Embed Size (px)
Citation preview
Status Perceptions in a Mental HospitalAuthor(s): Simon Dinitz, Mark Lefton and Benjamin PasamanickSource: Social Forces, Vol. 38, No. 2 (Dec., 1959), pp. 124-128Published by: Oxford University PressStable URL: http://www.jstor.org/stable/2573931 .
Accessed: 15/06/2014 07:02
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
Oxford University Press is collaborating with JSTOR to digitize, preserve and extend access to Social Forces.
http://www.jstor.org
This content downloaded from 91.229.229.177 on Sun, 15 Jun 2014 07:02:28 AMAll use subject to JSTOR Terms and Conditions
124 SOCIAL FORCES
All this suggests that there is little utility in conceiving of the "natural" areas of a city as implying the existence of a real kind of data or a real series of forces which produce real ecological areas. Paul Hatt's20 critical analysis of the natural area as a useful concept in the analysis of human behavior is confirmed by our findings. A distinc- tion needs to be made between natural areas as
logical, statistical constructs integrated with a plan of research, and the concept of natural areas as a series of spatial and social factors which act as coercive influences in ordering the activities of every person within some geographically or cul- turally defined area. The problem of explaining the choices in facilities related to certain common activities of urban dwellers, for example, would seem to require other than an ecological approach in the Park tradition.
20 "The Concept of Natural Area," American Soci- ological Review, 11 (1946), pp. 423-27.
STATUS PERCEPTIONS IN A MENTAL HOSPITAL*
SIMON DINITZ, MARK LEFTON AND BENJAMIN PASAMANICK, M.D.
Columbus Psychiatric Institute and Hospital and Departments of Psychiatry and Sociology, The Ohio State University
A NUMBER of recent studies of the structure and functioning of the mental hospital have attempted to focus at-
tention upon the nature of and the operational consequences of status differences among par- ticipating professional clinical personnel.' These investigations have to a large extent been guided, implicitly or explicitly, by a major assumption concerning the effects of status differentiation upon the care and treatment of patients. It is generally argued that the status system tends to promote and perpetuate staff rigidity, discontent, unhappi- ness and frustration, and thus inhibits the realiza- tion of what is presumed to be an optimal therapeutic environment (i.e., warm, conflict free and harmonious working relationships be- tween and among staff and patients).2 It is ob- vious, then, that one of the crucial dimensions for study in the mental hospital would necessarily involve the ways in which staff members view
the status system which governs them and their interrelationships.
The study reported in this paper attempts to specify some of the conditions and circumstances which influence staff perceptions of accorded and desired status. Contrary to previous investigations in this area,3 it will be shown that staff perceptions of status are affected not only by professional group placement in the official hierarchy but also by the situational context in which they work.
METHOD
This study includes the entire professional staff (both clinical and administrative) of the Columbus Psychiatric Institute and Hospital. This institution is an adjunct of the State De- partment of Mental Hygiene and Correction and the Department of Psychiatry of the College of Medicine at the Ohio State University. The Columbus Psychiatric Institute and Hospital is a short-term, intensive therapy mental hospital with a capacity of 126 beds for voluntary ad- mission cases. This hospital is also a research and training center for a number of specialties including psychiatric residents, nurses, clinical psychologists,
* This research is being undertaken by the Re- search Division of the Columbus Psychiatric Institute and Hospital and is supported by a grant (M 2940) from the National Institute of Mental Health.
1 I See, for example, Alfred H. Stanton and Morris S. Schwartz, The Mental Hospital (New York: Basic Books, 1954); William Caudill, The Psychiatric Hos- pital as a Small Society (Cambridge: Harvard Univer- sity Press, 1958); and, Milton Greenblatt, Richard H. York, and Esther L. Brown, From Custodial to Thera- peutic Patient Care in Mental Hospitals (New York: Russell Sage Foundation, 1955).
2 For a concise summary of this point of view see, Greenblatt, et al, op. cit., pp. 421-422.
3 Two representative works are Alvin Zander, Ar- thur R. Cohen and Ezra Stotland, Role Relations in the Mental Health Professions (Ann Arbor: University of Michigan, 1957); and Salomon Rettig, Frank N. Jacob- son and Benjamin Pasamanick, "Status Overestima- tion, Objective Status and Job Satisfaction Among the Professions," American Sociological Review, XXIII (1958), 75-81.
This content downloaded from 91.229.229.177 on Sun, 15 Jun 2014 07:02:28 AMAll use subject to JSTOR Terms and Conditions

STATUS PERCEPTIONS 125
psychiatric social workers, and occupational therapists. The importance of this hospital for the purposes of this study lies in its attempt to provide each of its five wards with all the various types of psychiatric specialists presumed to be necessary for the effective functioning of the "ideal" clinical team.
Each of the five relatively autonomous wards contains a chief unit psychiatrist, three psychiatric residents, a clinical psychologist, a psychiatric social worker, a complement of registered psy- chiatric nurses, and an occupational therapist. Representatives of each specialty participate in tri-weekly morning conferences designed to provide a formally structured forum for the ex- change of information and the discussion of pa- tients assigned to their particular wards.
As part of a larger study dealing with staff and patient relationships and functioning, all pro- fessional ward personnel of this hospital (total population, 53 persons) were interviewed in- dividually and were asked to make judgments regarding the status and prestige of all the par- ticipating professional groups, including their own. Each of these staff members was asked to estimate the status and prestige levels of each of the co- operating professional groups in terms of (1) how the "general public" would rate each speci- alty, (2) how the entire professional staff of the hospital would rate each of the groups, and (3) how much status and prestige each of the groups, including their own, should have.
These ratings, as well as others pertaining to decision-making influence, competence, job satis- faction, and the effectiveness of the different therapies were made on a magnetic board in- strument which had been developed, tested, and used by another research team at the same hos- pital. Use of this instrument requires the re- spondent to place a magnet or a series of magnets to which the stimuli have been attached upon one or more rating scales ranging from 0-100. This technique permits quantitative comparisons, allows for modification of responses by the in- terviewee, and generally evokes the respondent's interest.4
The entire interview schedule was pre-tested at another institution and appropriate changes
were made. In order to determine instrument -and rater reliability, 25 staff members of the 53 originally tested were retested in three to 51 days after the initial interview. The schedule was found to be reliable and, similarly, respondents were found to be consistent over time. Test- retest reliability was found to be +.78.
Status evaluations were measured in two ways. A status differential score was computed for each respondent by measuring the discrepancy between the ratings he assigned to the highest and lowest professional groups. A second status score involved the raw score given by each respondent for each of the professions evaluated. Both measures were computed in terms of the preferred or "should be" status frame of reference as well as for per- ceived actual status ascriptions of the hospital specialties. 5
FINDINGS
Specifically, the data in this study indicate that perceptions of the hospital status system vary with the professions of the staff members and with the ward settings. Other variables such as length of time in the profession, length of service in the hospital or on a particular ward, and age seem to be relatively minor factors in the per- ceptions of status gradations-actual or ideal.
As noted in Table 1, the profession of the individual as senior psychiatrist, psychologist, nurse, social worker or occupational or recrea- tional therapist seems to be the chief determi- nant of the status and prestige the person feels he should have and the actual amount or level which he feels he is accorded in the hospital. The ward situation operates, however, to maximize or minimize interprofessional differences in status. The ward setting is also highly related to the amount of discrepancy between the status po- sition one perceives himself to have and the amount which he feels he deserves. The characteristics of the role and status incumbent are significant in
4 Salomon Rettig, Frank N. Jacobson and Benjamin Pasamanick, "The Magnetic Board Rating Tech- nique," Journal of Psychology, XXXXV (1958), 201- 206.
5 In addition to the use of rating scales such as those just described, the larger study also involved an analy- sis of the ward behavior of the patients as recorded every half hour over a three-week period. The authors also attended staff conferences on the various wards over a long period of time and participated in all formal and many informal meetings. Lorr Psychiatric Rating Scales were also used. All staff members rated patients 10 days after admission to the ward. In this manner, it was possible to relate staff interaction with patient functioning.
This content downloaded from 91.229.229.177 on Sun, 15 Jun 2014 07:02:28 AMAll use subject to JSTOR Terms and Conditions
126 SOCIAL FORCES
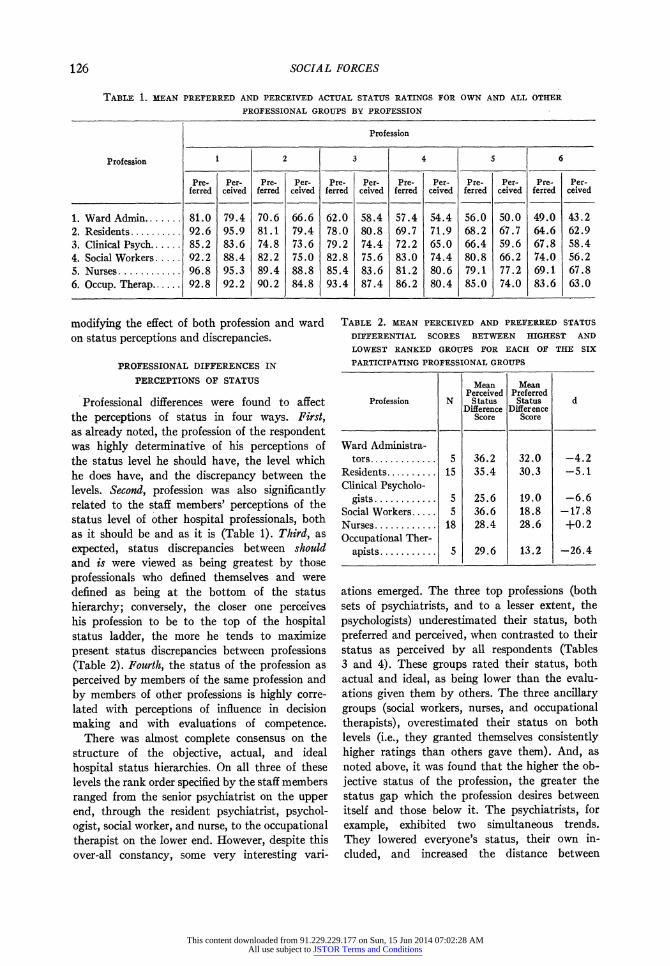
TABLE 1. MEAN PREFERRED AND PERCEIVED ACTUAL STATUS RATINGS FOR OWN AND ALL OTHER
PROFESSIONAL GROUPS BY PROFESSION
Profession
Profession 2 3 4 6
Pre- Per- Pre- Per- Pre- Per- Pre- Per- Pre- Per- Pre- Per- ferred ceived ferred ceived ferred ceived ferred ceived ferred ceived ferred ceived
1. Ward Admin.. 81.0 79.4 70.6 66.6 62.0 58.4 57.4 54.4 56.0 50.0 49.0 43.2 2. Residents .......... 92.6 95.9 81.1 79.4 78.0 80.8 69.7 71.9 68.2 67.7 64.6 62.9 3. Clinical Psych..... . 85.2 83.6 74.8 73.6 79.2 74.4 72.2 65.0 66.4 59.6 67.8 58.4 4. Social Workers. . . . . 92.2 88.4 82.2 75.0 82.8 75.6 83.0 74.4 80.8 66.2 74.0 56.2 5. Nurses ............ 96.8 95.3 89.4 88.8 85.4 83.6 81.2 80.6 79.1 77.2 69.1 67.8 6. Occup. Therap ...... 92.8 92.2 90.2 84.8 93.4 87.4 86.2 80.4 85.0 74.0 83.6 63.0
modifying the effect of both profession and ward on status perceptions and discrepancies.
PROFESSIONAL DIFFERENCES IN
PERCEPTIONS OF STATUS
Professional differences were found to affect the perceptions of status in four ways. First, as already noted, the profession of the respondent was highly determinative of his perceptions of the status level he should have, the level which he does have, and the discrepancy between the levels. Second, profession was also significantly related to the staff members' perceptions of the status level of other hospital professionals, both as it should be and as it is (Table 1). Third, as expected, status discrepancies between should and is were viewed as being greatest by those professionals who defined themselves and were defined as being at the bottom of the status hierarchy; conversely, the closer one perceives his profession to be to the top of the hospital status ladder, the more he tends to maximize present status discrepancies between professions (Table 2). Fourth, the status of the profession as perceived by members of the same profession and by members of other professions is highly corre- lated with perceptions of influence in decision making and with evaluations of competence.
There was almost complete consensus on the structure of the objective, actual, and ideal hospital status hierarchies. On all three of these levels the rank order specified by the staff members ranged from the senior psychiatrist on the upper end, through the resident psychiatrist, psychol- ogist, social worker, and nurse, to the occupational therapist on the lower end. However, despite this over-all constancy, some very interesting vari-
TABLE 2. MEAN PERCEIVED AND PREFERRED STATUS
DIFFERENTIAL SCORES BETWEEN HIGHEST AND
LOWEST RANKED GROUPS FOR EACH OF THE SIX
PARTICIPATING PROFESSIONAL GROUPS
Mean Mean Perceived Preferred
Profession N Status Status d Difference Difference
Score Score
Ward Administra- tors ............. 5 36.2 32.0 -4.2
Residents...... 15 35.4 30.3 -5.1 Clinical Psycholo-
gists ............ 5 25.6 19.0 -6.6 Social Workers ..... 5 36.6 18.8 -17.8 Nurses ............ 18 28.4 28.6 +0.2 Occupational Ther-
apists ........... 5 29.6 13.2 -26.4
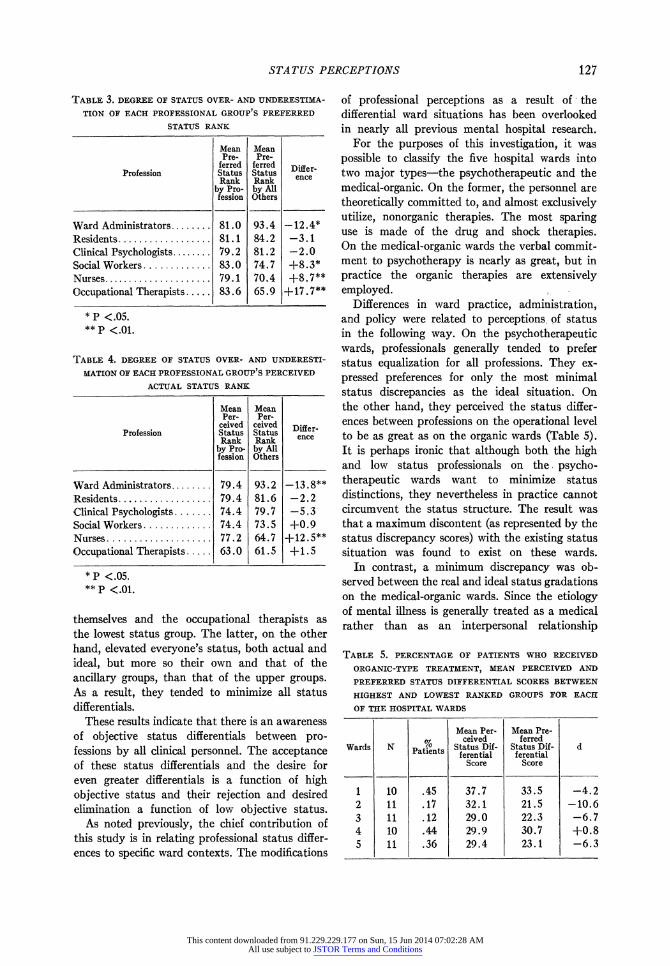
ations emerged. The three top professions (both sets of psychiatrists, and to a lesser extent, the psychologists) underestimated their status, both preferred and perceived, when contrasted to their status as perceived by all respondents (Tables 3 and 4). These groups rated their status, both actual and ideal, as being lower than the evalu- ations given them by others. The three ancillary groups (social workers, nurses, and occupational
therapists), overestimated their status on both
levels (i.e., they granted themselves consistently higher ratings than others gave them). And, as noted above, it was found that the higher the ob- jective status of the profession, the greater the status gap which the profession desires between itself and those below it. The psychiatrists, for example, exhibited two simultaneous trends. They lowered everyone's status, their own in- cluded, and increased the distance between
This content downloaded from 91.229.229.177 on Sun, 15 Jun 2014 07:02:28 AMAll use subject to JSTOR Terms and Conditions
STATUS PERCEPTIONS 127
TABLE 3. DEGREE OF STATUS OVER- AND UNDERESTIMA-
TION OF EACH PROFESSIONAL GROUP S PREFERRED
STATUS RANK
Mean Mean Pre- Pre-
ferred ferred Differ- Profession Status Status enc
Rank Rank ence by Pro- by All fession Others
Ward Administrators ........ 81.0 93.4 -12.4* Residents .................. 81.1 84.2 -3.1 Clinical Psychologists ........ 79.2 81.2 -2.0 Social Workers ............. 83.O 74.7 +8.3* Nurses .................... 79.1 70.4 +8.7** Occupational Therapists. 83.6 65.9 +17.7**
*P <.05. ** P <.01.
TABLE 4. DEGREE OF STATUS OVER- AND UNDERESTI-
MATION OF EACH PROFESSIONAL GROUP S PERCEIVED
ACTUAL STATUS RANK
Mean Mean Per- Per-
ceived ceived Differ- Profession Status Status ee
Rank Rank ec by Pro- by All fession Others
Ward Administrators ........ 79.4 93.2 -13.8** Residents .................. 79.4 81.6 -2.2 Clinical Psychologists ....... 74.4 79.7 -5.3 Social Workers ............. 74.4 73.5 +0.9 Nurses .................... 77.2 64.7 +12.5** Occupational Therapists ..... 63.0 61.5 +1.5
*p <.05. ** P <.01.
themselves and the occupational therapists as the lowest status group. The latter, on the other hand, elevated everyone's status, both actual and ideal, but more so their own and that of the ancillary groups, than that of the upper groups. As a result, they tended to minimize all status differentials.
These results indicate that there is an awareness of objective status differentials between pro- fessions by all clinical personnel. The acceptance of these status differentials and the desire for even greater differentials is a function of high objective status and their rejection and desired elimination a function of low objective status.
As noted previously, the chief contribution of this study is in relating professional status differ- ences to specific ward contexts. The modifications
of professional perceptions as a result of - the differential ward situations has been overlooked in nearly all previous mental hospital research.
For the purposes of this investigation, it was possible to classify the five hospital wards into two major types-the psychotherapeutic and the medical-organic. On the former, the personnel are theoretically committed to, and almost exclusively utilize, nonorganic therapies. The most sparing use is made of the drug and shock therapies. On the medical-organic wards the verbal commit- ment to psychotherapy is nearly as great, but in practice the organic therapies are extensively employed.
Differences in ward practice, administration, and policy were related to perceptions, of status in the following way. On the psychotherapeutic wards, professionals generally tended to prefer status equalization for all professions. They ex- pressed preferences for only the most minimal status discrepancies as the ideal situation. On the other hand, they perceived the status differ- ences between professions on the operational level to be as great as on the organic wards (Table 5). It is perhaps ironic that although both the high and low status professionals on the. psycho- therapeutic wards want to minimize status distinctions, they nevertheless in practice cannot circumvent the status structure. The result was that a maximum discontent (as represented by the status discrepancy scores) with the existing status situation was found to exist on these wards.
In contrast, a minimum discrepancy was ob- served between the real and ideal status gradations on the medical-organic wards. Since the etiology of mental illness is generally treated as a medical rather than as an interpersonal relationship
TABLE 5. PERCENTAGE OF PATIENTS WHO RECEIVED
ORGANIC-TYPE TREATMENT, MEAN PERCEIVED AND
PREFERRED STATUS DIFFERENTIAL SCORES BETWEEN
HIGHEST AND LOWEST RANKED GROUPS FOR EACH
OF THE HOSPITAL WARDS
Mean Per. Mean Pre- %C ceived ferred
Wards N PainsStatus Dif- Status Dif- d Wa N Patients ferential f erential Score Score
1 10 .45 37.7 33.5 -4.2 2 11 .17 32.1 21.5 -10.6 3 11 .12 29.0 22.3 -6.7 4 10 .44 29.9 30.7 +0.8 5 11 .36 29.4 23.1 -6.3
This content downloaded from 91.229.229.177 on Sun, 15 Jun 2014 07:02:28 AMAll use subject to JSTOR Terms and Conditions

128 SOCIAL FORCES
problem on these organic type wards, the tradi- tional medical status hierarchy tends to be ac- cepted as the ideal and is also perceived as the real. The result is that status aspirations and expectations tend to coincide with the traditional medical profession distinctions.
DISCUSSION AND CONCLUSIONS
The findings indicated that professionals tend to perceive their actual and preferred status through the eyes of their profession or specialty. All specialists agreed on the status hierarchy as presently constituted but disagreed on the ideal status and prestige gradations.
Those occupying the upper rungs of the status ladder underestimated their own status when compared to the amount ascribed to them by the other professions. Similarly, the ancillary pro- fessional specialists overestimated their own status. The higher one perceives the status of his profession to be, the greater his desire to main- tain and enlarge present status discrepancies between his own and the lower status professions. Those professionals desiring status equality or near equality as the ideal were inevitably those who perceived themselves as having little actual status.
Apart from these profession related discrepancies in perceptions of actual and ideal status, the great- est and most interesting differences were those related to ward assignment. Professionals as- signed to the two wards which shun the use of organic therapies (drugs and electroshock) espoused the concept of relative status equality among all professional personnel. In practice, however, professionals on these wards indicated they had no greater amount of status and influence on decisions than comparable professionals on
the organic type wards. Hence, the greatest discrepancy between the "should" and the "is" occurred precisely on those wards which deem such discrepancies as most deleterious for patient welfare and for the smoothly functioning clinical team.
On the organic wards, in contrast, wide dis- crepancies were perceived in the status of the different professions. However, these same status discrepancies were preferred as the ideal ward hospital situation. Professionals accepted these differences as both real and ideal. Furthermore, on these wards the various professions indicated a greater feeling of achievement, ascribed greater competence to each profession and tended to have greater consensus on the evaluation of patients.
It would appear, therefore, that in the absence of adequate criteria through which the specific contributions to patient improvement of all pro- fessional groups can be measured, the ancillary hospital professionals will continue to aspire to the greater equalization of status. The develop- ment of these measurable criteria of contributions to patient improvement should result in more rational status distinctions and the greater pro- fessional acceptance of these gradations. To the extent that each specialist, whether in a mental hospital or elsewhere can, or believes he can, function as adequately and perform the same duties as well as other specialists, he will tend to be dissatisfied with any lesser status than that which the specialists with whom he shares thera- peutic responsibilities are endowed. On medical type wards there are, of necessity, fewer areas of aggrandizement of functions, while psycho- therapeutic wards lend themselves to this blurring of functions and with it, to increased conflicts over status.
This content downloaded from 91.229.229.177 on Sun, 15 Jun 2014 07:02:28 AMAll use subject to JSTOR Terms and Conditions