Embed Size (px)
Citation preview

CASE REPORT
Spontaneous twin anemia–polycythemia sequence complicated by recipient
placental vascular thrombosis and hydrops fetalis
SAMER A. ASSAF1, KURT BENIRSCHKE2, & RAMEN H. CHMAIT1
1Division of Maternal–Fetal Medicine, Department of Obstetrics and Gynecology, Keck School of Medicine, University of Southern
California, Los Angeles, CA, USA and 2Department of Pathology, School of Medicine, University of California, San Diego, CA,
USA
(Received 17 November 2009; revised 26 January 2010; accepted 12 May 2010)
Abstract
Twin anemia–polycythemia sequence (TAPS) is an atypical form of twin–twin transfusion syndrome (TTTS) thatpresents as a large intertwin hemoglobin difference with one twin developing anemia and the other developing polycythemia,without oligohydramnios–polyhydramnios sequence (Lopriore et al., Placenta 2007;28:47–51). The prenatal diagnosticcriteria for TAPS require that the middle cerebral artery-peak systolic velocity (MCA-PSV) measure greater than 1.5multiples of median (MoM) in the donor twin and less than 0.8 MoM in the recipient twin (Robyr et al., Am J ObstetGynecol 2006;194:796–803; Klaritsch et al., Ultrasound Obstet Gynecol 2009;34:149–154; Mari et al., N Engl Med2000;342:9–14). The presumed etiology of TAPS involves the presence of small caliber arteriovenous anastomoses, whichgenerate a slow transfusional process allowing for hemodynamic compensation (Lopriore et al., Placenta 2007;28:47–51;Lopriore et al., Placenta 2009;30:223–225; Lewi et al., Am J Obstet Gynecol 2006;194:790–795; Lopriore et al., Am JObstet Gynecol 2008;112:753–758; Van den Wijngaard et al., Placenta 2007;28:611–615). The resulting polycythemia inthe recipient twin is a risk factor for fetal and placental thrombosis (Van den Wijngaard et al., Am J Physiol 2005;288:R799–R814). We present a case of spontaneous TAPS complicated by a large placental vessel thrombosis and hydrops fetalis.Treatment via selective laser photocoagulation of communicating vessels (SLPCV) resulted in normalization of the MCA-PSV discordance.
Keywords: Placental thrombosis, hydrops fetalis, twin anemia–polycythemia sequence, twin–twin transfusion syndrome, selective laserphotocoagulation of communicating vessels
Introduction
Twin–twin transfusion syndrome (TTTS) has been attrib-uted to shared vascular communications in the placenta,resulting in a net transfer of blood from the donor to therecipient twin. TTTS characteristically causes donor twinoligohydramnios and recipient twin polyhydramnios [1]. Arare form of TTTS without oligohydramnios–polyhydram-nios was first described by Lopriore et al. and termed twinanemia–polycythemia sequence (TAPS) [2]. In TAPS, alarge intertwin hemoglobin difference exists, causing onetwin to become anemic and the other to becomepolycythemic [2]. TAPS has been documented to occurspontaneously in up to 6% of monochorionic twinpregnancies [3] and in up to 13% of cases post-lasersurgery for TTTS [4]. The prenatal diagnostic criteria forTAPS require that the middle cerebral artery-peak systolicvelocity (MCA-PSV) measure greater than 1.5 multiples ofmedian (MoM) and less than 0.8 MoM, respectively [4–6].The placental findings commonly associated with TAPSare very small arteriovenous anastomoses [2,7–10]. Thesesmall anastomoses generate a slow transfusional process
allowing for hemodynamic compensation, thus creating anabsence of the oligohydramnios–polyhydramnios sequencetypical of TTTS [2,7,9]. However, the compensatoryhematopoiesis may not be sufficient to prevent anemiafrom developing in one twin, and polycythemia in the co-twin [2,7,9]. The mechanism underlying the formation ofhematocrit discordance has been supported by a mathe-matical model developed by van den Wijngaard et al. [10].We present a case of spontaneous TAPS complicatedby recipient placental vascular thrombosis and hydropsfetalis.
Case report
A 47-year-old gravida 4, para 0, with monochorionicdiamniotic twins complicated by hydrops fetalis wasreferred for umbilical cord occlusion. The pregnancy wasconceived via in vitro fertilization with two embryosimplanted, resulting in a dichorionic triamniotic tripletgestation. The first trimester growth of the ‘singleton’ fetuswas noted to lag behind the monochorionic pair.
Correspondence: Ramen Chmait, MD, Assistant Professor, Obstetrics and Gynecology, Keck School of Medicine, University of Southern California, 1300 N
Vermont Avenue, Suite 706, Los Angeles, California 90027, USA. Tel: (323) 361-6074. Fax: (323) 361-6099. E-mail: [email protected]
The Journal of Maternal-Fetal and Neonatal Medicine, March 2011; 24(3): 549–552
ISSN 1476-7058 print/ISSN 1476-4954 online � 2011 Informa UK, Ltd.
DOI: 10.3109/14767058.2010.497878
J M
ater
n Fe
tal N
eona
tal M
ed 2
011.
24:5
49-5
52.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
The
Uni
vers
ity o
f M
anch
este
r on
11/
05/1
4. F
or p
erso
nal u
se o
nly.

The patient underwent a first trimester selective reductionof the ‘singleton’ fetus at another institution.
Ultrasound assessment at 19 weeks’ 6 days’ gestationconfirmed monochorionic diamniotic twins with an ante-rior placenta. Twin A had an amniotic fluid maximumvertical pocket (MVP) of 6.6 cm and grossly normalanatomy. Twin B was severely hydropic, with scalp edema,pericardial and pleural effusions, ascites, and a thickenedplacenta, but no structural abnormalities were identified.The intertwin weight discordance was 8%. The MVP inTwin B’s sac measured 9.5 cm. Spectral Doppler analysisof the umbilical artery demonstrated reversed diastolicflow, pulsatile flow in the umbilical vein, and reversed atrialand ventricular systolic flow in the ductus venosus. Fetalechocardiogram findings in Twin B were significant forthickened pulmonary valve with no forward flow consistentwith functional pulmonary atresia, thickened tricuspidvalve with severe tricuspid valve regurgitation, moderateright atrial enlargement, moderate biventricular hypertro-phy, retrograde ductal flow, and moderate pericardialeffusion. MCA-PSV was assessed for each twin. Twin Ahad a MCA-PSV of 43.2 cm/s, 1.70 MoM, suggestive offetal anemia. In contrast, Twin B had a MCA-PSV of15.4 cm/s, 0.6 MoM, suggestive of fetal polycythemia. Thepatient was informed of these findings and counseledregarding all management alternatives; she elected toproceed with selective laser photocoagulation of commu-nicating vessels (SLPCV) with possible cord occlusion ofTwin B.
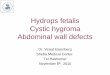
At 20 weeks’ gestation the patient underwent operativefetoscopy and SLPCV. Upon fetoscopic assessment, TwinA appeared pale while Twin B appeared plethoric(Figure 1). A large thrombosed vessel was visualized alongthe surface of the placenta arising from the velamentouscord insertion of Twin B. This vessel was documented withconcurrent ultrasound and was found to have absent bloodflow via color Doppler (Figure 2A,B). Only two smallunidirectional arterio-venous anastomoses were identifiedfrom Twin A to Twin B (Figure 3); these were laserphotocoagulated without complication. No septostomywas detected in the dividing membranes.
On post-operative day 1, Twin B remained hydropic.Cardiac and Doppler findings for both fetuses wereunchanged. Post-operative day 4 ultrasound revealednormalized MCA-PSV Dopplers for both twins. Twin Ahad a MCA-PSV of 30.4 cm/s (1.16 MoMs) and Twin B
had a MCA-PSV of 24.6 cm/s (0.94 MoMs). Twin Bcontinued to have severe pulmonary outflow tract obstruc-tion/dysfunction and worsening heart failure, along withhydrops and abnormal Dopplers, and at 22 weeks’ 4 days’gestation suffered an intrauterine demise. The remainingtwin, Twin A, showed appropriate fetal growth, normal
Figure 1. Fetoscopic image showing the plethoric and pale
extremities of Twin B and Twin A, respectively.
Figure 2. A: Ultrasound showing the large placental vessel with no
documentable blood flow via color Doppler near the velamentous
umbilical cord insertion site of Twin B. B: Fetoscopic view of
thrombosed placental vessel.
Figure 3. Fetoscopic confirmation of one of the two small caliber
unidirectional arterio-venous anastomoses.
550 S. A. Assaf et al.
J M
ater
n Fe
tal N
eona
tal M
ed 2
011.
24:5
49-5
52.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
The
Uni
vers
ity o
f M
anch
este
r on
11/
05/1
4. F
or p
erso
nal u
se o
nly.

development, and normal fetal Dopplers for the remainderof the pregnancy.
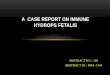
The patient delivered via cesarean section at 37 weeks’and 4 days’ gestation. Twin A was born alive with normalApgar scores. The hematocrit was 50.2%. Placentalpathology revealed a triamniotic, dichorionic triplet pla-centa with a thrombosed surface vessel (Figure 4A). Thehistological view of the thrombosed fetal blood vessel inFigure 4B shows complete occlusion of this vessel bycoagulated fibrin and clot. Infarcted villous tissue is seenbelow the chorionic plate.
Comment
We describe a case of spontaneous TAPS complicated by alarge placental vessel thrombosis and hydrops fetalis in thepolycythemic twin. We propose that the TAPS-inducedpolycythemia was a risk factor for a large placental vascularthrombosis near the cord insertion of that twin. Treatmentvia laser surgery resulted in normalization of the MCA-PSV discordance, and a normal hematocrit at the time ofbirth in the surviving twin.
TAPS is characterized by a large intertwin hemoglobindifference without the classic findings of TTTS [2].Prenatal diagnosis requires the absence of oligohydram-nios–polyhydramnios yet the presence of severe discor-dance in the MCA-PSV such that the anemic twinmeasures greater than 1.5 MoM and the polycythemictwin measures less than 0.8 MoM [4–6]. In our case, Twin
A had an MCA-PSV of 1.7 MoM and Twin B measured0.6 MoM. Fetoscopic assessment of the placenta revealedtwo small caliber arteriovenous anastomoses, which havebeen commonly associated with TAPS [2,7–10]. Thesesmall vessels may have created a slow transfusional processallowing for hemodynamic compensation, thus creating anabsence of the oligohydramnios–polyhydramnios sequencetypical of TTTS [2,7,9]. However, the compensatoryhematopoiesis was not sufficient to prevent anemia fromdeveloping in Twin A, and polycythemia in Twin B[2,7,9].
We suspect that the etiology of the thrombosed vessel onthe surface of Twin B’s portion of the placenta may beexplained by the polycythemia that developed in therecipient twin, thereby resulting in hyperviscosity andhypercoagulation, producing erythrocyte aggregation [11].Although, similar reported cases of TAPS [2,12] did notpresent with a placental vessel thrombosis, we believe thepathophysiology may potentially support its occurrence. Itis also plausible that the cardiac derangements were aconsequence of the increased work load on the heart due tothe hyperviscosity of the blood, or be of unrelatedcongenital origin. The ulterior demise of Twin B mayhave ultimately been caused by the TAPS, placental vesselthrombosis, the critical cardiac findings of functionalpulmonary atresia, or any combination thereof.
The reported management for iatrogenic TAPS follow-ing laser surgery treatment for TTTS includes intrauterinetransfusion, selective feticide, and repeat laser surgery[4,8,13]. In our case, laser treatment of spontaneous TAPSwas successful as evidenced by the normalization of MCA-PSV measurements and normal hematocrit levels demon-strated by Twin A at birth. The resolution of TAPSfollowing SLPCV may lend support to laser surgery as apotential treatment for spontaneous TAPS.
Declaration of interest: The authors report no conflictsof interest. The authors alone are responsible for thecontent and writing of the paper.
References
1. Quintero R. Ultrasound assessment in twin-twin transfusion
syndrome. In: Quintero R, editor. Twin–twin transfusion
syndrome. UK: Informa Healthcare; 2007. pp 71.
2. Lopriore E, Middeldorp JM, Oepkes D, Kanhai HH,
Walther FJ, Vandenbussche FP. Twin anemia–polycythemia
sequence in two monochorionic twin pairs without oligo-
polyhydramnios sequence. Placenta 2007;28:47–51.
3. Lewi I, Jani J, Blickstein I, Huber A, Gucciardo L, Van
Mieghem T, Done E, Boes AS, Hecher K, Gratacos E. The
outcome of monochorionic diamniotic twin gestation in the
era of invasive fetal therapy: a prospective cohort study. Am J
Obstet Gynecol 2008;199:514.e1–514.e8.
4. Robyr R, Lewi L, Salomon LJ, Yamamoto M, Bernard JP,
Deprest J, Ville Y. Prevalence and management of late fetal
complications following successful selective laser coagulation
of chorionic plate anastomoses in twin-to-twin tansfusion
syndrome. Am J Obstet Gynecol 2006;194:796–803.
5. Klaritsch P, Deprest J, Van Mieghem T, Gucciardo L,
Done E, Jani J, Lewi P, Rasmussen S, Lewi L. Reference
ranges for middle cerebral artery peak systolic velocity in
monochorionic diamniotic twins: a longitudinal study. Ultra-
sound Obstet Gynecol 2009;34:149–154.
6. Mari G, Deter RL, Carpenter RL, Rahman F, Zimmerman R,
Moise KJ, Dorman KF, Ludomirsky A, Gonzalez R,
Gomez R, et al. Noninvasive diagnosis by Doppler ultra-
Figure 4. A: Gross view of the placenta showing the thrombosed
vessel of Twin B. The two laser sites of the former arterio-venous
communications are labeled. B: Histological view of thrombosed
placental vessel.
Spontaneous TAPS 551
J M
ater
n Fe
tal N
eona
tal M
ed 2
011.
24:5
49-5
52.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
The
Uni
vers
ity o
f M
anch
este
r on
11/
05/1
4. F
or p
erso
nal u
se o
nly.

sonography of fetal anemia due to maternal red-cell alloim-
munization. N Engl Med 2000;342:9–14.
7. Lopriore E, van den Wijngaard JP, Pasman SA, Oepkes D,
Walther FJ, Van Gemert MJC, Vandenbussche FPHA.
Quantification of feto–fetal transfusion rate through a single
placental arterio-venous anastomosis in a monochorionic twin
pregnancy. Placenta 2009;30:223–225.
8. Lewi L, Jani J, Cannie M, Robyr R, Ville Y, Hecher K,
Gratacos E, Vandecruys H, Vanecaveye V, Dymarkowski S,
et al. Intertwin anastomoses in monochorioinic placentas after
fetoscopic laser coagulation for twin-to-twin transfsuion
syndrome: is there more than meets the eye? Am J Obstet
Gynecol 2006;194:790–795.
9. Lopriore E, Deprest J, Slaghekke F, Oepkes D,
Middeldorp JM, Vandenbussche FPHA, Lewi L. Placental
characteristics in monochorionic twins with and without twin
anemia–polycythemia sequence. Am J Obstet Gynecol
2008;112:753–758.
10. Van den Wijngaard JPHM, Lewi L, Lopriore E, Robyr R,
Middeldorp JM, Vandenbussche FPHA, Devlieger R,
Deprest J, Ville Y, van Gemert MJC. Modeling severely
discordant hematocrits and normal amniotic fluids after
incomplete laser therapy in twin-to-twin transfusion syn-
drome. Placenta 2007;28:611–615.
11. Van den Wijngaard JPHM, Umur A, Krediet RT, Ross MG,
van Gemert MJC. Modeling a hydropic recipient twin in twin–
twin transfusion syndrome. Am J Physiol 2005;288:
R799–R814.
12. Van Meir H, Slaghekke F, Lopriore E, van Wijngaarden WJ.
Arterio-arterial anastomoses do not prevent the development
of twin anemia–polycythemia sequence. Placenta 2010;
31:163–165.
13. Herway C, Johnson A, Moise K, Moise KJ Jr. Fetal
intraperitoneal transfusion for iatrogenic twin anemia–poly-
cythemia sequence after laser surgery. Ultrasound Obstet
Gynecol 2009;33:592–594.
552 S. A. Assaf et al.
J M
ater
n Fe
tal N
eona
tal M
ed 2
011.
24:5
49-5
52.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
The
Uni
vers
ity o
f M
anch
este
r on
11/
05/1
4. F
or p
erso
nal u
se o
nly.