Embed Size (px)
Citation preview

32
© 2003 Diabetes UK.
Diabetic Medicine
,
21
, 32–38
DOI: 10.1046/j.1464–5491.2003.01063.x
Introduction
The increasing prevalence of diabetes highlights the urgency ofensuring that appropriate services are accessible to the patients
who need them. This has led, in both affluent and less developedcountries, to examination of ways in which services could bereconfigured, frequently with an emphasis on the developmentof primary care services. In the UK, the concept of specialistgeneral practitioners (GPs) and clinics in primary care hasattracted increasing interest and support. Professionalswelcome it as a means of providing local services for patientsand developing specialist clinical interests [1,2]. Planners and
Correspondence to
: Professor John Wright, Department of Clinical Epidemiology and Public Health, Bradford Hospitals NHS Trust, Bradford BD9 6RJ, UK. E-mail: [email protected]
Abstract
Aims
The aim of this study was to evaluate an innovative approach to the provisionof primary care-based diabetes services in Bradford, UK. The service model differsfrom others in comprising 19 clinics which offer a specialist service, intermediatebetween primary and secondary care, to all patients within the Bradford area.
Methods
The study included: analysis of referral, attendance and register data;questionnaires to general practitioners (GPs) and specialist clinic providers;qualitative interviews with clinic and other professional staff and patients; andan economic analysis.
Results
The 19 clinics adopt a range of organizational models. In the first3
1
/
2
years, 2415 patients were referred. There was a significant reduction in out-patient attendances at hospital, but also a significant increase in overall patientattendances. Specialist clinic patients differed from hospital patients in being olderand having had diabetes for longer since diagnosis. Ten of the 14 clinics run bypractising GPs attracted more referrals from within their practices than fromoutside. GPs and patients across the city believed the clinics were valuable, themain benefits being geographical accessibility, availability of specialists in a com-munity setting, short waiting times for first appointments at most clinics, andcontinuity of staff. Their reservations included a lack of strategic planning inthe location of clinics, long waiting times at some clinics, and poor communica-tion at some clinics with referring GPs. The cost of the primary care clinics issimilar to hospital clinics.
Conclusions
This model of specialist primary care services offers an opportunityto develop diabetes services that are convenient to patients, popular with prac-titioners, and increase capacity. However, the shortcomings as well as the advant-ages of the model need to be addressed if it is to be implemented elsewhere orfor other patient groups.
Diabet. Med. 21, 32–38 (2004)
Keywords
specialist general practitioners, primary care, quality, hospital demand
Blackwell Publishing Ltd.Oxford, UKDMEDiabetic Medicine1464-5491Blackwell Science Ltd, 200320Original ArticleOriginal articleSpecialist GPs and diabetes clinics in primary care
A. Nocon et al.
Specialist general practitioners and diabetes clinics in primary care: a qualitative and descriptive evaluation
A. Nocon, P. J. Rhodes, J. P. Wright, J. Eastham*, D. R. R. Williams†, S. R. Harrison‡ and R. J. Young§
Department of Clinical Epidemiology and Public Health, Bradford Hospitals NHS Trust, Bradford, *Nuffield Institute for Health, University of Leeds, Leeds, †The Clinical School, University of Wales Swansea, Swansea, ‡Department of Applied Social Science, University of Manchester, Manchester, and §Department of Diabetes and Endocrinology, Salford Royal Hospitals NHS Trust, Salford, UK
Accepted 6 May 2003

Original article
33
© 2003 Diabetes UK.
Diabetic Medicine
,
21
, 32–38
politicians see the potential to reduce pressure on over-stretchedsecondary care and to meet increasing demand [3,4].
Well-organized primary care can be as effective as second-ary care in relation to follow-up and metabolic control, butstandards are variable [5,6]. It is essential that primary careshould meet the standards in the National Service Frameworkfor Diabetes, which include comprehensive, high-quality, par-ticipative and supportive care in managing diabetes (standard3) and regular surveillance for the long-term complications ofdiabetes (standard 10) [7,8].
There are a number of models of specialist diabetes serviceswithin primary care in the UK [4,9,10]. The development ofshared disease management, rather than the traditional demar-cation between primary and secondary care, provides modelsfor primary care involving specialist practitioners, team-working, and a graded system of responsibility based on existingexpertise, though clear role definition and avoidance of bothduplication and gaps in care are essential [9,11–13]. This studyreports on the evaluation of a service model which involves theprovision of secondary care services in a primary care settingby specialist primary care teams.
In Bradford, specialist diabetes clinics led by GPs with aspecial interest in diabetes were established in 1998 to alleviateincreasing waiting times for secondary care following theretirement of a hospital diabetologist and a delay in recruitinga successor. Health Action Zone status provided the resourcesto finance 19 clinics, with support from diabetes specialistnurses, part-time podiatrists and dieticians, and community-based retinal screening cameras. The clinics serve three Pri-mary Care Trusts (PCTs) with a population of 380 000, 32%of whom are registered with practices that have specialist clin-ics. Training initially consisted of a 2-day workshop for GPs;more frequent workshops were subsequently introduced, withsome sessions for GPs to discuss individual cases with consult-ants and others open to other healthcare professionals.
The clinics are for patients with: (i) insulin-treated diabetes—newly diagnosed; (ii) insulin-treated diabetes with poorcontrol (for stabilization); (iii) insulin-treated diabetes—forreview and follow-up; (iv) non-insulin-treated diabetes—for transfer to insulin and referral back to practice; (v) non-insulin-treated diabetes—receiving maximum oral therapy;HbA
1c
> 9% (for control).
Methods
The evaluation was carried out between 1999 and 2001 andused a range of sources. Data were extracted on referrals to andattendance at the specialist clinics (from a dedicated clinic data-base) and the hospital out-patient clinics (from the Trust’s PASdatabase). Characteristics of patients were obtained from theBradford diabetes register, containing data on 12 000 patientsreceiving care in primary and secondary care locations. Inter-views were conducted with 24 specialist clinic and other profes-sional staff to gain familiarity with clinics’ operation and staff’sviews. A detailed questionnaire was sent to the 19 specialistclinic providers to obtain information about staffing, clinic
operation, relationships with other GPs and with the hospital,the benefits of the clinics, and problems that still needed to beaddressed. A separate questionnaire was sent to all (142) GPs out-side the specialist clinic practices about their referral practice,relationship with the clinics, and assessment of the clinics’advantages and shortcomings. This was followed by face-to-faceand telephone interviews with a sample of eight GPs (includingsix non-respondents to the questionnaire) and two practicenurses (nominated by GPs as responsible for diabetes clinics intheir practices), in order to examine the issues in more depth.Semistructured interviews were undertaken with 55 patients (intheir own homes, places of work, or the researchers’ offices) toexplore their experiences of diabetes and of health services:names were selected at random from the diabetes registerfollowing purposive sampling to include different age groups,ethnic origin and care locations, and 26 interviews were carriedout in South Asian languages. Economic analysis used datafrom the diabetes register, the clinics’ activity database, expend-iture data for service components and professional groups, andinformation from laboratory and pharmacy systems. Projectmanagement included a multidisciplinary steering group withservice user representation, a mixed service users’ advisory group,and an Asian women’s advisory group for participants who didnot speak English [14,15].
Semistructured tape-recorded interviews with patients werebased on closed questions and a detailed topic guide: these werenecessary in order to undertake comparable interviews in SouthAsian languages using bilingual interviewers. Interviews in Eng-lish were partially transcribed. Those with South Asian patientswere fully transcribed and translated by the interviewers.Coding and analysis were undertaken jointly by two membersof the research team using Text Detective software. Analysisfollowed a framework approach [16], based on themes bothpre-identified and emergent from the interviews. Themes werediscussed with service users at advisory group meetings.
Quantitative data were analysed using SPSS (SPSS Inc., Chicago,IL, USA), which generated descriptive statistics. Townsenddeprivation scores were calculated from postcode data [17].Changes in hospital attendances during three 1-year periods(1 year before introduction of specialist clinics, introductoryyear and second year) were analysed using one-way
ANOVA
.
Results
Clinic operation
Two of the specialist clinics were run by a community diabet-ologist (on a sessional basis on behalf of two GPs), one by adiabetes specialist nurse, three by a former GP (two later takenover by GPs working outside their own practices), and 13 byGPs in their own practices. The clinics ran from one to fourtimes a month and lasted around 3 h, with a target attendanceof eight patients per clinic. Clinical support was provided by thecommunity diabetologist. Diabetes specialist nurses attended13 of the 19 clinics regularly and two further clinics occasion-ally; in the remainder, practice nurses worked alongside GPs.The role of diabetes specialist nurses varied from workingalongside the GP to running the clinic with the practice nurse.

© 2003 Diabetes UK.
Diabetic Medicine
,
21
, 32–38
34
Specialist GPs and diabetes clinics in primary care •
A. Nocon
et al.
Podiatrists and dieticians were available at approximatelyevery other session at 13 clinics, at other clinics less frequentlyor not at all. Team-working was variable, with some profes-sionals excluded from case discussions and service planning atsome clinics. Some clinics offered on-site eye testing, someoffered domiciliary visits, some employed interpreters.
Referrals and attendances
From April 1998 to September 2001, 2415 referrals weremade to the clinics, of which 42% were internal referrals fromGPs within the clinic practices. Of the remaining 58%, halfwere to the 13 specialist GPs based in their own practices andhalf to the other six clinics run by non-GPs or, more recently,to GPs based outside their own practices, all of which were ininner-city locations with high demand. Only four of the clinicsled by GPs in their own practices received more external thaninternal referrals.
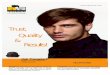
As at August 2001, 2067 patients were attending the clinics(17% of all patients on the diabetes register), 1746 attendedthe hospital (14%), and 8359 received care from their GPor mini-clinic (69%). Figure 1 shows the trends of hospitaland primary care clinic attendances. Mean monthly hospitalattendance fell from 478.5 in the year preceding specialistclinics (1997/1998), to 396.8 in the introductory year and 361.6in the second year (1999/2000), a 25% reduction (
F
= 13.0,
P
< 0.0001). There was no significant fall in numbers of newreferrals to or new attendances at the hospital. The mean monthlynumber of attendances in hospital and specialist clinicscombined was 648.1 by 1999/2000, an increase of 35% (169.6;95% confidence interval 109.5, 229.6) from 1997/1998.
Recorded attendance at the clinics has varied between twoand 20 patients, with some clinics consistently running at lowor high levels of activity. Three clinics (initially run by theformer GP, in inner-city areas with high minority ethnic
populations) had developed waiting lists for first appointments,reflecting the hospital situation that the clinics were set upto address—in the 2 years from October 1999, 16% of allnew hospital patients waited > 12 weeks for an out-patientappointment. Overall, non-attendance rates in 2000 at thespecialist clinics stood at 25%, with a range of 12–37% atdifferent clinics: higher non-attendance rates were recorded atinner-city clinics with high minority ethnic populations. Thetotal number of attendances at the clinics was 3809. Non-attendance at the hospital out-patient department was 19%during the same period, with 2405 actual attendances, eventhough hospital follow-up procedures were more limited thanthose at the clinics.
Register data
Table 1 provides information on the characteristics of thepatients attending the specialist clinics and hospital service.Specialist clinics provide access to a higher proportion ofpatients from non-white ethnic minorities. This difference isstatistically significant [
χ
2
= 12.7,
P
< 0.0001)]. There was nosignificant difference in the Townsend deprivation scores ofspecialist clinic and hospital patients.
We were unable to use the register data to evaluate eitherprocess or biomedical outcomes for patients attending thespecialist clinics, as problems with incomplete data entry andinconsistencies in practice information led to major concernsover their accuracy, while over-writing of information made itimpossible to track patients who moved between different carelocations. Clinic providers did, however, extract data for2000 from individual practice databases, which were thenaggregated by PCT. According to these, HbA
1c
was measuredfor 99–100% (depending on PCT) of patients attending thespecialist clinics, blood pressure for 99–100%, cholesterol86–99%, foot examination 78–79%, and retinal screening
Figure 1 Trends in patient attendances at hospital and specialist primary care clinics.

Original article
35
© 2003 Diabetes UK.
Diabetic Medicine
,
21
, 32–38
68–73%. Within the first 3 years of operation, over 700patients attending the clinics were started on insulin therapywithin the community.
GPs’ views
Of 85 GPs outside the clinics who completed the questionnaire(60% response rate), 84% had made referrals to the clinics.
Reasons for not referring included: patients’ preference forhospital (17 respondents), unknown quality of care (11), lackof transport (8), inconvenient locations for patients (6), andlack of confidence in the skills of specialist clinic staff (4). OnePCT restricted referrals to clinics within the trust, even thoughpatients might live nearer to clinics outside the PCT boundary.
Most (84%) GPs who responded (including 97% of thosewho had made referrals) stated, in response to a closed ques-tion, that the clinics were providing a valuable service, 4%disagreed, and the remainder gave no opinion. In response to anopen-ended question, they cited a range of benefits and criti-cisms (Box 1). These were corroborated in the interviews. FiveGPs selected a specialist clinic in the belief that the clinic wouldnot ‘poach’ patients: the fear that patients would register withthe clinic practice was cited in other interviews as a concern forGPs. The potential for GP deskilling was raised by both spe-cialist GPs and diabetic specialist nurses, who expressed con-cern about the inappropriate referral of patients who did notneed specialist care. Lack of back-up from, or integration with,secondary care was mentioned by some GPs and in discussionswith other professionals. There was also some concern aboutlack of clarity about the respective roles of referring GPs andspecialist clinics, which meant that duplication and omissionscould occur. For example, responsibility for managing associ-ated factors (such as hypertension or cholesterol) was not setout in advance. It is important to note that most GPs’ viewswere based on their contacts with their nearest specialistclinics, rather than the full range of clinics.
Patients’ views
Twenty-four of the interviews with service users were withpatients attending the specialist clinics. The majority spokepositively about the clinics, often comparing them favourablywith their experiences of hospital care; their evaluation
Table 1 Characteristics of patients
Specialist clinics Hospital clinic
Patients (n)Type 1 203 440Type 2 1757 1250
Age (years)Type 1 median 35 31IQR (Q1–Q3)* 28–45 17–43Type 2 median 64 63IQR (Q1–Q3) 53–72 52–71
Age at onset (years)Type 1 median 18 14IQR (Q1–Q3) 11–25 9–23Type 2 median 53 49IQR (Q1–Q3) 44–62 40–59
Duration (years)Type 1 median 18 13IQR (Q1–Q3) 9–29 6–25Type 2 median 8 10IQR (Q1–Q3) 4–13 5–17
Ethnicity (Types 1 and 2)Percentage of patients: White 56.0% 61.9%
Non-white 44.0% 38.1%
*IQR, Interquartile range expressed in terms of the values Q1 (first quartile, or 25th percentile) and Q3 (third quartile, or 75th percentile).
Box 1 General practitioners’ views of specialist clinies
AdvantagesI Geographical convenience for patientsII Access to specialists in a community settingIII Short waiting times for first appointmentsIV Continuity of and familiarity with staffV Sufficient time for patients in appointmentsVI The availability of diabetes specialist nursesVII A range of services on the same siteVIII Improved diabetic control, compared with standard GP careIX Better communication with GPs, compared with hospital
CriticismsI Lack of planning in location of clinicsII Long waiting times for first appointments (for three clinics)III Poor communication with referring GPsIV Lack of information provided about the clinicsV Concerns about the quality of care from specialist GPs (both general concerns and in relation to individual patients)VI Confusion over clinics’ and referring GPs’ responsibilities for patient careVII Concern about the potential for ‘poaching’ of patientsVIII Concern over the potential for atrophy of relevant clinical skills in non-specialist GPs

© 2003 Diabetes UK.
Diabetic Medicine
,
21
, 32–38
36
Specialist GPs and diabetes clinics in primary care •
A. Nocon
et al.
overlaps considerably with GPs’ own comments (Box 2). Somepatients nonetheless expressed criticisms of the clinics, withthree people highlighting, variously, a long waiting time andshort consultation at the clinic, the quality of care provided,and lack of cover by specialist clinic staff other than diabetesspecialist nurses outside clinic times.
Few patients who did not attend a specialist clinic had heardabout them. Where patients had been offered a choice of carelocation, they were most willing to attend a specialist clinic ifit was run by their own GP or within the same practice. Ifattendance at a specialist clinic meant going to another prac-tice, some patients preferred to remain with their own GP. Ofthose who had attended hospital, some had been willing tomove, especially if their condition was stable and they had lim-ited time to attend hospital appointments.
Economic evaluation
Costings were based on a range of actual and apportionedexpenditures for both the specialist and hospital out-patientclinics. Information on resource use by types of input and set-ting was derived from the diabetes register, a separate databaseset up to record the work of the specialist clinics, actual expen-ditures on service components and staffing, and informationfrom laboratory and pharmacy systems. As the primary focusof this part of the evaluation was on estimating the resourceconsequences of any new configuration of services on localhealthcare budgets, the work reported here adopts a purelyNational Health Service perspective and focuses on the costs ofambulatory management. Given that patients at the specialistclinics would otherwise have been referred to hospital, ratherthan being seen by non-specialist GPs, we did not calculate thecosts of being seen by the latter. Additional secondary carecosts related to the management of patients in each of thesettings were not included at this stage.
The average cost per patient attendance at the specialist clin-ics in 2000 was £165, with a range of £111–239 at individualclinics. This includes medical, general nursing, diabetes spe-cialist nursing, dietetic and podiatric inputs, consultant sup-port, drugs and pharmacy costs, diagnostic testing and other
laboratory expenses. Administrative and clerical supportcosts are included within sessional fees to clinics. The cost perpatient attendance at the hospital diabetes and endocrinologyout-patient clinics during the same period, and for a compara-ble range of inputs, was £123 with allocated Trust high-leveloverheads included and £86 without. Cost per patient attend-ance at consultant-led hospital clinics was £194 and £136(with and without Trust overheads, respectively). Althoughthere is overlap in case-mix between the two settings, the hos-pital department is likely to include a higher proportion ofpatients with complications or with diabetes that is moredifficult to control.
Table 2 shows the distribution of costs by category. By farthe single most important component in the overall cost ofmanaging patients in either the hospital or specialist clinicswas staffing. Medical and nurse staffing accounted for a simi-lar proportion of the total costs of providing the service in bothsettings: 59% and 65%, respectively. The relative difference inpodiatry costs in part reflected a recognized supply constrainton the provision of a community-based service. For ‘othercosts’, a major contributory factor to the relative differencewas the cost of HbA
1c
testing, which was significantly moreexpensive in the community setting than through the central-ized pathology service. The variation in average total costsacross the individual specialist clinics was largely due to differ-ences in the organization and scale of service delivery in theseclinics, particularly overall attendance levels and non-attendance
Box 2 Patients’ views of specialist clinics
AdvantagesI More frequent and more convenient appointmentsII Shorter waiting timesIII Clinics nearer to people’s homesIV Easier parkingV A more friendly and personal service
CriticismsVI Inconvenience of having to make a separate appointment with an optician for an eye examinationVII No facility for contact with a consultant diabetologist on a regular basisVIII Lack of cover outside clinics, other than through the diabetes specialist nursesIX Telephone calls to the diabetes specialist nurses being met by an answering machine and messages not passed onX Lack of transport meant that some people had difficulties attending the clinicsXI Criticisms of the quality of care
Table 2 Distribution of total costs by category*
Specialist clinics, % Hospital clinic, %
Medical and nurse staffing 42 42Diabetes specialist nurses 23 17Dietician services 9 6Podiatry services 7 19Eye screening 4 6Other costs† 15 10
*Based on totals which exclude high-level overhead charges.†‘Other costs’ primarily comprise pharmacy and pathology costs.

Original article
37
© 2003 Diabetes UK.
Diabetic Medicine
,
21
, 32–38
rates. Although a more appropriate basis for the comparisonof cost would have been in relation to patient-based outcomesrather than the number of patients seen, problems with dataquality prevented this.
Discussion
Most GPs outside the clinics believe the clinics are providinga valuable and popular service, a view that is shared by thepatients who attend them. The clinics offer a local service andenable a shift of responsibility from secondary to primary care.Although there was a reduction in hospital out-patient activityof 25%, the total number of hospital and specialist clinicattendances increased by 35% by the second year of theservice. This may reflect a greater awareness of diabeteson the part of both patients and practitioners and the higherprofile of diabetes locally. It may also reflect specialist clinicsbeing used inappropriately to review patients normally seenin routine general practice. In addition, the finding that 42%of referrals were internal practice referrals raises a questionabout equity of access for patients across the city.
Healthcare quality can be evaluated along six dimensions:accessibility, equity, acceptability, efficiency, appropriatenessand effectiveness [18]. Our evaluation gathered qualitativeand descriptive data on the first four. Although the specialistclinics appear to be popular with both service users and pro-fessionals, we need to be wary of an over-reliance on satisfac-tion levels [19]. It is not enough for people to like and besatisfied with a service: effectiveness and appropriateness alsoneed to be demonstrated. We were unable to compare clinicaloutcomes between clinics, standard primary care and hospitalbecause of systematic flaws in the diabetes register. Even if thishad been possible, attribution would have been difficult. Inaddition, the heterogeneity of the clinics would make com-parison of combined outcomes of limited value. We were alsounable to assess the appropriateness of referrals to the clinics,although professionals who were interviewed expressed someconcern.
The specialist clinics presented a range of different modelsrather than a single uniform approach. GPs’ variable experiencesof the clinics may have been a reflection of this variability. The
specialist clinic providers’ group has recognized the need toensure uniformly high standards of care at all clinics and addi-tional training has been introduced, linked to re-accreditation.
The location of the clinics was based on GPs’ interest in dia-betes rather than a strategic response to need. The proportionof minority ethnic patients from inner city wards is higher atthe clinics than among hospital attendees; however, not allareas of the city with high-density minority ethnic populationshave convenient access to clinics.
The economic evaluation highlights difficulties in relation tooverheads, the range of costs for individual specialist clinics,and, crucially, outcomes for patients. The overall finding,nonetheless, is that there is no noticeable difference in the costof the specialist and hospital out-patient clinics, even thoughthe sessional payments to GPs are considerably higher than the£160–200 national norm for GPs with special interests [20].The average cost of the specialist clinics could be reduced byaddressing the lower attendance rates at some clinics.
In conclusion, the clinics represent an important and inno-vative extension of traditional primary care for patients withdiabetes. They go further than many current examples of spe-cialization within primary care, in that secondary care tasksare taken on not by one or a few interested individuals, butacross a large number of practices serving three PCTs. TheBradford approach does have a unique history and fundingsource, which resulted in a unique response. The key com-ponents of the model can, nonetheless, be applied to othersettings, provided that its shortcomings are recognized andaddressed.
We do not suggest that the Bradford approach is the onlymeans of improving the quality of primary care diabetes ser-vices. An alternative is to raise standards throughout primarycare [13,21], rather than relying on islands of specialist exper-tise. Such an approach also involves costs, often considerable,if GPs are to take on responsibilities they would previouslyhave passed to secondary care, as well as the additional train-ing required. There is also a danger that a focus on one specia-lism, underpinned by financial incentives, could lead to adecreased emphasis on other areas of healthcare. Such a dan-ger is at least reduced in Bradford, where PCTs commission awide range of specialist primary care services [22,23].
Box 3 Conclusions from the evaluation
I The need for strategic planning, to ensure equity of accessII Effective capacity planning, to avoid both under-utilization and the saturation of clinic lists through appointments
for routine monitoring, while ensuring that patients needing more intensive longer-term support can receive itIII The need for agreed quality standards and protocolsIV Audit mechanisms to monitor the appropriateness of patients attending clinicsV Clarity about shared responsibility with referring GPsVI Adequate funding to ensure consistent provision of relevant staffVII Multidisciplinary team-working, in both sharing information and making decisionsVIII Multidisciplinary representation, including primary and secondary care, at policy and planning forumsIX An integrated system of patient care, with direct referral pathways and single overall clinical co-ordination of hospital
and community-based specialist clinicsX The need for reliable register data for monitoring performance and outcomes [8]

© 2003 Diabetes UK.
Diabetic Medicine
,
21
, 32–38
38
Specialist GPs and diabetes clinics in primary care •
A. Nocon
et al.
This evaluation has, nevertheless, highlighted a number oflessons that can be learned from the Bradford experience andseveral key points that need to be addressed when developingspecialist primary care services elsewhere. Issues arising directlyfrom the data are highlighted in Box 3. Two additional issuesthat require consideration emerged from this study. First, theclarification about the role of specialist clinics: whether theseshould carry out a tightly defined set of tasks, provide a screen-ing service for secondary care, and/or act as local centres ofexcellence, offering advice and support to other primary carepractices. Second, the recognition of the opportunity costs ofGPs running specialist clinics, and of the implications for otherGPs and practice staff.
Acknowledgements
This evaluation was funded by Diabetes UK under grantnumber BDA:RD99/0001833.
References
1 Pringle M.
Implementing a Scheme for General Practitioners withSpecial Clinical Interests.
London: Royal College of General Practi-tioners, 2001.
2 Department of Health.
The NHS Plan.
Cm 4818. London: Depart-ment of Health, 2000.
3 Department of Health.
Shifting the Balance of Power Within theNHS: Securing Delivery.
London: Department of Health, 2001.4 Audit Commission.
Testing Times: a Review of Diabetes Services inEngland and Wales.
London: Audit Commission, 2000.5 Griffin S. Diabetes care in general practice: meta-analysis of ran-
domised control trials.
Br Med J
1998;
317
: 390–396.6 Khunti K, Ganguli S, Lowy A. Inequalities in provision of systematic
care for patients with diabetes.
Fam Pract
2001;
18
: 27–32.7 Department of Health.
National Service Framework for Diabetes:Standards.
London: Department of Health, 2001.
8 Department of Health.
National Service Framework for Diabetes:Delivery Strategy.
London: Department of Health, 2002.9 Greenhalgh PM.
Shared Care for Diabetes: a Systematic Review.
Occasional paper 67. London: Royal College of General Practitioners,1994.
10 Whitford DL, Roberts SH. Sustainability of organised care in aDistrict.
Diabet Med
2002;
2
(Suppl.): A100.11 Vrijhoef HJM, Spreeuwenberg C, Eijkelberg IMJG, Wolffenbuttel BHR,
van Merode GG. Adoption of disease management model for dia-betes in region of Maastricht.
Br Med J
2001;
323
: 983–985.12 Eijkelberg IMJG, Spreeuwenberg C, Mur-Veeman IM, Wolffenbuttel
BHR. From shared care to disease management: key influencingfactors.
Int J Integrated Care
2001;
1
: 2. http://www.roquade.nl /IntegratedCare
13 Audit Commission.
http://www.diabetes.audit-commission.gov.uk/casestudies/
Accessed 2002.14 Rhodes P, Nocon A, Booth M, Chowdrey M, Fabian A, Lambert N
et al.
A service users’ research advisory group from the perspectivesof both service users and researchers.
Health Soc Care Community
2002;
10
: 402–409.15 Rhodes P, Nocon A, Darr A. A research advisory group for South
Asian women with diabetes who do not speak English.
Consumers inNHS Research News
2002; Summer: 4.16 Ritchie J, Spencer L. Qualitative data analysis for applied policy
research. In Bryman A, Burgess RG, eds.
Analysing Qualitative Data.
London: Routledge, 1994; 173–194.17 Townsend P, Phillimore P, Beattie A.
Health and Deprivation.
London:Croom-Helm, 1988.
18 Maxwell R. Quality assessment in health.
Br Med J
1984;
288
:1470–1472.
19 Williams B. Patient satisfaction: a valid concept?
Soc Sci Med
1994;
38
: 509–16.20 Sanderson D.
Evaluation of the GPs with Special Interests (GPwSIs)Pilot Projects within the Action On ENT Programme.
York: YorkHealth Economics Consortium, 2002.
21 Whitford DL, Southern AJ, Braid E, Roberts SH. Comprehensivediabetes care in North Tyneside.
Diabet Med
1995;
12
: 691–695.
22 Hill L, Rutter I. Cut to the quick.
HSJ
2001;
111
: 24–25.23 McLellan A. Smooth operators.
HSJ
2002;
112
: 16.