Embed Size (px)
Citation preview

0270-9139/88/0801-0171$02.00/0 HEPATOLOGY Copyright 0 1988 by the American Association for the Study of Liver Diseases
Vol. 8, No. 1, pp. 171-175, 1988 Printed in U. S. A.
Spontaneous Bacterial Peritonitis: An Explosion of Information
The paper by Tito et al. ( l ) , in this issue of Hepatology, is the latest in a fine series of publications on sponta- neous bacterial peritonitis (SBP) from the Barcelona group. We have witnessed in the 1980’s an explosion of information regarding spontaneous bacterial peritonitis, which was a medical curiosity in the early 1970’s. Per- haps because of reluctance to perform a paracentesis (caused by fear of complications) and also because of the subtle manifestations of this infection, many physicians “never saw a case” and did not believe that it existed. However, since paracentesis has been shown to be a safe procedure (2), admission paracentesis is being performed routinely at many liver units. Routine paracentesis has documented a 10 to 27% prevalence of SBP (or one of its variants) at the time of hospital admission of patients with ascites (3-5). At the 46 bed Liver Unit where I practice, SBP is diagnosed as many as three times a day and at least once a week! This infection is now recognized as a very common complication of severe liver disease.
Some skeptics are of the opinion that paracentesis causes rather than detects a significant proportion of ascitic fluid infections. However, in our experience, in- fection is caused by paracentesis only when the paracen- tesis needle enters the bowel (2, 6). Fortunately, this is a rare occurrence-10 “needle perforations” were docu- mented among 1,578 taps in a retrospective study (6) and one iatrogenic peritonitis occurred among more than 800 taps in a prospective study (Runyon, B. A., unpub- lished observations). None of these needle perforations have resulted in a death, and only 2 of the 11 have resulted in clinical peritonitis.
Should cirrhotics with coagulopathy receive prophy- lactic transfusion of fresh frozen plasma or platelets prior to paracentesis? At the USC Liver Unit, our answer is an emphatic “no.” We perform over 1,000 abdominal paracenteses per year. No one at our unit can remember ever giving or recommending prophylactic transfusions for this purpose in over 38 years of practice. The risk of bleeding from a paracentesis has been shown to be 1% (2). Prophylactic transfusions are unlikely to reduce this risk further. The risk is so low that it would take an enormous study to demonstrate the benefit of transfu- sion or to achieve an acceptable Type I1 error. Such a study will probably never be done. The risk of posttrans- fusion hepatitis exceeds the risk of bleeding from the paracentesis needle puncture. If the needle enters an artery or high pressure abdominal wall collateral vein,
Address reprint requests to: Bruce A. Runyon, M.D., USC Liver Unit, Building 500, Room 114, Rancho Los Amigos Medical Center, 7601 East Imperial Highway, Downey, California 90242.
hemorrhage is likely to occur regardless of coagulopathy. The midline is avascular and probably the best location for needle insertion (2). Cirrhotics who develop post- transfusion hepatitis frequently die of liver failure during their acute hepatitis event.
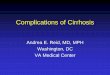
What has all this “tapping” of ascitic fluid resulted in? A large amount of information has been published about ascitic fluid infections in recent years (Figure 1). A review of our files with the assistance of a MEDLINE computer search revealed that 69 papers regarding SBP were pub- lished in the 1980’s (as of July, 1987), 21 in the 1970’s and only 1 in the 1960’s. Have we learned anything worthwhile from all of these publications? I believe the answer is a resounding yes. One of the most important pieces of information is the astounding prevalence of infected ascites at the time of admission to the hospital (vide supra). This may still be only the tip of the iceberg. These patients may be repeatedly developing coloniza- tion of their ascites with bacteria. However, only the patients whose colonizations are detected by fortuitous surveillance paracenteses or who undergo paracenteses because of signs or symptoms of peritonitis come to our attention. Many “spontaneous” colonizations probably “spontaneously” resolve without detection just as tran- sient bacteremias that follow mastication resolve without sequelae.
We have learned much about the pathogenesis of as- citic fluid infections. The mechanism of ascitic fluid infection due to gut rupture (e.g., perforated duodenal ulcer or colonic diverticulum) into ascites has never been a mystery. However, the pathogenesis of SBP has been elusive. These recent publications have brought us a growing body of evidence suggesting that SBP is the result of “spontaneous bacteremia” with seeding of “sus- ceptible” ascites (7). Patients with severe acute and/or chronic liver disease: (i) are frequently complement- deficient; (ii) may have serious defects in neutrophil function, and (iii) often have deficiencies in reticuloen- dothelial system function (8-11). These defects in host defense would be expected to result in frequent and prolonged bacteremia. In an animal model, it has been shown that rats with cirrhotic ascites inoculated intra- tracheally with pneumococci have more frequent bacte- remia, more prolonged antigenemia and higher mortality than normal rats and cirrhotic rats without ascites (12).
The unifying feature of the types of ascites that are susceptible to spontaneous infection (i.e., portal hyper- tension-related ascites and ascites associated with child- hood nephrotic syndrome) is low protein concentration (7). Ascites that is relatively resistant to SBP (i.e., ascites due to peritoneal carcinomatosis or heart failure or phys- iologic peritoneal fluid) usually has a high protein con-
171

172 RUNYON HEPATOLOGY
15-
v) Z Q 2 10- u 2 m 3 a
8 CL 5 -
3 w m
Z
I 1960 1970 1980 1907
FIG. 1. Numbers of publications regarding SBP over three decades (as of July, 1987).
centration (13, 14). The protein concentration of ascites does not change when it becomes spontaneously infected (15). The opsonic activity (endogenous antimicrobial activity) of ascites correlates closely with the protein concentration (16). Patients with low protein concentra- tion ascites and, more importantly, patients with defi- cient ascitic fluid opsonic activity have been shown to be unusually predisposed to SBP (3, 17). The pathogenesis of SBP thus probably involves bacteremia with seeding of opsonin-deficient ascites.
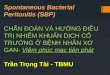
The recent literature on SBP has also focused atten- tion on the analysis of the ascitic fluid itself, including ascitic fluid cultures, cell counts and “chemistries.” Many have noted the insensitivity of the “conventional” culture technique in detecting bacterial growth in ascites (18). Because of dissatisfaction with routine cultures, some laboratories where large numbers of patients with SBP are seen (USC Liver Unit, West Haven VA and the Hijpital Albert-Chenevier in Crbteil, France) converted quietly to inoculation of blood culture bottles with ascites back in the mid-1970’s. Only Kammerer et al. (19) in Crbteil drew attention to their change in culture method. Because their study was published in French, few Eng- lish-speaking physicians are aware of the results, which demonstrated the superiority of the blood culture method. The original series of patients with SBP (which apparently identified cases by utilizing microbiology lab records) excluded cases that did not have positive cul- tures (20,21). Therefore, many physicians developed the impression, based on the uniformly culture-positive as- citic fluid of SBP patients in the literature, that all SBP patients had positive ascitic fluid cultures. We performed a chart review study that identified cases by discharge diagnosis rather than by microbiology department rec- ords; 35% of patients with neutrocytic ascites and sus- pected SBP were found to be culture-negative, using conventional culture methods (18). We chose to label this condition culture-negative neutrocytic ascites. A subsequent study over 2 years, comparing conventional culture results vs. blood culture bottle results in patients with neutrocytic ascites, yielded 42% vs. 91% culture- positivity [(22), Figure 21. Many physicians around the country have indicated that the majority of their cases are culture-negative. Probably the majority of cases of suspected SBP in the United States are in fact culture-
negative because of routine use of the conventional cul- ture method. The American Society for Microbiology [the organization that officially recommended the con- ventional method without evident validation studies (23)] should now officially recommend the blood culture bottle method. If the American Society for Microbiology were to promote use of this method: (i) laboratories would be more willing to convert to the improved method; (ii) the majority of cases of SBP in the United States would then be culture-positive, and (iii) physicians could then stop requesting the unnecessary tuberculosis and chlamydia cultures and the cytologies, scans and lapa- roscopies which are ordered when the ascitic fluid poly- morphonuclear (PMN) cell count is elevated but the conventional bacterial culture grows no bacteria!
Much has also been learned about the utility of the ascitic fluid cell count in the diagnosis of SBP. Eight studies have been published comparing the neutrophil (PMN) count to ascitic fluid pH and/or lactate in making a rapid presumptive diagnosis of SBP, using bacterial culture as the gold standard (24-31). The PMN count (with a cut-off of 250,450 or 500 cells per mm3) remains the single best test. In only four of these studies, however, was the use of blood culture bottles specifically men- tioned (26, 28-30). Only two mentioned bedside inocu- lation (26, 30). Since the median bacterial concentration in spontaneously infected ascites is only two organisms per ml (32), all of the bacteria could die en route to the laboratory; bedside inoculation is probably preferable to laboratory inoculation. Most of these studies of pH and/ or lactate were trying to validate “silver standards” using inadequate gold standards. The gold standard (i.e., the ascite fluid culture) must be optimized before other tests can be compared to it.
Another serious problem with the ascitic fluid pH is that it does not become abnormal until the ascitic fluid PMN count is already 2250 cells per mm3; therefore, this test has little impact on clinical decision making regarding use of empiric antibiotics. Physicians should proceed with antibiotic therapy if the PMN count is elevated, or if the patient has convincing signs or symp- toms of infection, regardless of the pH. In our experience with 79 episodes of SBP (or a variant thereof) in which
ASClTlC FLUID CULTURE TECHNIQUES
CONVFNTIONAL METHOD BLOOD CULTURE BOTTLE INOCULATION METHOD
P MI( ROB101 OGY LAB
:i
I - _._ - ~~~ - A __ ~
LCSL 1 I IAN I rnl FLUID IIJOCOL ATED TOTO IN TOTO
10 ml FLUID INOCULATED
91 % SENSITIVE 4: Y/, SENSITIVE FIG. 2. Diagrammatic representation of conventional ascitic fluid
culture method and blood culture bottle method.

Vol. 8, No. 1, 1988 SPONTANEOUS BACTERIAL PERITONITIS 173
ascitic fluid pH was performed, no treatment decisions were affected by this test. In our series, all 66 patients with a PMN count 2250 cells per mm3 (39 SBP, 17 culture-negative variant and 10 secondary peritonitis) received empiric antibiotics despite the fact that only 27 (41%) of these had an ascites pH less than 7.35 (Runyon, B. A., unpublished observations). One might hope that the ascitic fluid pH would be of value in making a presumptive diagnosis of monomicrobial bacterascites, i.e., ascitic fluid infection in which the ascitic fluid cul- ture is positive with PMN count less than 250 cells per mm3. However, 7 of 13 patients with monomicrobial bacterascites in our series received antibiotics because of symptoms or signs of infection; none of the 13 had an ascitic fluid PMN count greater than 250 or an ascitic fluid pH of less than 7.35 (Runyon, B. A., unpublished observations). Unfortunately, in patients with monomi- crobial bacterascites, the ascitic fluid pH (7.45 & 0.08) is not statistically significantly different from sterile non- neutrocytic controls (7.47 k 0.07) (p > 0.5). Since mon- omicrobial bacterascites has an ascitic fluid pH similar to sterile controls, and SBP ascites has a pH (7.34 & 0.16) that is lower than either monomicrobial bacteras- cites (p < 0.001) or sterile controls (p < 0.001), the PMNs themselves rather than the bacteria appear to alter the ascitic fluid pH. Culture-negative neutrocytic ascites, which has a significantly lower PMN count (1,380 f 1500 cells per mm3) than SBP (7,790 k 11,200 cells per mm3) (p < 0.001), also has an ascitic fluid pH (7.45 k 0.05) similar to sterile controls (p > 0.1) and similar to monomicrobial bacterascites (p > 0.5). There appears to be a threshold of concentration of PMNs in ascites below which the pH remains normal; only 3 of 93 specimens (including 27 culture-positive specimens) with a PMN count less than 2,000 cells per mm3 had a pH less than 7.35 (Runyon, B. A., unpublished observations). Therefore, the ascitic fluid pH appears to be an indirect measurement of the presence of PMNs, and large num- bers of PMNs must be present before the pH decreases. The cost of measurement of ascitic fluid pH is $30.00 in our hospital. Performing an arterial pH doubles this cost and does not add a significant amount of information in our experience. The patients’ money is probably better spent on the direct measurement of the PMN count, the $17.25 ascitic fluid cell count!
When should we think about secondary bacterial per- itonitis in a sick patient with neutrocytic ascites? We should always consider the possibility. The recent liter- ature of SBP provides us with some guidelines regarding which patients should undergo radiographic testing in the search for gut perforation or loculated pus (33-35). Unfortunately, physical findings do not help in the dif- ferential diagnosis. Patients with 10 to 20 liters of ascites never develop a rigid abdomen even with free perforation of the gut (33). It is the ascitic fluid analysis and the response of the PMN count and culture to treatment that: (i) help distinguish SBP from secondary peritonitis and (ii) help determine which patients should undergo radiographic testing (33-35). The ascitic fluid of a patient with SBP that is detected early in its course, usually has a total protein less than 1 gm per dl, glucose similar to the simultaneous serum value and lactate dehydrogenase
less than the upper limit of normal for serum, and the fluid grows a single organism (33). In contrast, the ascitic fluid of a patient with gut perforation into ascites usually grows multiple organisms (occasionally including fungi) and fulfills at least two of the following criteria: (i) protein greater than 1 gm per dl; (ii) glucose less than 50 mg per dl, and (iii) lactate dehydrogenase greater than the upper limit of normal for serum (33). After antibiotic therapy of SBP is started, the ascitic fluid rapidly be- comes sterile and the PMN count drops exponentially; whereas in secondary peritonitis (perforation or nonper- foration type), the culture remains positive and the PMN count usually rises despite therapy (35). Patients with ascites and peritonitis should be taken to the operating room only if there is convincing radiographic evidence of perforation (extravasation of water-soluble contrast) or loculated pus (e.g., perinephric abscess). The mortality of laparotomy in patients with SBP is 80% (36). Patients with secondary peritonitis can survive operative inter- vention (33). Free perforation of the gut into ascites does not respond to medical therapy alone.
Which antibiotic(s) should be used empirically in the treatment of a patient with neutrocytic ascites and sus- pected SBP? The older literature recommended ampicil- lin and gentamycin (37). However, this recommendation was not based on adequate efficacy data. Now we know that: (i) the volume of distribution of aminoglycosides is unpredictable in ascites patients; (ii) aminoglycosides are probably too nephrotoxic to be used in ascites pa- tients, and (iii) cefotaxime has been shown to be more efficacious and to have fewer side effects than the com- bination of ampicillin and aminoglycosides (38-41).
Unfortunately, not everyone has incorporated recent data on SBP into their clinical decision making. In a recent Case Record of the Massachusetts General Hos- pital, a patient with ascites was admitted repeatedly with abdominal pain, fever and encephalopathy, but a para- centesis was not discussed or performed (42). Perhaps the coagulopathy in this case was viewed as a contrain- dication to paracentesis. However, coagulopathy may be, in part, a manifestation of Gram-negative infection. In our opinion, a manifestation of infection should not prevent the performance of the procedure that could diagnose the infection. Cultures of blood grow bacteria in 54% of patients with SBP, but do not substitute for paracentesis with ascitic fluid culture (7). The Case Record patient was treated with multiple courses of antibiotics (including gentamycin). SBP was not men- tioned in the case discussion. The absence of fibrinous peritonitis at autopsy does not exclude the prior presence of SBP; only 19% of SBP patients show this (7). Despite all of the recent publications about SBP, some physicians continue to have a high threshold for performing a par- acentesis and a low index of suspicion of ascitic fluid infection. Some concepts in medicine change slowly.
What can we learn from the SBP paper published in this issue of Hepatology? The message is both encourag- ing and discouraging. The older literature of SBP re- ported essentially 100% mortality (20, 21). The mean weighted mortality (during the hospitalization in which SBP was diagnosed) has been calculated to be 78% (7). Tito et al. very humbly state that their mortality of 54%

174 RUNYON HEPATOLOGY
is “within the range” of other reports. Actually, they are reporting the best survival of a series of SBP patients of this size. As we diagnose SBP early in its course (before irreversible renal failure occurs) and treat with nonne- phrotoxic antibiotics, the survival would be expected to improve. In our controlled trial of cefotaxime treatment of SBP, which has enrolled 27 patients in 7 months, the hospitalization mortality has been only 30% (Runyon, B. A., unpublished observations). Therefore, the good news is that the mortality of SBP is declining. The bad news of the study by Tito et al. is that recurrence is very common (69% at 1 year) and frequently fatal (31%). The final message of the paper is a clear one-every effort should be made to prevent recurrent infection in patients who survive the first episode.
Low-protein ascites ( 5 1 gm per dl) was shown in this study to be associated with a particularly high rate of recurrence, just as it has been shown to be a good predictor of the first episode of SBP (3). Since diuresis has been shown to increase ascitic fluid protein concen- tration 2-fold and opsonic activity 10-fold, this form of treatment may help prevent recurrence (43). Oral non- absorbable antibiotics help prevent SBP in the setting of variceal hemorrhage (44). This method of prophylaxis should be studied in patients who survive an episode of SBP. Treatment of the underlying liver disease (e.g., abstinence in the alcoholic) may be of value. Finally, liver transplantation should be considered in the patient who is otherwise a candidate for transplantation and who has survived SBP. “History of SBP” should be factored into the complicated decision making that de- termines timing of transplant and prioritization of can- didates for transplant. However, before a patient with SBP can receive a transplant, (s)he must first survive SBP. To do so requires a high index of suspicion of ascitic fluid infection on the part of the attending phy- sician, a low threshold for performing a paracentesis, appropriate cultures, timely institution of nonnephro- toxic antibiotics and consideration of “nonspontaneous” causes of infection.
BRUCE A. RUNYON USC Liver Unit Ranchos Los Amigos Medical Center Downey, California 90242
REFERENCES
1. Tito L, Rimola A, Gines P, et al. Recurrence of spontaneous bacterial peritonitis in cirrhosis: frequency and predictive factors. Hepatology 1988; 827-31.
2. Runyon BA, Paracentesis of ascitic fluid a safe procedure. Arch Intern Med 1986,1462259-2261.
3. Runyon BA. Low-protein-concentration ascitic fluid is predisposed to spontaneous bacterial peritonitis. Gastroenterology 1986;
4. Almdal TP, Skinh0j P. Spontaneous bacterial peritonitis in cirrho- sis: incidence, diagnosis, and prognosis. Scand J Gastroenterol 1987; 22:295-300.
5. Pinzello G, Simonetti RG, Craxi A, et al. Spontaneous bacterial peritonitis: a prospective investigation in predominantly nonalco- holic cirrhotic patients. Hepatology 1983; 3545-549.
6. Runyon BA, Hoefs JC, Canawati HN. Polymicrobial bacterascites: a unique entity in the spectrum of infected ascitic fluid. Arch Intern Med 1986; 1462173-2175.
91:1343-1346.
7. Hoefs JC, Runyon BA. Spontaneous bacterial peritonitis. Disease- A-Month 1985; 31:l-48.
8. Fox RA, Dudley FS, Sherlock S. The serum concentrations of the third component of complement in liver disease. Gut 1971; 12:574- 578.
9. Kourilsky 0, LeRoy C, Peltier AP. Complement and liver cell function in 53 patients with liver disease. Am J Med 1973; 55783- 790.
10. Rajkovic IA, Williams R. Abnormalities of neutrophil phagocytosis, intracellular killing, and metabolic activity in alcoholic cirrhosis and hepatitis. Hepatology 1986; 6252-262.
11. Rimola A, Soto R, Bory F, et al. Reticuloendothelial system phag- ocytic activity in cirrhosis and its relation to bacterial infections and prognosis. Hepatology 1984; 453-58.
12. Mellencamp MA, Preheim LC. Effect of cirrhosis on bacteremia and capsular antigenemia during experimental pneumococcal pneumonia. Proceedings of the 26th Interscience Conference on Antimicrobial Agents and Chemotherapy (Abstract), 1986, p. 283.
13. Kurtz RC, Bronzo RL. Does spontaneous bacterial peritonitis occur in malignant ascites? Am J Gastroenterol 1982; 77:146-148.
14. Runyon BA. Spontaneous bacterial peritonitis associated with cardiac ascites. Am J Gastroenterol 1984; 79796.
15. Runyon BA, Hoefs JC. Ascitic fluid analysis before, during, and after spontaneous bacterial peritonitis. Hepatology 1985; 5:257- 259.
16. Runyon BA, Morrissey R, Hoefs JC, et al. Opsonic activity of human ascitic fluid a potentially important protective mechanism against spontaneous bacterial peritonitis. Hepatology 1985; 5634- 637.
17. Runyon BA. Patients with deficient ascitic fluid opsonic activity are predisposed to spontaneous bacterial peritonitis (Abstract). Hepatology 1986; 61139.
18. Runyon BA, Hoefs JC. Culture-negative neutrocytic ascites: a variant of spontaneous bacterial peritonitis. Hepatology 1984;
19. Kammerer J, Dupeyron C, Vuillemin N, et al. Apport des examens cytologiques et bacteriologiques du liquide d’ascite cirrhotique au diagnostic de peritonite bacterienne. Med Chir Dig 1982; 11:243- 251.
20. Conn HO, Fessel JM. Spontaneous bacterial peritonitis in cirrho- sis: variations on a theme. Medicine 1971; 50:161-197.
21. Correia JP, Conn HC. Spontaneous bacterial peritonitis in cirrho- sis: endemic or epidemic? Med Clin North Am 1975; 59963-981.
22. Runyon BA, Umland ET, Merlin T. Inoculation of blood culture bottles with ascitic fluid improved detection of spontaneous bac- terial peritonitis. Arch Intern Med 1987; 147:73-75.
23. Isenberg HD, Schoenknecht FD, Von Graevenitz A. Cumitech 9: Collection and Processing of Bacteriological Specimens, Rubin SJ (coordinating ed). Washington, D.C.: American Society for Micro-
41209-1211.
biology, 1979. 24. Brook I. Altman RS. Loebman WW. et al. Measurement of lactate
in ascitic fluid an aid in the diagnosis of peritonitis with particular relevance to spontaneous bacterial peritonitis of the cirrhotic. Dig Dis Sci 1981; 261089-1094.
25. Gitlin N, Stauffer JL, Silvestri RC. The pH of ascitic fluid in the diagnosis of spontaneous bacterial peritonitis in alcoholic cirrhosis. Hepatology 1982; 2:40&411.
26. Scemama-Clergue J, Doutrellot-Philippon C, Metreau J-M, et al. Ascitic fluid pH in alcoholic cirrhosis: a reevaluation of its use in the diagnosis of spontaneous bacterial peritonitis. Gut 1985;
27, Yang C-Y, Liaw Y-F, Chu C-M, et al. White count, pH and lactate in ascites in the diagnosis of spontaneous bacterial peritonitis. Hepatology 1985; 5%-90.
28. Garcia-Tsao G, Conn HO, Lerner E. The diagnosis of bacterial peritonitis: comparison of pH, lactate concentration and leukocyte count. Hepatology 1985; 591-96.
29. Pinzello G, Virdone R, Lajacono F, et al. Is the acidity of ascitic fluid a reliable index in making the presumptive diagnosis of spontaneous bacterial peritonitis. Hepatology 1986; 6:244-247.
30. Attali P, Turner K, Pelletier G, et al. pH of ascitic fluid diagnostic and prognostic value in cirrhotic and noncirrhotic patients. Gas- troenterology 1986; 901255-1260.
31. Stassen WN, McCullough AJ, Bacon BR, et al. Immediate diag- nostic criteria for bacterial infection of ascitic fluid evaluation of ascitic fluid polymorphonuclear leukocyte count, pH, and lactate
26332-335.

Vol. 8, No. 1, 1988 SPONTANEOUS BACTERIAL PERITONITIS 175
concentration, alone and in combination. Gastroenterology 1986;
32. Runyon BA, Canawati HN, Akriviadis EA. Optimization of ascitic fluid culture technique and explanation of the insensitivity of the conventional method (Abstract). Hepatology 1987; 7:1055.
33. Runyon BA, Hoefs JC. Ascitic fluid analysis in the differentiation of spontaneous bacterial peritonitis from gastrointestinal tract perforation into ascitic fluid. Hepatology 1984; 4:447-50.
34. Caralis PV, Sprung CL, Schiff ER. Secondary bacterial peritonitis in cirrhotic patients with ascites. South Med J 1984; 77:579-583.
35. Runyon BA, Hoefs JC. Spontaneous vs secondary bacterial peri- tonitis: differentiation by response of ascitic fluid neutrophil count to antimicrobial therapy. Arch Intern Med 1986; 1461563-1565.
36. Garrison RN, Cryer HM, Howard DA, et al. Clarification of risk factors for abdominal operations in patients with hepatic cirrhosis. Ann Surg 1984; 199648-655.
37. Weinstein MP, Iannini PB, Stratton CW, et al. Spontaneous bacterial peritonitis: a review of 28 cases with emphasis on im- proved survival and factors influencing prognosis. Am J Med 1978;
901247-1254.
64592-598.
38. Gill MA, Kern JW. Altered gentamicin distribution in ascitic patients. Am J Hosp Pharm 1979; 361704-1706.
39. Cabrera J, Arroyo V, Ballestra AM, et al. Aminoglycoside nephro- toxicity in cirrhosis: value of urinary P2-microglobulin to discrim- inate functional renal failure from acute tubular damage. Gastro- enterology 1982; 82:97-105.
40. Moore RD, Smith CR, Lietman PS. Increased risk of renal dys- function due to interaction of liver disease and aminoglycosides. Am J Med 1986; 80:1093-1097.
41. Felisart J, Rimola A, Arroyo V, et al. Cefotaxime is more effective than is ampicillin-tobramycin in cirrhotics with severe infections. Hepatology 1985; 5:457-462.
42. Case 45-1985. Case records of the Massachusetts General Hospital. N Engl J Med 1985; 3131210-1219.
43. Runyon BA, Van Epps DE. Diuresis of cirrhotic ascites increases its opsonic activity and may help prevent spontaneous bacterial peritonitis. Hepatology 1986; 6396-399.
44. Rimola A, Bory F, Teres J , et al. Oral, nonabsorbable antibiotics prevent infection in cirrhotics with gastrointestinal hemorrhage. Hepatology 1985; 5:463-467.