Embed Size (px)
Citation preview

Somatosensory Disinhibition in Dystonia
Emma Frasson, MD,1 Alberto Priori, MD,2 Laura Bertolasi, MD,1 Francois Mauguie`re, PhD,3
Antonio Fiaschi, MD,1 and Michele Tinazzi, MD1*
1Dipartimento di Scienze Neurologiche e Della Visione, Sez. di Neurologia e Sez. di Neurologia Riabilitativa, Verona, Italy2Istituto di Clinica Neurologica, Universita` di Milano, IRCCS Ospedale Maggiore di Milano, Italy
3Functional Neurology and Epileptology Department, Hopital Neurologique, Lyon, France
Abstract: Despite the fact that somatosensory processing isinherently dependent on inhibitory functions, only excitatoryaspects of the somatosensory feedback have so far been as-sessed in dystonic patients. We studied the recovery functionsof spinal N13, brainstem P14, parietal N20, P27, and frontalN30 somatosensory evoked potentials (SEPs) after paired me-dian nerve stimulation in 10 patients with dystonia and in 10normal subjects. The recovery functions were assessed (condi-tioning stimulus: S1; test stimulus: S2) at interstimuls intervals(ISIs) of 5, 20, and 40 ms. SEPs evoked by S2 were calculatedby subtracting the SEPs of the S1 only response from the SEPsof the response to the paired stimuli (S1 + S2), and their am-plitudes were compared with those of the control response (S1)at each ISI considered. This ratio, (S2/S1)*100, investigateschanges in the excitability of the somatosensory system. Nosignificant difference was found in SEP amplitudes for single
stimulus (S1) between dystonic patients and normal subjects.The (S2/S1)*100 ratio at the ISI of 5 ms did not significantlydiffer between dystonic patients and normal subjects, but atISIs of 20 and 40 ms, this ratio was significantly higher inpatients than in normals for spinal N13 and cortical N20, P27,N30 SEPs.
These findings suggest that in dystonia there is an impairedinhibition at spinal and cortical levels of the somatosensorysystem which would lead to an abnormal sensory assistance tothe ongoing motor programs, ultimately resulting in the motorabnormalities present in this disease. © 2001 Movement Dis-order Society.
Key words: upper limb SEPs; somatosensory evoked poten-tials; dystonia; somatosensory system; recovery cycle; pairedstimulation
Dystonic movements typically imply cocontractionand overflow activity of inappropriate muscles. It hasbeen widely held that a dysfunction of cortical-striato-thalamo-cortical motor circuits plays a major importancein the pathophysiology of dystonia.1–4 However, there isclinical and neurophysiological evidence suggesting thatabnormalities of somatosensory feedback may contributeto dystonia.4,5 The stimulation of afferents which sub-serve the sensation of joint position, obtained by a tonicvibration of the biceps brachii, induced an abnormal per-ception of arm movements in patients with idiopathicfocal dystonia; this hints at a disorder of the processingof muscle spindle inputs in these patients.6 Similarly,
while vibration of the tendon or the belly of a givenmuscle can induce dystonia in patients with hand cramp,a reduction of the effectiveness of muscle spindle affer-ents, obtained through local injection of an anesthetic,can ameliorate dystonia.7 Moreover, it has been observedclinically that dystonic spasms are alleviated by provid-ing cutaneous and proprioceptive inputs (“sensorytricks).2,3,8 Patients with focal hand dystonia may alsopresent with an impairment of graphesthesia and stere-ognosis as well as impaired temporal discrimination ofsomesthetic stimuli.9,10 Finally, we observed that spa-tially separated somatosensory inputs have a reduced in-hibition in dystonic patients.11
The positron-emission tomographic (PET) techniquehas been used in dystonic patients to show metabolicactivation of basal ganglia and cortical areas. Passivevibrotactile stimulation of the hand resulted in attenu-ated regional cerebral blood flow increase in the senso-rimotor cortex,12,13and metabolic underactivation of thesensory-motor cortex was present during active hand
*Correspondence to: Dr. Michele Tinazzi, Dipartimento di ScienzeNeurologiche e della Visione, Sez. di Neurologia Riabilitativa, via delleMenegone 6, 37134 Verona, Italy.
Received 20 May 2000; Revised 26 August 2000; Accepted 4 Sep-tember 2000
Published online 16 July 2001; DOI 10.1002/mds.1142
Movement DisordersVol. 16, No. 4, 2001, pp. 674–682© 2001 Movement Disorder SocietyPublished by Wiley-Liss, Inc.
674

movement.14–16However, we cannot establish from PETfindings whether these abnormal changes in cortical ar-eas refer to abnormal excitatory and/or inhibitory neuralactivity, since this technique detects the total regionalmetabolism and thus only gives an indirect measure ofneural activity, nor are we able to demonstrate changes inspinal and brainstem structures of the somatosensorypathway which may be involved in dystonia.
Somatosensory evoked potentials (SEPs) offer theunique opportunity to assess the neural activity of dorsalhorn (DH) and of dorsal column-lemniscus medialis(DC) systems of the lemniscal pathway. For upper limbSEPs, DH activity is assessed by recording of spinalN13, while DC activity is assessed by recording of brain-stem P14 and cortical N20, P27 and N30 potentials. Rou-tine SEP studies have produced conflicting results. Up-per limb SEP studies reported in several dystonic pa-tients an increased amplitude of the N30 potentialpossibly arising from motor cortices,17–20 while othersreported a decreased amplitude.21 The only availableSEP study from the lower limbs also showed an in-creased amplitude of some cortical potentials.22 How-ever, all these studies deal with the excitatory aspects ofsomatosensory feedback despite the fact that somatosen-sory processing is inherently dependent on inhibitoryfunctions. Activity of inhibitory and excitatory neuronalpopulations at the spinal, brainstem, and cortical levelsof the somatosensory system may be evaluated with theSEP technique by means of peripheral paired stimuli. Inboth normal animals and humans, a conditioning stimu-lus induces, via different mechanisms, suppression ofspinal, brainstem, and cortical SEP amplitudes evokedby a following test stimulus.23–33
To assess possible abnormalities of the balance be-tween excitation and inhibition both in DH and in DCsystems in dystonia, we studied SEP with paired stimuliat interstimulus intervals of 5, 20, and 40 ms in a groupof patients affected by idiopathic dystonia.
PATIENTS AND METHODS
We studied SEPs in 10 dystonic patients (sevenwomen and three men, age range 21–55 years, mean age38.9 years) and in 10 healthy subjects (six women andfour men, age range 26–52 years, mean age 37.3 years).No patient had a family history of dystonia. Clinicalfindings from dystonic patients are shown in Table 1.Eight patients had generalized dystonia involving all fourlimbs, axis and neck (complex torticollis in patients 1,4,7; retrocollis in patients 2, 10; right torticollis in patients,5, 8; left torticollis in patient 3). Two patients had seg-mental dystonia (right arm dystonia and right torticollisin patient 9; left arm dystonia and retrocollis in patient
6). Motor impairment of the arms was graded by calcu-lating the arm subscore (0–4) of the Fahn-Marsden Rat-ing Scale.34
All patients underwent an extensive neurological ex-amination paying special attention to possible clinicalsensory abnormalities (tactile sensation and positionsense). No patient had sensory abnormalities and nonehad tremor. The results of biochemical, computed tomo-graphic, and magnetic resonance imaging examinationswere normal, indicating idiopathic dystonia.
Four patients received treatment with botulinum toxin(BTX-A) until 6 months before the SEP recording ses-sion, three with anticholinergic drugs (2–6 mg triexyphe-nidyl daily) and the remaining three patients were nottreated. BTX-A (Dysport; Speywood Biopharm LTD,U.K.) was injected locally into the cervical muscles in allthe treated patients and also into forearm flexors in twoof them based on previous clinical and electromyo-graphic (EMG) observations. BTX-A was used at a con-centration of 200 U/ml. The number of BTX treatmentsessions were three in three patients and two in one pa-tient. The amount of BTX-A injected in each treatmentsession ranged from 300 to 400 U and the interval be-tween each session ranged from 3 to 5 months. Beforethe study began, the three patients treated with anticho-linergic drugs had been off therapy for at least 2 days. Allsubjects gave their written informed consent prior to par-ticipation in the study, and the protocol was approved bythe Local Ethical Committee.
SEP Recording ProcedureIn the SEP recording session, subjects were instructed
to lie supine on an examination couch in a relaxed andcomfortable position. Right and left median nerve SEPswere recorded in all subjects. The median nerve was
TABLE 1. Clinical findings in dystonic patients
SubjectAge
(years) Sex Diagnosis
Arm motorimpairment*
Rightside
Leftside
1 43 F Generalized dystonia 3 32 55 F Generalized dystonia 3 33 35 F Generalized dystonia 2 24 25 M Generalized dystonia 3 35 21 F Generalized dystonia 1 16 37 M Left-sided segmental
dystonia0 3
7 39 M Generalized dystonia 4 48 48 F Generalized dystonia 3 39 46 F Right-sided segmental dystonia 4 0
10 40 F Generalized dystonia 3 2
*Arm motor impairment subscore (from 0 to 4) according to theFahn-Marsden Rating Scale of Dystonia.
PAIRED STIMULATION SEPS IN DYSTONIA 675
Movement Disorders, Vol. 16, No. 4, 2001

stimulated at the wrist. Stimuli were electrical squarepulses of 0.2 ms duration delivered at a rate of 2.2 Hzthrough Ag/AgCl surface electrodes (cathode proximal;impedance below 5 Kohm) over the nerve. The groundelectrode was placed over the forearm. The stimulus in-tensity was at motor threshold (eliciting a visible andstable twitching of the thenar eminence). Four trials wereperformed for left and right side: the median nerve wasstimulated with single stimuli (S1) and with pairedstimuli (S1 + S2) at interstimulus intervals (ISIs) of 5,2,0 and 40 ms. The sequence of these trials was random-ized among the subjects. To isolate SEP of the test stimu-lus (S2), it was necessary to subtract the conditioning(S1) response from the paired (S1 + S2) response.Samples with excess of interference were automaticallyrejected from the average. In patients, the rejection ratiowas about 50% and the duration of these recordings wasabout 2 hours for each side. This was due to the narrowrejection window we used in order to reduce muscularartifact determined by eventual dystonic contractions.Seven hundred sweeps were averaged for each trial. Eachtrial was repeated at least twice to confirm reproducibil-ity. Summated tracings of two repeatable averages wereused for amplitude and latency measurements. Analysistime was 100 ms and filtering band-width was 5–1,500Hz (−6dB octave roll-off).
SEPs were recording using an ESAOTE BIOMEDICAReporter (ESAOTE BIOMEDICA, Florence, Italy). Re-cording electrodes were placed over the spinous processof the sixth cervical vertebra (Cv6), and over the parietalP3 (P4) and frontal F3 (F4) scalp regions contralateral tothe stimulation side. The Cv6 electrode was referred toan electrode located immediately above the process ofthe thyroid cartilage (Ac). Parietal and frontal electrodeswere referred to the earlobe of the stimulated side. Toensure full muscle relaxation, muscular activity wasmonitored through surface EMG recordings from theflexor and extensor muscles of the stimulated arm. Infive normal subjects, SEPs were also recorded while thesubject maintained a tonic isometric wrist flexion at 10%of maximum EMG activity level. Acoustic EMG feed-back helped the subjects to maintain a constant level ofcontraction.
We identified the following SEP components: the N13potential was recorded at Cv6, which originates in thedorsal horn of the cervical spinal cord35,36 and which ispreceded by a peripheral P9 far-field potential arisingfrom the brachial plexus;35 the scalp P14 far-field poten-tial was recorded over the parietal and frontal electrodes,which originates in the medial lemniscal pathway;35 theN20 and P27 potentials were recorded over the parietalregion contralateral to the stimulation side, which arise in
the primary somatosensory cortex;37,38the N30 potentialwas recorded over the contralateral frontal region, whichprobably originates from multiple generators located inthe frontal lobe37,39and in the posterior wall of the cen-tral sulcus.38 Amplitudes of all SEPs were measuredfrom the preceding peak (peak-to-peak) to prevent theimpact of baseline shift on the results, while latencieswere measured at the peak of each component.
We measured the amplitude of the subtracted waveform (test response) and compared it with the controlsingle stimulus response at each ISI. The amplitude ratioof the test response was expressed as percentage of theamplitude of the component obtained in S1 condition foreach ISI. We evaluated SEP amplitudes of control re-sponse (S1) and the amplitude ratio (S2/S1)*100 at 5, 20,and 40 ms of ISIs between SEPs of the test response (S2)and the control response (S1).
For statistical analysis, we used the analysis of vari-ance (ANOVA) equivalent for non-parametric data(Kruskal-Wallis). We used Spearman’s correlation test tocompare amplitude of brainstem P14 and cortical N20,P27, and N30 at the ISIs of 20 and 40 ms. The level ofsignificance was set atP < 0.05. Values in the text aremeans ± 1 S.D.
RESULTSThe mean peak-to-peak amplitude values of central
SEPs obtained by single stimulus (S1) from normal sub-jects and dystonic patients are listed in Table 2. Themean amplitude of SEP components did not significantlydiffer between patients and control group, although SEPamplitudes were slightly larger in patients. In normalsubjects, amplitude values of SEPs did not significantlydiffer between left and right hemisphere.
In patients, amplitude values of SEPs were slightly butnot significantly larger over the left hemisphere. Amongpatients with torticollis (patients 3, 5, 8, and 9), patientwith right-sided segmental dystonia (patient 9) had alarger N30 potential recorded over the left frontal region.
TABLE 2. Mean amplitude measured peak-to-peak (µV) andstandard deviation (S.D.) of somatosensory evoked potentials(SEP) components obtained in response to single stimuli (S1)
in normal subjects and in dystonic patients.
Components N13 P14 N20 P27 N30
SideRight arm Controls Mean 1.06 0.9 2 2.05 2.4
S.D. 0.49 0.31 0.44 0.66 0.93Patients Mean 1.22 0.96 2.29 2.43 2.86
S.D. 0.65 0.48 0.75 1.3 1.31Left arm Controls Mean 0.88 0.81 1.66 1.73 1.89
S.D. 0.34 0.21 0.31 0.47 0.66Patients Mean 1.13 0.99 2.09 2.18 2.27
S.D. 0.53 0.52 0.62 0.96 1.09
E. FRASSON ET AL.676
Movement Disorders, Vol. 16, No. 4, 2001

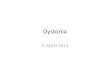
In normal subjects, N13, P14, N20, P27, and N30,SEP amplitudes of the S2 response were significantlysuppressed at ISIs of 5, 20, 40 ms with respect to thoseof the S1 control response; more specifically, SEP am-plitudes of the test S2 response were always smaller thanthose of the control S1 response (Fig. 1). The P9 behaveddifferently: the amplitude of the conditioned-test S2 re-sponse was similar to the amplitude of the unconditionedcontrol P9 elicited by single stimulus. There were noside-to-side amplitude differences between right and leftside in subjects.
In patients, N13, P14, N20, P27, and N30, SEP am-plitudes of the S2 response were significantly suppressedonly at the ISI of 5 ms, while these were not suppressedat ISIs of 20 and 40 ms. There were no side-to-sideamplitude differences between right and left arms in pa-tients.
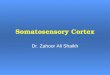
The (S2/S1)*100 ratio was significanlty (P < 0.05)higher in patients for spinal N13 and cortical N20, P27,N30 SEPs at the ISIs of 20 and 40 ms (Fig. 2). This ratiowas also higher but not significantly in patients for P14at the ISIs of 20 and 40 ms. The (S2/S1)*100 ratio of allcentral SEPs did not differ between patients and controlsat the ISI of 5 ms. The mean ratio of peripheral P9potential did not differ between patients and controls,thus suggesting that SEP abnormalities in patients occurwithin the central somatosensory pathway.
Latencies of S2 responses were greater than S1 re-sponses for N13 at the ISIs of 5 and 20 ms and for P14,N20, P27, and N30 at all ISIs in normal subjects and indystonic patients. In some patients (1, 3, 4, 6, 7, 9), oneor more components for right and left arm stimulationSEP amplitudes of S2 had even larger amplitudes thanthose of S1 both at 20 ms and 40 ms of ISI (Figs. 3 and4); this phenomenon, which was never observed in nor-mal subjects, was found for N13 in 10 and 9 sides, re-spectively, for P14 in 3 and 4 sides, for N20 in 7 and 8sides, for P27 in 8 and 9 sides, for N30 in 11 and 9 sides.Abnormalities were concomitant in the DH system (asreflected by N13) and in the DC system (as reflected byP14, N20, P27, and N30) on 10 and 8 sides, while theabnormalities were either in the DH or in the DC systemalone on 2 and 3 sides. Within the DC system, there wasno significant correlation between brainstem P14 andcortical N20, P27, and N30 SEP abnormalities (Spear-man’s correlation at 20 ms of ISI: R4 0.27 for N20, R4 0.19 for P27, R4 0.30 for N30; at 40 ms of ISI: R4 0.28 for N20, R4 0.40 for P27, R4 0.23 for N30).
To assess whether our findings in patients could haveaspecifically originated from a possible facilitation of themotor system, we studied the SEP (S2/S1)*100 ratio ofN13, N20, P27, and N30 responses at 20 and 40 ms of
ISIs at rest and during voluntary contraction in the fivenormal subjects. The ratio did not significantly differ atrest and during voluntary contraction (87.5% ± 5.3 at theISI of 20 ms and 85.4% ± 6.8 at the ISI of 40 ms duringcontraction, vs. 89.9% ± 6.8 at the ISI of 20 ms and86.1% ± 8.4 at the ISI of 40 ms during relaxation for
FIG. 1. Somatosensory evoked potentials (SEPs) of control responsebaseline (S1) and of test response (S2) at 5, 20, and 40 ms of inter-stimuls intervals (ISIs) obtained after stimulation of the right mediannerve in a 36-year-old healthy male subject. The N13 potential isrecorded with a sixth cervical vertebra-thyroid cartilage (Cv6-Ac) mon-tage. It is preceded by a P9 far-field potential reflecting the activity ofthe brachial plexus. Over the scalp, the N20 potential recorded over theparietal electrode (P3) contralateral to the stimulation side is precededby a P14 potential and followed by a P27 potential. The N20 potentialexhibits a reversed-phase P20 potential over the frontal electrode (F3)followed by a large negativity (N30 potential). Note that the amplitudeof spinal N13, parietal N20, P27, and frontal N30 potentials of the S2response at 5, 20, and 40 msec of ISI is reduced as compared withamplitude of SEPs of the S1 response. Note that the peripheral P9potential of the S2 response has the same amplitude as the S1 response.
PAIRED STIMULATION SEPS IN DYSTONIA 677
Movement Disorders, Vol. 16, No. 4, 2001

N13; 74.8% ± 15 and 80.9% ± 16.3 vs. 76.6± 17.9 and82.7 ± 16.6 for N20; 74.2 % ± 13.3 and 64.1% ± 11.6 vs.70.9 ± 16.5 and 63.4 ± 12 for P27; 74% ± 19.4 and68.3% ± 14.5 vs. 70.5± 20.7 and 70.2 ± 18.2 for N30).
DISCUSSION
Our data show that the suppression of median nerveSEPs evoked by paired stimuli is reduced at multiplelevels of the lemniscal pathway in dystonic patients.These SEP abnormalities occurred at interstimulus inter-vals of 20 and 40 ms, but not at 5 ms. The lack ofsuppression of SEP components to paired stimuli indi-cates an abnormal excitability within the somatosensorypathway in dystonia, which would in turn lead to a dis-turbed sensorimotor integration.
Previous routine studies in dystonia showed that insome patients the median nerve-derived N30 potentialhas an increased amplitude17–20but others failed to rep-licate this finding.21 In the present study, single stimuliof the median nerve elicited slightly but not significantlylarger N30 in patients. These discrepant results couldreflect methodological differences between our studyand previous reports. For example, we delivered stimuli
at a higher rate, which is a variable inversely related toamplitude of the N30 SEP component.40 In addition,some studies reported an increased N30 above the hemi-sphere contralateral to the direction of head deviation incervical dystonia.18–20 We observe this finding only inone patient with segmental right-sided dystonia withright torticollis. This SEP feature was not observed in theother three patients with torticollis affected by general-ized dystonia. This finding may be consistent with therecent observation of Kanovsky et al.20 who showed thatSEP abnormalities are bilaterally present in patients withdystonic head tremor.20 We can therefore speculate thatin generalized dystonia, there is a bilateral cortical in-volvement.
On the other hand, using paired nerve stimulation, thesuppression of SEP components was lower; i.e.,we foundless inhibited SEPs in dystonic patients than in normals.Our control recordings in normal subjects during a slightvoluntary contraction and the careful control of relax-ation in dystonic patients exclude the possibility that theabnormal SEP suppression in dystonic patients arisefrom changes in the excitability of the motor system.
Under normal conditions, different mechanisms ac-
FIG. 2. Histogram of mean amplitude ratio [expressed as (S2/S1)*100] at 5, 20, and 40 ms of ISI for N13, P14, N20, P27, and N30 potentials obtainedin response to stimulation of the right and left arm in patients and in control subjects. Note that the mean ratio of all central SEPs at the ISI of 5 msecdid not differ between dystonic patients and normal subjects, but that at the ISI of 20 and 40 ms, this ratio was significantly higher in patients thanin normals for spinal N13 and cortical N20, P27, N30 potentials.
E. FRASSON ET AL.678
Movement Disorders, Vol. 16, No. 4, 2001

count for the suppression of central SEP components atDC and DH.26,27,29,32,33At ISI of 5 ms, the suppressionof all central SEPs is probably determined by interposedsynapses.27,29,32At ISIs of 20 and 40 ms, the suppressionat the DH level (as reflected by the spinal N13 potential)is mediated through DH interneurons,32 while at the DClevel (as reflected by the lemniscal P14 and cortical N20,P27, N30), the suppression is due to postsynaptic poten-
tials (IPSPs) probably mediated by interneurons withinthe thalamus (ventral postero-lateral nucleus).26,33 Thereduced suppression of central SEPs elicited by pairedstimuli at ISIs of 20 and 40 ms, but not at 5 ms, suggeststhat in dystonia the excitability of inhibitory systemswithin the somatosensory pathway decreased. This find-ing is in line with data obtained from animal studieswhich proposed a cortical reduction of inhibitory func-tions to explain the altered differentiation of normallyseparate representations of the body maps in the primarysensory cortex in dystonia,41 and with the observation of
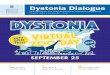
FIG. 3. Somatosensory evoked potentials of control response (S1) andof test response (S2) at 5, 20, and 40 ms of ISI obtained followingstimulation of the right median nerve in a 43-year-old female patientwith generalized dystonia. Note that the amplitude of spinal N13, lem-niscal P14 , parietal N20, P27, and frontal N30 potentials of the test(S2) responses at 20 and 40 msec of ISI is greater than that of thecontrol (S1) response, while at 5 ms of ISI it is normally suppressed.
FIG. 4. Somatosensory evoked potentials of control response (S1) andof test response (S2) at 5, 20, and 40 ms of ISI obtained followingstimulation of the right median nerve in a 25-year-old male patientaffected by generalized dystonia. Also note that in this patient theamplitude of spinal N13, parietal N20, P27, and frontal N30 potentialsof the test (S2) responses at 20 and 40 ms of ISI is greater than that ofthe control (S1) response, while at 5 ms of ISI it is normally sup-pressed. Also note that the P9 potential of the S2 and S1 responses issimilar.
PAIRED STIMULATION SEPS IN DYSTONIA 679
Movement Disorders, Vol. 16, No. 4, 2001

an altered representation of the fingers in the primarysomatosensory cortex of dystonic musicians reported bya recent magnetoencephalographic study.42 This reducedsuppression was observed for spinal N13 and corticalN20, P27, N30 SEPs. The finding of a reduced suppres-sion of different cortical SEPs, which are thought to dis-tinctly originate from different areas, suggests a wide-spread abnormality of intracortical inhibitory circuits.Moreover, these abnormal cortical responses to pairedstimuli seem unrelated to brainstem abnormalities, sincethere was no significant correlation between abnormali-ties of the P14 and N20, P27, N30 SEPs. Reduced ac-tivity in inhibitory circuits might also account for thedecreased blood flow in the primary sensory-motor cor-tices both during passive vibrotactile stimulation of thehand and during active paced joystick movements.12–16
In dystonic patients, our data showing that N13 suppres-sion was also impaired suggest that abnormal inhibitionin dystonia is not restricted to the cortex but also occursat the spinal level and that abnormalities at this level andwithin the cortex are not related, since no changes of P14were present. Our data do not permit us to establishwhich afferent inputs (muscle spindle and/or cutaneous)are involved by the reduction of inhibition. However, inpatients with dystonia, several data suggest a rather spe-cific involvement of muscle spindle inputs;6 further, wepreviously observed more SEP inhibition stimulatingmixed, rather than digital nerve in dystonia, thus sug-gesting an abnormality of muscle spindle inputs and to alesser extent of cutaneous inputs.11 We can thereforespeculate that the same afferent involvement is also pres-ent in this study.
Reduced inhibitory functions during paired stimula-tion implies an impaired temporal processing of afferentinputs in dystonia. Normally, a “conditioning” inputwhich engages the sensory system prior to a “test” input,has an inhibitory action that gates the total signal at allcentral levels, temporally limiting the amount of input tothe central nervous system. This appears not to be thecase in dystonia. Although the functional importance ofthis gating is not fully understood, this mechanism couldplay an important role in preserving the temporal sepa-ration of the two stimuli.43 In this way, sensory inhibitionenhances the temporal contrast between stimuli, so thatinformation from a single body part is perceived and,more importantly, processed separately in time. Themore immediate and challenging question is to determineprecisely what afferent input overflow does. A possibleanswer is to be found in an incomplete processing of theincoming signal, resulting in temporally distorted infor-mation. This may explain why dystonic patients presentwith deficits in kinesthesia, graphesthesia, and stereog-
nosis,6,9 since all these rely heavily upon an adequatetemporal sampling of afferent stimuli,43 and is consistentwith our recent finding of an impairment of somesthetictemporal discrimination threshold in dystonic patients.10
In turn, temporally distorted sensory information wouldprovide a distorted assistance to the processing of motorprograms, leading to the clinical appearance of dystonia.In normal conditions, afferent input to the motor systemleads to a finely tuned activation of neural elements andultimately results in the correct execution of move-ment.44–48Disinhibited afferent inputs could give rise toabnormal sensory feedback to ongoing motor tasks indystonia. This hypothesis is in keeping with the obser-vation that patients with writer’s cramp have an impair-ment in regulation of temporal sequencing of variousmovement phases during precision grip.49 In otherwords, a reduced temporal filtering of sensory signals indystonia could result in an alteration of sequential phasesof grip forces, which gives rise to an inefficient regula-tion of force during precision grip tasks resulting in mo-tor overflow.
Our data and previous observation show that in dys-tonia there is a temporal and spatial sensory overflow. InHuntington’s disease and in Parkinson’s disease, abnor-malities of cortical SEP components are present, andpaired stimuli induce reduced suppression of corticalSEP components.50,51This implies that the basal gangliainfluence sensory inputs to the cerebral cortex.52–54. Thecarrefour for the interaction between the motor and sen-sory systems may be the reticular nucleus of the thala-mus. This nucleus has a mainly inhibitory control func-tion on all the other nuclei of the thalamus, and its stimu-lation inhibits SEP transmission in the rat.52–54
Interestingly, chronic stimulation of the thalamus, whichis supposed to activate the reticular thalamic nucleus, isalso effective for dystonia.53 This would suggest that indystonia there is a hypofunction of the reticular nucleusof the thalamus which, in turn, could determine the over-flow of the lemniscal pathway. On the other hand, tha-lamic abnormalities would not explain the impaired in-hibition of SEPs at the spinal level. Spinal abnormalitiescan be due to the influence exerted by the basal ganglialoop on spinal interneurons responsible for the N13 com-ponent via the peduncolopontine nucleus and the reticu-lar formation.55 In contrast, the normal P14 would beconsistent with the lack of functional interactions be-tween the posterior column nuclei and the basal gan-glia.55
In conclusion, though our data did not permit us toestablish whether the abnormal central processing of so-matosensory inputs is causally involved with the devel-opment of dystonia, they do suggest that motor distur-
E. FRASSON ET AL.680
Movement Disorders, Vol. 16, No. 4, 2001

bances in this disease might at least partially depend onintegration of abnormal excessive afferent inputs intoabnormal motor outputs.
Acknowledgments:This research was supported by grantsfrom the Centro di Riabilitazione Polifunzionale, Zevio, Ve-rona, Italy. We thank Mr. D. Volpato for technical assistance,Dr. T. Pawelzik for assistance in editing the manuscript, andDr. M. Fiorio for aid in the statistical analysis of data.
REFERENCES
1. Alexander GE, Crutcher MD. Functional architecture of basal gan-glia circuits: neural substrates of parallel processing. Trends Neu-rosci 1990;13:266–271.
2. Marsden CD, Sheehy MP. Writer’s cramp. Trends Neurosci 1990;13:148–153.3.
3. Sheehy MP, Marsden CD. Writer’s cramp: a focal dystonia. Brain1982;105:461–480.
4. Berardelli A, Rothwell JC, Hallett M, Thompson PD, Manfredi M,Marsden CD. The pathophysiology of primary dystonia. Brain1998;121:1195–1212.
5. Hallett M. Is dystonia a sensory disorder? Ann Neurol 1995;38:139–140.
6. Grunewald RA, Yoneda Y, Shipman M, Sagar HJ. Idiopathic focaldystonia: a disorder of muscle spindle afferent processing? Brain1997;120:2179–2185.
7. Kaji R, Rothwell JC, Katayama M, et al. Tonic vibration reflex andmuscle afferent block in writer’s cramp. Ann Neurol 1995;38:155–162.
8. Leis AA, Dimitrijevic MR, Delapasse JS, Sharkey PC. Modifica-tion of cervical dystonia by selective sensory stimulation. J NeurolSci 1992;110:79–89.
9. Byl NN, Wilson F, Merzenich M. Sensory dysfunction associatedwith repetitive strain injuries of tendinitis and focal hand dystonia:a comparative study. JOSPT 1996;23:234–244.
10. Tinazzi M, Frasson E, Bertolasi L, Fiaschi A, Aglioti S. Temporaldiscrimination of somesthetic stimuli is impaired in dystonic pa-tients. Neuroreport 1999;10:1–4.
11. Tinazzi M, Priori A, Bertolasi L Frasson E, Mauguie`re F, FiaschiA. Abnormal central integration of a dual somatosensory input indystonia: evidence for a sensory overflow. Brain 2000;123:42–50.
12. Tempel LW, Perlmutter JS. Abnormal vibration-induced cerebralflow responses in idiopathic dystonia. Brain 1990;113:691–697.
13. Tempel LW, Perlmutter JS. Abnormal cortical responses in pa-tients with writer’s cramp. Neurology 1993;43:2252–2257.
14. Ceballos-Baumann AO, Passingham RE, Warner T , Playford ED,Marsen CD, Brooks DJ. Overactive prefrontal and underactivemotor cortical areas in idiopathic dystonia. Ann Neurol 1995;37:363–372.
15. Ceballos-Baumann AO, Sheean G, Passingham RE, Marsden CD,Brooks DJ. Botulinum toxin does not reverse the cortical dysfunc-tion associated with writer’s cramp. A PET study. Brain 1997;120:571–582.
16. Playford ED, Passingham RE, Marsden CD, Marsden CD, BrooksDJ. Increased activation of frontal areas during arm movement inidiopathic torsion dystonia. Mov Disord 1998;13:309–318.
17. Reilly JA, Hallett M, Cohen LG, Tarkka IM, Dang N. The N30component of somatosensory evoked potentials in patients withdystonia. Electroenceph Clin Neurophysiol 1992;84:243–247.
18. Kanovsky P, Streitova H, Dufek J, Rektor I. Lateralization of theP22/N30 component of somatosensory evoked potentials of themedian nerve in patients with cervical dystonia. Mov Disord 1997;12:553–560.
19. Kanovsky P, Streitova H, Dufek J, Znojil V, Daniel P, Rector P.Change in lateralization of the P22/N30 cortical component ofmedian nerve somatosensory evoked potentials in patients with
cervical dystonia after successful treatment with botulinum toxinA. Mov Disord 1998;13:108–117.
20. Kanovsky P, Streitova h, Dufek J, Znojil V, Daniel P, Rektor I.Lateralization of the P22/N30 precentral cortical component of themedian nerve somatosensory evoked potentials is different in pa-tients with a tonic or tremolous form of cervical dystonia. MovDisord 1999;14:642–651.
21. Mazzini L, Zaccala M, Balzarini C. Abnormalities of somatosen-sory evoked potentials in spasmodic torticollis. Mov Disord 1994;9:426–430.
22. Tinazzi M, Frasson E, Polo A, et al. Evidence for an abnormalcortical sensory processing in dystonia: selective enhancement oflower limb P37-N50 somatosensory evoked potential. Mov Disord1999;14:473–480.
23. Shagass C, Schwartz M. Recovery functions of somatosensoryperipheral nerve and cerebral evoked responses in man. Electro-encephal Clin Neurophysiol 1964;17:126–135.
24. Angel A. Cortical responses to paired stimuli applied peripherallyand at sites along the somatosensory pathway. J Physiol (Lond)1967;191:427–448.
25. Wiederholt WC. Recovery function of short latency components ofsurface and depth recorded somatosensory evoked potentials in thecat. Electroenceph Clin Neurophysiol 1978;45:259–267.
26. Lueders H, Lesser RP, Hahn J, Dinner DS, Klem G. Corticalsomatosensory evoked potentials in response to hand stimulation.J Neurosurg 1983;58:885–894.
27. Meyer-Hardting E, Wiederholt WC, Budnick B. Recovery functionof short-latency components of the human somatosensory evokedpotential. Arch Neurol 1983;40:290–293.
28. Kaji R, Sumner AJ. Bipolar recording of short latency evokedpotentials after median nerve stimulation. Neurology 1987;37:410–418.
29. Emori T, Yamada T, Seki Y, et al. Recovery functions of fastfrequency potentials in the initial negative wave of median SEP.Electroenceph Clin Neurophysiol 1991;78:116–123.
30. Saito T, Yamada T, Hasegawa A, et al. Recovery functions ofcommon peroneal, posterior tibial and sural nerve somatosensoryevoked potentials. Electroenceph Clin Neurophysiol 1992;85:337–344.
31. Romani A, Bergamaschi R, Versino M, Callieco R, Calabrese G,Cosi. Recovery functions of early cortical median nerve SSEPcomponents: normative data. Electroenceph Clin Neurophyisiol1995;96:475–478.
32. Araki A, Yamada T, Ito T, Urushibara N, Kohira R, Hsu SP, YehM. Dissociation between upper and lower neck N13 potentialsfollowing paired median nerve stimuli. Electroenceph Clin Neu-rophysiol 1997;104:68–73.
33. Eccles JC. Properties and functional organization of cells in theventrobasal complex of the thalamus. In: Purpura DP, Yahr MD,eds. The thalamus. New York: Columbia University Press; 1966:129–141.
34. Fahn S. Assessment of the primary dystonia. In: Munsat TL, ed.Quantification of the neurological deficit. Stoneham, MA: Butter-worths; 1989:241–270.
35. Desmedt JE, Cheron G. Prevertebral (oesophageal) recording ofsubcortical somatosensory evoked potentials in man: the spinalP13 component and the dual nature of the spinal generators. Elec-troenceph Clin Neurophysiol 1981;52:257–276.
36. Restuccia D, Mauguie`re F. The contribuiton of median nerve SEPsin functional assessment of the cervical spinal cord in syrinogo-myelia. Brain 1991;114:361–379.
37. Desmedt JE, Nguyen TH, Bourguet M. Bit-mapped color imagingof human evoked potentials with reference to the N20, P22, P27and N30 somatosensory components. Electroenceph Clin Neuro-physiol 1987;68:1–19.
38. Allison T, McCarthy G, Wood CC, Jones SJ. Potentials evoked inhuman and monkey cerebral cortex by stimulation of the mediannerve. A review of scalp and intracranial recordings. Brain 1991;114:2465–2503.
PAIRED STIMULATION SEPS IN DYSTONIA 681
Movement Disorders, Vol. 16, No. 4, 2001

39. Mauguie`re F, Desmedt JE, Courjon J. Astereognosis and dissoci-ated loss of frontal or parietal components of somatosensoryevoked potentials in hemispheric lesion: detailed correlations withclinical signs and computed tomographic scanning. Brain 1983;106:271–311.
40. Fuji M, Yamada T, Aihara M, Kokubun Y, Noguchi Y, MatsubaraM, Yeh MH.. The effects of stimulus rate upon median, ulnar andradial nerve somatosensory evoked potentials. Electroenceph ClinNeurophysiol 1994;92:518–526.
41. Byl NN, Merzenich M, Wilson WM. A primate genesis model offocal dystonia and repetitive strain injury: Learning-induced de-differentiation of the representation of the hand in the primarysomatosensory cortex in adult monkeys. Neurology 1996;47:508–520.
42. Elbert T, Candia V, Altenmuller E, et al. Alteration of digitalrepresentations in somatosensory cortex in focal hand dystonia.Neuroreport 1998;9:3571–3575.
43. Mountcastle VB. Neural mechanisms in somesthesis. In: Mount-castle VB, ed. Medical physiology. St. Louis: CV Mosby; 1980:348–390.
44. Porter R, Lemon R. Corticospinal function and voluntary move-ment. Oxford: Oxford University Press; 1993.
45. Rothwell JC. Control of voluntary movement. London: Chapmann& Hall; 1994.
46. Bertolasi L, Priori A, Tinazzi M, Bertasi V, Rothwell JC. Inhibi-tory action of forearm flexor muscle afferents on corticospinaloutputs to antagonist muscles in man. J Physiol 1998;511:947–956.
47. Hikosaka O, Tanaka M, Sakamoto M, Iwamura Y. Deficits in
manipulative behaviors induced by local injections of muscimol inthe first somatsensory cortex of the conscious monkey. Brain Res1985;325:375–380.
48. Alloway KD, Burton H. Differential effects of GABA and bicu-culline on rapidly- and slowly -adapting neurons in the primarysomatosensory cortex of primates. Exp Brain Res 1991;85:598–610.
49. Odergren T, Iwasaki N, Borg J, Forssberg H. Impaired sensory-motor integration during grasping in writer’s cramp. Brain 1996;119:569–583.
50. Kanda F, Jinnai k, Takahashi H, Abe H, Yasuda M, Tada K, FujitaT. Somatosensory evoked potentials in Huntington’s disease—Studies with paired stimulation. Electromyogr Clin Neurophysiol1989;29:287–291.
51. Nakashima K, Nitta T, Takahashi K. Recovery functions of so-matosensory evoked potentials in parkinsonian patients. J NeurolSci 1992;108:24–31.
52. Block F, Schwartz M, Sontag KH. Non-NMDA mediated trans-mission of somatosensory evoked potentials in the rat thalamus.Brain Res Bull 1992;31:449–454.
53. Ahsby P, Lang AE, Lozano AM, Dostrovsky JO. Motor effect ofstimulating the human cerebellar thalamus. J Physiol 1995;489:287–298.
54. Lidsky TI, Manetto C, Schneider JS. A consideration of sensoryfactors involved in motor functions of the basal ganglia. Brain ResRev 1985;9:133–146.
55. Parent A, Cicchetti F. The current model of basal ganglia organi-sation under scrutiny. Mov Disord 1998;13:199–202.
E. FRASSON ET AL.682
Movement Disorders, Vol. 16, No. 4, 2001