Embed Size (px)
Citation preview

ENCEPHALOS 51, 47-54, 2014
Summary
In this retrospective study we report four cases ofspontaneous cervical spine epidural hematomas(SCSEH) during last twelve years and review the rel-evant literature. The average age of our patients was56 years, all had various sensorimotor neurologicaldeficits, and two of them had certain predisposingfactors. T1 and T2 sequences of spinal MRI variedon clot characteristics, age, size, and oxygenation ofthe hematomas. In our series, all SCSEHs locatedposterolaterally, extending along three to eight verte-bral levels, and treated by wide laminectomy,hematoma removal, and cord decompression with orwithout vertebral stabilization. One case was con-firmed pathologically as hematoma due to bleedingfrom a true dural AVM. Three patients had gradually significant improve-
ment of the preoperative neurological status, but inone case there was no functionally useful improve-ment. Spontaneous epidural hematomas of the cervical
spine are uncommon neurosurgical entities which,because of their localization is important to promptlydiagnosed and treated appropriately, so that thisgroup of patients to be driven in as more favorableoperating results. Although the cause has not exactly been made
clear, most authors have reported that is the result ofanticoagulant and antiplatelet therapy, vascular mal-formations, venous epidural plexus defects, andinherited or acquired bleeding disorders. These hematomas should always be suspected in
patients with acute neck pain followed by neurologi-cal deficits or myelopathy in the presence of such
risk factors. The diagnostic procedure of choice isMRI, and standard treatment is urgent surgicaldecompression. The two main predictors of outcomeare surgery timing and preoperative neurological sta-tus. Though differential diagnosis of this clinical entity is
extensive, careful neurological examination com-bined with modern imaging techniques and earlyintervention allows patients with spontaneous cervi-cal epidural hematoma have a safe diagnosis, signif-icant neurologic improvement, and good outcome.
Keywords: Spontaneous epidural hematoma, cervi-cal spine, treatment
Introduction
Spontaneous epidural hematoma of the spine is anextremely rare but important cause of compressionof the spinal cord or cauda equina, which requiresincreased suspicion, prompt diagnosis, and appropri-ate treatment, otherwise it leads to permanent neuro-logical deficit or death. Since Jackson first describedthis unusual disease in 186911, 500 cases of patientshave been published worldwide. Although the etiolo-gy of spinal epidural hematomas is not completelyunderstood, most researchers implicate as the mostcommon etiologic factors anticoagulant andantiplatelet agents , vascular malformations , andcongenital or acquired coagulation disorders andblood dyscrasias2,3,9,19,21. Tsai27 named them asidiopathic spinal hematomas, when there is no iden-tifiable etiologic factor, and as spontaneous whenthere is no bone injury after minor trauma or afternormal daily activity.The usually applied therapeutic approach is the
earliest possible evacuation of the hematoma and
Spontaneous epidural hematomas of cervical spine.Report of our casesROVLIAS ARISTEDIS*, THEODOROPOULOS SPYRIDON**, PAPOUTSAKIS DIMITRIOS**, SIAKAVELLAMARIA**, GOULIOPOULOU KONSTANDINA**
* Director of Neurosurgical Department of Asclepeion General Hospital of Voula**Staff of the Neurosurgical Department

48
decompression of the spinal cord10,18. However,some researchers have reported that conservativetreatment is also an option in some selected cases14,26.Spontaneous spinal epidural hematomas can occur
at any level of spinal axis , although the most com-mon site is the thoracic area8,9. The purpose of thispaper is to present our experience in the treatment ofspontaneous epidural hematomas of the cervicalspine, and review the recent literature.
Material and method - Results
During the last twelve years, four patients withspontaneous epidural hematoma of the cervicalspine (Spontaneous Cervical Spine EpiduralHematoma, SCSEH), were treated surgically inNeurosurgical Clinic of Asklipeio Hospital of Voula.
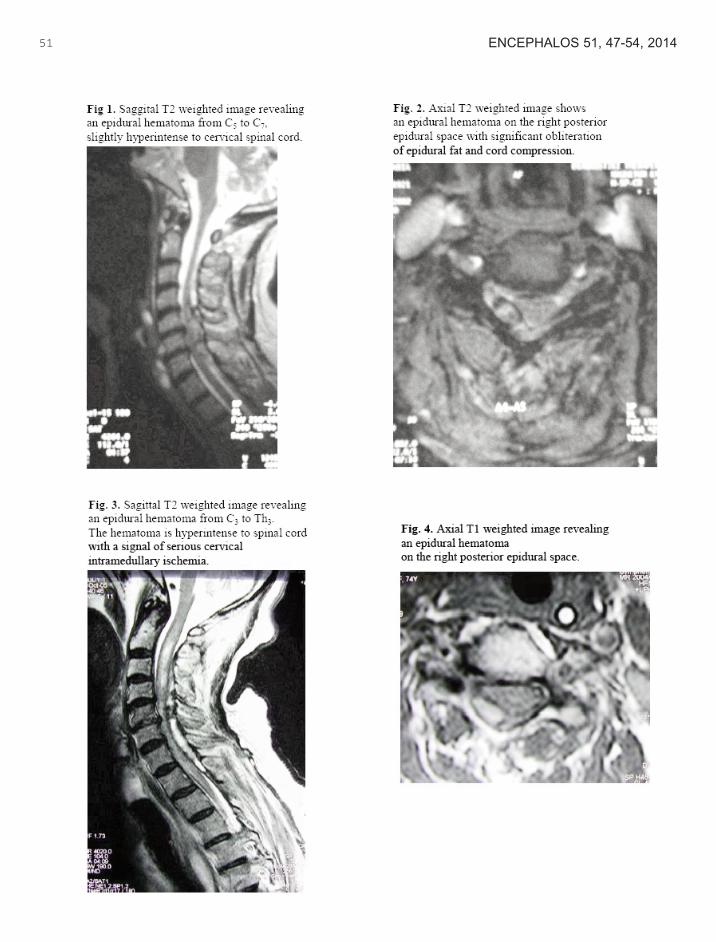
1st patient: A 80 years old woman with a history ofrheumatoid arthritis and hypertension since 20 yearsreceiving anticoagulation therapy (coumarin) due toatrial fibrillation, presented with sudden neck painand standing – walking weakness since 12 hours. Onneurological examination we found a normal level ofconsciousness with flaccid tetraparesis mainly right,without sensory or sphincter disorders. MagneticResonance Imaging (MRI) revealed a space - occu-pying lesion of the cervical spine from C5 to C7 withcharacteristics of an epidural hematoma (Fig. 1, 2).She immediately discontinued anticoagulation thera-py, received vitamin K, and after improvement of pro-thrombin time was subjected to C5, C6 laminectomyand total removal of the hematoma. The postopera-tive course was excellent with gradual neurologicalimprovement until almost complete recovery.
2nd patient: A 74 - year - old woman with a historyof coronary heart disease and arterial hypertensionreceiving antiplatelet therapy was hospitalized else-where because of sudden neck pain, headache, stiffneck, and right hemiparesis with a good level of con-sciousness. By the suspicion of a subarachnoid hem-orrhage she was subjected to computed tomographyof the brain and lumbar puncture that were normal. Adigital subtraction angiography of the brain was alsonegative for a cerebral aneurysm or other vascular
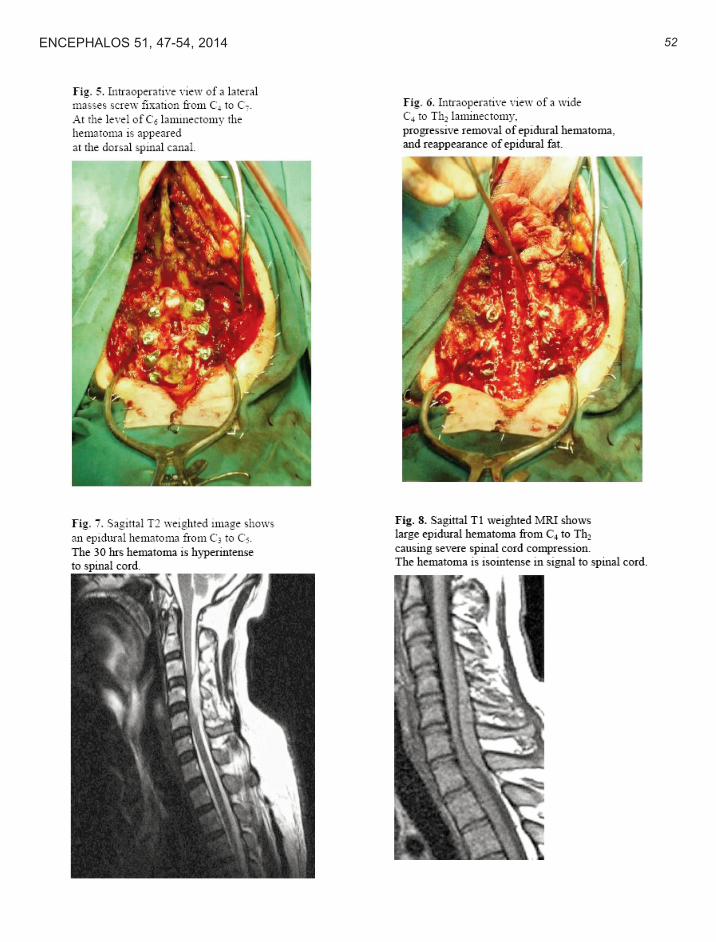
malformation. After 48 hours the patient showed dra-matic neurological deterioration with flaccid quadri-plegia and respiratory failure. She was taken undermechanical ventilation in the ICU and the next dayunderwent cervical spine MRI, which revealed anextensive epidural hematoma of cervicothoracicspine from C3 to T3 (Fig. 3, 4). She was transferredto our Neurosurgical Clinic and underwent an exten-sive laminectomy C4 - T2, total evacuation of thehematoma, and posterior lateral masses fusion of C4up to C7 (Fig. 5, 6). The postoperative course wasaccompanied by a slight improvement in musclestrength without significant functional equivalent, thepatient remained with a permanent tracheostomy,and transferred to the Physical Medicine andRehabilitation Clinic.
3rd patient: A 49 years old male without medicalhistory had a sudden neck pain with radiation to theback and shoulders since 30 hours and progressivelyworsening left hemiparesis with sphincter disorders.He underwent urgent MRI which revealed a freshepidural hematoma expanding from C3 to C5 verte-bra (Fig. 7). He was operated urgently and under-went laminectomy of C3, C4, and C5. With theremoval of the hematoma and washing of bloodclots, we found the cause of the hematoma, a smallarteriovenous malformation of the dura mater at theC4 level (dural arteriovenous fistula), which alsotreated by thermocoagulation with bipolar diathermyThe postoperative course was excellent with fullrecovery of the initial neurological deficits.
4th patient: A young man aged 21 years withoutmedical history or preceding injury was admittedbecause of intermittent headache and neck painsince twelve hours. Cranial computed tomographyscan was normal. During hospitalization he devel-oped a serious bilateral upper limb paresis, and uri-nary retention. MRI of the cervical spine showed anextensive epidural hematoma from C4 to T2 (Fig. 8,9). He underwent a C4 to T1 laminectomy, removalof the hematoma, and posterior cervicothoracicspinal fusion. The postoperative period was withoutcomplications, and after an intensive physiotherapyprogramme his muscle strength returned almost full(4/5).
ENCEPHLOS 51, 47-54, 2014

49
Discussion - Conclusion
SCSEH is a rare neurosurgical entity. Due to its crit-ical localization is very important to be diagnosedearly and treated adequately with the promisingprospect of permanent and non – reversible cervicalmyelopathy. These hematomas usually affectpatients between 50 - 80 years (mean age of ourgroup: 56 years), with a relative superiority of menover women (1.4 - 2:1)9.
The exact cause of these hematomas remainsunknown in the majority of patients and is probablymultifactorial. The most common risk factor is thecongenital or acquired hematological disorders,coagulation disorders, intravenous or oral anticoagu-lants, antiplatelet agents or subcutaneous adminis-tration of high doses of low molecular weightedheparin (used most widely , prophylactically or thera-peutically, in everyday present medical practice),hypertension, diabetes mellitus, pregnancy,preeclampsia, childbirth, thrombolysis, using ofcocaine, vasculitis, non - Hodgkins lymphoma, spinalhemangioma, and epidural vascular malformations3 ,4,9,13,19,20,23. Minor injuries of the cervical spine inpatients with ankylosing spondylitis have also beenimplicated as a predisposing factor22. In 40% ofcases the cause of SCSEH remains unknown6. Inour small series, two patients had a predisposing fac-tor such as hypertension and the use of anticoagu-lants and antiplatelet agents.
Beatty and Winston2 believe that the combinationof non-steroidal anti-inflammatory drugs (NSAID),anticoagulants, and chronic alcohol intake is verydangerous for development of a spontaneous epidur-al or subdural hematoma of the cervical spine fromthe rupture of small epidural arteries. Spontaneousspinal epidural hematoma is more often than subdur-al, because of plenty of blood vessels in the epiduralversus subdural space. Gundry and Heithoff12 sug-gest that an acute prolapsus of intervertebral disccan tear the fragile venous plexus of Batson and thisleads to epidural hemorrhage. Variations in intratho-racic or intra-abdominal pressure after intense phys-ical exertion, seems to be one of the possible mech-anisms of rupture of a vessel of epidural venousplexus, whose veins lack valves and have thin wall.
This explains why the great majority of thesehematomas are located on the dorsal (posterior) sur-face of the dura mater, which has a complex welldeveloped venous plexus4. SCSEHs usually extendalong two or three vertebral levels7,25. The usualpresence of SCSEH at the dorsal epidural spacefacilitates the surgical access. In our serieshematoma always involved the posterior spinal canaland thus typically accessed by a posterior approach.The greater length of the SCSEH covered eight ver-tebral levels, and the lower three levels.
In contrast to older studies that epidural venousplexus is responsible for causing SCSEHs, mostrecent data suggest that bleeding has an arterial ori-gin4. In general, the pressure within the cervicalepidural veins is lower than the intradural veins, thusa venous bleeding cannot strongly compress the cer-vical spinal cord. Moreover, in some cases an arteri-ovenous malformation or angioma9,21 have beenimplicated as the cause of the epidural hematoma.We encountered one case of dural arteriovenouscommunication that was dealt simultaneously withthe removal of the hematoma.Neurological findings usually include sudden intenseneck pain with a possible extension to the back, andrapid radiation to the upper extremities. Gradually,within minutes, hours, or days, a cervical spinal cordpressure appears with various degrees of neurologi-cal deficits and myelopathy below the level of injury(transverse medullary sensorimotor quadraparesisor semi-transverse medullary syndromes Brown -Sequard with hemiparesis)1,4,10,24.
Differential diagnosis is not always easy, requires ahigh degree of suspicion, and involves a wide spec-trum of diseases. In cases of an acute paresis differ-ential diagnostic includes acute prolapse of a cervicalintervertebral disc, spinal cord ischemia (anteriorspinal artery syndrome), extradural or intraduraltumors, epidural abscess, hematomyelia, andpolyradiculoneuropathy or transverse myelitis1,20.
In past decades, diagnosis could be made only withComputed Tomography in combination with myelog-raphy1. Nowadays, the gold standard in the diagnos-tic approach of SCSEH is MRI. It clearly highlightsthe hematoma and its exact location, the size and
ENCEPHALOS 51, 47-54, 2014

50ENCEPHALOS 51, 47-54, 2014
age of the hematoma, the compression and swellingof the spinal cord, and the post-operative visualiza-tion of the region. Hematoma is illustrated with equalto the spinal cord signal intensity in T1 sequenceswithin the first 24 hours (oxyhaemoglobin and deoxy-haemoglobin ), and as high signal on both T1 and T2sequences after 36 hours (extracellular methaemo-globin). Thus, the display of a superacute SCSEHmay resemble that of an epidural abscess or tumor.The contrast enhancement with paramagnetic sub-stance is extremely rare. Generally, in cases ofuptake of the contrast a strong suspicion of epiduraltumor or infection should be raised5,7. Selectivespinal angiography is indicated on suspicion of avascular malformation.
Preoperative neurological status is perhaps themost important factor in relation to the degree of neu-rological recovery6,7,17. Patients with incompletesensorimotor deficit have a better neurological out-come, and this is in agreement with our series. Incontrast, patients with complete sensorimotor paral-ysis and sphincter disorders have the worst progno-sis. Another important predictor is the interval fromthe onset of symptoms until operation. According tothe literature the surgical hematoma evacuation with-in 8 - 36 hours of onset of symptoms increases sig-nificantly the chances of complete recovery15,17,18.In our series, the second patient operated too latewith fully installed spinal cord compression, andeventually had an unfavorable outcome.Furthermore, in experimental models of spinal cord
injury in animals, it was confirmed that as greater thetime length of spinal cord pressure then more severepathological changes are identified in the nerve fibers, in the vascular endothelium, and microcircula-tion. Other factors that seem to affect prognosis areage, the extent and location of the hematoma, andthe speed of neurological deterioration20.Preoperatively, it is necessary to discontinue the
anticoagulant and antiplatelet therapy, administerfresh frozen plasma or vitamin K, as well as highdoses of prednisolone.Some authors report that in some cases conserva-
tive management of SCSEH could be just as effec-tive as surgical evacuation of the hematoma, provid-ed the ability of a close neurological and MRI follow up14,16, 26. These authors suggest non – operativetreatment in selected patients with clotting disordersin which the hematoma has not been organized insolid clot, but the epidural blood remains in a liquidstate. In these patients, usually with hemophilia, theneurological picture was usually mild and radi-ographic findings improved enough in the nexthours5,14,16,26. All our patients were in a severe con-dition with progressive neurological deterioration dueto the effects of spinal cord compression, and wereall treated surgically.Intraoperatively, we found that epidural tissue was
immersed in both hard blood clots and fresh bloodcollection. All removed material was sent for fullhistopathological examination to be examined forany possible cryptic vascular malformation.
51 ENCEPHALOS 51, 47-54, 2014
52ENCEPHALOS 51, 47-54, 2014

References
1. Alexiadou – Roudolf C, Ernestus RI, Nanassis K, LanfermannH, Klug N. Acute nontraumatic spinal epidural hematomas. Animportant differential diagnosis in spinal emergencies. Spine1998; 23: 1810 – 1813.2.Beatty RM, Winston KR. Spontaneous cervical epiduralhematoma. J Neurosurg 1984; 61: 143 – 148. 3.Cooper DW. Spontaneous spinal epidural hematoma. Casereport. J Neurosurgery 1967; 26: 343 – 345. 4.Dinsmore AJ, Leonard RB, Manthey D. Spontaneous spinalepidural hematoma: a case report. J Emerg Medicine 2005; 28:423 – 426.5.Duffill J, Sparrow OC, Millar J, Barker CS. Can spontaneousspinal epidural haematoma be managed safely without opera-tion? A report of four cases. J Neurol Neurosurg Psychiatry 2000;69: 816 – 819. 6.Foo D, Rossier AB. Preoperative neurological status in predict-ing surgical outcome of spinal epidural hematomas. Surg Neurol1981; 15: 389 – 401.7.Fukui MB, Swarnkar AS, Williams RL. Acute spontaneousspinal epidural hematomas. Am J Neuroradiol 1999; 20: 1365 –1372.8.Groen RJ. Non – operative treatment of spontaneous spinalepidural hematomas: a review of the literature and a comparisonwith operative cases. Acta Neurochir (Wien) 2004;146:103– 110.9.Groen RJ, Ponssen H. The spontaneous spinal epiduralhematoma A syudy of the etiology, Neurol Sci 1990;98:121– 138.10.Groen RJ, van Alphen HA. Operative treatment of sponta-neous spinal epidural hematomas: a study of the factors deter-mining postoperative outcome. Neurosurgery 1996;39:494– 508.11.Grollmus J, Hoff J. Spontaneous spinal epidural haemor
rhage: good results after early treatment. J Neurol NeurosurgPsychiatry 1975; 38: 89 – 90.12.Gundry CR, Heithoff KB. Epidural hematoma of the lumbarspine: 18 surgically confirmed cases. Radiology 1993; 187: 427– 431.13.Harik SI, Raichle ME, Reis DJ. Spontaneously remittingspinal epidural hematoma in a patient on anticoagulants. N EnglJ Med 1971; 284: 1355 – 1357.14.Inamasu H, Hori S, Aoki K, Aikawa N, Maruiwa H, Toyama Y.Spontaneous spinal epidural hematoma. Am J Emerg Med 2000;18: 837 – 839. 15.Klossek H, Huller E. Spontaneous spinal epiduralhematomas. Zentralbl Neurochir 1984; 45: 116 – 123.16.Le Coz P, Helias A, Woimant F, Haguenau M. Transient neu-rological manifestations disclosing spontaneous acute cervicalepidural hematoma. Rev Neurol (Paris) 1997; 153: 325 – 330.17.Liao CC, Lee ST, Hsu WC, Chen LR, Lui TN, Lee SC.Experience in the surgical management of spontaneous spinalepidural hematoma. J Neurosurg Spine 2004; 100: 38 – 45.18.Markham JW, Lynge HN, Stahlman GE. The syndrome ofspontaneous spinal epidural hematoma. Report of three cases.J Neurosurg 1967; 26: 334 – 342.19.Mattle H, Sieb JP, Rohner M, Mumenthaler M. Nontraumaticspinal epidural and subdural hematomas. Neurology 1987; 37:1351 – 1356.20.Morales Ciancio RA, Drain O, Rillardon L, Guigui P. Acutespontaneous spinal epidural hematoma: an important differentialdiagnosis in patients under clopidogrel therapy. Spine J 2008; 8:544 – 547.
53 ENCEPHALOS 51, 47-54, 2014

21.Olivero WC, Hanigan WC, McCluney KW. Angiographicdemonstration of a spinal epidural arteriovenous malformation.Case report. J Neurosurg 1993; 79: 119 – 120.22.Perez – Lopez C, Isla A, Gomez Sierra A, Budke M. Cervicalepidural hematoma without fracture in a patient with ankylosingspondylitis. A case report. J Neurosurg Sci 2004; 48: 43 – 47. 23.Ravi D, Dwarakanath S, Satish S, Gopal S, VenkataramanaNK. Spontaneous spinal extradural hematomas. J Clin Neurosci2006; 13: 269 – 272.24.Ravid S, Schneider S, Maytal J. Spontaneous spinal epidural-hematoma: an uncommon presentation of a rare disease. ChildsNerv Syst 2002; 18: 345 – 347.
25.Rohde V, Kuker W, Reinges MH, Gilsbach JM. Microsurgicaltreatment of spontaneous and non – spontaneous spinal epidur-al haematomas: neurological outcome in relation to aetiology.Acta Neurochir (Wien) 2000; 142: 787 – 792. 26.Serizawa Y, Ohshiro K, Tanaka K, Tamaki S, Matsuura K,Uchihara T. Spontaneous resolution of an acute spontaneousspinal epidural hematoma without neurological deficits. InternMed 1995; 34: 992 – 994.27.Tsai FY, Popp AJ, Waldman J. Spontaneous spinal epiduralhematoma. Neuroradiology 1975; 10: 15 – 30.
54ENCEPHALOS 51, 47-54, 2014






![A Traumatic Cervical Epidural Hematoma that Showed Rapid · Cervical spinal epidural hematoma is rare, and most cases are caused by spontaneous bleeding [1]. Traumatic cervical spinal](https://img.pdfslide.net/doc/110x75/5d1b365088c993dc468c7296/a-traumatic-cervical-epidural-hematoma-that-showed-rapid-cervical-spinal-epidural.jpg)