. After the first mailing, only40 per cent of general dentistsresponded. Non-respondents weresent a further reminder in Augustand the same questionnaire wasenclosed with each reminder. BySeptember, a response rate of 50per cent was obtained. Dentistsfailing to respond to the secondmailing were telephoned and werehanded another questionnaire by amessenger, however, those in ruralareas could not be reached. Aresponse rate of 72.2 per cent wasachieved by December 1999. Nonresponders (27.8 per cent) weremost likely due to either being toobusy to return the questionnaire ormay not have received it at allbecause of mailing problems.
Survey instrument tool
The data were collected througha questionnaire constructed especially for this study by the authorand was designed in Arabic(mother language of Jordanians).
The self-reported questionnairecontained items that inquiredabout dentists' basic characteristicsregarding gender, age, smokingbehaviour and practice type; theirawareness of the health consequences of smoking, as well as theiropinions on factors that influencetobacco use (Tables 2-4 and Figures1 and 2).
Statistical analysis
From the responses, the data werecoded and entered into a databaseprior to analysis using SPSS.Descriptive statistics were generated to characterise the sample.Percentages were based on thenumber of respondents for eachvariable. The statistical significancewas determined by the Chi-squaretest.
Results
Respondents
Of the respondents, 71.1 per centwere male aged 23 to 65 years,with a mean of 35 years. The yearof basic graduation ranged from1956 to 1998 and covered a42-year period. Approximatelyhalf of respondents (51.1 per cent)had never smoked, 13.9 per centwere ex-smokers, and 35 per centcurrently smoked, of whom 83.3per cent were daily smokers. Mostof the current smokers (95.3 percent) use cigarettes, and the remainder (4.7 per cent) used cigars,pipes or Hubbly Bubbly. Withrespect to practice type, 70.8 percent of respondents were from theprivate sector, 17.5 per cent fromthe ministry of health, 5.5 per centfrom the military services, and 6.2per cent were from other formsof practice (which constitutesUNRWA, Voluntary Dental Asso-

465
Table 2 Profile of 613 general dentists
n %
GenderMale 436 71.1Female 177 28.9
Smoking habitsNever smoker 313 51.1Ex-smoker 85 13.9Current smoker 215 35.0
Practice typePrivate sector 434 70.8Ministry of health 107 17.5Military services 34 5.5Others 38 6.2
Table 3 Dentists' awareness on the impact of smoking on health (%)
Agreed Total never smoker ex-smoker current smoker Chi squaren (613) (313) (85) (215)
12.9"Causes premature death (39.0) 45.0 38.8 30.2Doesn't affect health (3.1) 3.5 2.4 2.8Its effect on health vary (57.9) 51.4 58.8 67.0
" differences significant at P .s 0.01
Table 4 Dentists' opinions on factors that influence tobacco use (%)
Important Total never smoker ex-smoker current smoker Chi squaren (613) (313) (85) (215)
Friends (83.7) 86.3 88.2 78.1 7.7"Stress (80.8) 84.0 69.4 80.5 9.2"Parent attitude (39.6) 44.1 37.6 34.0 5.6 NsIncome (13.1 ) 16.6 9.4 9.3 8.9 NsEducation (10.4) 11.5 5.9 10.7 3.3 Ns
" differences significant at P ~ 0.05
lLung cancer •••
Chronicairway diseases
Coronay heartdisease
Hypertension~
Stroke _45Othercancers~ 33.6
I i
91.8
85
o 20 40 80 100
%
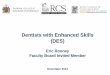
Figure 1. General health risks associated with smoking reported by 613 dentists
ciations and Labor Dental Clinics)(Table 2).
Dentists' awareness onsmoking and general health
Regarding the association of smok-
ing with lung cancer, other cancers(cancer of the oesophagus, pancreasor urinary bladder), chronic respiratory tract diseases, coronary heartdisease, stroke and hypertension,responses were as recorded inFigure 1. Only 39 per cent of
respondents reported that smoking is the most important cause ofpremature death, more who hadnever smoked agreed with thiscompared with current smokers (Ps 0.01). Disappointingly, 3.1 percent reported that smoking does
Burgan: Smoking and dentists in Jordan

466
%Figure 2. Oral health consequences of smoking reported by 613 dentists
diseases, in addition to chronicairway diseasesb'", The majority ofrespondents in this study (91.8 percent) agreed that smoking is themajor cause of lung cancer,followed by chronic airwaydiseases and cardiovascular diseases.However, cancers of the oesophagus, pancreas and urinary bladderwere least reported, with only 33.6per cent being aware of the linkbetween smoking and these cancers.It is well established that smokingis the chief cause of prematuredeaths throughout the world'r'.Between 25 and 30 per cent of allcancer deaths in Europe are due totobacco use"; However, only 39per cent of respondents believedthat smoking is the most importantcause of premature death, and thiswas significantly more reported bynon-smokers.
Lack of awareness amongJordanian dentists of links betweensmoking and malignancies orpremature deaths may be influencedby their smoking behaviour.Twenty-nine per cent ofJordaniandentists smoke daily in comparisonwith only 10 per cent of Europeandentists, who were more aware ofthe harmful effects of tobacco useon health".
Tobacco smoking is the mostimportant cause of oral cancers!",and most associated with potentially malignant oral lesions":".Mirbod and Ahing'" have linkedtobacco use with increased susceptibility to acute NUG, periodontaldiseases, white lesions, black hairytongue and tooth staining. Destructive periodontitis that is attributableto smoking may be responsible formore than half of periodontitiscases among adults in the USA7,21.Furthermore, the association ofsmoking with edentulousness wasreported by Axelsson and others",who found a significantly fewernumber of remaining teeth amongsmokers as compared with nonsmokers.
In the current study, the vastmajority ofparticipants consideredsmoking as the leading cause of
that income (13.1 per cent) andeducation level (10.4 per cent)influence this habit (Table 4).
Discussion
Tobacco related morbidity andmortality is shifting from industrialised countries to developingcountries '". As a high proportionof adult Jordanians smoke, it isimperative that dentists shoulddiscourage their patients fromsmoking, thus preventing life-threatening illnesses and malignancies",Sufficient evidence is presented inthe literature to associate smokingwith many oral and systemicdiseases. A strong relationship hasbeen found between smoking andlung cancer, which has nowbecame the fifth leading cause ofpreventable deaths among smokers, as well as with other cancers':".Lung cancer is one of the mostcommon cancers in Jordan andranked first among males". Recentstudies have also confirmed theassociation of smoking withelevated risk of coronary heartdisease and other cardiovascular
97.2
89.7
83.7
76.7
71
00.4
00.4
57.1
55
53.2
43.6
40.3
20 40 00 80 100
Dentists' awareness ofsmoking and oral health
When asked as to the implicationof tobacco use in the aetiology ofvarious diseases and conditions,dentists' responses were as recordedin Figure 2.
not affect health. However, 57.9per cent thought that its effect onhealth varied from one person toanother. Those currently smokingbelieved more significantly with thisthan those who had never smoked(P 50 0.01) (Table 3).
Halitosis
Stained teeth
Oralpremalignant lesions
Gingival colour changes
Susceptability to infections
More gingMtis
More periodontitis
Delayed wound healing
Susceptability to NUG-l
Hairy tongue ••••••1
Loss of teeth J~~~~~~---r--..,...---,o
Oral cancer
Dentists' opinions on factorsthat influence tobacco use
The majority ofrespondents reportedthat friends (83.7 per cent) andstress (80.8 per cent) were of greatinfluence on the act of smoking.Those who had never smoked weresignificantly more likely to reportthis than those currently smoking.Parental attitude towards smokingwas considered an importantfactor by only 39.6 per cent.However, a few respondents agreed
International Dental Journal (2001) Vol. 51/No.6

staining of teeth, whereas fewerassociated tobacco use with oralcancers and potentially malignantoral lesions.This indicates that thereis still a considerable need forimprovement ofknowledge amongJordanian dentists with respect toserious oral health consequences ofsmoking. Research is needed inJordan to investigate the association of smoking with oral andgeneral diseases and malignanciesand to estimate fatalities attributedto tobacco use.
A number of factors have beenassociated with the habit of smoking and most dentists in this studyconsidered friends and stress ofmajor influence, which accordswith the findings reported by Aroand Hasarr", Interestingly, respondents who quit smoking believedmore significantly than thosecurrently smoking that friends wereof prime importance in tobaccouse, whereas stress was moreacknowledged by those whosmoke. Although positive parentalmodeling and active parentingincluding strict rules about notsmoking were important strategiesfor preventing tobacco use amongadolescents.", only 39.6 per cent ofrespondents considered this issue.Studies on factors that influencetobacco dependence are lacking inthe literature and further researchis needed in this area.
Conclusions
General dentists in Jordan lackawareness on the serious healtheffects of tobacco use and thisappears to be influenced bydentists' smoking status. As a largeproportion of Jordanian dentistssmoke, help is needed to encourage them quit smoking. Moreover,there is a clear need for educational
trammg that increases dentists'knowledge on the major illnessesand fatalities associated withtobacco use. Thus Jordaniandentists could then become moreeffective health educators ininforming their patients about theill effects of smoking.
Acknowledgements
The author wishes to thank DrKhalid I. Ajluni and Dr Bassam Q.Hijawi for their valuable assistancein the survey and all dentists whocompleted and returned the questionnaire.
References
1. u.s. Centers for Disease Control andPrevention. Cigarette smoking-relatedMortality. CDC fact sheet: CDC'stobacco information and preventionsourcepage, 1996.
2. UK governments smoking strategy"Smoking Kills". 1998
3. U.S. Department of Health and HumanServices. Public Health Service,National Institutes of Health, NationalCancer Institute. How to help yourpatients be tobacco free, 1997.
4. World Health Organisation. Tobaccoor Health: a global status report, 1997.
5. Christen, A G. The impact of tobaccouse and cessation on oral and dentaldiseases and conditions. Am ] Med
1992 15: 93(lA): 25S-31S.6. Axelsson P, Paulander J, Lindhe J.
Relationship between smoking anddental status in 35-, 50-, and 75-yearold individuals. ] cs« Periodontol 199825: 297-305.
7. Bergstrom J, Eliasson S, Dock J. A10-year prospective study of tobaccosmoking and periodontal health. ]Periodontol 2000 71: 1338-1347.
8. Crews K M, Gordy F M, PentonEklund N, et al. Tobacco cessation: apractical dental service. Gen Dent1999 47: 476-483.
9. Jones R B. Tobacco or oral health:past progress, impending challenge. ]Am Dent Assoc 2000 131: 1130-1136.
467
10. Smoking habits among the adult population in Jordan. Ministry of Health inco-operation with the USAID. 1996.
11. Smoking habits among school studentsin Jordan. Ministry of Health in cooperation with the USAID, 1999.
12. National Cancer Registry (NCR). TheHashemite Kingdom of Jordan, Ministry of Health. 1998 report
13. Sarna L. Prevention: tobacco controland cancer nursing. Cancer Nurs 1999
22: 21-28.14. Benninger M S. The impact of ciga
rette smoking and environmental tobacco smoke on nasal and sinus disease: a review of the literature. Am]
Rhinol 1999 13: 435-438.15. Levi F, Lucchini F, Negri E, et al.
Worldwide patterns of cancer mortality, 1990-1994. Bur] Cancer Preu 1999
8: 381-400.16. Allard R H. Tobacco and oral health:
attitudes and opinions of Europeandentists; a report of the EU workinggroup on tobacco and oral health. Int
Dent] 2000 50: 99-102.17. Hart G T, Brown D M, Mincer H H.
Tobacco use and dental disease. ] Tenn
Dent Assoc 1995 75: 25-27.18. Reichart P A, Kohn H. Prevalence of
oral leukoplakia in 1000 Berliners.Oral Dis 1996 2: 291-294.
19. Hashibe M B, Mathew B, Kuruvilla Bet al. Chewing tobacco, alcohol, andthe risk of erythroplakia. Cancer
Epidemiol Biomarkers Preu 2000 9(7):639-645.
20. Mirbod S M, Ahing S 1. Tobacco-associated lesions of the oral cavity: Part1. Nonmalignant lesions. ] Can DentAssoc 2000 66: 252-256.
21. Tomar S L, Asma S. Smoking-attributable periodontitis in the UnitedStates: findings from NHANES III.National Health and Nutrition Examination Survey. ] Periodontol 200071: 743-751.
22. Aro S, Hasan J. Occupational class,psychological stress and morbidity.Ann cs» Res 1987 19: 62-68.
23. Rissel C, McLellan L, Bauman A. Factors associated with delayed tobaccouptake among Vietnamese/Asian andArabic youth in Sydney, NSW. Aust NZ ] Public Health 2000 24: 22-28.
Burgan: Smoking and dentists in Jordan