Embed Size (px)
Citation preview

Eciri
Fpv
M
aa
Hb
Step-Cut Distal Ulnar–ShorteningOsteotomy
Nickolaos A. Darlis, MD, Italo C. Ferraz, MD,Robert W. Kaufmann, MD, Dean G. Sotereanos, MD, Pittsburgh, PA
Purpose: Several techniques for ulnar-shortening osteotomies have been described in recent years,reflecting the difficulties that sometimes are encountered in what seems to be a relatively simpleprocedure. We describe the use of a simple step-cut ulnar-shortening osteotomy stabilized with alag screw and a palmarly placed 3.5-mm neutralization plate.Methods: Twenty-nine patients had the surgery. The indication was ulnar-impaction syndrome in23 patients and symptomatic ulnar-plus variance secondary to trauma in 6 patients (4 with previousdistal radius fractures, 2 with Essex-Lopresti injuries). The preoperative ulnar variance ranged from�1 mm to �6 mm.Results: The mean follow-up period was 34 months. All osteotomies healed uneventfully. Themean postoperative ulnar variance was �0.2 mm (range, �1 mm to �1.5 mm). Three patients hadhardware removal.Conclusions: The step-cut osteotomy resulted in solid union in all patients. It provides ample bone-to-bone contact and easier control of rotation, and no special instrumentation is necessary. Stablefixation permitted early mobilization of the wrist and palmar placement of the plate minimizedthe need for plate removal. This is a simple and effective technique for ulnar shortening. (JHand Surg 2005;30A:943–948. Copyright © 2005 by the American Society for Surgery of theHand.)
Key words: Osteotomy, step-cut, ulna shortening, ulnar-impaction syndrome.vbfis
vbomguvpctme
xtra-articular ulnar shortening is an established pro-edure for treating ulnar-impaction syndrome. It alsos used to treat distal radioulnar joint (DRUJ) de-angement secondary to malunions or Essex-Loprestinjuries provided that DRUJ arthritis has not pre-
rom the Department of Orthopaedic Surgery, Allegheny General Hos-ital, Pittsburgh, PA; and the Department of Orthopaedic Surgery, Uni-ersity of Pittsburgh Medical Center, Pittsburgh, PA.Received for publication February 14, 2005; accepted in revised formay 30, 2005.No benefits in any form have been received or will be received fromcommercial party related directly or indirectly to the subject of this
rticle.Corresponding author: Dean G. Sotereanos, MD, Allegheny General
ospital, Department of Orthopaedic Surgery, 1307 Federal St, Pitts-urgh, PA 15212; e-mail: [email protected] © 2005 by the American Society for Surgery of the Hand0363-5023/05/30A05-0009$30.00/0
pdoi:10.1016/j.jhsa.2005.05.010
ailed. Several techniques for this osteotomy haveeen described in recent years,1–11 reflecting the dif-culties that sometimes are encountered in whateems to be a relatively simple procedure.
The configuration of the cut usually is either trans-erse or oblique. Difficulties are encountered withoth of these configurations. With transverse osteot-mies1,2,5–7 the rotation control can be problematic;oreover the cuts must be perfectly parallel to ensure
ood bone apposition and compression to avoid non-nion or malunion. Oblique osteotomies3,4,8–11 pro-ide a larger contact surface, facilitating union, butroper alignment still necessitates perfectly paralleluts and rotation control. Their fixation must followhe principles of antiglide plating12 and the place-
ent of a lag screw can be difficult. Furthermore thexact amount of shortening achieved is highly de-
endent on the exact angle of the osteotomy—it canThe Journal of Hand Surgery 943

br
mwesbftdommaconpcosl
dcsoti
oovacsspsaptu
w
MFtys
(vriu(La(Utpia2b3pumpce
Fftimapp
944 The Journal of Hand Surgery / Vol. 30A No. 5 September 2005
e as much as double the size of the wafer of boneemoved for a 60o osteotomy.4
Several devices that can facilitate these osteoto-ies have been described. Single-cut osteotomiesith multiple blades mounted on the power saw4
nsure parallel cuts, but the amount of shorteningtill depends on the angle of the cut and multiplelade sizes must be available to accommodate dif-erent amounts of shortening. Shortening by usinghe compression features of the limited contact–ynamic compression plate plate applied before thesteotomy11 is complicated and limits shortening to aaximum of 2.5 mm. A long oblique osteotomyade with a specialized jig10 allows control over the
mount of shortening but translation of the bone endsan be problematic with larger shortenings. Fixationf the long oblique osteotomy with only 4 screws isot as secure as plate fixation and requires longerrotection. The use of external fixation devices toontrol rotation and facilitate reduction in transversesteotomies has been proposed3,5 but these do notolve the problem of parallel cuts and involve aearning curve.
Dedicated ulnar-shortening devices also have beenescribed.3,8 These provide parallel cuts that are ac-urate both in width and in angle but they requirepecialized equipment (eg, jigs,3,8 plates3). Becausef the bulky jigs that must be used volar placement ofhe plate (which is desired to avoid extensor tendonrritation caused by attrition) is difficult.
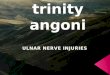
Bowers13 alluded to the use of a step-cut osteot-my for ulnar shortening. The step-cut configurationffers larger contact surfaces compared with trans-erse osteotomies and better control of rotation. Withppropriate surgical technique accurate shorteningan be performed freehand. The technique we use fortep-cut ulnar shortening places the long arm of thetep-cut in the coronal plane and the short armserpendicular to that in the axial plane (Fig. 1A), andtable fixation can be achieved with a lag screw andvolarly placed 3.5-mm neutralization plate. Volar
lacement of the plate avoids extensor tendon irrita-ion. The osteotomy can be designed reproduciblysing the 3.5-mm plate as a template.In this study we present our technique and results
ith a step-cut ulnar-shortening osteotomy.
aterials and Methodsrom 2000 to 2003, there were 29 consecutive pa-
ients (13 male, 16 female) with a mean age of 35.3ears (range, 14–55 y) who had a step-cut ulnar-
hortening osteotomy performed by the senior author fD.G.S.). The records of those patients were re-iewed retrospectively after obtaining institutionaleview board approval. The indication was ulnar-mpaction syndrome in 23 patients and symptomaticlna-plus variance secondary to trauma in 6 patients4 with previous distal radius fractures, 2 with Essex-opresti injuries). The preoperative ulnar varianceveraged �2.7 mm and ranged from �1 to �6 mm�1 to �4 mm in the ulnocarpal-impaction group).lnar variance was assessed radiographically with
he pronated grip view14 in all patients. Fourteenatients had previous procedures performed includ-ng distal radius fracture open reduction internal fix-tion in 1, radial head excision and DRUJ pinning in, arthroscopic triangular fibrocartilage complex de-ridement in 8, and arthroscopic wafer procedures in. Eleven of the patients systematically used tobaccoroducts. The goal of the osteotomy was to reducelnar variance to neutral or to �1 mm. In posttrau-atic cases with distorted anatomy, slight (1–2 mm)
ostoperative ulnar-positive variance was allowed iforrection to neutral would cause DRUJ incongru-nce.
Wrist arthroscopy before ulnar shortening was per-
igure 1. (A) A 3.5-mm 7-hole AO plate is used as a templateor the osteotomy. The step-cut is designed to extend be-ween the third and fifth holes of the plate. (B) After complet-ng the initial cuts the intended length of shortening isarked and cut on both the proximal and distal osteotomy
rms. (C) After reduction a dorsal-to-volar lag screw first islaced to compress the arms of the osteotomy. A volarlylaced 3.5-mm AO neutralization plate is applied next.
ormed in the same setting in 19 of the 29 patients.

Weqout(cl
STppptltTcciflaTH
iuuddctisrlfilmdecItsaor
o
mbaiptbt1staom
tOwclv(papanooTpcpptmri
pttrta
aipaa
Darlis et al / Step-Cut Distal Ulnar–Shortening Osteotomy 945
rist arthroscopy was performed if after clinicalxamination and imaging studies there still wereuestions regarding the diagnosis of ulnar impactionr if other intra-articular pathology was noted. Wesed arthroscopy before ulnar shortening to confirmhe diagnosis or address the intra-articular pathologyunstable triangular fibrocartilage complex flaps,hondral flaps, partial scapholunate or lunotriquetraligament lesions).
urgical Techniquehe procedure may be performed with the arm sus-ended from a traction tower if wrist arthroscopy iserformed before ulnar shortening. Nineteen of therocedures were performed in this position. Alterna-ively the procedure can be performed with the armying on the armboard (with the shoulder abducted,he elbow flexed, and the forearm fully pronated).hrough an 8-cm incision slightly volar to the sub-utaneous border of the distal third of the ulna, ac-ess to the bone is obtained after dissecting thenterval between the extensor carpi ulnaris and theexor carpi ulnaris. The periosteum is elevated onlyt the intended site of the osteotomy for 2 to 3 cm.he ulnar artery and nerve are protected with smalloman retractors.The step-cut osteotomy has its long arm oriented
n the coronal plane parallel to the long axis of thelna. The short arms of the osteotomy are perpendic-lar to the long axis in the axial plane (ie, volar toorsal and dorsal to volar) (Fig. 1A). To facilitateesigning the osteotomy a 7-hole 3.5-mm dynamicompression plate (Synthes, Paoli, PA) is apposed tohe ulna (Fig. 1A). The plate should be placed prox-mal enough that neither the plate nor the distalcrews will impinge into the DRUJ with forearmotation. The osteotomy, approximately 2 cm inength, is designed to extend from the third to thefth holes of the plate, making sure that there is room
eft for bicortical screw placement in these 2 holes. Inost situations a 2- to 4-mm shortening of the ulna is
esired, and use of the 7-hole plate as a templatensures that the arms of the step-cut will have suffi-ient length for lag-screw placement after shortening.f an unusual amount of ulnar shortening is intendedhe osteotomy can be designed between the third andixth holes of an 8-hole plate, thus creating longerrms. The planed osteotomy is outlined on the cortexf the ulna with a marking pen and the plate isemoved from the field.
The long arm of the osteotomy is cut first using an
scillating saw. Care is taken to orient this cut in a pedial-to-lateral (coronal plane) direction and to cutoth cortexes. The 2 short arms are cut next in thexial plane perpendicular to the first cut. Next thentended length of shortening is marked on both theroximal and distal osteotomy arms (Fig. 1B). Notehat the full amount of shortening (not half of it) muste marked on both arms. A close approximation ofhe precise shortening can be achieved by subtracting
mm from the intended shortening to account foraw kerf width and marking that length on the os-eotomy arms. The bone is removed by cutting par-llel to the short arms of the osteotomy. The 2 wafersf bone that are removed then are compared andeasured, with corrections made if necessary.The osteotomy then is reduced. Ulnar deviation of
he wrist facilitates approximation of the bone ends.nce reduction is deemed satisfactory it is securedith a reduction clamp across the osteotomy, with
are taken to leave room for lag screw placement. Aag screw then is drilled and inserted from dorsal toolar perpendicular to the long arm of the osteotomyFig. 1C). Finally the 7-hole dynamic compressionlate is placed on the volar flat surface of the ulnand centered on the osteotomy (the fourth hole of thelate being opposite to the lag screw). Three screwsre inserted on each side of the osteotomy in theeutralization mode. The 2 screws adjacent to thesteotomy are angled slightly away from the osteot-my to avoid insertion through the osteotomy site.he fixation technique can be modified so that com-ression is applied through the plate as well. In thatase the plate is applied first, the osteotomy is com-ressed longitudinally, and then the lag screw com-ressing the long arm of the osteotomy is insertedhrough the plate. We find the latter technique to beore cumbersome. Before closure the tourniquet is
eleased, local bleeding is controlled, and the wounds irrigated.
A short-arm plaster splint is applied and is re-laced with a removable thermoplast splint at theime of suture removal in 2 weeks. Removal of thehermoplast splint is allowed for hygiene and gentleange of motion exercises. Unprotected range of mo-ion is initiated at 6 weeks but weight bearing isvoided until clinical and radiologic union.
The preoperative and postoperative office notesnd radiographs of all patients were reviewed. Typ-cally a pronated grip view was obtained for allatients at 6 weeks and the postoperative ulnar vari-nce was assessed from those radiographs. Themount of shortening was measured by comparing
reoperative and postoperative posteroanterior pro-
notl
Uot
Fusc
946 The Journal of Hand Surgery / Vol. 30A No. 5 September 2005
ated grip view radiographs. Oblique views werebtained to assess the progression of healing becausehe plate obstructs the view to the osteotomy site in
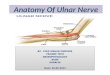
igure 2. (A) Preoperative pronated grip view radiograph of alnar side of the lunate can be observed. Progression of heaame patient: (B) intraoperative, (C) at 6 weeks, and (D) at 10orrection of ulnar variance.
ateral radiographs obtained in a routine fashion. n
nion was defined as blurring of the cortical marginsf osteotomy and trabecular bone bridging the os-eotomy site3 in conjunction with absence of tender-
nt with ulnocarpal impaction. The cystic kissing lesion at thethe step-cut osteotomy on oblique-view radiographs of the
s. (E) Postoperative pronated grip-view radiographs showing
patieling ofweek
ess at the osteotomy site (clinical union). Because

omoTcc
RA(hwgot1awng
mswag
hrp
DWurd
rwceuedttopc
rt
trnteryficws
u�wi
fpceptprrce
R
Darlis et al / Step-Cut Distal Ulnar–Shortening Osteotomy 947
f the osteotomy and fixation techniques used, pri-ary bone healing usually ensued along the long arm
f the osteotomy without visible callus formation.he incidence of union, time to union, and compli-ations and incidence of plate removal were re-orded.
esultsll patients had a follow-up period of at least 1 year
mean, 34 mo; range, 12–48 mo). All osteotomiesealed uneventfully with a mean time to union of 8.3eeks (range, 6–18 wk) (Fig. 2). In 1 patient radio-raphic healing of the proximal short arm of thesteotomy was observed at 18 weeks whereas bothhe long arm and distal short arm appeared healed by0 weeks. No additional measures were taken tochieve union in that case. Union was observedithin 12 weeks in all other patients. No cases ofonunion or delayed union were encountered. Boneraft was not used in any of the patients.The mean postoperative ulnar variance was �0.2m (range, �1 to �1.5 mm) after a mean overall
hortening of 2.5 mm. The mean ulnar shorteningas 2.8 mm (range, 2–5 mm) for the traumatic group
nd 2.4 mm (range, 2–4 mm) for the ulnar-impactionroup.Persistent plate-related symptoms necessitated
ardware removal in 3 patients. The plates wereemoved after a minimum of 16 months after therocedure. No other complications occurred.
iscussione describe a simple and effective technique for
lnar-shortening osteotomy. The step-cut osteotomyesulted in solid union in all patients with no cases ofelayed union or nonunion.Both nonunions and delayed unions have been
eported for ulnar-shortening osteotomies1,3,6,15–17
ith rates up to 15%.15 The transverse osteotomyonfiguration3,15 and smoking18 have been consid-red predisposing factors. Comparison of the time tonion between reports is difficult because of differ-nces in the definition of union. Regardless of theifferences in the definition it seems that ulnar os-eotomy union must be expected within a 5-monthime frame.1,3,5 All of our patients had well-healedsteotomies by that time (even patients using tobaccoroducts) and the mean time to union of 8.3 weeksompares favorably with other reports.
Plate prominence and irritation can be reasons foreoperation because of the subcutaneous position of
he ulna. Hardware removal rates ranging from 25%8o 88%5 have been reported. Fractures after plateemoval also have been reported.7,8 With the tech-ique described in this article, the plate is placed onhe volar surface of the ulna where soft-tissue cov-rage is better. This led to a decreased rate of plateemoval (10% at a minimum follow-up period of 1ear) while maintaining the advantages of rigid platexation. Palmar placement of the plate can be diffi-ult with techniques that use specialized bulky jigshen more extensive periosteal stripping is neces-
ary to apply the jig.Friedman and Palmer19 suggested shortening the
lna to neutral or �1 mm. Shortening of more than2 mm may lead to DRUJ incongruence. Shorteningas accurate in all of our patients in the ulnar-
mpaction group based on these guidelines.The step-cut configuration is an excellent option
or extra-articular ulnar-shortening osteotomies. Itrovides ample bone-to-bone contact area and easyontrol of rotation; no special instrumentation is nec-ssary. Fixation with a 7-hole 3.5-mm dynamic com-ression plate and a lag screw proved to be sufficiento permit early mobilization of the wrist and palmarlacement of the plate minimized the need for plateemoval caused by irritation. This technique accu-ately restored ulnar variance with minimal compli-ations. It facilitates simple and reproducible short-ning without the use of special equipment.
eferences1. Darrow JC Jr, Linscheid RL, Dobyns JH, Mann JM 3rd,
Wood MB, Beckenbaugh RD. Distal ulnar recession fordisorders of the distal radioulnar joint. J Hand Surg 1985;10A:482–491.
2. Boulas HJ, Milek MA. Ulnar shortening for tears of thetriangular fibrocartilaginous complex. J Hand Surg 1990;15A:415–420.
3. Rayhack JM, Gasser SI, Latta LL, Ouellette EA, Milne EL.Precision oblique osteotomy for shortening of the ulna.J Hand Surg 1993;18A:908–918.
4. Labosky DA, Waggy CA. Oblique ulnar shortening osteot-omy by a single saw cut. J Hand Surg 1996;21A:48–59.
5. Wehbé MA, Cautilli DA. Ulnar shortening using the AOsmall distractor. J Hand Surg 1995;20A:959–964.
6. Hulsizer D, Weiss APC, Akelman E. Ulnar-shortening os-teotomy after failed arthroscopic debridement of the trian-gular fibrocartilage complex. J Hand Surg 1997;22A:694–698.
7. Minami A, Kato H. Ulnar shortening for triangular fibrocar-tilage complex tears associated with ulnar positive variance.J Hand Surg 1998;23A:904–908.
8. Mizuseki T, Tsuge K, Ikuta Y. Precise ulnar-shorteningosteotomy with a new device. J Hand Surg 2001;26A:931–939.
9. Chen NC, Wolfe SW. Ulna shortening osteotomy using a
compression device. J Hand Surg 2003;28A:88–93.
1
1
1
1
1
1
1
1
1
1
948 The Journal of Hand Surgery / Vol. 30A No. 5 September 2005
0. Horn PC. The long ulnar sliding osteotomy. J Hand Surg2004;29A:871–876.
1. Chennagiri R, Burge P. Pre-osteotomy plate applicationtechnique for ulnar shortening. J Hand Surg 2004;29B:453–457.
2. Khan MI. Comments inspired by two letters on ulnar short-ening osteotomy for ulnar impaction syndrome. J Hand Surg1994;19A:871–872.
3. Bowers WH. The distal radioulnar joint. In: Green DP, Hotch-kiss RN, Pederson WC, eds. Green’s operative hand surgery.4th ed. Philadelphia: Churchill Livingstone, 1999:1017.
4. Tomaino MM. The importance of the pronated grip x-rayview in evaluating ulnar variance. J Hand Surg 2000;25A:
352–357.5. Köppel M, Hargreaves IC, Herbert TJ. Ulnar shorteningosteotomy for ulnar carpal instability and ulnar carpal im-paction. J Hand Surg 1997;22B:451–456.
6. Loh YC, Van Den Abbeele K, Stanley JK, Trail IA. Theresults of ulnar shortening for ulnar impaction syndrome.J Hand Surg 1999;24B:316–320.
7. Scheker LR, Severo A. Ulnar shortening for the treatment ofearly post-traumatic osteoarthritis at the distal radioulnarjoint. J Hand Surg 2001;26B:41–44.
8. Chen F, Osterman AL, Mahony K. Smoking and bony unionafter ulnar-shortening osteotomy. Am J Orthop 2001;30:486–489.
9. Friedman SL, Palmer AK. The ulnar impaction syndrome.
Hand Clin 1991;7:295–310.