Embed Size (px)
Citation preview
Orientation on Referral System in RHSDP
(Under Aegis of Rajasthan Health System Development Project)
May 2005
State Institute of Health & Family Welfare
Rajasthan, Jaipur
PrefacePrefacePrefacePreface
SIHFW, Rajasthan is involved in selected in-service trainings in Rajasthan Health System Development Project. Trainings in context of strengthening referral system happens to be one of them. As per
project implementation plan selected professionals from each of the secondary facilities of the project would be given an in-service orientation on referral system.
SIHFW has proposed a strategy in which the trainees to be
identified by the RHSDP shall be oriented for two days covering the
diseases from various specialties. We speculate around 42 training program of two days each which will be conducted at two HFWTCs and at our own Institute. Further, we propose sensitization program for primary and tertiary level facilities may be convened to complete the
chain of referral.
I must bring on record the effective contribution from Dr. J.P. Jain our Consultant, Dr. B.N. Sharma, Nodal Officer from this Institute
and Dr. P.C. Ranka of the RHSDP in bringing out this module.
31.5.2005 Shiv Chandra Mathur SIHFW, Rajasthan, Jaipur Director
CO#TE#TS
Chapter. - Title - Page No.
1. Introduction 1
RHSDP goal & objective
Proposed Referral System
Manpower deployment
2. Structure of organization 7
& Medical care facilities
3. Linkage at various levels 10
Decision Making
Transport and communication
Management of Blood
4. Referral Norms in RSHDP 15
a) Disease-wise services at
various facilities
b) Directives for Referral Norms
5. Feed back and Follow-up 41
6. Rajasthan State Essential 44
Medicines List
Appendices 1 Manpower Norms
2. Referral Cards
3 Referral Register
4 Program for Training of Referral System
Chapter – 1
I#TRODUCTIO#
Rajasthan Health System Development Project (RHSDP) was conceived with
the support of World Bank. The ultimate goal of the project is improvement in
the Health of people of the State, with the following aims and objectives.
1. To enhance the effectiveness and quality of health services at the
primary and secondary levels through policy and institutional
development.
2. To increase access to and equity in health care service delivery with
particular focus to the underserved sections. {
To achieve these objectives the whole project has following components.
1. Policy Development and Project Management
2. Improving Quality and Efficiency of Public Health Care services at
Primary/secondary level.
3. Improving access to Health care services for poor.
In consonance with the components it is proposed to strengthen the referral
system. In this context quality norms have been decided for various levels of
Medical Care facilities.
Referral services are non-existent in the state and do not have definite norms.
Patient is at liberty to seek care at any level of his/her choice and convenience.
In other words a patient does not require referral slip or prior appointment to
seek care at higher level facilities. Most of the in- patients at the secondary level
institutions, such as CHCs or district hospitals, by pass the primary health
facilities, whenever they wish. Self referrals even for common ailments create
overcrowding at higher-level institutions. CHCs are also bypassed for even
minor ailments resulting in extremely poor bed occupancy. The main reasons
for bypassing lower level institutions seem to be lack of diagnostic and
treatment facilities at these centers, absence of qualified medical
1
and nursing staff, non-availability of drugs, poor equipment, and people’s lack
of knowledge about the available services. On the other hand, people often
refuse to be referred to higher-level institutions, especially in backward areas,
due to high transportation and other costs, and apprehension of mistreatment or
poor attention there. In improving quality of health services, a key instrument is
referral system, which has to be reviewed to make it stream lined.
The project strongly emphasizes that strengthening of secondary level hospitals
would raise credibility of the primary health care system as the referred cases
from the primary level will get better quality care on the one hand while
reducing the work load of tertiary care hospitals on the other. It is thus
imperative to have a good referral system with adequate support so that services
are available in a comprehensive manner nearer their doorsteps. An efficient
and effective referral system depends upon
• Linkages between different levels of health care
• Availability of specialists and support services
• Resources
• Timely decision
• Transport and communication
• Referral criteria and protocols
• Feedback and follow-up
Proposed Referral System
With the up gradation of health facilities provision of additional inputs, and
enhancement of skills of service providers it is expected that the health facilities
would comply with the requirements of the clients. The utilization of these
institutions depends upon the flow of the patients from the outreach area.
Referral at appropriate institutions will reduce the gap between illness and
seeking treatment and out-of-pocket expenditure. The institutions below district
level would be able to screen the patients, limiting the load on district hospitals.
However,
2
the above investments could really bring forth the desired results if only they
are backstopped by an effective referral system. An effective referral system
would derive its substance from the following elements.
▪ Procedural directives;
▪ Dissemination of information to the community about the available
services
▪ Referral protocols with explicitly laid methodology of the working
of referral system;
▪ Improved support to enhance the referral of cases from remote
areas;
▪ Sensitization and training of those who refer and those who receive
the referred; and
▪ Timeliness
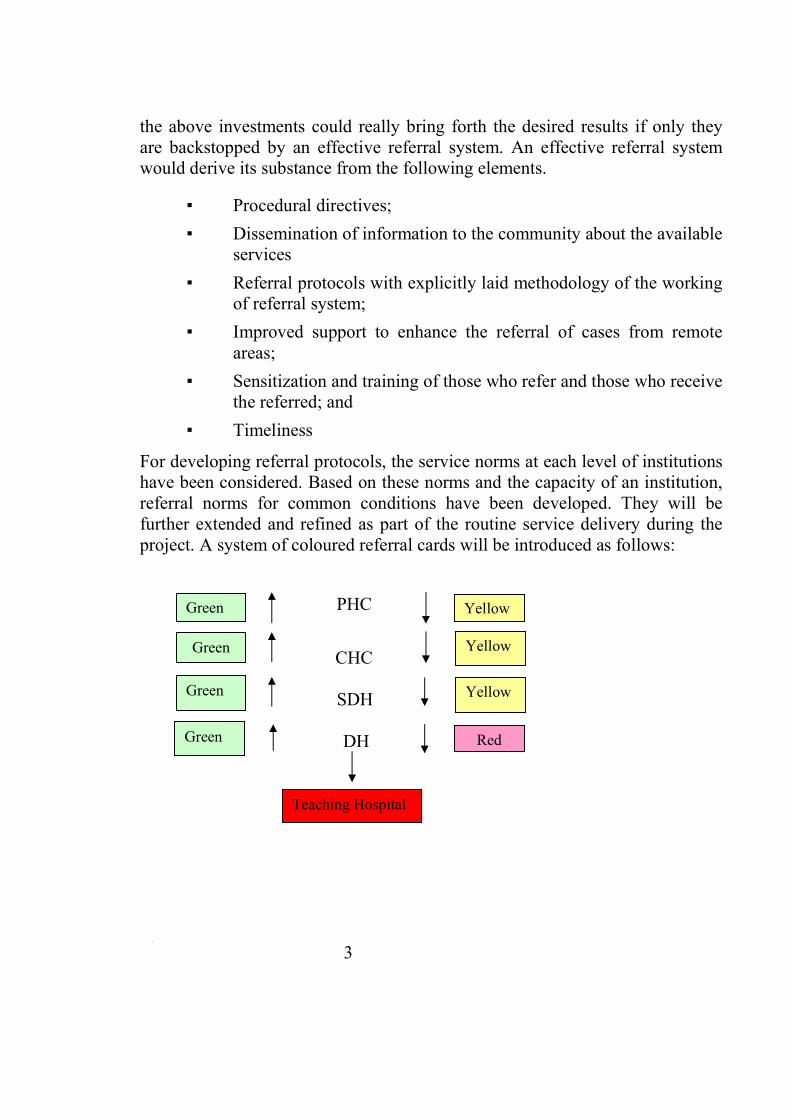
For developing referral protocols, the service norms at each level of institutions
have been considered. Based on these norms and the capacity of an institution,
referral norms for common conditions have been developed. They will be
further extended and refined as part of the routine service delivery during the
project. A system of coloured referral cards will be introduced as follows:
PHC
CHC
SDH
DH
[[[
3
Green
Green
Green
Red
Yellow
Yellow
Yellow
Teaching Hospital
Green
The Referral Card (given in appendix) would have basic patient identification
and clinical information like:
a) Patient identification (Name, age, sex, address)
b) A brief history of sickness (major complaints, findings and
treatment taken)
c) Clinical diagnosis
d) Treatment given (including date and admission and length of
stay)
e) Diagnostic tests and their results (reports to be attached)
f) Condition at the time of referral
g) Centre to which referred
h) Reasons for referral
This card along with the available diagnostic test reports shall be taken to
higher levels where the patients are referred. The down-referral/feed back
would be made to the referring institution and will include final diagnosis,
treatment to be continued and other follow-up instruction. The Feedback Card
is given in appendix.
For people to know the health facility and the services it offers, all district
hospitals are in the process of developing Citizen Charter, in a participatory
manner keeping in view the beneficiary needs and services available at the
facility, which would make people aware of services, staff, structure, fee,
facilities and free services. To start with, CHC/SDH will be covered through
effective IEC and gradually it is intended to have a Citizen Charter for every
CHC/SDH/DH. Referral Norms have been developed keeping in view the
assignment of Health Care providers and their expertise/skills in diagnosis and
treatment of respective illness of their discipline. For Health care provider at
different facilities referring the case to higher level institution, it is imperative
to know the availability of expertise of the specialty and supportive staff.
Looking to the necessity and capacity of beds at different levels the specialist,
SMO, MO and supportive staff are deployed (man power is given in the
appendix.1)
4
The department will issue the procedural directive to avoid delays and
confusions. Some of them relate to the following.
▪ All patients will be entitled for use of ambulance/vehicle on
payment.
▪ At receiving institutions a referred patient would be an out of
queue priority.
▪ A record of referrals received and referrals made will be
maintained to facilitate follow up.
▪ If necessary, to be justified by the treating physician, a member of
the medical staff would escort referred cases.
▪ A minimum set of clinical documents to be sent with the patient in
order to avoid duplication, cut costs and reduces treatment
initiation time.
The proposed Project Coordination and Monitoring Committee at the district
level will ensure creation of a District Referral, Committee at each hospital. The
committee will consist of the following members: PMO, CMHO, DY. CMHO
at sub-divisional level, Medical Officer In-charge of hospitals/CHCs located at
sub-divisional, Medical Officer In-charge of all CHCs and Superintendents of
teaching hospital (wherever applicable). This committee will meet once in a
month and ensure the following activities.
▪ Monitoring upward as well as down ward referrals.
▪ Mobilizing NGO/community support for transporting patients.
▪ Disseminating information to health staff and public on guidelines
of referral and services available at each level.
▪ Using referral data for decision-making.
The follow-up will be done through the feedback received from the district
referral Committees. Initially, on the basis of two or three major disease will be
considered for follow-up of referral interventions.
5
Incentive for good referral practices will encourage and be considered at the
time of ranking of hospital on quality indicators.
The mobile camps to be organized to extend the out-reach services in the tribal
and desert areas will also follow the same referral system.
With above background, the Referral System Training aims at:
(a) Orienting the medical care professionals posted at secondary
facilities on the process of referral.
(b) Enhancing the capacity of trainees to disseminate the referral
related information to primary and tertiary level facilities.
6
Knowing is not enough,
We must apply,
Willing is not enough,
We must act,
Johann Wolfgang Von Goethe
Chapter -2
STRUCTURE OF ORGANIZATION
To implement the proposed project strategy, a project management structure is
required. The proposed Project Management structure would have identified
roles and responsibilities of individuals in implementing the project. Among
these roles would be those that seek to strengthen management and institutional
capacity through improved management and development of human resources.
It is expected the HR management will go beyond and include personnel
policies and decisions affecting recruitment, posting, performance, appraisal,
and rewards. Support by way of improved management of information through
a comprehensive and integrated information system would be provided such
that it would enable managers at all levels to access performance. Importantly,
this would be done through decentralized structures and systems that facilitate
implementation.
Organization of medical care facilities
The districts are divided into a number of administrative blocks (conforming to
the area of Panchayat Samiti). At the Block HQ, the Medical Officer In-charge
of the Block PHC is responsible for implementing all national health
programmes, family welfare and reproductive health and curative services in
the block area through the network of PHCs and Sub-centres. From the
administrative point of view the block PHC compiles all the performance
reports sent by CHCs and PHCs.
At the PHC level the Medical Officer in charge is responsible for implementing
all the programmes in his PHC area. Sector supervisors assist him in monitoring
the progress of various activities. At the village level, an Auxiliary Nurse
Midwife (ANM) manages Sub-centre. She is responsible for implementing all
the programmes in the Sub-centre area, which usually covers 4-6 villages. At
the village level, Village Health Committees have been already constituted
which include ANM, teacher, Anganwadi worker,
7
and Patwari, for implementing various health and family welfare activities at
the village level and enhance community participation in health planning and
monitoring at the grass roots level.
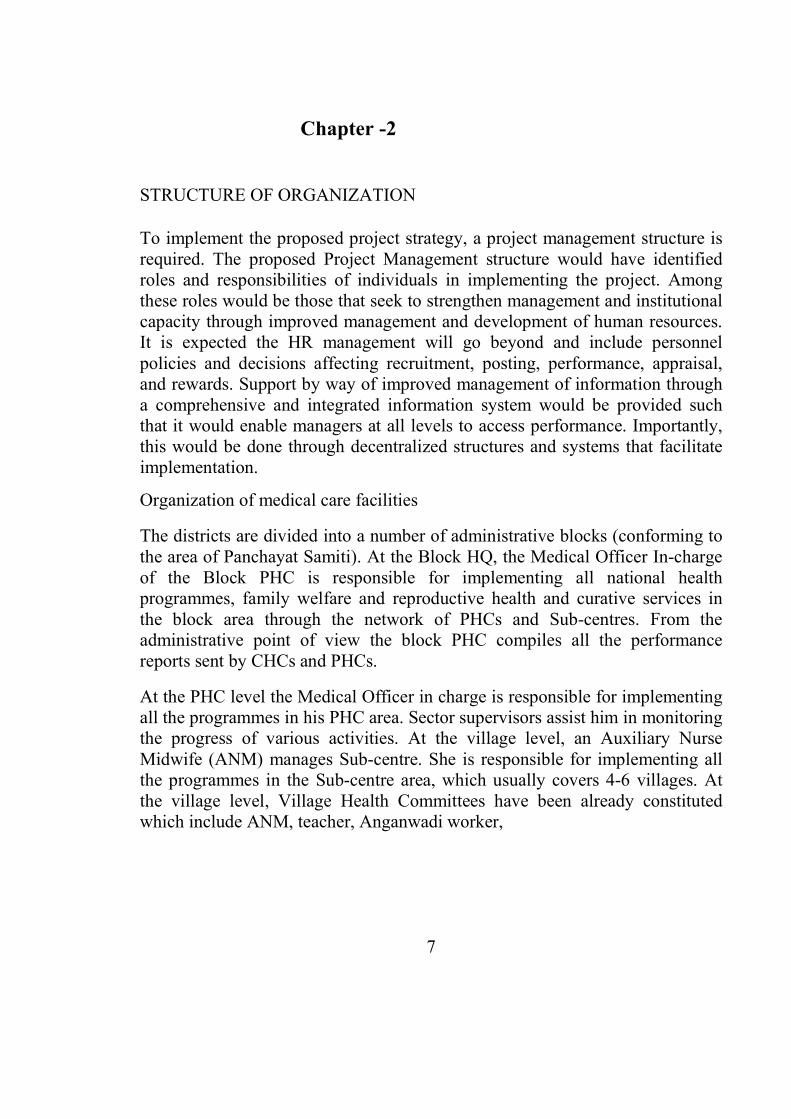
Tertiary Level Medical College
District Hospital
Secondary Level
Sub Division Hospital/ CHC
Block PHC
Primary Level PHC
Sub Centers
Health Care Services Constitute a critical core in the organizational set up of
Medical, Health, and Family welfare services provided through a public system.
In this background Medical, Health and Family welfare Department bears an
onerous responsibility to manage more than 12000 rural health facilities ranging
from sub divisional Hospital/CHC through PHC to sub centre. These facilities
cater to the medical care, health and family welfare needs of three- fourth of the
communities of the State whose total population has already gone beyond 55
million.
8
Administratively:- The State has been divided in to 7 Divisions, 32 Districts,
which are further sub divided in to various peripheral urban/rural health
facilities Viz, DH/CHC/FRU/ PHC and Sub centers etc.
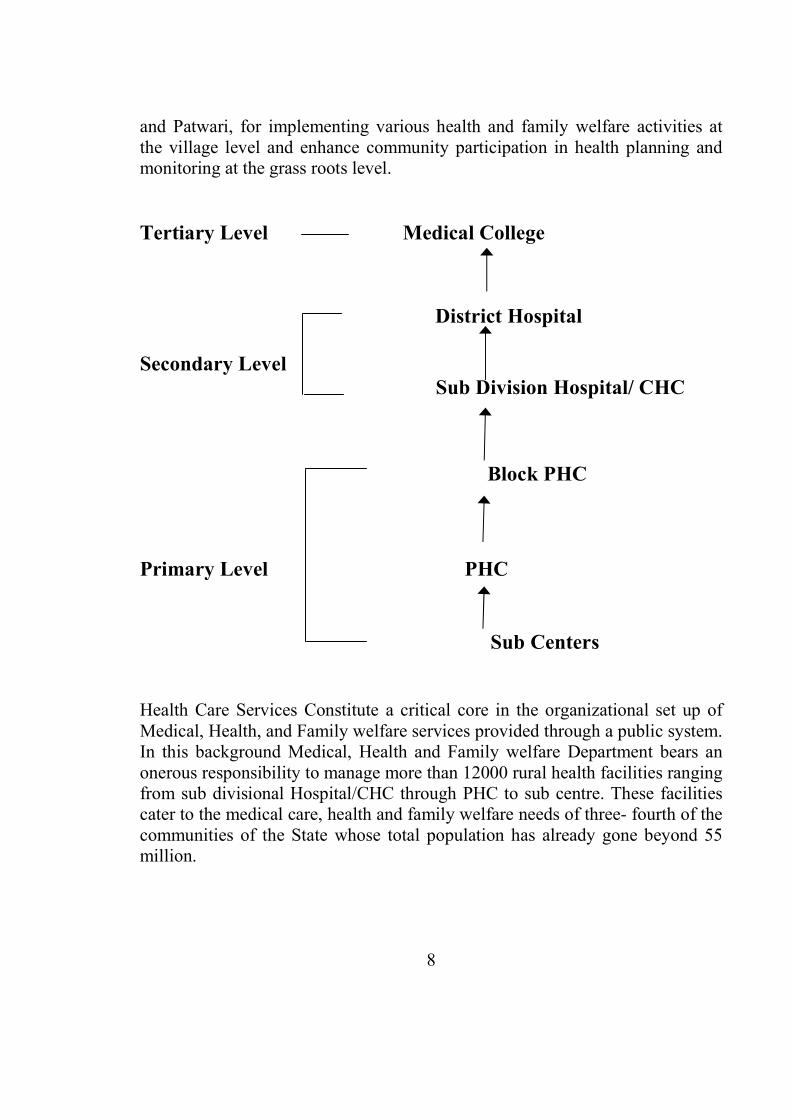
The services at District to village level are provided by the network of health
facilities of different levels determined by their bed strengths as follows:
No. of beds 300 bed 150 bed 100 beds 50 beds 30beds PHC Sub center
No of Hospitals 8 20 12 81 226 1706 10387
9
All beings are born free and equal in dignity and rights
Article 1, UDHR
Chapter -3
LI#KAGE
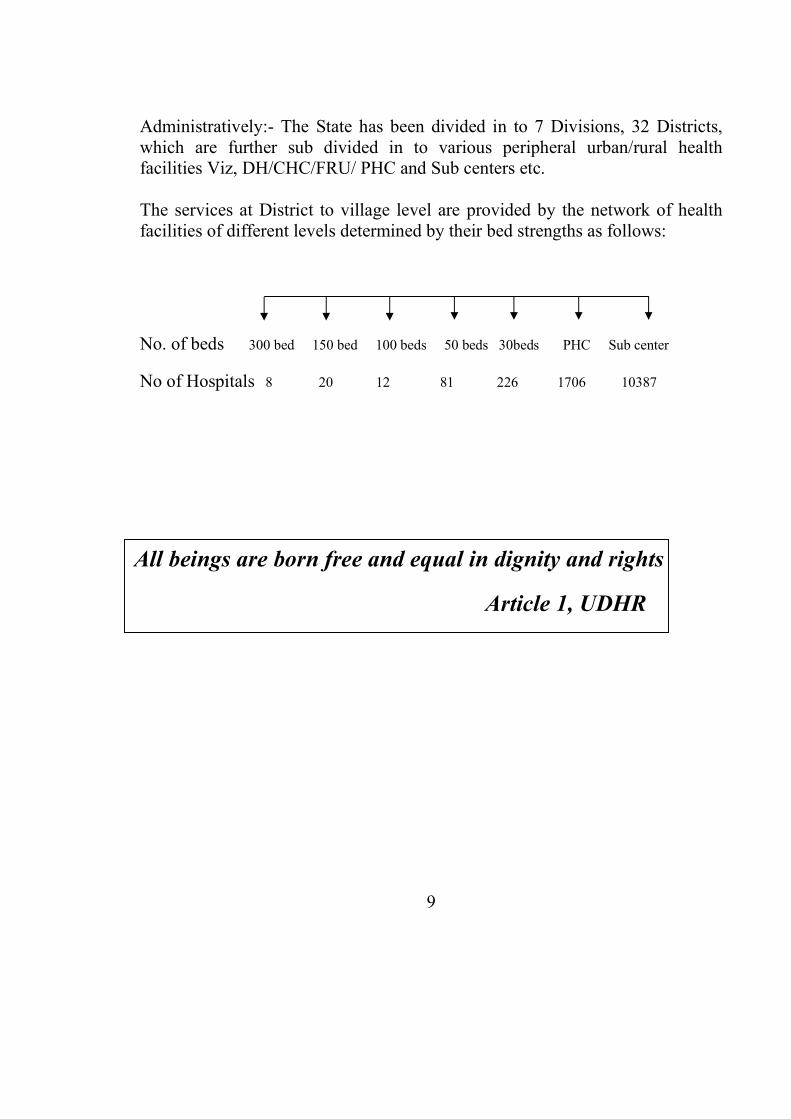
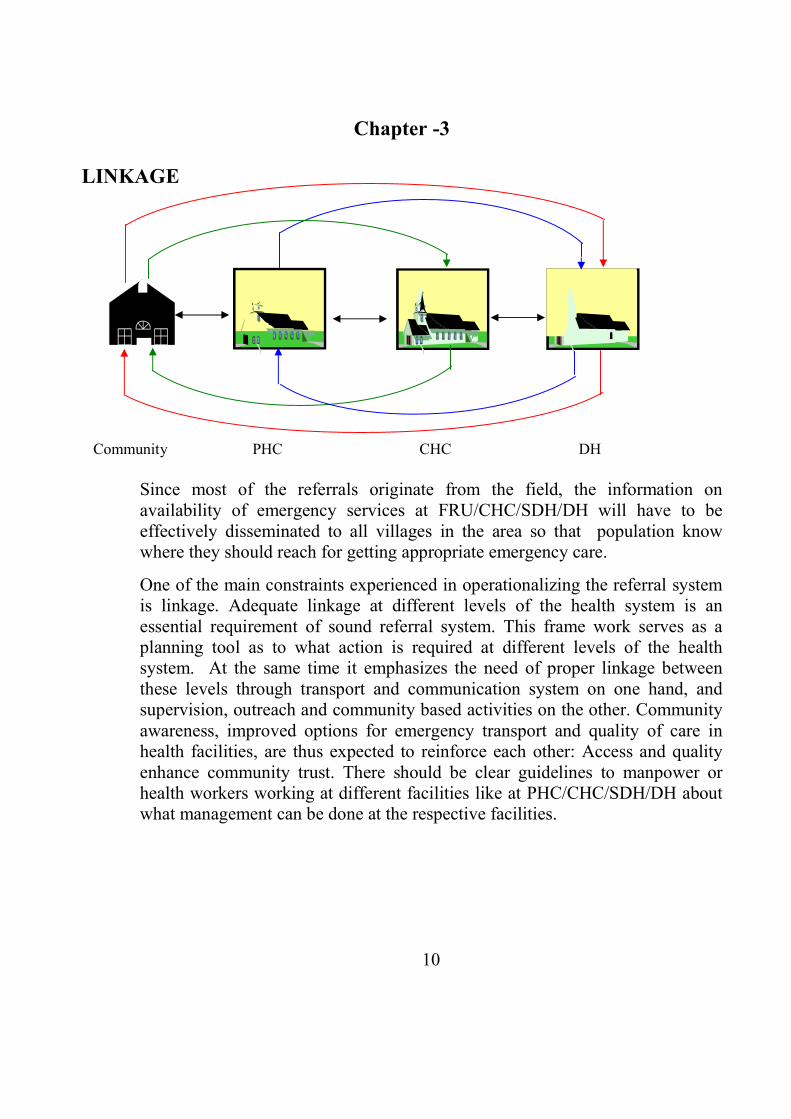
Community PHC CHC DH
Since most of the referrals originate from the field, the information on
availability of emergency services at FRU/CHC/SDH/DH will have to be
effectively disseminated to all villages in the area so that population know
where they should reach for getting appropriate emergency care.
One of the main constraints experienced in operationalizing the referral system
is linkage. Adequate linkage at different levels of the health system is an
essential requirement of sound referral system. This frame work serves as a
planning tool as to what action is required at different levels of the health
system. At the same time it emphasizes the need of proper linkage between
these levels through transport and communication system on one hand, and
supervision, outreach and community based activities on the other. Community
awareness, improved options for emergency transport and quality of care in
health facilities, are thus expected to reinforce each other: Access and quality
enhance community trust. There should be clear guidelines to manpower or
health workers working at different facilities like at PHC/CHC/SDH/DH about
what management can be done at the respective facilities.
10
They should also guide the patient where he needs to go for further diagnosis/
treatment pertaining to the ailment.
Many times, to facilitate appropriate level of reference in cases of emergency
where high risk cases present with threat of life and hierarchy of referral is not
feasible to follow, the cases may be referred directly and immediately to the
higher level facilities as per need. For example in Obstetrics cases of severe
APH/PPH, obstructed/ Complicated labour, Eclampsia, Ectopic Pregrency,
Vesicular Mole and Severe Anemia needs immediate referral. In Paediatrics
viz. cases of Birth Asphyxia, Low Birth rate babies, Meconium Aspiration
Jaundice, Convulsions, Tetanus Neo-natorum, septicemia and congenital
Anomalies may need immediate referral from community /PHC to DH or
Tertiary Level facilities by bypassing the PHC/CHC/SDH/DH.
The referring centre should also communicate relevant information like
investigation carried out with reports there of etc., probable diagnosis and
treatment given. This can be ensured by filling referral cards properly after
careful examination of the patient. To differentiate the cards to be used at
different levels (upwards and down wards), separate colors have been used.
Proper receipt and monitoring of these cards will be verified through referral
register (enclosed). District level officers such as PMO, CMHO and district
project officer will be required to monitor the referral system regularly so that,
the prescribed linkage chain is not disrupted.
Referral system is a system of team work and to manage the referral system
meticulously, the formation of referral committee at district level are suggested.
The proposed project coordination and monitoring committee at district level
will ensure creation of a District Referral Committee at each district hospital.
The committee will consist of PMO, CM&HO, DY. CM&HO, at sub divisional
level, Medical Officer in charge of Hospital/CHCs located at subdivision,
Medical Officer in charge of all CHCs and superintendents of teaching hospitals
(wherever applicable) . The committee will meet once in a month to monitor
and review entire referral, the follow-ups of referral data will be used for
decision making pertaining to improvement in existing scenario.
11
Decision-Making
Decision Making is really a complex mental exercise in turbulent situations.
Vital decisions are taken in crises, at speed with little time for thought or
consultation. There are four `Cs’ of decision making – checking, consulting,
considering and communicating.
Appropriate timely decision requires better interpersonal relationship between
clients and service providers informing them about causes and seriousness of
their health problems and types of services currently available and their sources.
You have to also provide counseling services wherever needed so that the
clients are enabled to take correct decision for accepting services. This, in turn,
is expected to increase satisfaction with the services received among clients and
thereby further increase the acceptance of services.
Adoption of wrong referral may lead to heighten the cost of treatment and
involving risk of life. Delay in decision making may be defined in phase
manner as below:-
○ Phase 1 delay : Decision-making at community level.
○ Phase 2 delay : Accessibility, transport and communication.
○ Phase 3 delay : Accessibility of appropriate care, quality of care.
Examining the decision-making process regarding primary health care,
especially in pregnancy/childbirth in communities, will highlight both the
‘birth- preparedness’ at community level (delay1), the options for
communication and transport from community to health facility (delay 2) and
the (perceived) quality of care (delay 3).
The risk assessment should be done with out delay at primary level itself and
decision should be communicated to companions of the patient without creating
panicky. Health provider should motivate and be able to help the attendants to
arrive at some decision by way of counseling for referral. He should also
address the relevant information like general condition of patient, prognosis,
probable need of blood transfusion and need of vehicle for shifting the patient
to higher level facilities. In other words helping people to make decisions about
the type of specific health care they need with a minimum inconvenience and
delay.
12
It is no longer our resources that limit our decisions; It’s
our decisions that limit our resources. U Thant
Transport and Communication.
For emergency cases ambulance will be provided to the patient by the MO in
charge of the hospital referring the case. He may also communicate to the
referred specialist simultaneously on telephone (land line/mobile) regarding
status of patient, purpose of referring and services urgently required. Providing
Government procured vehicles should not be seen as the only option for referral
transport. To make local arrangement for referral PRIs, Community members
and NGOs should also be motivated to take part in this process. A social
response for effective communication and transport arrangement for women
experiencing complication can tremendously cut-down delays and save lives.
With the consensus of community leaders a list of vehicles along with owners
available in the village/town should be recorded with the health facilities so that
at the time of crisis these vehicles can be utilized.
In emergency, before transporting the case to higher level facility, treating
physician/medical officer should ensure.
1. The patency of fluid infusion
2. Sufficient quantity and regular supply of oxygen, if required
3. Availability of possible need of drugs during transportation.
The attendant/ companions from family and friends of the same blood group
must accompany the patient so that they might be used as blood donor if need
arises. They should also carry some money in cash for forthcoming
expenditures during treatment.
If necessary and justified by the treating physician a member of
Medical/Trained paramedical staff would escort the referred case. During the
way to higher level facility he will make possible sincere efforts to maintain the
vital signs of the patient with his own knowledge and judgment. At last the
patient will be handed over to receiving institute/ specialist providing out of
queue priority along with referral cards and reports with briefing.
13
Management of Blood
Availability of blood is critical to reducing mortality, as hemorrhage is the
leading cause of accidental and maternal death. Availability of blood is
dependent upon blood donors as it cannot be synthesized artificially even today.
Lack of donors is frequently cited as the cause of unavailability of blood. Blood
banking services by Government should not be seen as the only place of
availability of blood. Strong advocacy in the form of information, education
and counseling (IEC) for blood donation must be undertaken to overcome this
barrier to save the human lives. This advocacy also stems from religious and
cultural values that support the act of giving blood to ensure the health and
survival of others. Alternatively we must also give a thought to involve
voluntary organizations, NGOs and other individuals who come forward of
their own for blood donation.
In context to referrals, medical officer, is a key person who should have good
reputation in the community and among government officials. He should keep
close liaison with the community leaders, persons from ICDS, Revenue,
Auyurved, Police, Education and various social welfare agencies. He must use
his goodwill and do counseling in motivating the volunteers for blood donation.
The attendant of patient should also be made clear regarding the need of blood
at the place where patient is being referred. Following thorough counseling, the
companions should be advised to get ready for blood donation when need
arises.
14
Compassion is a sense of caring or sympathy for the suffering of others that
brings clarity regarding their needs and pain. It is also practical
determination to do whatever is possible to help alleviate their suffering.
Compassion is not true compassion unless it is active. Sogyal Rinpoche
Chapter -4
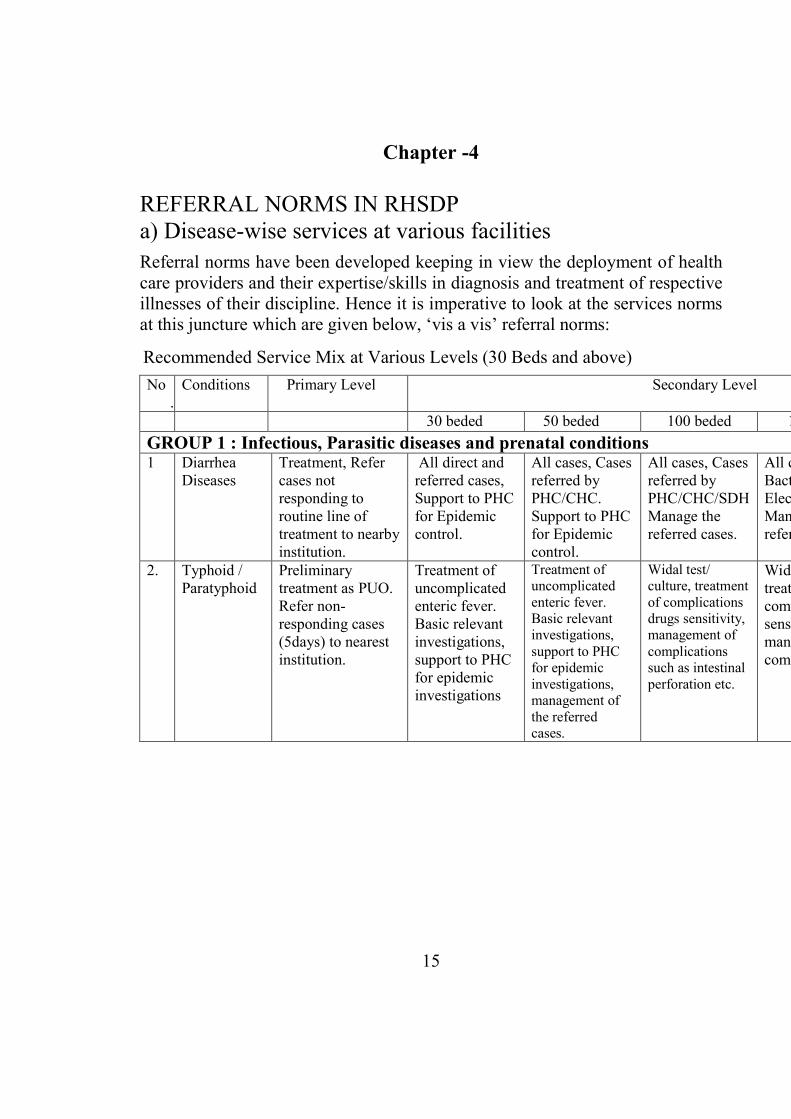
REFERRAL NORMS IN RHSDP
a) Disease-wise services at various facilities
Referral norms have been developed keeping in view the deployment of health
care providers and their expertise/skills in diagnosis and treatment of respective
illnesses of their discipline. Hence it is imperative to look at the services norms
at this juncture which are given below, ‘vis a vis’ referral norms:
Recommended Service Mix at Various Levels (30 Beds and above)
No
.
Conditions Primary Level Secondary Level
30 beded 50 beded 100 beded 150 beded
GROUP 1 : Infectious, Parasitic diseases and prenatal conditions
1 Diarrhea
Diseases
Treatment, Refer
cases not
responding to
routine line of
treatment to nearby
institution.
All direct and
referred cases,
Support to PHC
for Epidemic
control.
All cases, Cases
referred by
PHC/CHC.
Support to PHC
for Epidemic
control.
All cases, Cases
referred by
PHC/CHC/SDH
Manage the
referred cases.
All cases,
Bacteriological,
Electrolyte Test.
Manage the
referred cases.
2. Typhoid /
Paratyphoid
Preliminary
treatment as PUO.
Refer non-
responding cases
(5days) to nearest
institution.
Treatment of
uncomplicated
enteric fever.
Basic relevant
investigations,
support to PHC
for epidemic
investigations
Treatment of
uncomplicated
enteric fever.
Basic relevant
investigations,
support to PHC
for epidemic
investigations,
management of
the referred
cases.
Widal test/
culture, treatment
of complications
drugs sensitivity,
management of
complications
such as intestinal
perforation etc.
Widal test/ culture,
treatment of
complications drugs
sensitivity,
management of
complications.
15
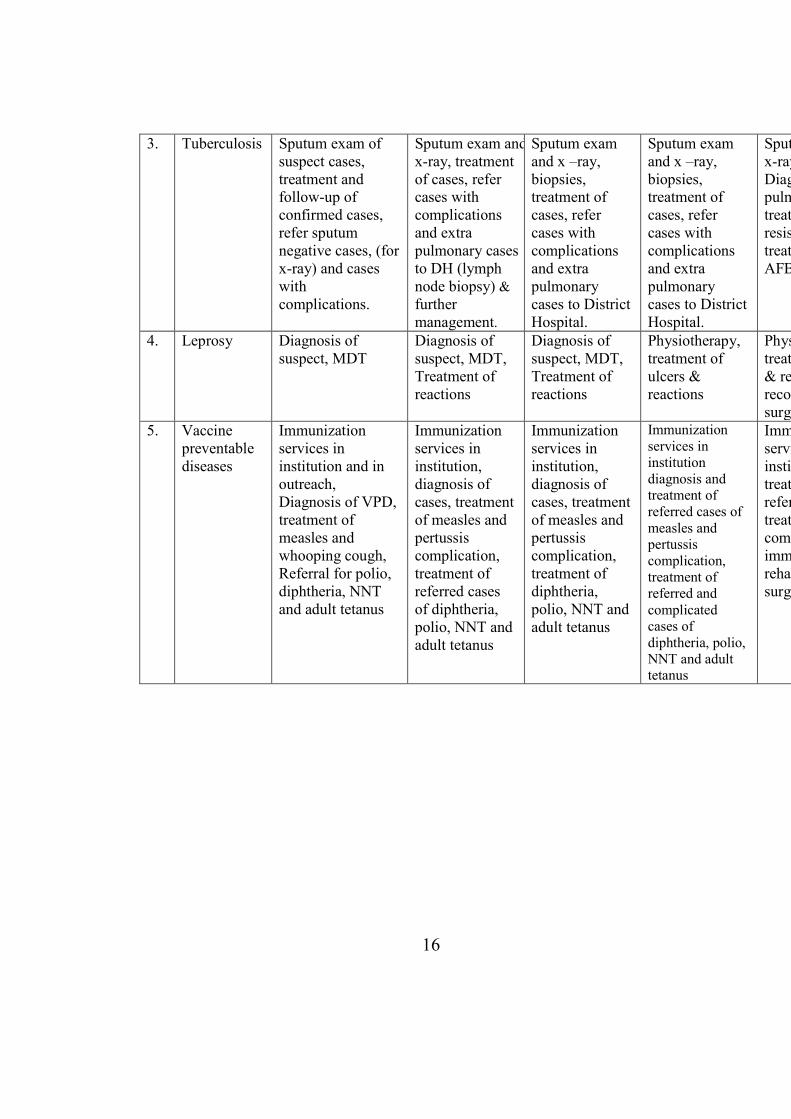
3. Tuberculosis Sputum exam of
suspect cases,
treatment and
follow-up of
confirmed cases,
refer sputum
negative cases, (for
x-ray) and cases
with
complications.
Sputum exam and
x-ray, treatment
of cases, refer
cases with
complications
and extra
pulmonary cases
to DH (lymph
node biopsy) &
further
management.
Sputum exam
and x –ray,
biopsies,
treatment of
cases, refer
cases with
complications
and extra
pulmonary
cases to District
Hospital.
Sputum exam
and x –ray,
biopsies,
treatment of
cases, refer
cases with
complications
and extra
pulmonary
cases to District
Hospital.
Sputum e
x-ray biopsies,
Diagnosis of extra
pulmonary cases,
treatment of
resistant cases,
treatment of TBM,
AFB culture
4. Leprosy Diagnosis of
suspect, MDT
Diagnosis of
suspect, MDT,
Treatment of
reactions
Diagnosis of
suspect, MDT,
Treatment of
reactions
Physiotherapy,
treatment of
ulcers &
reactions
Physiotherapy,
treatment of ulcers
& reactions,
reconstructive
surgery
5. Vaccine
preventable
diseases
Immunization
services in
institution and in
outreach,
Diagnosis of VPD,
treatment of
measles and
whooping cough,
Referral for polio,
diphtheria, NNT
and adult tetanus
Immunization
services in
institution,
diagnosis of
cases, treatment
of measles and
pertussis
complication,
treatment of
referred cases
of diphtheria,
polio, NNT and
adult tetanus
Immunization
services in
institution,
diagnosis of
cases, treatment
of measles and
pertussis
complication,
treatment of
diphtheria,
polio, NNT and
adult tetanus
Immunization
services in
institution
diagnosis and
treatment of
referred cases of
measles and
pertussis
complication,
treatment of
referred and
complicated
cases of
diphtheria, polio,
NNT and adult
tetanus
Immunization
services in
institution,
treatment of
referred cases,
treatment for
complication of
immunization,
rehabilitative
surgery
16
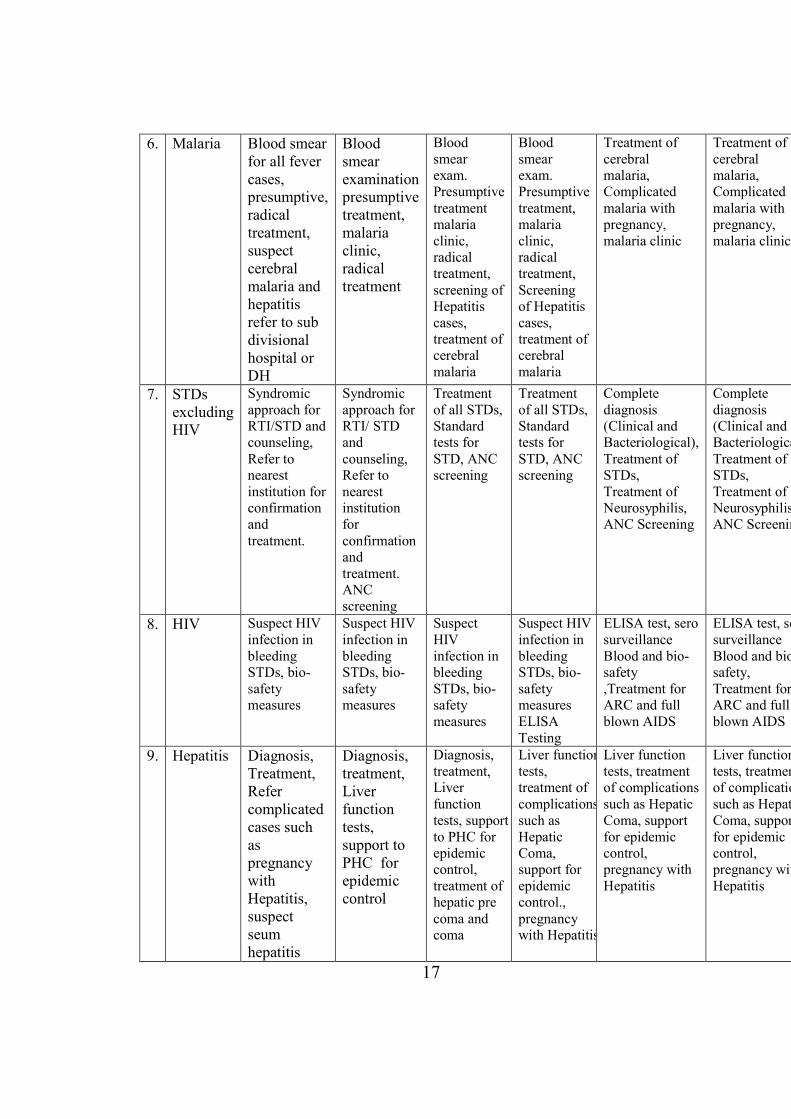
6. Malaria Blood smear
for all fever
cases,
presumptive,
radical
treatment,
suspect
cerebral
malaria and
hepatitis
refer to sub
divisional
hospital or
DH
Blood
smear
examination
presumptive
treatment,
malaria
clinic,
radical
treatment
Blood
smear
exam.
Presumptive
treatment
malaria
clinic,
radical
treatment,
screening of
Hepatitis
cases,
treatment of
cerebral
malaria
Blood
smear
exam.
Presumptive
treatment,
malaria
clinic,
radical
treatment,
Screening
of Hepatitis
cases,
treatment of
cerebral
malaria
Treatment of
cerebral
malaria,
Complicated
malaria with
pregnancy,
malaria clinic
Treatment of
cerebral
malaria,
Complicated
malaria with
pregnancy,
malaria clinic.
7. STDs
excluding
HIV
Syndromic
approach for
RTI/STD and
counseling,
Refer to
nearest
institution for
confirmation
and
treatment.
Syndromic
approach for
RTI/ STD
and
counseling,
Refer to
nearest
institution
for
confirmation
and
treatment.
ANC
screening
Treatment
of all STDs,
Standard
tests for
STD, ANC
screening
Treatment
of all STDs,
Standard
tests for
STD, ANC
screening
Complete
diagnosis
(Clinical and
Bacteriological),
Treatment of
STDs,
Treatment of
Neurosyphilis,
ANC Screening
Complete
diagnosis
(Clinical and
Bacteriological),
Treatment of
STDs,
Treatment of
Neurosyphilis,
ANC Screening
8. HIV Suspect HIV
infection in
bleeding
STDs, bio-
safety
measures
Suspect HIV
infection in
bleeding
STDs, bio-
safety
measures
Suspect
HIV
infection in
bleeding
STDs, bio-
safety
measures
Suspect HIV
infection in
bleeding
STDs, bio-
safety
measures
ELISA
Testing
ELISA test, sero
surveillance
Blood and bio-
safety
,Treatment for
ARC and full
blown AIDS
ELISA test, sero
surveillance
Blood and bio
safety,
Treatment for
ARC and full
blown AIDS
9. Hepatitis Diagnosis,
Treatment,
Refer
complicated
cases such
as
pregnancy
with
Hepatitis,
suspect
seum
hepatitis
Diagnosis,
treatment,
Liver
function
tests,
support to
PHC for
epidemic
control
Diagnosis,
treatment,
Liver
function
tests, support
to PHC for
epidemic
control,
treatment of
hepatic pre
coma and
coma
Liver function
tests,
treatment of
complications
such as
Hepatic
Coma,
support for
epidemic
control.,
pregnancy
with Hepatitis
Liver function
tests, treatment
of complications
such as Hepatic
Coma, support
for epidemic
control,
pregnancy with
Hepatitis
Liver function
tests, treatment
of complications
such as Hepatic
Coma, support
for epidemic
control,
pregnancy with
Hepatitis
17
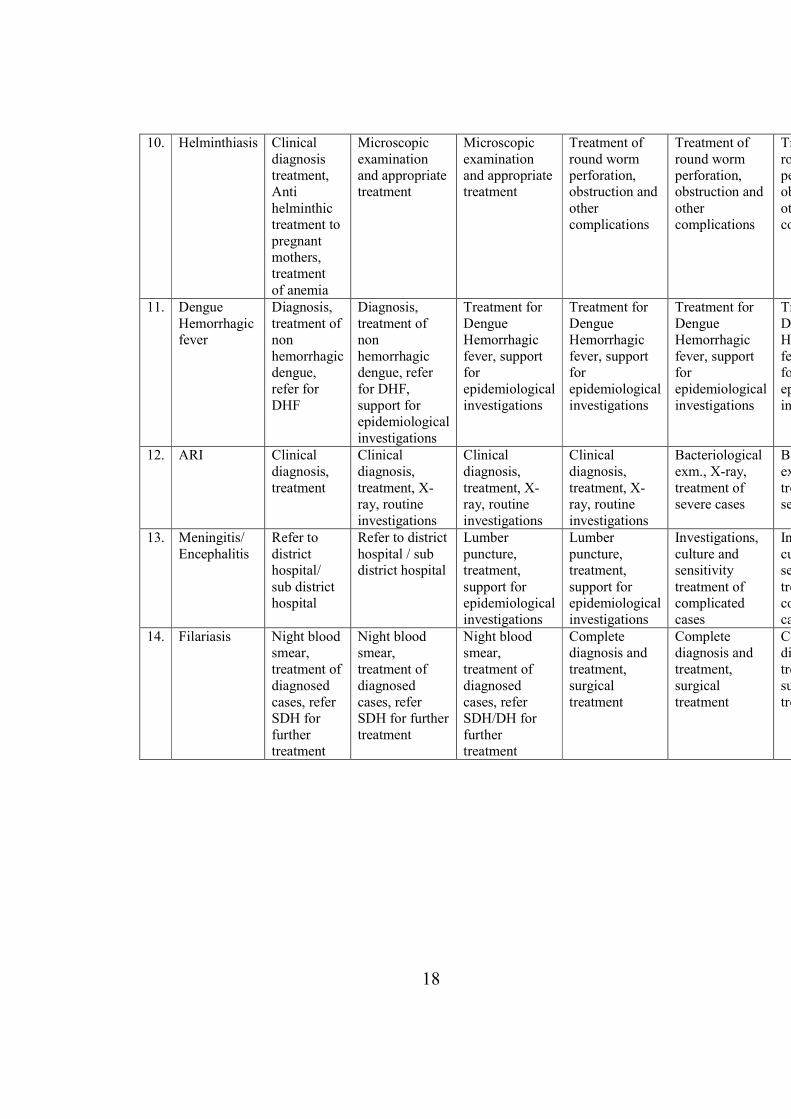
10. Helminthiasis Clinical
diagnosis
treatment,
Anti
helminthic
treatment to
pregnant
mothers,
treatment
of anemia
Microscopic
examination
and appropriate
treatment
Microscopic
examination
and appropriate
treatment
Treatment of
round worm
perforation,
obstruction and
other
complications
Treatment of
round worm
perforation,
obstruction and
other
complications
Treatment of
round worm
perforation,
obstruction and
other
complications
11. Dengue
Hemorrhagic
fever
Diagnosis,
treatment of
non
hemorrhagic
dengue,
refer for
DHF
Diagnosis,
treatment of
non
hemorrhagic
dengue, refer
for DHF,
support for
epidemiological
investigations
Treatment for
Dengue
Hemorrhagic
fever, support
for
epidemiological
investigations
Treatment for
Dengue
Hemorrhagic
fever, support
for
epidemiological
investigations
Treatment for
Dengue
Hemorrhagic
fever, support
for
epidemiological
investigations
Treatment for
Dengue
Hemorrhagic
fever, support
for
epidemiological
investigations
12. ARI Clinical
diagnosis,
treatment
Clinical
diagnosis,
treatment, X-
ray, routine
investigations
Clinical
diagnosis,
treatment, X-
ray, routine
investigations
Clinical
diagnosis,
treatment, X-
ray, routine
investigations
Bacteriological
exm., X-ray,
treatment of
severe cases
Bacteriological
exm.,X
treatment of
severe cases
13. Meningitis/
Encephalitis
Refer to
district
hospital/
sub district
hospital
Refer to district
hospital / sub
district hospital
Lumber
puncture,
treatment,
support for
epidemiological
investigations
Lumber
puncture,
treatment,
support for
epidemiological
investigations
Investigations,
culture and
sensitivity
treatment of
complicated
cases
Investigations,
culture and
sensitivity
treatment of
complicated
cases
14. Filariasis Night blood
smear,
treatment of
diagnosed
cases, refer
SDH for
further
treatment
Night blood
smear,
treatment of
diagnosed
cases, refer
SDH for further
treatment
Night blood
smear,
treatment of
diagnosed
cases, refer
SDH/DH for
further
treatment
Complete
diagnosis and
treatment,
surgical
treatment
Complete
diagnosis and
treatment,
surgical
treatment
Complet
diagnosis and
treatment,
surgical
treatment
18
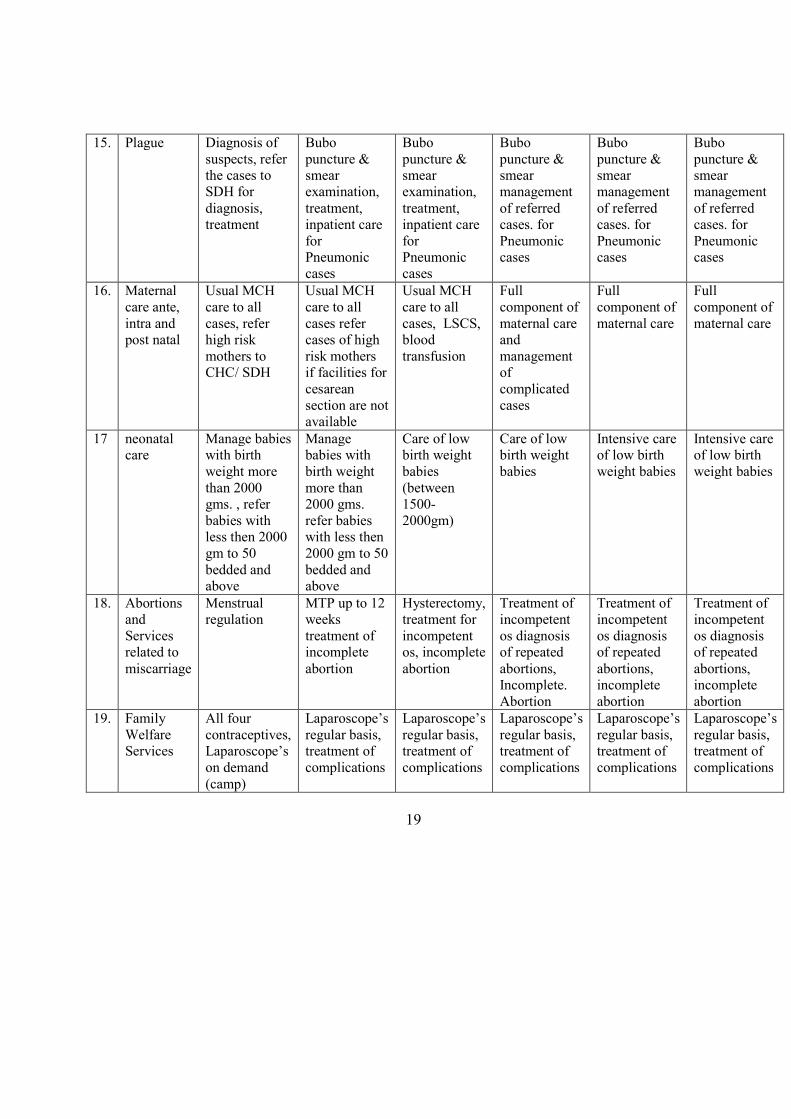
15. Plague Diagnosis of
suspects, refer
the cases to
SDH for
diagnosis,
treatment
Bubo
puncture &
smear
examination,
treatment,
inpatient care
for
Pneumonic
cases
Bubo
puncture &
smear
examination,
treatment,
inpatient care
for
Pneumonic
cases
Bubo
puncture &
smear
management
of referred
cases. for
Pneumonic
cases
Bubo
puncture &
smear
management
of referred
cases. for
Pneumonic
cases
Bubo
puncture &
smear
management
of referred
cases. for
Pneumonic
cases
16. Maternal
care ante,
intra and
post natal
Usual MCH
care to all
cases, refer
high risk
mothers to
CHC/ SDH
Usual MCH
care to all
cases refer
cases of high
risk mothers
if facilities for
cesarean
section are not
available
Usual MCH
care to all
cases, LSCS,
blood
transfusion
Full
component of
maternal care
and
management
of
complicated
cases
Full
component of
maternal care
Full
component of
maternal care
17 neonatal
care
Manage babies
with birth
weight more
than 2000
gms. , refer
babies with
less then 2000
gm to 50
bedded and
above
Manage
babies with
birth weight
more than
2000 gms.
refer babies
with less then
2000 gm to 50
bedded and
above
Care of low
birth weight
babies
(between
1500-
2000gm)
Care of low
birth weight
babies
Intensive care
of low birth
weight babies
Intensive care
of low birth
weight babies
18. Abortions
and
Services
related to
miscarriage
Menstrual
regulation
MTP up to 12
weeks
treatment of
incomplete
abortion
Hysterectomy,
treatment for
incompetent
os, incomplete
abortion
Treatment of
incompetent
os diagnosis
of repeated
abortions,
Incomplete.
Abortion
Treatment of
incompetent
os diagnosis
of repeated
abortions,
incomplete
abortion
Treatment of
incompetent
os diagnosis
of repeated
abortions,
incomplete
abortion
19. Family
Welfare
Services
All four
contraceptives,
Laparoscope’s
on demand
(camp)
Laparoscope’s
regular basis,
treatment of
complications
Laparoscope’s
regular basis,
treatment of
complications
Laparoscope’s
regular basis,
treatment of
complications
Laparoscope’s
regular basis,
treatment of
complications
Laparoscope’s
regular basis,
treatment of
complications
19
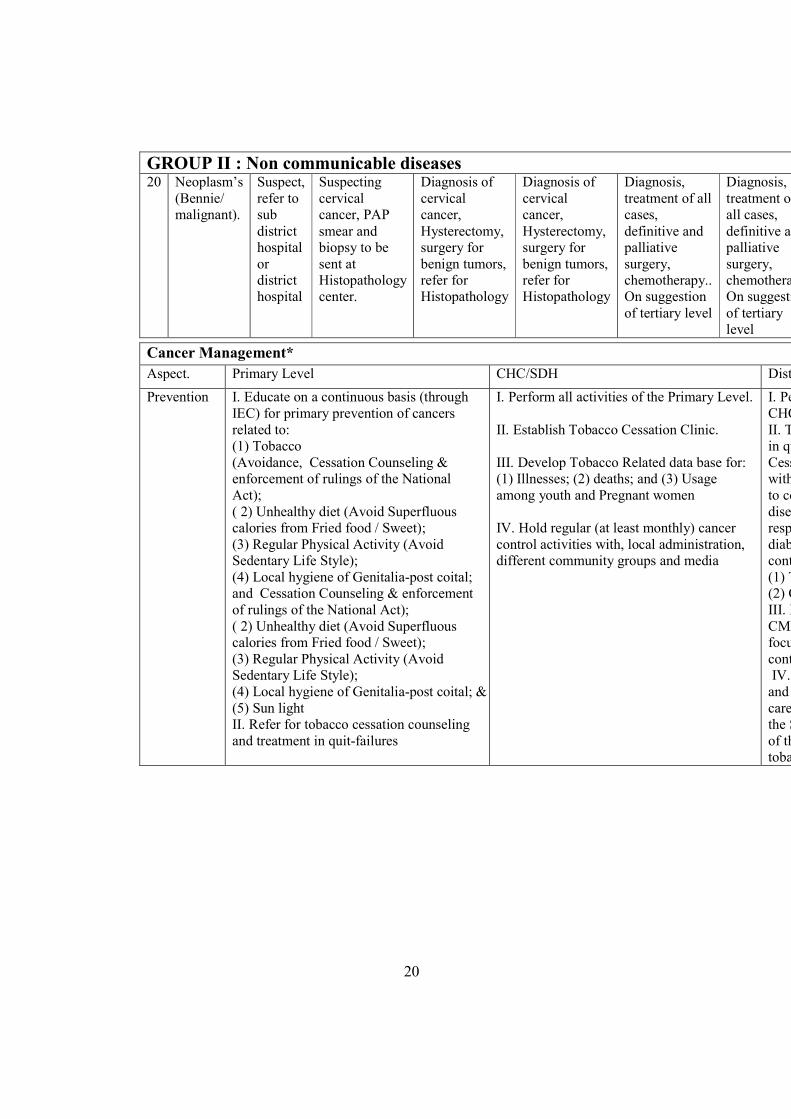
GROUP II : #on communicable diseases
20
Neoplasm’s
(Bennie/
malignant).
Suspect,
refer to
sub
district
hospital
or
district
hospital
Suspecting
cervical
cancer, PAP
smear and
biopsy to be
sent at
Histopathology
center.
Diagnosis of
cervical
cancer,
Hysterectomy,
surgery for
benign tumors,
refer for
Histopathology
Diagnosis of
cervical
cancer,
Hysterectomy,
surgery for
benign tumors,
refer for
Histopathology
Diagnosis,
treatment of all
cases,
definitive and
palliative
surgery,
chemotherapy..
On suggestion
of tertiary level
Diagnosis,
treatment of
all cases,
definitive and
palliative
surgery,
chemotherapy.
On suggestion
of tertiary
level
Cancer Management*
Aspect. Primary Level CHC/SDH District Hospital
Prevention I. Educate on a continuous basis (through
IEC) for primary prevention of cancers
related to:
(1) Tobacco
(Avoidance, Cessation Counseling &
enforcement of rulings of the National
Act);
( 2) Unhealthy diet (Avoid Superfluous
calories from Fried food / Sweet);
(3) Regular Physical Activity (Avoid
Sedentary Life Style);
(4) Local hygiene of Genitalia-post coital;
and Cessation Counseling & enforcement
of rulings of the National Act);
( 2) Unhealthy diet (Avoid Superfluous
calories from Fried food / Sweet);
(3) Regular Physical Activity (Avoid
Sedentary Life Style);
(4) Local hygiene of Genitalia-post coital; &
(5) Sun light
II. Refer for tobacco cessation counseling
and treatment in quit-failures
I. Perform all activities of the Primary Level.
II. Establish Tobacco Cessation Clinic.
III. Develop Tobacco Related data base for:
(1) Illnesses; (2) deaths; and (3) Usage
among youth and Pregnant women
IV. Hold regular (at least monthly) cancer
control activities with, local administration,
different community groups and media
I. Perform all the activities of
CHC/SDH Level.
II. Target an annual 5% increase
in quit rate through Tobacco
Cessation Clinic. Collaborate
with t
to control non
diseases (including heart
respiratory diseases and
diabetes) through optimal
controls for:
(1) Tobacco; and
(2) Obesity.
III. Hold regular (quarterly)
CMEs” on Cancer Control with
focus on Tobac
controls.
IV. Networking cooperation
and collaboration with tertiary
care centers within
the State for primary prevention
of the most frequent cancers; for
tobacco control on priority.
20
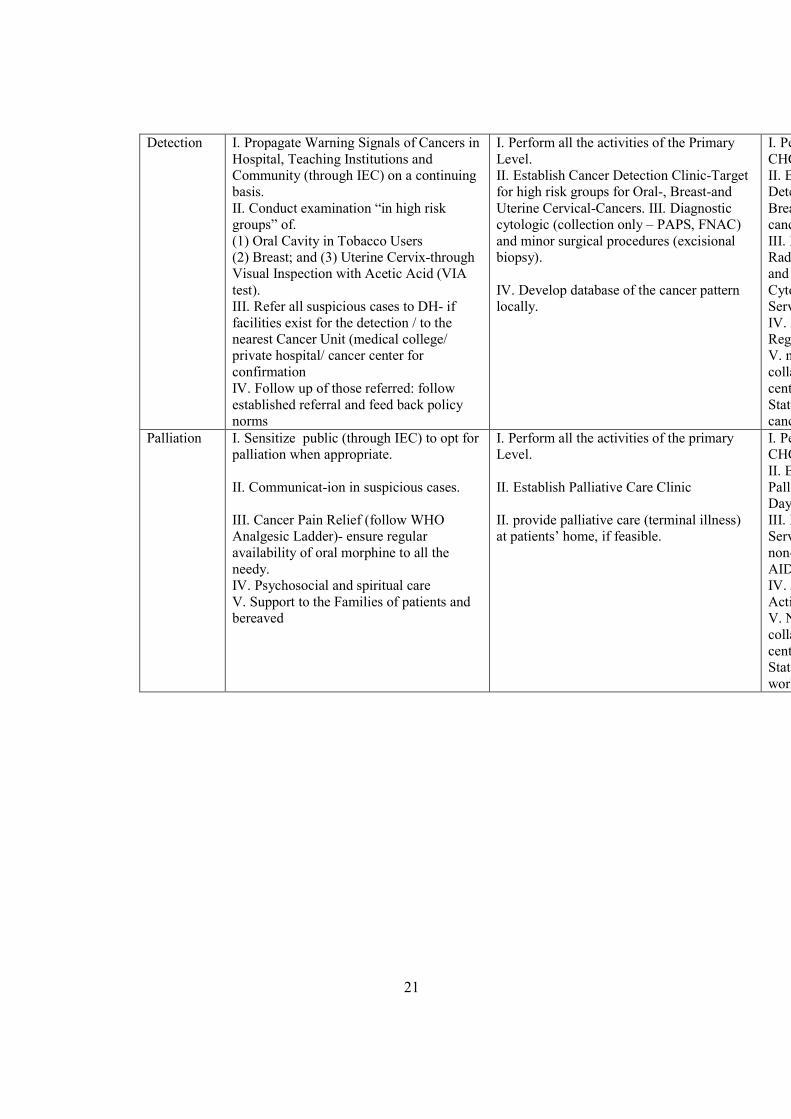
Detection
I. Propagate Warning Signals of Cancers in
Hospital, Teaching Institutions and
Community (through IEC) on a continuing
basis.
II. Conduct examination “in high risk
groups” of.
(1) Oral Cavity in Tobacco Users
(2) Breast; and (3) Uterine Cervix-through
Visual Inspection with Acetic Acid (VIA
test).
III. Refer all suspicious cases to DH- if
facilities exist for the detection / to the
nearest Cancer Unit (medical college/
private hospital/ cancer center for
confirmation
IV. Follow up of those referred: follow
established referral and feed back policy
norms
I. Perform all the activities of the Primary
Level.
II. Establish Cancer Detection Clinic-Target
for high risk groups for Oral-, Breast-and
Uterine Cervical-Cancers. III. Diagnostic
cytologic (collection only – PAPS, FNAC)
and minor surgical procedures (excisional
biopsy).
IV. Develop database of the cancer pattern
locally.
I. Perform all the activities of
CHC/SDH Level.
II. Establish Early Cancer
Detection Programme for Oral
Breast
cancers.
III. Develop Endoscopy_,
Radio
and ultra
Cytology
Services
IV. Develop District Cancer
Registry.
V. networking cooperation and
collaboration with tertiary care
centers within
State for early detection of
cancers and cancer registry.
Palliation I. Sensitize public (through IEC) to opt for
palliation when appropriate.
II. Communicat-ion in suspicious cases.
III. Cancer Pain Relief (follow WHO
Analgesic Ladder)- ensure regular
availability of oral morphine to all the
needy.
IV. Psychosocial and spiritual care
V. Support to the Families of patients and
bereaved
I. Perform all the activities of the primary
Level.
II. Establish Palliative Care Clinic
II. provide palliative care (terminal illness)
at patients’ home, if feasible.
I. Perform all the activities of
CHC/SDH Level.
II. Establish an In
Palliative Care Unit along with a
Day
III. Extend Palliative Care
Services to patients with oth
non-
AIDS.
IV. Audit Palliative Care
Activities.
V. Networking cooperation and
collaboration with tertiary care
centers within
State including CMEs’ and
workshops.
21
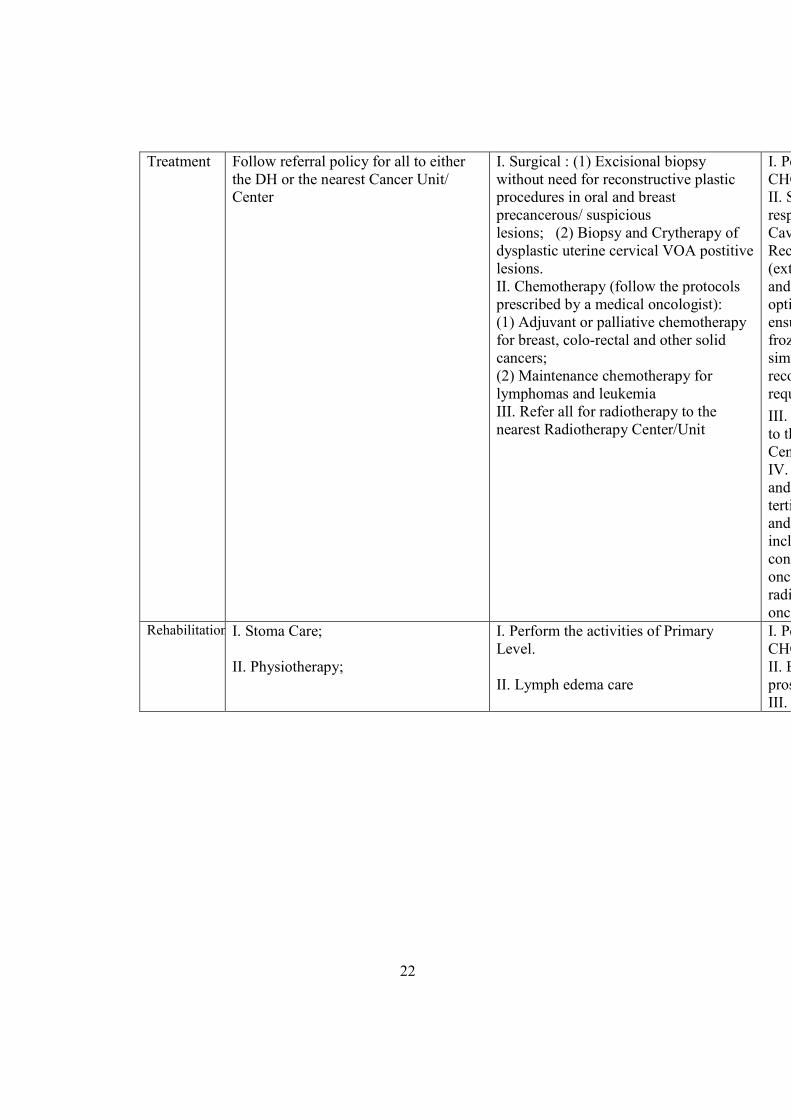
Treatment Follow referral policy for all to either
the DH or the nearest Cancer Unit/
Center
I. Surgical : (1) Excisional biopsy
without need for reconstructive plastic
procedures in oral and breast
precancerous/ suspicious
lesions; (2) Biopsy and Crytherapy of
dysplastic uterine cervical VOA postitive
lesions.
II. Chemotherapy (follow the protocols
prescribed by a medical oncologist):
(1) Adjuvant or palliative chemotherapy
for breast, colo-rectal and other solid
cancers;
(2) Maintenance chemotherapy for
lymphomas and leukemia
III. Refer all for radiotherapy to the
nearest Radiotherapy Center/Unit
I. Perform all the activities of
CHC/SDH Level.
II. Surgical treatment of
respectable cancers of : Oral
Cavity, Breast, Colon and
Rectum, Male
(external)
and Soft tissue, provided an
optimal respectability can be
ensured without a need for
frozen control and a
simultaneous (one
reconstruction procedure (if
required ) can be performed.
III. Refer all for radiotherapy
to the nearest Ra
Center/unit
IV. Networking, cooperation
and colloaboration with
tertiary care centers within
and outside
including CMEs’ and
conferences on surgical
oncology and principles of
radiation
oncology.Rehabilitation I. Stoma Care;
II. Physiotherapy;
I. Perform the activities of Primary
Level.
II. Lymph edema care
I. Perform all the activities of
CHC/SDH Level.
II. Breast, Limb and other
prosthesis.
III. Occupational therapy.
22
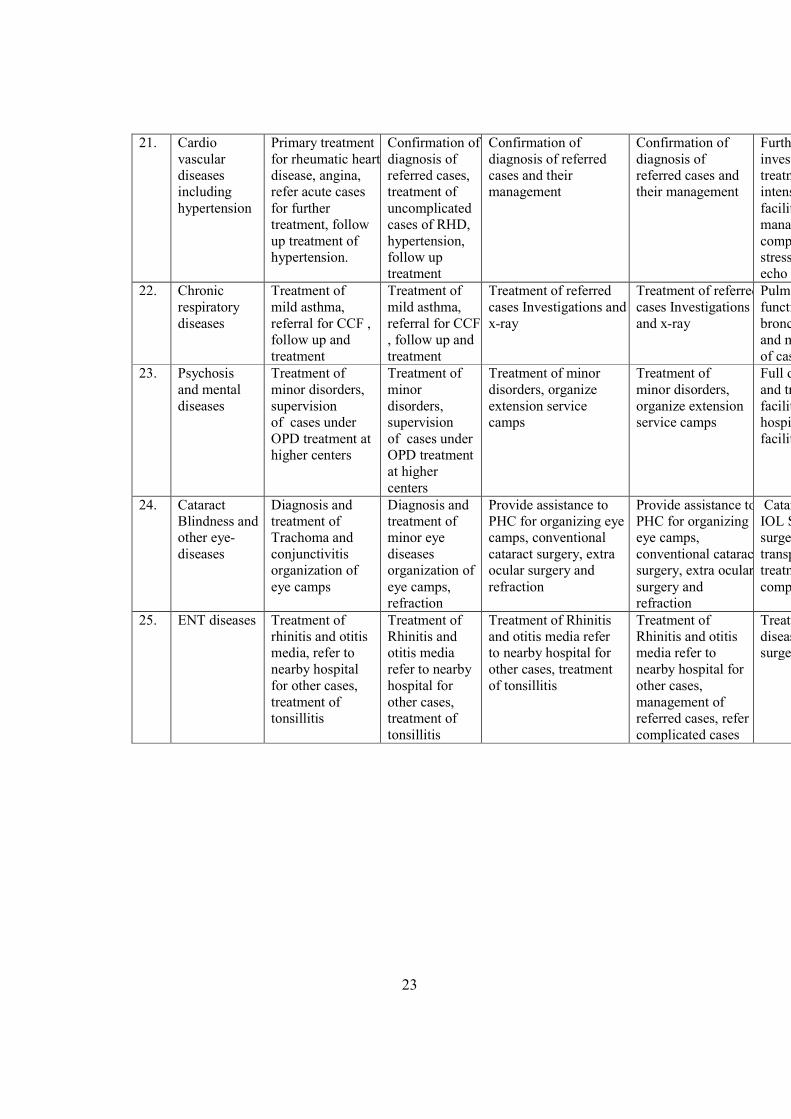
21. Cardio
vascular
diseases
including
hypertension
Primary treatment
for rheumatic heart
disease, angina,
refer acute cases
for further
treatment, follow
up treatment of
hypertension.
Confirmation of
diagnosis of
referred cases,
treatment of
uncomplicated
cases of RHD,
hypertension,
follow up
treatment
Confirmation of
diagnosis of referred
cases and their
management
Confirmation of
diagnosis of
referred cases and
their management
Further
investigation and
treatment,
intensive care unit
facility,
management of
complicated case
stress test, 2 D
echo
22. Chronic
respiratory
diseases
Treatment of
mild asthma,
referral for CCF ,
follow up and
treatment
Treatment of
mild asthma,
referral for CCF
, follow up and
treatment
Treatment of referred
cases Investigations and
x-ray
Treatment of referred
cases Investigations
and x-ray
Pulmonary
function tests
bronchoscope
and management
of cases.
23. Psychosis
and mental
diseases
Treatment of
minor disorders,
supervision
of cases under
OPD treatment at
higher centers
Treatment of
minor
disorders,
supervision
of cases under
OPD treatment
at higher
centers
Treatment of minor
disorders, organize
extension service
camps
Treatment of
minor disorders,
organize extension
service camps
Full diagnostic
and treatment
facilities,
hospitalization
facility
24. Cataract
Blindness and
other eye-
diseases
Diagnosis and
treatment of
Trachoma and
conjunctivitis
organization of
eye camps
Diagnosis and
treatment of
minor eye
diseases
organization of
eye camps,
refraction
Provide assistance to
PHC for organizing eye
camps, conventional
cataract surgery, extra
ocular surgery and
refraction
Provide assistance to
PHC for organizing
eye camps,
conventional cataract
surgery, extra ocular
surgery and
refraction
Cataract surgery
IOL Squint
surgery corneal
transplant,
treatment of
complication
25. ENT diseases Treatment of
rhinitis and otitis
media, refer to
nearby hospital
for other cases,
treatment of
tonsillitis
Treatment of
Rhinitis and
otitis media
refer to nearby
hospital for
other cases,
treatment of
tonsillitis
Treatment of Rhinitis
and otitis media refer
to nearby hospital for
other cases, treatment
of tonsillitis
Treatment of
Rhinitis and otitis
media refer to
nearby hospital for
other cases,
management of
referred cases, refer
complicated cases
Treatment of all
diseases, ENT
surgery
23
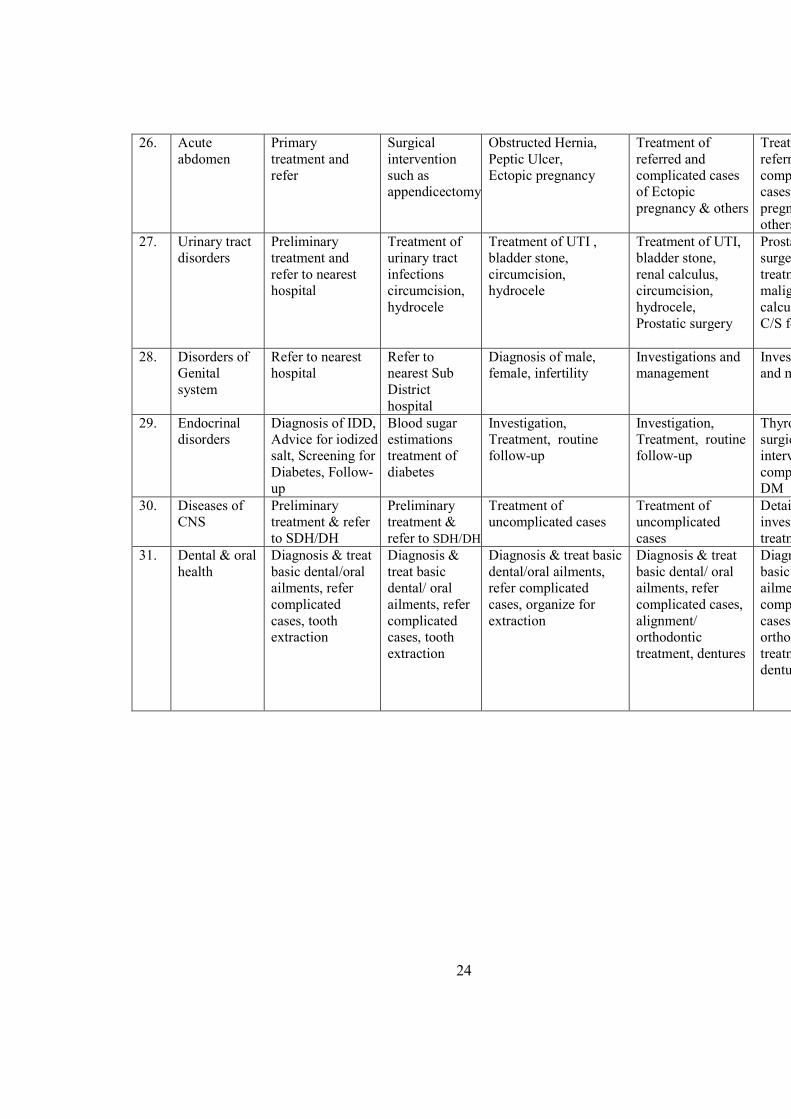
26. Acute
abdomen
Primary
treatment and
refer
Surgical
intervention
such as
appendicectomy
Obstructed Hernia,
Peptic Ulcer,
Ectopic pregnancy
Treatment of
referred and
complicated cases
of Ectopic
pregnancy & others
Treatment of
referred and
complicated
cases of Ectopic
pregnancy &
others
27. Urinary tract
disorders
Preliminary
treatment and
refer to nearest
hospital
Treatment of
urinary tract
infections
circumcision,
hydrocele
Treatment of UTI ,
bladder stone,
circumcision,
hydrocele
Treatment of UTI,
bladder stone,
renal calculus,
circumcision,
hydrocele,
Prostatic surgery
Prostatic, ureteric
surgery,
treatment of
malignancies,
calculus disease,
C/S for infections
28. Disorders of
Genital
system
Refer to nearest
hospital
Refer to
nearest Sub
District
hospital
Diagnosis of male,
female, infertility
Investigations and
management
Investigations
and management
29. Endocrinal
disorders
Diagnosis of IDD,
Advice for iodized
salt, Screening for
Diabetes, Follow-
up
Blood sugar
estimations
treatment of
diabetes
Investigation,
Treatment, routine
follow-up
Investigation,
Treatment, routine
follow-up
Thyroid assay,
surgical
interventi
complete care of
DM
30. Diseases of
CNS
Preliminary
treatment & refer
to SDH/DH
Preliminary
treatment &
refer to SDH/DH
Treatment of
uncomplicated cases
Treatment of
uncomplicated
cases
Detailed
investigation and
treatment
31. Dental & oral
health
Diagnosis & treat
basic dental/oral
ailments, refer
complicated
cases, tooth
extraction
Diagnosis &
treat basic
dental/ oral
ailments, refer
complicated
cases, tooth
extraction
Diagnosis & treat basic
dental/oral ailments,
refer complicated
cases, organize for
extraction
Diagnosis & treat
basic dental/ oral
ailments, refer
complicated cases,
alignment/
orthodontic
treatment, dentures
Diagnosis & treat
basic dental/
ailments, refer
complicated
cases, alignment/
orthodontic
treatment,
dentures
24
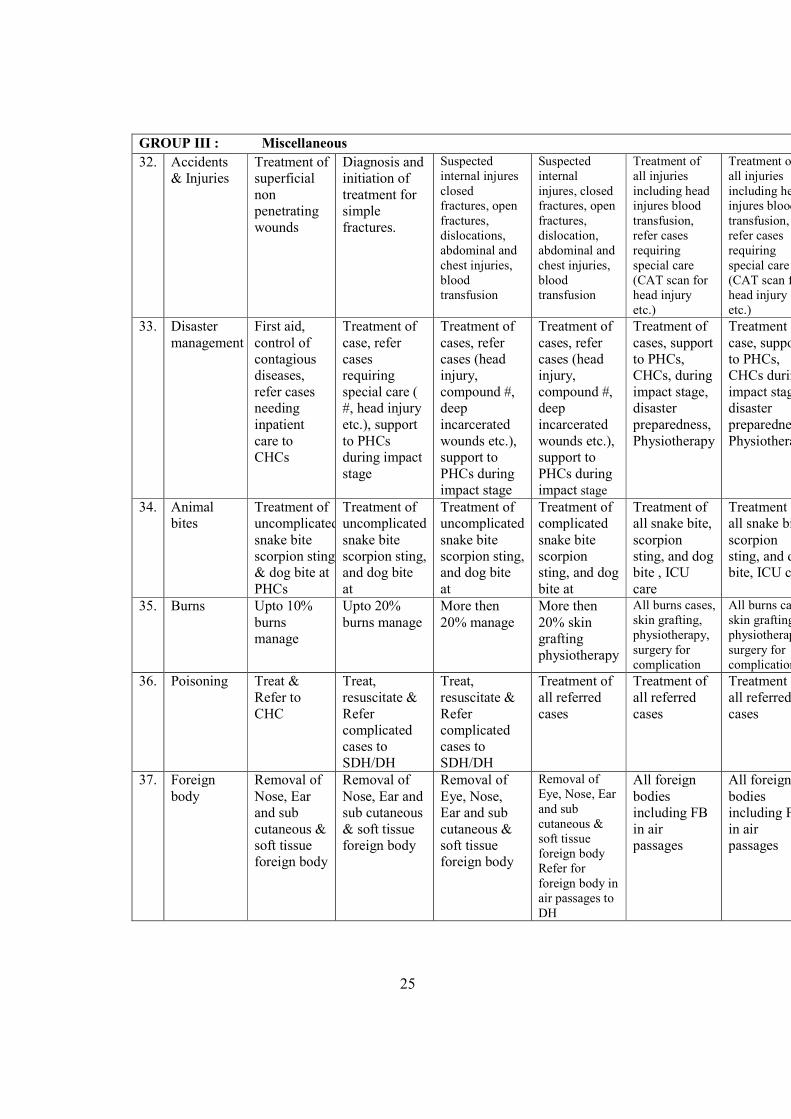
GROUP III : Miscellaneous
32. Accidents
& Injuries
Treatment of
superficial
non
penetrating
wounds
Diagnosis and
initiation of
treatment for
simple
fractures.
Suspected
internal injures
closed
fractures, open
fractures,
dislocations,
abdominal and
chest injuries,
blood
transfusion
Suspected
internal
injures, closed
fractures, open
fractures,
dislocation,
abdominal and
chest injuries,
blood
transfusion
Treatment of
all injuries
including head
injures blood
transfusion,
refer cases
requiring
special care
(CAT scan for
head injury
etc.)
Treatment of
all injuries
including head
injures blood
transfusion,
refer cases
requiring
special care
(CAT scan for
head injury
etc.)
33. Disaster
management
First aid,
control of
contagious
diseases,
refer cases
needing
inpatient
care to
CHCs
Treatment of
case, refer
cases
requiring
special care (
#, head injury
etc.), support
to PHCs
during impact
stage
Treatment of
cases, refer
cases (head
injury,
compound #,
deep
incarcerated
wounds etc.),
support to
PHCs during
impact stage
Treatment of
cases, refer
cases (head
injury,
compound #,
deep
incarcerated
wounds etc.),
support to
PHCs during
impact stage
Treatment of
cases, support
to PHCs,
CHCs, during
impact stage,
disaster
preparedness,
Physiotherapy
Treatment of
case, support
to PHCs,
CHCs during
impact stage,
disaster
preparedness,
Physiotherapy
34. Animal
bites
Treatment of
uncomplicated
snake bite
scorpion sting,
& dog bite at
PHCs
Treatment of
uncomplicated
snake bite
scorpion sting,
and dog bite
at
Treatment of
uncomplicated
snake bite
scorpion sting,
and dog bite
at
Treatment of
complicated
snake bite
scorpion
sting, and dog
bite at
Treatment of
all snake bite,
scorpion
sting, and dog
bite , ICU
care
Treatment of
all snake bite,
scorpion
sting, and dog
bite, ICU care
35. Burns Upto 10%
burns
manage
Upto 20%
burns manage
More then
20% manage
More then
20% skin
grafting
physiotherapy
All burns cases,
skin grafting,
physiotherapy,
surgery for
complication
All burns case,
skin grafting,
physiotherapy,
surgery for
complication
36. Poisoning Treat &
Refer to
CHC
Treat,
resuscitate &
Refer
complicated
cases to
SDH/DH
Treat,
resuscitate &
Refer
complicated
cases to
SDH/DH
Treatment of
all referred
cases
Treatment of
all referred
cases
Treatment of
all referred
cases
37. Foreign
body
Removal of
Nose, Ear
and sub
cutaneous &
soft tissue
foreign body
Removal of
Nose, Ear and
sub cutaneous
& soft tissue
foreign body
Removal of
Eye, Nose,
Ear and sub
cutaneous &
soft tissue
foreign body
Removal of
Eye, Nose, Ear
and sub
cutaneous &
soft tissue
foreign body
Refer for
foreign body in
air passages to
DH
All foreign
bodies
including FB
in air
passages
All foreign
bodies
including FB
in air
passages
25
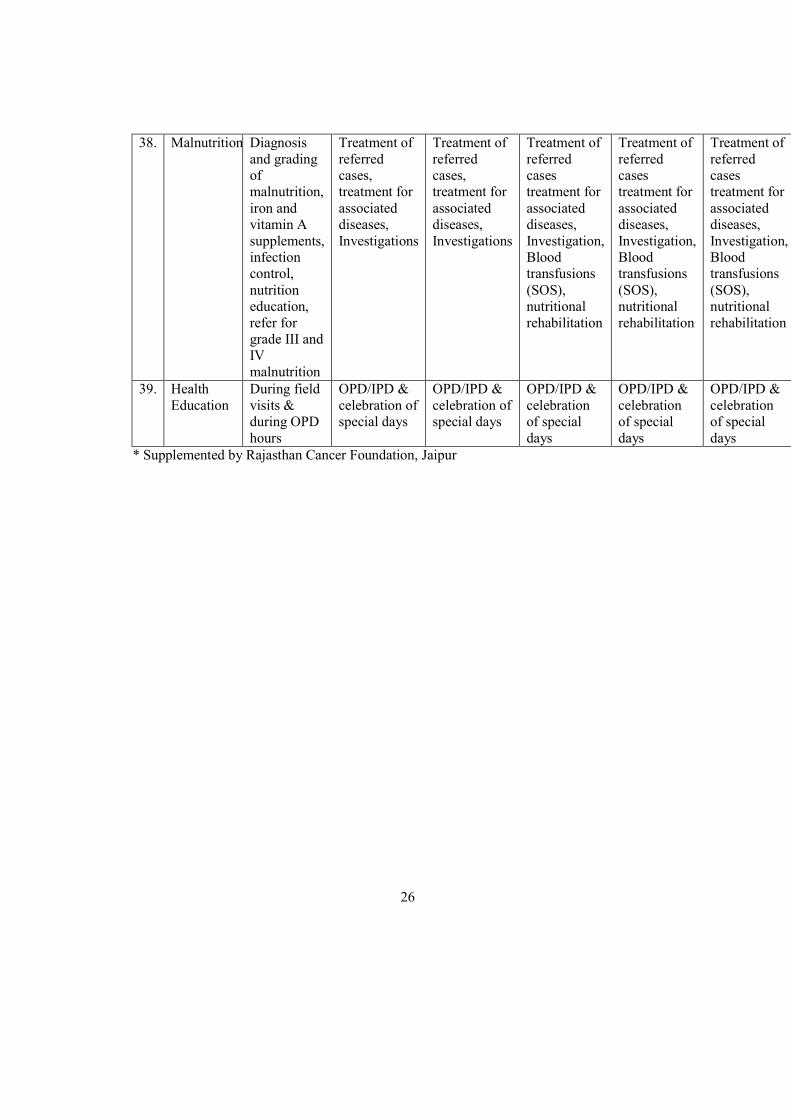
38. Malnutrition Diagnosis
and grading
of
malnutrition,
iron and
vitamin A
supplements,
infection
control,
nutrition
education,
refer for
grade III and
IV
malnutrition
Treatment of
referred
cases,
treatment for
associated
diseases,
Investigations
Treatment of
referred
cases,
treatment for
associated
diseases,
Investigations
Treatment of
referred
cases
treatment for
associated
diseases,
Investigation,
Blood
transfusions
(SOS),
nutritional
rehabilitation
Treatment of
referred
cases
treatment for
associated
diseases,
Investigation,
Blood
transfusions
(SOS),
nutritional
rehabilitation
Treatment of
referred
cases
treatment for
associated
diseases,
Investigation,
Blood
transfusions
(SOS),
nutritional
rehabilitation
39. Health
Education
During field
visits &
during OPD
hours
OPD/IPD &
celebration of
special days
OPD/IPD &
celebration of
special days
OPD/IPD &
celebration
of special
days
OPD/IPD &
celebration
of special
days
OPD/IPD &
celebration
of special
days
* Supplemented by Rajasthan Cancer Foundation, Jaipur
26
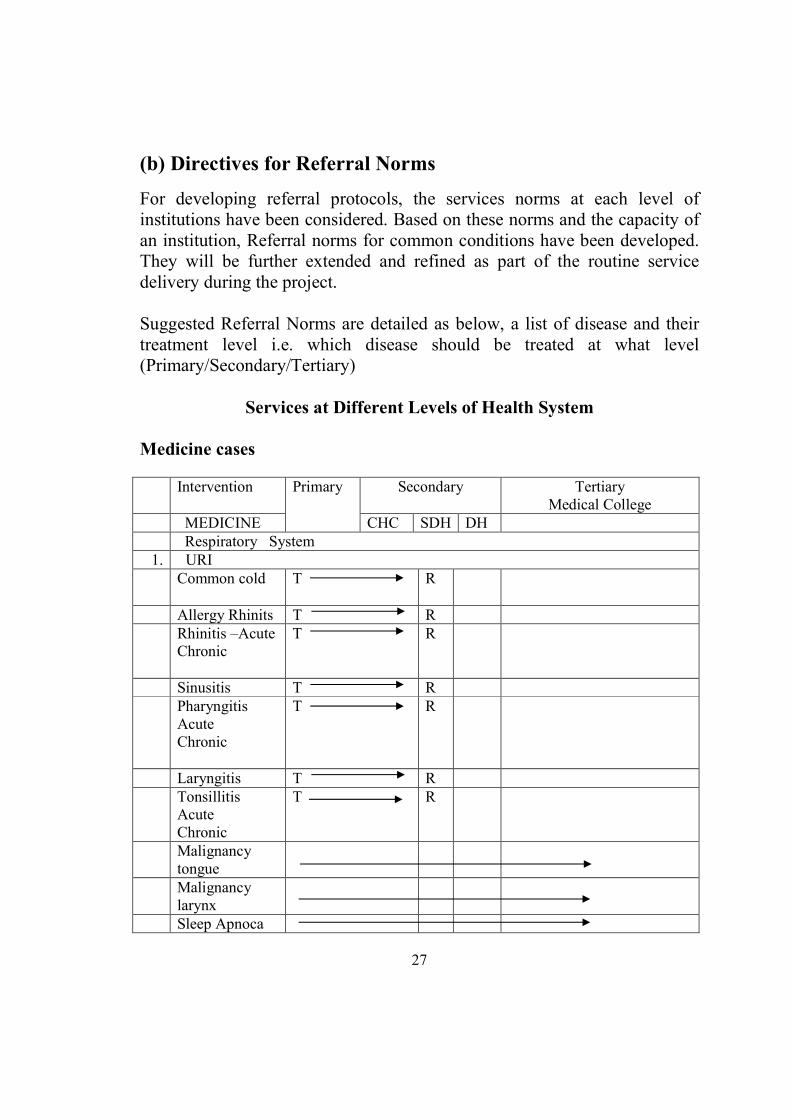
(b) Directives for Referral #orms
For developing referral protocols, the services norms at each level of
institutions have been considered. Based on these norms and the capacity of
an institution, Referral norms for common conditions have been developed.
They will be further extended and refined as part of the routine service
delivery during the project.
Suggested Referral Norms are detailed as below, a list of disease and their
treatment level i.e. which disease should be treated at what level
(Primary/Secondary/Tertiary)
Services at Different Levels of Health System
Medicine cases
Intervention Primary Secondary Tertiary
Medical College
MEDICINE CHC SDH DH
Respiratory System
1. URI
Common cold T R
Allergy Rhinits T R
Rhinitis –Acute
Chronic
T R
Sinusitis T R
Pharyngitis
Acute
Chronic
T R
Laryngitis T R
Tonsillitis
Acute
Chronic
T R
Malignancy
tongue
Malignancy
larynx
Sleep Apnoca
27
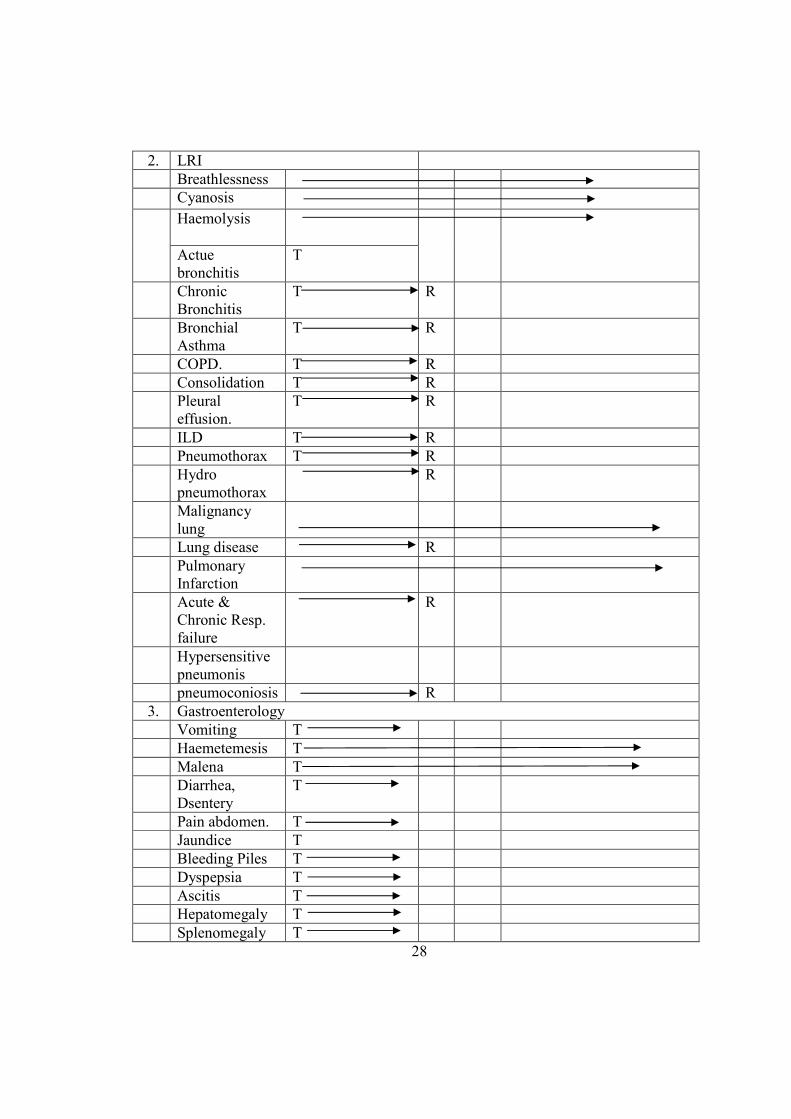
2. LRI
Breathlessness
Cyanosis
Haemolysis
Actue
bronchitis
T
Chronic
Bronchitis
T R
Bronchial
Asthma
T R
COPD. T R
Consolidation T R
Pleural
effusion.
T R
ILD T R
Pneumothorax T R
Hydro
pneumothorax
R
Malignancy
lung
Lung disease R
Pulmonary
Infarction
Acute &
Chronic Resp.
failure
R
Hypersensitive
pneumonis
pneumoconiosis R
3. Gastroenterology
Vomiting T
Haemetemesis T
Malena T
Diarrhea,
Dsentery
T
Pain abdomen. T
Jaundice T
Bleeding Piles T
Dyspepsia T
Ascitis T
Hepatomegaly T
Splenomegaly T
28
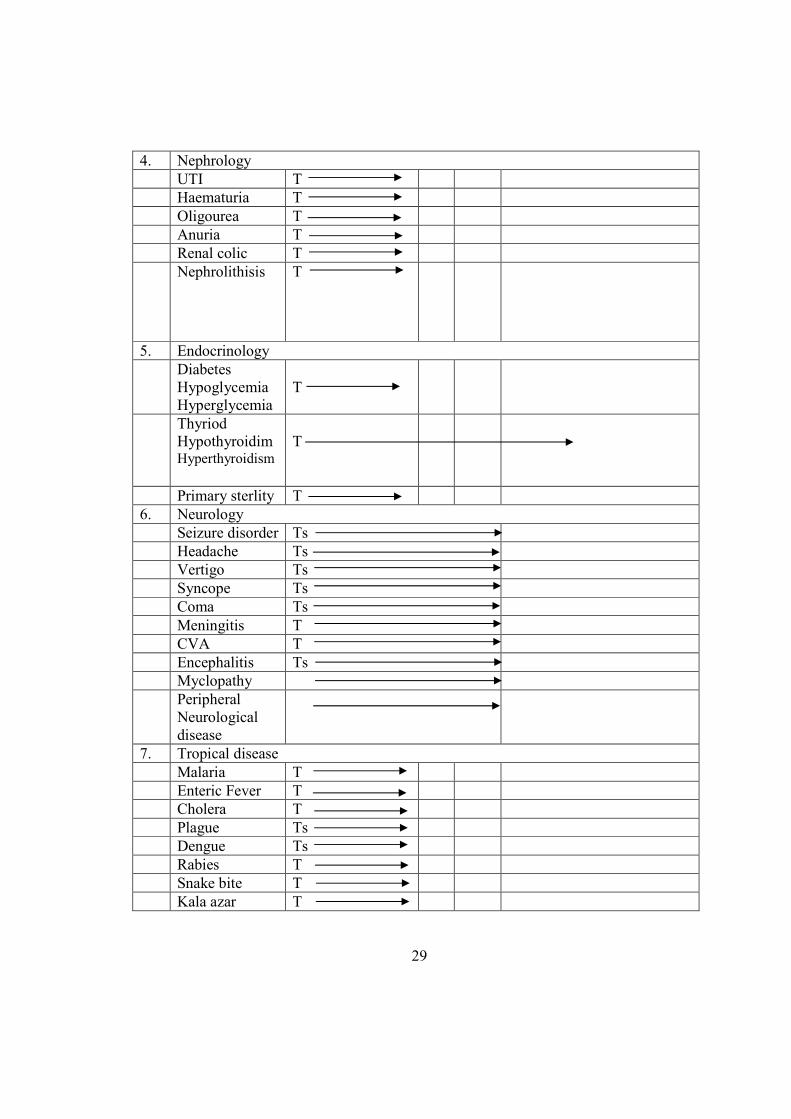
4. Nephrology
UTI T
Haematuria T
Oligourea T
Anuria T
Renal colic T
Nephrolithisis T
5. Endocrinology
Diabetes
Hypoglycemia
Hyperglycemia
T
Thyriod
HypothyroidimHyperthyroidism
T
Primary sterlity T
6. Neurology
Seizure disorder Ts
Headache Ts
Vertigo Ts
Syncope Ts
Coma Ts
Meningitis T
CVA T
Encephalitis Ts
Myclopathy
Peripheral
Neurological
disease
7. Tropical disease
Malaria T
Enteric Fever T
Cholera T
Plague Ts
Dengue Ts
Rabies T
Snake bite T
Kala azar T
29
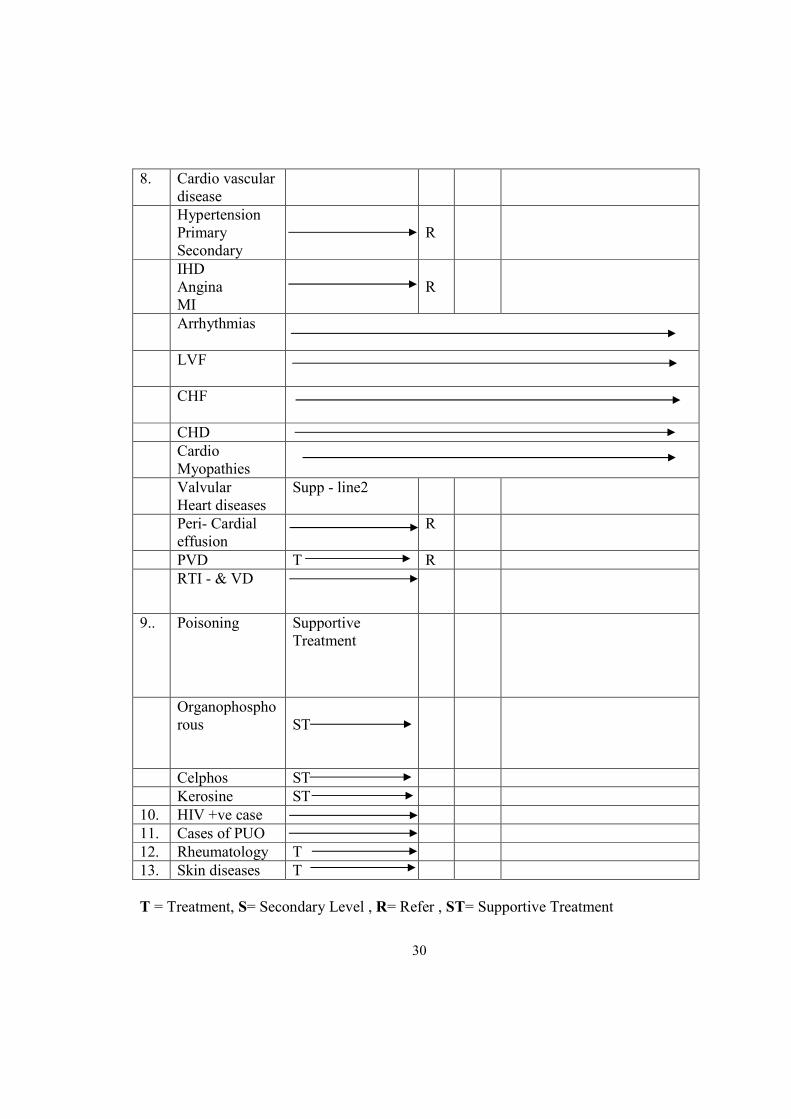
8. Cardio vascular
disease
Hypertension
Primary
Secondary
R
IHD
Angina
MI
R
Arrhythmias
LVF
CHF
CHD
Cardio
Myopathies
Valvular
Heart diseases
Supp - line2
Peri- Cardial
effusion
R
PVD T R
RTI - & VD
9.. Poisoning Supportive
Treatment
Organophospho
rous
ST
Celphos ST
Kerosine ST
10. HIV +ve case
11. Cases of PUO
12. Rheumatology T
13. Skin diseases T
T = Treatment, S= Secondary Level , R= Refer , ST= Supportive Treatment
30
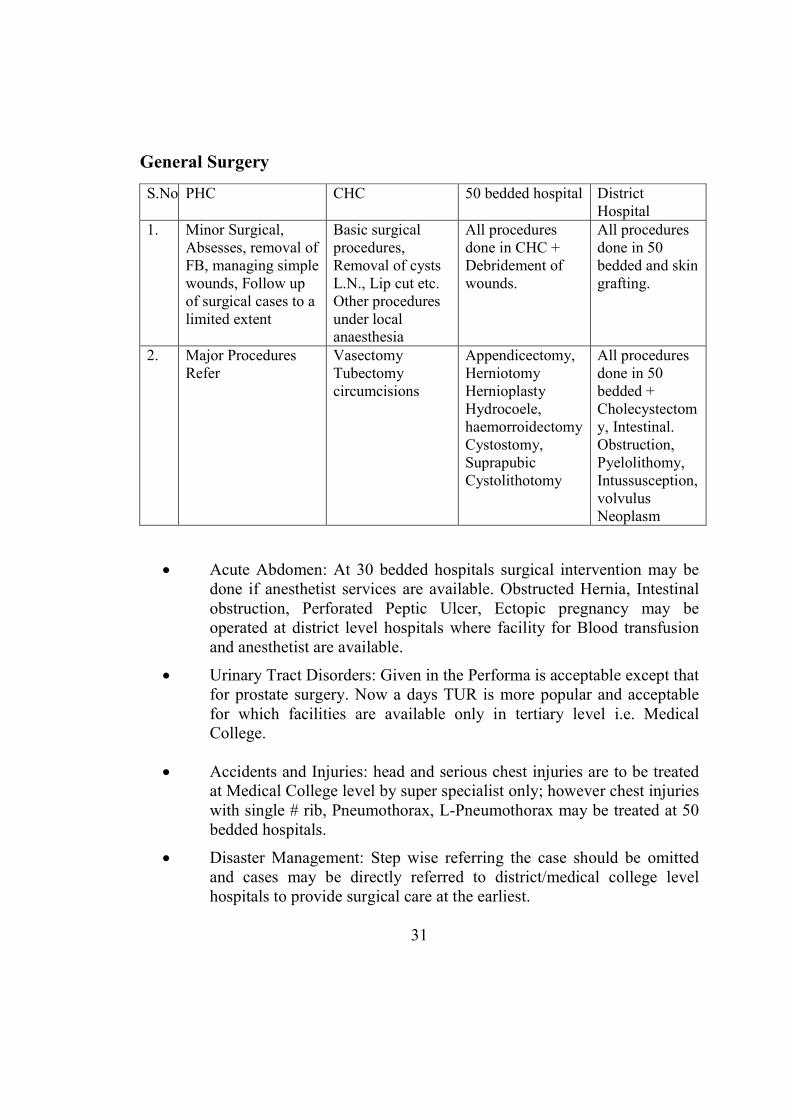
General Surgery
S.No. PHC CHC 50 bedded hospital District
Hospital
1. Minor Surgical,
Absesses, removal of
FB, managing simple
wounds, Follow up
of surgical cases to a
limited extent
Basic surgical
procedures,
Removal of cysts
L.N., Lip cut etc.
Other procedures
under local
anaesthesia
All procedures
done in CHC +
Debridement of
wounds.
All procedures
done in 50
bedded and skin
grafting.
2. Major Procedures
Refer
Vasectomy
Tubectomy
circumcisions
Appendicectomy,
Herniotomy
Hernioplasty
Hydrocoele,
haemorroidectomy
Cystostomy,
Suprapubic
Cystolithotomy
All procedures
done in 50
bedded +
Cholecystectom
y, Intestinal.
Obstruction,
Pyelolithomy,
Intussusception,
volvulus
Neoplasm
• Acute Abdomen: At 30 bedded hospitals surgical intervention may be
done if anesthetist services are available. Obstructed Hernia, Intestinal
obstruction, Perforated Peptic Ulcer, Ectopic pregnancy may be
operated at district level hospitals where facility for Blood transfusion
and anesthetist are available.
• Urinary Tract Disorders: Given in the Performa is acceptable except that
for prostate surgery. Now a days TUR is more popular and acceptable
for which facilities are available only in tertiary level i.e. Medical
College.
• Accidents and Injuries: head and serious chest injuries are to be treated
at Medical College level by super specialist only; however chest injuries
with single # rib, Pneumothorax, L-Pneumothorax may be treated at 50
bedded hospitals.
• Disaster Management: Step wise referring the case should be omitted
and cases may be directly referred to district/medical college level
hospitals to provide surgical care at the earliest.
31
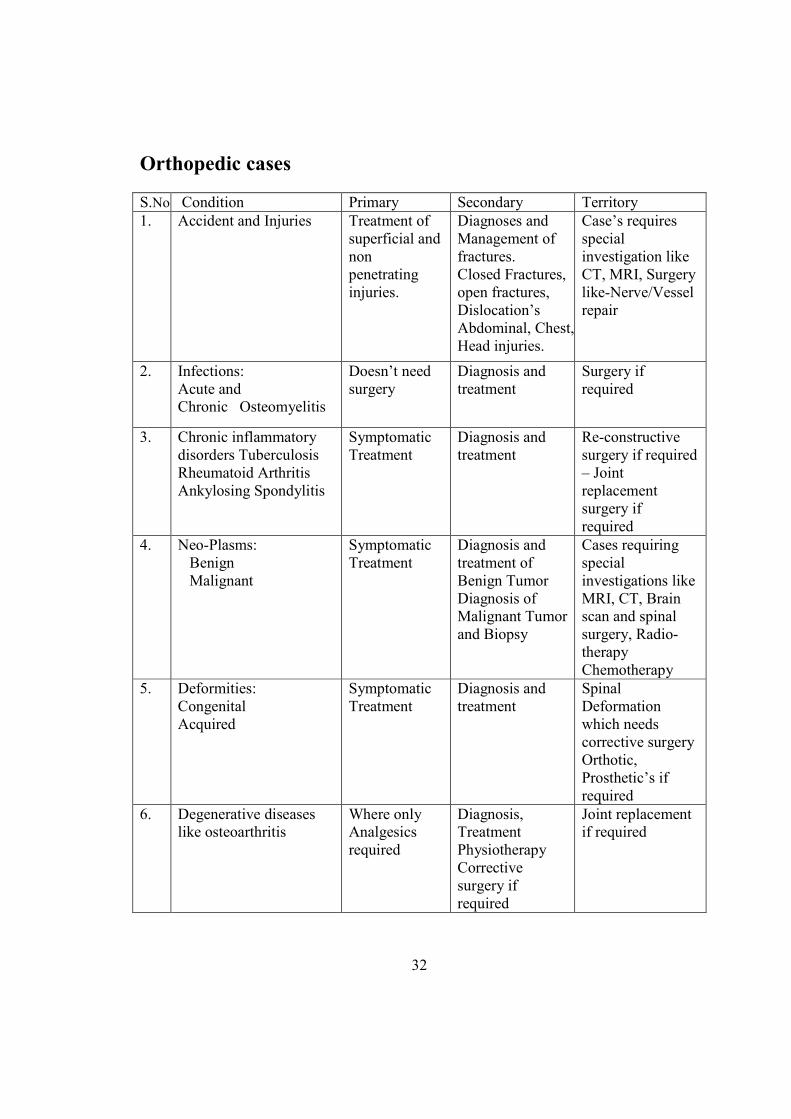
Orthopedic cases
S.No Condition Primary Secondary Territory
1. Accident and Injuries Treatment of
superficial and
non
penetrating
injuries.
Diagnoses and
Management of
fractures.
Closed Fractures,
open fractures,
Dislocation’s
Abdominal, Chest,
Head injuries.
Case’s requires
special
investigation like
CT, MRI, Surgery
like-Nerve/Vessel
repair
2. Infections:
Acute and
Chronic Osteomyelitis
Doesn’t need
surgery
Diagnosis and
treatment
Surgery if
required
3. Chronic inflammatory
disorders Tuberculosis
Rheumatoid Arthritis
Ankylosing Spondylitis
Symptomatic
Treatment
Diagnosis and
treatment
Re-constructive
surgery if required
– Joint
replacement
surgery if
required
4. Neo-Plasms:
Benign
Malignant
Symptomatic
Treatment
Diagnosis and
treatment of
Benign Tumor
Diagnosis of
Malignant Tumor
and Biopsy
Cases requiring
special
investigations like
MRI, CT, Brain
scan and spinal
surgery, Radio-
therapy
Chemotherapy
5. Deformities:
Congenital
Acquired
Symptomatic
Treatment
Diagnosis and
treatment
Spinal
Deformation
which needs
corrective surgery
Orthotic,
Prosthetic’s if
required
6. Degenerative diseases
like osteoarthritis
Where only
Analgesics
required
Diagnosis,
Treatment
Physiotherapy
Corrective
surgery if
required
Joint replacement
if required
32
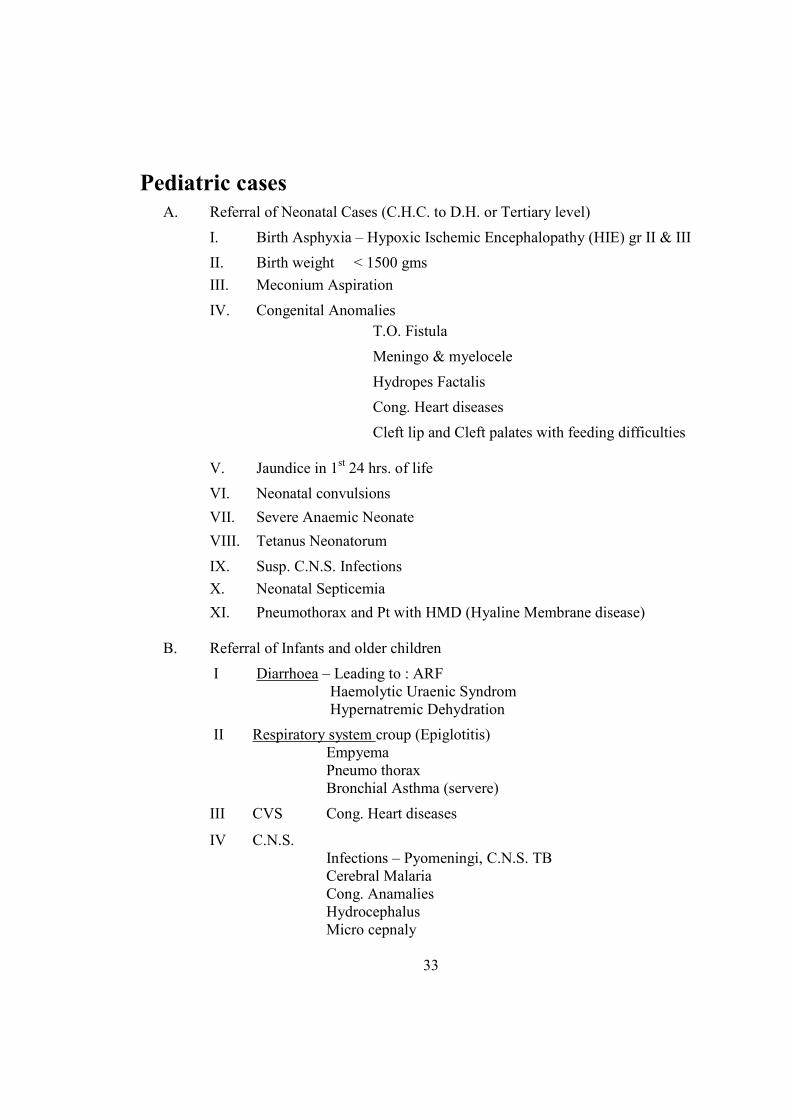
Pediatric cases
A. Referral of Neonatal Cases (C.H.C. to D.H. or Tertiary level)
I. Birth Asphyxia – Hypoxic Ischemic Encephalopathy (HIE) gr II & III
II. Birth weight < 1500 gms
III. Meconium Aspiration
IV. Congenital Anomalies
T.O. Fistula
Meningo & myelocele
Hydropes Factalis
Cong. Heart diseases
Cleft lip and Cleft palates with feeding difficulties
V. Jaundice in 1st 24 hrs. of life
VI. Neonatal convulsions
VII. Severe Anaemic Neonate
VIII. Tetanus Neonatorum
IX. Susp. C.N.S. Infections
X. Neonatal Septicemia
XI. Pneumothorax and Pt with HMD (Hyaline Membrane disease)
B. Referral of Infants and older children
I Diarrhoea – Leading to : ARF
Haemolytic Uraenic Syndrom
Hypernatremic Dehydration
II Respiratory system croup (Epiglotitis)
Empyema
Pneumo thorax
Bronchial Asthma (servere)
III CVS Cong. Heart diseases
IV C.N.S.
Infections – Pyomeningi, C.N.S. TB
Cerebral Malaria
Cong. Anamalies
Hydrocephalus
Micro cepnaly
33
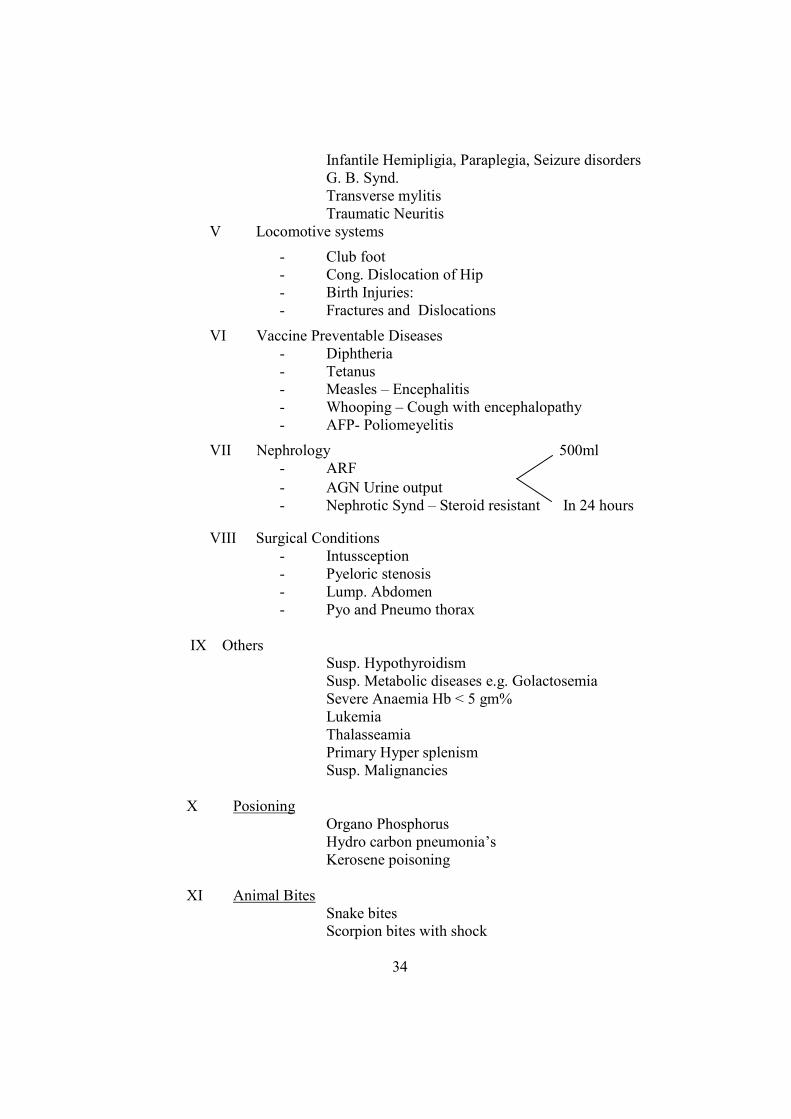
Infantile Hemipligia, Paraplegia, Seizure disorders
G. B. Synd.
Transverse mylitis
Traumatic Neuritis
V Locomotive systems
- Club foot
- Cong. Dislocation of Hip
- Birth Injuries:
- Fractures and Dislocations
VI Vaccine Preventable Diseases
- Diphtheria
- Tetanus
- Measles – Encephalitis
- Whooping – Cough with encephalopathy
- AFP- Poliomeyelitis
VII Nephrology 500ml
- ARF
- AGN Urine output
- Nephrotic Synd – Steroid resistant In 24 hours
VIII Surgical Conditions
- Intussception
- Pyeloric stenosis
- Lump. Abdomen
- Pyo and Pneumo thorax
IX Others
Susp. Hypothyroidism
Susp. Metabolic diseases e.g. Golactosemia
Severe Anaemia Hb < 5 gm%
Lukemia
Thalasseamia
Primary Hyper splenism
Susp. Malignancies
X Posioning
Organo Phosphorus
Hydro carbon pneumonia’s
Kerosene poisoning
XI Animal Bites
Snake bites
Scorpion bites with shock
34
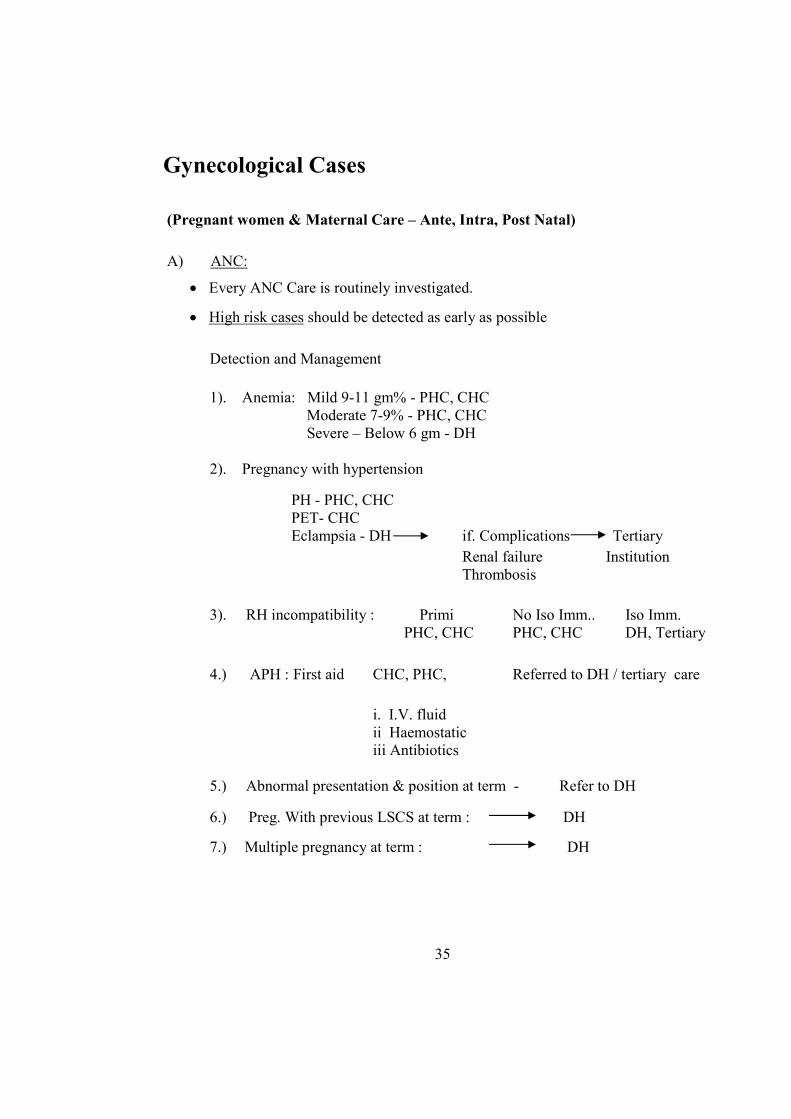
Gynecological Cases
(Pregnant women & Maternal Care – Ante, Intra, Post #atal)
A) ANC:
• Every ANC Care is routinely investigated.
• High risk cases should be detected as early as possible
Detection and Management
1). Anemia: Mild 9-11 gm% - PHC, CHC
Moderate 7-9% - PHC, CHC
Severe – Below 6 gm - DH
2). Pregnancy with hypertension
PH - PHC, CHC
PET- CHC
Eclampsia - DH if. Complications Tertiary
Renal failure Institution
Thrombosis
3). RH incompatibility : Primi No Iso Imm.. Iso Imm.
PHC, CHC PHC, CHC DH, Tertiary
4.) APH : First aid CHC, PHC, Referred to DH / tertiary care
i. I.V. fluid
ii Haemostatic
iii Antibiotics
5.) Abnormal presentation & position at term - Refer to DH
6.) Preg. With previous LSCS at term : DH
7.) Multiple pregnancy at term : DH
35
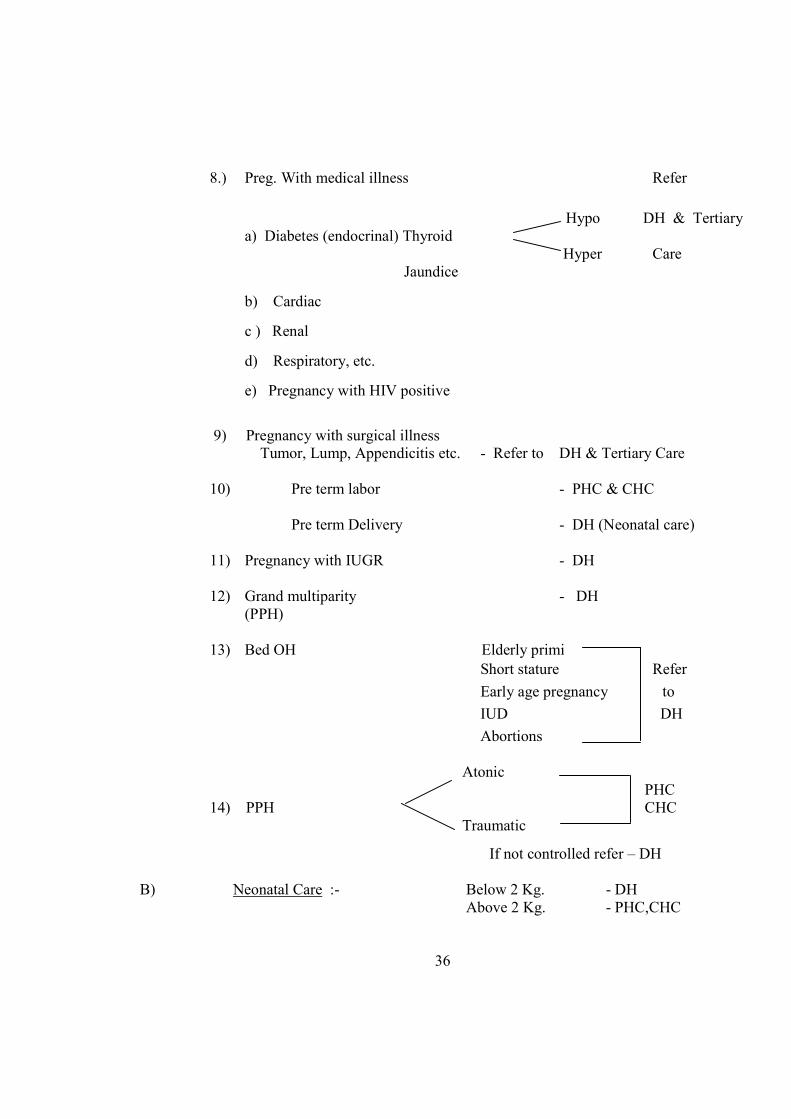
8.) Preg. With medical illness Refer
Hypo DH & Tertiary
a) Diabetes (endocrinal) Thyroid
Hyper Care
Jaundice
b) Cardiac
c ) Renal
d) Respiratory, etc.
e) Pregnancy with HIV positive
9) Pregnancy with surgical illness
Tumor, Lump, Appendicitis etc. - Refer to DH & Tertiary Care
10) Pre term labor - PHC & CHC
Pre term Delivery - DH (Neonatal care)
11) Pregnancy with IUGR - DH
12) Grand multiparity - DH
(PPH)
13) Bed OH Elderly primi }
Short stature Refer
Early age pregnancy to
IUD DH
Abortions
Atonic
PHC
14) PPH CHC
Traumatic
If not controlled refer – DH
B) Neonatal Care :- Below 2 Kg. - DH
Above 2 Kg. - PHC,CHC
36
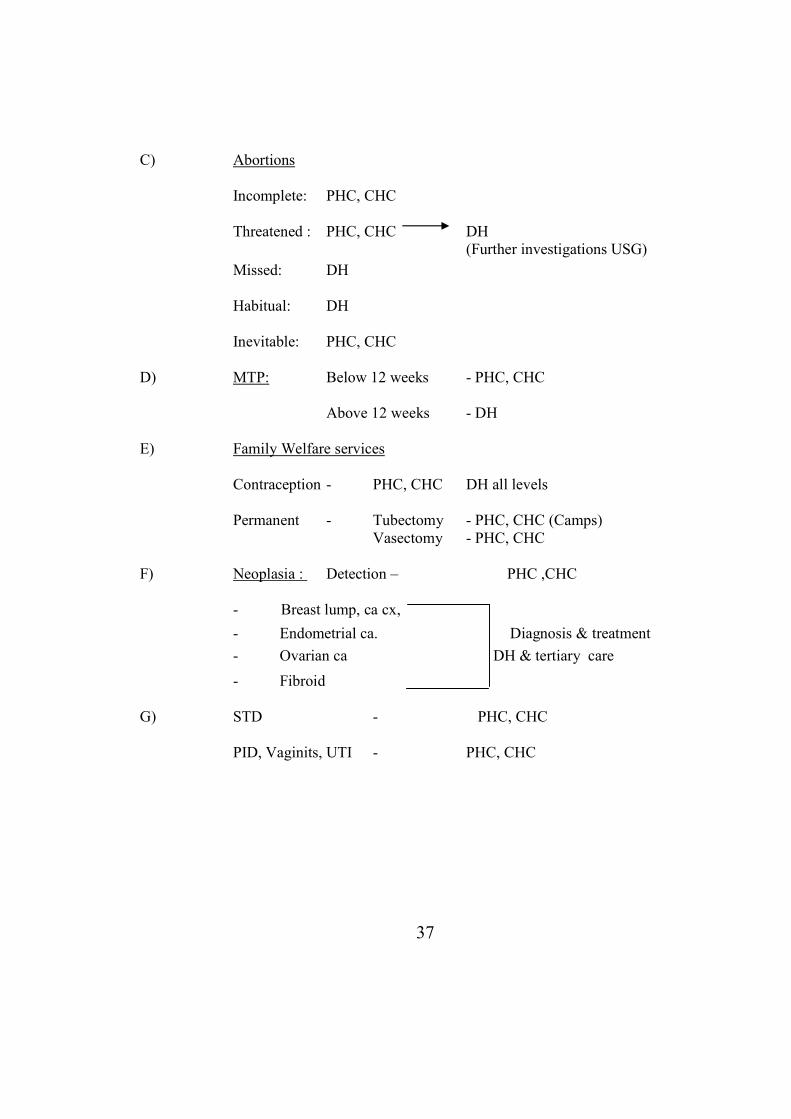
C) Abortions
Incomplete: PHC, CHC
Threatened : PHC, CHC DH
(Further investigations USG)
Missed: DH
Habitual: DH
Inevitable: PHC, CHC
D) MTP: Below 12 weeks - PHC, CHC
Above 12 weeks - DH
E) Family Welfare services
Contraception - PHC, CHC DH all levels
Permanent - Tubectomy - PHC, CHC (Camps)
Vasectomy - PHC, CHC
F) Neoplasia : Detection – PHC ,CHC
- Breast lump, ca cx,
- Endometrial ca. Diagnosis & treatment
- Ovarian ca DH & tertiary care
- Fibroid
G) STD - PHC, CHC
PID, Vaginits, UTI - PHC, CHC
37
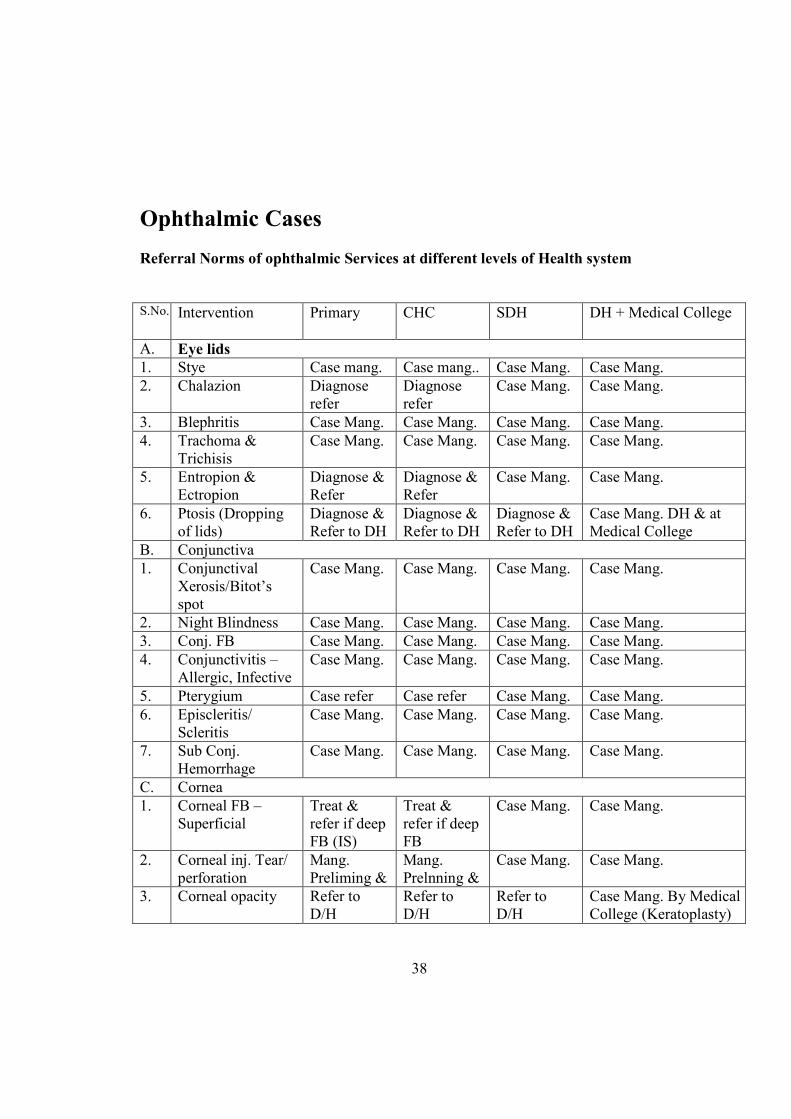
Ophthalmic Cases
Referral #orms of ophthalmic Services at different levels of Health system
S.No. Intervention Primary CHC SDH DH + Medical College
A. Eye lids
1. Stye Case mang. Case mang.. Case Mang. Case Mang.
2. Chalazion Diagnose
refer
Diagnose
refer
Case Mang. Case Mang.
3. Blephritis Case Mang. Case Mang. Case Mang. Case Mang.
4. Trachoma &
Trichisis
Case Mang. Case Mang. Case Mang. Case Mang.
5. Entropion &
Ectropion
Diagnose &
Refer
Diagnose &
Refer
Case Mang. Case Mang.
6. Ptosis (Dropping
of lids)
Diagnose &
Refer to DH
Diagnose &
Refer to DH
Diagnose &
Refer to DH
Case Mang. DH & at
Medical College
B. Conjunctiva
1. Conjunctival
Xerosis/Bitot’s
spot
Case Mang. Case Mang. Case Mang. Case Mang.
2. Night Blindness Case Mang. Case Mang. Case Mang. Case Mang.
3. Conj. FB Case Mang. Case Mang. Case Mang. Case Mang.
4. Conjunctivitis –
Allergic, Infective
Case Mang. Case Mang. Case Mang. Case Mang.
5. Pterygium Case refer Case refer Case Mang. Case Mang.
6. Episcleritis/
Scleritis
Case Mang. Case Mang. Case Mang. Case Mang.
7. Sub Conj.
Hemorrhage
Case Mang. Case Mang. Case Mang. Case Mang.
C. Cornea
1. Corneal FB –
Superficial
Treat &
refer if deep
FB (IS)
Treat &
refer if deep
FB
Case Mang. Case Mang.
2. Corneal inj. Tear/
perforation
Mang.
Preliming &
Mang.
Prelnning &
Case Mang. Case Mang.
3.
Corneal opacity Refer to
D/H
Refer to
D/H
Refer to
D/H
Case Mang. By Medical
College (Keratoplasty)
38
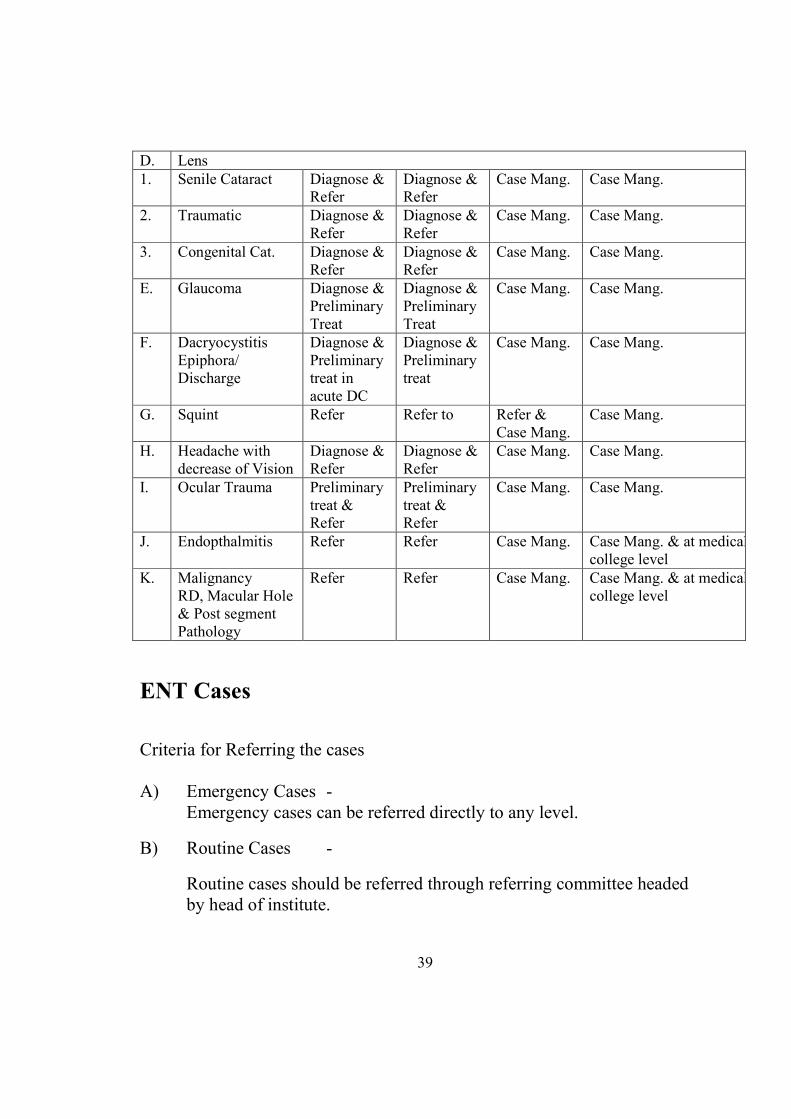
D. Lens
1. Senile Cataract Diagnose &
Refer
Diagnose &
Refer
Case Mang. Case Mang.
2. Traumatic Diagnose &
Refer
Diagnose &
Refer
Case Mang. Case Mang.
3. Congenital Cat. Diagnose &
Refer
Diagnose &
Refer
Case Mang. Case Mang.
E. Glaucoma Diagnose &
Preliminary
Treat
Diagnose &
Preliminary
Treat
Case Mang. Case Mang.
F. Dacryocystitis
Epiphora/
Discharge
Diagnose &
Preliminary
treat in
acute DC
Diagnose &
Preliminary
treat
Case Mang. Case Mang.
G. Squint Refer Refer to Refer &
Case Mang.
Case Mang.
H. Headache with
decrease of Vision
Diagnose &
Refer
Diagnose &
Refer
Case Mang. Case Mang.
I. Ocular Trauma Preliminary
treat &
Refer
Preliminary
treat &
Refer
Case Mang. Case Mang.
J. Endopthalmitis Refer Refer Case Mang. Case Mang. & at medical
college level
K. Malignancy
RD, Macular Hole
& Post segment
Pathology
Refer Refer Case Mang. Case Mang. & at medical
college level
E#T Cases
Criteria for Referring the cases
A) Emergency Cases -
Emergency cases can be referred directly to any level.
B) Routine Cases -
Routine cases should be referred through referring committee headed
by head of institute.
39
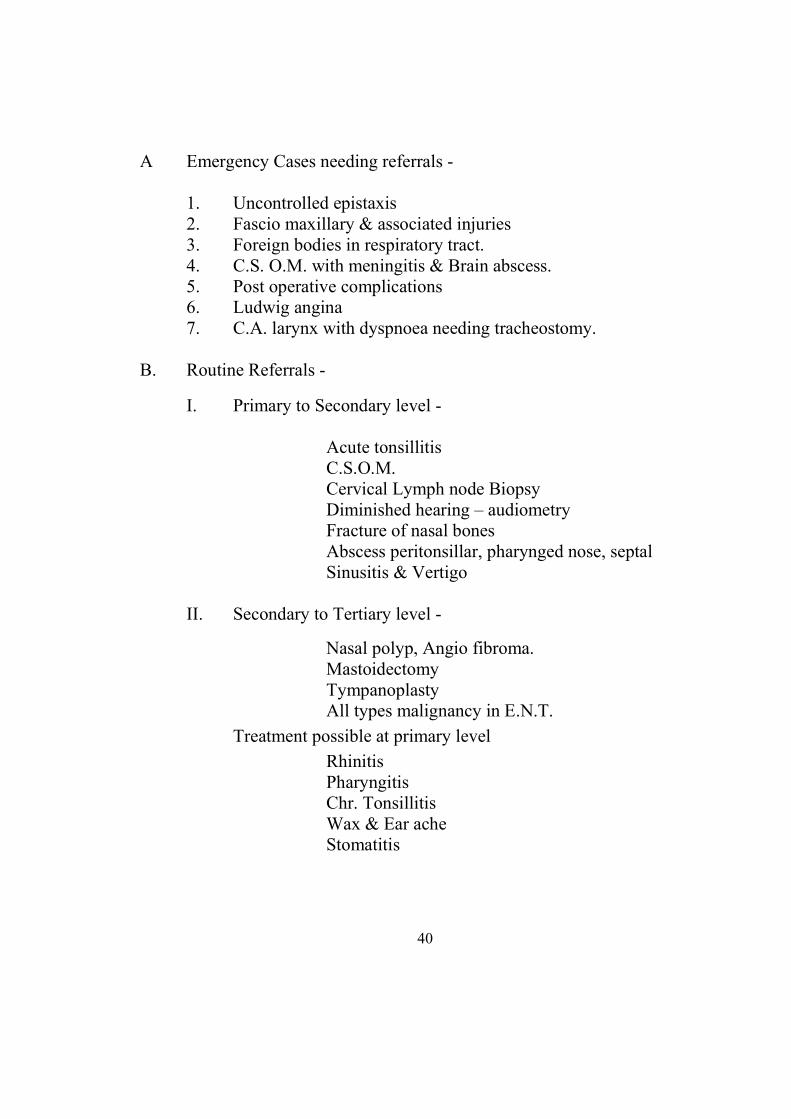
A Emergency Cases needing referrals -
1. Uncontrolled epistaxis
2. Fascio maxillary & associated injuries
3. Foreign bodies in respiratory tract.
4. C.S. O.M. with meningitis & Brain abscess.
5. Post operative complications
6. Ludwig angina
7. C.A. larynx with dyspnoea needing tracheostomy.
B. Routine Referrals -
I. Primary to Secondary level -
Acute tonsillitis
C.S.O.M.
Cervical Lymph node Biopsy
Diminished hearing – audiometry
Fracture of nasal bones
Abscess peritonsillar, pharynged nose, septal
Sinusitis & Vertigo
II. Secondary to Tertiary level -
Nasal polyp, Angio fibroma.
Mastoidectomy
Tympanoplasty
All types malignancy in E.N.T.
Treatment possible at primary level
Rhinitis
Pharyngitis
Chr. Tonsillitis
Wax & Ear ache
Stomatitis
40
Chapter- 5
Feed back and Follow-up
The purpose of this activity is not just for evaluation purpose, but also
for the promotion and sustainability of referral system. The evaluation
of referral system is a critical factor for determining the strength,
weakness and out come of the services. Each user or client should be
viewed as a potential ‘ambassador’ of the referral system. Users who
are satisfied with care and services they received at hospital will
encourage their family, friends and neighbors to use the facility.
Feed back
There has to be a proper feed back from FRU or District level
facilities so that progress of the referred patient is known by the
medical officer who has referred the case. This feed back system will
be ensured by making use of specific card (green) meant for the level
where referral services have been availed by the patient.
The down- referral/ feed back would be made to the referring
institution or facility. It will include investigations carried out, final
diagnosis, treatment given, treatment to be continued and for how
long. Other follow-up instructions to be carried out by the patient or
attendant are given in the appendices in the feedback cards. Follow –
up instructions are given in Hindi and complete so that client can
follow and comply these instructions. To ensure proper follow-up,
detail and complete address must be recorded in the referral register.
This would be of immense help if the patient fails to turn-up on time
and date assigned for follow-up. If the complete address is available
then the patient can be contacted and male or female health worker
can be asked to pay a visit.
Feed back cards may be utilized as a ready reference in forthcoming
ailments of similar course and nature so that the sufferer may be
benefited without wasting time. On the other hand, by using
laboratory investigations and clinical findings the patients illness can
be reviewed accordingly and progress as well as prognosis can be
judged. 41
Follow up
More crucial and important part of treatment is follow up in the light
of instruction / advice given by the treating specialist. Obstetric
emergency and pediatric emergency need special mention in this
context. Client should follow the instructions regarding intake of
drugs prescribed and strictly adhere to the instructions given by the
treating specialist.
The health provider should ensure appropriate follow-up care.
Important aspects of follow-up care includes:
• feedback to - Patient
- family (attendant)
- authorities – i.e., supervisor etc
- care providers at other levels
• future prevention, including the need for the cooperation
of families
• planning, and identification of persons at risk.
Health education, family planning and counseling were considered to
be key issues in follow-up care. For example, in a case of eclampsia,
subsequent monitoring of blood pressure, renal function and general
health is also important. Communication with the family, community
and health care personnel is necessary if support for a woman
following an eclamptic fit is to be provided and maintained.
To provide follow-up care to patients referred to or discharged from
hospital, follow-up has to be planned according to the disease in
question. In certain conditions e.g. diseases where hospitalization is
not indicated might require only one follow-up while in other
conditions patient may have to be followed up more often as in the
case of obstetric surgery, pediatrics, tuberculosis, leprosy,
psychiatrics, etc. For further follow-up the following schedule should
be followed. A case of surgery may thus have follow-up plan as given
below.
42
First follow up: - Soon after the discharge from hospital or
when she/he comes for removal of stitches, which should be
removed by clean and sterile instruments, dressing should be
applied by MO, PHC/LHV or staff nurse may be deputed from
CHC for this work. The incision/formative scar should be kept
clean and dry. Any complain/ side effect /complications should
be given due care.
Second follow up: - After one month or any
discomfort/complaint which ever is earlier. Thorough
examination should be done.
Emergency follow up: - This can be done at any time.
Subsequent follow up: - It will occur if the client has any
questions/ complain / complications.
In tribal, hilly, desert and temperate plane areas, health facilities are
widely scattered and forcing inhabitants have to walk several miles to
avail health care services. The referral feed back and follow up
services have paramount importance to play a pivotal role in
providing easy and rapid access to health care in such areas.
Therefore, distance, road, weather conditions must also be considered
when setting up the referral system. Besides government owned
ambulance, alternative transport system be considered in early stages
of planning. To stream line the referral system in these difficult areas
more inputs are needed in terms of transport at health facilities.
.
43
Chapter- 6
RAJASTHA# STATE ESSE#TIAL MEDICI#ES LIST- 2005
In pursuance of the initiative taken under the WHO India Programme
for the Promotion of Rational Use of Drugs, an endeavour was made
by the State Institute of Health & Family Welfare, Jaipur. Rajasthan,
to launch a similar Programme in Rajasthan in the year 1997. One of
the important steps identified for this purpose was to prepare an
Essential Drugs List for adoption in the state. The Ministry of Health,
Government of India, has already introduced the National Essential
Drugs List for adoption in the country. This list is modeled on the
WHO Essential Drugs List, and follows the general principles
recommended by WHO in the preparation of such lists (Annexure- A)
In Rajasthan, health care is provided by both private and public
sectors. Initially the responsibility was primarily of the public sector
to establish health care institutions accessible to all sections of the
population in all parts of the State so as to provide a whole spectrum
of diagnostic and treatment facilities. However, very sizeable
proportion of health care is now being provided by the private sector
establishments at individual/ institutional levels. In public sector
institutions, medicines are supplied free of cost or against token
payment to the government employees and free of cost to the weaker
sections of the population who avail of the treatment facilities
provided by the Government through primary, secondary or tertiary
level institutions. The drugs are also supplied through National
programmes for control of diseases of high morbidity and endemicity
to all patients who approach the treatment centers established under
such programmes.
The National Essential Drugs List implies that the drugs included in it
are adequate to meet the common contemporary health needs of the
general population and health administrators should ensure abundant
availability of such drugs in the State. The drugs included in the list
are known to be effective and generally safe and are approved by the
Drugs Controller General, India and are currently available at
affordable prices to the general public. 44
The exclusion of any drugs in the State List which is currently
available and recommended by physicians does not imply that they
are less effective or unsuitable for the patients. Their exclusion may
have been influenced by one or more of the following factors : - cost-
benefit ratio, dependence on imports or imported raw materials,
indicated in the treatment of diseases not considered significant in the
State context, insufficient experience with the drugs in India. Not
approved for use in the specific indication by the Drugs Controller
General, India or for which no standard is approved under the Drugs
& Cosmetics Act and Rules. The safety, efficacy and quality of drugs
currently available in India are according to the standards Prescribed
in India and the exclusion of any drug from this list does not mean
that it is less effective in comparison to any alternative drug which h
as found its place in the list.
The State List is not intended as an imposition on the rights of
Government institutions or private healthcare providers. It is meant to
be used as a guideline to the concept of rational therapeutics and as an
indicator of availability in the country. The drugs selected are
considered adequate to treat diseases common to most parts of the
state.
In view of the above facts the State Government constituted a
Committee for preparation of the essential Drugs List (EDLC) in the
year 1999 which would be relevant to the problems peculiar to the
State and would be acceptable to all sections of healthcare providers
both in private and public sectors.
In February 2000, the State Government was pleased to accept the
report of the EDLC and declare the recommended essential drugs list
as the Rajasthan State Essential Drugs (RSEDL-2000) for the State of
Rajasthan. As per its guidelines the doctors of the state working under
government were required to prescribe and use medicines out of this
list only, as far as possible. Similarly procurement of drugs and
medicines in the government hospitals and institutions was to be done
through the approved rate contract for all medicines in the EDL. As
such a beginning was made to rationalize use of drugs through
adoption of EDL.
45
However in pursuance of the fact that the EDL is not static and needs
to be revised periodically to cope with the advances made in the
medical sciences, the government of Rajasthan reconstituted the EDL
committee to review/update RSEDL – 2000 in March, 2000. Its
membership was further revised in February, 2004. The reconstituted
EDLC later invited suggestions for additions/ alterations and deletions
in the RSEDL-2000 from the faculty of the Medical Colleges, District
Health Administrators and Specialists from District and sub district
hospitals. In addition, the core group of the EDLC also visited all the
medical colleges for interaction with the medical community.
Suggestion made during these interactions, and accepted by the core
group, was compiled and computerized. This list was thereafter shared
with one of the WHO expert on essential drugs. The revised Essential
Drugs List (EDL) was finally placed before the members of the EDLC
for consideration, discussion and finalization in its meeting held on
25th March, 2004.
In accordance with the WHO revised concept, the committee has now
decided to recommend that the new Essential Drugs List (EDL)
should now be titled as Rajasthan State Essential Medicines List-2004
(RSEML-2004). The list uses generic names for scientific clarity.
For convenience and easy comparison, the same category numbers
and heading have been used as in the WHO Model List (1995).
However, only the names of the active bases have been used, avoiding
the names of salts and esters, e.g. morphine instead of morphine
suplphate. The quantity mentioned in the strength of the dosage forms
refers to the base unless by established practice or by pharmacopoeial
standards, it refers to the salt or the esters. The quality control
standards are as in the Indian Pharmacopoeia, unless the drugs in not
included in the I. P. Although, a due care has been taken to ensure the
correct nomenclature with strength of each dosage forms, yet for any
error/omission, pharmacopeial recommendation would prevail.
Drugs marked with an asterisk (*) are to be considered as
complimentary drugs i.e., those that are used if the other drugs are not
available or they are required for specific patients situations or
locations for valid reasons.
46
The names of drugs are followed by the letters given below to indicate
their need at various levels of medical care:
P - Primary Health Care
S - Secondary Health Care
T - Tertiary Health Care
U - Universal
WHO Criteria for the Selection of Essential Drugs
Essential drugs are those that satisfy the health care needs of the
majority of the population; they should therefore be available at all
times in adequate amounts and in the appropriate dosage forms.
The choice of such drugs depends on many factors, such as the
pattern of prevalent diseases, the treatment facilities, the training and
experience of the available personnel, the financial resources and
generic, demographic and environmental factors.
Because of differing views on the definition of any essential
drugs in terms of what is meant by the healthcare needs of the
“majority” of the population, the model list has been gradually
expanded since its introduction. Some drugs that are included are
essential only if a therapeutic Programme is planned to address the
diseases for which these drugs are used. For examples, the cytotoxic
drugs (section 8.2 of the model list) are essential only if a
comprehensive cancer treatment Programme is planned. Such a
Programme requires adequate hospitals, diagnostic and clinical
laboratory facilities for its implementation. In contrast, the drugs used
in palliative care (Section 8.4) are always, even when a
comprehensive cancer treatment Programme does not exist.
Only those drugs should be selected for which sound and
adequate data on efficacy and safety are available from clinical
studies, and for which evidence of performance in general use in
variety of medical settings has been obtained.
47
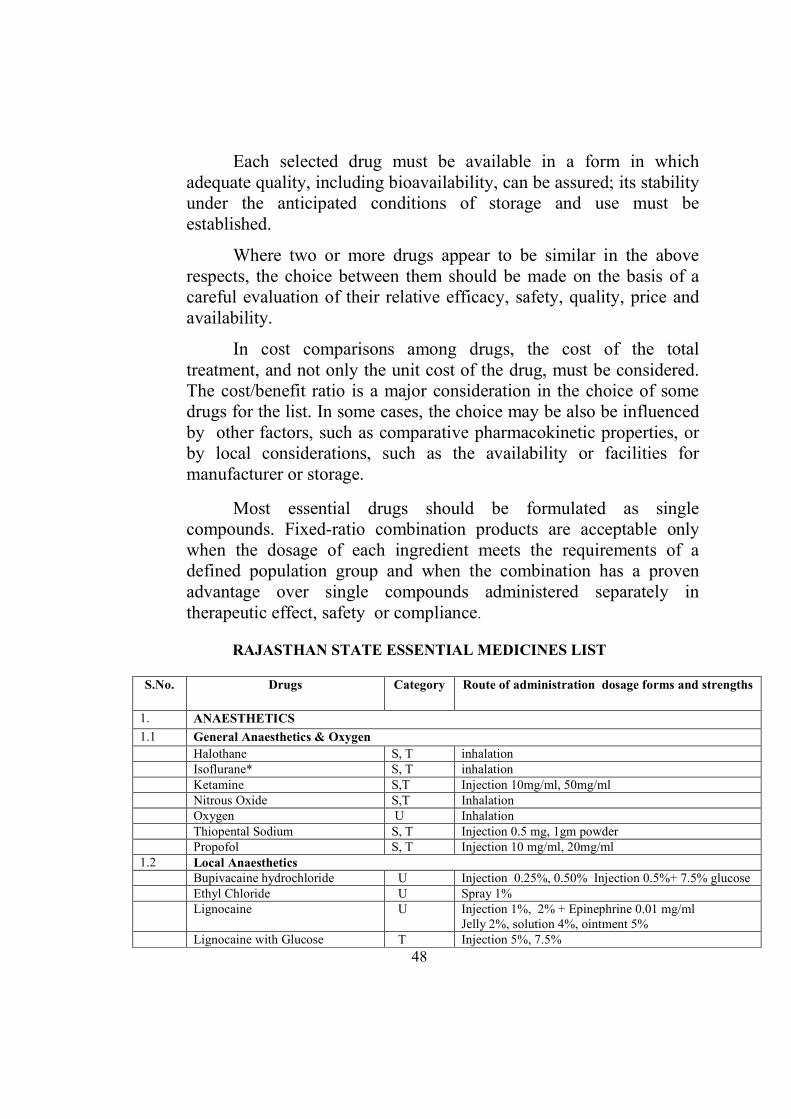
Each selected drug must be available in a form in which
adequate quality, including bioavailability, can be assured; its stability
under the anticipated conditions of storage and use must be
established.
Where two or more drugs appear to be similar in the above
respects, the choice between them should be made on the basis of a
careful evaluation of their relative efficacy, safety, quality, price and
availability.
In cost comparisons among drugs, the cost of the total
treatment, and not only the unit cost of the drug, must be considered.
The cost/benefit ratio is a major consideration in the choice of some
drugs for the list. In some cases, the choice may be also be influenced
by other factors, such as comparative pharmacokinetic properties, or
by local considerations, such as the availability or facilities for
manufacturer or storage.
Most essential drugs should be formulated as single
compounds. Fixed-ratio combination products are acceptable only
when the dosage of each ingredient meets the requirements of a
defined population group and when the combination has a proven
advantage over single compounds administered separately in
therapeutic effect, safety or compliance.
RAJASTHA# STATE ESSE#TIAL MEDICI#ES LIST
S.#o. Drugs Category Route of administration dosage forms and strengths
1.
A#AESTHETICS
1.1
General Anaesthetics & Oxygen
Halothane S, T inhalation
Isoflurane* S, T inhalation
Ketamine S,T Injection 10mg/ml, 50mg/ml
Nitrous Oxide S,T Inhalation
Oxygen U Inhalation
Thiopental Sodium S, T Injection 0.5 mg, 1gm powder
Propofol S, T Injection 10 mg/ml, 20mg/ml
1.2 Local Anaesthetics
Bupivacaine hydrochloride U Injection 0.25%, 0.50% Injection 0.5%+ 7.5% glucose
Ethyl Chloride U Spray 1%
Lignocaine U Injection 1%, 2% + Epinephrine 0.01 mg/ml
Jelly 2%, solution 4%, ointment 5%
Lignocaine with Glucose T Injection 5%, 7.5%
48
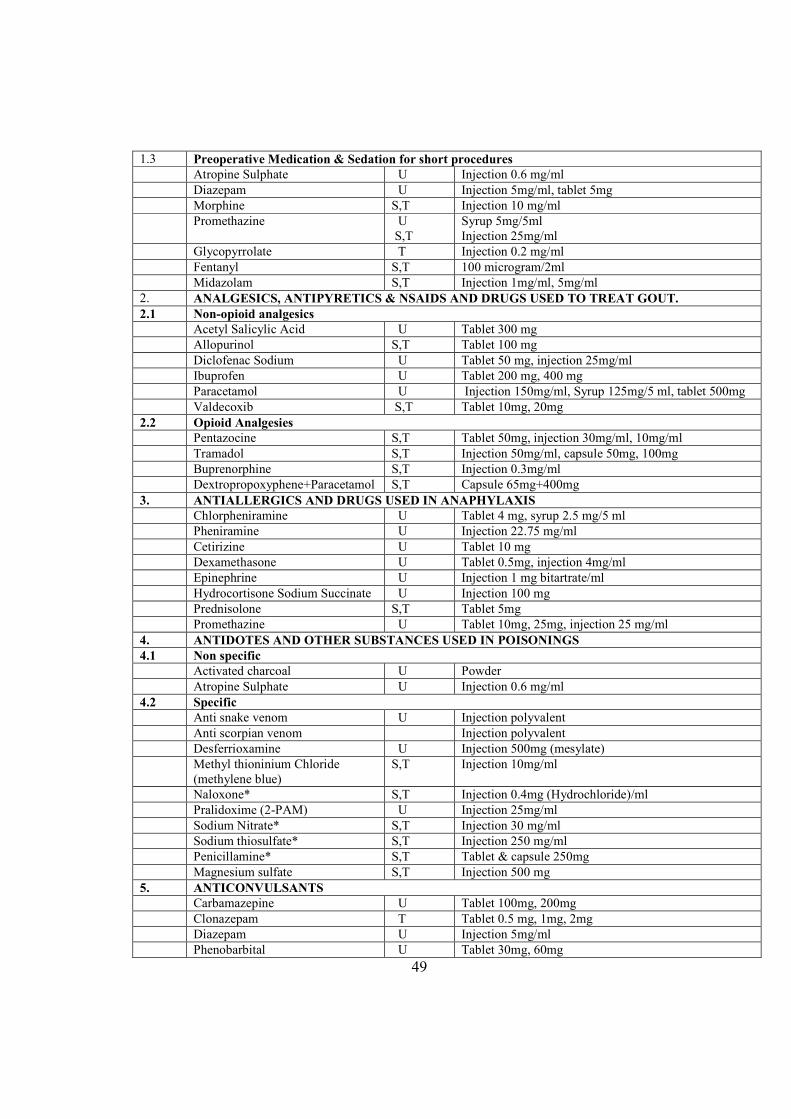
1.3 Preoperative Medication & Sedation for short procedures
Atropine Sulphate U Injection 0.6 mg/ml
Diazepam U Injection 5mg/ml, tablet 5mg
Morphine S,T Injection 10 mg/ml
Promethazine U
S,T
Syrup 5mg/5ml
Injection 25mg/ml
Glycopyrrolate T Injection 0.2 mg/ml
Fentanyl S,T 100 microgram/2ml
Midazolam S,T Injection 1mg/ml, 5mg/ml
2. A#ALGESICS, A#TIPYRETICS & #SAIDS A#D DRUGS USED TO TREAT GOUT.
2.1 #on-opioid analgesics
Acetyl Salicylic Acid U Tablet 300 mg
Allopurinol S,T Tablet 100 mg
Diclofenac Sodium U Tablet 50 mg, injection 25mg/ml
Ibuprofen U Tablet 200 mg, 400 mg
Paracetamol U Injection 150mg/ml, Syrup 125mg/5 ml, tablet 500mg
Valdecoxib S,T Tablet 10mg, 20mg
2.2 Opioid Analgesies
Pentazocine S,T Tablet 50mg, injection 30mg/ml, 10mg/ml
Tramadol S,T Injection 50mg/ml, capsule 50mg, 100mg
Buprenorphine S,T Injection 0.3mg/ml
Dextropropoxyphene+Paracetamol S,T Capsule 65mg+400mg
3. A#TIALLERGICS A#D DRUGS USED I# A#APHYLAXIS
Chlorpheniramine U Tablet 4 mg, syrup 2.5 mg/5 ml
Pheniramine U Injection 22.75 mg/ml
Cetirizine U Tablet 10 mg
Dexamethasone U Tablet 0.5mg, injection 4mg/ml
Epinephrine U Injection 1 mg bitartrate/ml
Hydrocortisone Sodium Succinate U Injection 100 mg
Prednisolone S,T Tablet 5mg
Promethazine U Tablet 10mg, 25mg, injection 25 mg/ml
4. A#TIDOTES A#D OTHER SUBSTA#CES USED I# POISO#I#GS
4.1 #on specific
Activated charcoal U Powder
Atropine Sulphate U Injection 0.6 mg/ml
4.2 Specific
Anti snake venom U Injection polyvalent
Anti scorpian venom Injection polyvalent
Desferrioxamine U Injection 500mg (mesylate)
Methyl thioninium Chloride
(methylene blue)
S,T Injection 10mg/ml
Naloxone* S,T Injection 0.4mg (Hydrochloride)/ml
Pralidoxime (2-PAM) U Injection 25mg/ml
Sodium Nitrate* S,T Injection 30 mg/ml
Sodium thiosulfate* S,T Injection 250 mg/ml
Penicillamine* S,T Tablet & capsule 250mg
Magnesium sulfate S,T Injection 500 mg
5. A#TICO#VULSA#TS
Carbamazepine U Tablet 100mg, 200mg
Clonazepam T Tablet 0.5 mg, 1mg, 2mg
Diazepam U Injection 5mg/ml
Phenobarbital U Tablet 30mg, 60mg
49
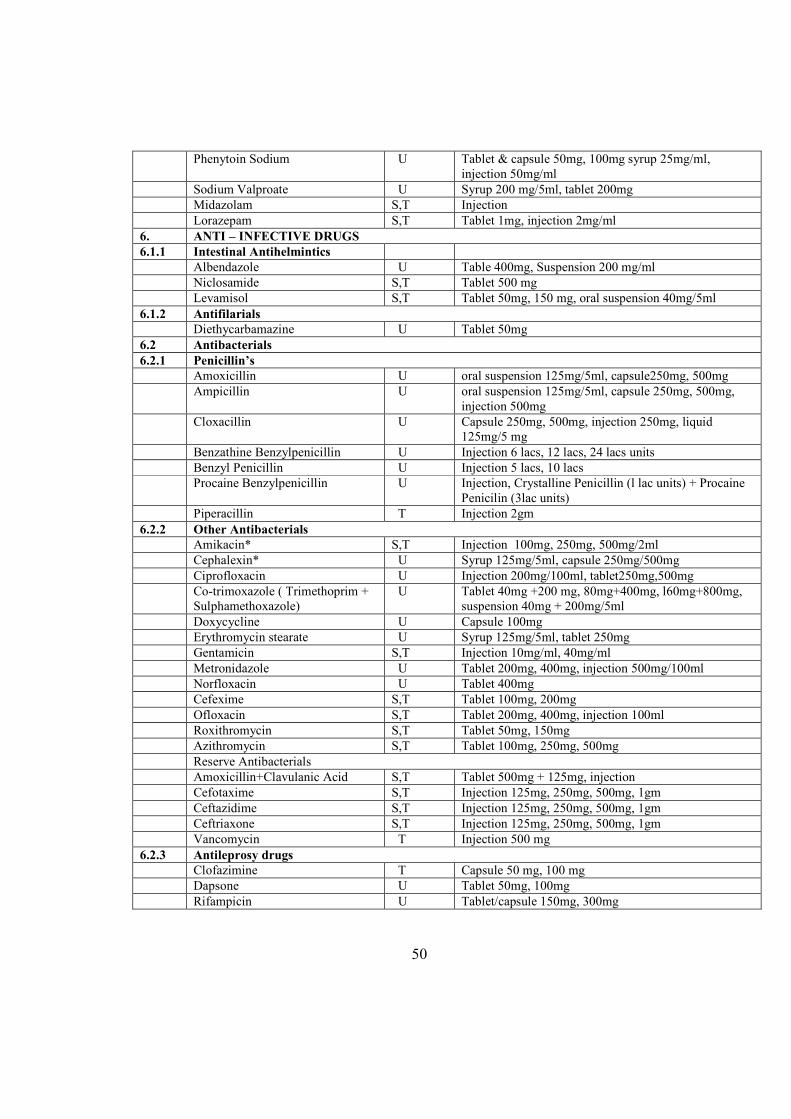
Phenytoin Sodium U Tablet & capsule 50mg, 100mg syrup 25mg/ml,
injection 50mg/ml
Sodium Valproate U Syrup 200 mg/5ml, tablet 200mg
Midazolam S,T Injection
Lorazepam S,T Tablet 1mg, injection 2mg/ml
6. A#TI – I#FECTIVE DRUGS
6.1.1 Intestinal Antihelmintics
Albendazole U Table 400mg, Suspension 200 mg/ml
Niclosamide S,T Tablet 500 mg
Levamisol S,T Tablet 50mg, 150 mg, oral suspension 40mg/5ml
6.1.2 Antifilarials
Diethycarbamazine U Tablet 50mg
6.2 Antibacterials
6.2.1 Penicillin’s
Amoxicillin U oral suspension 125mg/5ml, capsule250mg, 500mg
Ampicillin U oral suspension 125mg/5ml, capsule 250mg, 500mg,
injection 500mg
Cloxacillin U Capsule 250mg, 500mg, injection 250mg, liquid
125mg/5 mg
Benzathine Benzylpenicillin U Injection 6 lacs, 12 lacs, 24 lacs units
Benzyl Penicillin U Injection 5 lacs, 10 lacs
Procaine Benzylpenicillin U Injection, Crystalline Penicillin (l lac units) + Procaine
Penicilin (3lac units)
Piperacillin T Injection 2gm
6.2.2 Other Antibacterials
Amikacin* S,T Injection 100mg, 250mg, 500mg/2ml
Cephalexin* U Syrup 125mg/5ml, capsule 250mg/500mg
Ciprofloxacin U Injection 200mg/100ml, tablet250mg,500mg
Co-trimoxazole ( Trimethoprim +
Sulphamethoxazole)
U Tablet 40mg +200 mg, 80mg+400mg, l60mg+800mg,
suspension 40mg + 200mg/5ml
Doxycycline U Capsule 100mg
Erythromycin stearate U Syrup 125mg/5ml, tablet 250mg
Gentamicin S,T Injection 10mg/ml, 40mg/ml
Metronidazole U Tablet 200mg, 400mg, injection 500mg/100ml
Norfloxacin U Tablet 400mg
Cefexime S,T Tablet 100mg, 200mg
Ofloxacin S,T Tablet 200mg, 400mg, injection 100ml
Roxithromycin S,T Tablet 50mg, 150mg
Azithromycin S,T Tablet 100mg, 250mg, 500mg
Reserve Antibacterials
Amoxicillin+Clavulanic Acid S,T Tablet 500mg + 125mg, injection
Cefotaxime S,T Injection 125mg, 250mg, 500mg, 1gm
Ceftazidime S,T Injection 125mg, 250mg, 500mg, 1gm
Ceftriaxone S,T Injection 125mg, 250mg, 500mg, 1gm
Vancomycin T Injection 500 mg
6.2.3 Antileprosy drugs
Clofazimine T Capsule 50 mg, 100 mg
Dapsone U Tablet 50mg, 100mg
Rifampicin U Tablet/capsule 150mg, 300mg
50
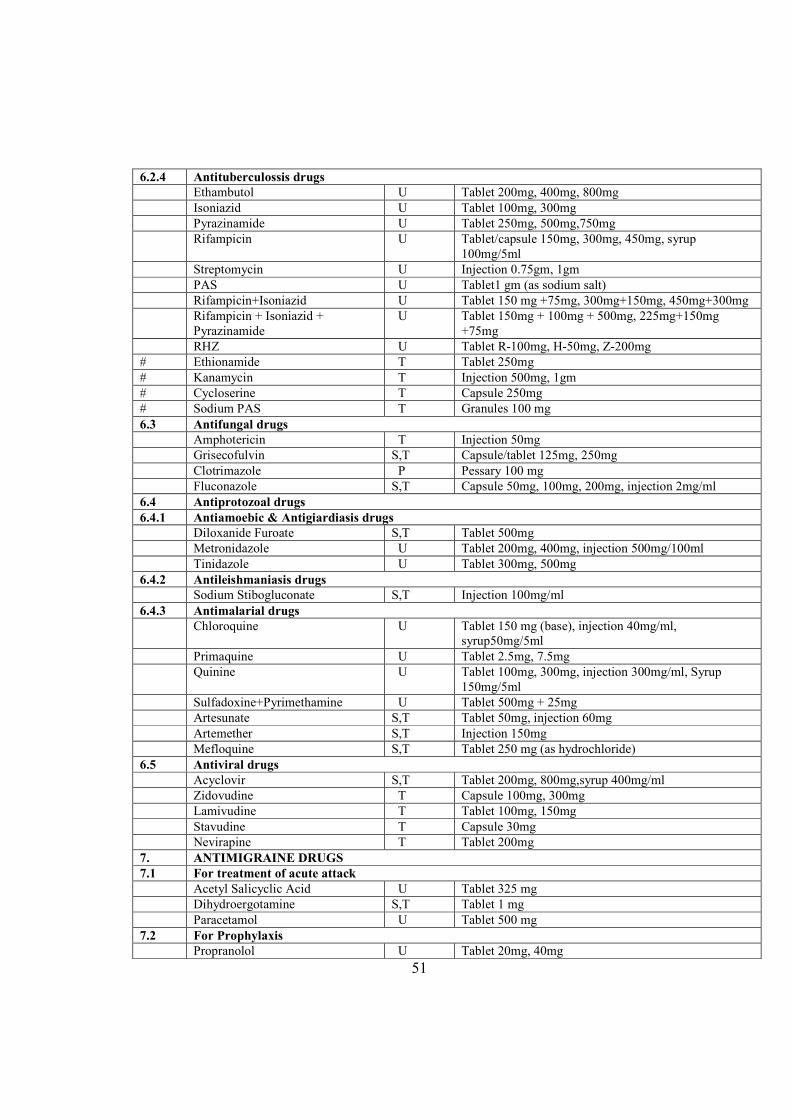
6.2.4 Antituberculossis drugs
Ethambutol U Tablet 200mg, 400mg, 800mg
Isoniazid U Tablet 100mg, 300mg
Pyrazinamide U Tablet 250mg, 500mg,750mg
Rifampicin U Tablet/capsule 150mg, 300mg, 450mg, syrup
100mg/5ml
Streptomycin U Injection 0.75gm, 1gm
PAS U Tablet1 gm (as sodium salt)
Rifampicin+Isoniazid U Tablet 150 mg +75mg, 300mg+150mg, 450mg+300mg
Rifampicin + Isoniazid +
Pyrazinamide
U Tablet 150mg + 100mg + 500mg, 225mg+150mg
+75mg
RHZ U Tablet R-100mg, H-50mg, Z-200mg
# Ethionamide T Tablet 250mg
# Kanamycin T Injection 500mg, 1gm
# Cycloserine T Capsule 250mg
# Sodium PAS T Granules 100 mg
6.3 Antifungal drugs
Amphotericin T Injection 50mg
Grisecofulvin S,T Capsule/tablet 125mg, 250mg
Clotrimazole P Pessary 100 mg
Fluconazole S,T Capsule 50mg, 100mg, 200mg, injection 2mg/ml
6.4 Antiprotozoal drugs
6.4.1 Antiamoebic & Antigiardiasis drugs
Diloxanide Furoate S,T Tablet 500mg
Metronidazole U Tablet 200mg, 400mg, injection 500mg/100ml
Tinidazole U Tablet 300mg, 500mg
6.4.2 Antileishmaniasis drugs
Sodium Stibogluconate S,T Injection 100mg/ml
6.4.3 Antimalarial drugs
Chloroquine U Tablet 150 mg (base), injection 40mg/ml,
syrup50mg/5ml
Primaquine U Tablet 2.5mg, 7.5mg
Quinine U Tablet 100mg, 300mg, injection 300mg/ml, Syrup
150mg/5ml
Sulfadoxine+Pyrimethamine U Tablet 500mg + 25mg
Artesunate S,T Tablet 50mg, injection 60mg
Artemether S,T Injection 150mg
Mefloquine S,T Tablet 250 mg (as hydrochloride)
6.5 Antiviral drugs
Acyclovir S,T Tablet 200mg, 800mg,syrup 400mg/ml
Zidovudine T Capsule 100mg, 300mg
Lamivudine T Tablet 100mg, 150mg
Stavudine T Capsule 30mg
Nevirapine T Tablet 200mg
7. A#TIMIGRAI#E DRUGS
7.1 For treatment of acute attack
Acetyl Salicyclic Acid U Tablet 325 mg
Dihydroergotamine S,T Tablet 1 mg
Paracetamol U Tablet 500 mg
7.2 For Prophylaxis
Propranolol U Tablet 20mg, 40mg
51
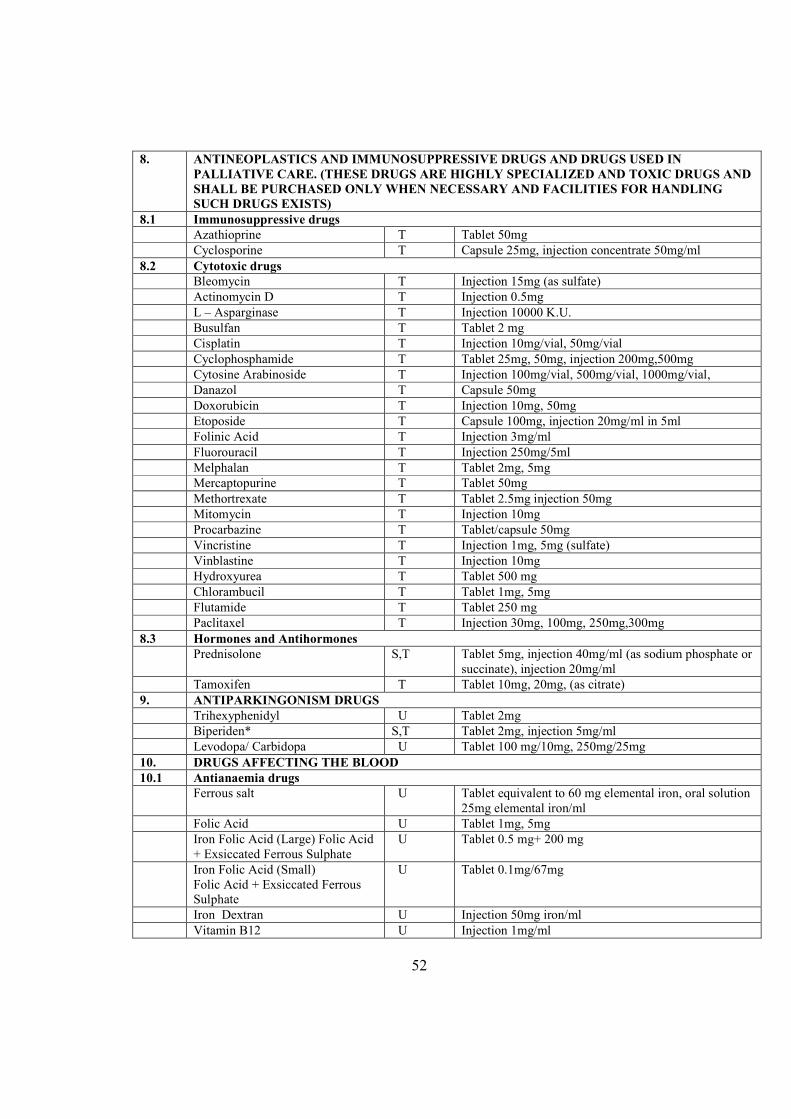
8. A#TI#EOPLASTICS A#D IMMU#OSUPPRESSIVE DRUGS A#D DRUGS USED I#
PALLIATIVE CARE. (THESE DRUGS ARE HIGHLY SPECIALIZED A#D TOXIC DRUGS A#D
SHALL BE PURCHASED O#LY WHE# #ECESSARY A#D FACILITIES FOR HA#DLI#G
SUCH DRUGS EXISTS)
8.1 Immunosuppressive drugs
Azathioprine T Tablet 50mg
Cyclosporine T Capsule 25mg, injection concentrate 50mg/ml
8.2 Cytotoxic drugs
Bleomycin T Injection 15mg (as sulfate)
Actinomycin D T Injection 0.5mg
L – Asparginase T Injection 10000 K.U.
Busulfan T Tablet 2 mg
Cisplatin T Injection 10mg/vial, 50mg/vial
Cyclophosphamide T Tablet 25mg, 50mg, injection 200mg,500mg
Cytosine Arabinoside T Injection 100mg/vial, 500mg/vial, 1000mg/vial,
Danazol T Capsule 50mg
Doxorubicin T Injection 10mg, 50mg
Etoposide T Capsule 100mg, injection 20mg/ml in 5ml
Folinic Acid T Injection 3mg/ml
Fluorouracil T Injection 250mg/5ml
Melphalan T Tablet 2mg, 5mg
Mercaptopurine T Tablet 50mg
Methortrexate T Tablet 2.5mg injection 50mg
Mitomycin T Injection 10mg
Procarbazine T Tablet/capsule 50mg
Vincristine T Injection 1mg, 5mg (sulfate)
Vinblastine T Injection 10mg
Hydroxyurea T Tablet 500 mg
Chlorambucil T Tablet 1mg, 5mg
Flutamide T Tablet 250 mg
Paclitaxel T Injection 30mg, 100mg, 250mg,300mg
8.3 Hormones and Antihormones
Prednisolone S,T Tablet 5mg, injection 40mg/ml (as sodium phosphate or
succinate), injection 20mg/ml
Tamoxifen T Tablet 10mg, 20mg, (as citrate)
9. A#TIPARKI#GO#ISM DRUGS
Trihexyphenidyl U Tablet 2mg
Biperiden* S,T Tablet 2mg, injection 5mg/ml
Levodopa/ Carbidopa U Tablet 100 mg/10mg, 250mg/25mg
10. DRUGS AFFECTI#G THE BLOOD
10.1 Antianaemia drugs
Ferrous salt U Tablet equivalent to 60 mg elemental iron, oral solution
25mg elemental iron/ml
Folic Acid U Tablet 1mg, 5mg
Iron Folic Acid (Large) Folic Acid
+ Exsiccated Ferrous Sulphate
U Tablet 0.5 mg+ 200 mg
Iron Folic Acid (Small)
Folic Acid + Exsiccated Ferrous
Sulphate
U Tablet 0.1mg/67mg
Iron Dextran U Injection 50mg iron/ml
Vitamin B12 U Injection 1mg/ml
52
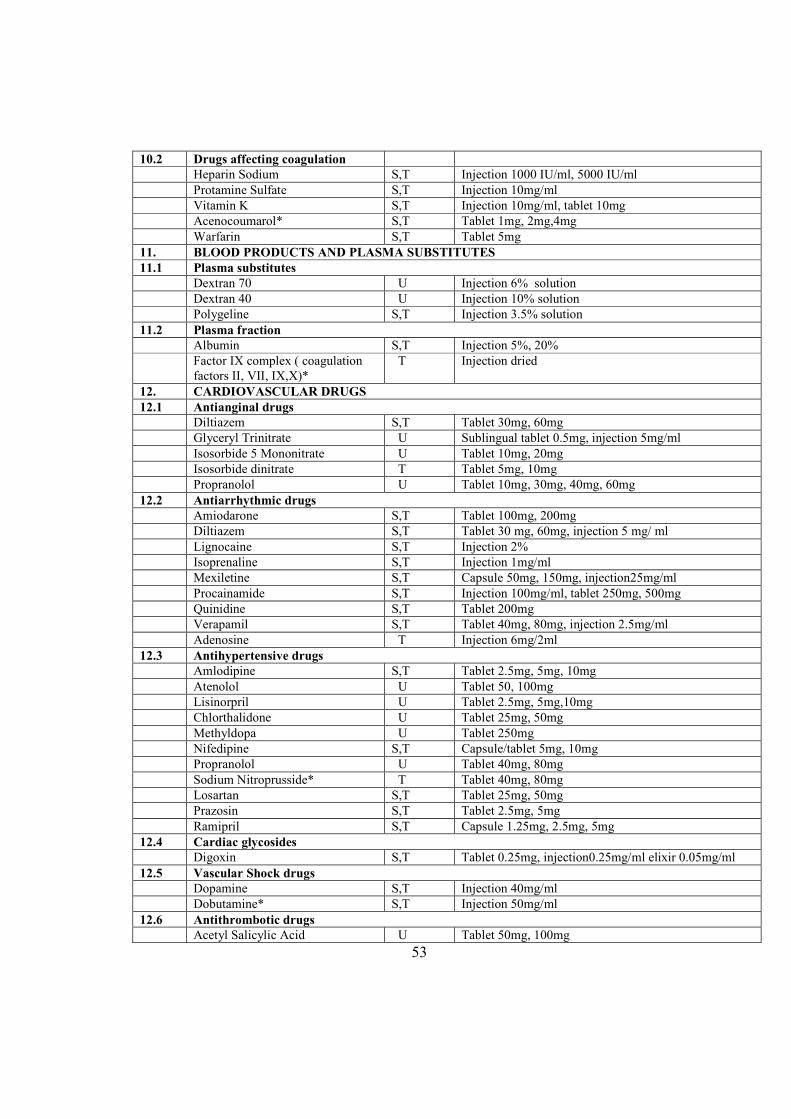
10.2 Drugs affecting coagulation
Heparin Sodium S,T Injection 1000 IU/ml, 5000 IU/ml
Protamine Sulfate S,T Injection 10mg/ml
Vitamin K S,T Injection 10mg/ml, tablet 10mg
Acenocoumarol* S,T Tablet 1mg, 2mg,4mg
Warfarin S,T Tablet 5mg
11. BLOOD PRODUCTS A#D PLASMA SUBSTITUTES
11.1 Plasma substitutes
Dextran 70 U Injection 6% solution
Dextran 40 U Injection 10% solution
Polygeline S,T Injection 3.5% solution
11.2 Plasma fraction
Albumin S,T Injection 5%, 20%
Factor IX complex ( coagulation
factors II, VII, IX,X)*
T Injection dried
12. CARDIOVASCULAR DRUGS
12.1 Antianginal drugs
Diltiazem S,T Tablet 30mg, 60mg
Glyceryl Trinitrate U Sublingual tablet 0.5mg, injection 5mg/ml
Isosorbide 5 Mononitrate U Tablet 10mg, 20mg
Isosorbide dinitrate T Tablet 5mg, 10mg
Propranolol U Tablet 10mg, 30mg, 40mg, 60mg
12.2 Antiarrhythmic drugs
Amiodarone S,T Tablet 100mg, 200mg
Diltiazem S,T Tablet 30 mg, 60mg, injection 5 mg/ ml
Lignocaine S,T Injection 2%
Isoprenaline S,T Injection 1mg/ml
Mexiletine S,T Capsule 50mg, 150mg, injection25mg/ml
Procainamide S,T Injection 100mg/ml, tablet 250mg, 500mg
Quinidine S,T Tablet 200mg
Verapamil S,T Tablet 40mg, 80mg, injection 2.5mg/ml
Adenosine T Injection 6mg/2ml
12.3 Antihypertensive drugs
Amlodipine S,T Tablet 2.5mg, 5mg, 10mg
Atenolol U Tablet 50, 100mg
Lisinorpril U Tablet 2.5mg, 5mg,10mg
Chlorthalidone U Tablet 25mg, 50mg
Methyldopa U Tablet 250mg
Nifedipine S,T Capsule/tablet 5mg, 10mg
Propranolol U Tablet 40mg, 80mg
Sodium Nitroprusside* T Tablet 40mg, 80mg
Losartan S,T Tablet 25mg, 50mg
Prazosin S,T Tablet 2.5mg, 5mg
Ramipril S,T Capsule 1.25mg, 2.5mg, 5mg
12.4 Cardiac glycosides
Digoxin S,T Tablet 0.25mg, injection0.25mg/ml elixir 0.05mg/ml
12.5 Vascular Shock drugs
Dopamine S,T Injection 40mg/ml
Dobutamine* S,T Injection 50mg/ml
12.6 Antithrombotic drugs
Acetyl Salicylic Acid U Tablet 50mg, 100mg
53
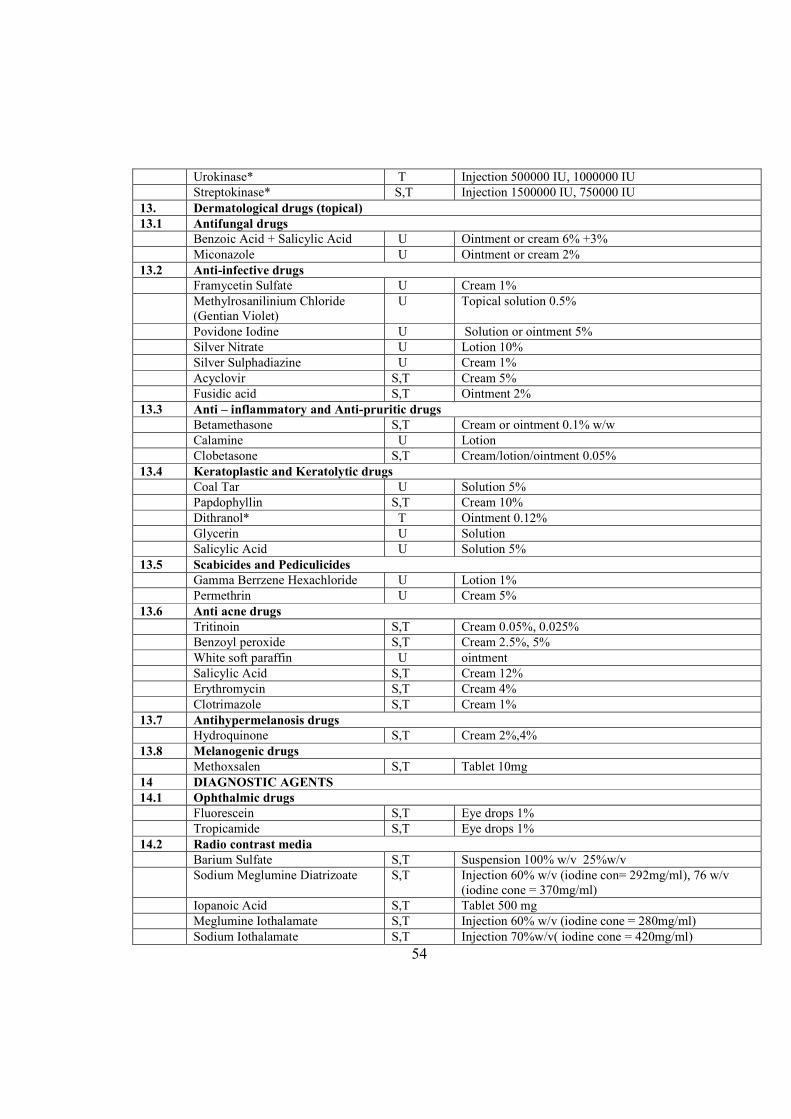
Urokinase* T Injection 500000 IU, 1000000 IU
Streptokinase* S,T Injection 1500000 IU, 750000 IU
13. Dermatological drugs (topical)
13.1 Antifungal drugs
Benzoic Acid + Salicylic Acid U Ointment or cream 6% +3%
Miconazole U Ointment or cream 2%
13.2 Anti-infective drugs
Framycetin Sulfate U Cream 1%
Methylrosanilinium Chloride
(Gentian Violet)
U Topical solution 0.5%
Povidone Iodine U Solution or ointment 5%
Silver Nitrate U Lotion 10%
Silver Sulphadiazine U Cream 1%
Acyclovir S,T Cream 5%
Fusidic acid S,T Ointment 2%
13.3 Anti – inflammatory and Anti-pruritic drugs
Betamethasone S,T Cream or ointment 0.1% w/w
Calamine U Lotion
Clobetasone S,T Cream/lotion/ointment 0.05%
13.4 Keratoplastic and Keratolytic drugs
Coal Tar U Solution 5%
Papdophyllin S,T Cream 10%
Dithranol* T Ointment 0.12%
Glycerin U Solution
Salicylic Acid U Solution 5%
13.5 Scabicides and Pediculicides
Gamma Berrzene Hexachloride U Lotion 1%
Permethrin U Cream 5%
13.6 Anti acne drugs
Tritinoin S,T Cream 0.05%, 0.025%
Benzoyl peroxide S,T Cream 2.5%, 5%
White soft paraffin U ointment
Salicylic Acid S,T Cream 12%
Erythromycin S,T Cream 4%
Clotrimazole S,T Cream 1%
13.7 Antihypermelanosis drugs
Hydroquinone S,T Cream 2%,4%
13.8 Melanogenic drugs
Methoxsalen S,T Tablet 10mg
14 DIAG#OSTIC AGE#TS
14.1 Ophthalmic drugs
Fluorescein S,T Eye drops 1%
Tropicamide S,T Eye drops 1%
14.2 Radio contrast media
Barium Sulfate S,T Suspension 100% w/v 25%w/v
Sodium Meglumine Diatrizoate S,T Injection 60% w/v (iodine con= 292mg/ml), 76 w/v
(iodine cone = 370mg/ml)
Iopanoic Acid S,T Tablet 500 mg
Meglumine Iothalamate S,T Injection 60% w/v (iodine cone = 280mg/ml)
Sodium Iothalamate S,T Injection 70%w/v( iodine cone = 420mg/ml)
54
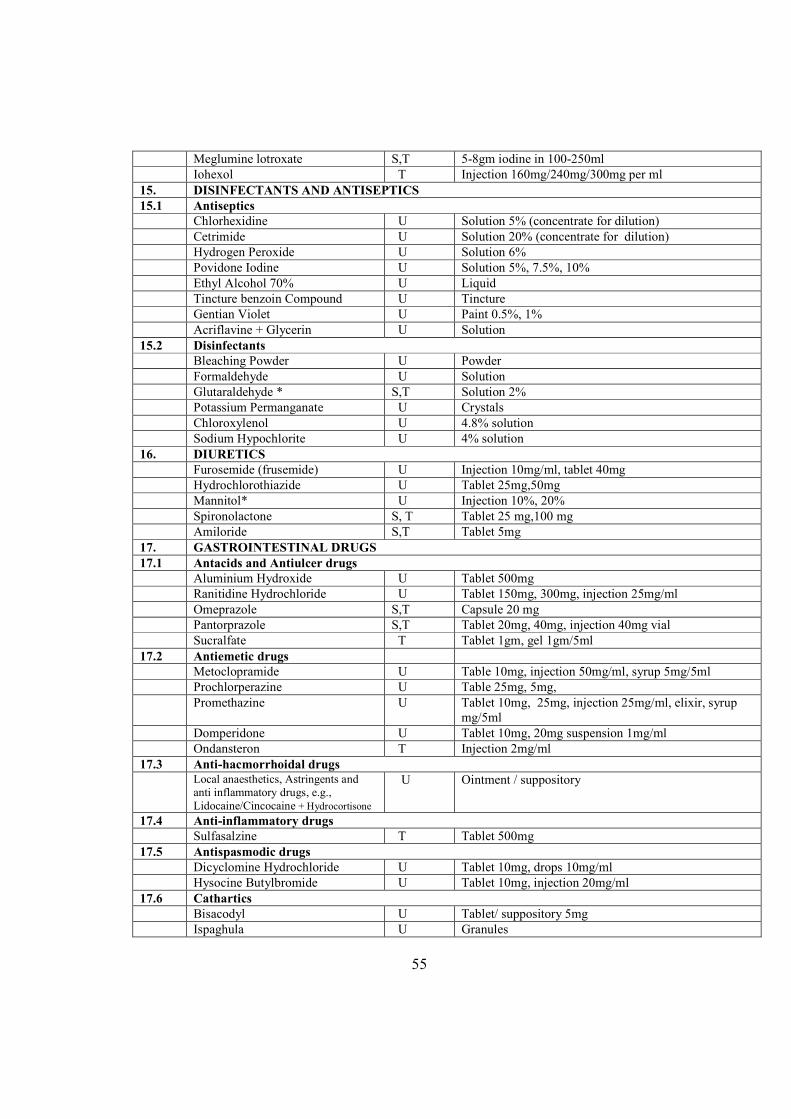
Meglumine lotroxate S,T 5-8gm iodine in 100-250ml
Iohexol T Injection 160mg/240mg/300mg per ml
15. DISI#FECTA#TS A#D A#TISEPTICS
15.1 Antiseptics
Chlorhexidine U Solution 5% (concentrate for dilution)
Cetrimide U Solution 20% (concentrate for dilution)
Hydrogen Peroxide U Solution 6%
Povidone Iodine U Solution 5%, 7.5%, 10%
Ethyl Alcohol 70% U Liquid
Tincture benzoin Compound U Tincture
Gentian Violet U Paint 0.5%, 1%
Acriflavine + Glycerin U Solution
15.2 Disinfectants
Bleaching Powder U Powder
Formaldehyde U Solution
Glutaraldehyde * S,T Solution 2%
Potassium Permanganate U Crystals
Chloroxylenol U 4.8% solution
Sodium Hypochlorite U 4% solution
16. DIURETICS
Furosemide (frusemide) U Injection 10mg/ml, tablet 40mg
Hydrochlorothiazide U Tablet 25mg,50mg
Mannitol* U Injection 10%, 20%
Spironolactone S, T Tablet 25 mg,100 mg
Amiloride S,T Tablet 5mg
17. GASTROI#TESTI#AL DRUGS
17.1 Antacids and Antiulcer drugs
Aluminium Hydroxide U Tablet 500mg
Ranitidine Hydrochloride U Tablet 150mg, 300mg, injection 25mg/ml
Omeprazole S,T Capsule 20 mg
Pantorprazole S,T Tablet 20mg, 40mg, injection 40mg vial
Sucralfate T Tablet 1gm, gel 1gm/5ml
17.2 Antiemetic drugs
Metoclopramide U Table 10mg, injection 50mg/ml, syrup 5mg/5ml
Prochlorperazine U Table 25mg, 5mg,
Promethazine U Tablet 10mg, 25mg, injection 25mg/ml, elixir, syrup
mg/5ml
Domperidone U Tablet 10mg, 20mg suspension 1mg/ml
Ondansteron T Injection 2mg/ml
17.3 Anti-hacmorrhoidal drugs
Local anaesthetics, Astringents and
anti inflammatory drugs, e.g.,
Lidocaine/Cincocaine + Hydrocortisone
U Ointment / suppository
17.4 Anti-inflammatory drugs
Sulfasalzine T Tablet 500mg
17.5 Antispasmodic drugs
Dicyclomine Hydrochloride U Tablet 10mg, drops 10mg/ml
Hysocine Butylbromide U Tablet 10mg, injection 20mg/ml
17.6 Cathartics
Bisacodyl U Tablet/ suppository 5mg
Ispaghula U Granules
55
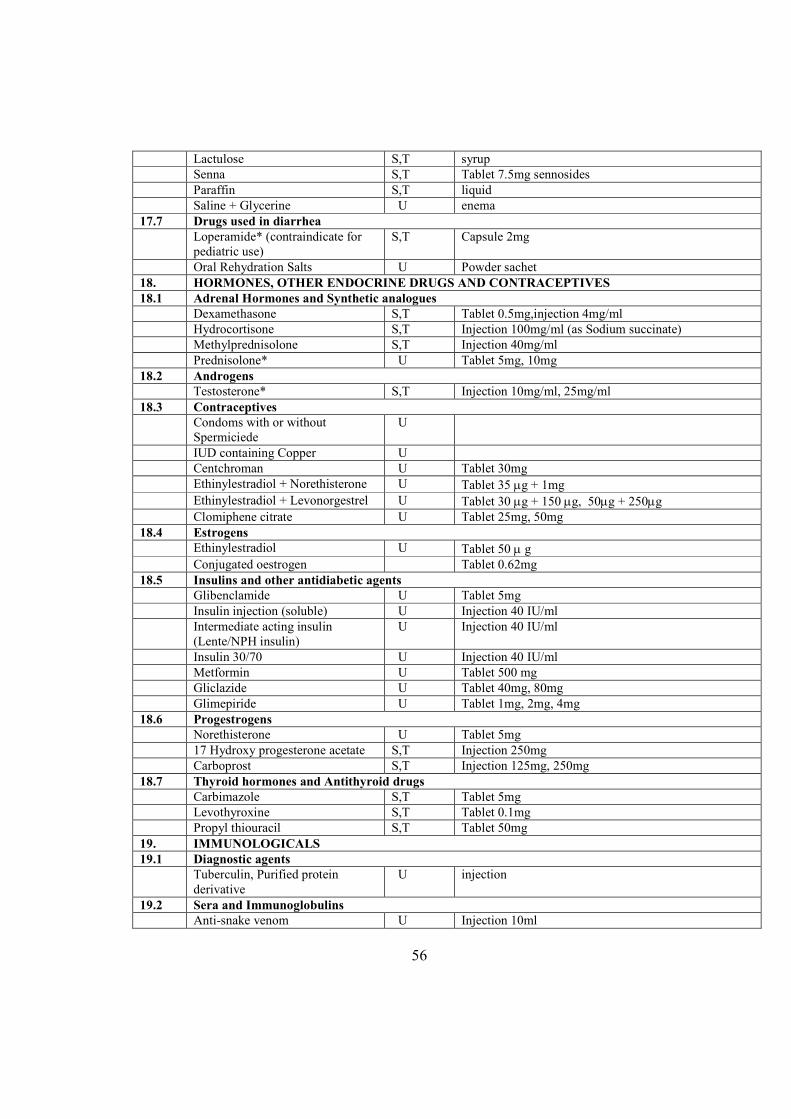
Lactulose S,T syrup
Senna S,T Tablet 7.5mg sennosides
Paraffin S,T liquid
Saline + Glycerine U enema
17.7 Drugs used in diarrhea
Loperamide* (contraindicate for
pediatric use)
S,T Capsule 2mg
Oral Rehydration Salts U Powder sachet
18. HORMO#ES, OTHER E#DOCRI#E DRUGS A#D CO#TRACEPTIVES
18.1 Adrenal Hormones and Synthetic analogues
Dexamethasone S,T Tablet 0.5mg,injection 4mg/ml
Hydrocortisone S,T Injection 100mg/ml (as Sodium succinate)
Methylprednisolone S,T Injection 40mg/ml
Prednisolone* U Tablet 5mg, 10mg
18.2 Androgens
Testosterone* S,T Injection 10mg/ml, 25mg/ml
18.3 Contraceptives
Condoms with or without
Spermiciede
U
IUD containing Copper U
Centchroman U Tablet 30mg
Ethinylestradiol + Norethisterone U Tablet 35 µg + 1mg
Ethinylestradiol + Levonorgestrel U Tablet 30 µg + 150 µg, 50µg + 250µg
Clomiphene citrate U Tablet 25mg, 50mg
18.4 Estrogens
Ethinylestradiol U Tablet 50 µ g
Conjugated oestrogen Tablet 0.62mg
18.5 Insulins and other antidiabetic agents
Glibenclamide U Tablet 5mg
Insulin injection (soluble) U Injection 40 IU/ml
Intermediate acting insulin
(Lente/NPH insulin)
U Injection 40 IU/ml
Insulin 30/70 U Injection 40 IU/ml
Metformin U Tablet 500 mg
Gliclazide U Tablet 40mg, 80mg
Glimepiride U Tablet 1mg, 2mg, 4mg
18.6 Progestrogens
Norethisterone U Tablet 5mg
17 Hydroxy progesterone acetate S,T Injection 250mg
Carboprost S,T Injection 125mg, 250mg
18.7 Thyroid hormones and Antithyroid drugs
Carbimazole S,T Tablet 5mg
Levothyroxine S,T Tablet 0.1mg
Propyl thiouracil S,T Tablet 50mg
19. IMMU#OLOGICALS
19.1 Diagnostic agents
Tuberculin, Purified protein
derivative
U injection
19.2 Sera and Immunoglobulins
Anti-snake venom U Injection 10ml
56
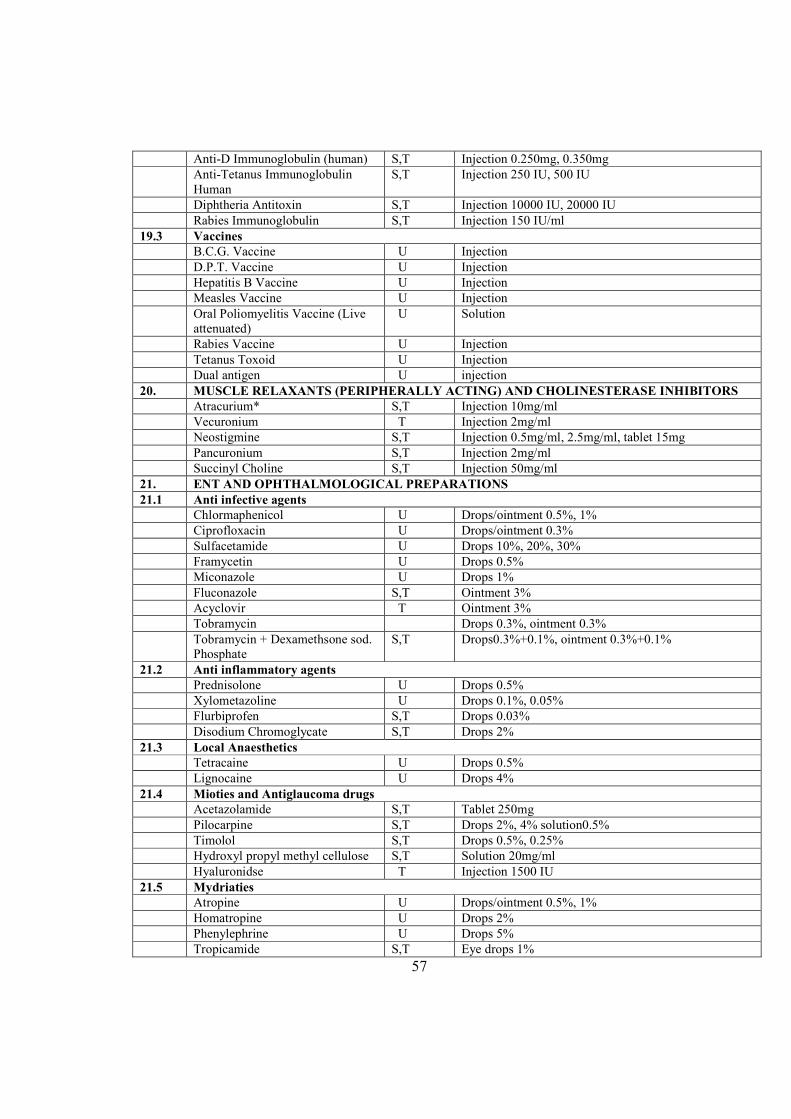
Anti-D Immunoglobulin (human) S,T Injection 0.250mg, 0.350mg
Anti-Tetanus Immunoglobulin
Human
S,T Injection 250 IU, 500 IU
Diphtheria Antitoxin S,T Injection 10000 IU, 20000 IU
Rabies Immunoglobulin S,T Injection 150 IU/ml
19.3 Vaccines
B.C.G. Vaccine U Injection
D.P.T. Vaccine U Injection
Hepatitis B Vaccine U Injection
Measles Vaccine U Injection
Oral Poliomyelitis Vaccine (Live
attenuated)
U Solution
Rabies Vaccine U Injection
Tetanus Toxoid U Injection
Dual antigen U injection
20. MUSCLE RELAXA#TS (PERIPHERALLY ACTI#G) A#D CHOLI#ESTERASE I#HIBITORS
Atracurium* S,T Injection 10mg/ml
Vecuronium T Injection 2mg/ml
Neostigmine S,T Injection 0.5mg/ml, 2.5mg/ml, tablet 15mg
Pancuronium S,T Injection 2mg/ml
Succinyl Choline S,T Injection 50mg/ml
21. E#T A#D OPHTHALMOLOGICAL PREPARATIO#S
21.1 Anti infective agents
Chlormaphenicol U Drops/ointment 0.5%, 1%
Ciprofloxacin U Drops/ointment 0.3%
Sulfacetamide U Drops 10%, 20%, 30%
Framycetin U Drops 0.5%
Miconazole U Drops 1%
Fluconazole S,T Ointment 3%
Acyclovir T Ointment 3%
Tobramycin Drops 0.3%, ointment 0.3%
Tobramycin + Dexamethsone sod.
Phosphate
S,T Drops0.3%+0.1%, ointment 0.3%+0.1%
21.2 Anti inflammatory agents
Prednisolone U Drops 0.5%
Xylometazoline U Drops 0.1%, 0.05%
Flurbiprofen S,T Drops 0.03%
Disodium Chromoglycate S,T Drops 2%
21.3 Local Anaesthetics
Tetracaine U Drops 0.5%
Lignocaine U Drops 4%
21.4 Mioties and Antiglaucoma drugs
Acetazolamide S,T Tablet 250mg
Pilocarpine S,T Drops 2%, 4% solution0.5%
Timolol S,T Drops 0.5%, 0.25%
Hydroxyl propyl methyl cellulose S,T Solution 20mg/ml
Hyaluronidse T Injection 1500 IU
21.5 Mydriaties
Atropine U Drops/ointment 0.5%, 1%
Homatropine U Drops 2%
Phenylephrine U Drops 5%
Tropicamide S,T Eye drops 1%
57
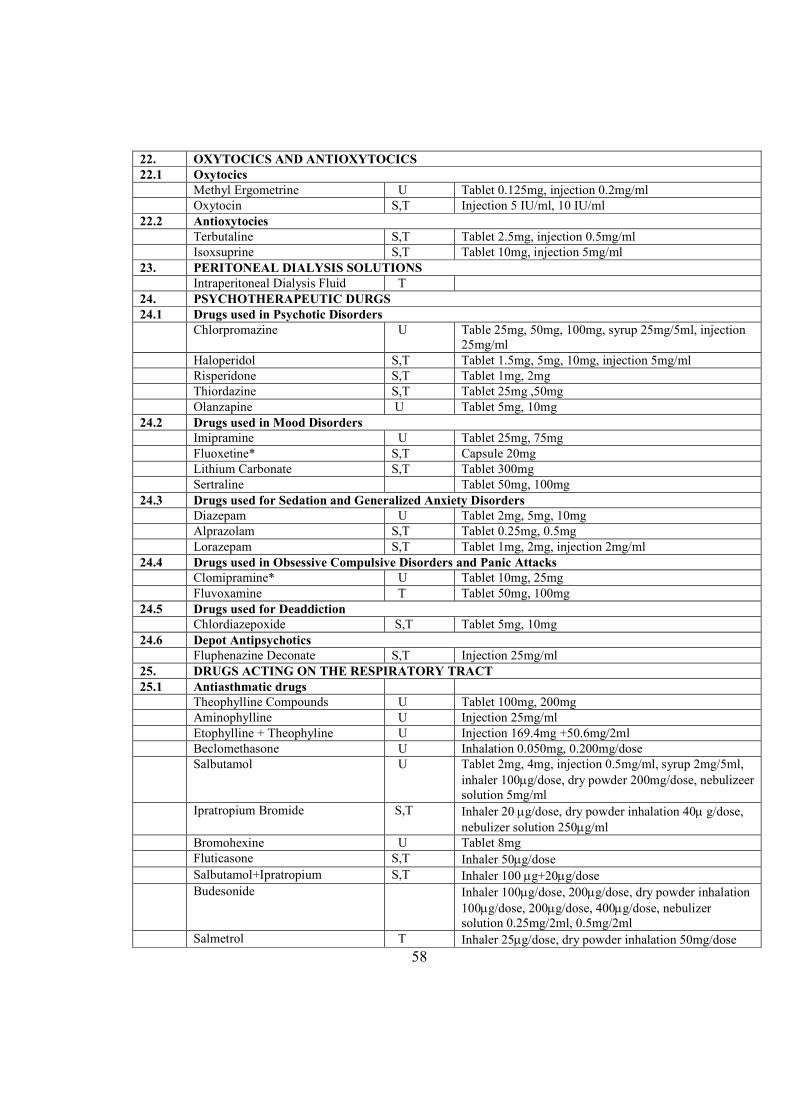
22. OXYTOCICS A#D A#TIOXYTOCICS
22.1 Oxytocics
Methyl Ergometrine U Tablet 0.125mg, injection 0.2mg/ml
Oxytocin S,T Injection 5 IU/ml, 10 IU/ml
22.2 Antioxytocies
Terbutaline S,T Tablet 2.5mg, injection 0.5mg/ml
Isoxsuprine S,T Tablet 10mg, injection 5mg/ml
23. PERITO#EAL DIALYSIS SOLUTIO#S
Intraperitoneal Dialysis Fluid T
24. PSYCHOTHERAPEUTIC DURGS
24.1 Drugs used in Psychotic Disorders
Chlorpromazine U Table 25mg, 50mg, 100mg, syrup 25mg/5ml, injection
25mg/ml
Haloperidol S,T Tablet 1.5mg, 5mg, 10mg, injection 5mg/ml
Risperidone S,T Tablet 1mg, 2mg
Thiordazine S,T Tablet 25mg ,50mg
Olanzapine U Tablet 5mg, 10mg
24.2 Drugs used in Mood Disorders
Imipramine U Tablet 25mg, 75mg
Fluoxetine* S,T Capsule 20mg
Lithium Carbonate S,T Tablet 300mg
Sertraline Tablet 50mg, 100mg
24.3 Drugs used for Sedation and Generalized Anxiety Disorders
Diazepam U Tablet 2mg, 5mg, 10mg
Alprazolam S,T Tablet 0.25mg, 0.5mg
Lorazepam S,T Tablet 1mg, 2mg, injection 2mg/ml
24.4 Drugs used in Obsessive Compulsive Disorders and Panic Attacks
Clomipramine* U Tablet 10mg, 25mg
Fluvoxamine T Tablet 50mg, 100mg
24.5 Drugs used for Deaddiction
Chlordiazepoxide S,T Tablet 5mg, 10mg
24.6 Depot Antipsychotics
Fluphenazine Deconate S,T Injection 25mg/ml
25. DRUGS ACTI#G O# THE RESPIRATORY TRACT
25.1 Antiasthmatic drugs
Theophylline Compounds U Tablet 100mg, 200mg
Aminophylline U Injection 25mg/ml
Etophylline + Theophyline U Injection 169.4mg +50.6mg/2ml
Beclomethasone U Inhalation 0.050mg, 0.200mg/dose
Salbutamol U Tablet 2mg, 4mg, injection 0.5mg/ml, syrup 2mg/5ml,
inhaler 100µg/dose, dry powder 200mg/dose, nebulizeer
solution 5mg/ml
Ipratropium Bromide S,T Inhaler 20 µg/dose, dry powder inhalation 40µ g/dose,
nebulizer solution 250µg/ml
Bromohexine U Tablet 8mg
Fluticasone S,T Inhaler 50µg/dose
Salbutamol+Ipratropium S,T Inhaler 100 µg+20µg/dose
Budesonide Inhaler 100µg/dose, 200µg/dose, dry powder inhalation
100µg/dose, 200µg/dose, 400µg/dose, nebulizer
solution 0.25mg/2ml, 0.5mg/2ml
Salmetrol T Inhaler 25µg/dose, dry powder inhalation 50mg/dose
58
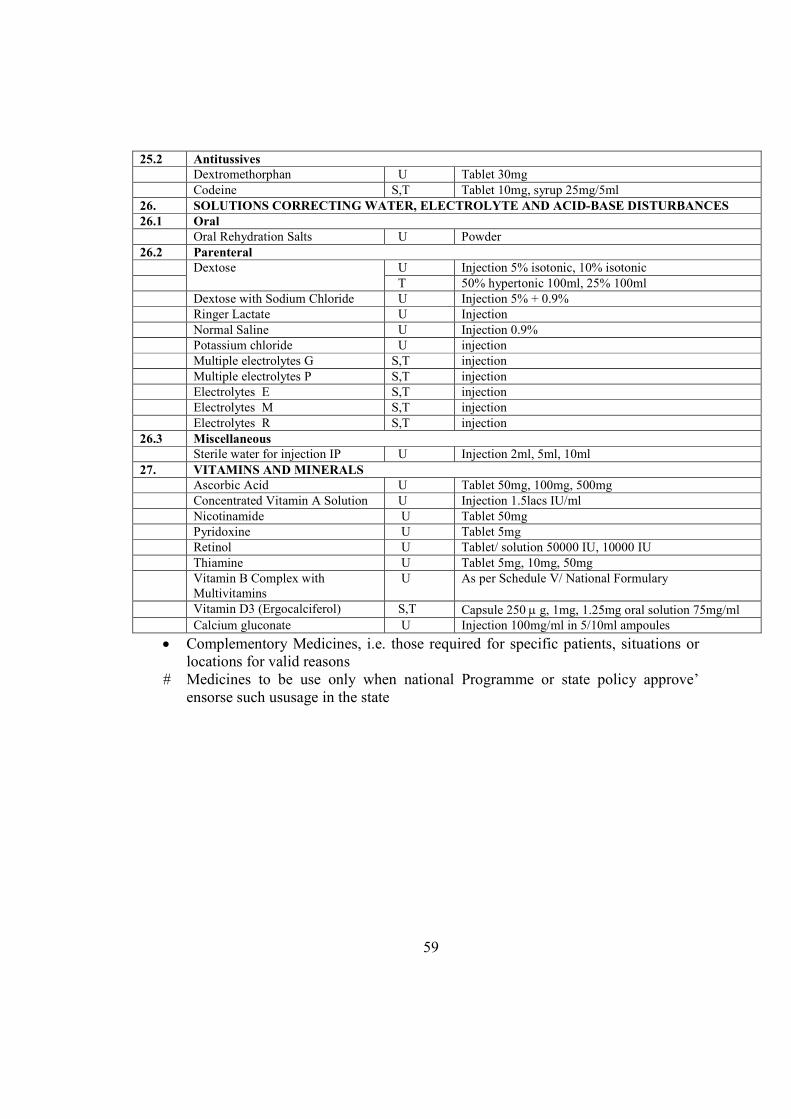
25.2 Antitussives
Dextromethorphan U Tablet 30mg
Codeine S,T Tablet 10mg, syrup 25mg/5ml
26. SOLUTIO#S CORRECTI#G WATER, ELECTROLYTE A#D ACID-BASE DISTURBA#CES
26.1 Oral
Oral Rehydration Salts U Powder
26.2 Parenteral
Dextose U Injection 5% isotonic, 10% isotonic
T 50% hypertonic 100ml, 25% 100ml
Dextose with Sodium Chloride U Injection 5% + 0.9%
Ringer Lactate U Injection
Normal Saline U Injection 0.9%
Potassium chloride U injection
Multiple electrolytes G S,T injection
Multiple electrolytes P S,T injection
Electrolytes E S,T injection
Electrolytes M S,T injection
Electrolytes R S,T injection
26.3 Miscellaneous
Sterile water for injection IP U Injection 2ml, 5ml, 10ml
27. VITAMI#S A#D MI#ERALS
Ascorbic Acid U Tablet 50mg, 100mg, 500mg
Concentrated Vitamin A Solution U Injection 1.5lacs IU/ml
Nicotinamide U Tablet 50mg
Pyridoxine U Tablet 5mg
Retinol U Tablet/ solution 50000 IU, 10000 IU
Thiamine U Tablet 5mg, 10mg, 50mg
Vitamin B Complex with
Multivitamins
U As per Schedule V/ National Formulary
Vitamin D3 (Ergocalciferol) S,T Capsule 250 µ g, 1mg, 1.25mg oral solution 75mg/ml
Calcium gluconate U Injection 100mg/ml in 5/10ml ampoules
• Complementory Medicines, i.e. those required for specific patients, situations or
locations for valid reasons
# Medicines to be use only when national Programme or state policy approve’
ensorse such ususage in the state
59
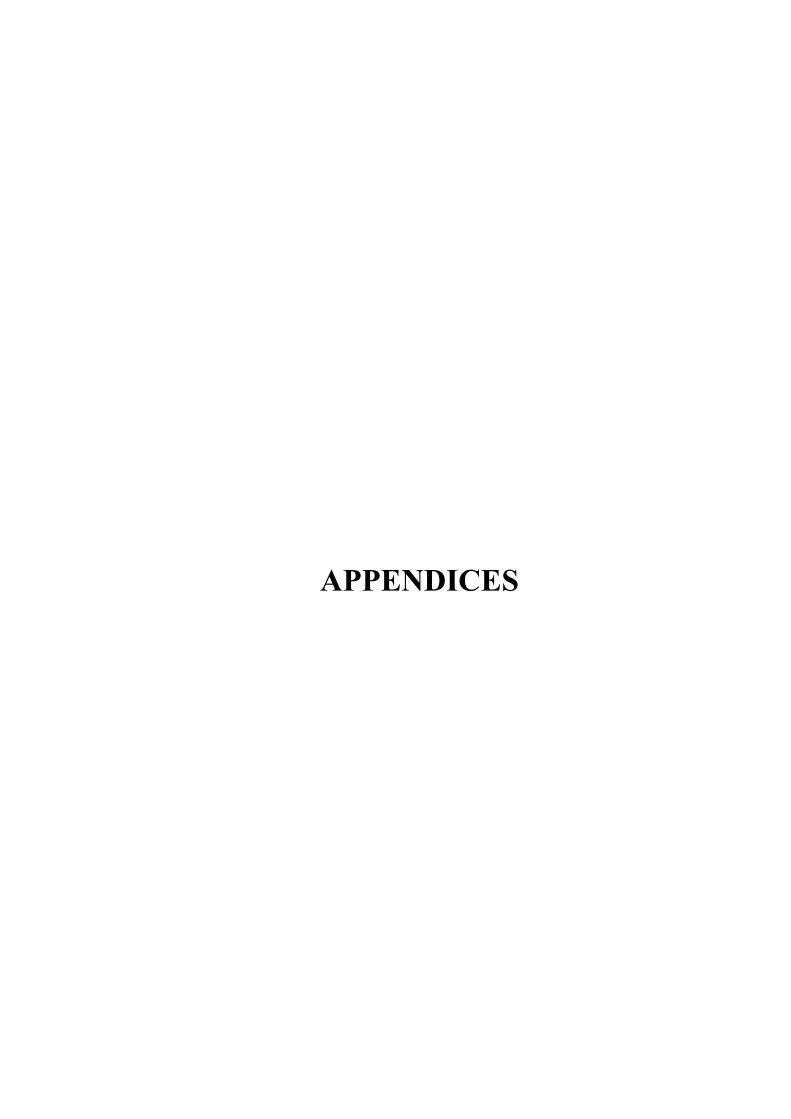
APPE#DICES
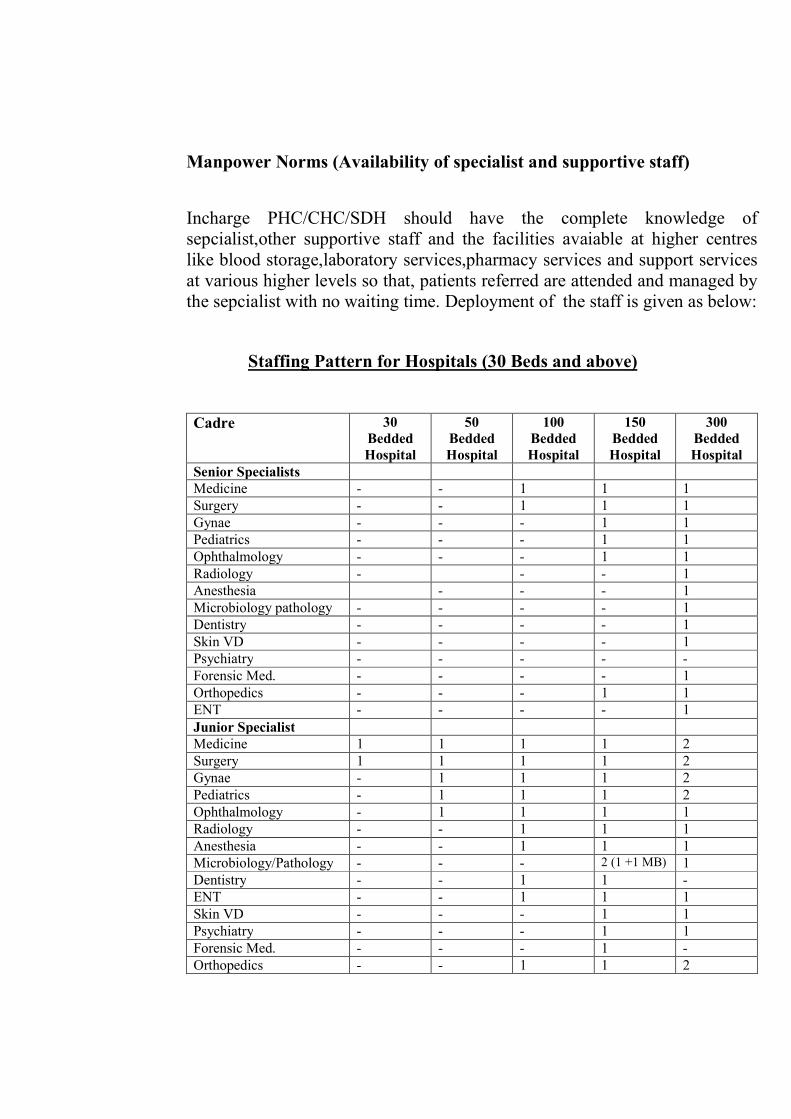
Manpower #orms (Availability of specialist and supportive staff)
Incharge PHC/CHC/SDH should have the complete knowledge of
sepcialist,other supportive staff and the facilities avaiable at higher centres
like blood storage,laboratory services,pharmacy services and support services
at various higher levels so that, patients referred are attended and managed by
the sepcialist with no waiting time. Deployment of the staff is given as below:
Staffing Pattern for Hospitals (30 Beds and above)
Cadre 30
Bedded
Hospital
50
Bedded
Hospital
100
Bedded
Hospital
150
Bedded
Hospital
300
Bedded
Hospital
Senior Specialists
Medicine - - 1 1 1
Surgery - - 1 1 1
Gynae - - - 1 1
Pediatrics - - - 1 1
Ophthalmology - - - 1 1
Radiology - - - 1
Anesthesia - - - 1
Microbiology pathology - - - - 1
Dentistry - - - - 1
Skin VD - - - - 1
Psychiatry - - - - -
Forensic Med. - - - - 1
Orthopedics - - - 1 1
ENT - - - - 1
Junior Specialist
Medicine 1 1 1 1 2
Surgery 1 1 1 1 2
Gynae - 1 1 1 2
Pediatrics - 1 1 1 2
Ophthalmology - 1 1 1 1
Radiology - - 1 1 1
Anesthesia - - 1 1 1
Microbiology/Pathology - - - 2 (1 +1 MB) 1
Dentistry - - 1 1 -
ENT - - 1 1 1
Skin VD - - - 1 1
Psychiatry - - - 1 1
Forensic Med. - - - 1 -
Orthopedics - - 1 1 2
TB - - - 1 1
Medical Officers
Senior Medical 1 1 3 4 (3+1*) 5 (4 +1*)
Medical Officer 5(2+3#) 5 8 12 30
#ursing Staff
Nursing Supdt. Gr. I/II - - 1 1 2 (1+1)
Nurse Gr. I 1 2 (1F +
1M)
8 10
(3F+7M)
20
(5F+15M)
Nurse Gr. II 9 (6+3 #) 14
(4F+10M)
28 30
(10F+20M)
60
(20F+40M)
Technical Staff
Radiographer/ Assistant
Radiographer
1 1 2 (1+1) 4 (2+2) 4 (2+2)
Lab. Technician 1 1 2 4 (3+1**) 5
Dental Technician - 1 1 1 2 (1J+1S)
Physiotherapist - - - 1J 1S
Pharmacist 1 1 1 1J 1S
Ophthalmic Assist - 1 1 2 2
Administrative Staff
Office Superintendent - - - - 1
Office Assistant - - - 1 -
Accountant - - - 1 1
Junior Accountant - - 1 1 2
UDC 1 1 2 2 3
LDC 1 1 4 4 5
Support Staff
Driver (Contract
Services)
- - - - -
Ward Boy 9 10 15 33 66
Sweeper 1 2 5 8 10
* Deputy Controller (SMO Cadre), ** Senior Technician, J Junior, S Senior,
MB Microbiologist, # Round the clock, F Female, M Male.
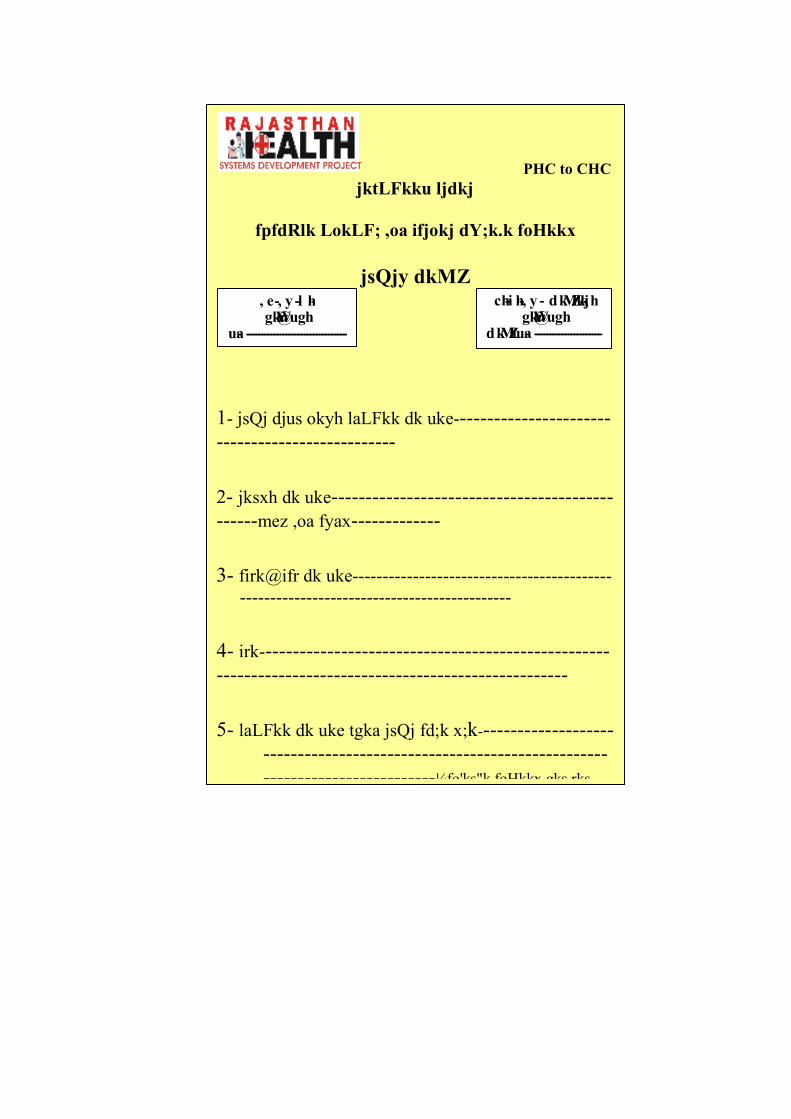
PHC to CHC
jktLFkku ljdkj
fpfdRlk LokLF; ,oa ifjokj dY;k.k foHkkx
jsQjy dkMZ ch-i h-, y - dkMZ/kkjh
gkWa@ugh dkMZa ua- ----------------------
, e-, y -l h- gkWa@ugh
ua- -----------------------------------
1- jsQj djus okyh laLFkk dk uke-----------------------
--------------------------
2- jksxh dk uke-----------------------------------------
------mez ,oa fyax-------------
3- firk@ifr dk uke-------------------------------------------
---------------------------------------------
4- irk---------------------------------------------------
---------------------------------------------------
5- laLFkk dk uke tgka jsQj fd;k x;k--------------------
--------------------------------------------------
-------------------------¼fo'ks"k foHkkx gks rks
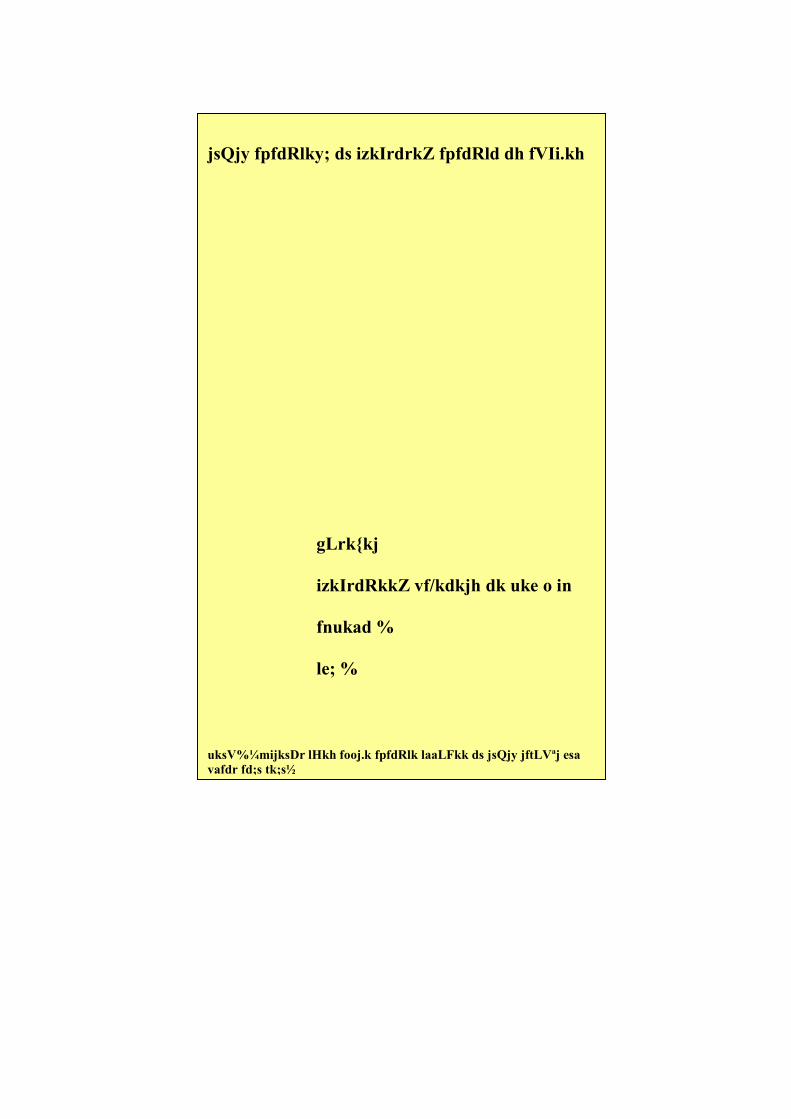
jsQjy fpfdRlky; ds izkIrdrkZ fpfdRld dh fVIi.kh
gLrk{kj
izkIrdRkkZ vf/kdkjh dk uke o in
fnukad %
le; %
uksV%¼mijksDr lHkh fooj.k fpfdRlk laaLFkk ds jsQjy jftLVªj esa
vafdr fd;s tk;s½
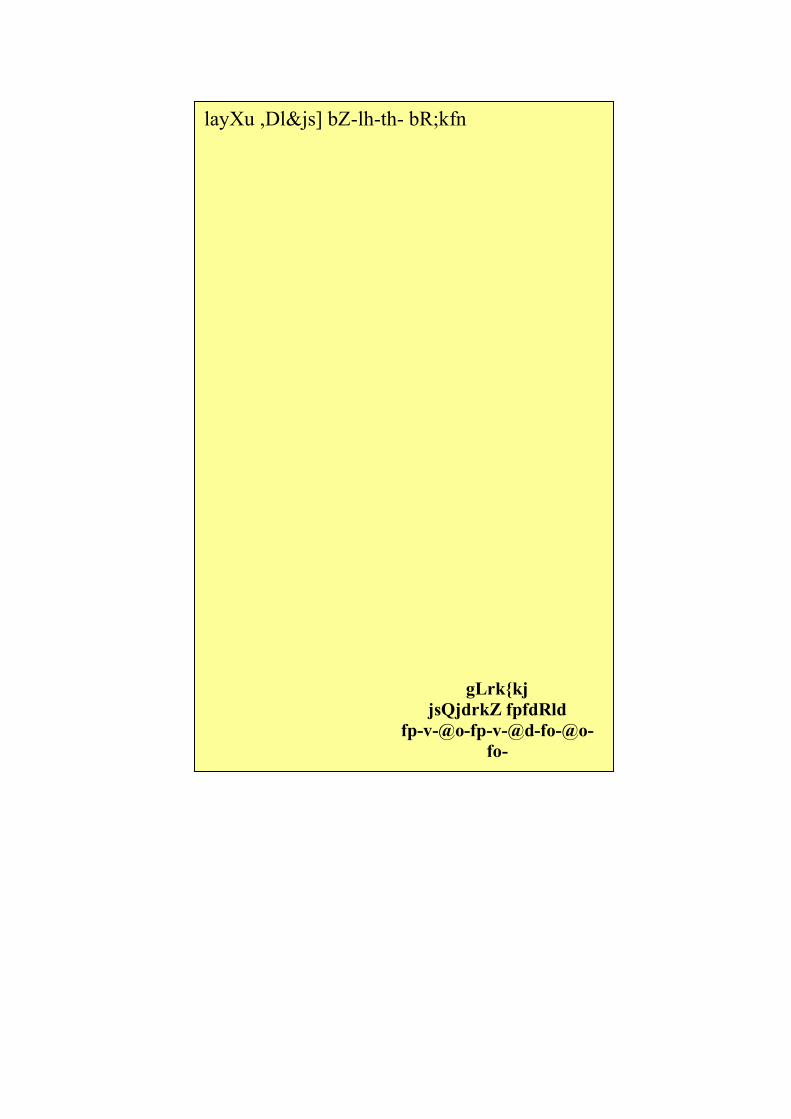
layXu ,Dl&js] bZ-lh-th- bR;kfn
gLrk{kj
jsQjdrkZ fpfdRld
fp-v-@o-fp-v-@d-fo-@o-
fo-
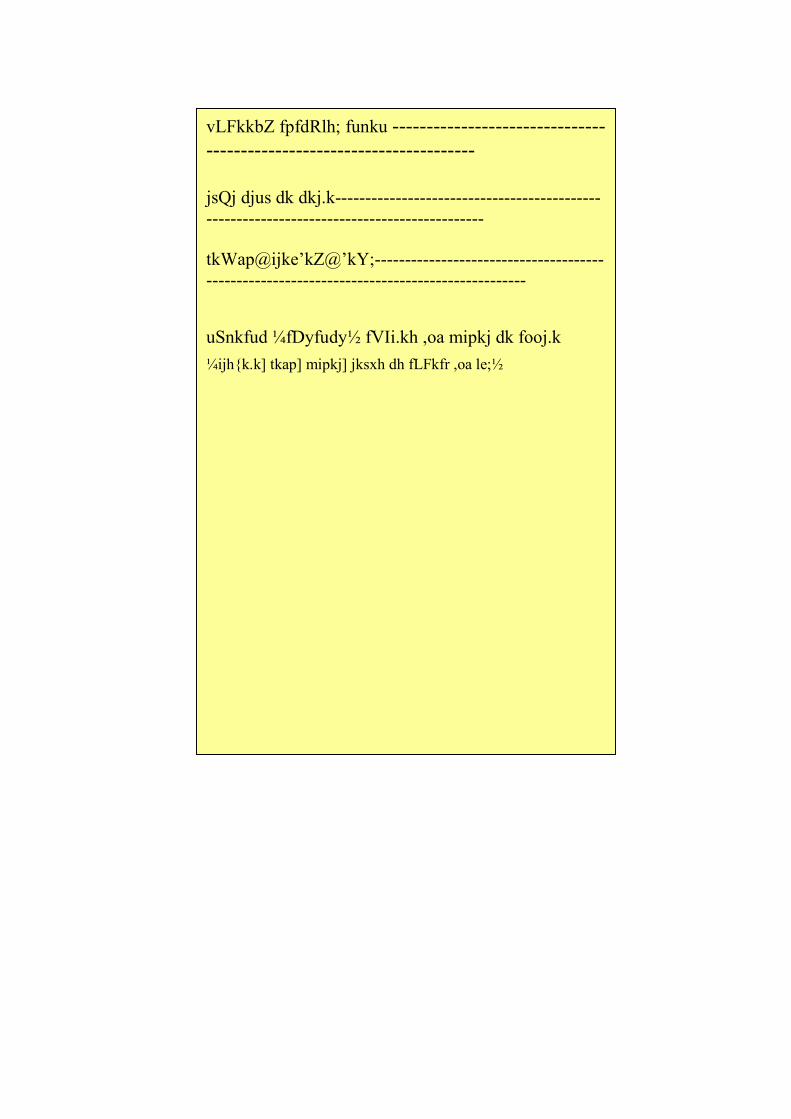
vLFkkbZ fpfdRlh; funku -------------------------------
---------------------------------------
jsQj djus dk dkj.k--------------------------------------------
----------------------------------------------
tkWap@ijke’kZ@’kY;--------------------------------------
-----------------------------------------------------
uSnkfud ¼fDyfudy½ fVIi.kh ,oa mipkj dk fooj.k
¼ijh{k.k] tkap] mipkj] jksxh dh fLFkfr ,oa le;½
CHC to SDH
jktLFkku ljdkj
fpfdRlk LokLF; ,oa ifjokj dY;k.k foHkkx
jsQjy dkMZ ch-i h-, y - dkMZ/kkjh
gkWa@ugh dkMZa ua- ----------------------
, e-, y -l h- gkWa@ugh
ua- -----------------------------------
1- jsQj djus okyh laLFkk dk uke-----------------------
--------------------------
2- jksxh dk uke-----------------------------------------
------mez ,oa fyax-------------
3- firk@ifr dk uke-------------------------------------------
---------------------------------------------
4- irk---------------------------------------------------
---------------------------------------------------
5- laLFkk dk uke tgka jsQj fd;k x;k--------------------
--------------------------------------------------
-------------------------¼fo'ks"k foHkkx gks rks

jsQjy fpfdRlky; ds izkIrdrkZ fpfdRld dh fVIi.kh
gLrk{kj
izkIrdRkkZ vf/kdkjh dk uke o in
fnukad %
le; %
uksV%¼mijksDr lHkh fooj.k fpfdRlk laaLFkk ds jsQjy jftLVªj esa
vafdr fd;s tk;s½
layXu ,Dl&js] bZ-lh-th- bR;kfn
gLrk{kj
jsQjdrkZ fpfdRld
fp-v-@o-fp-v-@d-fo-@o-
fo-
vLFkkbZ fpfdRlh; funku -------------------------------
---------------------------------------
jsQj djus dk dkj.k--------------------------------------------
----------------------------------------------
tkWap@ijke’kZ@’kY;--------------------------------------
-----------------------------------------------------
uSnkfud ¼fDyfudy½ fVIi.kh ,oa mipkj dk fooj.k
¼ijh{k.k] tkap] mipkj] jksxh dh fLFkfr ,oa le;½
SDH to DH
jktLFkku ljdkj
fpfdRlk LokLF; ,oa ifjokj dY;k.k foHkkx
jsQjy dkMZ ch-i h-, y - dkMZ/kkjh
gkWa@ugh dkMZa ua- ----------------------
, e-, y -l h- gkWa@ugh
ua- -----------------------------------
1- jsQj djus okyh laLFkk dk uke-----------------------
--------------------------
2- jksxh dk uke-----------------------------------------
------mez ,oa fyax-------------
3- firk@ifr dk uke-------------------------------------------
---------------------------------------------
4- irk---------------------------------------------------
---------------------------------------------------
5- laLFkk dk uke tgka jsQj fd;k x;k--------------------
--------------------------------------------------
-------------------------¼fo'ks"k foHkkx gks rks
jsQjy fpfdRlky; ds izkIrdrkZ fpfdRld dh fVIi.kh
gLrk{kj
izkIrdRkkZ vf/kdkjh dk uke o in
fnukad %
le; %
uksV%¼mijksDr lHkh fooj.k fpfdRlk laaLFkk ds jsQjy jftLVªj esa
vafdr fd;s tk;s½
layXu ,Dl&js] bZ-lh-th- bR;kfn
gLrk{kj
jsQjdrkZ fpfdRld
fp-v-@o-fp-v-@d-fo-@o-
fo-
vLFkkbZ fpfdRlh; funku -------------------------------
---------------------------------------
jsQj djus dk dkj.k--------------------------------------------
----------------------------------------------
tkWap@ijke’kZ@’kY;--------------------------------------
-----------------------------------------------------
uSnkfud ¼fDyfudy½ fVIi.kh ,oa mipkj dk fooj.k
¼ijh{k.k] tkap] mipkj] jksxh dh fLFkfr ,oa le;½
DH to TECHI#G HOSPITAL
jktLFkku ljdkj
fpfdRlk LokLF; ,oa ifjokj dY;k.k foHkkx
jsQjy dkMZ ch-i h-, y - dkMZ/kkjh
gkWa@ugh dkMZa ua- ----------------------
, e-, y -l h- gkWa@ugh
ua- -----------------------------------
1- jsQj djus okyh laLFkk dk uke-----------------------
--------------------------
2- jksxh dk uke-----------------------------------------
------mez ,oa fyax-------------
3- firk@ifr dk uke-------------------------------------------
---------------------------------------------
4- irk---------------------------------------------------
---------------------------------------------------
5- laLFkk dk uke tgka jsQj fd;k x;k--------------------
--------------------------------------------------
-------------------------¼fo'ks"k foHkkx gks rks
jsQjy fpfdRlky; ds izkIrdrkZ fpfdRld dh fVIi.kh
gLrk{kj
izkIrdRkkZ vf/kdkjh dk uke o in
fnukad %
le; %
uksV%¼mijksDr lHkh fooj.k fpfdRlk laaLFkk ds jsQjy jftLVªj esa
vafdr fd;s tk;s½

layXu ,Dl&js] bZ-lh-th- bR;kfn
gLrk{kj
jsQjdrkZ fpfdRld
fp-v-@o-fp-v-@d-fo-@o-
fo-
vLFkkbZ fpfdRlh; funku -------------------------------
---------------------------------------
jsQj djus dk dkj.k--------------------------------------------
----------------------------------------------
tkWap@ijke’kZ@’kY;--------------------------------------
-----------------------------------------------------
uSnkfud ¼fDyfudy½ fVIi.kh ,oa mipkj dk fooj.k
¼ijh{k.k] tkap] mipkj] jksxh dh fLFkfr ,oa le;½

jktLFkku ljdkj
fpfdRlk LokLF; ,oa ifjokj dY;k.k foHkkx
QhMcSd dkMZZ
, e-, y -l h- gkWa@ugh
ua- -----------------------------------
, e-, y -l h- gkWa@ugh
ua- -----------------------------------
1- laLFkku dk uke-------------------------------------------------------
-----------------------------------
2- jksxh dk uke----------------------------------------------------------
--------------------------------------
mez ,oa fyax--------------------------------------------
3- firk@ifr dk uke-------------------------------------------------------
--------------------------------
4- irk----------------------------------------------------------------------
-----------------------------------------------------------------------------
-----------------------------------------------------------------------------
-------------------------
5- laLFkk dk uke]ftls QhMcSd fn;k x;k------------------------------
---------------------
---------------------------------------------------------------------------
layXu ,Dl&js] bZ-lh-th-]bR;kfn
ijke'kZ
¼Qksyksvi ,Mokbt½
gLrk{kj
fpfdRld dk uke ,oa in
fnukad ,oa le;
LFkkbZ fpfdRlh; funku
tkap@ fn;k x;k mipkj
¼tkap] ijh{k.k] fn;k x;k mipkj ,oa okilh ij ejht dh fLFkfr½
State Institute of Health & Family Welfare Rajasthan, Jaipur
Training on Referral System
Program
Day 1
9.30 -10.00 Hrs. Registration
1st Session
(10.00 - 11.30 Hrs.) RHSDP - Introduction, Goals, Objectives
and Structure of organization
2nd
Session
(11.30 - 1.00 Hrs.) Referral norms for Medicine and Psychiatric
cases
1.00 - 2.00 Hrs. Lunch
3rd
Session
(2.00 -3.30 Hrs.) Referral norms for Surgical and Orthopedic
Cases
4th
Session
(3.30 -5.00 Hrs.) Referral norms for Obs. & Gynae diseases
Day 2
1st Session Referral norms for Pediatrics cases
(10.00 - 11.30 Hrs.)
2nd
Session
(11.30 - 1.00 Hrs.) Referral norms for E#T and Ophthalmology
cases
1.00 - 2.00 Hrs. Lunch
3rd
Session
(2.00 -3.30 Hrs.) EML Orientation
4th
Session Orientation on Referral, Feed back Cards and
(3.30 -5.00 Hrs.) Referral register
Expectation from trainee

_________________________________________________________________
Courtesy : Ms. Aparna Arora
Project Director, RHSDP, Jaipur
Concept : Dr. Shiv Chandra Mathur
Director, State Institute of Health & Family Welfare,
Jaipur
Edited by : Dr. B.#. Sharma
Prepared by : Dr. J.P. Jain
Contribution : Dr. S.C. Gupta
Dr. P.S. Bhatnagar
Published by : State Institute of Health & Family Welfare
Rajasthan, Jaipur
May, 2005
___________________________________________________________________