Embed Size (px)
Citation preview
J. clin. Path. (1965), 18, 715
Squamous cell carcinoma ofthe body of the uterusHANNA BARNETT'
From the Department ofPathology, South London Hospital for Women, Clapham, London
SYNOPSIS A case of primary squamous cell carcinoma of the body of the uterus is reported. Thenumber of authentic cases of this tumour which meet the rigid criteria referred to is extremelysmall. The histological findings are described in detail and some aetiological considerations arementioned briefly. Certain special aspects of the diagnosis are discussed.
The incidence of primary squamous cell carcinomaof the body of the uterus is extremely rare. Fluhmann(1928) formulated the following conditions whichmust be met before the diagnosis can be consideredas established. 1 There must be no co-existingadenocarcinoma. 2 There must be no connexionbetween the tumour and the squamous epithelium ofthe cervix. 3 The absence of a primary growth in thecervix must be established conclusively. Following'Present address: Department of Pathology, Lewisham GeneralHospital, Lewisham High Street, London S.E.13.Received for publication 23 March 1965.
jA'4 7
.440*
it, i, .wot''* * %
.444~~~~r
J,IsV* ,
4 1~~~~~~~~~~~44.~
these rigid criteria, only five cases were accepted byFluhmann. Two further cases were described byWahi and Jain (1949) and by Chu, Lepow, andGodsick (1958). Peris, Jernstrom, and Bowers (1958)published another case and reviewed the literature.The prerequisites for the diagnosis which wereformulated by Peris exclude Fluhmann's firstcriterion, consequently his list of 25 cases publishedup to 1958 includes tumours which contained bothsquamous and columnar malignant elements. Onefurther case was published by Mazzella (1963). Thefollowing case meets Fluhmann's full requirements.
* * * 44
.4' 4,~*,;
;Wp
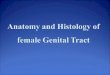
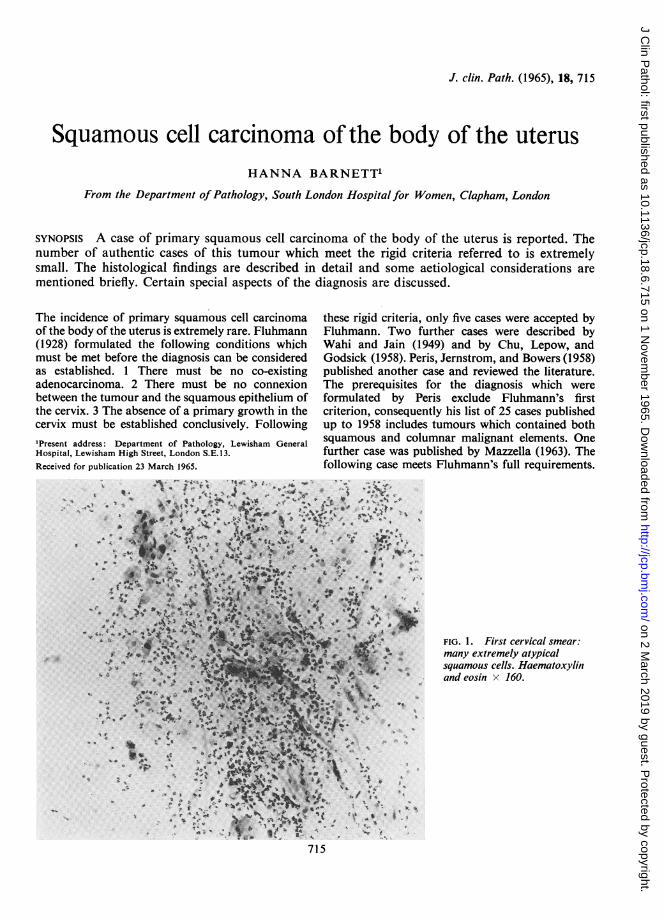
itrIG. 1. First cervical smear:Tr ~~~~~many extremely atypical4. 4 ~~~~squamous cells. Haematoxylinlb
andeosin x 160.
715
on 2 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.18.6.715 on 1 Novem
ber 1965. Dow
nloaded from
Hanna Barnett
CASE REPORT
A married multiparous woman aged 59 presented with ahistory of occasional very slight vaginal bleeding for threemonths. Some discharge was also noted. The menopausehad occurred 14 years previously and she had had nobleeding since till the present episode. She was anapparently healthy woman with nothing remarkable inher previous history or family history. Vaginal examina-tion revealed no abnormalities; the cervix appearedhealthy, the uterus was small. Routine cervical andvaginal smears were taken. These smears showed amoderate number of extremely atypical squamous cellswhich were suspicious (Fig. 1) and a cone biopsy wasrequested. The patient was admitted 10 days later forcurettage and biopsy. No abnormalities were found atoperation. The uterine cavity measured 6 cm., thecurettings were scanty but an adequate cone biopsy wastaken. Histological examination of the curettings revealedthe presence of blood clot and strips of markedly atypicalsquamous epithelium only (Figs. 2, 3). The cone wassectioned serially, and the squamous epithelium showedminimal atypia only. The patient was discharged andfollowed up. On her first follow-up visit six weeks laterno further vaginal bleeding had occurred. Smears wererepeated and these again revealed the presence ofabnormal squamous cells (Fig. 5a). The patient wasadvised to undergo a hysterectomy but she refused. Shewas seen at frequent intervals during the following sevenmonths; slight vaginal 'spotting' persisted but no other
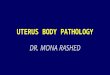
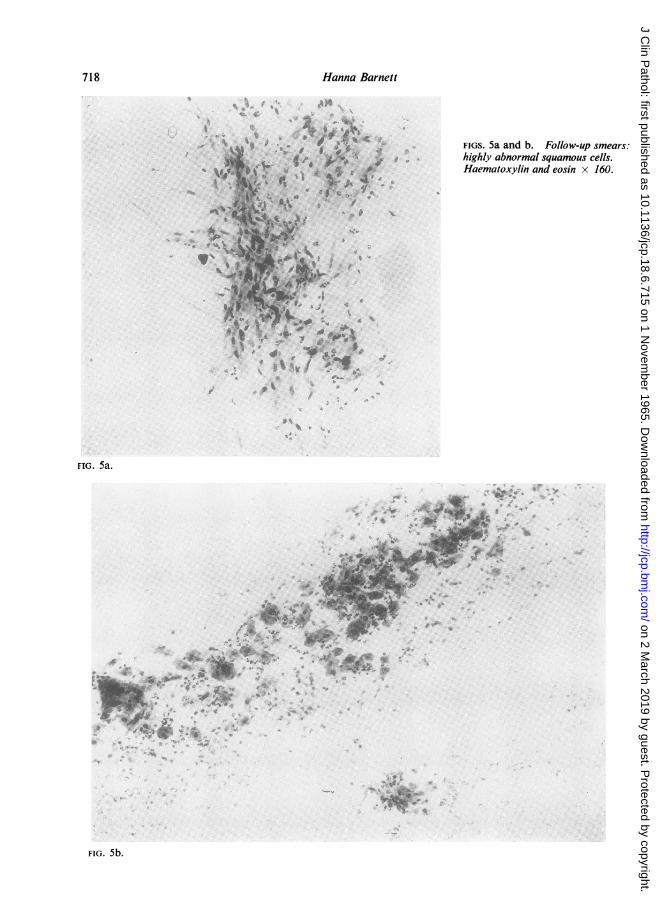
abnormalities were evident on vaginal examination. Thesmears consistently showed abnormal squamous cells(Fig. 5). (At no time were any abnormal columnar cellsfound in the smears.) The patient was finally persuadedto undergo hysterectomy preceded by the application ofradium at another hospital. Before the insertion of theradium (40 mg. in intrauterine tubes, 35 mg. in a cervicalbox, 15 mg. in the vagina for 30 hours) a fractionalcurettage was done and multiple cervical biopsies weretaken. This material was reported as showing chronicinflammatory changes only in the cervix; the curettingsconsisted of keratin debris, blood clot, and strips ofsquamous epithelium showing marked atypia (Fig. 6).Having thus excluded an invasive squamous carcinomaof the cervix, the patient returned to this hospital 10 dayslater for a total hysterectomy and bilateral salpingo-oophorectomy, after one dose of radium only. At opera-tion a fundal growth infiltrating the entire thickness ofthe wall was found. Post-operative recovery was good,and a course of high-voltage radiotherapy was given. Thepatient is well four months later.
PATHOLOGY
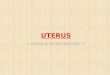
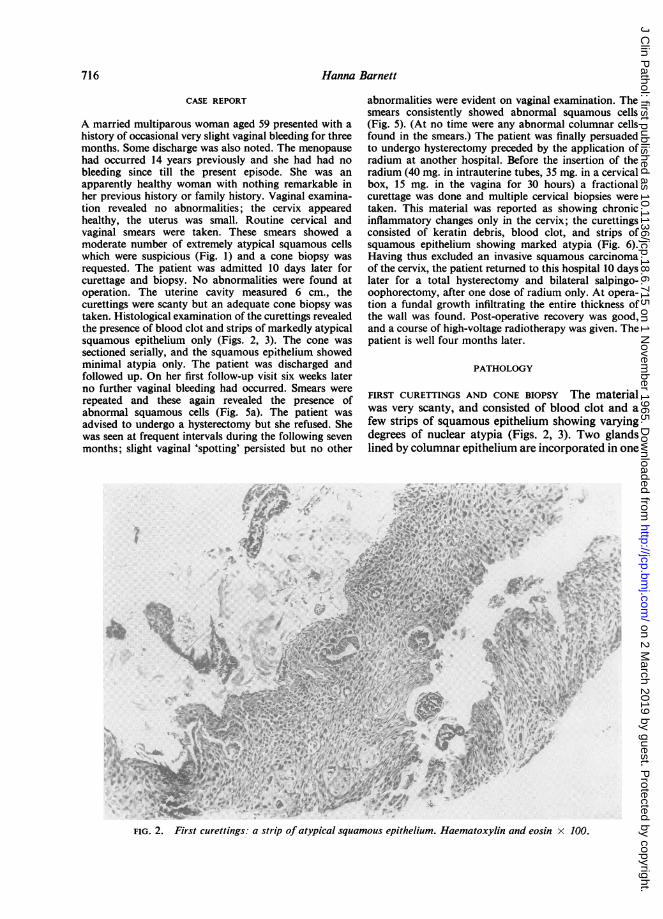
FIRST CURETTINGS AND CONE BIOPSY The materialwas very scanty, and consisted of blood clot and afew strips of squamous epithelium showing varyingdegrees of nuclear atypia (Figs. 2, 3). Two glandslined by columnar epithelium are incorporated in one
vu~~~~~*
\ 4'-- :' ' - s ew
tKt 4 ,,4,;'''t;"''¢4~~~~~~~~~~4
* L s s X - It
..IF ..
.*
*: lle
S.i ...
FIG. 2. First curettings: a strip of atypical squamous epithelium. Haematoxylin and eosin x 100.
716
.11.I-..A.
on 2 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.18.6.715 on 1 Novem
ber 1965. Dow
nloaded from
Squamous cell carcinoma of the body of the uterus 717
r * . e~~~~~~~~~~~~~~~~~~~~~~...:} *s w; | *ma -4
tt^4' 4 0,$ 0~~~~~~~S~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.J.@Z
.~~~~~~~~~~~~~~~~~~~~~~~~~~~:A,~~~~~TFI.4.Frs on ips:choiciflmaor hags.Edoevca anllie b oumaeiVeimHaematoxylinandeosin x 100
on 2 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.18.6.715 on 1 Novem
ber 1965. Dow
nloaded from
7uHanna Barnett
FIGS. 5a and b. Follow-up smears:highly abnormal squamous cells.Haematoxylin and eosin x 160.
..
FIG. 5a.
rwrap.V
.4',
C*
V 2'
O
.4
FIG. 5b.
>718
on 2 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.18.6.715 on 1 Novem
ber 1965. Dow
nloaded from
Squamous cell carcinoma of the body of the uterus
.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~MJ~ ~ ~ ~ ~ J~~~~~~ A
<v-~ ~ ~ 4' 4..y+ t ..'f'.
Kw
V47 .~~~~~
e~ ~~ ~ ~ ~~~~-v~4.^Z0ZAv*..Z< *9E
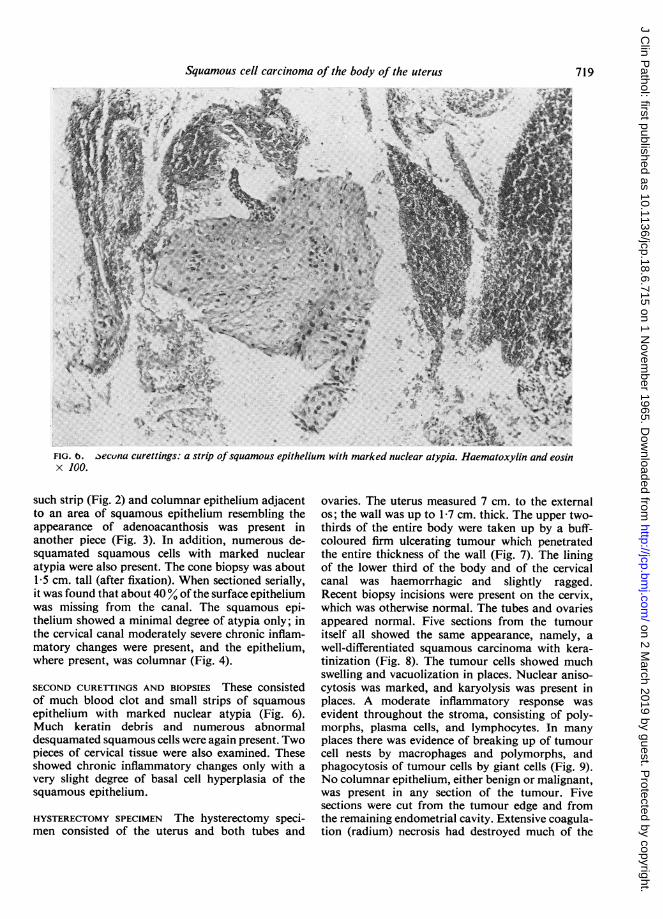
FIG. b. aecuna curettings: a strip ofsquamous epithelium with marked nuclear atypia. Haematoxylin and eosinx 100.
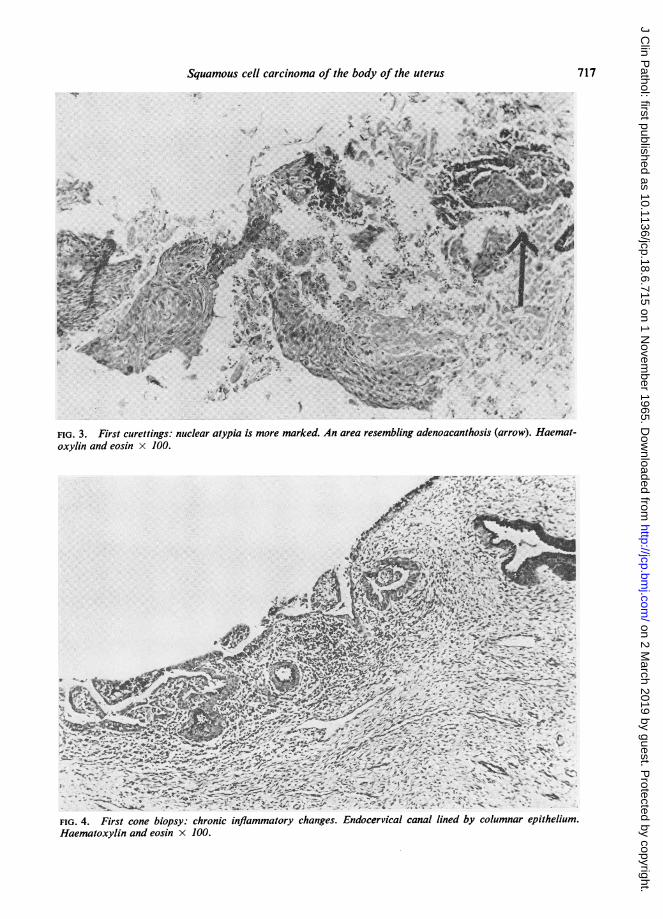
such strip (Fig. 2) and columnar epithelium adjacentto an area of squamous epithelium resembling theappearance of adenoacanthosis was present inanother piece (Fig. 3). In addition, numerous de-squamated squamous cells with marked nuclearatypia were also present. The cone biopsy was about1-5 cm. tall (after fixation). When sectioned serially,it was found that about 40% of the surface epitheliumwas missing from the canal. The squamous epi-thelium showed a minimal degree of atypia only; inthe cervical canal moderately severe chronic inflam-matory changes were present, and the epithelium,where present, was columnar (Fig. 4).
SECOND CURETTINGS AND BIOPSIES These consistedof much blood clot and small strips of squamousepithelium with marked nuclear atypia (Fig. 6).Much keratin debris and numerous abnormaldesquamated squamous cells were again present. Twopieces of cervical tissue were also examined. Theseshowed chronic inflammatory changes only with avery slight degree of basal cell hyperplasia of thesquamous epithelium.
HYSTERECTOMY SPECIMEN The hysterectomy speci-men consisted of the uterus and both tubes and
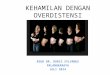
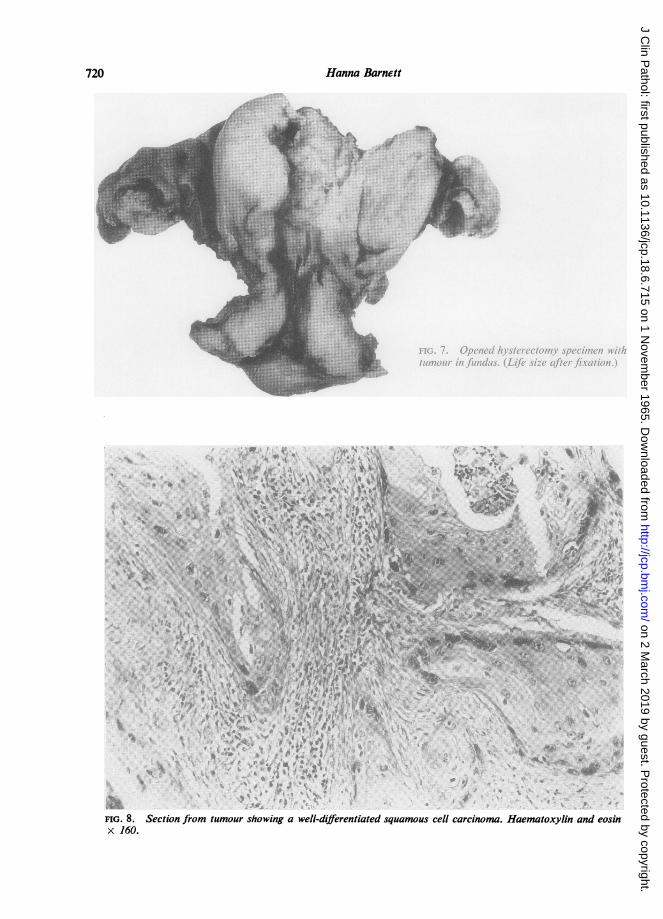
ovaries. The uterus measured 7 cm. to the externalos; the wall was up to 1-7 cm. thick. The upper two-thirds of the entire body were taken up by a buff-coloured firm ulcerating tumour which penetratedthe entire thickness of the wall (Fig. 7). The liningof the lower third of the body and of the cervicalcanal was haemorrhagic and slightly ragged.Recent biopsy incisions were present on the cervix,which was otherwise normal. The tubes and ovariesappeared normal. Five sections from the tumouritself all showed the same appearance, namely, awell-differentiated squamous carcinoma with kera-tinization (Fig. 8). The tumour cells showed muchswelling and vacuolization in places. Nuclear aniso-cytosis was marked, and karyolysis was present inplaces. A moderate inflammatory response wasevident throughout the stroma, consisting of poly-morphs, plasma cells, and lymphocytes. In manyplaces there was evidence of breaking up of tumourcell nests by macrophages and polymorphs, andphagocytosis of tumour cells by giant cells (Fig. 9).No columnar epithelium, either benign or malignant,was present in any section of the tumour. Fivesections were cut from the tumour edge and fromthe remaining endometrial cavity. Extensive coagula-tion (radium) necrosis had destroyed much of the
719
on 2 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.18.6.715 on 1 Novem
ber 1965. Dow
nloaded from
Hanna Barnett.w 02s,#t~~~~~~~~~~~~lti;I AsZ W*' '
,,'.,.. 'j.t: ar }P
* O.%.
t4. 6"-2i 4,
*F ~ ~~ ~ ~~~*.'
FIG. 8. Section from tumour showing a well-differentiated squamous cell carcinoma. Haematoxylin and eosinx 160.
720
1:
It
on 2 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.18.6.715 on 1 Novem
ber 1965. Dow
nloaded from
Squamous cell carcinoma of the body of the uterus 721
v .,.K O,_YJ I ,4t6 O' V#J :io
-14
-P T
NAM
t
t)17iiY
:441
.R;P.
41,
44
V
A.
Al 14.vl.,.,:
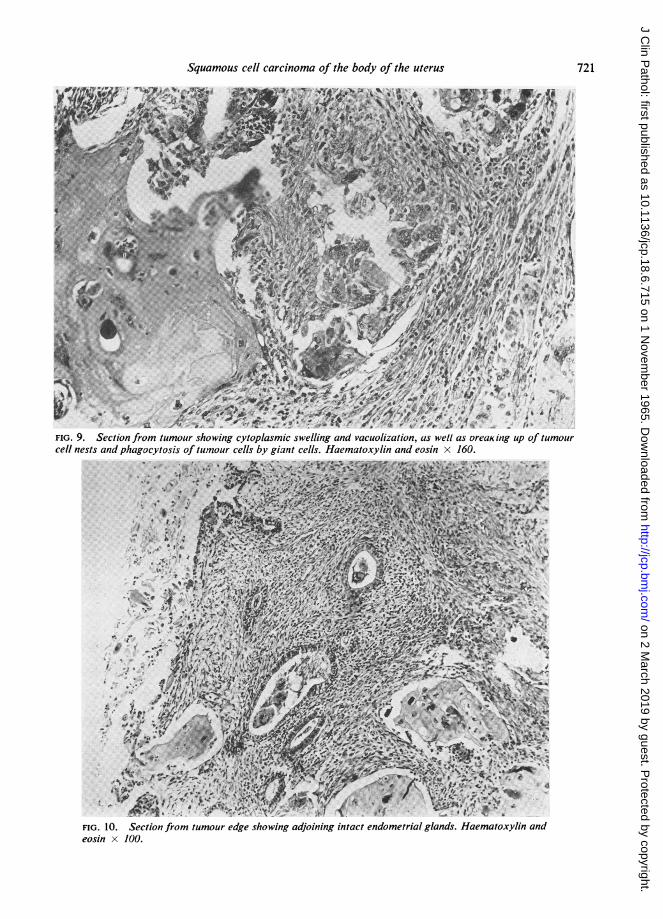
FIG. 9. Section from tumour showing cytoplasmic swelling and vacuolization, as well as oreaic ing up of tumourcell nests and phagocytosis of tumour cells by giant cells. Haematoxylin and eosin x 160.
AW
4 N..4
ti A.
t4 vp
f 4%
-tio;'AIf
/V
O' t`fi to'! 4111
FI.1.Seto rm uoregesoigadonn itc nomtilgansamtoJi n
eosinx100.T
on 2 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.18.6.715 on 1 Novem
ber 1965. Dow
nloaded from

72Hanna Barnett
surface layers of the entire uterus and cervix. It was,however, possible to demonstrate endometrium withcuboidal epithelium lining the surface and glands inthe immediate vicinity of the tumour (Fig. 10) andin several other places. In one section a circumscribedarea of squamous epithelium was found merging intocuboidal epithelium on either side on the endo-metrial surface; cuboidal epithelium was lining theglands beneath this. The lining of the cervical canal,where preserved, was columnar epithelium. Noevidence of invasive growth was found in foursections of the cervix. All surface epithelium showeda marked response to radium.
DISCUSSION
The following points of interest emerge from thiscase:The case presented here is a true primary squamous
carcinoma of the body of the uterus. A primaryinvasive carcinoma of the cervix was ruled out con-clusively by serial sectioning of the original conebiopsy, by later cervical biopsies, and finally bymultiple sections from the hysterectomy specimen.No coexisting adenocarcinoma was found. In spiteof extensive damage to surface layers caused byradium, it was possible to demonstrate columnarepithelium in the cervical canal and cuboidal epi-thelium on the endometrial surface and in the glands.This uterine tumour was therefore not preceded by ageneralized squamous metaplasia of the entiresurface epithelium as was described by Chu et al.(1958) in his case. While much discussion stillcentres on the problem of the aetiology ofsquamous metaplasia in the endometrium of adultwomen (Novak, and Woodruff, 1962), the pre-sence of a squamous cell carcinoma of the bodyis easier to understand when it appears as a sequelto such a generalized metaplastic process than whenit arises apparently de novo. Nor was there in thiscase any evidence in the hysterectomy specimen of apre-existing endometrial glandular hyperplasia withacanthosis, which, at least in theory, could give riseto a squamous carcinoma. The origin of this tumourremains therefore problematical. It could beassumed to have arisen in a localized area ofsquamous metaplasia of surface epithelium, theaetiology of which is unknown. At least one suchisolated area of squamous metaplasia was demon-strated.The swelling of the tumour cells, the occasionally
marked nuclear irregularities, as well as the appear-ance of phagocytosis of tumour cells by macrophagesand giant cells (Fig. 9) were all interpreted as theresponse to radium. This interpretation wouldexplain the apparent dissimilarity between the
appearances of the 'atypical' epithelium in bothcurettings and the appearances of the tumour in thesections. The 'atypical' squamous epithelium in bothcurettings must, in retrospect, be assumed to haveoriginated in the same tumour which was present allalong and caused the patient's symptoms.
Finally, while there is no question of the value ofvaginal cytology in general, and while it may haveplayed a minor role even in this case, it would appearthat on balance cytology-conscious thinking hadtended to obscure the real issue. From the appear-ances of the first smears a squamous carcinoma ofthe cervix, or at least a lesion in situ, was suspected.A negative cone biopsy, from which, however, muchsurface epithelium was missing, does not exclude alesion in situ: when curettage precedes conization,accidental scraping of the endocervical canal is oftenunavoidable. It was reasonable to assume that acarcinoma in situ could have been present in thesedenuded areas; the finding of detached strips of veryatypical squamous epithelium in the curettings lentsupport to this view. These strips of epithelium couldnot be diagnosed as unequivocally malignant. Wehave become familiar with the very gradual mergingof the 'borderline squamous dysplasias' of thecervix with carcinoma in situ, and the differentiationof one lesion from the other is a highly individualjudgment. The appearance of the strips of epitheliumin the curettings resembled this type of intermediatelesion. Thus, while an invasive squamous carcinomaof the cervix was excluded, the findings in the originalsmears, in the cone biopsy, and in the curettingscould reasonably lead to the diagnosis of 'borderlinesquamous dysplasia' merging into carcinoma in situ.In previous cases with similar findings such an inter-pretation has proved correct; however, it was anerroneous explanation for the findings presentedhere. Had there not been a satisfactory interpretationfor these findings, the possibility of a squamouscarcinoma of the body of the uterus, however rare,might have been considered more readily.
I wish to thank Dr. A. Gibson for her interest andencouragement and Miss E. Sibthorpe for her assistancein clinical matters and for helpful discussion. I amindebted to Dr. M. Bennett for permission to use hismaterial from this case. I am deeply grateful to Mr. A. L.Barron for preparing the photomicrographs and toMiss K. Hastings for technical assistance.
REFERENCES
Chu, F., Lepow, H., and Godsick, W. (1958). Arch. Path., 65, 13.Fluhmann, C. F. (1928). Surg. Gynec. Obstet., 46, 309.Mazzella, G. (1963). Rass. int. Clin. Ter., 43, 613.Novak, E. R., and Woodruff, J. D. (1962). Gynecologic and Obstetric
Pathology, 5th ed., p. 155. Saunders, Philadelphia.Peris, L. A., Jernstrom, P., and Bowers, P. A. (1958). Amer. J. Obstet.
Gynec., 75, 1019.Wahi, P. N., and Jain, R. L. (1949). Indian J. med. Sci., 3, 417.
722
on 2 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.18.6.715 on 1 Novem
ber 1965. Dow
nloaded from