Embed Size (px)
DESCRIPTION
Evaluation of the effect of Bruhatpanchamooladi Yoga in Medoroga By VEENA S. JIGALUR, Department of Kayachikitsa, Post graduate studies and research center D.G. MELMALAGI AYURVEDIC MEDICAL COLLEGE, Gadag - 582 103
Citation preview
“Evaluation of the effect of
Bruhatpanchamooladi Yoga in Medoroga”
By
VEENA S. JIGALUR
Dissertation submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore
In partial fulfillment of the degree of
Ayurveda Vachaspati M.D. In
Kayachikitsa Under the Guidance of
Dr. Shiva Rama Prasad Kethamakka M.D. (Ayu) (Osm), C.O.P. (German) M.A., [Ph.D] (Jyotish)
Department of Kayachikitsa Post Graduate Studies & Research Center D.G. MELMALAGI AYURVEDIC MEDICAL COLLEGE, GADAG
2006-2009
D.G.M.AYURVEDIC MEDICAL COLLEGE
POST GRADUATE STUDIES AND RESEARCH CENTER GADAG, 582 103
This is to certify that the dissertation “Evaluation of the effect of
Bruhatpanchamooladi Yoga in Medoroga” is a bonafide research work done by
Veena. S. Jigalur in partial fulfillment of the requirement for the post graduation degree of
“Ayurveda Vachaspati M.D. (Kayachikitsa)” Under Rajeev Gandhi University of Health
Sciences, Bangalore, Karnataka.
Guide
Prof. Dr. Shiva Rama Prasad Kethamakka
M.D. (Ayu) (Osm), C.O.P (German), M.A., [Ph.D] (Jyotish)
Professor in Kayachikitsa
DGMAMC, PGS&RC, Gadag
Date:
Place:
J.S.V.V. SAMSTHE’S
D.G.M.AYURVEDIC MEDICAL COLLEGE
POST GRADUATE STUDIES AND RESEARCH CENTER GADAG, 582 103
Endorsement by the H.O.D, principal/ head of the institution This is to certify that the dissertation entitled “Evaluation of the effect of
Bruhatpanchamooladi Yoga in Medoroga” is a bonafide research work done by
Veena. S. Jigalur under the guidance of Prof. Dr. Shiva Rama Prasad Kethamakka,
M.D. (Ayu) (Osm), C.O.P (German), M.A., [Ph.D] (Jyotish), Professor in Kayachikitsa in partial
fulfillment of the requirement for the post graduation degree of “Ayurveda Vachaspati M.D.
(Kayachikitsa)” Under Rajeev Gandhi University of Health Sciences, Bangalore,
Karnataka.
.
(Dr. G. B. Patil) Principal,
DGM Ayurvedic Medical College, Gadag
Date: Place:
Professor & HOD Dept. of Kayachikitsa
PGS&RC Date: Place: Gadag
Declaration by the candidate
I here by declare that this dissertation / thesis entitled “Evaluation of the effect of
Bruhatpanchamooladi Yoga in Medoroga” is a bonafide and genuine research work
carried out by me under the guidance of Prof. Dr. Shiva Rama Prasad Kethamakka,
M.D. (Ayu) (Osm) M.A. (Jyotish), [Ph.D (Jyotish)], Professor in Kayachikitsa, DGMAMC,
PGS&RC, Gadag.
Date
Place
Veena S Jigalur
Copy right
Declaration by the candidate
I here by declare that the Rajiv Gandhi University of Health Sciences, Karnataka
shall have the rights to preserve, use and disseminate this dissertation/ thesis in print or
electronic format for the academic / research purpose.
Date
Place
Veena S Jigalur
© Rajiv Gandhi University of Health Sciences, Karnataka
Acknowledgement
First and foremost, I salute almighty God who is omnipresent, omniscient and
omnipotent. He is the possessor of the ocean of knowledge and wisdom-to which I would
like to contribute a drop in the form of my dissertation. As it is said, each and every drop
goes to make an ocean; this is my humble endeavor towards its goal of wisdom. It gives
me in expressible pleasure to offer my sincere thanks to all who have rendered their
wholehearted support, guidance and co-operation in completing the thesis work.
I am extremely happy to express my deepest sense of gratitude to my beloved and
respected guide Prof. Dr. K. Shiva Rama Prasad, M.D., C.O.P. (German), M.A., [Ph.D.]
(Jyotish), Department of Kayachikitsa (PG), for his guidance and timely help.
I am sincerely gratefulness to Dr.G.B.Patil, Principal, for his encouragement and
providing all necessary facilities for this research work.
I extend my gratitude to Dr. R.V.Shettar, Dr.Mulki Patil, Dr. Shankaragouda,
Dr.V.Varadacharlu, Dr.P.Shivaramudu, Dr.G.Purushottamacharyulu, Dr.M.C.Patil, Dr.
G.Danappagoudar, Dr.S.N.Belawadi, Dr.Nedugundi, Dr.Samudri, Dr,Kuber sankh.
Dr.Mulgund, Dr.J.Mitti, Dr.Yasmin A.P. and all my U.G. Lecturers for time-to-time help
offered by them.
I express my immense gratitude to my statistician Nandakumar, librarian V.B.
Mundinamani and assistant Shavi & Kerur for facilitating me in collection and
production of my thesis.
I would like to thank my family members who have given love and care during
my studies. My deep sense of gratification is due for my Father Dr.S.B.Jigalur and my
mother Smt.Bhagirathi S. Jigalur who are the architects of my career. The culture,
discipline and perseverance, which I could imbibe, are solely because of their
painstaking, upbringing and strong moral support. I express my deep gratitude to
Dr.Gachinmani N.G. for inspiring me to higher studies, and helped me in each and every
step of this course with his valuable suggestions.
I express my heartfelt gratitude to my brother, Mr.Vivek Jigalur and my Sister
Smt.Vidya Modi for constant help and encouragement to move ahead. My deepest
gratitude to my husband for enormous love and moral support.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA - ACKNOWLEDGEMENT
I feel proud in expressing my gratitude to final year UGS who helped me in
carrying trial work.
I take this moment to express my thanks to all my Post gratude colleagues, Dr.
Ashok M.G., Dr.Kamalaxi, Dr.Sulochana, Dr.Shivaleela Kalyani, Dr.Prasann Joshi, Dr.
Sanjeev Choudhari, Dr.Neeraj kumar, Dr. Vijayalakshmi B, Dr. Anupama Bijjal,
Dr.Trupti Itagi, Dr.Ishwar Patil, Dr.Bodke, Dr.Kanthi, Dr.Praveen, Dr.Deepa T, Dr.Asha
M.
Finally I am thankful to all those who helped directly or indirectly for the
completion of this work.
(Veena S Jigalur.)
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA - ACKNOWLEDGEMENT
Contents of “Evaluation of the effect of Bruhatpanchamuladi Yoga
in Medoroga” By
Veena S. Jigalur
CHAPTER
CONTENTS
PAGES
1 Introduction
1 -3
2 Objectives
4 -5
3 Review of literature
6 - 78
4 Methods
79 - 87
5 Results
88 - 101
6 Discussion
102 - 113
7 Conclusion
114- 115
8 Summary
116- 117
9 Bibliographic References
1 to 9
10 Annex – data of clinical trial
1 to 12
11 Annex – Case sheet
1 to 6
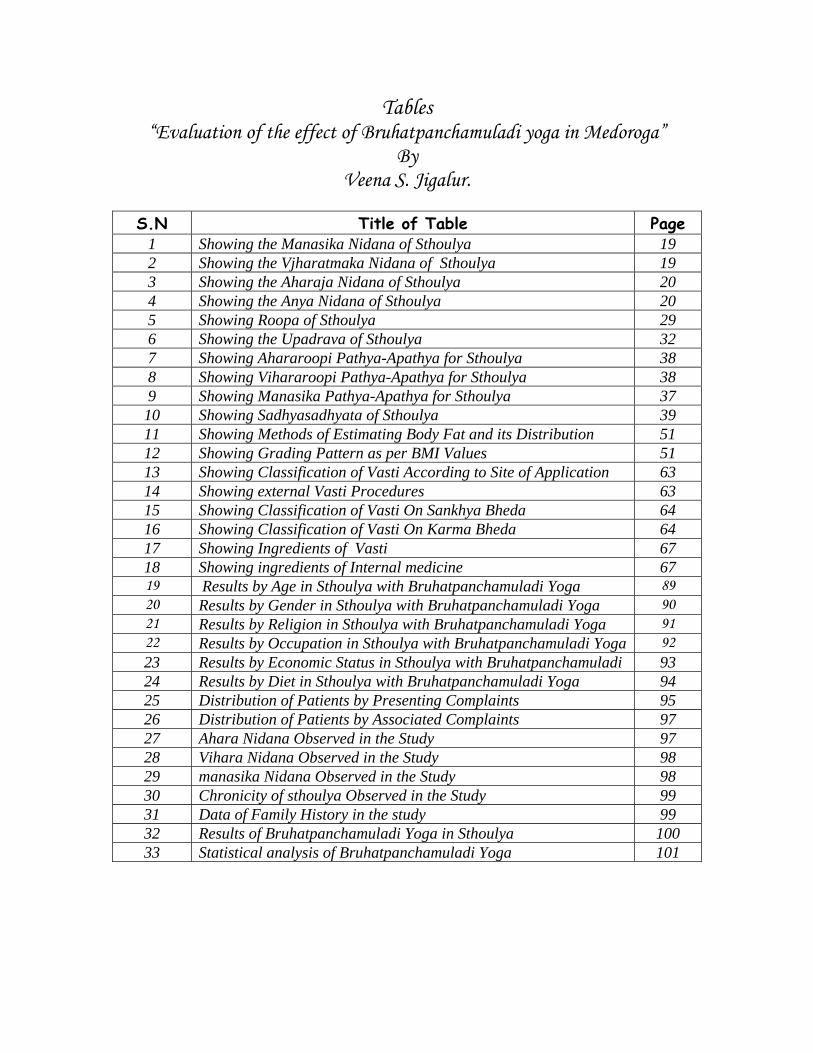
Tables “Evaluation of the effect of Bruhatpanchamuladi yoga in Medoroga”
By Veena S. Jigalur.
S.N Title of Table Page
1 Showing the Manasika Nidana of Sthoulya 19 2 Showing the Vjharatmaka Nidana of Sthoulya 19 3 Showing the Aharaja Nidana of Sthoulya 20 4 Showing the Anya Nidana of Sthoulya 20 5 Showing Roopa of Sthoulya 29 6 Showing the Upadrava of Sthoulya 32 7 Showing Ahararoopi Pathya-Apathya for Sthoulya 38 8 Showing Vihararoopi Pathya-Apathya for Sthoulya 38 9 Showing Manasika Pathya-Apathya for Sthoulya 37 10 Showing Sadhyasadhyata of Sthoulya 39 11 Showing Methods of Estimating Body Fat and its Distribution 51 12 Showing Grading Pattern as per BMI Values 51 13 Showing Classification of Vasti According to Site of Application 63 14 Showing external Vasti Procedures 63 15 Showing Classification of Vasti On Sankhya Bheda 64 16 Showing Classification of Vasti On Karma Bheda 64 17 Showing Ingredients of Vasti 67 18 Showing ingredients of Internal medicine 67 19 Results by Age in Sthoulya with Bruhatpanchamuladi Yoga 89 20 Results by Gender in Sthoulya with Bruhatpanchamuladi Yoga 90 21 Results by Religion in Sthoulya with Bruhatpanchamuladi Yoga 91 22 Results by Occupation in Sthoulya with Bruhatpanchamuladi Yoga 92 23 Results by Economic Status in Sthoulya with Bruhatpanchamuladi 93 24 Results by Diet in Sthoulya with Bruhatpanchamuladi Yoga 94 25 Distribution of Patients by Presenting Complaints 95 26 Distribution of Patients by Associated Complaints 97 27 Ahara Nidana Observed in the Study 97 28 Vihara Nidana Observed in the Study 98 29 manasika Nidana Observed in the Study 98 30 Chronicity of sthoulya Observed in the Study 99 31 Data of Family History in the study 99 32 Results of Bruhatpanchamuladi Yoga in Sthoulya 100 33 Statistical analysis of Bruhatpanchamuladi Yoga 101
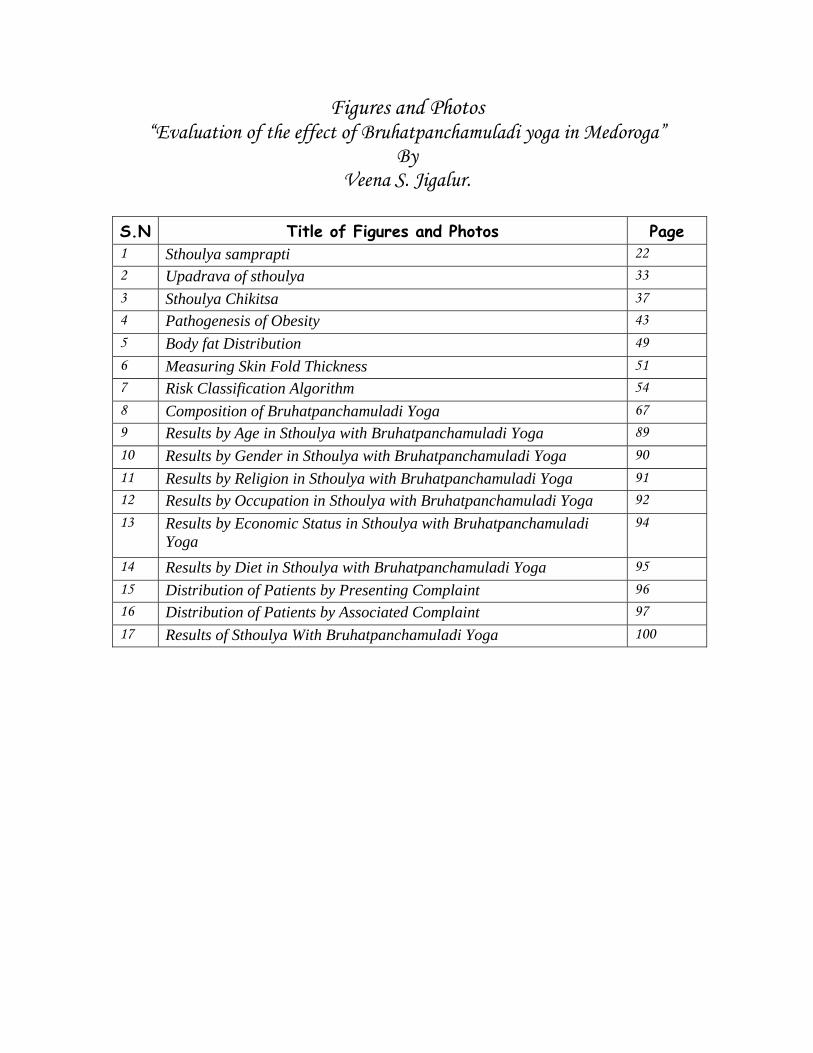
Figures and Photos “Evaluation of the effect of Bruhatpanchamuladi yoga in Medoroga”
By Veena S. Jigalur.
S.N Title of Figures and Photos Page 1 Sthoulya samprapti 22 2 Upadrava of sthoulya 33 3 Sthoulya Chikitsa 37 4 Pathogenesis of Obesity 43 5 Body fat Distribution 49 6 Measuring Skin Fold Thickness 51 7 Risk Classification Algorithm 54 8 Composition of Bruhatpanchamuladi Yoga 67 9 Results by Age in Sthoulya with Bruhatpanchamuladi Yoga 89 10 Results by Gender in Sthoulya with Bruhatpanchamuladi Yoga 90 11 Results by Religion in Sthoulya with Bruhatpanchamuladi Yoga 91 12 Results by Occupation in Sthoulya with Bruhatpanchamuladi Yoga 92 13 Results by Economic Status in Sthoulya with Bruhatpanchamuladi
Yoga 94
14 Results by Diet in Sthoulya with Bruhatpanchamuladi Yoga 95 15 Distribution of Patients by Presenting Complaint 96 16 Distribution of Patients by Associated Complaint 97 17 Results of Sthoulya With Bruhatpanchamuladi Yoga 100

Abstract of “Evaluation of the effect of Bruhatpanchamuladi Yoga in Medoroga” Key words: Sthoulya, Chala udara, Bahudoshja vyadhi, Sedentary lifestyle, Waist hip
ratio, Phenotype obesity, Bruhatpanchamuladi yoga
A recent world health study reports that obesity is included among the top ten
selected risks to health. Sedentary lifestyle and inclusion of increased intake of oily and
fatty foods in the daily diet result in this disorder. 75% Indian women in the cities are
apple-shaped, while 58% men are so. As Charka’s explanation of sthoulya matches with
phenotype of obesity, W.H.Ratio and skin fold thickness can be taken as parameters to
assess the sthoulya, as W.H.Ratio helps to check the abdominal fat (Chala udara) and
gluteal fat (chala sphik) & Skin fold thickness helps to measure regional fat (chala sthana).
Charaka has described sthoulya under 8 undesirable constitutions based on their
ugly/awkward appearance, victims of public abuse, unmanageable health condition.
Sthoulya is one among kapha predominant diseases (sleshma nanatmaja) involving kapha
and medas as main dosha and dushya in the pathogenesis. Charaka clearly mentioned that
sthoulya and prameha have a direct relation because both have kledaka kapha and medas
dominance in their pathogenesis. It is also prescribed that sthoulya is a bahudoshaja vyadhi
which further proves that it is the root cause of many killer diseases like diabetes, HTN,
and heart diseases.
Bruhatpanchamuladi yoga ingredients are kapha and medohara dravyas collected
form local area and prepared under GMP conditions, weighing about 500mg tablet form.
Patients of Sthoulya fulfilling the criteria of diagnosis were selected in the present study.
The female and male ratio in the study is approximately 3:2 patients and 76% patients were
recorded with sedentary life styles. In the present study 53.3% patients had family history.
Apart from the symptoms which show high significance in the study the key parameters to
assess “sthoulya”, W.H.Ratio has shown highly significance than any other with 8.04 % of
mean reduction, and Chala Udara with 68.25% of mean reduction. This is strong evidence
to state that the Bruhatpanchamuladi yoga is good combination of Ayurveda in reducing
Sthoulya / obesity.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA - ABSTRACT
Chapter -1
Introduction
“You are not good enough, is the message family and society send to Overweight
and Obese people especially to women”. It’s nearly 60 years since a poet Simone de
Beauvoir famously wrote, one is not born a woman but becomes one. Many of Obese
lives are bedeviled by the three-letter word, ‘FAT’ along with “social anxiety, loss of
self-esteem, isolation and vulnerability in social and private lives”.
In the present days the man has to run with the time and he is trying to lead
mechanical life. Though he knows the ill effects of such mechanical life, he made himself
victim to it by suffering with many disorders, among these sthoulya is a global problem
and more common in modernized man and in present era.
This sthoulya is considered as Santarpanajanya vyadhi and one among the Ashta
nidhita purushas and also as Kaphaja nanatmaja vyadhi. The obesity is the certainly the
mother of dangerous diseases1 and most burning problem in the present society. Obesity
has become an epidemic in 21st century2. It is a bitter truth to swallow about every 4th
person on earth is too fat. Weighty women get six times more diseases3. Obesity is fast
becoming one of the worlds leading reason why the people die4.
The ancient Indian science of health, Ayurveda is now being increasingly accepted
by the world at large for its facilities and adoptability even to the modern times. It is not
surprising that, the ancient science is accorded such importance in countries where
modern medicine itself has made immense advances. The only reasonable explanation
for this phenomenon is the fact that Ayurveda remains the only system of medicine that
possesses a natural form of treatment, one that prescribes remedies in accordance with
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-INTRODUCTION
1
nature itself. It approaches a patient holistically, taking in to account while treating
person, not only the patient but also his general condition.
Prevalence:
According to WHO this obesity is considered as secondary in the list of dangerous
diseases in the world5 many remedies have been put forwarded till now like surgical
lipisection, treatments etc. but there are so many complications observed with those. Due
to lack of knowledge about the diet & rules for taking the food this is greatly observed in
the developed countries like USA that showing approx one in six or 39.8 million people
and over 300 million adults worldwide (WHO world health report, 2003) were suffering
from obesity6. 75% Indian women in the cities are apple shaped, while 58% of men are
so7. They are searching for the solutions either by dietary things as well as keeping stress
on need of exercise. So by observing these facts & statistics prevalence of over weight
and obesity in India it is badly in need of a better remedy.
Previous research literatures:
1) Clinical trial on obesity with lekhanvasti, Yoga and diet control. 2004 .AKDA,
Amravati university Maharashtra.
2) Evaluation of efficacy of tryushanadhya loham in sthoulya w.s.r. to
Hyperlipidaemia. 2004. Gadag Karnataka.
3) Effect of Guduchyadi yoga in Sthoulya. 2005, Pune.
4) Evaluation of Efficacy of Bhadradi Asthapana Vasti in Sthoulya 2007 Gadag,
Karnataka.
Research question:
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-INTRODUCTION
2
The transformation of India into an affluent nation has brought changes in life
style, and junk food diet that have led to an increase in Obesity8. Accumulated wealth and
lower physical activity in the setting of deskwhite color jobs with more mental activity
has created a population who has a net increase in available energy stored as fat9,10. and
to set a disease called as Obesity.
Many research works have been carried out in relation to shamana treatment as
mentioned in classics and their therapeutic values are proved. Present research work is
intended to evaluate the effect of herbal combinations used as different line of treatments
( Block box clinical trial). So looking for a better management needed.
About concept:
As Sthoulya being a morbid disease only Shamana can not give a better remedy,
hence treatment can be better done if it is done after deha shodhana11, as shodhana
prevents the relapse of the condition. If treatment is given without shareera shudhi it is
almost like colouring a dirty cloth12. Hence here an attempt is made to treat Sthoulya with
shodhana then with shamanoushadhi.
In this study the selected drug Brihatpanchamoola are having laghu, rooksha
guna, kashaya, tikta rasa, katu vipaka and ushna veerya. Due to these properties it acts as
vatakaphahara and relives the medavrutavata.
The study description:
The study description consists of the headings according to the RGUHS protocol
followed from 2nd chapter.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-INTRODUCTION
3
Chapter -2
Objectives
Ayurvedic science, a boon in today’s world, describes swastha parayanata,
which means maintenance of health in the one hand and treatment of disease on the other.
It has been described in Ayurveda that it is not rational treatment where the medicine
modifies one disease; on the other hand it provokes new complications. So here, we are
putting our step forward to find safe and effective remedy for weight reduction.
Thirty years ago13 overweight and obesity was defined as a nutritional disorder but
it continues to be one of the most important yet preventable health hazards. The
transformation of India in to an affluent nation has brought changes in lifestyle, and junk
food diet that have led to an increase in Obesity14 Accumulated wealth and lower
physical activity in the setting ‘desk’ white collar jobs with more mental activity has
created a population who has a net increase in available energy stored as fat15&16 and to
set a disease called as obesity.
Obesity i.e. sthoulya is a chronic disease that is increasing in prevalence and poses
a serious risk for the development of many metabolic diseases such as diabetes mellitus,
hypertension, heart diseases etc. To prevent such diseases it is very much required to
attend the problem which is told as Sthoulya\ medoroga in Ayurveda.
Till today many research works were taken up on the basis of Medohar and
Kaphahara therapy. The present study intended to focus on the disease evaluation i.e.
Sthoulya and the management with Bruhatpanchamuladi yoga as a shamana as well as
shodhana chikitsa. In this regard the objectives proposed in the study are -
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-OBJECTIVES
4
Objectives:
1) Evaluation of the effect of Bruhatpanchamuladi yoga in medoroga w.s.r.t. weight.
2) Evaluation of the effect of Bruhatpanchamuladi yoga in medoroga w.s.r.t. B.M.I.
3) Evaluation of the effect of Bruhatpanchamuladi yoga in medoroga
w.s.r.t. Waist Hip Ratio.
The drugs which come under Brihatpanchamula (Bilwa, Agnimantha,
Shyonaka, Gambhari and Patala) are having laghu and ruksha guna, kashaya and tikta
rasa, katu vipaka, ushna veerya. Due to these properties it acts as vata kaphahara and at
the same time relieves the Medavruta vata inturn does samprapti vighatana, hence helps
to overcome Sthulata in terms of weight, B.M.I. and W.H.Ratio.
In Indian population we observe many people with relatively lower B.M.I. but
with higher W.H.Ratio. It indicates presence of phenotype of obesity in Indians which is
exactly explained as lakshanas of Sthoulya by Charaka as spik, udara, sthana chalatwa. In
this study we have an aim to study the effect of the drug in Indian population by
observing effect on W.H.Ratio.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-OBJECTIVES
5
Chapter -3
Review of literature
Medoroga – Sthoulya.
Sthoulya and Medoroga are the two words used to describe the obese person in
Ayurvedic literature. There are two different views one supporting the thought that the
Sthoulya and Medoroga are one and same, and others opine that they are different
entities.
Supporting view for sthoulya as equivalent to medoroga:
1) Chakrapani in his book Chakradutta has fallowed the sequence adopted by
Madhvakara in Madhava Nidana for description of various Diseases. But Chakrapani had
described Sthoulya under the heading of Sthoulya chikitsa17. Where as in Madhavanidana
this is described under Medoroga described by Madhava18, treatment is advised by
Chakrapani under Sthoulya Chikitsa.
2) Charaka had used the terms like Medasvi, Medovruddhi in context of Sthoulya to
describe a Sthula person19.
3) Sharangadhara has specified Medoroga is of only one type20. Adhamalla comments
and made clear that medoroga is one in which Medomamsa ativrudhi is seen i.e.,
Sthoulya21.
Supporting view for sthoulya and medoroga as different entities:
One who differs with the above opinion gives the reason as, Medoroga is enlisted
among “Vamana arha Vyadhi” by Sushruta22 and by Vagbhata Sthoulya is
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
6
enlisted under “Vamana anarha Vyadhi”23 by the authors. But acharya Vagbhata
himself opines to adopt Samshodhana roopi, Langhana in case of Atisthoulya24.
So the indication and contra-indication is general guidelines. It is up to the
physician to decide the proper line of treatment depending upon various factors
like Dosha, Dushya, Vyadhi, Bala etc. However by analyzing, one can speculate the
Sthoulya and Medoroga suggest the different stages of same disease process.
1) Medovrudhi is Pathogenesis
2) Medoroga and Medodosha are the Pathophysiology
3) Sthoulya is the resultant Diseases
Depending upon Nidana, Lakshana, Upadrava and Chikitsa one can say that
Sthoulya is nothing but Obesity told by cotemporary system.
PHYSIOLOGICAL CONSIDERATION OF MEDODHATU Sthoulya being a Dooshya dominant disorder, in that, Meda plays a major role in
pathogenesis. Meda is one among the saptha dhatu.
Nirukti: Literally the word meda is derived from the root,
This means “Jhimida snehane” stands for sneha, fat, oil etc25
Definition: This produces smoothness in the body
Synonyms of Meda: Vapa, Vasa, Mamsa Sara, Mamsa sneha, Mamsasara bhuta dhatu,
Asthikrit(as it forms asthi), Majja(Asthi majjagata sneha), Gada(mastishkagata sneha)
etc.
Sthana and Swarupa of Meda dhatu: There are 2 types of Medadhatu. One is
Poshaka and second is Poshya. Among these two, poshaka meda dhatu is gatiyukta,
this is circulated, in the whole body along the Rasa – Rakta dhatu, to give the nutrition
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
7

to poshya meda dhatu. Second poshya meda dhatu is Gativivarjita, which is stored in
Medodharakala. The site of medodharakala is Udara and Anuasthi, Udara, Sphik, Sthana,
Gala are also depots of poshya meda. It is also found in mamsa as Vasa26.
Utpatti of meda dhatu: According to Caraka, when rakta dhatu gets solidified in the
presence of vayu, jala & agni mahabhuta and digested by raktagni, it forms mamsa dhatu.
This mamsa dhatu being digested by mamsa dhatvagni and mixed with its own agni and
jala property, transformed into meda dhatu27.
Pramana of Meda dhatu: Two anjali is said to be the quantity of Meda dhatu28.
Meda Dhatu Mala: Sweda is the mala of Meda dhatu29.
Meda Dhatu Upadhatu: Snayu and sandhis are the upadhatu of Medas30.
Medavaha srotas: The internal transportation system of the body is represented as srotas.
Medovaha srotas are the channels that transport poshaka meda dhatu to the seat of poshya
or sthayi meda dhatu
Moola of Medovaha Srotas: According to Ayurvedic classics every srotas has its
definite roots or place of origin, same in case of Medovaha srotas. Different ancient
Acharyas have drawn their opinions regarding root or moola of meda vaha srotas as
follows,
Charaka - Vrikka, Vapavahana31
Sushrut - Vrikka, Kati32
Vagbhata -Vrikka, mamsa (Vasa)
Sushruta and Vagbhata quotes anatomical preference than the physiological point
of view in considering kati and mamsa as mula of medovaha srotas. Where as Charaka’s
consideration of Vapavahana was physiological one.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
8
Medodhara Kala: It is the third Kala, present in Udara and Sukshma Asthi33.
Ashrayashrayeebhava of Meda: Kapha resides in Meda and Kapha is Ashrayee and
Meda is Ashraya34.
Karma of Meda dhatu: 35
• Sneha: Sneha property helps to keep luster of skin, hairs and eyes etc.
• Sweda: During the stage of Meda dhatvagnipaka, sweda is produced as kitta
bhaga36. Sharangadhar has considered sweda as the upadhatu of meda.
• Drudhata: According to Caraka snayu and sandhis are upadhatus of Meda37
which gives strength to the body
• Asthipusthi: Nourishment of further dhatu i.e. asthi and its upadhatu is Snayu and
Sandhi38.
• Further Vagbhata has mentioned, Netra and gatrasnigdhata are the symptoms of
sthoulya may arise through increased Snehana function of Meda39.
Meda Dhatu Vridhi Lakshana: Snigdhata of Shareera, vrudhi of Udara and parshwa,
kasa, swasa, hikka, dourgandha of shareera are seen as Meda vrudhi lakshana. It is also
mentioned that these persons will have Shrama and increase in size of Sphik, sthana and
Udara40.
NIRUKTI &VYUTPATTI
Vyutpatti: The word Sthoulya is derived from root “Sthu” with suffix “Ach” which
stands probably for thick or solid or strong or big or bulky41.
• Shtulasya bhavam Sthoulyam – vachaspathyam (6/358)
• Sthulayathi te cha athaha Sthoulyam - vachaspathyam (6/358)
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
9
• Sthula paribhrane - Amarakosha (Nanartha varga 204)
Nirukti: According to Sabdakalpadruma the existence of Sthoolatva (bulkiness) is
known as Sthoulya42.
Paribhasha: A person having pendulous appearance of sphik, udara, and sthana due to
excess deposition of meda along with mamsa dhatu and also having unequal an abnormal
distribution of meda with reduced zeal towards life is called Atisthula43.
Paryaya: Pinam, Pivara, Pivaram, Sthoola, Pina, Piva, Pivam, Pivasa, Pivasa, Pivistha,
Medana, Medini, Medasvina44.
HISTORICAL ELUCIDATION
Vedic and Purana kala
Sthoulya is not a new concept. It can be traced to Vedic and Purana kala as well.
The first person to be described as Lambodara, Mahakaya etc. is lord Ganesha.
According to Sanatana Dharma Shastra lord Ganesh is considered to be the lord
of Jala Mahabuta.
The lakshanas ascribed to Vinayaka are of Sthouly. Lord Ganesh is also named
modaka priya. Modaka is a sweet dish prepared of red gram flour, ghee and sugar,
possessing the properties of Madhura, Guru and Snigdha. These factors are likely to
cause Sthoulya.
The offerings of leaves made to the Lord are also specific and are 21 in
number. Durva, Bilwa, Karaveera, Arka , Kanchanara, Badar, Devadaru, Dhatura, Jati,
Shami, Nirgundi, Dronapushpi, Dhataki, Kapitta, Shigru, Apamarga, Ashwatta,
Machipatra, Brihati, Vishnukranta, Dadimapatra. All these are Kapha, Kandu, Kushta,
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
10
Twagroganashakas, Pramehahara and some are Medohara, few are Atisaraharas. These
are described as the Upadravas of Sthoulya roga.
The later references of Sthoulya can be traced to the Rakshasa or Nishachara
who have been mentioned at the Deva-Danava struggle for Amritha at the sandhikala of
Satayuga and Tretayuga, later in the Ramayanakala and Dwaparayuga . The life style of
Asuras in almost all periods is similarly described. As nitya Mamsahara sevana,
Madhyapana, Atinidra etc.. are all the Nidana for Sthoulya. This sect in itself is Sthoola,
the Sthoolatva in Asuras is hereditary and natural which can be attributed to the beeja
swabhava they are the Nindita as out cast of the community just as Charaka has described
Atisthoola as nindita purusha.
BRUHATRAYI
Charaka samhita(Before 1000 BC)
Incidence of disease may be high during that period; hence they were able to
study the disease clinically. Charaka has considered sthoola as one of the Asta Nindita
Purusha. He explains about stholya and its management in detail noting this as a grave
problem45.
Sushruta samhita(1000-1500 BC)
Increased incidences might have forced them to find the root cause. So
Sushruta clearly quotes rasa is the cause for both sthoulya and krushata46.
Astanga Hridaya(550C AD)
Vagbhata discussed sthoulya in Dwividopakramaneeya chapter and included it
under ‘langhana’ therapy. Classification of Sthoulya and its management. Pathogenesis
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
11
and symptoms of Sthoulya are highlighted. Treatment aspect of sthoulya is discussed
vivid but further states that there is no specific medicine for Sthoulya47.
LAGHUTRAYI
Madhava nidana (9C AD)
He is the first author to describe this disease under separate heading called “Medo
Roga” in 34th chapter. He has mentioned Nidana, Lakshana and Samprapthi of this
disease. Madhavakara renamed Sthoulya as medoroga and compiled the disease from the
previous authors. But change of nomenclature indicates instead of considering anatomical
change i.e. shareera sthulata he wanted to consider physiological change in the
condition48.
Sharangadhara Samhita(13C AD)
This textbook is known for its many unique things like Nadi pareeksha, clear
definition of pharmacological terms etc. He mentions about Sthoulya in rogaganana
adhyaya, but has no details of it except about the management of medodosha as
yogatraya49,50.
Bhava Prakasha(16C AD)
Author has stressed more on the treatment aspects compared to
Brihatrayi.Acharya Bhava mishra has explained regarding a popular Dhupa called
“Malayanila Dhupa” in 39th chapter of Chikitsa sthana. He has also explained regarding
various Lepa and Udvartana to treat sthoulya. This author has explained sthoulya in
separate chapter51.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
12
OTHER CLASSICAL TEXTS
Kashyapa Samhita:
As this book gives more importance for “Koumarabruthya” and “Prasuthi tantra”,
hence Acharya Kashyapa has described “Medasvi Dhatri Chikitsa”. Another specialty of
this text is that Rakta mokshana(SIRAVYADHA) is explained as Chikitsa for Sthoulya52.
Bhela Samhita: It is one of the popular texts of Ayurveda. In 11th Chapter of sutrasthana, various
aspects of Sthoulya have been explained. In Bhela samhita Sthoulya is described as a
disorder of vitiated Meda 53.
Yogaratnakara:
Sthoulya is explained under a separate chapter. Many of the formulations to treat
Sthoola are explained. Explains Sthoulya under Medoroga nidanachikitsa adhyaya.
Various herbo-mineral preparations been prescribed in the management of Sthoulya54.
Chakradatta:
Acharya Chakrapani datta has explained treatment of Sthoulya in 36th chapter55.
Bhaishajyaratnavali:
It is famous for various treatment and preparations of medicines. In 39th chapter
Sthoulya Chikitsa is explained56.
Gada Nigraha:
In 31st chapter, Sthoulya Roga and its Chikitsa is explained57.
SANGRAHAKALA & COMMENTATORS
Chakrapani (11th Century):
In line of treatment of Sthoulya he has commented that guru and Apatarpana
property helps to alleviate Kshudha and reduce Meda respectively58.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
13
Dalhana (12th Century):
Explains regarding Ama formation in tikshnagni, Regarding line of treatment he
has interpreted virukshana as medoghna and chedaniya as sroto vishodhana.59
Indu (13th Century):
He has given explanation of Saktu, Loha etc. words used in the line treatment of
Sthoulya.60
Arunadutta (13th Century):
The word “sthavima” has been used for the sthoulya, explained on the basis of
etymology in sarvanga sundari commentary in Astanga Hridaya.61
Hemadri (13th Century):
He has advised to take choorna of Yavani, Madukajalam as Madhu mishrita
udaka Dandahata as Takra, Agnimantha as Tarkari, Kshara as Yavakshara, while
management of Sthoulya in his Ayurveda Rasayana commentary on Astanga Hridaya.62
Adhamalla(14thcentury) & Kashiram(17thcentury):
Kashiram explained definition of Sarakthameda is the one which is situated inner
to the majja of the sthulasthi.63 Medo dosha is of only one type and it is of vata pradhana
is explained in Adhamalla gudartha deepika.64
Vangasena (12thcentury):
Explains Karana, Samprapti, laxana, Chikista of Sthoulya in Medorogadhikara.65
Nidana The low of nature states that without cause effect is not possible. As per the
sequence of Pathogenesis of disease given by Madhavakara, Nidana is the first and
foremost step for the manifestation of the disease and it gives the particular knowledge
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
14
about the Pathogenesis of the disease, hence etiological factors provides vital information
regarding diagnosis as well as involved pathological entities of a disease. More
importantly, most of the times guide the physician towards therapeutics & aid in advising
pathyapathya. In the context of Sthoulya causes may be of two types,
1. Exogenous causes are potentiating diet and regimen
2. Endogenous causes are dosha, dhatu, mala, srotas etc.
• Acharya Charaka has mentioned the nidana of Sthoulya analytically 66.
Most of them are of exogenous type. Charaka has also defined Beejadosha as one of the
cause besides the other.
• Acharya Sushruta and Vagbhsta have made mention of the endogenous type.
By telling that rasa is the prime cause for the sthoulya67.
• Vagbhata has also mentioned ama as a causative factor68.
Further all the causative factors described in the Ayurvedic classics can be classified into
four groups.
1) Aharathamaka nidana
2) Viharathamaka nidana
3) Manasika nidana
4) Beeja swabhavaja nidana
Aharaja nidana: On the basis of the samanya and vishesha sidhanta69 the excessive consumption of
similar substance(dravya samanys), similar quality(guna samanya) or similar in action
(karma samanya) help in the overproduction of dhatu. When one or two or all the three
properties are similar, then such substances boost up the growth of the dhatus which
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
15
result as dhatuvrudhi. In the same way, the growth of medodhatu is observed by
excessive consumption of:
Dravyasamanya: Mamsa and meda (animal and plant fats) Gunasamanya: Food with snigdha,guru guna like - ghrita, vasa, taila, dugdha etc. Food and drugs with sheetaveerya Substance with madhura rasa and vipaka. Karmasamanya: Sedentary life, avyayama, diwaswapna etc. Aharaja nidana are wide spectrum of etiological factors, which is having variation
in Ahara krama at one end, and Rasadi factors at another end. The following are the
Aharaja Hetu70:
1. Adhyashana
2. Athi matra ahara
3. Athi sampurana
4. Guru, sheeta, pichila, snigdha guna ahara
5. Madhura Rasapradhana ahara
6. Specific dravya pradhana ahara
• Adhyashana: Food that is consumed before the digestion of previous meal is called as
Adhyashana. Here the patient will be not following the ahara ashta vidha visheshayatana.
• Ati matra Ahara:
Excess consumption of food is called as Athi matra Ahara sevana. Here the
consumption of food is related not only for quantity of intake but also the frequency of
intake. As the formation of Rasa is more, it over- nourishes the Dhatu of the body; there
by leading to Brihath Shareera.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
16
• Ati sampurana:
Intake of food up to ones full belly is called as Athi sampurana. To assess
the quantity of food in take the parameters had been explained in the classics.
• Guru, sheeta, pichila, snigdha guna ahara:
All these guna have an affinity towards the Kapha and the Medas there by
leading to increase in their quality and quantity. More over due to Picchila and Snigdha
guna, it causes the obstruction of the Vata in the srotas, in turn leads to sandukshana of
Agni. Guru and Snigdha are the properties of Meda or body fat. Acharya Caraka has
mentioned that, Meda is the seat of sleshma190 more over Meda and Sleshma possess
similar properties. So sleshmala ahara ( guru & snigdha) can able to produce excess
amount of fat in the body by virture of Ashryashryaee bhava and samanya vriddhi karana
concept Thus guru and snigdha ahara leads to sthoulya)
• Madhura Rasapradana ahara:
Madhura Rasa is having the Kapha prakopaka property because of which
there will be increase of Kapha and Medas. When the Madhura Rasa is added to Snigdha
guna then there will be more vitiation of Dosha.
Viharaja nidana: Following life style factors play an important role in Sthoulya71: 1. Avyayama 2. Avyavaya 3. Divaswapna
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
17
4. Asanasukha 5. Swapnasukha
• Avyayama & Avyavaya:
A person one who is not indulging in physical exercise, lives luxuriously with
sedentary life style will always tend to accumulation of kapha & meda in the body & this
leads to Sthoulya.
• Diwaswapna & atinidra:
All the acharyas have specially mentioned that day sleep is the one of the cause
for aggravation of kapha and also a santarpaka hetu and increases the abhishyandi guna
which obstructs the srotases of the body, leads to sthoulya in due course of time.
Manasika nidana: Manasika bhavas have an important role in Sthoulya72,viz. 1. Harshanityatwa 2. Achintana 3. Soukhya. Mental disterbances (chinta) cause vata vrudhi, which indirectly cause dhatu
kshaya, where as prasanna manas always increases kapha and does tarpana hence
becomes hetu for the Sthoulya.
Beejaswabhavaja:
• Acharya Charaka has specifically mentioned Beejadosha as the nidana for Sthoulya. Chakrapani and Gangadhara comments over this statement as “Ati sthula mata pitru shonita shukra swabhavat”, which means the character of Sthoulya is inherited from
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
18
Obese parents73.
• In Bhavaprakasha it has been mentioned that decreased proportion of ‘shonita’
and increased proportion of ‘shukra’ in beeja at the time of conception, results in development of lean but potent body, while increased proportion of ‘shonita’ and decreased proportion of ‘shukra’ predisposes towards the development of stout but weak body74. These genetic disorders are said to be incurable.
• Apart from that overnutrition during pregnancy, particularly with madhurarasa is
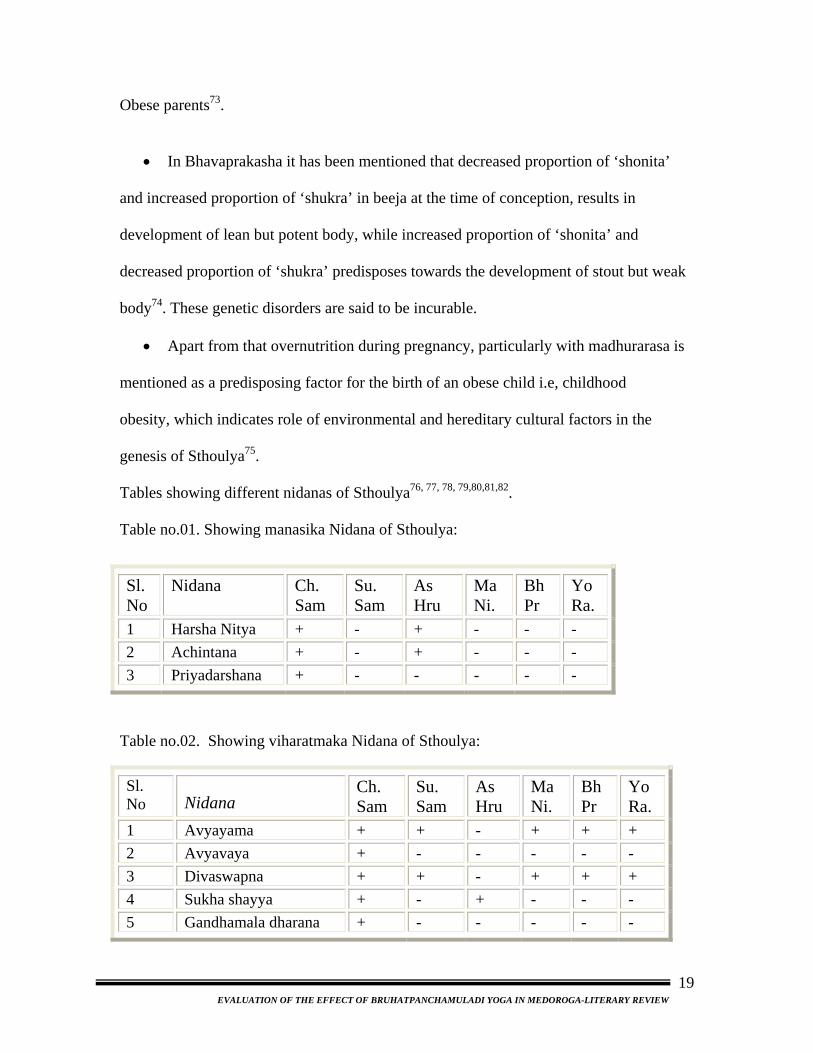
mentioned as a predisposing factor for the birth of an obese child i.e, childhood obesity, which indicates role of environmental and hereditary cultural factors in the genesis of Sthoulya75. Tables showing different nidanas of Sthoulya76, 77, 78, 79,80,81,82. Table no.01. Showing manasika Nidana of Sthoulya:
Sl. No
Nidana Ch. Sam
Su. Sam
As Hru
Ma Ni.
Bh Pr
Yo Ra.
1 Harsha Nitya + - + - - - 2 Achintana + - + - - - 3 Priyadarshana + - - - - -
Table no.02. Showing viharatmaka Nidana of Sthoulya:
Sl. No Nidana
Ch. Sam
Su. Sam
As Hru
Ma Ni.
Bh Pr
Yo Ra.
1 Avyayama + + - + + + 2 Avyavaya + - - - - - 3 Divaswapna + + - + + + 4 Sukha shayya + - + - - - 5 Gandhamala dharana + - - - - -
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
19
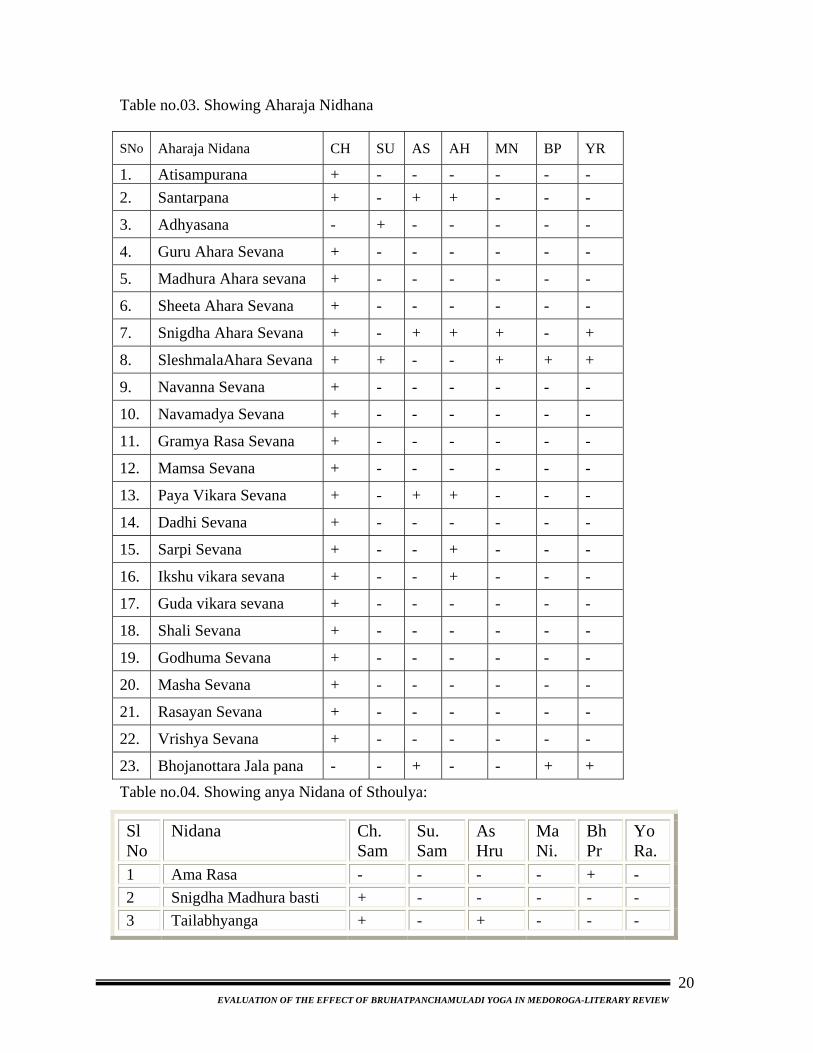
Table no.03. Showing Aharaja Nidhana
SNo Aharaja Nidana CH SU AS AH MN BP YR
1. Atisampurana + - - - - - - 2. Santarpana + - + + - - -
3. Adhyasana - + - - - - -
4. Guru Ahara Sevana + - - - - - -
5. Madhura Ahara sevana + - - - - - -
6. Sheeta Ahara Sevana + - - - - - -
7. Snigdha Ahara Sevana + - + + + - +
8. SleshmalaAhara Sevana + + - - + + +
9. Navanna Sevana + - - - - - -
10. Navamadya Sevana + - - - - - -
11. Gramya Rasa Sevana + - - - - - -
12. Mamsa Sevana + - - - - - -
13. Paya Vikara Sevana + - + + - - -
14. Dadhi Sevana + - - - - - -
15. Sarpi Sevana + - - + - - -
16. Ikshu vikara sevana + - - + - - -
17. Guda vikara sevana + - - - - - -
18. Shali Sevana + - - - - - -
19. Godhuma Sevana + - - - - - -
20. Masha Sevana + - - - - - -
21. Rasayan Sevana + - - - - - -
22. Vrishya Sevana + - - - - - -
23. Bhojanottara Jala pana - - + - - + +
Table no.04. Showing anya Nidana of Sthoulya:
Sl No
Nidana Ch. Sam
Su. Sam
As Hru
Ma Ni.
Bh Pr
Yo Ra.
1 Ama Rasa - - - - + - 2 Snigdha Madhura basti + - - - - - 3 Tailabhyanga + - + - - -
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
20
Samprapti It is defined as “the description of the evolution of the disease in sequential
order, commencing with Dosha-Dushya vaishyamya till the disease manifests
completely. For the manifestation of a disease various deranged structural and functional
elements of the body are responsible and all such things are studied under Samprapti. The
knowledge of Samprapti (also called as jathi and agathi) is very helpful to the physician
both for accurate diagnosis and also for planning appropriate treatment. It is essential to
know about “Ghataka” of the Samprapti because Samprapti vighatana itself is Chikitsa.
Samanya Samprapti of sthoulya:
• According to Charaka, Due to the avarana (obstruction) all srotases (channels) the
meda, vata vriddi occurs in the koshta leading to the ati sandhukshana of jatharagni. By
that, the consumed food will be digested rapidly and makes the person to crave for more
food. If at all due to any reason the person does not receive food in time may lead to
various complications. But repeated consumption of food in turn helps in meda vriddi
only leads to Sthoulya83.
• According to Sushruta Ama Rasa is produced due to Kaphavardhakaahara,
Adhysana, Avyayama, Divaswapana. The Madhura Bhava Ama Rasa moves within the
body, Snigdhansha of this Anna Rasa cause sthoulya that produces excessive stoutness in
turn Sthoulya84.
• According to Vagbhata, due to the nidana sevana medovrudhi takes place.This
vrudha meda does srotorodha(Obstructs the srotus) because of which Koshthachara vayu
cannot move out of the koshtha resulting into agni prajwalana. This prajwalita agni in the
koshtha does kshudha vrudhi hence person consumes more and more food (repeatedly).
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
21
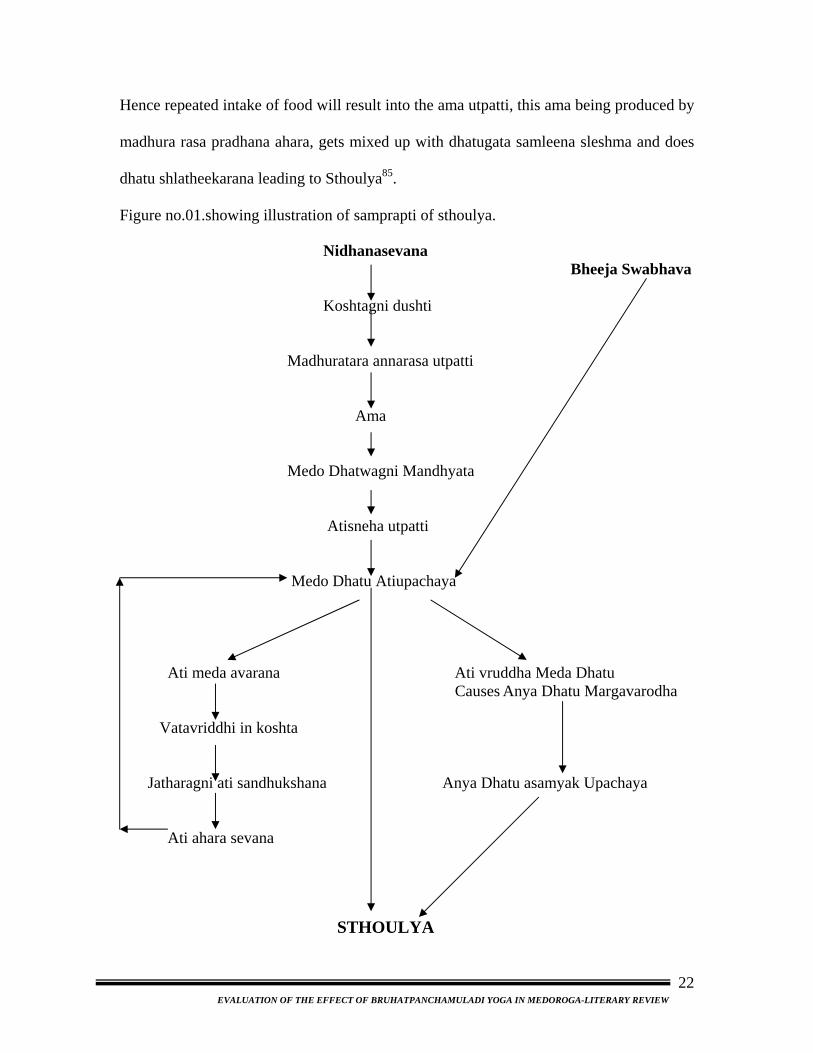
Hence repeated intake of food will result into the ama utpatti, this ama being produced by
madhura rasa pradhana ahara, gets mixed up with dhatugata samleena sleshma and does
dhatu shlatheekarana leading to Sthoulya85.
Figure no.01.showing illustration of samprapti of sthoulya.
Nidhanasevana Bheeja Swabhava Koshtagni dushti Madhuratara annarasa utpatti Ama Medo Dhatwagni Mandhyata Atisneha utpatti Medo Dhatu Atiupachaya
Ati meda avarana Ati vruddha Meda Dhatu Causes Anya Dhatu Margavarodha
Vatavriddhi in koshta Jatharagni ati sandhukshana Anya Dhatu asamyak Upachaya Ati ahara sevana STHOULYA
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
22
Vishesha Samprapti of Sthoulya:
For the manifestation of any disease, vitiation of few basic components of the
body required aredosha, dushya, srotas, agni and ama.
Dosha:
1) Kapha: In the samprapti of Sthoulya all the 3 doshas are involved. Acharya charaka
has considered Atisthoulya as one among the kaphajananatmaja vyadhi 86 which is clearly
observed by the nidanas of Sthoulya like guru, snigdha, sheeta, madhura and diwaswapna
etc. which are also considered as kaphakara nidanas. Hence inspite of involvement of
tridosha Kapha is the main dosha involved in pathogenesis of the Sthoulya.
2) Pitta: In obese persons, pitta also remains in a higher sight because the symptoms of
the Sthoulya like atikshudha, atipipasa, swedadhikyata, dourgandhya have also been
mentioned in the pittavrudhi. Mainly the pachaka pitta is involved in the etiopathogenesis
of the Sthoulya.
3) Vata:The process of circulation, digestion and proper distribution of dhatus including
medas is controlled by Samana and Vyana vayu.
Involvement of samanavayu can be clearly postulated with the evidence of
Agnisandhukshana.
Improper distribution of fat in the body proves the involvement of vyanavayu.
Vata has been mentioned in the state of Avruta in koshtha,which makes the
agnivaishamya,ultimately increases the the abhyavarana shakti or demand of
food.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
23
Dushya:
Acharya Sushruta has mentioned Sthoulya as a Dushya dominant disorder87 .Here,
Rasa, Mamsa, Meda, majja and shukra Dhatus are taken as Dushyas, as Kapha is seated
in all these Dhatus on the basis of Ashrayashrayeebhava. So, vitiation of Kapha also leads
to vitiation of dhatus in which kapha is seated88.
Srotas:
Involvement of medovahasrotas is the main factor along with the involvement of
other srotas in Sthoulya.
Charaka specifies Avyayama, Diwaswapna, Madhuradravyas and varuni(madya)
as nidanas of Sthoulya.It indicates clear involvement of rasavahasrotas.
Atisweda and dourgandhya indicate the involvement of swedavahasrotas.
Presence of Atipipasa indicates the involvement of udakavahasrotas.
An increased fat deposit inside the muscle indicates the involvement of
mamsavahasrotas.
Harshanityata, Achinta, Soukhya indicate the involvement of manovahasrotas.
Agni & Ama:
According to Vagbhata, mandagni, jatharagni and dhatwagni level are considered
root cause of all diseases “Rogo sarveapi mandagnou”89. In Sthoulya, due to vitiation of
vata by obstruction of medas, teekshnagni is a prominent feature. Here a question arises
how ama formation can take place instead of teekshnagni. Commentators Chakrapani and
Dalhana have tried to clarify this controversy by giving explanation, that in the state of
teekshnagni, person go for adhyashana, kalavyateeta ahara sevana again and again, which
leads to disturbance in agni which subsequently leads to the formation of ama. It has been
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
24
further explained by Dalhana that in the Sthoulya, formation of ama is due to the decrease
of medodhatwagni than jatharagni. Due to increased in sheeta, snigdha & madhura guna
which is opposite to that of Pitta the jataragni mandya take place leading to
Jataragnijanitaama. This further accumulation of Ama in Medovaha srotas due to
Medodhatwagni mandya the dhatwagni janita ama is resulted90.
Samprapti ghataka: Dosha : Kapha : Kledaka
Pitta : Pachaka
Vata : Samana, Vyana
Dushya : Rasa,Mamsa & Meda dhatu
Agni : Jatharagni
: Rasa and Meda Dhatvagni
Srotas : Meda vaha Srotas
: Rasa vaha Srotas
: Sweda vaha Srotas
: Udakavaha
Srota Dushti : Sanga
: Margavoradha91
: Amatah 92
Adhisthan : Whole body (Particularly Vapavahana & Meda dhara kala.)
Udbhava Sthala: Amashaya
Sanchara Sthana: Rasayani
Roga marga : Bahya
Ama : Jatharagni Vikriti Janita.
Dhatvagni Mandya Janita
Vyatktsthana : Sarvanga, Specifically Sphik, Udara, Stana & Gala.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
25
Poorvaroopa:
It refers to the features, which indicates the forth-coming disease. It usually
happens during (this corresponds with) fourth kriya kala called “Sthana samsraya”.
Clinically, this is important for early diagnosis, treatment and prognosis. Mild exhibition
of actual features of disease itself can be considered as Poorvaroopa.
Poorvaroopa is of two types: 1)Samanya poorvaroopa
2) Vishesha poorvaroop
Samanya poorva rupa gives the knowledge about forthcoming disease, but not regarding
the exact disease, where as Vishesha Poorvaroopa gives the knowledge regarding Dosha
as well as the disease.
In the context of present disease, none of the Acharayas have stressed upon the
poorva rupa, but it doesn’t mean that they are absent; Acharya charaka mentioned similar
pathogenesis of Prameha and Sthoulya93. Kapha and Meda also get vitiated in Sthoulya.
Therefore purvarupa of Prameha and Medovaha Srotodushti Lakshanas can be considered
as purvarupa of Sthoulya.
These are as follows:
• Atinidra
• Tandra
• Alasya
• Visra sharira gandha
• Anga gaurava
• Anga shaithilya etc.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
26
Roopa:
When the Vyadhi kriya kala is in fifth stage(Vyakthavastha), the disease will
produces the features called as “Rupa”. These rupa will indicate the manifestation of
disease. Rupa is having synonyms like Samsthana, Vyanjaka, Linga, Lakshana, Chinna,
and Akruthi. Rupa includes both subjective symptoms as well as objective signs. This is
the stage when Dosha -Dushya Sammurchana is completed.
All the lakshanas can be broadly classified as:
1) Sthoulya Pratyatmaka Lakshana
2) Sthoulya Samanya Lakshana
1. Sthoulya Pratyamtaka Lakshana:
The following are the diagnostic features of Sthoulya94:
• Medomamsa ativriddhi
• Chala sphik
• Chala udara
• Chala Stana
• Ayatha Upachaya
• Anutsaha
2. Sthoulya Samanya Lakshana:
Beside these Cardinal Symptoms, eight disabilities of Sthoulya are mentioned in
which can be considered as Sthoulya samanya lakshana are as follows95
Ayushohrasa - Life expectancy is decreased because other Dhatus could not be nourished
properly
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
27
Javoparodha - Shaithilya, Saukumarya and Guru poperties, causes Javoparodha
Kricchavyavaya - Due to obstruction in genital passage by Medodhatu and less
poduction of semen, the sex act becomes difficult
Daurbalya - This results because of the deranged metabolism owing to
mlnourishment of the Dhatus
Daurgandhya - Bad smelling results due to excessive sweating, innate quality of
Medodhatu and morbid nature of vitiated Meda
Swedabadha - It occurs due to sang in Swedavaha Srotas by ama
Kshudhatimatrata and Pipasatiyoga - Because of increased Agni in Koshtha and
vitiation of Vata by obstruction of Meda it results in excessive appetite and thirst.
All the symptoms of Sthoulya described in various Ayurvedic texts have been
summarized in the following table.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
28
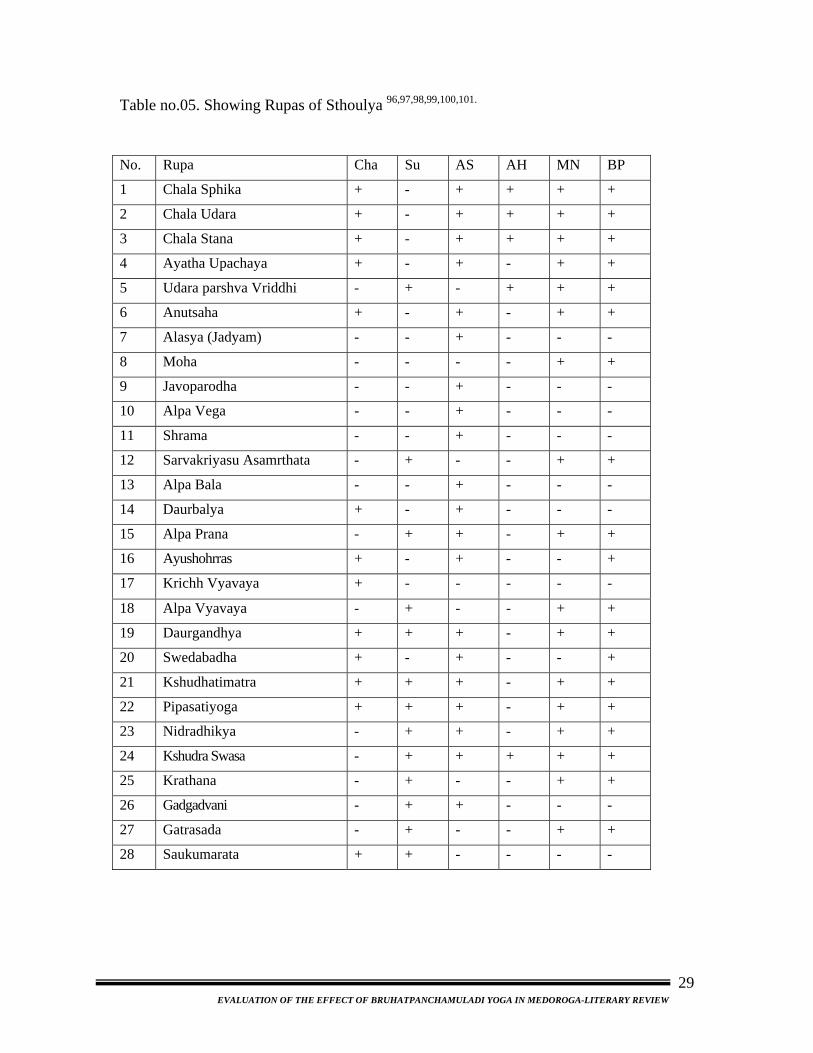
Table no.05. Showing Rupas of Sthoulya 96,97,98,99,100,101.
No. Rupa Cha Su AS AH MN BP
1 Chala Sphika + - + + + +
2 Chala Udara + - + + + +
3 Chala Stana + - + + + +
4 Ayatha Upachaya + - + - + +
5 Udara parshva Vriddhi - + - + + +
6 Anutsaha + - + - + +
7 Alasya (Jadyam) - - + - - -
8 Moha - - - - + +
9 Javoparodha - - + - - -
10 Alpa Vega - - + - - -
11 Shrama - - + - - -
12 Sarvakriyasu Asamrthata - + - - + +
13 Alpa Bala - - + - - -
14 Daurbalya + - + - - -
15 Alpa Prana - + + - + +
16 Ayushohrras + - + - - +
17 Krichh Vyavaya + - - - - -
18 Alpa Vyavaya - + - - + +
19 Daurgandhya + + + - + +
20 Swedabadha + - + - - +
21 Kshudhatimatra + + + - + +
22 Pipasatiyoga + + + - + +
23 Nidradhikya - + + - + +
24 Kshudra Swasa - + + + + +
25 Krathana - + - - + +
26 Gadgadvani - + + - - -
27 Gatrasada - + - - + +
28 Saukumarata + + - - - -
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
29
Classification of Sthoulya: For the purpose of diagnosis, prognosis and easy management disease should be
classified as per severity, as well as chronic. Hence classification of Sthoulya is essential,
but there is no such classification found in Ayurvedic texts. Astanga sangraha102,
Asthanga hrudaya103 and Sharangadhar samhita104 have thrown little light regarding
classification of Sthoulya as mentioned below.
In Astanga sangraha and hrudaya, three types of sthoulya i.e., adika, madhyama
and heena have been mentioned for better management while narrating the indications of
langhana upakrama.
From the above references Sthoulya may be classified as;
Charaka: Sthula, Atisthula
Sushruta: Sthoulya, medoroga
Vagbhata: Adhika, madhyama, heena.
Sharangadhara: Medodosha.
Though Vagbhata has classified sthoulya as of three types, he has not given any
explanation or parameters to consider so. Hence it is not clear that the classification
Adhika, Madhyama, Heena has been made by considering deha pramana or deha bala.
Upadrava:
The aliment, which is associated with a disease, and is manifested after the
manifestation of the main disease, is called Upadrava.
Describing the severity of Sthoulya, Charak has compared the aggravated vata
and Pitta with davanala, which destroys the whole forest.105 Though Charak has not
mentioned any specific Upadrava of Sthoulya, he describes that as Medas blocks the
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
30
Vayu in koshta it stimulates Agni which in turn digest the food quickly and wants more
and more food if not given enough food it causes severe Upadravas and kill the person
and also that Sthoola rogi always suffers from one or other disease106.
As Sthoulya is an Asadhya Vyadhi, it will always have the tendency to exhibit
upadrava. The concept of Sthoulya Ashta Maha Dosha can be considered as upadrava
itself. Here Agni and Vayu are important factors for upadrava. Prakupita Vata due to its
obstruction by Medas will make the Sandukshana of Agni. This Pradeepta Agni digests
the food as quick as fire burning the forest. Hence there will be Athi kshudha in the
Sthoola. If the proper quality and quantity of food is not supplied to this Teekshnagni, it
will produce hazardous effect, which may cause even death.
Bhava mishra and Yogaratnakara have used the word “Sudustara” in the place
of upadrava shabda.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
31
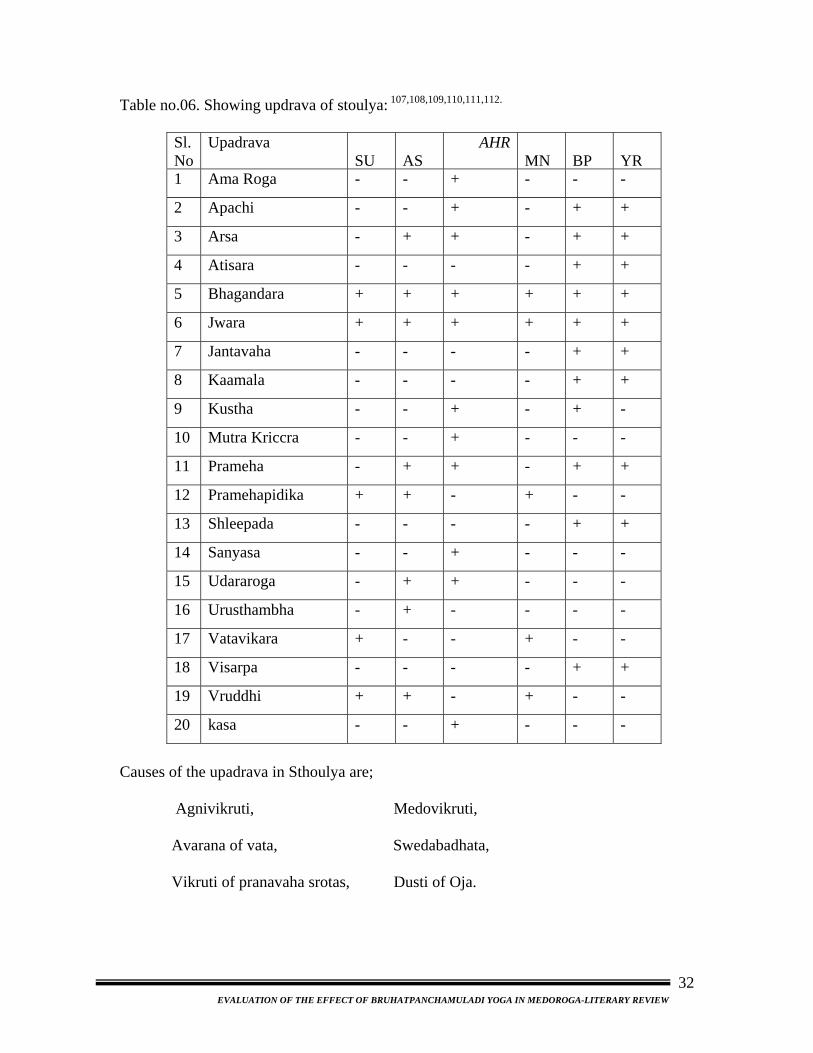
Table no.06. Showing updrava of stoulya: 107,108,109,110,111,112.
Sl. No
Upadrava SU
AS
AHR MN
BP
YR
1 Ama Roga - - + - - -
2 Apachi - - + - + +
3 Arsa - + + - + +
4 Atisara - - - - + +
5 Bhagandara + + + + + +
6 Jwara + + + + + +
7 Jantavaha - - - - + +
8 Kaamala - - - - + +
9 Kustha - - + - + -
10 Mutra Kriccra - - + - - -
11 Prameha - + + - + +
12 Pramehapidika + + - + - -
13 Shleepada - - - - + +
14 Sanyasa - - + - - -
15 Udararoga - + + - - -
16 Urusthambha - + - - - -
17 Vatavikara + - - + - -
18 Visarpa - - - - + +
19 Vruddhi + + - + - -
20 kasa - - + - - -
Causes of the upadrava in Sthoulya are;
Agnivikruti, Medovikruti,
Avarana of vata, Swedabadhata,
Vikruti of pranavaha srotas, Dusti of Oja.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
32
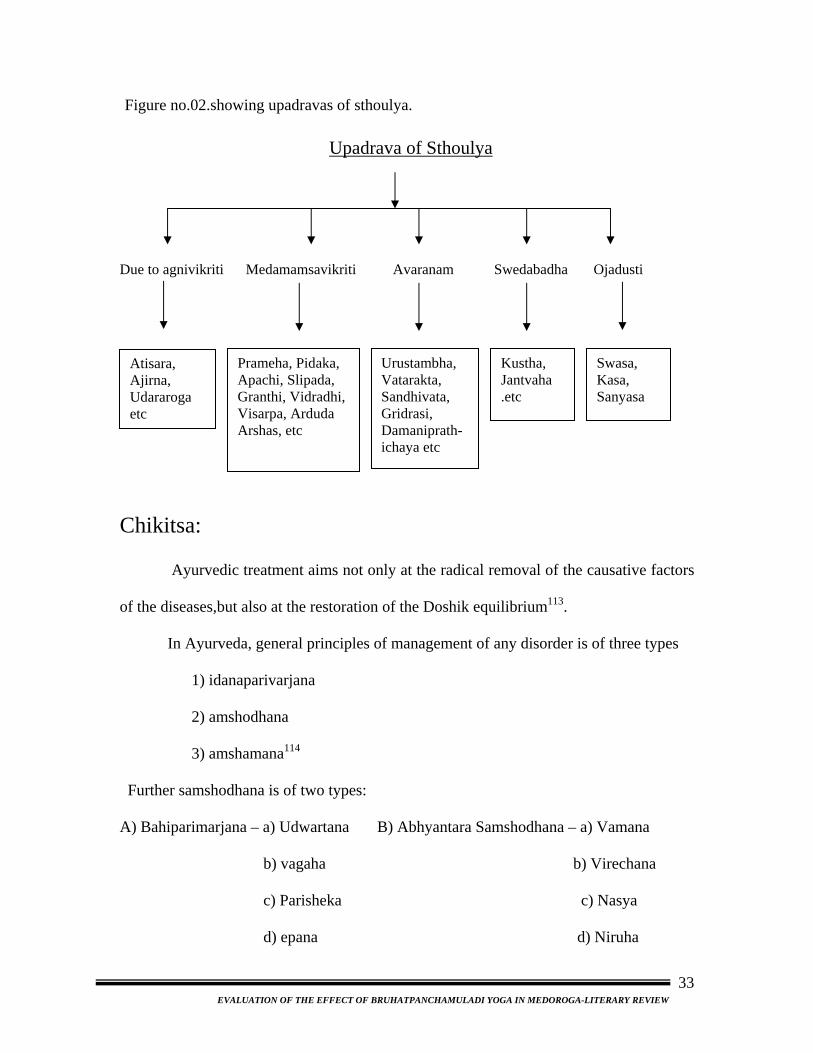
Figure no.02.showing upadravas of sthoulya. Upadrava of Sthoulya Due to agnivikriti Medamamsavikriti Avaranam Swedabadha Ojadusti
Chikitsa: Ayurvedic treatment aims not o
of the diseases,but also at the restoration
In Ayurveda, general principles
1) idanaparivarjana
2) amshodhana
3) amshamana114
Further samshodhana is of two types:
A) Bahiparimarjana – a) Udwartana
b) vagaha
c) Parisheka
d) epana
Prameha, Pidaka, Apachi, Slipada, Granthi, Vidradhi, Visarpa, Arduda Arshas, etc
-
EVALUATION OF THE EFFECT OF B
Urustambha, Vatarakta, Sandhivata, Gridrasi, Damaniprathichaya etc
nly at the radical r
of the Doshik equ
of management of
B) Abhyantara Sa
RUHATPANCHAMULADI Y
Kustha, Jantvaha.etc
emoval of the
ilibrium113.
any disorder is
mshodhana – a
b)
c
d)
OGA IN MEDOROGA-L
Swasa, Kasa, Sanyasa
Atisara, Ajirna, Udararogaetc
causative factors
of three types
) Vamana
Virechana
) Nasya
Niruha
ITERARY REVIEW
33
Aims of treatment in Sthoulya:
Alleviation of Vata and Kapha along with depleted Medodhatu by increasing
medodhatwagni is the main aim of treatment of Sthoulya.(Gada nigraha)
Guru cha Apatarpanam – Administration of the drugs which are guru and
karshana that results in thealleviation of medas, sleshma anvata115
Administration of virukshana and chedaniya dravyas116
Nidana Parivarjana:
Aharatmaka, Viharatamaka, Manasika and Anya Nidana, which are responsible
for the disease (apathya), should be avoided as a Nidanparivarjana chikitsa.
Samshodhana:
Bahir parimarjana chikitsa:
Acharyas have mentioned external purification therapy for management of
Sthoulya. Acharyas narrated Ruksha Udavartana for Sthoulya117. The benefits of
Udwartana also mentioned. I.e. Kaphahara, Medasa Pravilayana, Sthirikaranam
Angam118 etc.
Abhyantar Samshodhana:
According to Vagbhata, Atisthoulya patients with Adhika Dosha and Adhik Bala
should be treated by Samshodhana therapy including Vamana, Virechana, Ruksha
Niruha, Raktamokshana119 etc.
Charaka has mentioned Sthoulya under the caption of Santarpanajanita Vyadhi
and for its management; Vamana, Virechana and Raktamokshana are recommended120.
He also suggested Ruksha, Tikshna and Ushna vasti for the management purpose of
Sthoulya.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
34
Snehana: It is contraindicated for the patients of Sthoulya121. However, Lekhaniya,
Medohara properties122 and Sthulatvahara Karma123,124of Taila are described in
Ayurveda. So, on exigency usage of Taila is recommended125
Swedana: Swedana is also contraindicated in Sthoulya rogi but Niragni sweda can be
encouraged in Sthoulya in the form of Vyayama, Alpa Sevana and Upanaha are
advised.126
Vamana : Sushruta has recommended Vamana for the treatment of Medoroga127.
According to kashyapa by doing vamana the person is going to get laghuta in the body
and it irradicates the meda dourgandhya and kaphaja rogas128
Virechana: Virechana has been recommended for patients of Sthoulya129
Vasti: In classics Lekhan vasti is considered as a best therapy for Sthoulya /
medovriddhi130 The role of Ruksha, Ushna and Tikshna vasti in the management of
Sthoulya is very well explained by Gangadhara (Jalpakapataru Tika commentary on as it
alleviates kapha and meda131.Sharangahara has given a clear description regarding the
properties of lekhan dravyas and characteristics of lekhan vasti132
Practices in Sthoulya with vasti:
Vasti prepared with Taila, Gomutra, Kanji and Saindhava 133
Erandamuladi Niruha134
Kapha nashak Vasti135
Lekhan Vasti 136
Madhutailika Vasti 137,138
Rakata Mokshana: Maharshi Kashyapa has recommended Rakta mokshana with Urdhva
and Adhah samshodhana for sthoulya, especially for medosvi dhatri139 Similarly
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
35
Bhavaprakash has considered Rakta mokshana as a therapy for sthoulya 140. So we can
adopt Raktamokshana for the treatment of Rakta gata meda.
Shiro virechana: Kashyapa has considered karshana nasya as a treatment for disorders of
kapha141 and Sthoulya is enumerated as one of the twenty-kapha nanatmaja vyadhis, so it
can be applied to treat sthoulya. Triphaladya taila is indicated for nasya in the patients of
medovriddhi142.
Samshamana:
• Among Sad upakramas,langhana and rukshana can be administrated for
samshamana purpose in Sthoulya143. Samshamana chikitsa can be implemented through
seven different ways. All the seven ways of langhana can be applied to the patient of
Sthoulya according to rogi-roga bala.
• Charaka Samhita has been given treatment in following words.
I.e. Administration of Guru and Apatarpaka articles which possess additional Vata,
Shleshmala and Medonashaka properties are considered as an ideal for Samshaman
therapy. Chakrapani has explained that Guru Guna is sufficient to alleviate vitiated Agni
and Atikshudha. Apatarpana property provides less nourishment and thus leads to
depletion of Meda. For example Madhu possess Guru and Ruksha properties, hence it is
ideal for management of Sthoulya. Gangadhara has interpreted that Guru Property is
suitable to alleviate Tikshnagni and vitiated vata especially Kosthagata Vata which
ultimately reduces Atikshudha and Apatarpan property causes reduction of Meda144.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
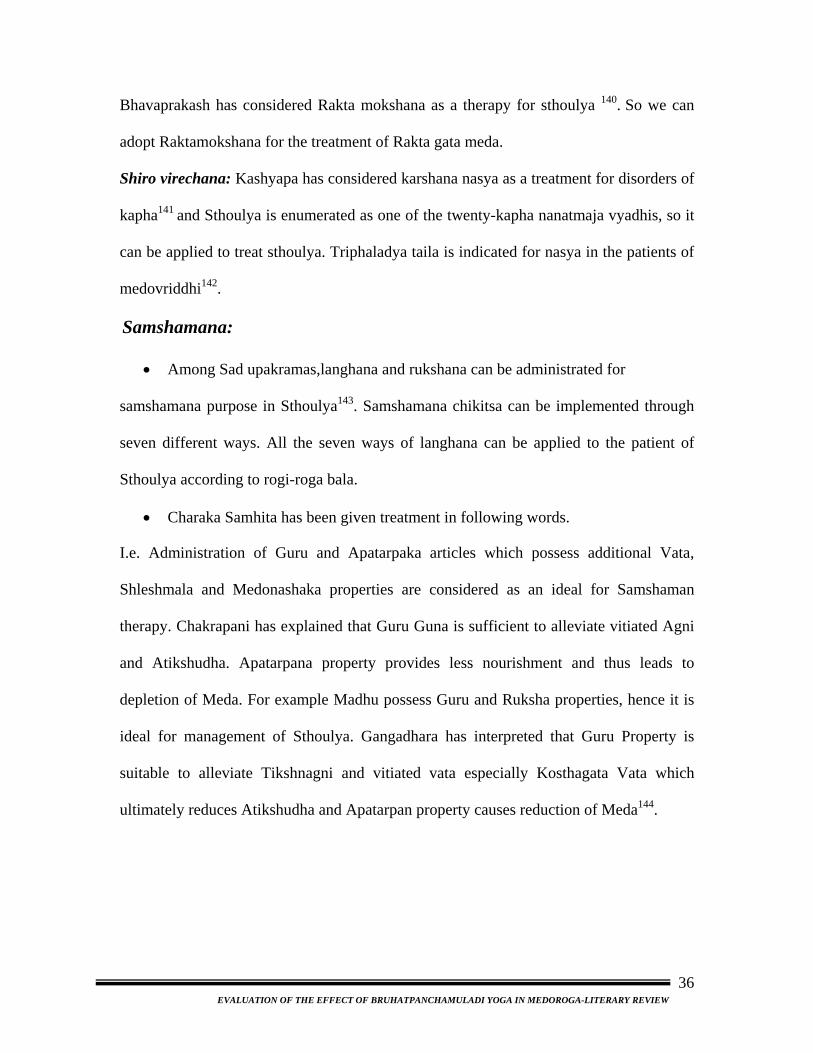
36
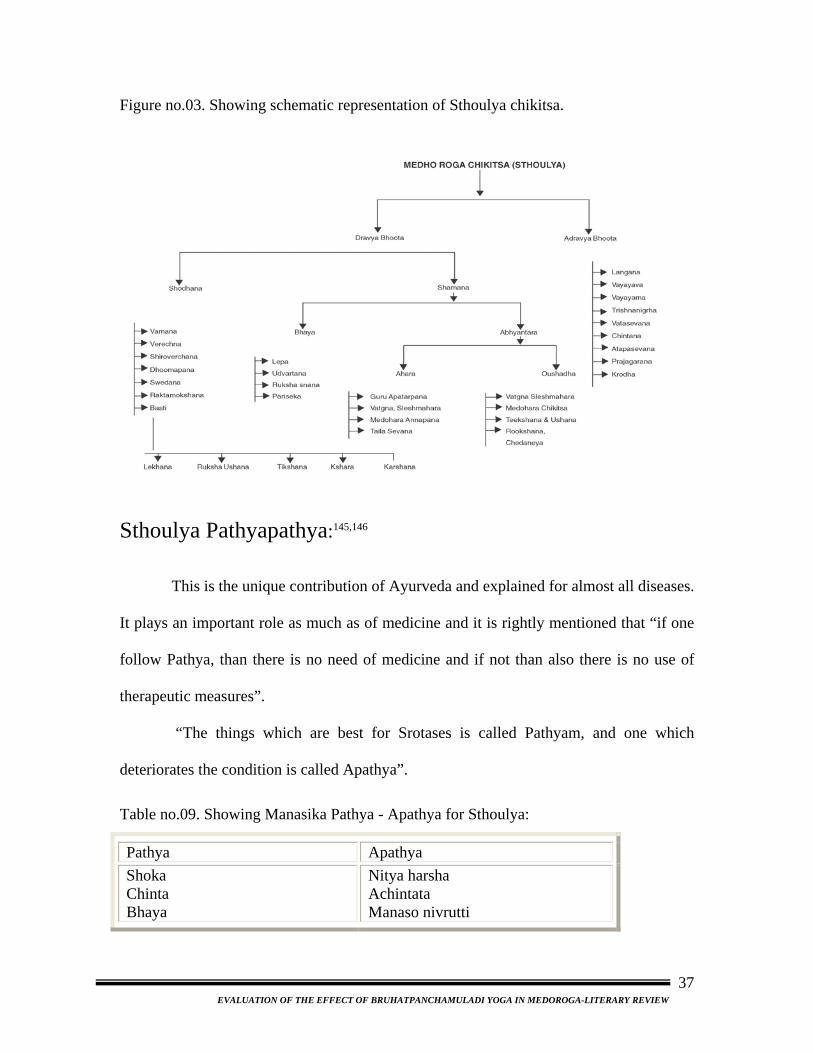
Figure no.03. Showing schematic representation of Sthoulya chikitsa.
Sthoulya Pathyapathya:145,146
This is the unique contribution of Ayurveda and explained for almost all diseases.
It plays an important role as much as of medicine and it is rightly mentioned that “if one
follow Pathya, than there is no need of medicine and if not than also there is no use of
therapeutic measures”.
“The things which are best for Srotases is called Pathyam, and one which
deteriorates the condition is called Apathya”.
Table no.09. Showing Manasika Pathya - Apathya for Sthoulya:
Pathya Apathya Shoka Chinta Bhaya
Nitya harsha Achintata Manaso nivrutti
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
37
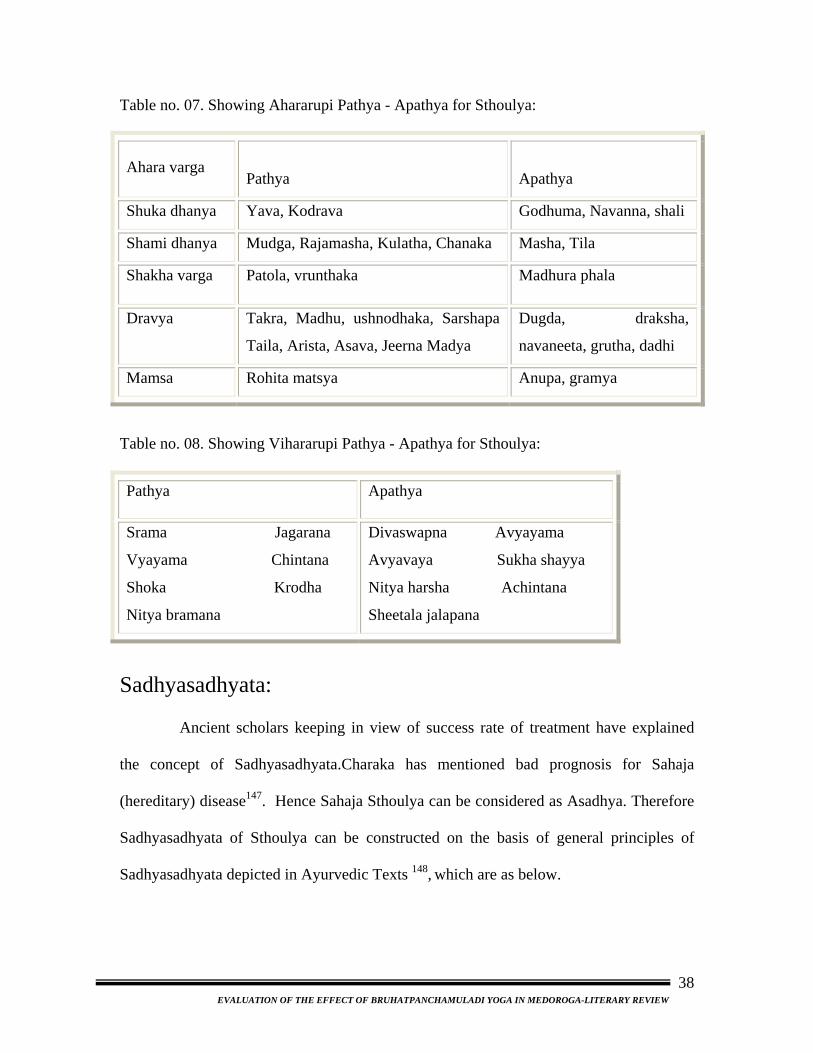
Table no. 07. Showing Ahararupi Pathya - Apathya for Sthoulya:
Ahara varga
Pathya
Apathya
Shuka dhanya Yava, Kodrava Godhuma, Navanna, shali
Shami dhanya Mudga, Rajamasha, Kulatha, Chanaka Masha, Tila
Shakha varga Patola, vrunthaka Madhura phala
Dravya Takra, Madhu, ushnodhaka, Sarshapa
Taila, Arista, Asava, Jeerna Madya
Dugda, draksha,
navaneeta, grutha, dadhi
Mamsa Rohita matsya Anupa, gramya
Table no. 08. Showing Vihararupi Pathya - Apathya for Sthoulya:
Pathya Apathya
Srama Jagarana
Vyayama Chintana
Shoka Krodha
Nitya bramana
Divaswapna Avyayama
Avyavaya Sukha shayya
Nitya harsha Achintana
Sheetala jalapana
Sadhyasadhyata:
Ancient scholars keeping in view of success rate of treatment have explained
the concept of Sadhyasadhyata.Charaka has mentioned bad prognosis for Sahaja
(hereditary) disease147. Hence Sahaja Sthoulya can be considered as Asadhya. Therefore
Sadhyasadhyata of Sthoulya can be constructed on the basis of general principles of
Sadhyasadhyata depicted in Ayurvedic Texts 148, which are as below.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
38
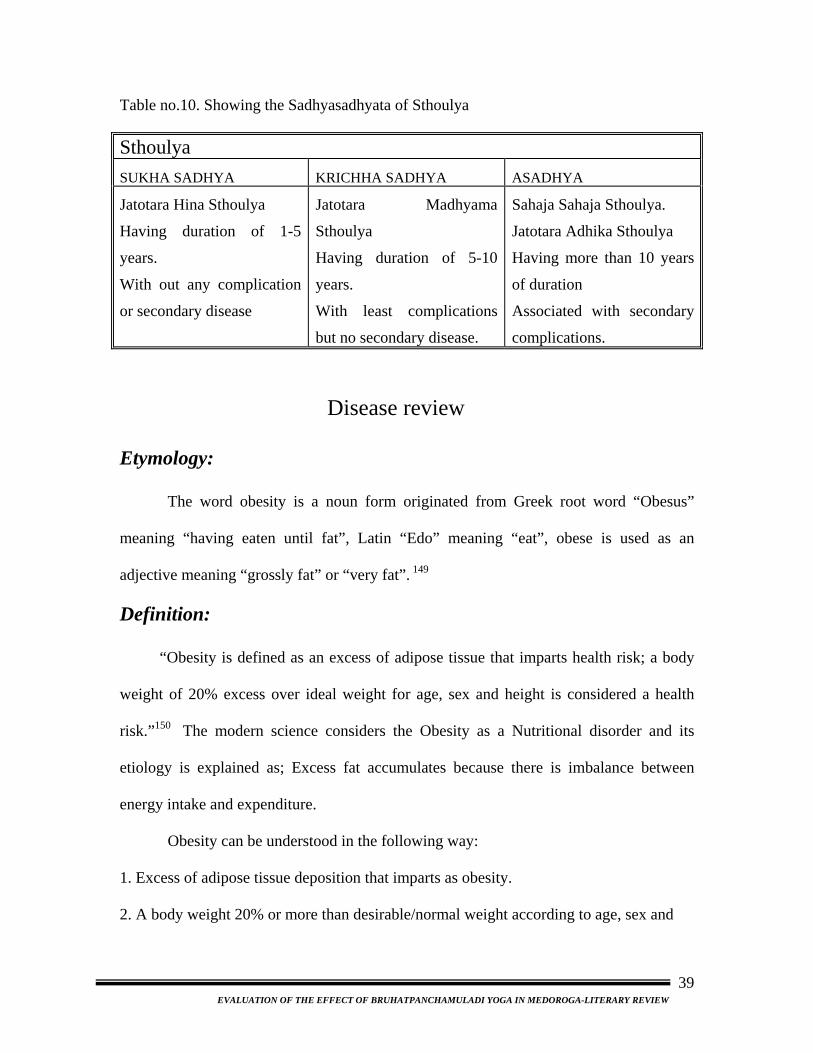
Table no.10. Showing the Sadhyasadhyata of Sthoulya
Sthoulya SUKHA SADHYA KRICHHA SADHYA ASADHYA
Jatotara Hina Sthoulya
Having duration of 1-5
years.
With out any complication
or secondary disease
Jatotara Madhyama
Sthoulya
Having duration of 5-10
years.
With least complications
but no secondary disease.
Sahaja Sahaja Sthoulya.
Jatotara Adhika Sthoulya
Having more than 10 years
of duration
Associated with secondary
complications.
Disease review Etymology:
The word obesity is a noun form originated from Greek root word “Obesus”
meaning “having eaten until fat”, Latin “Edo” meaning “eat”, obese is used as an
adjective meaning “grossly fat” or “very fat”. 149
Definition:
“Obesity is defined as an excess of adipose tissue that imparts health risk; a body
weight of 20% excess over ideal weight for age, sex and height is considered a health
risk.”150 The modern science considers the Obesity as a Nutritional disorder and its
etiology is explained as; Excess fat accumulates because there is imbalance between
energy intake and expenditure.
Obesity can be understood in the following way:
1. Excess of adipose tissue deposition that imparts as obesity.
2. A body weight 20% or more than desirable/normal weight according to age, sex and
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
39

height is regarded as obese.
3. Nowadays obesity is defined as BMI > 25kg/m2.
4. Obesity may be defined as an abnormal growth of adipose tissue which is in three
Ways as;
i. Enlargement of fat cells in size (hypertrophy obesity)
ii. Increase in the number of fat cells (hyperplasic obesity)
iii. Combination of the above two.
Etiology:151
1. Overeating: The overeating may be in terms of quantity (multiple meals and snaking)
as well as in terms of quality (high calorie diet). It has been shown that obese patients
tend to overeat which eventually results in the accumulation of fat. For example, 10.5
kcal excess energy would lead to a 10 kg weight gain over 20 years.
2. Age: Obesity is most prevalent in middle-age, but can occur at any stage of life.
Obesity n childhood and adolescence is likely to be followed by obesity in adult life.
3. Socio-economic: In affluent countries obesity is more common in the lower socio-
economic groups. In developing countries like India it can occur only in prosperous elite.
Some occupations predispose to obesity, e.g. cooks and barmen, IT experts, clerks,
managers etc.
4. Addictions: Frequent uses of alcohol will cause deposition of adipose as one gram of
alcohol gives 7 kcal of energy.
5.Smoking: Offspring’s of mother smoked during pregnancy have a significantly
increased risk of overweight later in life. While additional weight gain can be seen after
cessation of smoking in adults.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
40
6. Heredity: A familial tendency exists in many cases, but it is difficult to disentangle
environmental and genetic components. Pattern of eating and activity are influenced by
social, cultural and economic factors, which may be passed on from one generation to
another. However studies involving twins and adopted children indicate the importance
of genetic factor in both total body fat and its distribution. Genes in the individual decide
the number of Adiposities and set point of weight.
7. Environmental factors: This factor is divided into,
i. Physical environment – this includes air, water and food. In obesity only the food
factor is applicable which is already discussed.
ii. Psycho-social environment - it covers a complex of psychosocial factors which are
defined as those factors affecting personal health, health care and community well being.
The latest studies have proved that even stress ups weight.152 Nowadays this factor is
seen more in the society.
8. Endocrine factors: An endocrine influence on body fat is seen both in normal
physiological situations and in pathological states. Obesity in women commonly begins
at puberty, during pregnancy or at menopause, obesity frequently but not invariably
accompanies hypothyroidism, hypogonadism, hypopitutarism etc. However, the over
whelming majority of the obese patients show no clinical evidence of endocrinal
disorder. The plasma concentration of Insulin and Cortisol is commonly raised and that of
growth hormone is reduced.
9. Drugs: The use of steroids, oral contraceptives, phenothiazines and insulin is
commonly followed by weight gain, mainly because appetite is stimulated.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
41
10. Lack of sexual drive: ‘Losing interest’ is a refrain that revolves around the husband
in many a 35-plus woman’s life. The AIMS cardiology unit along with the Indian council
of medical research (ICMR) verified that in an obesity survey in 2004, a large number of
respondents blamed the lack of sexual drive in career-obsessed as the prime cause behind
their apathy towards their own self.153
Pathogenesis:154
Obese persons having an increase in number and/or size of adipose cells suggest
hypertrophy and/or hyperplasia of adiposities either due to functional demand in
particular age or sex or due to genetic, endocrine, behavioral, psychological or iatrogenic
factors. After reduction in weight the adipose cells shrink in size but hyperplasia remains
fixed. Adult onset obesity is characterized predominantly by adipose cell hypertrophy
with minimum hyperplasia. There are three main factors in the pathogenesis of obesity:
Excessive lipid deposition:
Excessive lipid deposition is due to either increased food intake, hypothalamic
lesions. Adipose cell hyperplasia or hyperlipogenesis. Increased food intake in form of
carbohydrates, proteins and fats by metabolic process lastly converts in fat and get stored
at fat depots.
Physiology of hunger and satiety is dependent upon hypothalamus. Lesions may
damage these centre leads to voracious appetite (Ventro medial and lateral nuclear area of
hypothalamus) and ultimately leads to obesity.
Similarly adipose cell hyperplasia or hyperlipognesis due to genetic or
endocrine pathology leads to obesity.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
42
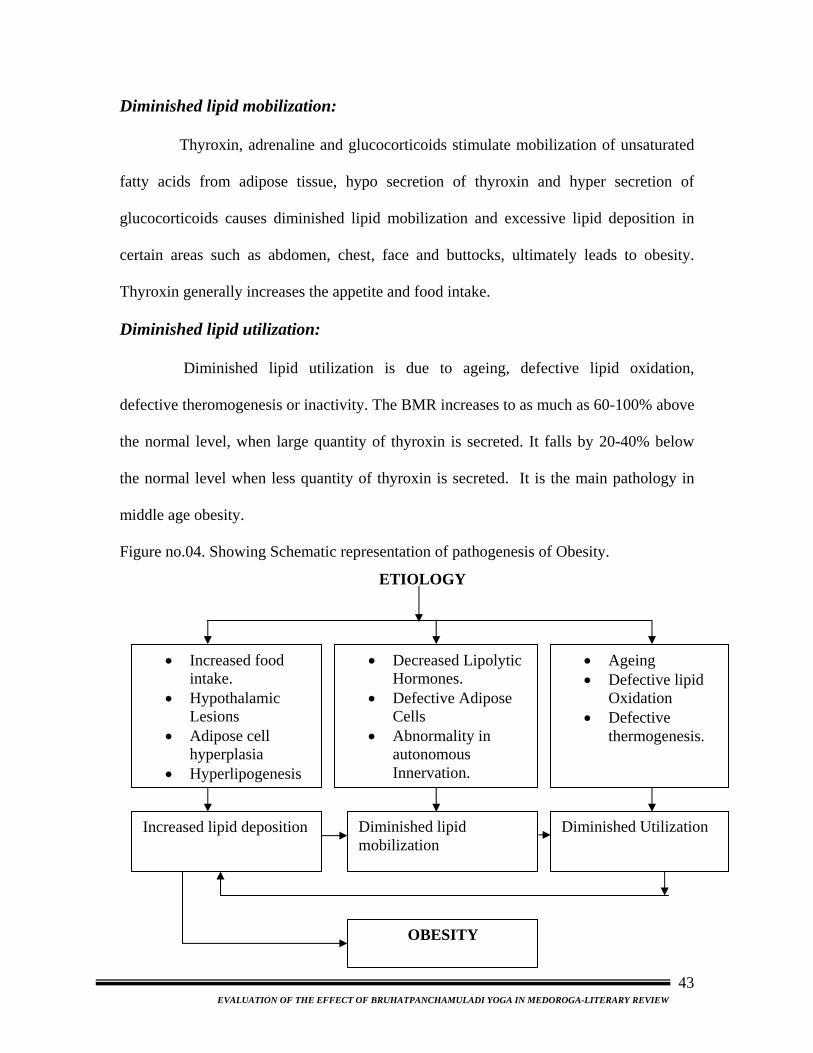
Diminished lipid mobilization:
Thyroxin, adrenaline and glucocorticoids stimulate mobilization of unsaturated
fatty acids from adipose tissue, hypo secretion of thyroxin and hyper secretion of
glucocorticoids causes diminished lipid mobilization and excessive lipid deposition in
certain areas such as abdomen, chest, face and buttocks, ultimately leads to obesity.
Thyroxin generally increases the appetite and food intake.
Diminished lipid utilization:
Diminished lipid utilization is due to ageing, defective lipid oxidation,
defective theromogenesis or inactivity. The BMR increases to as much as 60-100% above
the normal level, when large quantity of thyroxin is secreted. It falls by 20-40% below
the normal level when less quantity of thyroxin is secreted. It is the main pathology in
middle age obesity.
Figure no.04. Showing Schematic representation of pathogenesis of Obesity.
ETIOLOGY
• Increased food intake.
• Hypothalamic Lesions
• Adipose cell hyperplasia
• Hyperlipogenesis
• Decreased Lipolytic Hormones.
• Defective Adipose Cells
• Abnormality in autonomous Innervation.
• Ageing • Defective lipid
Oxidation • Defective
thermogenesis.
Increased lipid deposition Diminished lipid mobilization
Diminished Utilization
OBESITY
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
43
Lipid / Fat Metabolism, Transport, Storage:155
• Biomedical importance: Fat absorbed from the diet and lipids synthesized by the liver and adipose tissue
must be transported between the various tissue and organs for utilization and storage.
Since lipids are insoluble in water, the problem of how to transport them in the aqueous
blood plasma is solved by associating nonpolar lipids (triacylglycerol and cholesteryl
easters) with amphipathic lipids (phospholipids and cholesterol) and proteins to make
water miscible lipoproteins.
In a meal-eating omnivore such as the human, excess calories are ingested in the
anabolic phase of the feeding cycle, followed by a period of negative caloric balance
when the organism drows upon its carbohydrate and fat stores. Lipoproteins mediate this
cycle by transporting the lipids from the intestines as chylomicrons- and from the liver as
very low density lipoproteins (VLDL) – to most tissue for oxidation and to adipose tissue
for storage. Lipids are mobilized from adipose tissue as free fatty acids (FFA) attached to
serum albumin.
• Lipids are transported in the plasma as lipoproteins:
Four major lipid classes are present in Lipoproteins – Plasma lipids consists of
Triacylglycerol - 16 %
Phospholipids - 30 %
Cholesterol - 14 %
Cholesteryleasters–36%
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
44
and a much smaller fraction of uneasterified long-chain fatty acids (free fatty acids) – 4%
this latter fraction, the free fatty acids (FFA), is metabolically the most active of the
plasma lipids.
Four major groups of plasma lipoproteins have been identified – Because fat is
less dense than water, the density of lipoprotein decreases as the proportion of lipid to
protein increases. In addition to FFA, four major groups of lipoproteins have been
identified that are identified physiologically and in clinical diagnosis. These are:
i. Chylomicrons, derived from intestinal absorption of triacylglycerol and other lipids
ii. Very low density lipoproteins (VLDL),derived from the liver for export of triglycerol
iii. Low density lipoprotein (LDL), representing a final stage in the catabolism of VLDL
iiii. High density lipoprotein (HDL), involved in VLDL and Chylomicron metabolism
and also in cholesterol transport.
• Triacylglycerol is transported from the intestine in chylomicrons and
from the liver in VLDL:
By definition, chylomicrons are found in chyle formed only by the lymphatic
system draining the intestine. They are responsible for the transport of all dietary lipids
into the circulation. Small quantities of the VLDL are also to be found in chyle; however,
most of the plasma VLDL are of hepatic origin. They are the vehicle for transport of
triacylglycerol from the liver to the extra hepatic tissues.
• The Liver plays a central role in lipid Transport & Metabolism:
The Liver carries out the following major functions in lipid metabolism:
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
45
1) It facilitates the digestion and absorption of lipids by the production of bile, which
contains cholesterol and bile salts synthesized within the liver de novo or from uptake of
lipoprotein cholesterol.
2) The liver has active enzyme systems for synthesizing and oxidizing fatty acids, and for
synthesizing triacylglycerol and phospholipids.
3) It converts fatty acids to ketone bodies (ketogenesis).
4) It plays an integral part in the synthesis and metabolism of plasma lipoproteins.
• Adipose tissue is the main store of triacylglycerol in the body:
The triacylglycerol stores in adipose tissue are continually undergoing lipolysis
(hydrolysis) and reesterification. These two processes are entirely different pathways
involving different reactants and enzymes. This allows the process of esterification or
lipolysis to be regulated separately by many nutritional, metabolic and hormonal factors.
The resultant of these two processes determines the magnitude of the free fatty acid pool
in adipose tissue, which in turn determines the level of free fatty acids circulating in the
plasma. Since the latter has most profound effect on the metabolism of other tissues,
particularly liver and muscle, the factors operating in adipose tissue that regulate the out
flow of free fatty acids exert an influence far beyond the tissue itself. And there is a
continuous cycle of lipolysis and reesterification within the tissue. However, when the
rate of reesterification is not sufficient to match the rate of lipolysis, free fatty acids
accumulate and diffuse into the plasma, where they bind to albumin and raise the
concentration of plasma free fatty acids.
• Hormones regulate fat mobilization:
1) Insulin reduces the output of free fatty acids:
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
46
Insulin inhibits the release of free fatty acids from adipose tissue, which is followed by a
fall in circulating plasma free fatty acids. It enhances lipogenesis and the synthesis of
acylglycerol and increases the oxidation of glucose to CO2 via the pentose phosphate
pathway.
2) Several hormones promote lipolysis: Other hormones accelerate the release of free
fatty acids from adipose tissue and raise the plasma free fatty acid concentration by
increasing the rate of lipolysis of the triacylglycerol stores. These include epinephrine,
nor epinephrine, glucagon, adrenocorticotropic hormone (ACTH), thyroid stimulating
hormone (TSH), growth hormone (GH), and vasopressin. Many of these activate the
hormone-sensitive lipase. For an optimal effect, most of these lipolytic processes require
the presence of ‘glucocorticoids’ and ‘thyroid hormones’.
Totally the whole process can be summarized as triacylglycerol is the main
storage lipid in adipose tissue. Upon mobilization, free fatty acids and glycerol are
released. Free fatty acids are an important fuel source.
‘Even stress ups obesity’. Nature magazine reported last year how the body
releases a molecule, NPY (neuropeptide Y) when stressed. It unlocks the body’s fat cells
and makes them grow in both size and number. Cortisol, a hormone, released during the
stress response, has also been implicated in developing belly fat. Also, bodies that are not
rested produce increased amounts of ghrelin, a hormone that triggers the sensation of
hunger, and reduces production of leptin-a hormone that regulates appetite.
Intra abdominal (central) fat accumulation and increased Risk.
Compared with subcutaneous adipose tissue, intra abdominal adipose tissue has
more cells per unit mass. Intra-abdominal adipocytes are located upstream from liver in
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
47
the portal circulation. This means that there is a marked increase in the flux of
nonesterified fatty acid to the liver via the portal blood in patients with abdominal
obesity.
Classification:156
The most common cause of obesity is excess calorie intake coupled with physical
inactivity.
I. Anatomical characteristic of adipose tissue.
1. Hyper trophic obesity: (Increase in enalargement of fat cells) correlates with
android or truncal fat distribution and is more often associated with metabolic
disorders such as DM, HTN etc.
2. Hyperplastic obesity: Increase in no of fat cells.
II. Age at onset of obesity:
Obesity which starts in early childhood tends to be more severe and generalized
and obese children have a higher chance of being obese in adulthood. Over nutrition is
more often responsible for this condition.
III Etiological factors:
1. Neuro-endocrine disorders:
a) Hypothalamic disorders
b) Hypothyroidism
c) Cushings syndrome
d) Hyperinsulinism etc.
2. Genetic syndromes:
a) L.M.B
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
48
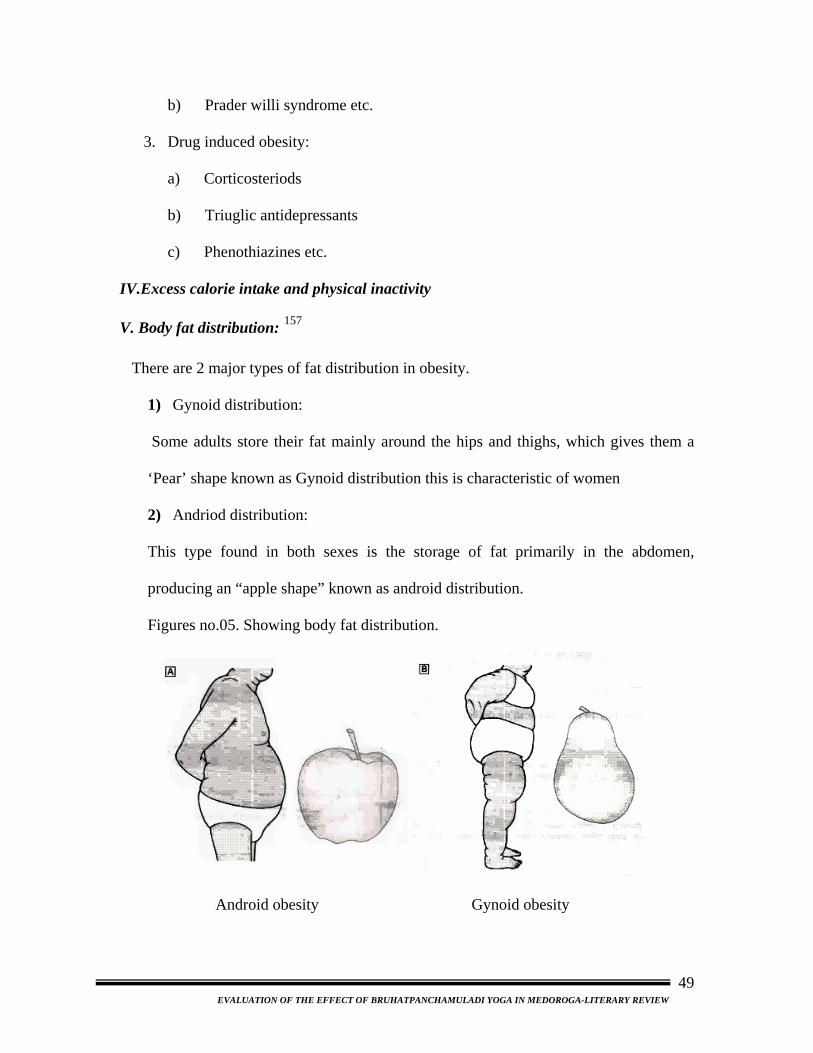
b) Prader willi syndrome etc.
3. Drug induced obesity:
a) Corticosteriods
b) Triuglic antidepressants
c) Phenothiazines etc.
IV.Excess calorie intake and physical inactivity
V. Body fat distribution: 157
There are 2 major types of fat distribution in obesity.
1) Gynoid distribution:
Some adults store their fat mainly around the hips and thighs, which gives them a
‘Pear’ shape known as Gynoid distribution this is characteristic of women
2) Andriod distribution:
This type found in both sexes is the storage of fat primarily in the abdomen,
producing an “apple shape” known as android distribution.
Figures no.05. Showing body fat distribution.
Android obesity Gynoid obesity
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
49
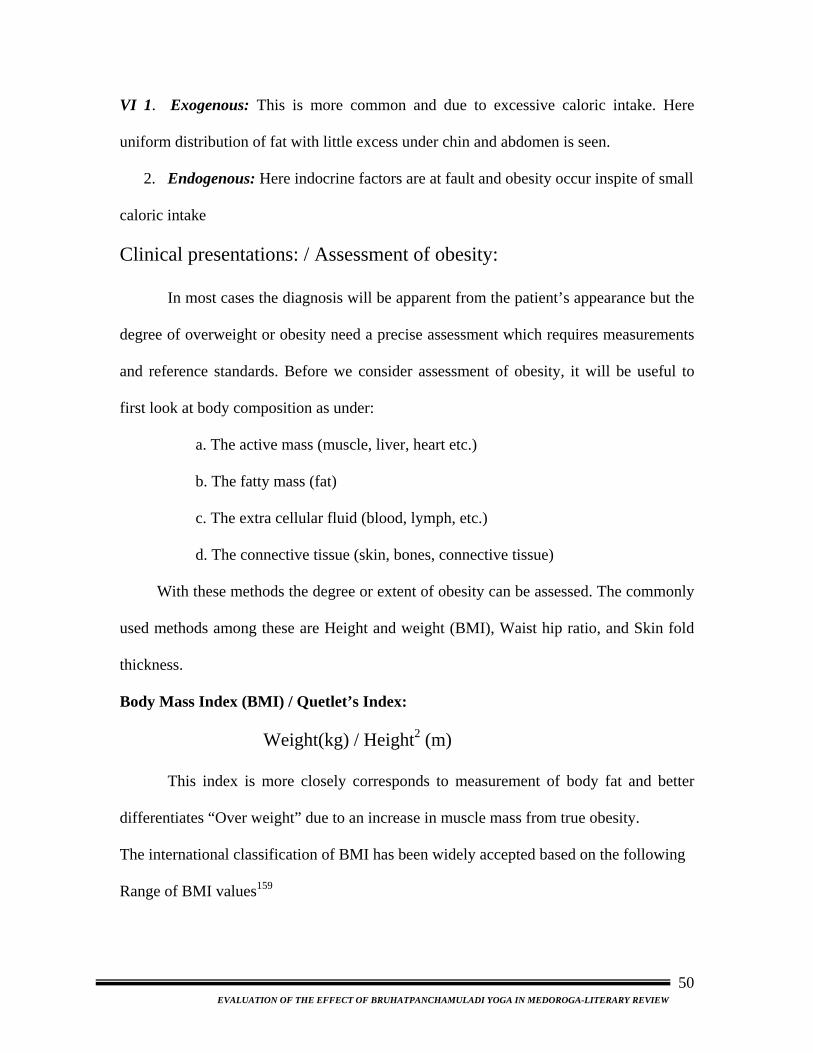
VI 1. Exogenous: This is more common and due to excessive caloric intake. Here
uniform distribution of fat with little excess under chin and abdomen is seen.
2. Endogenous: Here indocrine factors are at fault and obesity occur inspite of small
caloric intake
Clinical presentations: / Assessment of obesity:
In most cases the diagnosis will be apparent from the patient’s appearance but the
degree of overweight or obesity need a precise assessment which requires measurements
and reference standards. Before we consider assessment of obesity, it will be useful to
first look at body composition as under:
a. The active mass (muscle, liver, heart etc.)
b. The fatty mass (fat)
c. The extra cellular fluid (blood, lymph, etc.)
d. The connective tissue (skin, bones, connective tissue)
With these methods the degree or extent of obesity can be assessed. The commonly
used methods among these are Height and weight (BMI), Waist hip ratio, and Skin fold
thickness.
Body Mass Index (BMI) / Quetlet’s Index:
Weight(kg) / Height2 (m)
This index is more closely corresponds to measurement of body fat and better
differentiates “Over weight” due to an increase in muscle mass from true obesity.
The international classification of BMI has been widely accepted based on the following Range of BMI values159
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
50
Table no.12. showing Grading Pattern as per BMI values
Table no.11.showing Methods of Estimating Body fat and its distribution158
Skin fold thickness: Several varieties of calipers (e.g. Harpenden’s skin calipers) are
available for the purpose160
Normally most of the adipose tissue is in sub cutaneous
layer, is in sub cutaneous layer, the thickness of which
can estimate by measuring a skinfold thickness at
Terminology BMI Underweight Below 20Kg/m2
Normal 20-25 Kg/m2
Over weight 25-30 Kg/m2
Obese 30-40 Kg/m2
Very obese Above 40 Kg/m2
S.L.No Method Easy of use Accuracy Measures regional fat
1 Height and Weight (BMI) Easy High No
2 Skin folds Easy Low Yes
3 Circumferences (WH Ratio) Easy Moderate Yes
4 Ultrasound Moderate Moderate Yes
5 Density Immersion
Moderate difficult
High
No
6
Heavy water Tritiated Deuteriumonide or heavy oxygen
Moderate Moderate
High High
No No
7 Potassium isotope (40K) Difficult High No
8 Total-body electric moderate Conductivity
Moderate High No
9 Bio- electric impedance Easy High No
10 Fat-soluble Gas absorptiometry
Difficult High No
11 Computed tomography Difficult High Yes
12 Magnetic resonance imaging Difficult High Yes
13 Neuton activation Difficult High No
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
51
different sub cutaneous sites. Sites for taking measurements:
• Mid triceps
• Mid biceps
• Supra iliac regions
• Sub scapular
The sum of measurements should be less than 40 mm in males and 50mm in
females. Unfortunately standards for subcutaneous fat do not exist for comparison.
Further, in extreme obese, measurement may be impossible. The main draw back of skin
fold thickness measurement is their poor repeatability.
Body girth measurements: WHR:161
The measurement of body circumferences with a tape measure provides the
same advantages of portability and acceptability as height weight measurements. In
addition circumference measurement appears to be more precise and less subject to inter
observer errors than skin fold measurement even in very obese persons. Although they
have found their biggest use in the estimation of body fat distribution.
Some studies have shown that, both men and women, who have a high ratio of
waist to hip circumference, have increased risk of ischemic heart disease, stroke and
death. Studies have shown that a greater WHR ratio is associated with higher blood
pressure, glucose intolerance and higher serum lipid levels.
To check for abdominal obesity one measures the waist hip ratio this is given by,
Waist circumference (in cms)
Hip circumference (in cms)
The waist circumference is usually measured half –way between the superior iliac
crest and the rib cage in the mid axillary line, where as the hip circumference is measured
one third of the distance between the superior iliac spine and the patella.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
52
The ratio of the former to the later provides an index of the proportion of intra abdominal
fat.
The average value for men is about 0.93 with range 0.75 to 1.10
For women 0.83 Range 0.70 to 1.0
The other may be called as abdominal gluteal ratio or android gynoid ratio
(AGR). Patients with an elevated AGR i.g.greater than 0.9 for men and 0.8 for women
are said to have android or male pattern of obesity, while patients with low AGR are said
to have gynoid or female pattern of obesity. The persons with abdominal obesity are a
greater risk of cardio vascular complications than with gluteal obesity.
Complications of obesity: 162,163,164.
Obesity is termed as the storehouse of diseases as well as leading cause of
morbidity and mortality due to its manifold complications. Statistics on health shows that
a middle aged person who is 10kg over weight can expect to die roughly 4 years earlier
then one with normal weight Obese women are more likely than non-obese women to die
from cancer of the gall bladder, breast, uterus, cervix or ovaries. We can classify the
complication related to obesity according to various systems as follows:
Cardio Vascular System: Essential hypertension, coronary artery disease, left ventricular
hypertrophy, corpulmonale; this obesity is mainly associated with cardiomyopathy, and
pulmonary hypertension of obesity, cardiac arrythmias and atherosclerosis.
Respiratory systems: Chronic bronchitis, Hypoxemia, Alveolar Hypoventilation,
Hypoventilation syndrome (Pickwickian syndrome), Pulmonary Hypertension,
Pulmonary embolism, Obstructive sleep apnoea.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
53

Gastro intestinal system: Gall Stone, Hiatus Hernia, Cholecystitis, Pancreatitis, Hepatic
Stenosis, Diverticulosis of colon, Reflux Oesophagitis, Dyspepsia.
Central nervous system: Stroke, idiopathic intracranial hypertension, neuralgia
paresthesia.
Malignancies: Associated with endometria’s, prostate, gall bladder, breast, colon and
possibly lung cancer.
Musculo skeletal: Osteo arthritis, Back ache.
Endocrine and metabolic: Diabetes Mellitus, Hyper lipidaemia, Hypo metabolic State,
Hyper Cholesteraemia. , Fatty liver, Gout, Polycystic Ovarian Syndro
Miscellaneous: Reduced mobility, difficulty maintaining personal hygiene.
Risk classification algorithm165 The patient is first placed into a category based on body mass index. The presence or
absence of complicating factors determines the degree of health risk. Complicating
factors include elevated abdominal-gluteal ratio.
Figure no. 07. Showing risk classification algorithm.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
54
Treatment of Obesity:
Prevention: “Prevention is better than cure”
Prevention should begin in early childhood. Obesity is harder to treat in adult than
it is in children. This can be achieved by dietary changes, increased physical activity and
a combination of both.
The modern authors have narrated the treatment of obesity in following headings,
• Counseling of the Patient.
• Diet Therapy
• Behavioral Modification
• Exercise Therapy
• Drug Therapy
• Surgical
Counseling of patient: Patient counseling has utmost importance in the management of
obesity. Detail knowledge of the disease including cause and treatment need to be
explained in front of an obese person. Emphasis should be laid upon fat reduction rather
than weight loses. Patients must be made aware of the role of diet in accelerating weight
loss.
At the same time, patients must be disposed with confident opinion concerning
the successful out come of the prescribed programs as well as importance of gradual
weight loss instead of drastic. The weight loss will be very rapid in early period of dieting
and then gradual. This should be explained to the patients to avoid disappointment
Diet Therapy: 166 Caloric restrictions are the corner stone of weight reduction. If food
intake is less than energy expenditure, stored calories predominately in the form of fat
will be consumed. For any considering a weight- reducing diet, the quantity of food
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
55

intake and the avoidance of settings in which excess quantities of high fat food are eaten
are equally important. Controlling food intake is easier if the use of alcoholic beverages
is reduced or eliminated. People who eat breakfast have a lower risk of developing
obesity than the individuals who do not. Ingestion of frequent small meals with relatively
high carbohydrate and high fiber content is a way of decreasing fat intake.
While planning diet for an obese patient caloric intake should be reduced by 500
to 1500 calories per day from the current level and perfect aim should be fixed. Middle
aged obese house wife need 800 to 1000 kcal per day where as an obese man engaged in
active physical work, need 1500 to 2000 kcal per day. Rigid dieting is best treatment.
(LCD) 800 to 900 calories/day is best to reduce the weight. But it must contain all the
essential foodstuffs. Diet lower than 800 kcal/day (VLCD) have been found to be no
more effective than low caloric diets in producing weight loss on a long term basis.
The diet should contain – protein 50gm, carbohydrate 100 gm, fat 40gm, vitamin
A and C, minerals like iron and calcium, fluids and salts.
Planned Diet Rules:
• Eat when your are hungry
• Diet should contain liberal amount of salad, fresh fruits and vegetables and
dietary fibers.
• Daily required calorie should not less than 500 kcal.
• Reduce the amount of sugar and salt.
• Calorie Requirement should be adjusted with type of physical activity
• A chart of dietary calorie value is given below, which will be very helpful in
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
56

planning diet schedule for an obese person. (All valves are as per 100gms.of edible
portion)
Contra Indications: There are several categories of subjects in whom VLCD and LCDs
are contra indicated (absolutely or relatively), these include pregnant women,
adolescents, growing children and patients with significant liver, kidney and cardiac
diseases. In addition there are some conditions while, it should only be used under
medical supervision e.g. gout, diabetic patients taking insulin or hypoglycemic agents,
pre existing gall bladder disease and hypertensive patients on antihypertensive drugs.
Starvation: 167 Fasting as a method of treatment offers advantage of dramatic drop in
weight within one week of treatment and this may be of psychological benefit total
starvation for about 5-10 days prior to more conventional dietary therapy may be justified
in selected cases, like provided gout, renal insufficiency and ketosis prone diabetes are
not present Probably the major usefulness of total fasting is as motivational aid at the
beginning of dietary programme or when weight loss has stopped. The major problem in
the treatment of obesity is not weight reduction but maintenance of reduced weight.
Obesity is an eating disorder, and limiting food intake does not reverse the underlying
mechanisms.
Behavioral modification: 168 the principles of behavior modification provide the
underpinnings for many current programs of weight reduction. The basic principles are
those of operant conditioning and cognitive restructuring. Eating behavior is analyzed
into its antecedents, the act of eating, and the consequences of eating by asking the
patient to monitor and record these activities.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
57
The setting in which eating occurs, the eating event itself and the use of rewards
designed to change maladaptive behaviors are all monitored. Attempt are made to change
thinking patterns from negative once such as “I have just eaten a piece of cake, I am bad
person” into “I have just eaten a piece of cake and now I need to go exercise” or other
positive ways of solving the problem. Features of behavior modification of proven value
in people who are successful in maintaining the weight loss over an extended period of
time include:
• Continued monitoring of food related behaviors,
• Adoption of a low – fat diet, and
• Increased levels of physical activity.
Exercise therapy:169 Promotion of increased physical activity, which can be maintained
in the long term. Such exercises need not be over strenuous because health gain is
achieved at modest levels of exercise, as long as these are maintained. Walking briskly
for 30mins each day can result in an additional weight loss of 1kg per month.
Drug therapy:171 The goal of anti obesity drug is to include and maintain the state of
negative energy balance until the desired weight loss is achieved. Appetite suppressants
drugs are useful in this condition. These are two groups of drugs are available: namely,
those affecting the hypothalamic catecholaminergic pathway (e.g. amphetamine,
diethylepropion, phentermine and amino) and those affecting the hypothalamic
serotinergic system (fenfluramine, dexfenfluramine).
Two new drugs are available. Orlistat (seeEBM panel) inhibit pancreatic and
gastric lipases and thereby decreases the hydrolysis of ingested triglycerides. This
produces a 30% reduction in dietary fat absorption, which can contribute to a caloric
deficit of about 0.8 MJ (200) per 24hours.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
58
The second drug is sibutramine, which reduces food intake through beta -1 -
adrenoceptor and 5-HT receptor agonist activity. Metabolic rate may also be enhanced
via stimulation of peripheral beta-3 adreno receptors. Weight loss achieved with this
agent is 3-5 kg better than placebo with 6 months’ therapy and is associated with an
improvement in lipid profile.
Thyroid replacement therapy should only be used in the obese person when there
is definite biochemical evidence of hypothyroidism.
Is it possible to develop vaccine against obesity?:170
In what could become a new weapon in the battle of the bulge, scientists have had
initial success with an experimental vaccine for obesity.
The researchers have found that when they gave rats a vaccine against a hunger
hormone called ghrelin, the animals were able to live the dream of eating what they
wanted without packing on body fat.
The finding, published online by the proceedings of the national academy of
sciences, suggests a whole new approach to weight loss.
It is a long way however, from success in rats to similar results in people. more
research in animals and more data on safety will be needed before an obesity vaccine is
widely tested in humans, according to Dr. Kim Janda of the Scripps research institute in
lajolla California.
One of the next step to see whether ghrelin vaccination helps already obese
rodents shed ponds, Dr. Janda said, if a vaccine were to become a reality for humans, it
would be aimed at those obese individuals who continually “YO-YO” though diet &
exercise, he noted.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
59
Secreted primarily by the stomach, ghrelin is one of the hormones that help to
regulate appetite, metabolism & weight.
Surgical management:172 Surgical treatment is advised for the morbidly obese persons
with 100% weight above the weight for height standards and who are failed to loss their
weight by other means. This treatment can be performed in 3 categories, they are,
• Excision effect: This not a very practical form of surgery and the obese
individual is exposed to the risk of anesthesia, surgery and poor wound healing.
• Surgery to cause malabsorption: This includes jejuno ileal bypass surgery.
Where the upper jejunum is divided, the distal end is closed and the proximal end
is anatomized either end to side or end to end to the distal ileum. Decreased
absorption of nutrients results in diarrhoea and long term metabolic complication
• Operation to restrict the food intake: Both gastric bypass and gastroplasty or
gastric reduction operations, in which a new stomach is surgically constructed
from the upper part of the normal stomach. This procedure produces a sense of
fullness and helps the obese to stop eating. Obstruction to food intake can also be
achieved by wiring the jaw together.
Baratric surgery:173 These are 5 surgical methods of obesity,
• An adjustable gastric band.
• Vertical banded gastroplasty.
• A biliopancreatic bypass.
• A Rouse – en – y gastric bypass.
• A sleeve gastroctomy with duodenal swith.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-LITERARY REVIEW
60
VASTI REVIEW Nirukti:
The word ‘Vasti’ is derived from the root “Vas + Cit”.
‘Vasu – nivase’ means to reside.
‘Vas – Achadane’ means to cover or wrap.
‘Vas – Vasane’ – Surabhikarane – to give fragrance.
‘Vasti – Vaste avrunoti mutram’ that which covers the urine.
‘Vasti nabhir adho bhaga sthane’ – vasti is the reservoir of urine in the body and it is
situated in the sub umbilical area.
In the context of Panchakarma the term vasti is used in a different sence,
1)‘Vastina deeyate iti vasti’.174
2)‘Vastibhirdeeyate yasmat tasmat vastiriti smruta’.175
3)‘Vastina deeyate, vastim va purvamanvetyato vasti’.176
The term vasti means bladder.The bladders of animals were used as the device for
vasti karma in olden days.It is also said that medicine administered through the vasti
yantra, first reaches the lower abdominal area of the patient which contains the organ
vasti(urinary bladder).
Importance of Vasti karma:
• Charaka and Vagbhata have described vasti as ardha chikitsa.
• Vasti alone can cure many disorders.
• Multiple combinations are possible.
EVALUATION OF THE EFFECT OF THE BRUHATPANCHAMULADI YOGA IN MEDOROGA-VASTI REVIEW
61
• Used in infectious, immunological, autoimmune, degenerative, inflammatory,
infertility, metabolic and endocrine disorders.
• Prevents recurrence.
• Used from pediatrics to geriatrics (used in all 8 branches of Ayurveda).
• Used in shakhagata, tiryakgata and koshthagata rogas.
• Specific therapeutic effects like chakshushya are also possible.
Significance of Vastikarma:
All the texts in Ayurveda accept and talk high about vasti and its significance.
Large intestine is the main seat of Vata.Vata is a catalyst(yogavahi) which controls all
neurological activities.It controls dormant pitta and kapha and makes them active.
Anabolism and catabolism depends up on the normal physiological activities of the vata.
Agni the central factor of health and ill-health is also regulated and maintained by the
rhythm of vata. Vasti is the treatment which is applied directly to the main seat ofvata.177
When compaired with other therapeutic procedures like vamana, virechana etc.,
vasti has got multidimentional therapeutic effect.We can achieve brumhana, shamana,
shodhana, rasayana, vajikarana and any other desired therapeutic effect by vasti.
It might be the reason why Kashyapa equated vastikarma as ‘Amrutam’ (nector)
due to its wide application even in infants and aged.178
Classification of Vastikarma:
In Ayurveda, wide scope of vasti therapy is covered by many varieties of Vastis
that can be applied in different states. The following classification of vasti may highlight
this fact.
EVALUATION OF THE EFFECT OF THE BRUHATPANCHAMULADI YOGA IN MEDOROGA-VASTI REVIEW
62
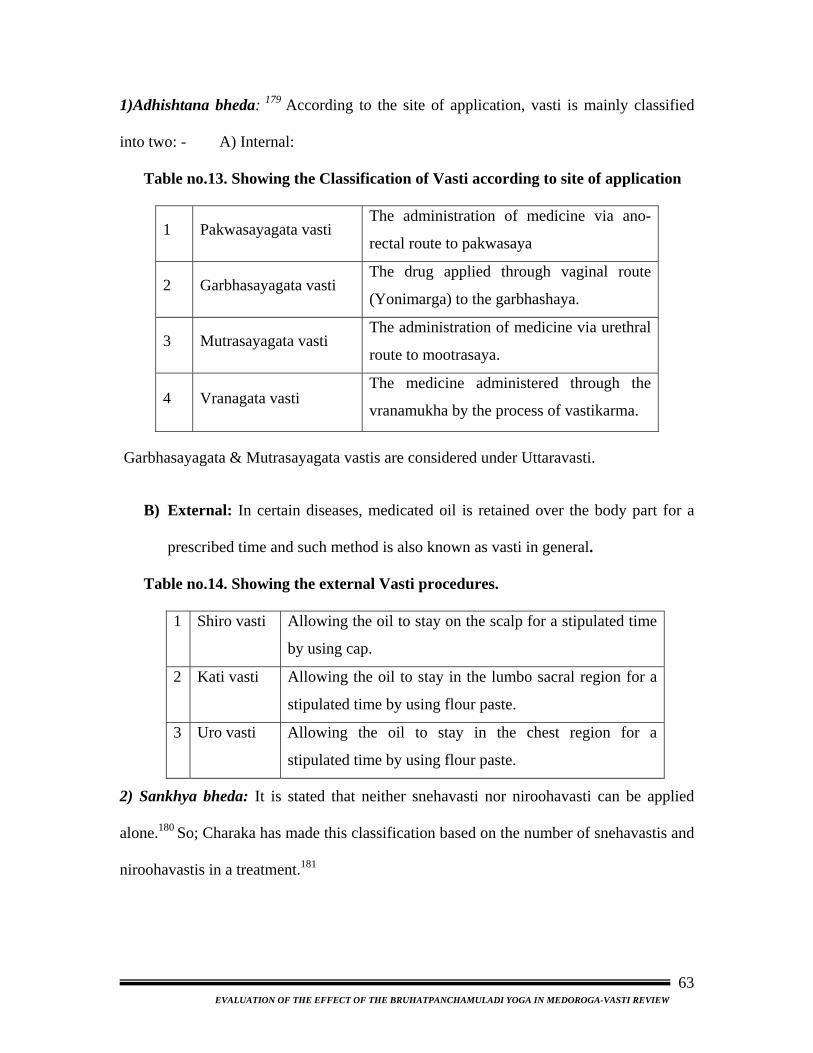
1)Adhishtana bheda: 179 According to the site of application, vasti is mainly classified
into two: - A) Internal:
Table no.13. Showing the Classification of Vasti according to site of application
1 Pakwasayagata vasti The administration of medicine via ano-
rectal route to pakwasaya
2 Garbhasayagata vasti The drug applied through vaginal route
(Yonimarga) to the garbhashaya.
3 Mutrasayagata vasti The administration of medicine via urethral
route to mootrasaya.
4 Vranagata vasti The medicine administered through the
vranamukha by the process of vastikarma.
Garbhasayagata & Mutrasayagata vastis are considered under Uttaravasti.
B) External: In certain diseases, medicated oil is retained over the body part for a
prescribed time and such method is also known as vasti in general.
Table no.14. Showing the external Vasti procedures.
1 Shiro vasti Allowing the oil to stay on the scalp for a stipulated time
by using cap.
2 Kati vasti Allowing the oil to stay in the lumbo sacral region for a
stipulated time by using flour paste.
3 Uro vasti Allowing the oil to stay in the chest region for a
stipulated time by using flour paste.
2) Sankhya bheda: It is stated that neither snehavasti nor niroohavasti can be applied
alone.180 So; Charaka has made this classification based on the number of snehavastis and
niroohavastis in a treatment.181
EVALUATION OF THE EFFECT OF THE BRUHATPANCHAMULADI YOGA IN MEDOROGA-VASTI REVIEW
63
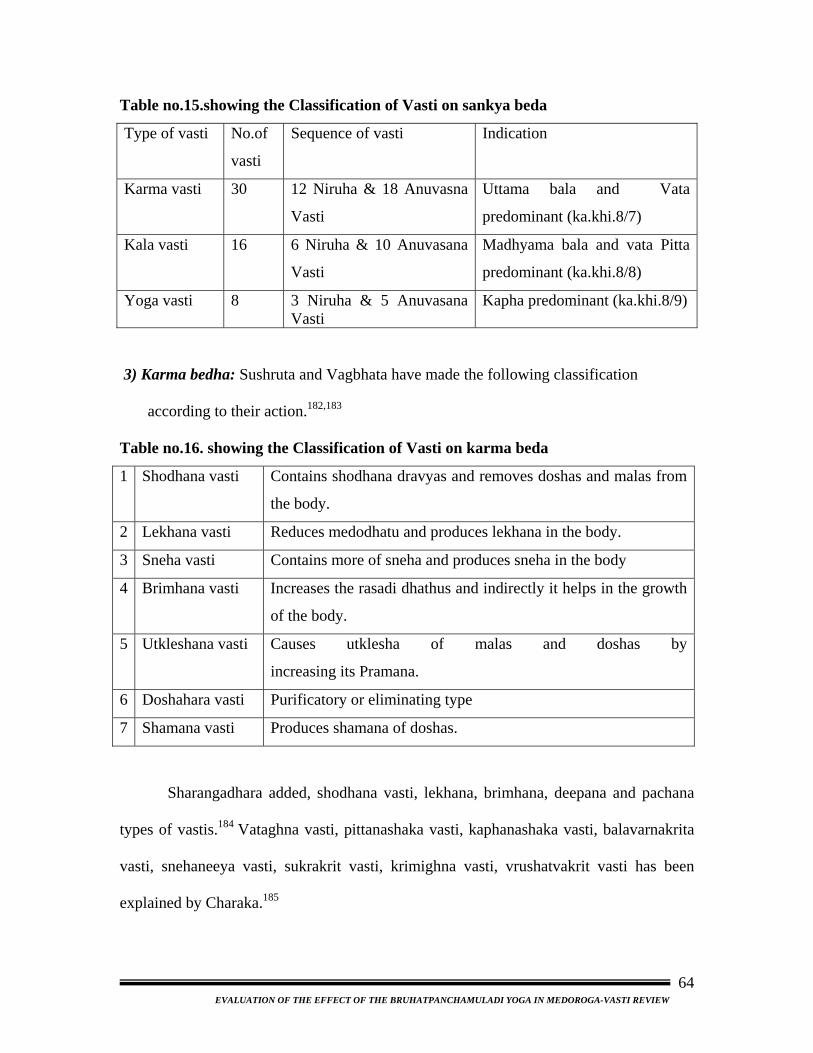
Table no.15.showing the Classification of Vasti on sankya beda
Type of vasti No.of
vasti
Sequence of vasti Indication
Karma vasti 30 12 Niruha & 18 Anuvasna
Vasti
Uttama bala and Vata
predominant (ka.khi.8/7)
Kala vasti 16 6 Niruha & 10 Anuvasana
Vasti
Madhyama bala and vata Pitta
predominant (ka.khi.8/8)
Yoga vasti 8 3 Niruha & 5 Anuvasana Vasti
Kapha predominant (ka.khi.8/9)
3) Karma bedha: Sushruta and Vagbhata have made the following classification
according to their action.182,183
Table no.16. showing the Classification of Vasti on karma beda
1 Shodhana vasti Contains shodhana dravyas and removes doshas and malas from
the body.
2 Lekhana vasti Reduces medodhatu and produces lekhana in the body.
3 Sneha vasti Contains more of sneha and produces sneha in the body
4 Brimhana vasti Increases the rasadi dhathus and indirectly it helps in the growth
of the body.
5 Utkleshana vasti Causes utklesha of malas and doshas by
increasing its Pramana.
6 Doshahara vasti Purificatory or eliminating type
7 Shamana vasti Produces shamana of doshas.
Sharangadhara added, shodhana vasti, lekhana, brimhana, deepana and pachana
types of vastis.184 Vataghna vasti, pittanashaka vasti, kaphanashaka vasti, balavarnakrita
vasti, snehaneeya vasti, sukrakrit vasti, krimighna vasti, vrushatvakrit vasti has been
explained by Charaka.185
EVALUATION OF THE EFFECT OF THE BRUHATPANCHAMULADI YOGA IN MEDOROGA-VASTI REVIEW
64
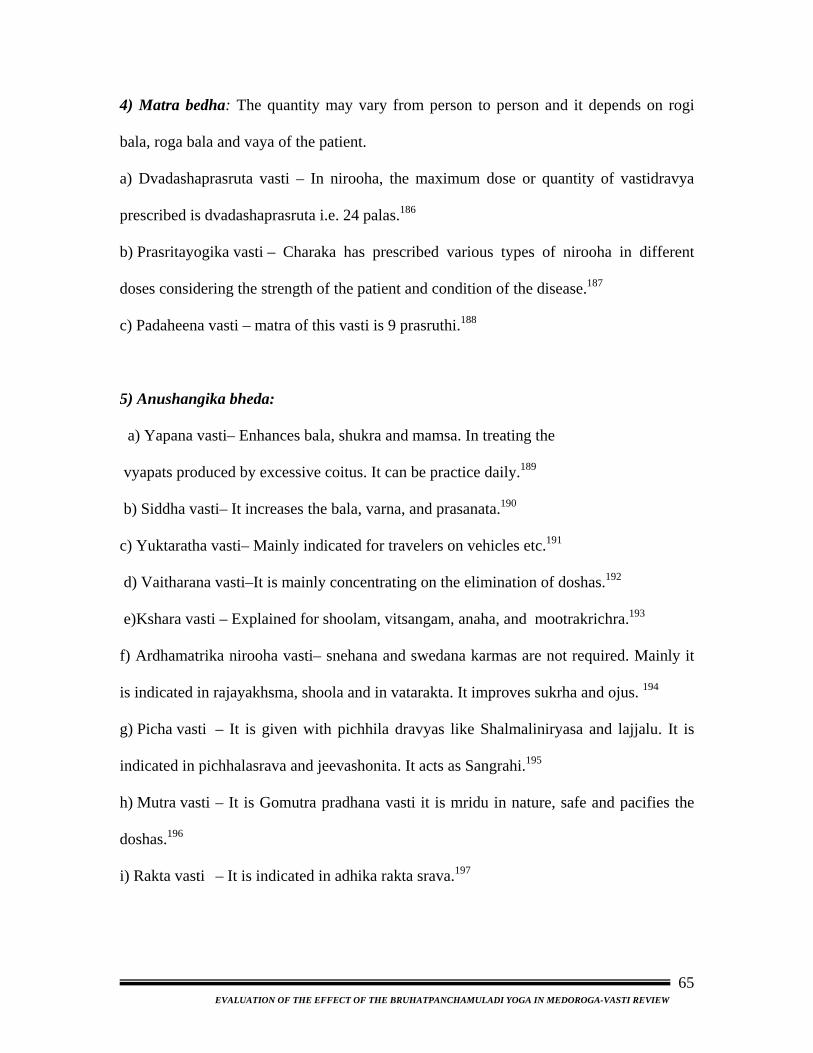
4) Matra bedha: The quantity may vary from person to person and it depends on rogi
bala, roga bala and vaya of the patient.
a) Dvadashaprasruta vasti – In nirooha, the maximum dose or quantity of vastidravya
prescribed is dvadashaprasruta i.e. 24 palas.186
b) Prasritayogika vasti – Charaka has prescribed various types of nirooha in different
doses considering the strength of the patient and condition of the disease.187
c) Padaheena vasti – matra of this vasti is 9 prasruthi.188
5) Anushangika bheda:
a) Yapana vasti– Enhances bala, shukra and mamsa. In treating the
vyapats produced by excessive coitus. It can be practice daily.189
b) Siddha vasti– It increases the bala, varna, and prasanata.190
c) Yuktaratha vasti– Mainly indicated for travelers on vehicles etc.191
d) Vaitharana vasti–It is mainly concentrating on the elimination of doshas.192
e)Kshara vasti – Explained for shoolam, vitsangam, anaha, and mootrakrichra.193
f) Ardhamatrika nirooha vasti– snehana and swedana karmas are not required. Mainly it
is indicated in rajayakhsma, shoola and in vatarakta. It improves sukrha and ojus. 194
g) Picha vasti – It is given with pichhila dravyas like Shalmaliniryasa and lajjalu. It is
indicated in pichhalasrava and jeevashonita. It acts as Sangrahi.195
h) Mutra vasti – It is Gomutra pradhana vasti it is mridu in nature, safe and pacifies the
doshas.196
i) Rakta vasti – It is indicated in adhika rakta srava.197
EVALUATION OF THE EFFECT OF THE BRUHATPANCHAMULADI YOGA IN MEDOROGA-VASTI REVIEW
65
6) Dravya bheda:198 Depending up on the nature of Vasti drugs i.e. Kashaya and Sneha
the Vasti is mainly sub-classified as
• Anuvasana Vasti.
• Niruha Vasti
Yoga vasti:
In this group, there are totally eight vastis, which include five anuvasana vastis
and three niruha vastis. As Kashyapa explained in khila sthana chap. 8, It is indicated in
Kapha – involved diseases.
In yogavasti, the number of anuvasana vasti are less when compared to other
types of vastikarma and so it is laghu. Hence, this type of vasti is indicated in kaphaja
diseases and minor vataja diseases.
EVALUATION OF THE EFFECT OF THE BRUHATPANCHAMULADI YOGA IN MEDOROGA-VASTI REVIEW
66

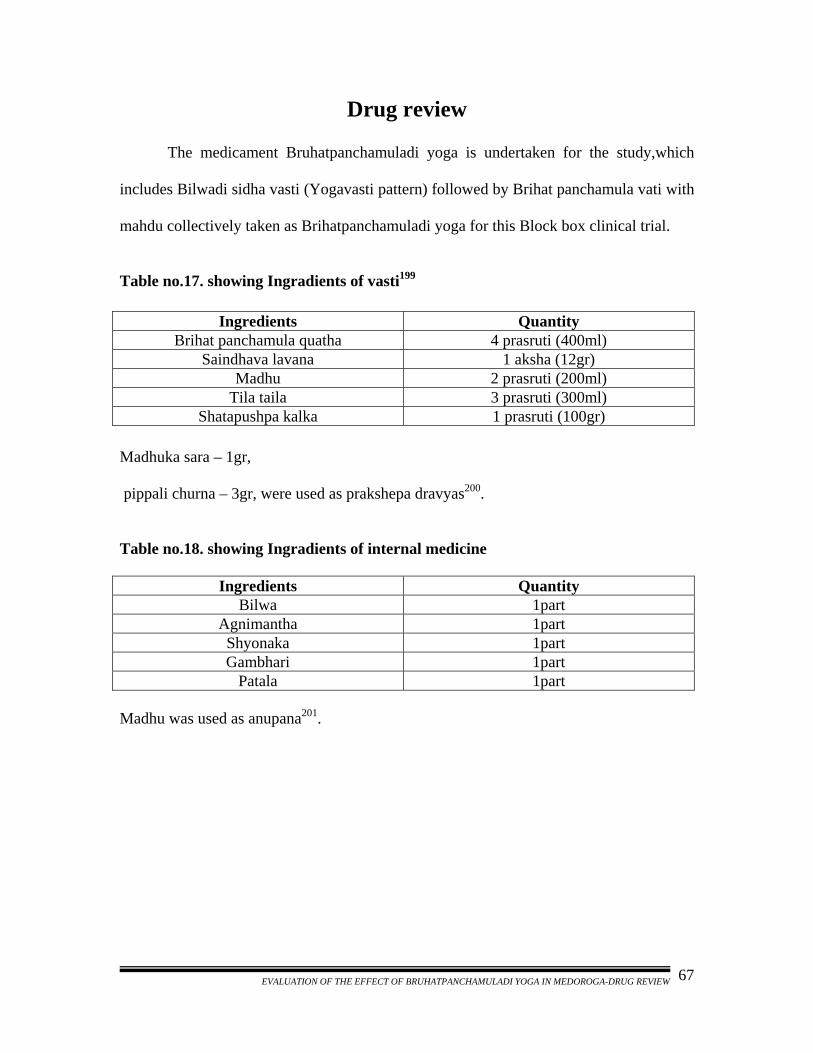
Drug review
The medicament Bruhatpanchamuladi yoga is undertaken for the study,which
includes Bilwadi sidha vasti (Yogavasti pattern) followed by Brihat panchamula vati with
mahdu collectively taken as Brihatpanchamuladi yoga for this Block box clinical trial.
Table no.17. showing Ingradients of vasti199
Ingredients Quantity
Brihat panchamula quatha 4 prasruti (400ml) Saindhava lavana 1 aksha (12gr)
Madhu 2 prasruti (200ml) Tila taila 3 prasruti (300ml)
Shatapushpa kalka 1 prasruti (100gr) Madhuka sara – 1gr,
pippali churna – 3gr, were used as prakshepa dravyas200.
Table no.18. showing Ingradients of internal medicine
Ingredients Quantity Bilwa 1part
Agnimantha 1part Shyonaka 1part Gambhari 1part
Patala 1part Madhu was used as anupana201. EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DRUG REVIEW
67
1) Bilwa: 202,203
Latin name: Aegel marmelos Gana : Cha - Shothahara,Arshoghna,Aasthapanopaga,Anuvasanopaga Su - Brihat panchamula,Varunadi,Ambhasthadi Vag - Varunadi Ambhasthadi Kula : Jambeera kula Family : Rutaceae Synonyms: :
Bilwa,Shandilya,Shailusha,Shreephala,Malura,Gandhagarbha,Kantaki,Sadaphala,Maha
kapitha,Granthila
Habitat : Found almost throughout India
Varieties : Graamya and Vanya
Botanical description: It is a medium to fairly large sized deciduous and glabrous tree
up to 6 – 7.5 mt. high and 90 – 120 cm. in girth
Properties: Rasa - Kashaya and tikta
Guna - Laghu and ruksha
Vipaka - Katu .
Veerya - Ushna
Mula - Vatanadi samsthana shaamaka, madhura, chardighna, vatahara204.
Parts used: Root, leaves and fruits Major chemical constituents: (Root):
Xanthotoxin, Umbelliferone, Marmesin, Marmin, Skimnin etc.
Dosha karma: Kapha vata shamaka Indications : Atisara,grahani,prameha,shotha,agnimandhya,etc.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DRUG REVIEW
68
2) Agnimantha205, 206: Latin name: Premna mucronata
Gana : Cha - Shothahara, Sheetaprashamana, Anuvasanopaga
Su - Veeratarvadi, Varunadi, Vatasamshamana
Vag - Veeratarvadi, Varunadi
Kula : Nirgundi kula Family : Verbinaceae Synonyms: Agnimantha, Jaya, Shreeparna, Ganikarika, Vaataghni Habitat : Found in the forest of south India and West Bengol, Uttarpradesh and Bihar
Varieties : Brihadagnimantha and kshudragnimantha Botanical description: A large shrub or small tree, short trunk, branches numerous,
often procumbent and rooting. Bark smooth, leaves dark brown, opposite, chordate,
errate, and flowers minute, numerous. Berries black, pea-sized
Properties: Rasa - Tikta,katu,kashaya madhura
Guna - Ruksha,laghu
Vipaka - Katu
Veerya - Ushna
Parts used: Root bark and leaves
Major chemical constituents: Aphelandrine, premnine, betulin, ganiarine, ganikarine,
caryophellen, premnenol and premnaspirodiene.
Doshakarma : Kapha vata shamaka.
Indications : Shotha, pandu, vasameha, sheetapitta, udara, kotha, sthoulya
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DRUG REVIEW
69
3) Shyonaka207,208: Latin name: Oroxylum Indicum Gana : Cha - Shothahara,Sheetaprashamana,Anuvasanopaga Su - Rodhradi,Veeratarvadi,Brihatpanchamula Vag - Rodhradi,Veeratarvadi Kula : Shyonaka kula Family : Bignonaceae Synonyms: Shyonaka, Tuntuka, Kutannata, Bhalluka, Pruthushimba, Arishimbi,
Katvanga, Deerghavranka, Mandukaparna, Shukanasha, Mayurajangha.
Habitat: Found in the warmer parts of the India (up to 4000 ft. height), also cultivated as
an avenue tree
Varieties: Katvanga and Shyonaka209
Botanical description: Small deciduous or medium sized tree up to 12 meters in height,
with few branches, small crown, wood (wt.480 Kg./Cu.m.) yellowish-white and soft
Properties: Guna – Laghu and Ruksha
Rasa – Madhura, Tikta, Kashaya
Vipaka – Katu
Veerya – Ushna
Parts used: Root bark Major chemical constituents: Stem and root bark contains three flavour colouring
matters which are Orozyline A, bioicalcin, chrysin
Doshakarma : Kaphavata shamaka Indications : Amavata,atisara,aruchi,kasa,basti vikara,vataroga and shotha. EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DRUG REVIEW
70
4) Gambhari210,211: Latin name: Gmelina arborea. Gana : Cha - Shothahara,Dahaprashamana,Virechanopaga Su - Sarivadi,Brihatppanchamula Vag - Sarivadi Kula : Nirgundi kula Family : Verbinaceae Synonyms: Gambhari, shreeparni, madhuparni, kashmari, peetarohini, kashmeeri Habitat : Found throughout Deccan peninsula Varieties: According to bhavaprakash nighantu two types, one with big pushpavyuha,
another with small pushpavyuha212
Botanical description: A moderate sized unarmed deciduous tree, reaching 18 meters
height, bark grayish yellow, rather corky. Branch lets and young parts clothed with fine
white mealy pubescent
Properties: Guna – Guru
Rasa – Tikta, kashaya, madhura
Vipaka – Katu
Veerya – Ushna
Parts used: Root, root bark, bark, fruits, flowers, leaves Major chemical constituents: Roots contain yellow thick oil, resin, an alkaloid, and
little Benzoic acid. Fruits contain butyric and sugar, tannin
Doshaghnata: Tridoshashamaka Indications : Bhrama, shotha,trushna, amashula, arsha, visharoga, daha and jwara.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DRUG REVIEW
71
5) Patala213,214: Latin name: Sterrosprmum Sauvealens Gana : Cha – Shothahara, Su – Aragwadhadi,Brihatpanchamula,adhobhagahara, Vag – Aragwadhadi Kula : Shyonaka Kula, Family : Bignonaceae Synonyms: Patala, krushnavrunta, madhuduti, alivallabha, tamrapushpi, kuberakshi,
amogha, Kumbhipushpi, ambuvasini
Habitat: North circa and Decan in deciduous forests, western ghats, in the hills of
Mysore, Malabarand Travancore, scarces
Varieties: Raktapushpa and Shetapushpa215
Botanical description: Tree 9-18 meters tall, large and deciduous, 1.8m.in girth, with a
clear hole of C.9 m. Bark grey or dark brown, with horizontal furrows, exfoliating in
large, flat scales
Properties: Guna – Laghu and ruksha , Rasa – Tikta,kashaya,
Veerya – Ushna, Vipaka – Katu
Parts used: Root bark, flower, seed, leaves, kshara
Major chemical constituents: The root fat is made up of palmitic, stiaric and oleic
Acids, ceryl alcohol is also present
Doshaghnata: Tridoshaghna Indications: Aruchi, shwasa, shotha, raktavikara, chardi, hikka, trushna, raktapitta and
sthouly.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DRUG REVIEW
72
6) Pippali216,217:
Latin name: Piper longum Gana : Cha - Deepaneeya, kanthya, asthapanopaga, shirovirechanopaga, sheetaprashamana, shulaprashamana, kasahara, truptaghna Su - Pippalyadi, urdhwabhagahara, tryushana, amalakyadi, Shirovirechanadi Vag - Pippalyadi Kula : Pippali kula Family : Piperaceae Synonyms : Pippali, magadhi, vaidehi, krishna,kanaa, chapala, teeksna tandula,
Ushana, upakulya, shoundi, kola
Habitat : Found in the hotter parts of India, from central Himalaya to Assam, and also
Found in the forests of Western Ghats from konkan to krrala
Verieties : Pippali, Gajapippali, Saihali,Vanapippali218
Botanical description: Slender aromatic climber with perennial woody roots, stems
creeping, young shoots downy, branches prostrate or creeping with broad leaves,
flowering shoots erect, fresh fruits ovoid, yellowish-orange, sunk fleshy spikes and dry
fruits are black.
Properties: Guna – Laghu, snigdha, teekshna Rasa – Katu
Vipaka – Madhura Veerya – Anushnasheeta
Parts used: Fruits and root Major chemical constituents: The dried fruits (on steam distilled) yield 0.7% of an
essential oil with spicy odour resembling that of pepper and ginger oil
Doshaghnata: Kaphavata shamaka
Indications: Udara, pleeharoga, jwara, kushtha, prameha, gulma, arsha, shula, amavata,
kamal, rasayana.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DRUG REVIEW
73
7) Madhuka219: Latin name: Madhuka longifolia \ latifolia. Gana : cha – Pureesha virajaneeya Su – Sarivadi gana Vag – Vidangadi gana. Family : Sapotaceae. Synonyms:
Dolaphala, teekshnasaara, madhuka, gudapushpa, elaphala, madhushteela, altitude.
rodhravruksha, vanavasa, mahadhruma
Habitat : It occurs throughout India up to 4000ft
Varieties: Madhuka and Jalamadhuka220
Botanical description: Large deciduous tree up to 20mt. high,young part pubescent,with
short,stout trunk and dence spreading crown.Bark grey or blakish,with shallow wrinkles
and vertical cracks. Flowers in dense fascide near the ends of branches
Properties: Pushpa221 : Guna – Snigdha,teekshna, vikasi
Rasa – Madhura
Vipaka – Madhura
Veerya – Ushna.
Parts used: Flower, twak and saara Major chemical constituents : Air dried flowers contain invert sugar 52.6%,can sugar
2.2%,albuminoids 2.2%,cellulose 2.4%,ash 4.8%,and aqueous content 15%.In addition
the flowers contain enzymes and yeast with high quantity
Doshaghnata: Vatapitta shamaka221
Indications : Raktapitta, trushna and kshaya.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DRUG REVIEW
74
8) Saindhava lavana222:
This is the best in the lavana varga. Rock salt is the common name for the mineral Halite.
Sanskrit - Saindava, Shitashiva, Manimantha, Sindooja
Hindi - Senda namak
English - Rock salt
Kannda - Saindava
VARGA : Lavana varga
Properties (Guna):
Rasa - Lavana
Guna - Snigdha, Rooksha, Sukshma
Veerya - Sheeta
Karma - Tridoshahara, Rochana, Deepana, Ushna & Teekshna
Indications: Ajeerna, Anaha, Vatavikara, Gulma, Shoola & Udara roga.
9) Madhu223,224:
Rasa - Madhura, Kashaya
Guna - Guru, Ruksha, yogavahi
Veerya - Sheeta
Properties - Grahi, vilekhana, srotoshodhaka, chakshushya, deepana, etc
Indication - kushta, Arsha, Kasa, Meha, Krimi, Meda, shwasa etc
In other words madhu due to its prabhava assumes & magnifies gunas of
whatever dravya is used along with it. Hence madhu is used along with most of the
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DRUG REVIEW
75
aharas & aushadhas which are Kaphamedo and mehahara but madhu should be used in
small quantities otherwise it causes vatavrudhi.
Contents: Alkaloids:
Moisture – 20.6% Pyrolizidine alkaloids
Proteins – 0.3% Jacohne, Jacozine
Carbohydrates – 79.5% Jacobine, seneciphylline
Minerals – 0.2% & senecionine
Calcium – 5%
Phosphorus – 16.0%
Iron - 0.9%
Riboflavin – 0.04%
Niacin – 0.2%
Vit C. - 4.0%
Energy – 319 K cal / 100g
Properties225:
Honey serves as mild laxative, bactericidal, sedative, antiseptic & alkaline
characteristics. It has ingredients which very similar to antibodies. Diet rich in honey is
recommended for infants, Convalescents & diabetic patients. It is generally
recommended as a remedy for cold, cough, fever, sore eyes & throat, tongue and
duodenal ulcers, liver disorders, constipation, diarrhea, kidney and other urinary
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DRUG REVIEW
76
disorders, pulmonary T.B. rickets, marasmus, scurvy and insomnia. It is used as a remedy
on open wounds after surgery. It is reported to prevent infection & promote heating.
Pharmacotherapeutics of honey:-
It has been proposed that honey contains a sucralfate like substance that may be
responsible for its antioxidant property and gastric protection, deterioration in the
processes of lipids peroxidation and rise in the activity of antioxidant system of an
organism.
10) Tila226,227: Latin name : Seasamum indicum
Family : Pedaliaceae
Part used : Beeja
Gana : Svedopaga (ch)
Properties : Guna - guru, sukshma, snigdha sara vikasi, vishada
Rasa - Madhura, Anurasa: kashaya, tikta
Veerya - Usna
Vipaka - Madhura
Dosaghnata - Vata Kaphashamaka
Action: Agnideepaka, lekhana,balakaraka, deepaka, medhya, brimhanakaraka, etc.
Composition: Palmitic acid (9.1%), stearic acid (4.3%), arachidic acid (0.8%), oleic acid
(45.4%), linoleic acid (40.4%).
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DRUG REVIEW
77
11) Shatapushpa228,229: Latin name: Anethum Sowa kurz
Gana : Cha – Asthapanopaga, anuvasanopaga
Kula : Shatapushpakula
Family : Umbelliferae
Synonyms: Atilambi,karavi,misi,madhura,chatra
Habitat : Often cultivated throughout the tropical and sub-tropical India
Verieties : Vanya and gramya
Botanical description: Herb 1-3” highwith pinnately devided leaves, glabrous, branched,
perennial herb; slender, erect, scented herb of green and striated stem.
Properties: Guna – Laghu,ruksha,teekshna.
Rasa – Katu,tikta
Vipaka – Katu
Veerya –Ushna.
Parts used: Fruits, leaves and oil.
Major chemical constituents: Fruits or seed contain oil- carvona, dihydrocarvone,
limovane, apiol, dill-apiol etc,.
Doshakarma : Kaphavata shamaka
Indications : Shula, jwara, netraroga, vruna, gulma, adhmana, yonishula.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DRUG REVIEW
78
Chapter - 4
Methods
The clinical study is based on the classical explanations with scientific well
designed research protocol, which enumerates the patient before to administrate the trial
drug to after effects in comparison.
Methods followed in trail:
1) Method of Research design
The trail is Simple Random sampling technique Block box clinical study. In this
Patients were taken in randomized selection.
2) Posology of Trial drug
Internally: 1500 mg/24hrs in distributed doses of TDS or
25 mg/kg body weight/24hrs.
Yogavasti: As presented in the classical text.
3) Anupana of Trial drug
Madhu is undertaken as it is stipulated for the medicine.
4) Study duration of Trial drug
Brihatpanchamuladi yoga Simple Random sampling technique clinical study was
conducted for 32 days in total divided protocol as under
8 days – Yoga vasti
24 days – internal medicine.
After giving Yogavasti, the internal medicine was dispensed for 7 days to all
patients and advised to report for every 7 days interval, noted the nature, frequency and
other symptoms during their visits.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-METHODS
79
5) Follow up of Trial drug Brihatpanchamuladi yoga trail offered a further follow up
15 days. The effect of yoga was analyzed according to clinical and functional response
before and after the treatment is compared to that of follow up data.
6) Source of data of Trial drug
In spite of this much of prevalence and increasing nature of the disease all over
the world, still researchers are struggling for a good, effective and harmless remedial
measure of thoulya. Diet control, exercise, oral lipolytic agents have tried and treated this
public health threat, Sthoulya. The data was collected from the patients suffering from
Sthoulya in the OPD of post graduation and research center DGM Ayurvedic medical
college Gadag. The method of the present study consists of following headings.
a) selection of the patient
b) examination of the patient
c) criteria of assessment
a) Selection of the patient
Patients of Sthoulya fulfilling the criteria of diagnosis were selected in the present
study. Patients were distributed based on preset inclusion and exclusion criteria. Patients
were excluded, as they are discontinuous at the treatment or unable to fulfill the study
design.
i) Inclusion criteria
Patients with symptoms of Sthoulya are included with classical symptoms
enumerated at the classical texts under the lime light of contemporary medical context
along with criteria of inclusion. The symptoms of inclusion are as under.
• All patients other than that of exclusive criteria are included
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-METHODS
80
• Age of patients between 20-60 years
• Irrespective of gender
• Patient having clinical features of Sthoulya viz.
1) Chala sthana
2) Chala udara
3) Chala sphik.
• Patients with raised BMI as per the WHO standards.
ii) Exclusion criteria
Patients other than inclusion criteria are excluded in the present study. The
specified exclusions are as under.
• Mechanical complications of Sthula– hip and lumbar spine developing
Osteoarthritic changes.
• Cardiovascular complications of Sthula – Angina pectoris, Hypertension,
Cardiac failure.
• Metabolic complications of Sthula – Diabetes, Gout, etc.
• Sthula with secondary causes like endocrinal and C.N.S. diseases.
• Sthula with any other major systemic pathology.
b) Examination of the patient
Patient through examination is necessary to obtain clear picture of disease and
also the effect of trail drug – Brihatpanchamuladi yoga. For that the following methods
are obtained in the study.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-METHODS
81
b-1) Physical signs of Sthula patients –
For diagnosis, a detailed medical history is taken and physical examination also
undertaken in detail according to Ayurvedic and contemporary clinical methods. Patients
are diagnosed according to diagnostic criteria given for Sthulya vis-à-vis Obesity. A
special case sheet is prepared incorporating all Sthoulya aspects, which is placed as
annexure.
b-2) Diagnosis measurements
The signs and symptoms of Sthoulya mentioned in Ayurveda and contemporary
science were the main basis of diagnosis and criteria for assessing the response to the
treatment. Assessments of results were made according to clinical improvement observed
in the study. Clinical assessment was made on the basis of symptoms viz. Chala sthana,
udara and sphik., which are allotted grades according to their severity or to that of
normalcy. The grades are followed as under.
GRADES OF ASSESSMENT
Chala sthana, udara, and sphik
Grade 0 = Absence of chalatva.
Grade 1 = Little visible movements (in the areas) after fast movement
Grade 2 = Little visible movements (in the areas) even after moderate movement
Grade 3 = Movements (in the areas) after mild movement
Grade 4 = Movements (in the areas) even after changing posture.
Grade 4 = continuously noticed
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-METHODS
82
b-3) Assessment measures and Laboratory-investigations
The following investigations are under taken to fulfill the criteria of inclusions
and exclusions. The effective parameters which are considered for the assessment are as
under.
Serum Cholesterol: 230
The Procedure was carried out with Cholesterol kit.
(CHOD-POD Enzymatic End Point Method).
Reagents: Enzymes reagent
Cholesterol standard- 200mg/dl
Test procedure: The reagent and sample were brought to room temperature prior to use.
Pipette intoTest tubes Blank Standard Sample
Reagent 1000ml 1000ml 1000ml
Sample - - 10ml
Standard - 10ml -
Pipettes are mixed gently and incubated for 10 minutes at 370 .
The absorbance of Sample and Standard against blank is measured.
Calculation: Conc. Of cholesterol in test sample (mg/dl ) =
Absorbance of sample Conc. of standard. Absorbance of standard Expected Values: 130 – 250 mg / dl.
Serum Triglycerides:231
The procedure was carried with ENZYMATIC – GPO METHOD principle.
Reagents: Buffered enzyme / chromogen
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-METHODS
83
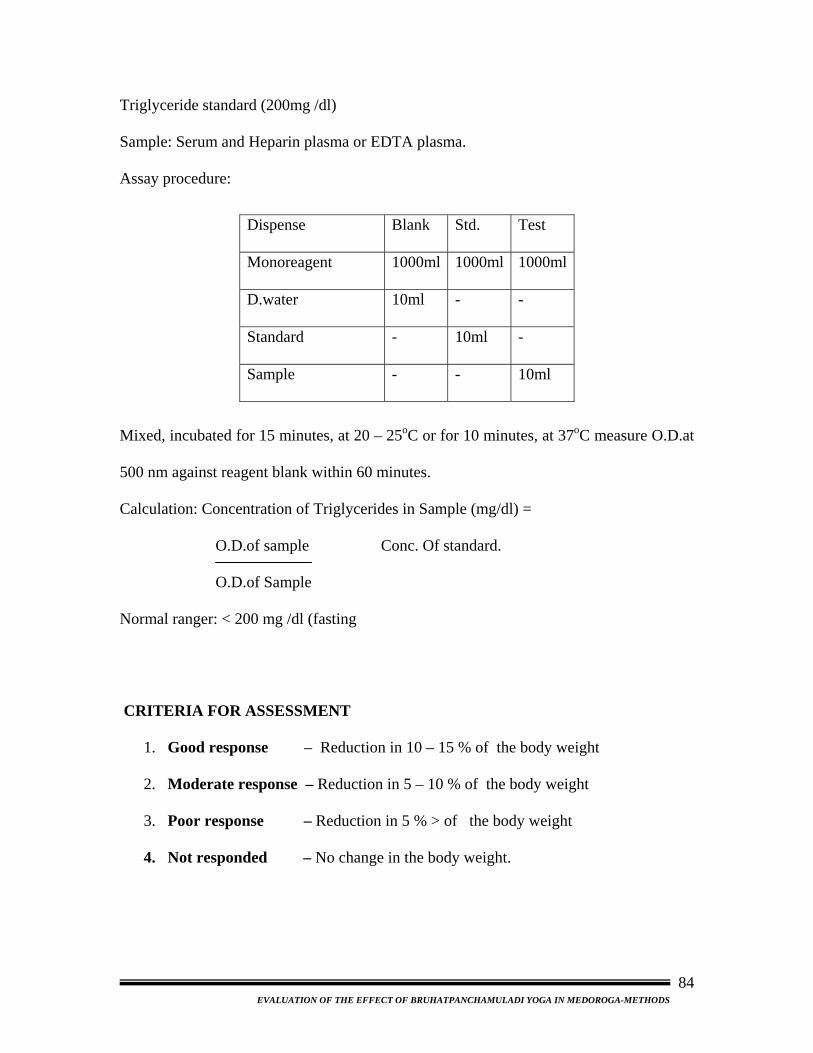
Triglyceride standard (200mg /dl)
Sample: Serum and Heparin plasma or EDTA plasma.
Assay procedure:
Dispense Blank Std. Test
Monoreagent 1000ml 1000ml 1000ml
D.water 10ml - -
Standard - 10ml -
Sample - - 10ml
Mixed, incubated for 15 minutes, at 20 – 25oC or for 10 minutes, at 37oC measure O.D.at
500 nm against reagent blank within 60 minutes.
Calculation: Concentration of Triglycerides in Sample (mg/dl) =
O.D.of sample Conc. Of standard.
O.D.of Sample
Normal ranger: < 200 mg /dl (fasting
CRITERIA FOR ASSESSMENT
1. Good response – Reduction in 10 – 15 % of the body weight
2. Moderate response – Reduction in 5 – 10 % of the body weight
3. Poor response – Reduction in 5 % > of the body weight
4. Not responded – No change in the body weight.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-METHODS
84
Preparation and procedures of vastikarma: Generally these procedures and preparations
are classified into three parts: -
1. Poorvakarma (pre-treatment)
2. Pradhanakarma (treatment)
3. Paschatkarma (post-treatment)
The patients selected for vasti therapy has to undergo through clinical
examinations to ascertain the physical as well as the mental conditions. The following ten
factors are to be considered.
1. Dosha 2.Oushada 3.Desa 4.Kala 5.Satmya
6. Agni 7.Satwa 8.Vaya 9.Bala
The critical study of the above factors will enable the physician to decide, the
type of vasti, number of vastis, vasti dravya, etc to be administered in the particular
patients.
Procedure of Anuvasanavasti
1. Poorvakarma (pre-treatment): The patient should pass is natural urges then body of
the patient should be anointed with suitable sneha and mrudu sweda with hot water. He is
advised to have his prescribed meal it is madyama matra and made to take a short walk.
Patient is asked to lie over vasti droni, which is not very high, and the head must be at
lower level. The patient should be on his left side drawing up the right leg and
straightening the left leg.232,233,234
2. Pradhanakarma (treatment): The prescribed amount of taila should be taken in the
vastiputaka and tied well placing the vastinetra in position. Air is trapped from
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-METHODS
85
vastiyantra by gently pressing the vastiputaka. Then the anal region and the netra should
be smeared with oil to minimize the pain and irritation. Gently probe the anal orifice with
the index finger of the left hand and introduce the vastinetra through it into the rectum up
to the mark of first karnika. Keeping in the same position press the vastiputaka by putting
the adequate force then withdraw from the sight, release carefully the vastinetra when a
little quantity of sneha remained inside the vastiputaka.235
3. Paschatkarma (post-treatment): The patient is kept in same position as long as it
would take to count up to hundred. The patient should be gently struck three times on
each of the soles and over the buttocks. The distal part of the cot should be raised thrice.
Allow him to lie for sometime in the same position, if given sneha passed immediately;
another anuvasanavasti should be adopted. After passing the motion with sneha in proper
time the patient is allowed to take light food if he feels hungry236,237. 9 hours is the
maximum time for vasti pratyagamana.
Procedure of Niroohavasti:
Purvakarma: Niroohavasti is indicated to be administered in noon, in a patient who has
an empty stomach. Abhyanga with suitable sneha and mild swedana should be done prior
to the process and the patient is advised to be on the cot as prescribed for anuvasanavasti.
Vastidravya prepared as per the direction should be taken in vastiyantra and introduced
into pakwasaya. The procedures followed for anuvasana during its applications are the
same for nirooha238.
Paschatkarma: After giving the vasti the patient should use pillows and lie in supine
position. Application of pressure on buttocks and other procedures followed in anuvasana
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-METHODS
86

should not be done. When he gets up urges for defecation he may do the same in
squatting posture. After passing motion he may be advised to take bath in hot water and
have some solid food along with yusha, mamsarasa or milk in kapha, vata and pitta
predominant diseases respectively. It is generally seen that the adverse symptoms are
produced if any, during the therapy will subside after taking bath and their food. The
maximum time allowed for passing out the motion after the administration of the nirooha
vasti is one muhurtha (48 minutes). If it did not pass out, giving vasti, which consists of
sneha, kshara, mutra and amla dravyas, can bring it out. It should have snigdha, Ushna,
and teekshna properties. Phalavarti may also be used for this purpose. If the nirooha is
passed out instantly and the patient is not showing desired symptoms and signs again 2 or
3 vastis can be given. But if the patient shows excited symptoms of vata, snehavasti
should be given immediately. No particular regimen of samsarjanakarma is needed for
vasti karma239.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-METHODS
87
Chapter -5
Results
Present study registers 30 patients, out of 35 approached patients. The 30 patients
of Sthoulya, fulfilling the criteria of diagnosis and inclusive criteria were included in the
study. The Weight, B.M.I., Serum Cholesterol and Triglycerides are considered as
objectives for the inclusion in the present study.
All the patients were examined before and after the trail, according to the case
sheet format given in the annex. Both the subjective and objective criteria were recorded
along with validation of disease state. The data recorded are presented under the
following headings.
A. Demographic data
B. Validation of disease Data
C. Result of the Bruhatpanchamuladi yoga and
D. Statistical analysis
A) Demographic data:
The details of Age, Gender, Religion, and Occupation etc. of the 30 patients are as
follows.
A1) distribution of patients by Age
Here in this study an attempt is made to understand the male female responses to
the management with respect to that of the age groups. An interval of 10 has considered
from the ages 20 to 60 as discussed in the methods. In the study it is revealed that though
Sthoulya is seen since childhood in some people, people become aware of it either in
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-RESULTS
88
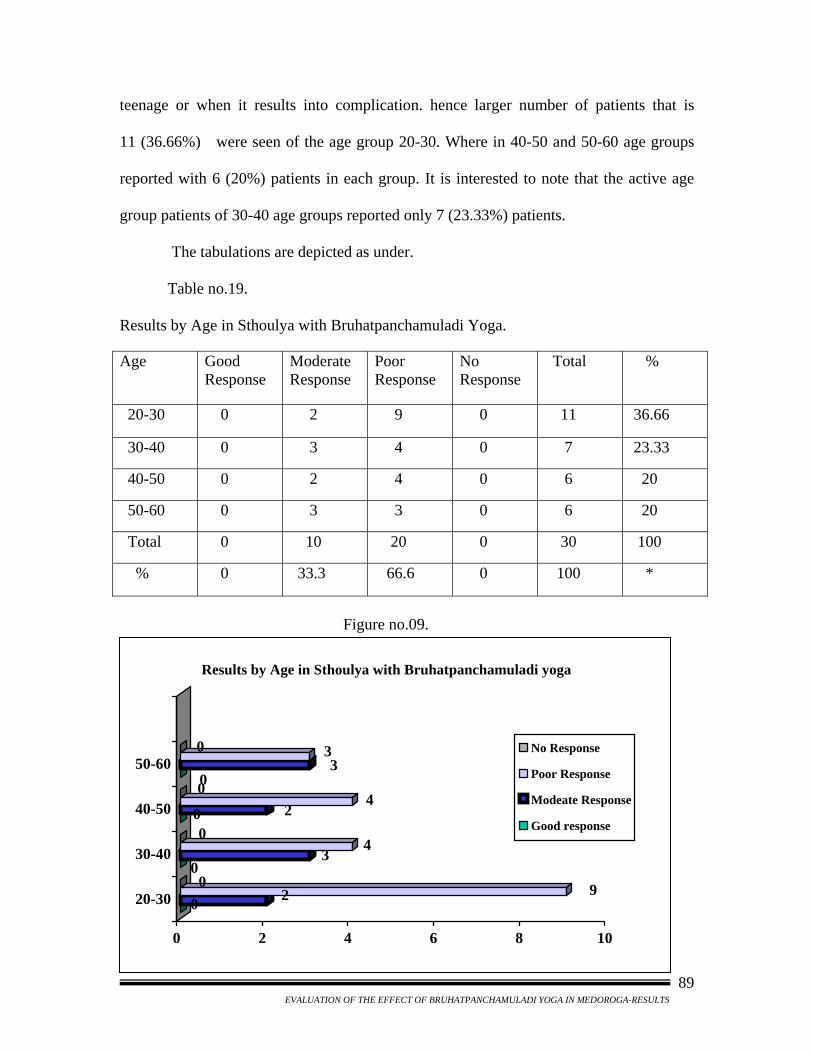
teenage or when it results into complication. hence larger number of patients that is
11 (36.66%) were seen of the age group 20-30. Where in 40-50 and 50-60 age groups
reported with 6 (20%) patients in each group. It is interested to note that the active age
group patients of 30-40 age groups reported only 7 (23.33%) patients.
The tabulations are depicted as under.
Table no.19.
Results by Age in Sthoulya with Bruhatpanchamuladi Yoga. Age Good
Response Moderate Response
Poor Response
No Response
Total %
20-30 0 2 9 0 11 36.66
30-40 0 3 4 0 7 23.33
40-50 0 2 4 0 6 20
50-60 0 3 3 0 6 20
Total 0 10 20 0 30 100
% 0 33.3 66.6 0 100 *
Figure no.09.
0 2 900
34
00 2
400
330
0 2 4 6 8 10
20-30
30-40
40-50
50-60
Results by Age in Sthoulya with Bruhatpanchamuladi yoga
No Response
Poor Response
Modeate Response
Good response
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-RESULTS
89
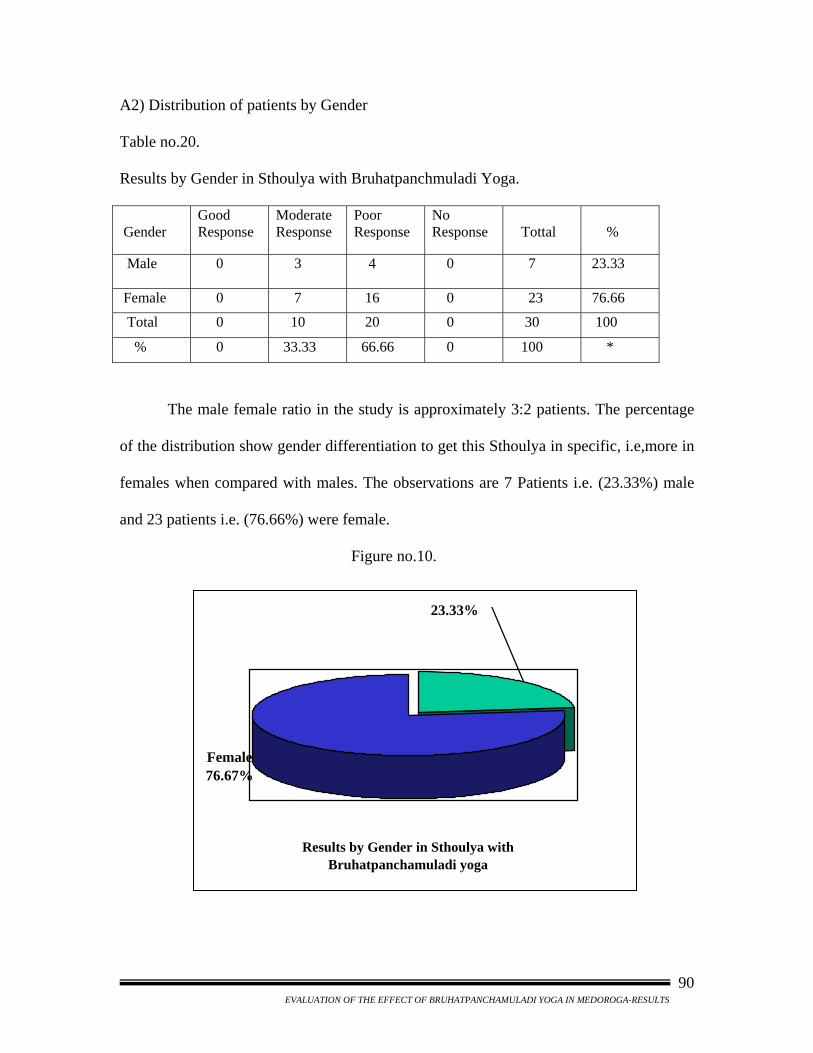
A2) Distribution of patients by Gender
Table no.20.
Results by Gender in Sthoulya with Bruhatpanchmuladi Yoga.
Gender
Good Response
Moderate Response
Poor Response
No Response
Tottal
%
Male
0 3 4 0 7 23.33
Female 0 7 16 0 23 76.66
Total 0 10 20 0 30 100
% 0 33.33 66.66 0 100 *
The male female ratio in the study is approximately 3:2 patients. The percentage
of the distribution show gender differentiation to get this Sthoulya in specific, i.e,more in
females when compared with males. The observations are 7 Patients i.e. (23.33%) male
and 23 patients i.e. (76.66%) were female.
Figure no.10.
Results by Gender in Sthoulya with Bruhatpanchamuladi yoga
23.33%
Female 76.67%
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-RESULTS
90
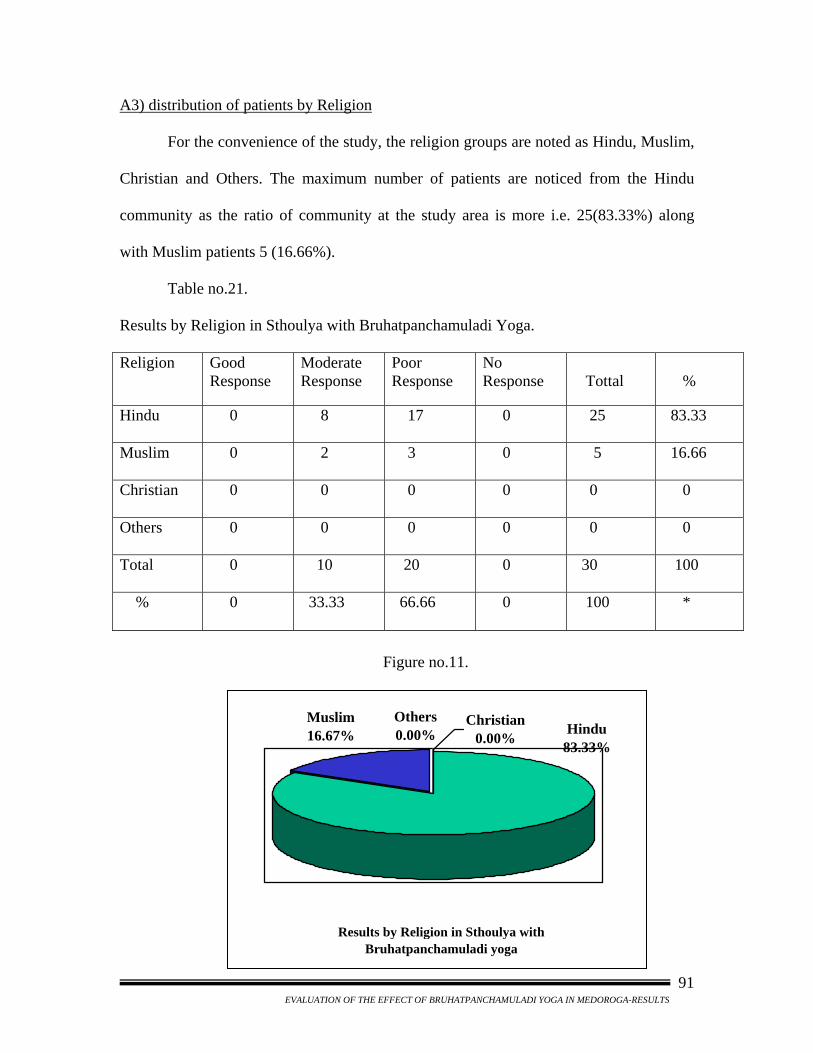
A3) distribution of patients by Religion
For the convenience of the study, the religion groups are noted as Hindu, Muslim,
Christian and Others. The maximum number of patients are noticed from the Hindu
community as the ratio of community at the study area is more i.e. 25(83.33%) along
with Muslim patients 5 (16.66%).
Table no.21.
Results by Religion in Sthoulya with Bruhatpanchamuladi Yoga. Religion
Good Response
Moderate Response
Poor Response
No Response
Tottal
%
Hindu
0 8 17 0 25 83.33
Muslim
0 2 3 0 5 16.66
Christian
0 0 0 0 0 0
Others
0 0 0 0 0 0
Total
0 10 20 0 30 100
%
0 33.33 66.66 0 100 *
Figure no.11.
Results by Religion in Sthoulya with Bruhatpanchamuladi yoga
Christian 0.00% Hindu
83.33%
Muslim16.67%
Others0.00%
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-RESULTS
91
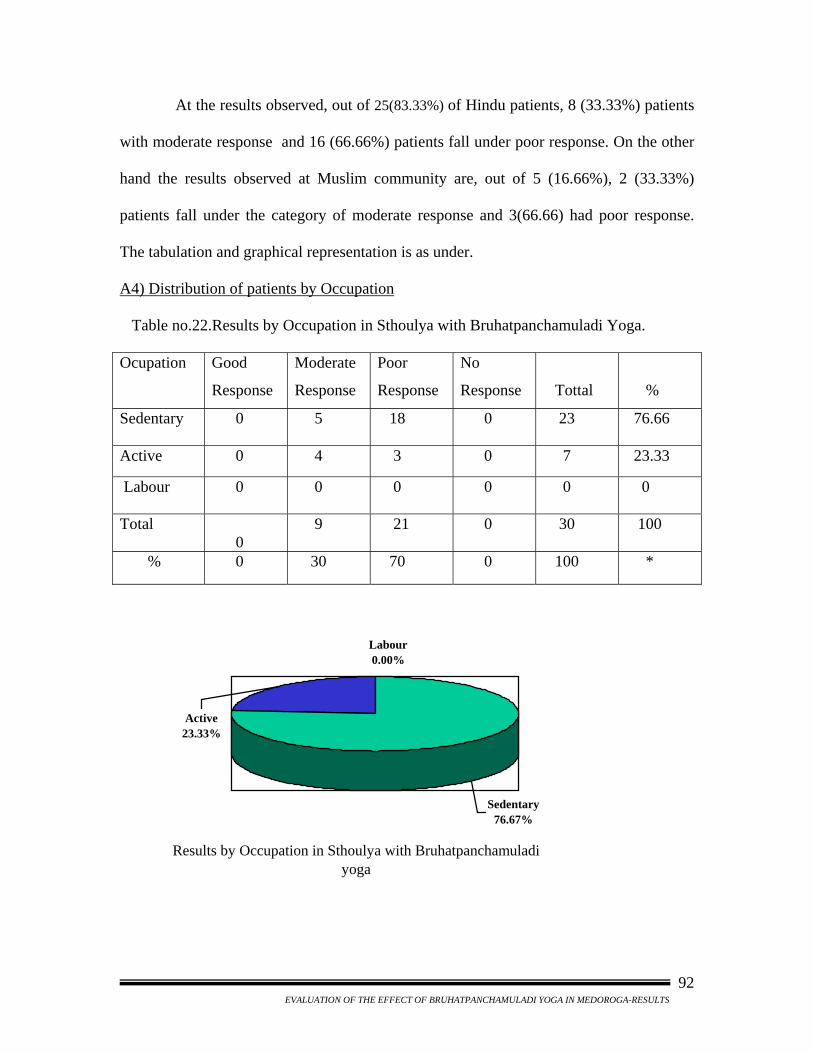
At the results observed, out of 25(83.33%) of Hindu patients, 8 (33.33%) patients
with moderate response and 16 (66.66%) patients fall under poor response. On the other
hand the results observed at Muslim community are, out of 5 (16.66%), 2 (33.33%)
patients fall under the category of moderate response and 3(66.66) had poor response.
The tabulation and graphical representation is as under.
A4) Distribution of patients by Occupation
Table no.22.Results by Occupation in Sthoulya with Bruhatpanchamuladi Yoga.
Ocupation Good
Response
Moderate
Response
Poor
Response
No
Response
Tottal
%
Sedentary
0 5 18 0 23 76.66
Active 0 4 3 0 7 23.33
Labour 0 0 0 0 0 0
Total 0
9 21 0 30 100
% 0 30 70 0 100 *
Results by Occupation in Sthoulya with Bruhatpanchamuladi yoga
Active23.33%
Sedentary76.67%
Labour0.00%
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-RESULTS
92
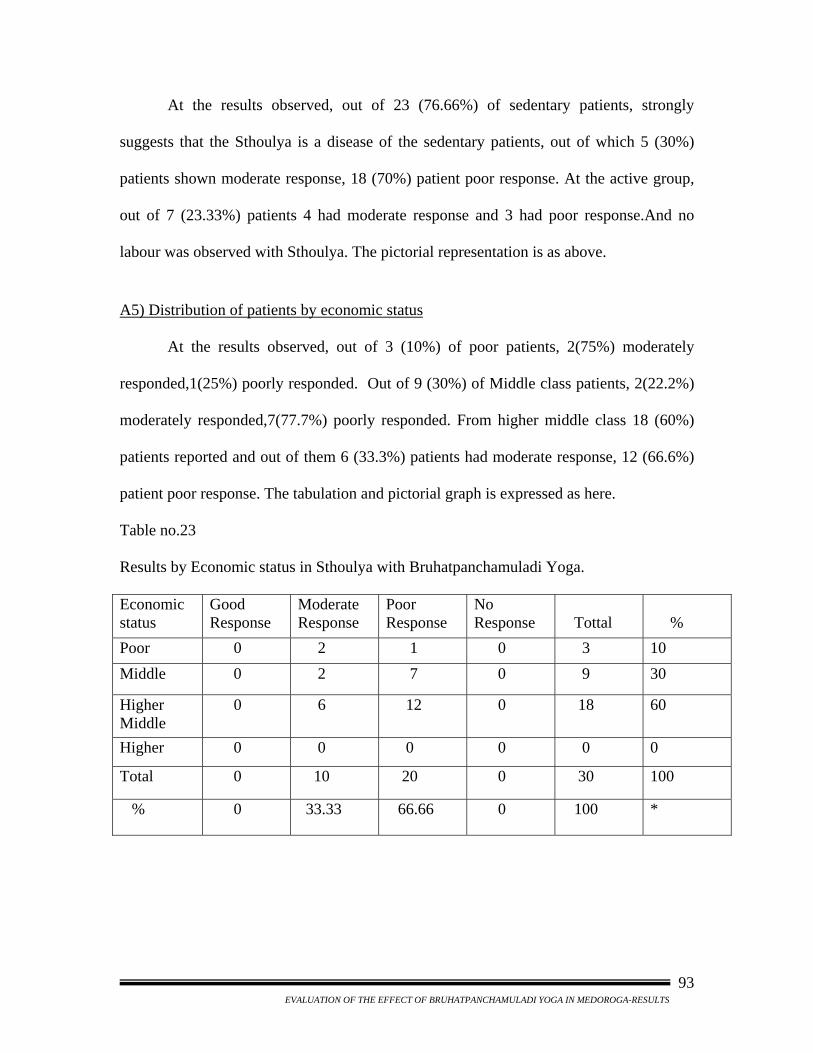
At the results observed, out of 23 (76.66%) of sedentary patients, strongly
suggests that the Sthoulya is a disease of the sedentary patients, out of which 5 (30%)
patients shown moderate response, 18 (70%) patient poor response. At the active group,
out of 7 (23.33%) patients 4 had moderate response and 3 had poor response.And no
labour was observed with Sthoulya. The pictorial representation is as above.
A5) Distribution of patients by economic status
At the results observed, out of 3 (10%) of poor patients, 2(75%) moderately
responded,1(25%) poorly responded. Out of 9 (30%) of Middle class patients, 2(22.2%)
moderately responded,7(77.7%) poorly responded. From higher middle class 18 (60%)
patients reported and out of them 6 (33.3%) patients had moderate response, 12 (66.6%)
patient poor response. The tabulation and pictorial graph is expressed as here.
Table no.23
Results by Economic status in Sthoulya with Bruhatpanchamuladi Yoga.
Economic status
Good Response
Moderate Response
Poor Response
No Response
Tottal
%
Poor 0 2 1 0 3 10 Middle 0 2 7 0 9 30
Higher Middle
0 6 12 0 18 60
Higher 0 0 0 0 0 0
Total 0 10 20 0 30 100
% 0 33.33 66.66 0 100 *
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-RESULTS
93
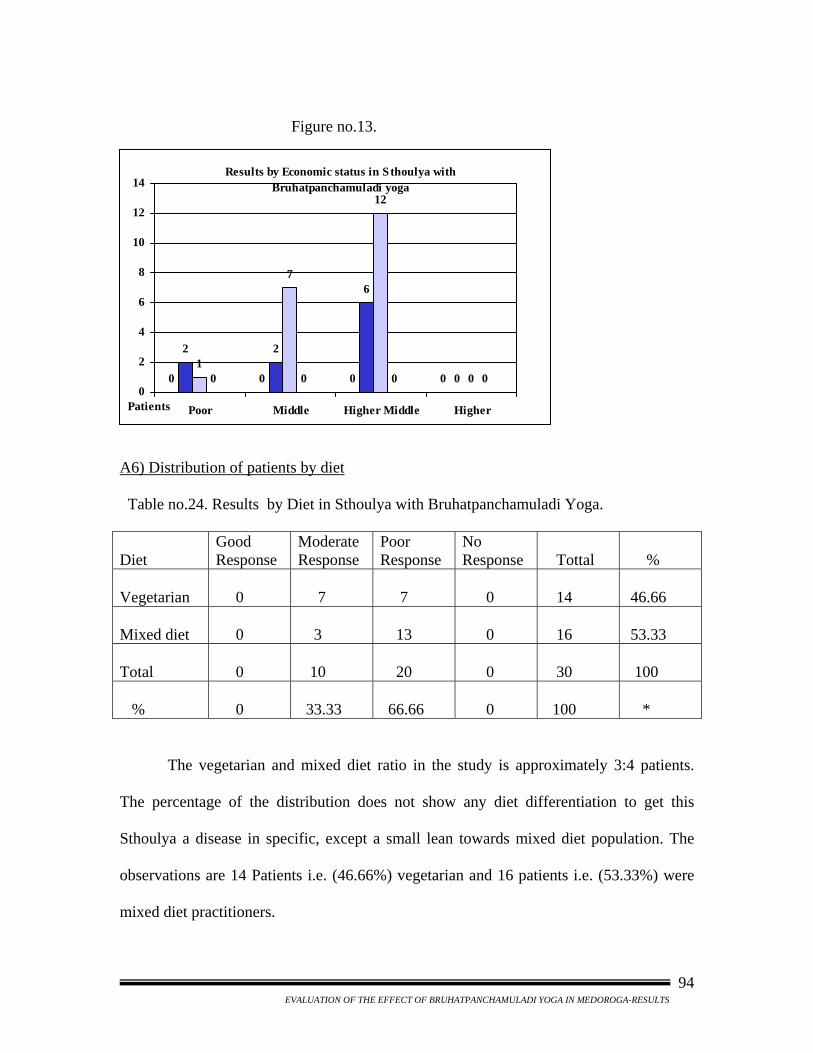
Figure no.13.
0 0 0 0
2 2
6
01
7
12
00 0 0 00
2
4
6
8
10
12
14
Poor Middle Higher Middle Higher
Results by Economic status in Sthoulya with Bruhatpanchamuladi yoga
Patients
A6) Distribution of patients by diet
Table no.24. Results by Diet in Sthoulya with Bruhatpanchamuladi Yoga. Diet
Good Response
Moderate Response
Poor Response
No Response
Tottal
%
Vegetarian
0
7
7
0
14
46.66
Mixed diet
0
3
13
0
16
53.33
Total
0
10
20
0
30
100
%
0
33.33
66.66
0
100
*
The vegetarian and mixed diet ratio in the study is approximately 3:4 patients.
The percentage of the distribution does not show any diet differentiation to get this
Sthoulya a disease in specific, except a small lean towards mixed diet population. The
observations are 14 Patients i.e. (46.66%) vegetarian and 16 patients i.e. (53.33%) were
mixed diet practitioners.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-RESULTS
94
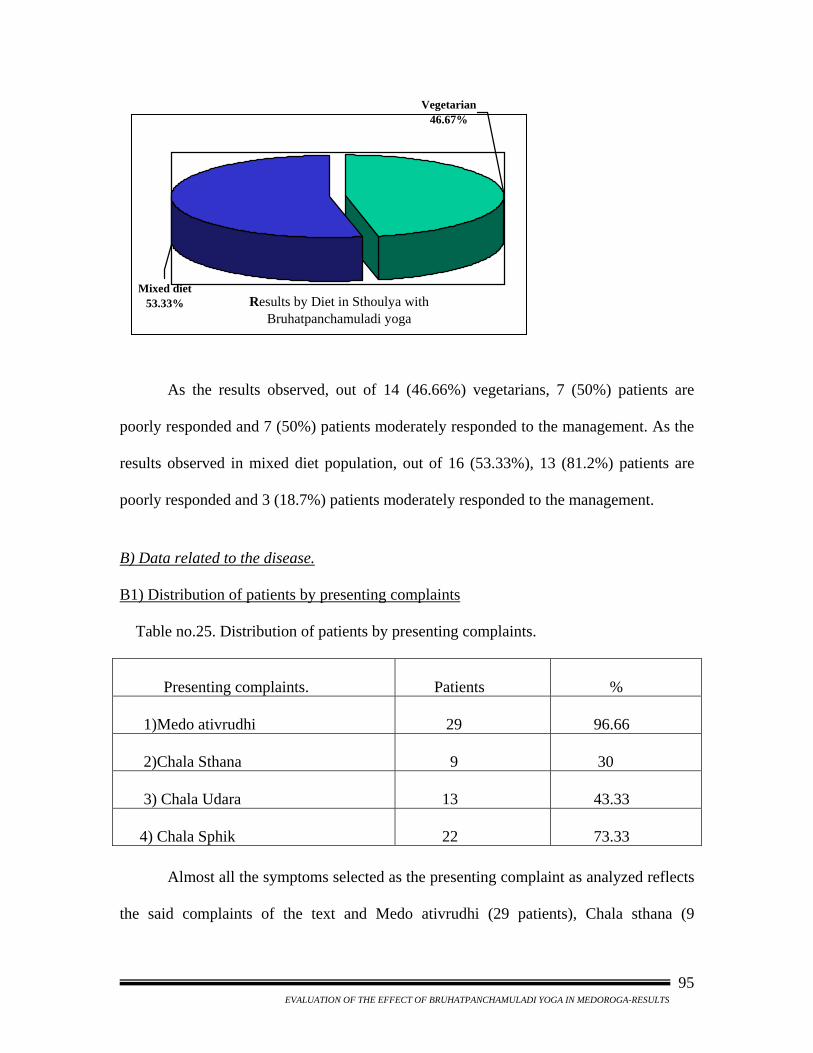
Results by Diet in Sthoulya with Bruhatpanchamuladi yoga
Mixed diet53.33%
Vegetarian 46.67%
As the results observed, out of 14 (46.66%) vegetarians, 7 (50%) patients are
poorly responded and 7 (50%) patients moderately responded to the management. As the
results observed in mixed diet population, out of 16 (53.33%), 13 (81.2%) patients are
poorly responded and 3 (18.7%) patients moderately responded to the management.
B) Data related to the disease.
B1) Distribution of patients by presenting complaints
Table no.25. Distribution of patients by presenting complaints. Presenting complaints.
Patients
%
1)Medo ativrudhi
29
96.66
2)Chala Sthana
9
30
3) Chala Udara
13
43.33
4) Chala Sphik
22
73.33
Almost all the symptoms selected as the presenting complaint as analyzed reflects
the said complaints of the text and Medo ativrudhi (29 patients), Chala sthana (9
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-RESULTS
95
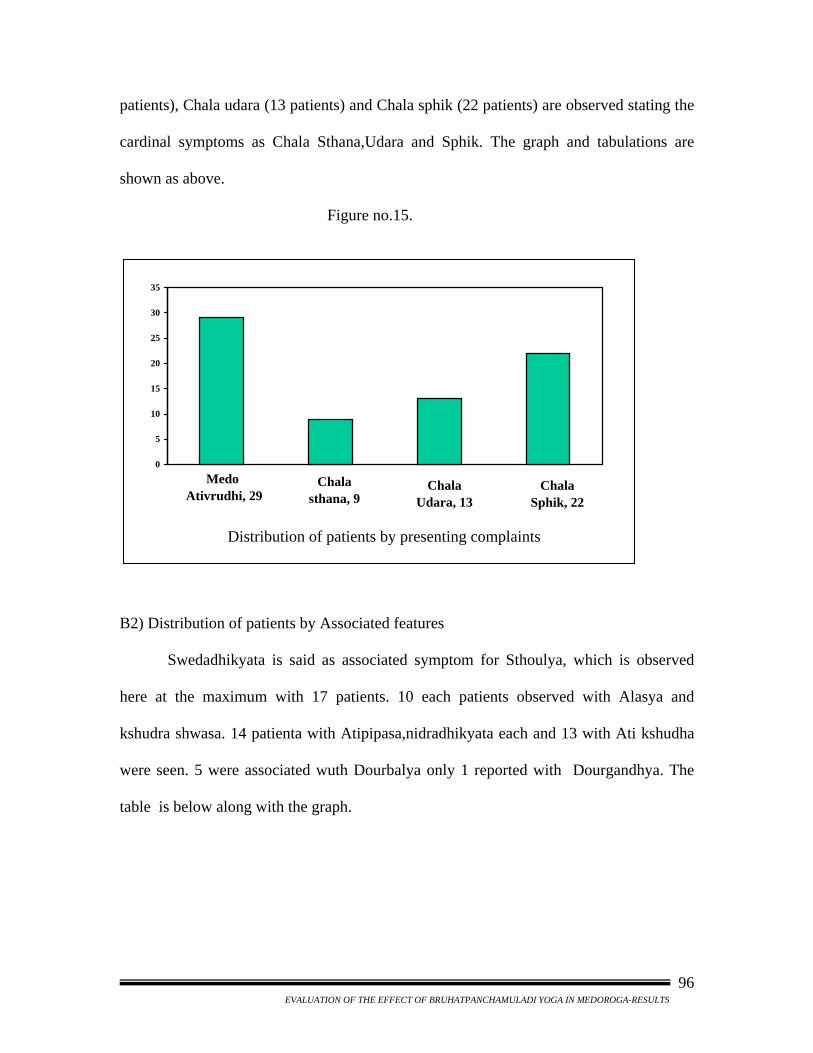
patients), Chala udara (13 patients) and Chala sphik (22 patients) are observed stating the
cardinal symptoms as Chala Sthana,Udara and Sphik. The graph and tabulations are
shown as above.
Figure no.15.
Distribution of patients by presenting complaints
Chala Udara, 13
Medo Ativrudhi, 29
Chala sthana, 9
Chala Sphik, 22
0
5
10
15
20
25
30
35
B2) Distribution of patients by Associated features
Swedadhikyata is said as associated symptom for Sthoulya, which is observed
here at the maximum with 17 patients. 10 each patients observed with Alasya and
kshudra shwasa. 14 patienta with Atipipasa,nidradhikyata each and 13 with Ati kshudha
were seen. 5 were associated wuth Dourbalya only 1 reported with Dourgandhya. The
table is below along with the graph.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-RESULTS
96
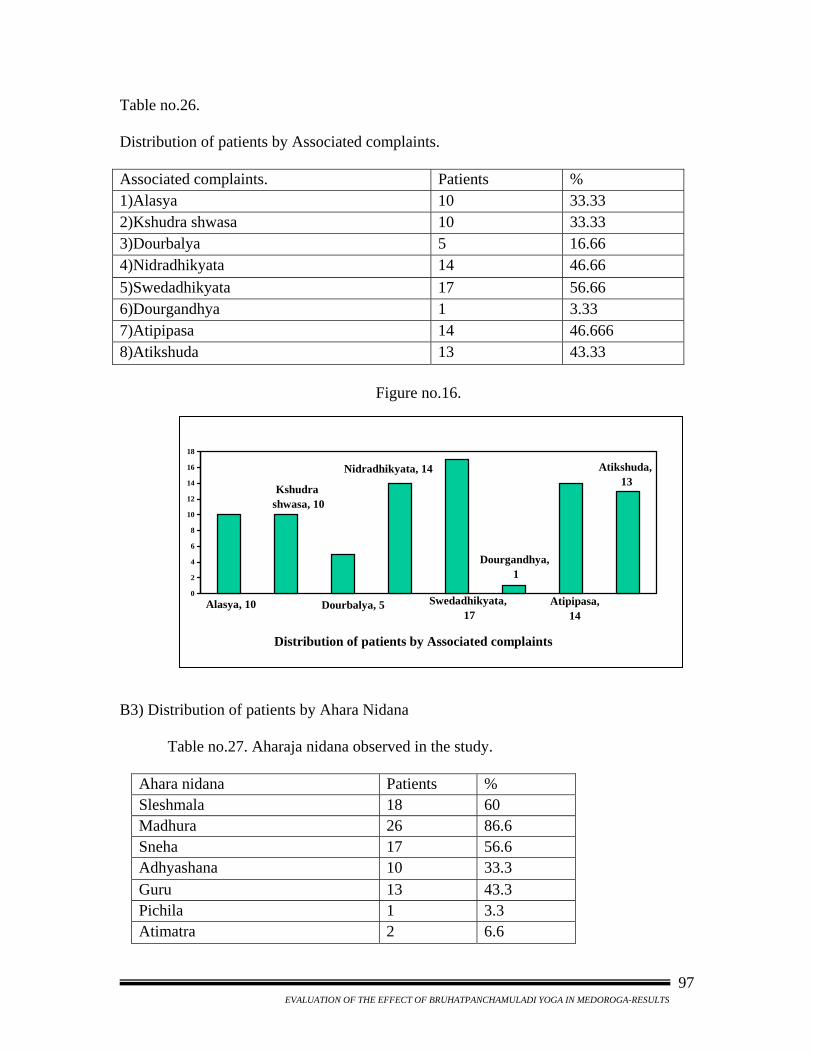
Table no.26. Distribution of patients by Associated complaints. Associated complaints. Patients % 1)Alasya 10 33.33 2)Kshudra shwasa 10 33.33 3)Dourbalya 5 16.66 4)Nidradhikyata 14 46.66 5)Swedadhikyata 17 56.66 6)Dourgandhya 1 3.33 7)Atipipasa 14 46.666 8)Atikshuda 13 43.33 Figure no.16.
Distribution of patients by Associated complaints
Dourgandhya, 1
Atikshuda, 13
Atipipasa, 14
Swedadhikyata, 17
Dourbalya, 5Alasya, 10
Kshudra shwasa, 10
Nidradhikyata, 14
0
2
4
6
8
10
12
14
16
18
B3) Distribution of patients by Ahara Nidana
Table no.27. Aharaja nidana observed in the study.
Ahara nidana Patients % Sleshmala 18 60 Madhura 26 86.6 Sneha 17 56.6 Adhyashana 10 33.3 Guru 13 43.3 Pichila 1 3.3 Atimatra 2 6.6
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-RESULTS
97
Ayurveda offered many causes especially in regard with food. The Madhura rasa
and Sleshmala ahara was observed in maximum patients the other factors also observed
in the study are tabulated above.
B4) Distribution of patients by Vihara Nidana
Many regimens are told in Ayurveda, out of which Diwaswapna is observed 60%
and Avyayama 86.6% of patients. The remaining vihara nidana tabulated are here under.
Table no.28. Vihara nidana observed in the study. Vihara nidana Patients % Avyayama 26 86.6 Cheshtadwesha 2 6.6 Arati - - Diwaswapna 18 60 Shayya &Asanasukha 4 13.3 B5) Distribution of patients by Manasika Nidana
The Manasika Nidana told in texts are very less observed here. Achinta wuth
76.6% the maximum,Harsha with 56.6% and Soukhya with 70%
Table no.29.
Manasika nidana observed in the study.
Manasika nidana
Patients
%
Achinta
23
76.6
Harsha
17
56.6
Soukhya
21
70
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-RESULTS
98
B6) Chronicity observed in the study. Table no.30. Chronicity of Sthoulya observed in the study. Chronicity of Sthoulya Patients % 1 yr. 1 3.3 1 – 2 yrs. 7 23.3 2 – 3 yrs. 6 20 3 – 4 yrs 4 13.3 >5 yrs. 10 33.3 Since Childhood 2 6.6
Maximum patients i.e.33.33% was observed with chronic history of Sthoulya
more than 5yrs. And next to that history of 1-2 yrs was found in 23.3% of patients. 20%
patients had history of 2-3yrs, and 13.3% with 3-4yrs.
B7) Data of Family history in the study
Table no.31.Data of Family history in the study
Family history Patients Percentage
Present 16 53.33 Absent 14 46.66
Total 30 100
The Sthulya observed as familial by researcher prove in study with 53.33%
family history. The rest of 46.66% show the instantaneous expression of the disease.
C) Result of the Bruhatpanchamuladi yoga
The result is drawn in four categories viz. Good response, Modarate response,
Poor response, and No response. In the study at the follow up is not included in the
results. The result of the Bruhatpanchamuladi yoga declared is representing the efficiency
of the drug with its embedded qualities. The tabulation is as below along with the graph.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-RESULTS
99
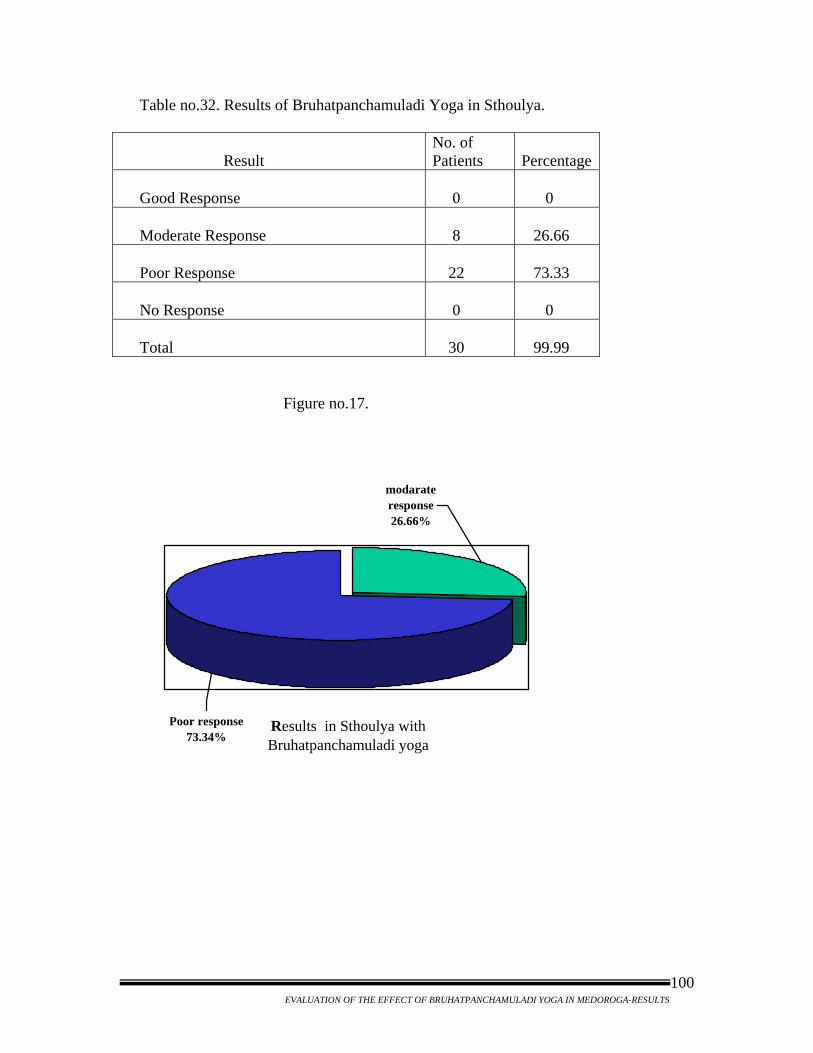
Table no.32. Results of Bruhatpanchamuladi Yoga in Sthoulya. Result
No. of Patients
Percentage
Good Response
0
0
Moderate Response
8
26.66
Poor Response
22
73.33
No Response
0
0
Total
30
99.99
Figure no.17.
Results in Sthoulya with Bruhatpanchamuladi yoga
Poor response73.34%
modarate response 26.66%
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-RESULTS
100
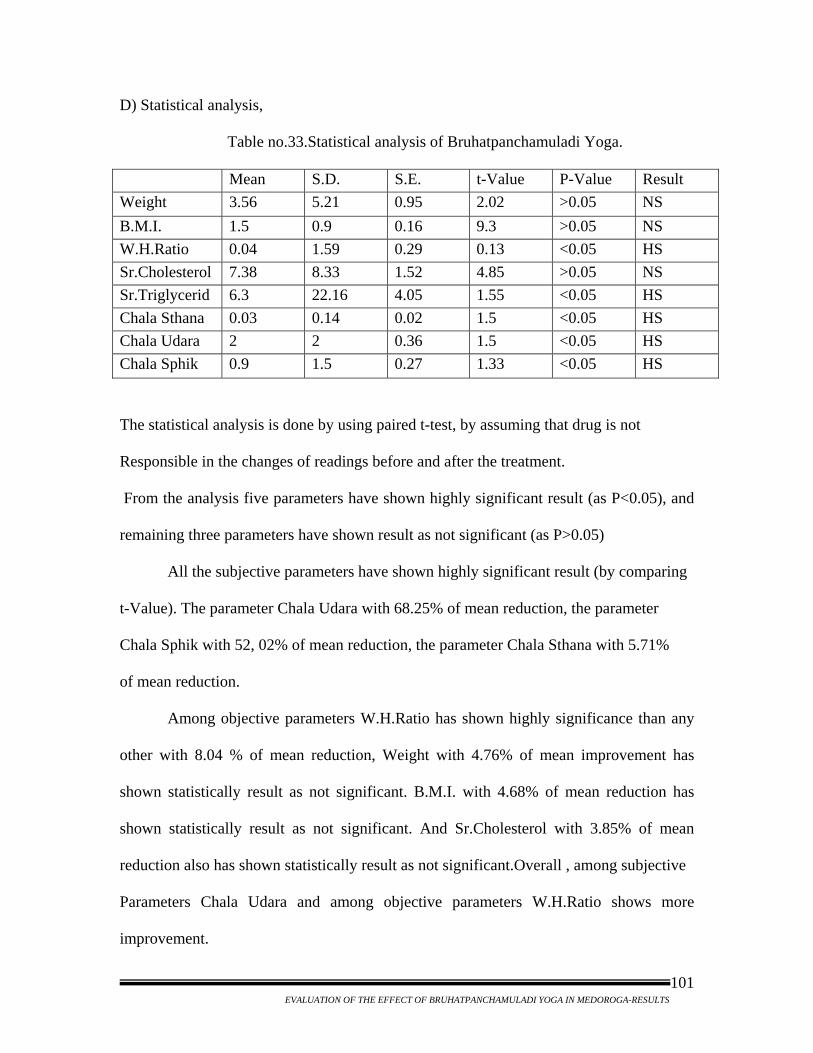
D) Statistical analysis,
Table no.33.Statistical analysis of Bruhatpanchamuladi Yoga.
Mean S.D. S.E. t-Value P-Value Result Weight 3.56 5.21 0.95 2.02 >0.05 NS B.M.I. 1.5 0.9 0.16 9.3 >0.05 NS W.H.Ratio 0.04 1.59 0.29 0.13 <0.05 HS Sr.Cholesterol 7.38 8.33 1.52 4.85 >0.05 NS Sr.Triglycerid 6.3 22.16 4.05 1.55 <0.05 HS Chala Sthana 0.03 0.14 0.02 1.5 <0.05 HS Chala Udara 2 2 0.36 1.5 <0.05 HS Chala Sphik 0.9 1.5 0.27 1.33 <0.05 HS The statistical analysis is done by using paired t-test, by assuming that drug is not Responsible in the changes of readings before and after the treatment. From the analysis five parameters have shown highly significant result (as P<0.05), and
remaining three parameters have shown result as not significant (as P>0.05)
All the subjective parameters have shown highly significant result (by comparing t-Value). The parameter Chala Udara with 68.25% of mean reduction, the parameter Chala Sphik with 52, 02% of mean reduction, the parameter Chala Sthana with 5.71% of mean reduction.
Among objective parameters W.H.Ratio has shown highly significance than any
other with 8.04 % of mean reduction, Weight with 4.76% of mean improvement has
shown statistically result as not significant. B.M.I. with 4.68% of mean reduction has
shown statistically result as not significant. And Sr.Cholesterol with 3.85% of mean
reduction also has shown statistically result as not significant.Overall , among subjective
Parameters Chala Udara and among objective parameters W.H.Ratio shows more
improvement.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-RESULTS
101
Chapter - 6
Discussion
The discussion is made under the following heads to facilitate discussion.
I) Discussion on Objectives.
II) Discussion on demographic data.
III) Discussion on disease aspects.
IV) Discussion on probable mode of action of Bruhatpanchamuladi Yoga.
V) Statistical discussion of parameters
I) Discussion on objectives:
Measures commonly used for assessing obesity are B.M.I., Waist circumference
(WC) & Waist hip ratio (W.H.Ratio). Unfortunately, B.M.I. is not considered to be a
good estimate of obesity in Asian Indians as they have a characteristic obesity phenotype,
with relatively lower B.M.I. but with central obesity.
The objectives proposed in the study are,
1) Evaluation of the effect of Bruhatpanchamuladi yoga in medoroga w.s.r.t. weight.
2) Evaluation of the effect of Bruhatpanchamuladi yoga in medoroga w.s.r.t. B.M.I.
3) Evaluation of the effect of Bruhatpanchamuladi yoga in medoroga
w.s.r.t. Waist Hip Ratio.
In the present study, though the results are given on the basis of weight reduction
(base to decide B.M.I.), but statistically significance is not observed in the reduction of
weight.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DISCUSSION
102
At the same time W.H.Ratio has shown significant result. This is because,
almost all the patients were observed with phenotype obesity where weight and B.M.I.
are not considered to be a good estimate of obesity. Hence the study being involved with
majority of phenotype obese patients, the statistical result was also found highly
significant in W.H.Ratio.
Prior to start this trial, a study of randomly selected 100 people was conducted in
the local area of Gadag province which showed majority of people having lower B.M.I.
with relatively higher Waist circumference and W.H.Ratio. Though lot of significance is
given to B.M.I. in relation with cerebro-vascular accidents, but in Asian Indian
population majority of people have phenotype of obesity with relatively less B.M.I. and
still suffering from cerebro-vascular accidents.
This study indicate that the threshold for obesity parameter i.e., B.M.I. is
relatively low when compared with W.C. and W.H.Ratio in rural.
Even some national level studies suggest that for any given B.M.I., Indians tend
to have increased waist circumference. Further Indians also tend to have excess body fat,
abdominal and truncal adiposity. These features have been referred to as the “Asian
Indian phenotype or paradox”. The W.H.O. has revised the B.M.I. cut-off for Asian
Indians and suggested a B.M.I. of 25 kg/m2 to define obesity against the 30 kg/m2 recom
mended for Europeans.
Several studies from India have attempted to modify the threshold for obesity and
abdominal obesity, and have suggested cut-off for B.M.I. ranging from 19-22 kg/m2,
while that of waist circumference ranges from 72-85cm in men and 65.5-80cm in women.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DISCUSSION
103
II) Discussion on demographic data:
a) Age relation discussion in Sthoulya:
Obesity can occur at any age and generally increases with age. It has been well
established that most adipose cells are formed earlier in life. Over feeding during infancy
and early childhood by over enthusiastic mothers can be an important cause for obesity in
adolescence and adults.
Though Sthoulya is seen since childhood in some people, people become aware
of it either in teenage or when it results into complication. Hence larger number of
patients that is 11 (36.66%) is seen of the age group 20-30 which is the age stage of
kapha. Where in 40-50 and 50-60 age groups reported with 6 (20%) patients in each
group. It is interested to note that the active age group patients of 30-40 age groups
reported only 7 (23.33%) patients.
b) Gender relation discussion in Sthoulya:
In the present study the male female ratio in the study is approximately 3:2
patients. The percentage of the distribution show gender differentiation to get this
Sthoulya in specific, i.e. more in females when compared with males. The observations
are 7 Patients i.e. (23.33%) male and 23 patients i.e. (76.66%) were female.
It occurs in either sex and it is generally found that men gain weight between the
ages of 29-35 while women gain most between 45-49 years of age. Women are more
prone than men in gaining weight. Women also go through three physiological
transitions- menarche, pregnancy and lactation, menopause- and at these thresholds; they
tend to put on weight.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DISCUSSION
104
c) Religion relation discussion in Sthoulya:
Religion is not a marker of the Sthoulya disturbances. The Sthoulya at communal
riots are may be claimed to insecurity, but the area of study is free of any disturbances the
religion relation is not existing. Thus the Maximum patients of 83.33% Hindus are
recorded in Hindu dominated area of the study.
d) Economic Status relation discussion in Sthoulya:
This condition is present more in affluent class of people in developing countries
and in low socio-economic group in developed countries. As the poor people in
developing countries cannot afford balanced diet, they are not prone to get affected. Due
to increased sedentary life styles and frequent social kitty parties the people of
economically rich group are affected in developing countries like India.
In the study observed, out of 30, 3 (10%) were poor patients, 9 (30%) of Middle
class patients, from higher middle class 18 (60%) patients were reported. This study
suggests maximum patients reported with obesity were belonging to higher socio-
economic status.
e) Occupation relation discussion in Sthoulya:
Occupation has a good role in the induction of Obesity naturally. Obesity is seen
more in the people associated with sedentary style occupations such as Computer / IT
experts, clerks, managers, etc.
In the present study, 23 (76.66%) are sedentary patients, strongly suggests that
the Sthoulya is a disease of the sedentary people, at the same time active group has only 7
(23.33%) patients. And no labour was observed with Sthoulya.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DISCUSSION
105
f) Diet Pattern relation discussion in Sthoulya:
Diets largely derived from carbohydrates and fats than protein rich diet. The
eating habits of obese people are varied. Some eat three large meals a day, while others
eat frequently five to six times a day. In both the cases excessive food intake is the cause
for Obesity. Not all obese patients eat more than an average person, but all obviously eat
more than they need.
The vegetarian and mixed diet ratio in the study is approximately 3:4 patients.
The percentage of the distribution does not show any diet differentiation to get this
Sthoulya a disease in specific, except a small lean towards mixed diet population. The
observations are 14 Patients i.e. (46.66%) vegetarian and 16 patients i.e. (53.33%) were
mixed diet practitioners.
This study strongly suggests that, whether the patient is vegetarian or non-
vegetarian doesn’t matter, it is the calorie which patient consumes and stores without
utilization of that energy to develop obesity.
III) Discussion on disease aspects:
a) Discussion over Nidana:
All the causative factors described in the Ayurvedic classics can be classified into
four groups.
1. Aharathamaka nidana
2. Viharathamaka nidana
3. Manasika nidana
4. Beeja swabhavaja nidana
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DISCUSSION
106
1) AHARAJA NIDANA -
26 patients in this present study are in the habit of consuming madhura rasa daily in
their diet. A very small excess of calorie if habitual can lead eventually to a large
accumulation of fat. 18 are habituated with sleshmala, 16 with sneha and 13 with guru
ahara. But when frequency of food intake was observed i.e. adhyashana was noted in 8
patients and atimatra in only 2 patients. This clearly indicates it is the quality of the food
that matters much than the frequency of intake because it is said that ‘prevalence of
obesity is greatest in those eating the highest fat intake’.
i.Overeating (qualitative & quantitative) is considered as prime cause for
obesity.In classical texts Adhyashana, Atimatrahara and Ati sampurana are the terms
used to indicate food consumption of patients. These collectively can be called as
Overeating indicating both quantitative and qualitative.
ii. Guru, sheeta, pichila, snigdha guna ahara are said to be causative factors of
sthoulya. Nowadays change in social circumstances and loss of intake of formalized meal
with consumption of milk products, oily and junk foods is remarkably increased which
are enriched with qualities such as guru, snigdha, pichila etc. and these have tendency to
get stored in the body at fat depots.
iii. Madhura rasa pradhana dravyas i.e. sweets are generally rich in calorie, a very
small excess of calories, if habitual, can lead eventually to a large accumulation of fat.
2) VIHARAJA NIDANA -
The viharaja nidana such as avyayama, avyavaya, diwaswapna etc. mentioned in
classics indicate the energy imbalance. As because of these factors the energy
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DISCUSSION
107
expenditure is reduced which results into stored energy and triggers the deposition of fat
in the body.
In the present study Avyayama was found in maximum patients i.e.26% and
diwaswapna in 18 . This suggests it is the sedentary and luxurious life which reduces the
energy expenditure and stored in the body as fat.
3) MANASIKA NIDANA -
In classical texts Achinta, Harsha and Soukhya are mentioned as manasika nidana
for sthoulya, whereas in modern science there is no such mention of causative factor but
nowadays the social factors, such as advertising and business launches, and repeated
involvement in such celebrations with festive moods may contribute for overeating and
some people eat because they are happy.
The Ayurvedic classical texts explain being happy enhances the obesity, where as
modern researches state a contradictory statement as stress ups obesity. But both the
factors in excess will lead to the obesity.
3) BEEJASWABHAVAJA NIDANA -
Acharya charaka, Chakrapani, Gangadhara and Bhavamishra considered that
sthoulya is inherited from obese parents.
Studies involving twins and adopted children indicate the importance of genetic
factor in both total body fat and its distribution. Genes in the individual decide the
number of adiposits and set point of weight. Even pattern of eating and activities are
influenced by social, cultural and economic factors which may be passed on from one
generation to another. In the present study 53.33% of the patients are found to be having
family history.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DISCUSSION
108
• Acharya Charaka has specifically mentioned Beejadosha as the nidana for Sthoulya.Chakrapani and Gangadhara comments over this statement as “Ati sthula mata pitru shonita shukra swabhavat”,which means the character of Sthoulya is inherited from Obese parents.
• In Bhavaprakasha it has been mentioned that decreased proportion of ‘shonita’
and increased proportion of ‘shukra’ in beeja at the time of conception, results in development of lean but potent body, while increased proportion of ‘shonita’ and decreased proportion of ‘shukra’ predisposes towards the development of stout but weak body.These genetic disorders are said to be incurable.
• Apart from that overnutrition during pregnancy, particularly with madhurarasa is
mentioned as a predisposing factor for the birth of an obese child i.e., childhood Obesity, which indicates role of environmental and hereditary cultural factors in the genesis of Sthoulya. The above three statements state the birth of obese child which can be taken as
Jata sthula. Though the term is not mentioned in the classics, the above statements
indicate the birth of obese child i.e, Jatasthula.
According to the moderners, being obese during pregnancy is dangerous for the
mother and expensive for the health care system. But does it affect the babies?
There are reasons to think it might. The period between conception and birth is
crucial- after all, one is growing from a single cell into a baby. The heart is being built,
brain is being wired. Exposure to alcohol during this time can disrupt brain development;
lack of iodine may permanently stunt growth. Being starved in the womb can lead to
health problems like heart disease later in life, especially if food becomes abundant. So
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DISCUSSION
109
what about over nourishment? Does an ‘obese’ environment in the womb somehow
predispose babies to obesity later on?
At the moment, such questions are difficult to answer. Humans are much harder to
study than animals and the phenomenon of obesity in pregnancy is relatively new, so we
don’t know much about it yet. Moreover many factors contribute to someone’s becoming
obese, and picking them apart is tricky. Added to that, an ‘obese’ environment in the
womb has two separate elements: the nutrients provided by the mother via the food she
eats, and the hormonal environment of someone who is overweight.
But the result of several studies suggests that the very fact of a woman being obese
during pregnancy may predispose her children to obesity. Why might this happen?
Perhaps an “obese” environment in the womb alters the wiring of the developing brain so
as to interfere with normal appetite control, fat deposition, taste in food, or metabolism.
Studies on other animals suggest that parts of the brain that control appetite develop
differently under ‘obese’ conditions. And in humans, one study has found that babies
born to obese mothers have lower resting metabolic rates than babies whose mothers are
of normal weight.
b) Discussion over chief complaints:
All most all patients i.e. 96.6% complained of medoativrudhi which indicates the
gross consideration of overweight and obesity by patient. Out of thirty patients all
complaint of Udara chalatwa, 22 complaint of spik chalatwa.this clearly shows that in
Indians we have phenotype obesity rather than generalized obesity
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DISCUSSION
110
c) Discussion over associated complaints:
Among all the patients 60% complained of swedadhikyta, this is because, due to
non utilization of lipids the BMR raises which results into excess sweating. 14
complained of atipipasa which is also resultant of raised BMR. Alasys, Kshudrashwasa,
Nidradhikyata seen in 33.3% of patients is because of Vrudha kapha (lipid deposition in
the body), leading to tamobhava.
IV) Statistical discussion of parameters:
All the subjective parameters have shown Highly Significant result. As charaka has
identified phenotype of obesity as sthoulya, and present trial is carried only in Indian
population the subjective parameters have shown Highly Significant result.
Among objective parameters, only W.H.Ratio and serum triglyceride have shown
Highly Significant result. Remaining objective parameters were found with Not
significant result. The waist hip ratio is the best measure to assess the regional fat. As
phenotype obesity has more of regional fat than generalized and the trial drug is effective
on regional fat. Weight and B.M.I. are measures to asses the generalized obesity which is
observed less in Indian population. Hence the trial drug is effective more on phenotype
obesity which is more seen in Indians.
V) Discussion on probable mode of action of Bruhatpanchamuladi Yoga:
To discuss about chikitsa, according to Gada nigraha, the sthoulya chikista need
mainly alleviation of Vata and Kapha along with depleted Medodhatu by increasing
medodhatwagni keeping in view regarding the agni as Charak said ‘ Laghu cha
apatarpana’. But in this study the drugs were selected on the basis of Shshruta’s statement
on sthoulya chikitsa as chedaneeya and virukshna dravya chikitsa.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DISCUSSION
111
The mode of action of trial drug can be analyzed on the basis of three factors:
1) Pharmacodynamics of drugs
2) Chemical composition of drugs
3) Site of action of drugs.
1) Pharmacodynamics of drugs \ Rasapanchaka:
Here the drugs of bruhatpanchamula i.e. Bilwa, Agnimantha, shyonaka,
Gambhari, Patala, all have ruksha guna, kashay and tikta rasa, katu vipaka and ushna
veerya (these are present commonly in internal medicine as well as in vasti as kashaya
churn a). Because of these properties they act on kapha and meda and relieve the
medavruta vata which is the main pathology found in manifestation of sthoulya. Hence
these drugs act as virukshana dravyas i.e. which remove avarana (dalhana) in treating
sthoulya.
The drugs pippali and madhuka saara which were added as prakshepa dravyas in
nirooha vasti and these being teekshna dravyas they does chedana of kapha and helps in
srotoshodhana.
The madhu which is used internally aswellas in vasti; it has kashaya rasa and
ruksha guna along with yogavahi property. Hence it helps in reducing meda.
2) Chemical composition of drugs:
In latest researches it has been proposed that honey contains a sucralfate like
substance that may be responsible for its antioxidant property and gastric protection,
deterioration in the processes of lipids peroxidation and rise in the activity of antioxidant
system of an organism.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DISCUSSION
112
3) Sites of drug metabolism:
The metabolizing enzymes are found in most tissues in the body with the highest
levels located in the tissues of the gastrointestinal tract (liver, small intestine and large
intestine). Drugs that are administered, absorbed by the gut and taken to the liver can be
extensively metabolized. The small intestine plays a crucial role in drug metabolism.
Since most drugs that are administered orally and through trans rectal route are absorbed
by the gut and taken to the liver through portal vein240. In the present trial, treatement is
initiated with rectal administration of drugs \ vasti, later with oral route.
The fluid containing the drug is retained in the rectum for local action; it may act
systemically after absorption through the mucous membrane. The portion absorbed from
the upper rectal mucosa is carried by the superior haemorrhoidal vein into the portal
circulation where as that absorbed from the lower rectum enters directly into the systemic
circulation via the middle and inferior haemorrhoidal veins241.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-DISCUSSION
113
Chapter - 7
Conclusion
On the basis of the study “Evaluation of the effect of Bruhatpanchamuladi Yoga
in Medoroga” the conclusion can be drown as;
Obesity is identified as a nutritional disorder, thirty years ago, still continues to be
one of the most important, yet preventable health hezard.
Obesity viz., sthoulya is characterized by pendulous abdomen, buttocks and
breasts.
The term Sthoulya and Medoroga are synonymous. They indicate the same
condition where medovrudhi in the body is noticed.
Charaka included the obese person under the category of eight undesirable
personalities in the society.
Acharya Sushruta considered the rasa as the major pathological factor involved in
both obesity and emaciation (sthoulya and kaarshya).
Of the two, obesity and emaciation, emaciation is less harmful than obesity, even
though both of them are equally in need of treatment. Because volume of
suffering is more in obese.
Measures commonly used for assessing obesity are BMI and waist circumference.
Unfortunately, BMI is not considered to be a good estimate of obesity in Asian
Indians as they have a characteristic obesity phenotype, with relatively lower BMI
but with central obesity. Several studies suggest that for any given BMI Indians
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-CONCLUSION
114
tend to have increased waist circumference and Indians also tend to have excess
body fat, abdominal and truncal obesity.
Weighty women get six times more diseases when compared with obese men.
Charaka has mentioned bad prognosis for Sahaja (hereditary) disease. Hence
Sahaja Sthoulya can be considered as Asadhya. Therefore Sadhyasadhyata of
Sthoulya can be constructed on the basis of general principles of Sadhyasadhyata
depicted in Ayurvedic Texts.
As Charka’s explanation of sthoulya matches with phenotype of obesity,
W.H.Ratio and skin fold thickness can be taken as parameters to assess the
sthoulya, as W.H.Ratio helps to check the abdominal fat (Chala udara ) and
gluteal fat (chala sphik) & Skin fold thickness helps to measure regional fat (chala
sthana ).
Acharya Charaka has specifically mentioned Beejadosha as the nidana for
sthoulya. In Bhavaprakasha it has been mentioned that increased proportion of
‘shonita’ and decreased proportion of ‘shukra’ predisposes towards the
development of stout but weak body
The result of Bruhatpanchamuladi Yoga declared is representing the efficacy of
the drug with its qualities, is 26.6% moderate response and 73.3% patients
observed with poor response.
The conclusion drown statistically for the present drug response is as highly
significant as P < 0.05
Obesity / Sthoulya are a chronic illness that requires continuous treatment.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-CONCLUSION
115
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-SUMMARY
116
Chapter - 8
Summary The present study entitled “Evaluation of the effect of Bruhatpanchamuladi
Yoga in Medoroga” is summarized as under.
“You are not good enough, is the message family and society send to
Overweight and Obese people especially to women”. It’s nearly 60 years since Simone de
Beauvoir famously wrote, one is not born a woman but becomes one. Many of Obese
lives are bedeviled by the three-letter word, ‘FAT’ along with “social anxiety, loss of
self-esteem, isolation and vulnerability in social and private lives”.
The behavioral changes conductive to weight gain are such as
a) High fat diets do not switch off appetite and induces very little energy expenditure.
b) Snaking and loss of formalized meal pattern.
c) Consumption of energy dense food and drinks high in fat but low in bulk.
d) Alcohol promotes weight gain
e) Decreasing physical activity with age
f) Declining overall levels of physical activity in society occur with sedentary jobs and
change in social circumstances and sedentary pastimes e.g. the television watching coach
potato
g) Giving up smoking induces fall in energy expenditure
h) Stress ups obesity
i) Lack of sexual drive in 30 plus women in today’s busy life.
Now a day in society these factors are triggering much in producing obesity.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-SUMMARY
117
In the present study 11 (36.66%) were seen of the age group 20-30. Where in 40-50 and
50-60 age groups reported with 6 (20%) patients in each group. It is interested to note
that the active age group patients of 30-40 age groups reported only 7 (23.33%) patients.
Sthoulya is seen since childhood in some people, people become aware of it either in
teenage or when it results into complication.
All most all patients complained of udara chalatwa, which indicates the phenotype
of obesity in Indians rather than the generalized one. Hence Charak’s definition for
sthoulya appropriately suits for phenotype of obesity seen in Asian Indians.
In classical texts though lot of explanation is available regarding the sthoulya,
there is no explanation or parameters given to assess it. In contemporary science number
of measures are there to assess the obesity, among them B.M.I is widely used. Where as it
does not suit in most of the Indians as they have phenotype of obesity. B.M.I. helps to
assess the total body fat where as skin fold thickness and waist hip ratio helps to assess
the regional fat which is seen more in Indians.
As Charka’s explanation of sthoulya matches with phenotype of obesity,
W.H.Ratio and skin fold thickness can be taken as parameters to assess the sthoulya, as
W.H.Ratio helps to check the abdominal fat (Chala udara ) and gluteal fat (chala sphik) &
Skin fold thickness helps to measure regional fat (chala sthana ).
In this it is observed that the administration of Ayurvedic herbal formulations
which is selected for the study has good results in reducing W.H.Ratio with 8.04% rather
than in reducing weight and B.M.I. by 4.76% & 4.68% respectively. The effectiveness of
drug is decided by statistical analysis is highly significant as P value < 0.05 & by
impairing the t – Values.
Bibliographic Refarences
1) http://www.anglefire.com/ar/laproscopy/obesity.html-60k2) http://www.hindu.com/the hindu/seta/2002/03/21/stories/2002 0321 00160 400.htm3) Damayanti Datta, Society & the arts,FAT of the Matter, INDIA TODAY, June 16, 2008, pp 59. 4) www.newsmas.com/archieves/articles/2004/5/9/150423.5.html-30k-55) www.wrongdiagnosis.com/NIDDK _ / Obesity. 6) ibid. 7) Damayanti Datta, Society & the arts,FAT of the Matter, INDIA TODAY, June 16, 2008, pp 57. ( Source; AIIMS, NFHS, IJO, IDEA 2004-2005 ). 8) Prakash Seshadri et.al., (University of Pensylvania school of Medicine), Low carbohydrate diets for weight loss : Historical & environmental perspective, Indian J Med Res 123, June 2006, pp 739-747 (Fall, CHD. Non-industrialized countries and affluence, Br. Med Bull 2001;60:33-50) pp 740. 9) Ibid, Indian J Med Res 123, June 2006, pp 739-747 (Mc Cann. BA, Reid E, Measuring the Health Effects of Sprawl, Smart growth America: Surface transportation policy project (Thesis on the internet), Am J of Health promotion September 2003 (cited 2006 Jan 6). Available from www.smartgrowth america.org/report/healthsprawl 8.03.pdf.) pp 740 10) Ibid, Indian J Med Res 123, June 2006, pp 739-747 (Peters JC, Wyatt HR, Donahoo WT, Hill JO. From instinct to intellect: the challenge of maintaining healthy weight in the modern world. Obes. Rev 2002; 3: 69-74) pp 740. 11) Dr.Brahmanand Tripathi ed., Astanga Hrudayam Sutrasthana 4/26, Edition;Reprint 2007, Pub;Chaukhamba Sanskrit Pratishthan,pp 59. 12) Ratna Bramhashankar shastri ed., Yogaratnakar uttarardha, Rasayanadhikara-1, Edition: 4th 1988, Pub: Chowkhamba Sanskrit sansthan, pp 498. 13) V. Mohan & R. Deepa (Dr. Madras Diabetics Research Foundation), Obesity & abdominal obesity in Asian Indians, Indian J Med Res 123, May 2006, (Infant and adult obesity, Lancet 1974; 1:178) pp 593-596. 14) Prakash Seshadri et.al., (University of Pensylvania school of Medicine), Low carbohydrate diets for weight loss : Historical & environmental perspective, Indian J Med Res 123, June 2006, pp 739-747 (Fall, CHD. Non-industrialized countries and affluence, Br. Med Bull 2001; 60:33-50) pp 740. 15) Ibid, Indian J Med Res 123, June 2006, pp 739-747 (Mc Cann. BA, Reid E, Measuring the Health Effects of Sprawl, Smart growth America: Surface transportation policy projec (Thesis on the internet), Am J of Health promotion September 2003 (cited 2006 Jan 6) Available from www.smartgrowth america.org/report/healthsprawl 8.03.pdf.) pp 740. 16) Ibid, Indian J Med Res 123, June 2006, pp 739-747 (Peters JC, Wyatt HR, Donahoo WT, Hill JO. From instinct to intellect: the challenge of maintaining healthy weight in the modern world. Obes. Rev 2002; 3: 69-74) pp 740. 17) Prof. Ramanath Dwivedi ed., Chakradatta 36.Sthoulya chikitsadhikara.,Edition:4th,2002, Pub: Chowkhamba Sanskrit sansthan, pp 221. 18) Sri Sudarshana Shastri ed., Madhava Nidana 34.Medoroga nidana, Edition:Reprint 2007, Pub: Choukhamba Prakashan, pp28. 19) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 21, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 398-411. 20) Prof. R.K.Srikanthamurthy ed., Sharangadhara Samhita Prathama Khanda 7/65, Edition:6th,2006, Pub: Choukhambha Orientalia, pp 37. 21) Pdt.Parashuram Shastri,Vidyasagar ed., Adhamall’s Gudhartha Deepika (Sharangadhara Samhita), Prathama Khanda 7/65,3rd Edition, Pub:Choukhambha Orientalia, pp 91. 22) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Chikitsasthana 33/18, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 143. 23) Vaidya Ranjit Ray Desai ed., Astanga Sangraha Sutrasthan 27/7, 2ndEdition1981, Pub: Sri Baidhyanath Ayurveda Bhavan Ltd. Pp 744. 24) Vaidya Ranjit Ray Desai ed., Astanga Sangraha Sutrasthan 24/66, 2ndEdition1981, Pub: Sri Baidhyanath Ayurveda Bhavan Ltd. Pp 702. 25) Syar-Raja Radhkantha Deva Bahuddurena, Shabdakalpadruma, Part –3, 3rd
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-BIBLIOGRAPHIC REFERENCES
1
Edition 1967, Pub:Choukambha sanskrita series,. pp 778- 779. 26) C.Dwarakanath,ed., Introduction To Kayachikitsa, Chapter No.17, 3rd Edition 1996, Pub:choukambha Orientalia,. pp 314, 333. 27) Pdt. Rajeshwara Datta Shastri ed.,Charaka Samhita, Chikitsasthana 15/29,30. Edition:Reprint 1998, Pub: Chaukhambha Bharati Academy, pp 458. 28) Dr Gangasahaya Pandeya ed., Charaka Samhita, Shareerasthana, 7/15, 5th Edition 1997, Pub:Chaukhambha Sanskrita Sansthan, Page No 810. 29) Dr.Brahmanand Tripathi ed., Charaka Samhita Chikitsasthana 15/18, Edition:Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 553. 30) Ibid., 15/17. 31) Dr.Brahmanand Tripathi ed., Charaka Samhita Vimanasthana 5/7, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 696. 32) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Shareera 9/12, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 72. 33) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Shareerasthana 4/12, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 30. 34) Dr.Brahmanand Tripathi ed., Astanga Hrudayam Sutrasthana 11/11, Edition;Reprint 2007, Pub;Chaukhamba Sanskrit Pratishthan,pp 162. 35) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Sutrasthana 15/7, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 57. 36) Dr.Brahmanand Tripathi ed., Charaka Samhita Chikitsasthana15/18, Edition:Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 553. 37) ibid. 15/17. 38) ibid. 39) Vaidya Ranjit Ray Desai ed., Astanga Sangraha Sutrasthan 19/4, 2ndEdition1981, Pub: Sri Baidhyanath Ayurveda Bhavan Ltd. Pp 588. 40) ibid 19/7, pp 590. 41) Syar-Raja RadhkanthaDeva Bahuddurena,Shabdakalpadruma, Part –5, 3rd Edition 1967., Pub: Choukambha sanskrita series, pp 450. 42) 43) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 21/9, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 401. 44) Sri. Monier Monier Williams, Sanskrit English Dictionary, New Delhi, Motilal Banarasi Das Publishers, 1999. Pp1333. 45) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 21/3, 22-24, Edition:Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 393,404. 46) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Sutrasthana 15/37, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 62. 47) Dr.Brahmanand Tripathi ed., Astanga Hrudayam Sutrasthana 14/10, Edition;Reprint 2007, Pub;Chaukhamba Sanskrit Pratishthan,pp 192. 48) Sri Sudarshana Shastri ed., Madhava Nidana 34.Medoroga nidana, Edition:Reprint 2007, Pub: Choukhamba Prakashan, pp28. 49) Prof. R.K.Srikanthamurthy ed., Sharangadhara Samhita Prathama Khanda 7/65, Edition: 6th, 2006, Pub: Choukhambha Orientalia, pp 37. 50) Prof. R.K.Srikanthamurthy ed., Sharangadhara Samhita Madhyama Khanda 2/115, Edition:6th,2006, Pub: Choukhambha Orientalia, pp 69. 51) Pandit Sri Brahma Shankar Sharma ed., Bhavaprakasha Madhyamakhanda, Chapter No 39, 5th Edition 1988, Pub:Chaukhambha Sanskrita Sansthan, , pp 405. 52) Prof. P.V.Tewari ed., Kashyapa Samhita, Chikitsastan18/13,14. Edition: Reprint 2002, Pub:Chaukhambha Vishwabharati, pp 248. 53) Prof.Priyavat Sharma,ed., Bhelasamhita Sutrasthana 11/10, Edition: Reprint 2005, Pub:Choukambha Vishwabharati, pp 52. 54) Brahmashankar Shastri ed., Yogaratnakar Medhoroga chikitsa Adhikara, 2nd Edition, Pub:Chaukhambha Sanskrit Series, pp 97. 55) Prof. Ramanath Dwivedi ed., Chakradatta 36.Sthoulya chikitsadhikara.,Edition:4th,2002, Pub: Chowkhamba Sanskrit sansthan, pp 221.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-BIBLIOGRAPHIC REFERENCES
2
56) Prof.Sidhi Nandan Mishra ed., Bhaishajya Ratnavali 39.Medorogadhikara, Edition:1st,2005, Pub: Choukhamba Surbharati Prakashan, pp 722. 57) Sri. Ganga Sahay Panday ed., Gadanigraha- Kayachikitsa khanda,31.Medorogadhikara, 1stEdition 1969, Pub: Chaukhambha Sanskrit Series, pp 680-686. 58) Vaidhya Jadavji Trikamji Acharya ed.,Chakrapanidatta commented Charaka Samhita, Sutrasthana 21/1- 20, Edition: Reprint 2004, Pub: choukambha Sanshkrita Sansthana, pp 116,117. 59) Vaidya Jadavji Trikamji Acharya ed.,Dalhanacharya, Sushruta Samhita, Sutrastana 15/37, 7th Edition 2002, Pub:Chaukhambha Orientalia, , pp 73. 60) Dr.D.V.Pandit Rao and Dr.Ayodhya Pandey ed., Indu, Astanga sangraha 24/20, 1stEdition, 1991. NewDelhi, CCRAS, pp 297. 61) Hari Sadashiva Shastri Paradakara ed., Arunadatta, Ashtangahrudaya, Sutrastana 14/32, Pub:Chaukhambha Surbharati Prakashan, 1997, pp 227. 62) Ibid, 14/21-24, pp 226. 63) Pt.Parashurama Shastri, Vaidyasagara ed., Adamalla, Sharangadhara Samhita, Prathamakhanda 5/6, 3rd Edition 1983, Pub:Chaukhambha Orientalia, pp 43. 64) Ibid, 7/65, pp 91. 65) Jain Sankarlalgi Vaidya ed.,Vangasena Samhita 39/170, Pub:Khemnath Sri krishnadas Publishers, 1996, pp 458. 66) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 21/4, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 399. 67) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Sutrasthana 15/37, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 62. 68) As.Hr. Ama as causative factor 69) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 1/44, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 15. 70) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 21/4, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 399. 71) ibid. 72) ibid. 73) ibid. 74) Pandit Sri Brahma Shankar Sharma ed., Bhavaprakasha Madhyamakhanda, 40/5, 6. 5th Edition 1988, Pub:Chaukhambha Sanskrita Sansthan, , pp 412. 75) Dr.Brahmanand Tripathi ed., Charaka Samhita Shareerasthana 8/29, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 950. 76) Dr.Gangasahaya Pandeya ed.,Charaka Samhita, Sutrasthana 21/4, 5th Edition1997, Pub:Chaukhambha Sanskrita Sansthan, pp 278. 77) Kaviraja Ambikadutta Shastri ed., Sushruta Samhita, Sutrasthana, 15/37, 14th Edition2003, Pub: Chaukhambha Sanskrit Sansthan, , pp 62. 78) Dr.Ravi Dutt Tripathi ed., Astangasamgraha, sutra sthana, 24/11-33, 1996, Pub:Chaukhambha Sanskrita Pratishthan, pp 435-439. 79) Indradev Tripathi, ed., Astanga Hridayam, sutrasthana, 14/9, 10. 1st Edition 1994, Pub: Krishnadas Academy, pp 149. 80) Prof.Yadunandana Upadhyaya, ed., Madhavanidhana, 34/1, Edition: Reprint 2005., Pub:Choukambha Sanskrita Sansthana, , pp 28. 81) Pandit Sri Brahma Shankar Sharma ed., Bhavaprakasha Madhyamakhanda, 39/1, 5th Edition 1988, Pub:Chaukhambha Sanskrita Sansthan, , pp 405. 82) Brahmashankar Shastri, ed., Yogaratnakar, Medhorog Nidhanchikitsa Adhikara-1, Edition:reprint 2005, Pub:Chaukhambha Sanskrit Series, pp 97. 83) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 21/5-7, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 400. 84) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Sutrasthana 15/37, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 62. 85) Vaidya Ranjit Ray Desai ed., Astanga Sangraha Sutrasthan 24/18-22, 2ndEdition1981, Pub: Sri Baidhyanath Ayurveda Bhavan Ltd. Pp 692-694. 86) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 20/17, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 395.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-BIBLIOGRAPHIC REFERENCES
3
87) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Sutrasthana 24/9, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 101. 88) Dr.Brahmanand Tripathi ed., Astanga Hrudayam Sutrasthana 11/26, Edition;Reprint 2007, Pub;Chaukhamba Sanskrit Pratishthan,pp 165. 89) Dr.Brahmanand Tripathi ed., Astanga Hrudayam Sutrasthana 13/25, Edition;Reprint 2007, Pub;Chaukhamba Sanskrit Pratishthan,pp 188. 90) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Sutrasthana 15/32, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 62. 91) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 21/3,4, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 398,399. 92) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Sutrasthana 15/37, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 62. 93) Dr.Brahmanand Tripathi ed., Charaka Samhita Nidanasthana 4/8, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 614. 94) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 21/9, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 401. 95) ibid. 96) ibid 97) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Sutrasthana 15/37, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 62. 98) Vaidya Ranjit Ray Desai ed., Astanga Sangraha Sutrasthan 24/22-24, 2ndEdition1981, Pub: Sri Baidhyanath Ayurveda Bhavan Ltd. Pp 694. 99) Dr.Brahmanand Tripathi ed., Astanga Hrudayam Sutrasthana 14/20, Edition;Reprint 2007, Pub;Chaukhamba Sanskrit Pratishthan,pp 194. 100) Sri Sudarshana Shastri ed., Madhava Nidana 34./9, Edition:Reprint 2007, Pub: Choukhamba Prakashan, pp 29. 101) Pandit Sri Brahma Shankar Sharma ed., Bhavaprakasha Madhyamakhanda, 39/9, 5th Edition 1988, Pub:Chaukhambha Sanskrita Sansthan, , pp 406. 102) Vaidya Ranjit Ray Desai ed., Astanga Sangraha Sutrasthan 24/13-16, 2ndEdition1981, Pub: Sri Baidhyanath Ayurveda Bhavan Ltd. Pp 691,692. 103) Dr.Brahmanand Tripathi ed., Astanga Hrudayam Sutrasthana 14/14, Edition;Reprint 2007, Pub;Chaukhamba Sanskrit Pratishthan,pp 193. 104) Prof. R.K.Srikanthamurthy ed., Sharangadhara Samhita Prathama Khanda 7/65, Edition:6th,2006, Pub: Choukhambha Orientalia, pp 37. 105) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 21/7, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 401. 106) ibid. 107) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Sutrasthana 15/37, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 62. 108) Vaidya Ranjit Ray Desai ed., Astanga Sangraha Sutrasthan 24/29, 2ndEdition1981, Pub: Sri Baidhyanath Ayurveda Bhavan Ltd, pp 694. 109) Dr.Brahmanand Tripathi ed., Astanga Hrudayam Sutrasthana 14/20, Edition;Reprint 2007, Pub;Chaukhamba Sanskrit Pratishthan,pp 194. 110) Prof.Yadunandana Upadhyaya, ed., Madhavanidhana, 34/1-9, Edition: Reprint 2005, Pub:Choukambha Sanskrita Sansthana, , pp 28. 111) Pandit Sri Brahma Shankar Sharma ed., Bhavaprakasha Madhyamakhanda, 39/10, 5th Edition 1988, Pub:Chaukhambha Sanskrita Sansthan, , pp 406. 112) Brahmashankar Shastri, ed., Yogaratnakar, Medhorog Nidhanchikitsa Adhikara-8, Edition:reprint 2005, Pub:Chaukhambha Sanskrit Series, pp 98. 113) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 9/5, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 208. 114) Dr.Brahmanand Tripathi ed., Charaka Samhita Vimanasthana 7/30, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 722. 115) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 21/20, 21. Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 404. 116) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Sutrasthana 15/38, Edition:Reprint 2007,
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-BIBLIOGRAPHIC REFERENCES
4
Pub: Chowkhamba Sanskrit sansthan, pp 62. 117) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 21/21. Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 404. 118) Dr.Brahmanand Tripathi ed., Astanga Hrudayam Sutrasthana 21/5, Edition;Reprint 2007, Pub;Chaukhamba Sanskrit Pratishthan ,pp 252. 119) ibid, 24/12, pp 271. 120) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 23/6-9. Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 422. 121) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 13/53, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 274. 122) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Sutrasthana 45/112, Edition: Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 178. 123) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Chikitsasthana 31/16, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 135. 124) Vaidya Ranjit Ray Desai ed., Astanga Sangraha Sutrasthan 6/100, 2ndEdition1981, Pub: Sri Baidhyanath Ayurveda Bhavan Ltd. Pp 244. 125) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 13/44-46, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 272. 126) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Chikitsasthana 32/15, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 410. 127) ibid. 33/18, pp 143. 128) Prof. P.V.Tewari ed., Kashyapa Samhita, Chikitsastan 2. Edition: Reprint 2002, Pub:Chaukhambha Vishwabharati, pp 163 . 129) Dr.Brahmanand Tripathi ed., Astanga Hrudayam Sutrasthana 14/14, Edition;Reprint 2007, Pub;Chaukhamba Sanskrit Pratishthan,pp 193. 130) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Chikitsasthana 38/82, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 174. 131) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 21/21. Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 404. 132) Prof. R.K.Srikanthamurthy ed., Sharangadhara Samhita Prathama Khanda 4/10, Edition: 6th,2006, Pub: Choukhambha Orientalia, pp 18. 133) Dr.Brahmanand Tripathi ed., Charaka Samhita Sidhisthana10/13,14., Edition:Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 1301. 134) ibid., 3/41, pp 1204. 135) ibid., 10/23,24. pp 1303. 136) Dr.Brahmanand Tripathi ed., Astanga Hrudayam Kalpasthana 4/7-10, Edition;Reprint 2007, Pub;Chaukhamba Sanskrit Pratishthan,pp 750. 137) Prof. R.K.Srikanthamurthy ed., Sharangadhara Samhita Uttara Khanda 6/32,33,. Edition:6th,2006, Pub: Choukhambha Orientalia, pp 219. 138) Pandit Sri Brahma Shankar Sharma ed., Bhavaprakasha Madhyamakhanda, 29/30, 5th Edition 1988, Pub:Chaukhambha Sanskrita Sansthan,. 139) Prof. P.V.Tewari ed., Kashyapa Samhita, Chikitsastan18/13,14. Edition: Reprint 2002, Pub:Chaukhambha Vishwabharati, pp 248. 140) Pandit Sri Brahma Shankar Sharma ed., Bhavaprakasha Madhyamakhanda, 39/12, 5th Edition 1988, Pub:Chaukhambha Sanskrita Sansthan,. 141) Prof. P.V.Tewari ed., Kashyapa Samhita Sidhiathana 2. Edition: Reprint 2002, Pub:Chaukhambha Vishwabharati, pp.266. 142) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Chikitsasthana 37/33-35, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 161. 143) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 22/9. Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 412. 144) ibid., 20/21,22. pp 404. 145) ibid., 21/25-27, pp 405. 146) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Sutrasthana 15/38, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 62. 147) Dr.Brahmanand Tripathi ed., Charaka Samhita Chikitsasthana 6/57, Edition: Reprint 2007,
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-BIBLIOGRAPHIC REFERENCES
5
Pub: Choukhamba Surbharati Prakashan, pp 295. 148) Dr.Brahmanand Tripathi ed., Charaka Samhita Nidanasthana 8/33-35, Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 652. 149) Dorland’s, Pocket Medical Dictionary, 2001, Pp 931, Page No. 600. 150) Harsh Mohan ed., Textbook of pathology, chap.9.Environmental and Nutritional Diseases,Obesity. 5thEdition,2005. Pub: Jaypee Brothers. pp 250. 151) Christipher Haslett ed., Davidson’s Principle and Practice of Medicine, 7.Diabetes Mellitus and Nutritional and Metabolic disorders, Obesity. 8thEdition, 1999. Pub:Churchill Livingstone. pp 527. 152) Damayanti Datta, Society & the arts,FAT of the Matter, INDIA TODAY, June 16, 2008, pp 59. 153) ibid., 154) K.Sembulingam, Essentials of Medical Physiology, Chapter No.67. 3rd Edition, New Delhi, Jaypee Brothers Medical Publishers (P) Ltd, 2005. & 70, Page No. 316-317 & 350. 155) Robert K. Murray ed., Harpers illustrated biochemistry. Section-II Bioenergetics & The metabolism of Carbohydrates and lipids. 25. lipid transport and storage.205-218. 26thedition, 2003. Pub: Mc.Graw-Hill. Pp 205-218. 156) G.S.Sainani ed., API Textbook of Medicine, Section V.Metabolism. Chap.11. Obesity, 6thEdition,1999. Pub: Association of Physicians of India. pp 208,209. 157) Christipher Haslett ed., Davidson’s Principle and Practice of Medicine, 7.Diabetes Mellitus and Nutritional and Metabolic disorders, Obesity. 8thEdition, 1999. Pub:Churchill Livingstone. pp 526. 158) Anthony S. Fauci ed., Harrison’s Principles of Internal Medicine. Part Five- Nutrition, Chap.75. Obesity. 14th Edition, 1998. Pub: Mc. Graw-Hill, Healyh proffesions divisions. pp 454. 159) Hutchison’s, Clinical Methods, Chapter No.7 Editor, Michel Swash, 21st Edition,Saunders an imprint of Elsevier Limited, international Edition, 2004, pp 129. 160) ibid., pp 130. 161) Davidson’s, Principle and Practice of Medicine, editor, Chapter No.7, Christopher Hasleet and Edwin .R.Chilvers, 18th Edition, Churchil livingtone, 1999, pp. 526. 162) Davidson’s, Principle and Practice of Medicine, Chapter No.7 editor, Christopher Hasleet and Edwin .R.Chilvers, 18th Edition, Churchil livingtone, 1999, Page No. 529. 163) Golwalla, Medicine for Students, Chapter No 5,18th Edition, Mumbai,Dr.A.F.Gowalla Empress court Church gate, 1999, Page No 339-340. 164)Harrison’s, Principle of internal Medicine, Vol.-1, Part –5, Chapter No.75, Editor, Anthoni.S.Fauci and Joseph.B.Martin, 14th Editon, international Edition 1998. Page No.459. 165) Anthony S. Fauci ed., Harrison’s Principles of Internal Medicine. Part Five- Nutrition,Chap.75. Obesity. 14th Edition, 1998. Pub: Mc. Graw-Hill, Healyh proffesions divisions. pp 460. 166) ibid., 167) Golwalla, Medicine for Students, Chapter No 5,18th Edition, Mumbai, Dr.A.F.Gowalla Empress court Church gate, 1999, Page No 340. 168) Anthony S. Fauci ed., Harrison’s Principles of Internal Medicine. Part Five- Nutrition,Chap.75. Obesity. 14th Edition, 1998. Pub: Mc. Graw-Hill, Healyh proffesions divisions. pp 460. 169) Christipher Haslett ed., Davidson’s Principle and Practice of Medicine, chapter 10. 8thEdition,1999. Pub:Churchill Livingstone. pp 304. 170) Towards a possible Vaccine against obesity;Hindu, 2nd August 2006, New scope, Page No.20. 171) Christipher Haslett ed., Davidson’s Principle and Practice of Medicine, chapter 10. 8thEdition,1999. Pub:Churchill Livingstone. pp 305. 172) G.S.Sainani ed., API Textbook of Medicine, Section V.Metabolism. Chap.11. Obesity, 6thEdition,1999. Pub: Association of Physicians of India. pp 210. 173) Rober Fear, Obesity Surgery Risks gets bigger; First Bariatric surgery; many methods: Deccan Chronicle July 27th , 2006, Health plus column. 174) Bhishagacharya Harishasti Paradakara Vaidya ed., Astanga Hridaya Sutrasthana, with Arunadatta Commentary 19/11, Reprint 9thEdition 2005, Pub: Choukhamba Orientalia. pp 273. 175) Prof. R.K.Srikanthamurthy ed., Sharangadhara Samhita Uttara Khanda 5/1, Edition:6th,2006, Pub: Choukhambha Orientalia, pp 209. 176) Vaidya Ranjit Ray Desai ed., Astanga Sangraha Sutrasthan 28/3, 2ndEdition1981, Pub: Sri Baidhyanath Ayurveda Bhavan Ltd. Pp 772. 177) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Chikitsasthana 35/6, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 153.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-BIBLIOGRAPHIC REFERENCES
6
178) Prof. P.V.Tewari ed., Kashyapa Samhita Sidhiathana 1/9,10. Edition: Reprint 2002, Pub:Chaukhambha Vishwabharati, pp. 258. 179) Kasture VG, ed., Ayurvediya Panchakarma vigyan, chapter 6, 6th edition,1998. Pub: Shree Baidyanath Ayurved Bhavan Ltd.; pp 373. 180) Kaviraja Ambikadutta Shastri ed., Sushruta Samhita, Chikitsasthana 37/77,14thEdition 2003,, Pub:Chaukhambha Sanskrit Sansthan, pp 164. 181) Pt. Rajeshwara Datta Shastri, ed., Charaka Samhita, Siddhistana, 1/47,48. Edition:Reprint 1998, Pub:Chaukhambha Bharati Academy, pp 973. 182) Kaviraja Ambikadutta Shastri ed., Sushrutha samhitha, Chikitsasthana 35/19, 14thEdition 2003,, Pub: Krishnadas Academy; pp 526 183) Indradev Tripathi,ed. ,ed., Astanga Hridayam sutrasthana 19/61, 1st Edition , 1994. Pub: Krishnadas Academy. Pp 192. 184) Prof. R.K.Srikanthamurthy ed., Sharangadhara Samhita, Uttarakhanda, 6/19-22, 4th Edition 2001, Pub: Chaukhambha Orientalia, pp 218. 185) Pt. Rajeshwara Datta Shastri ed., Charaka Samhita, Siddhistana10/17-42, Edition: Reprint 1998, Pub: Chaukhambha Bharati Academy, pp 1079-1082. 186) Kaviraja Ambikadutta Shastri, ed., Sushruta Samhita, Chikitsasthana, 38/39, 14th Edition 2003, Pub: Chaukhambha Sanskrit Sansthan, pp 171. 187) Pt.Rajeshwara Datta Shastri, ed.,Charaka Samhita, Siddhistana, 8/2-14, Edition: Reprint 1998, Pub: Chaukhambha Bharati Academy, pp 1044. 188)Kaviraja Ambikadutta Shastri, ed., Sushruta Samhita, Chikitsasthana, 38/118, 14th Edition 2003, Pub: Chaukhambha Sanskrit Sansthan, pp 176. 189) Pt. Rajeshwara Datta Shastri, ed., Agnivesh, Charaka Samhita, Siddhistana, 12/15, edition: Reprint 1998, Pub: Chaukhambha Bharati Academy, pp 1096. 190) Kaviraja Ambikadutta Shastri, ed., Sushruta Samhita, Chikitsasthana, 38/116, 14th Edition 2003, Pub: Chaukhambha Sanskrit Sansthan, pp 176. 191) Jain Sankarlalji Vaidya ,ed.,Vangasenasamhitha, Bastikarmaadhikara, -170, Pub: Khemnath Srikrishnadas publishers; 1996. pp 999. 192) Ibid. Bastikarmaadhikara, 186-190, pp 1000. 193) P.V.Sharma, ed., Chakradatta, 73/29, Pub: Chaukhambha Ayurveda series; 2nd edition,1998. pp. 628. 194) Ibid., 73/23-26, pp 627,628. 195) Dr.Brahmanand Tripathi ed., Astanga Hrudayam Chikitsasthana 9/72-76, Edition;Reprint 2007, Pub;Chaukhamba Sanskrit Pratishthan,pp 687. 196) Jain Sankarlalji Vaidya ed.,Vangasenasamhitha, Bastikarmaadhikara -182-185. Pub: Khemnath Srikrishnadas publishers; 1996. pp 999. 197) Pt.Rajeshwara Datta Shastri, ed.,Charaka Samhita, Siddhistana, 6/83, Edition:Reprint 1998, Pub: Chaukhambha Bharati Academy, pp 1031. 198) Kaviraja Ambikadutta Shastri ed.,Sushruta Samhita, Chikitsasthana, 35/18, 14th Edition 2003, Pub:Chaukhambha Sanskrit Sansthan, pp 154. 199) Kaviraja Ambikadutta Shastri ed.,Sushruta Samhita, Chikitsasthana, 38/37-39, Edition: Reprint 2007, Pub:Chaukhambha Sanskrit Sansthan, pp 172. 200) Prof. R.K.Srikanthamurthy ed., Sharangadhara Samhita Uttara Khanda 6/33, Edition:6th,2006, Pub: Choukhambha Orientalia, pp 219. 201) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 21/24. Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 404. 202) Prof.P.V.Sharma ed., Dravyaguna Vignana Vol.II. 186.Bilwa. 7th Edition, 1983, Pub: Chaukhambha Bharati Academy. pp 455-457. 203) Dr.J.L.N.Shastry ed., Dravyaguna Vignana Vol II, Bilwa. 2ndEdition 2005, Pub:Chaukhamba Orientalia, pp 108. 204) Dr.G.S.Panday ed., Bhavaprakasha Nighantu part I. Bilwa.Edition: Reprint 2004, Pub:Chaukhamba Bharati Academy, pp 275. 205) Dr.P.V.Sharma ed., Dravyaguna Vignana Vol II, 84.Agnimantha, Edition: Reprint 2005, Pub:Chaukhamba Bharati Academy, pp 221-223. 206) Dr.J.L.N.Shastry ed., Dravyaguna Vignana Vol II, 91.Agnimantha, 2ndEdition 2005, Pub:Chaukhamba Orientalia, pp 418-420. 207) Dr.P.V.Sharma ed., Dravyaguna Vignana Vol II, 192.Shyanaka, Edition: Reprint 2005,
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-BIBLIOGRAPHIC REFERENCES
7
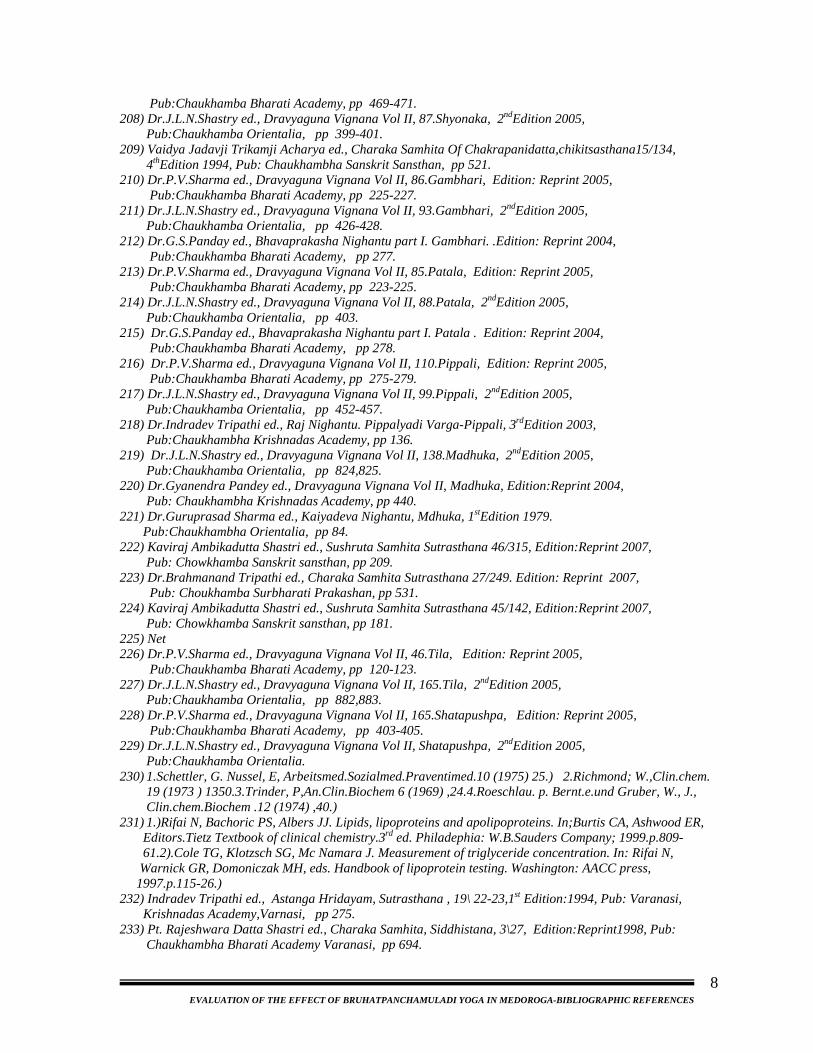
Pub:Chaukhamba Bharati Academy, pp 469-471. 208) Dr.J.L.N.Shastry ed., Dravyaguna Vignana Vol II, 87.Shyonaka, 2ndEdition 2005, Pub:Chaukhamba Orientalia, pp 399-401. 209) Vaidya Jadavji Trikamji Acharya ed., Charaka Samhita Of Chakrapanidatta,chikitsasthana15/134, 4thEdition 1994, Pub: Chaukhambha Sanskrit Sansthan, pp 521. 210) Dr.P.V.Sharma ed., Dravyaguna Vignana Vol II, 86.Gambhari, Edition: Reprint 2005, Pub:Chaukhamba Bharati Academy, pp 225-227. 211) Dr.J.L.N.Shastry ed., Dravyaguna Vignana Vol II, 93.Gambhari, 2ndEdition 2005, Pub:Chaukhamba Orientalia, pp 426-428. 212) Dr.G.S.Panday ed., Bhavaprakasha Nighantu part I. Gambhari. .Edition: Reprint 2004, Pub:Chaukhamba Bharati Academy, pp 277. 213) Dr.P.V.Sharma ed., Dravyaguna Vignana Vol II, 85.Patala, Edition: Reprint 2005, Pub:Chaukhamba Bharati Academy, pp 223-225. 214) Dr.J.L.N.Shastry ed., Dravyaguna Vignana Vol II, 88.Patala, 2ndEdition 2005, Pub:Chaukhamba Orientalia, pp 403. 215) Dr.G.S.Panday ed., Bhavaprakasha Nighantu part I. Patala . Edition: Reprint 2004, Pub:Chaukhamba Bharati Academy, pp 278. 216) Dr.P.V.Sharma ed., Dravyaguna Vignana Vol II, 110.Pippali, Edition: Reprint 2005, Pub:Chaukhamba Bharati Academy, pp 275-279. 217) Dr.J.L.N.Shastry ed., Dravyaguna Vignana Vol II, 99.Pippali, 2ndEdition 2005, Pub:Chaukhamba Orientalia, pp 452-457. 218) Dr.Indradev Tripathi ed., Raj Nighantu. Pippalyadi Varga-Pippali, 3rdEdition 2003, Pub:Chaukhambha Krishnadas Academy, pp 136. 219) Dr.J.L.N.Shastry ed., Dravyaguna Vignana Vol II, 138.Madhuka, 2ndEdition 2005, Pub:Chaukhamba Orientalia, pp 824,825. 220) Dr.Gyanendra Pandey ed., Dravyaguna Vignana Vol II, Madhuka, Edition:Reprint 2004, Pub: Chaukhambha Krishnadas Academy, pp 440. 221) Dr.Guruprasad Sharma ed., Kaiyadeva Nighantu, Mdhuka, 1stEdition 1979. Pub:Chaukhambha Orientalia, pp 84. 222) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Sutrasthana 46/315, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 209. 223) Dr.Brahmanand Tripathi ed., Charaka Samhita Sutrasthana 27/249. Edition: Reprint 2007, Pub: Choukhamba Surbharati Prakashan, pp 531. 224) Kaviraj Ambikadutta Shastri ed., Sushruta Samhita Sutrasthana 45/142, Edition:Reprint 2007, Pub: Chowkhamba Sanskrit sansthan, pp 181. 225) Net 226) Dr.P.V.Sharma ed., Dravyaguna Vignana Vol II, 46.Tila, Edition: Reprint 2005, Pub:Chaukhamba Bharati Academy, pp 120-123. 227) Dr.J.L.N.Shastry ed., Dravyaguna Vignana Vol II, 165.Tila, 2ndEdition 2005, Pub:Chaukhamba Orientalia, pp 882,883. 228) Dr.P.V.Sharma ed., Dravyaguna Vignana Vol II, 165.Shatapushpa, Edition: Reprint 2005, Pub:Chaukhamba Bharati Academy, pp 403-405. 229) Dr.J.L.N.Shastry ed., Dravyaguna Vignana Vol II, Shatapushpa, 2ndEdition 2005, Pub:Chaukhamba Orientalia. 230) 1.Schettler, G. Nussel, E, Arbeitsmed.Sozialmed.Praventimed.10 (1975) 25.) 2.Richmond; W.,Clin.chem. 19 (1973 ) 1350.3.Trinder, P,An.Clin.Biochem 6 (1969) ,24.4.Roeschlau. p. Bernt.e.und Gruber, W., J., Clin.chem.Biochem .12 (1974) ,40.) 231) 1.)Rifai N, Bachoric PS, Albers JJ. Lipids, lipoproteins and apolipoproteins. In;Burtis CA, Ashwood ER, Editors.Tietz Textbook of clinical chemistry.3rd ed. Philadephia: W.B.Sauders Company; 1999.p.809- 61.2).Cole TG, Klotzsch SG, Mc Namara J. Measurement of triglyceride concentration. In: Rifai N, Warnick GR, Domoniczak MH, eds. Handbook of lipoprotein testing. Washington: AACC press, 1997.p.115-26.) 232) Indradev Tripathi ed., Astanga Hridayam, Sutrasthana , 19\ 22-23,1st Edition:1994, Pub: Varanasi, Krishnadas Academy,Varnasi, pp 275. 233) Pt. Rajeshwara Datta Shastri ed., Charaka Samhita, Siddhistana, 3\27, Edition:Reprint1998, Pub: Chaukhambha Bharati Academy Varanasi, pp 694.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-BIBLIOGRAPHIC REFERENCES
8

234) Kaviraja Ambikadutta Shastri ed., Sushruta Samhita, Chikitsasthana, 38\1-6, 14th Edition 2003, Pub: Chaukhambha Sanskrit Sansthan Varanasi, pp 168-169. 235) Indradev Tripathi ed., Astanga Hridayam sutrasthana 19\24-26, 1st Edition 1994, Pub: Krishnadas Academy Varanasi, pp 276. 236) Ibid, 19\ 26-30, pp 276-277. 237) Pt Rajeshwara Datta Shastri ed., Charaka Samhita, Siddhistana, 3\28-29 , Editon:Reprint 1998, Pub: Chaukhambha Bharati Academy, Varanasi, pp 694. 238) Ibid, 3\13-17. pp 692. 239) Dr.Ravi Dutt Tripathi ed., Astangasamgraha, Sutrsthana, 28\19, edition:1996, Pub: Chaukhambha Sanskrita Pratishthan Delhi, pp 491. 240) Laurence L.brunton. PhD edited.,Goodman and Gilman’s The pharmacological Basis of Therapeutics. 3.Drug metabolism, Edition: 11th, Pub:Mc.Graw-Hill Medical publishing Division. Pp 73,74. 241) R.S.Satoskar ed., Pharmacology and pharmacotherapeutics, 19thEdition,2005, Pub: Ramdas Bhatkal for Popular prakashana Pvt. Ltd.,Mumbai. 1. Routes of drug administration and dosage forms. pp 5-9.
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA-BIBLIOGRAPHIC REFERENCES
9
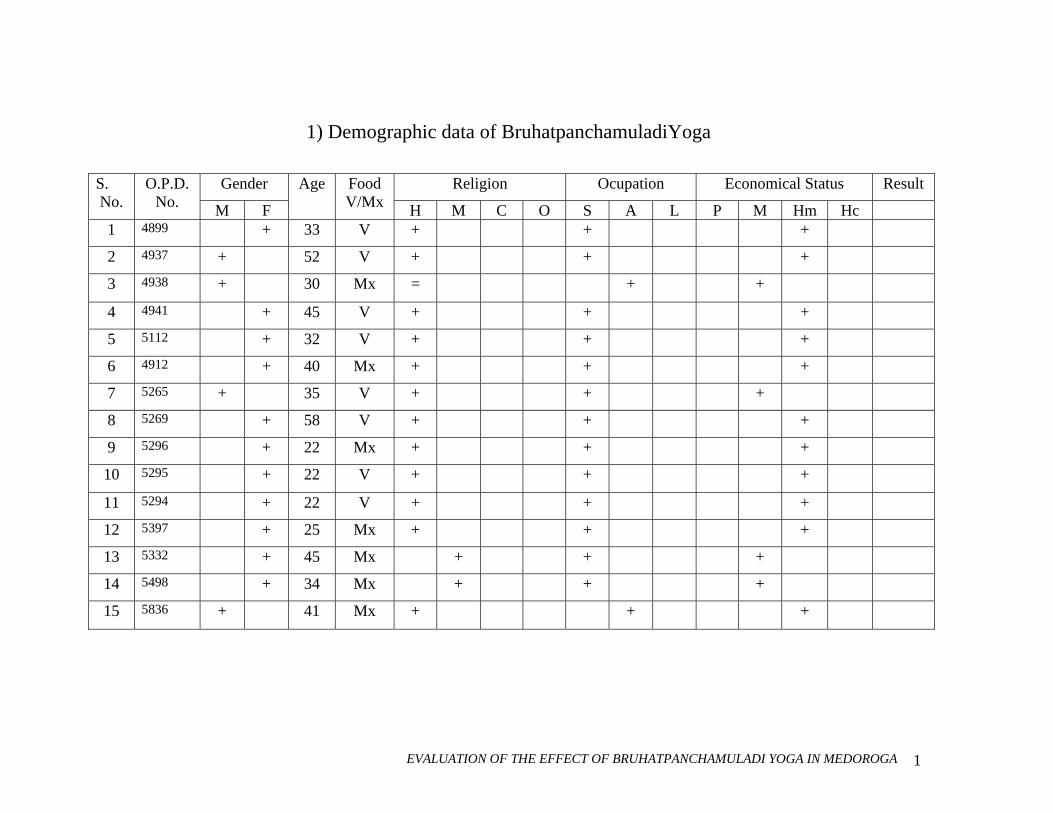
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA 1
1) Demographic data of BruhatpanchamuladiYoga
Gender Religion Ocupation Economical Status Result S. No.
O.P.D. No. M F
Age Food V/Mx H M C O S A L P M Hm Hc
1 4899 + 33 V + + +
2 4937 + 52 V + + +
3 4938 + 30 Mx = + +
4 4941 + 45 V + + +
5 5112 + 32 V + + +
6 4912 + 40 Mx + + +
7 5265 + 35 V + + +
8 5269 + 58 V + + +
9 5296 + 22 Mx + + +
10 5295 + 22 V + + +
11 5294 + 22 V + + +
12 5397 + 25 Mx + + +
13 5332 + 45 Mx + + +
14 5498 + 34 Mx + + +
15 5836 + 41 Mx + + +
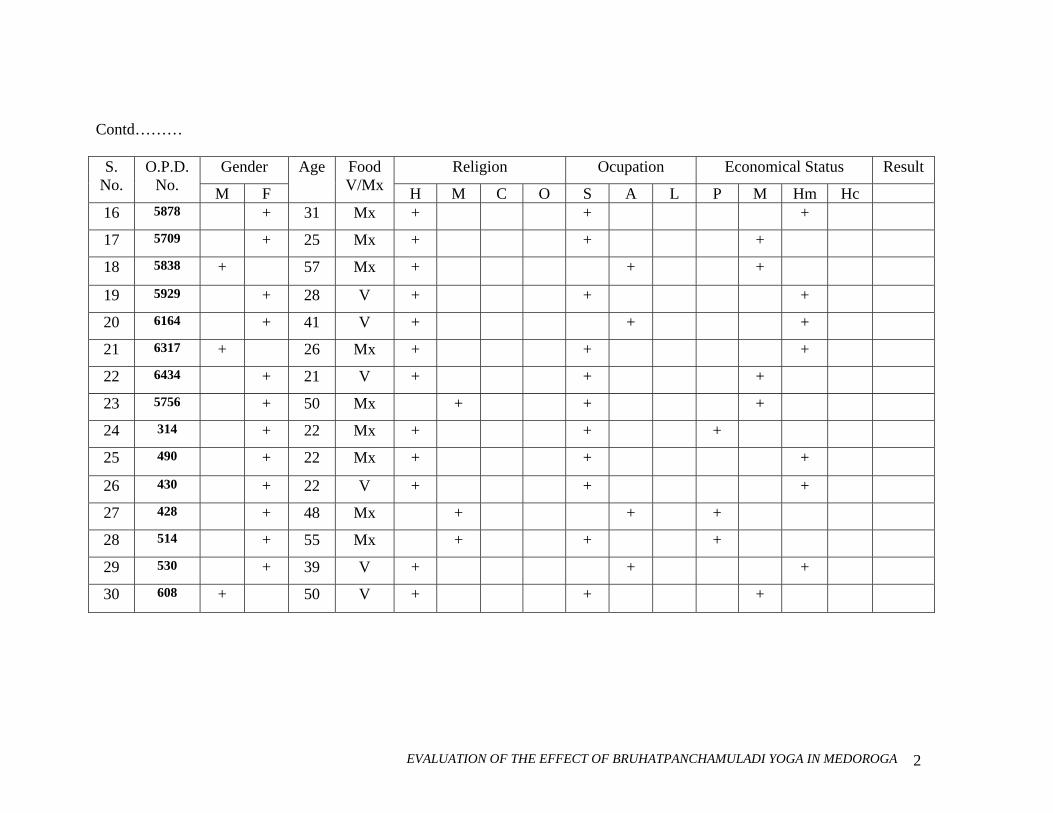
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA 2
Contd………
Gender Religion Ocupation Economical Status Result S. No.
O.P.D. No. M F
Age Food V/Mx H M C O S A L P M Hm Hc
16 5878 + 31 Mx + + +
17 5709 + 25 Mx + + +
18 5838 + 57 Mx + + +
19 5929 + 28 V + + +
20 6164 + 41 V + + +
21 6317 + 26 Mx + + +
22 6434 + 21 V + + +
23 5756 + 50 Mx + + +
24 314 + 22 Mx + + +
25 490 + 22 Mx + + +
26 430 + 22 V + + +
27 428 + 48 Mx + + +
28 514 + 55 Mx + + +
29 530 + 39 V + + +
30 608 + 50 V + + +
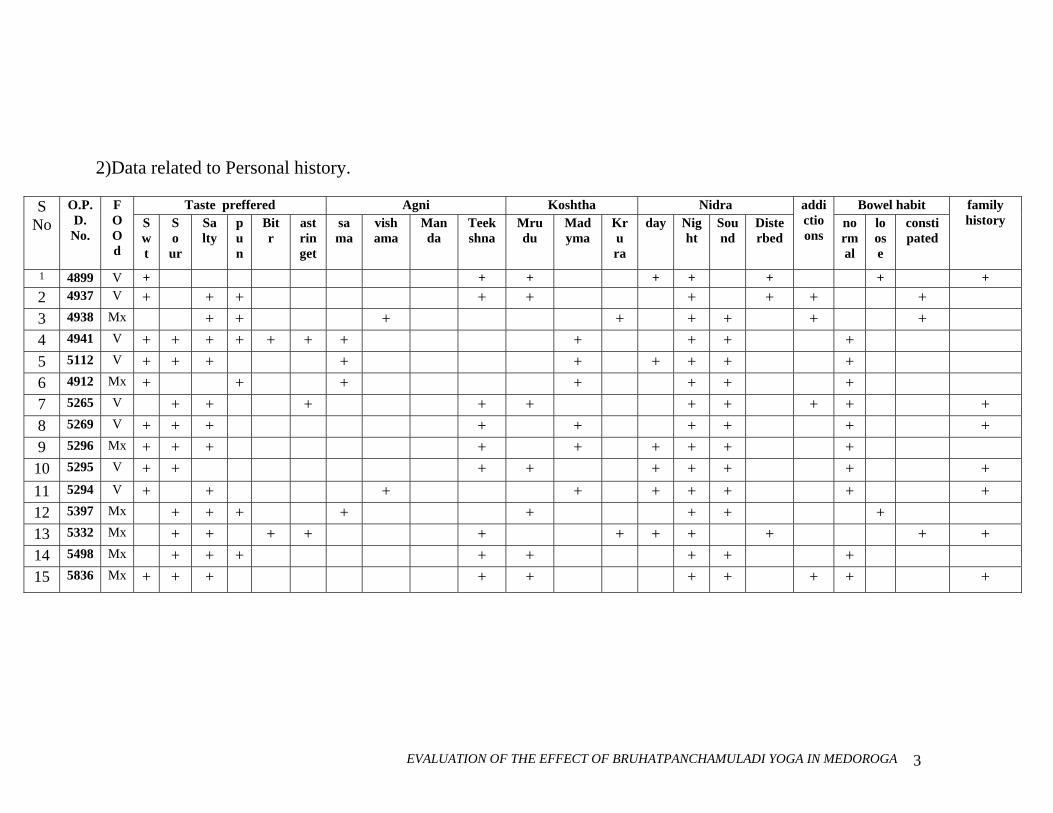
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA 3
2)Data related to Personal history.
Taste preffered Agni Koshtha Nidra Bowel habit S No
O.P.D. No.
F O O d
S wt
S o ur
Sa lty
pun
Bit r
astringet
sama
vish ama
Man da
Teek shna
Mru du
Mad yma
Kru ra
day Nig ht
Sound
Diste rbed
addictioons
normal
loose
constipated
family history
1 4899 V + + + + + + + + 2 4937 V + + + + + + + + + 3 4938 Mx + + + + + + + + 4 4941 V + + + + + + + + + + + 5 5112 V + + + + + + + + + 6 4912 Mx + + + + + + + 7 5265 V + + + + + + + + + + 8 5269 V + + + + + + + + + 9 5296 Mx + + + + + + + + + 10 5295 V + + + + + + + + + 11 5294 V + + + + + + + + + 12 5397 Mx + + + + + + + + 13 5332 Mx + + + + + + + + + + + 14 5498 Mx + + + + + + + + 15 5836 Mx + + + + + + + + + +
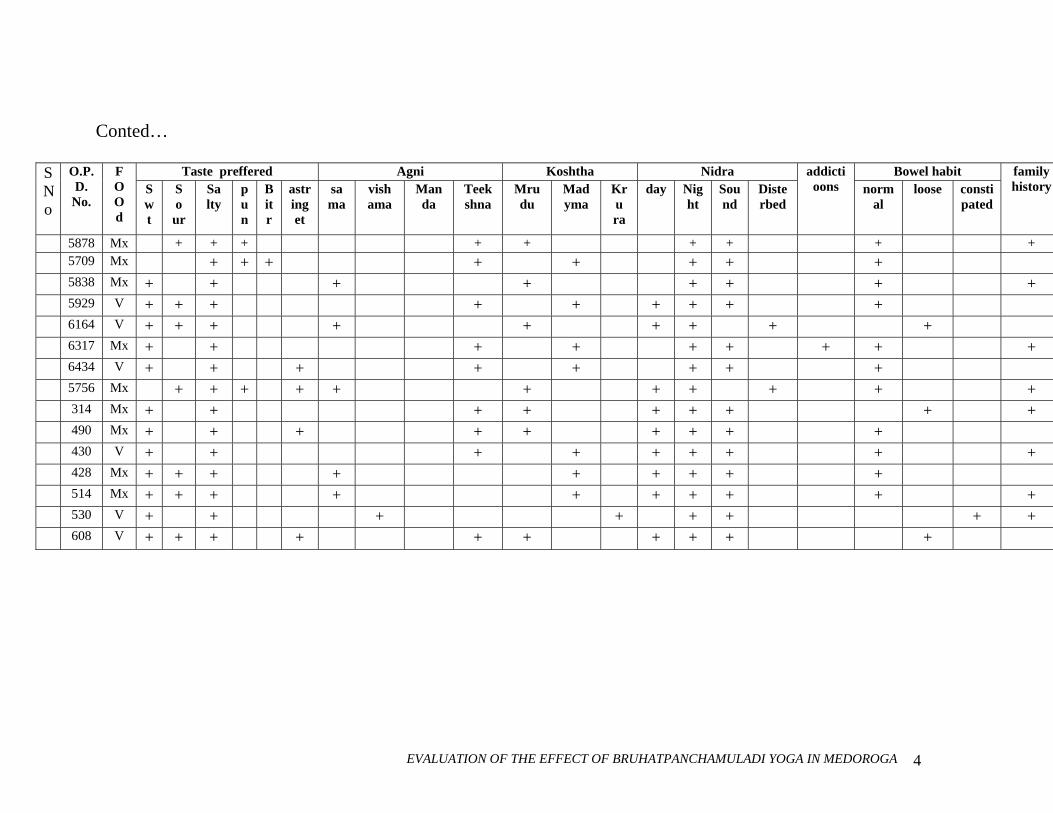
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA 4
Conted…
Taste preffered Agni Koshtha Nidra Bowel habit S No
O.P.D.
No.
F O O d
S wt
S o ur
Sa lty
pun
Bit r
astringet
sama
vish ama
Man da
Teek shna
Mru du
Mad yma
Kru ra
day Nig ht
Sou nd
Diste rbed
addictioons norm
al loose consti
pated
family history
5878 Mx + + + + + + + + + 5709 Mx + + + + + + + + 5838 Mx + + + + + + + + 5929 V + + + + + + + + + 6164 V + + + + + + + + + 6317 Mx + + + + + + + + + 6434 V + + + + + + + + 5756 Mx + + + + + + + + + + + 314 Mx + + + + + + + + + 490 Mx + + + + + + + + + 430 V + + + + + + + + + 428 Mx + + + + + + + + + 514 Mx + + + + + + + + + + 530 V + + + + + + + + 608 V + + + + + + + + + +
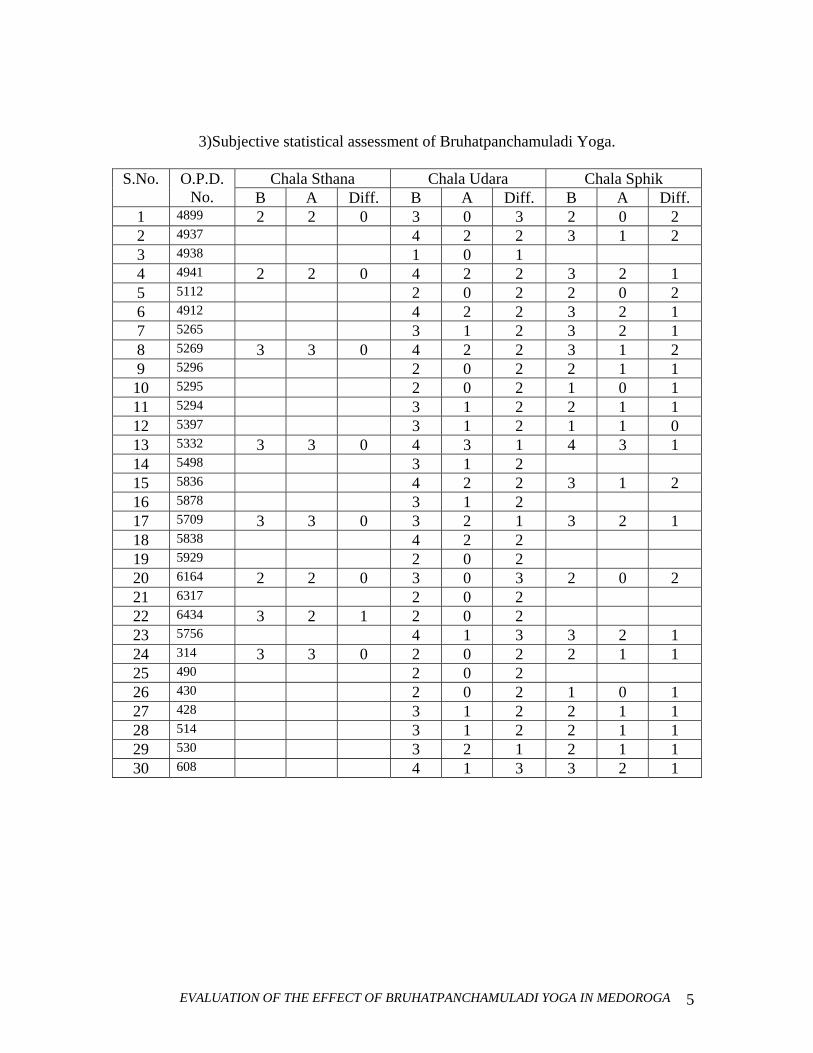
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA 5
3)Subjective statistical assessment of Bruhatpanchamuladi Yoga.
Chala Sthana Chala Udara Chala Sphik S.No. O.P.D. No. B A Diff. B A Diff. B A Diff.
1 4899 2 2 0 3 0 3 2 0 2 2 4937 4 2 2 3 1 2 3 4938 1 0 1 4 4941 2 2 0 4 2 2 3 2 1 5 5112 2 0 2 2 0 2 6 4912 4 2 2 3 2 1 7 5265 3 1 2 3 2 1 8 5269 3 3 0 4 2 2 3 1 2 9 5296 2 0 2 2 1 1 10 5295 2 0 2 1 0 1 11 5294 3 1 2 2 1 1 12 5397 3 1 2 1 1 0 13 5332 3 3 0 4 3 1 4 3 1 14 5498 3 1 2 15 5836 4 2 2 3 1 2 16 5878 3 1 2 17 5709 3 3 0 3 2 1 3 2 1 18 5838 4 2 2 19 5929 2 0 2 20 6164 2 2 0 3 0 3 2 0 2 21 6317 2 0 2 22 6434 3 2 1 2 0 2 23 5756 4 1 3 3 2 1 24 314 3 3 0 2 0 2 2 1 1 25 490 2 0 2 26 430 2 0 2 1 0 1 27 428 3 1 2 2 1 1 28 514 3 1 2 2 1 1 29 530 3 2 1 2 1 1 30 608 4 1 3 3 2 1
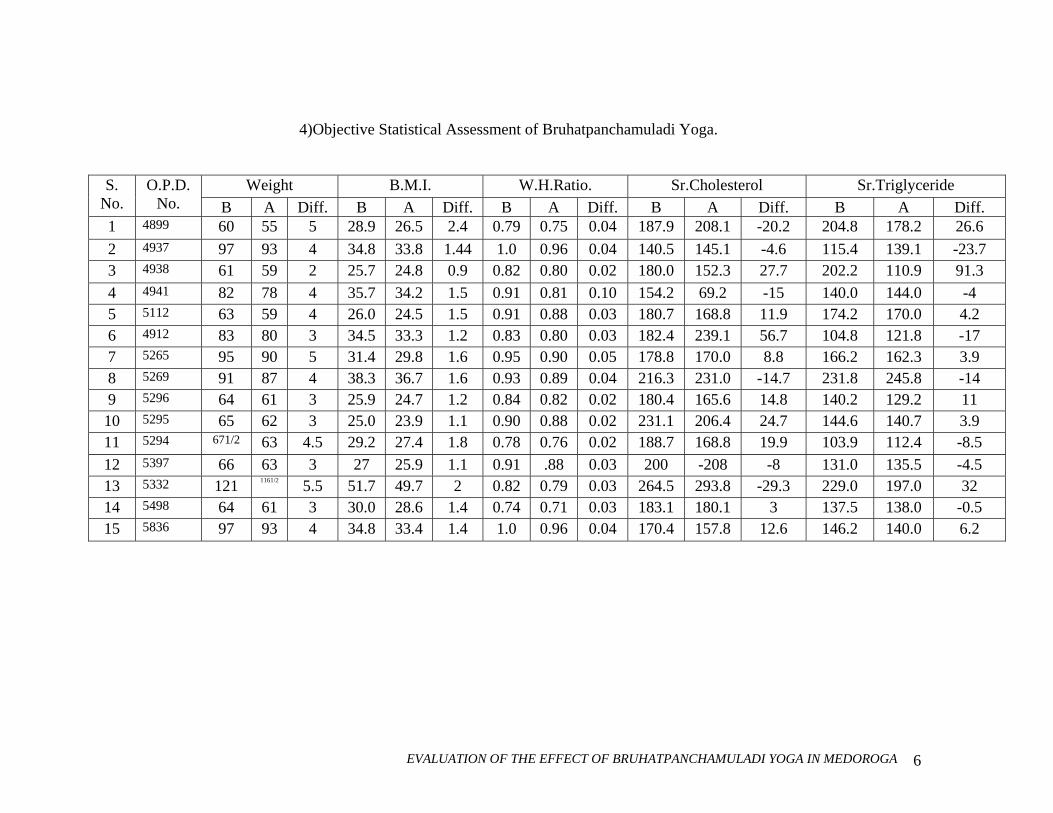
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA 6
4)Objective Statistical Assessment of Bruhatpanchamuladi Yoga.
Weight B.M.I. W.H.Ratio. Sr.Cholesterol Sr.Triglyceride S. No.
O.P.D. No. B A Diff. B A Diff. B A Diff. B A Diff. B A Diff.
1 4899 60 55 5 28.9 26.5 2.4 0.79 0.75 0.04 187.9 208.1 -20.2 204.8 178.2 26.6 2 4937 97 93 4 34.8 33.8 1.44 1.0 0.96 0.04 140.5 145.1 -4.6 115.4 139.1 -23.7 3 4938 61 59 2 25.7 24.8 0.9 0.82 0.80 0.02 180.0 152.3 27.7 202.2 110.9 91.3 4 4941 82 78 4 35.7 34.2 1.5 0.91 0.81 0.10 154.2 69.2 -15 140.0 144.0 -4 5 5112 63 59 4 26.0 24.5 1.5 0.91 0.88 0.03 180.7 168.8 11.9 174.2 170.0 4.2 6 4912 83 80 3 34.5 33.3 1.2 0.83 0.80 0.03 182.4 239.1 56.7 104.8 121.8 -17 7 5265 95 90 5 31.4 29.8 1.6 0.95 0.90 0.05 178.8 170.0 8.8 166.2 162.3 3.9 8 5269 91 87 4 38.3 36.7 1.6 0.93 0.89 0.04 216.3 231.0 -14.7 231.8 245.8 -14 9 5296 64 61 3 25.9 24.7 1.2 0.84 0.82 0.02 180.4 165.6 14.8 140.2 129.2 11 10 5295 65 62 3 25.0 23.9 1.1 0.90 0.88 0.02 231.1 206.4 24.7 144.6 140.7 3.9 11 5294 671/2 63 4.5 29.2 27.4 1.8 0.78 0.76 0.02 188.7 168.8 19.9 103.9 112.4 -8.5 12 5397 66 63 3 27 25.9 1.1 0.91 .88 0.03 200 -208 -8 131.0 135.5 -4.5 13 5332 121 1161/2 5.5 51.7 49.7 2 0.82 0.79 0.03 264.5 293.8 -29.3 229.0 197.0 32 14 5498 64 61 3 30.0 28.6 1.4 0.74 0.71 0.03 183.1 180.1 3 137.5 138.0 -0.5 15 5836 97 93 4 34.8 33.4 1.4 1.0 0.96 0.04 170.4 157.8 12.6 146.2 140.0 6.2
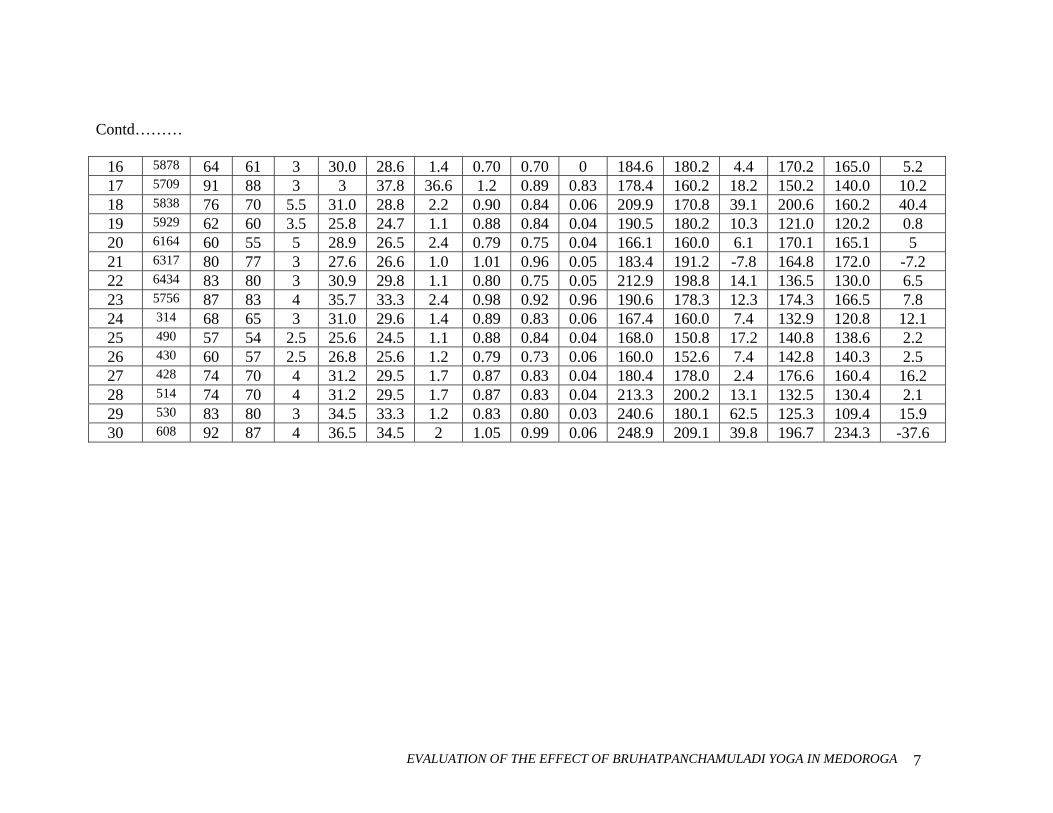
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA 7
Contd………
16 5878 64 61 3 30.0 28.6 1.4 0.70 0.70 0 184.6 180.2 4.4 170.2 165.0 5.2 17 5709 91 88 3 3 37.8 36.6 1.2 0.89 0.83 178.4 160.2 18.2 150.2 140.0 10.2 18 5838 76 70 5.5 31.0 28.8 2.2 0.90 0.84 0.06 209.9 170.8 39.1 200.6 160.2 40.4 19 5929 62 60 3.5 25.8 24.7 1.1 0.88 0.84 0.04 190.5 180.2 10.3 121.0 120.2 0.8 20 6164 60 55 5 28.9 26.5 2.4 0.79 0.75 0.04 166.1 160.0 6.1 170.1 165.1 5 21 6317 80 77 3 27.6 26.6 1.0 1.01 0.96 0.05 183.4 191.2 -7.8 164.8 172.0 -7.2 22 6434 83 80 3 30.9 29.8 1.1 0.80 0.75 0.05 212.9 198.8 14.1 136.5 130.0 6.5 23 5756 87 83 4 35.7 33.3 2.4 0.98 0.92 0.96 190.6 178.3 12.3 174.3 166.5 7.8 24 314 68 65 3 31.0 29.6 1.4 0.89 0.83 0.06 167.4 160.0 7.4 132.9 120.8 12.1 25 490 57 54 2.5 25.6 24.5 1.1 0.88 0.84 0.04 168.0 150.8 17.2 140.8 138.6 2.2 26 430 60 57 2.5 26.8 25.6 1.2 0.79 0.73 0.06 160.0 152.6 7.4 142.8 140.3 2.5 27 428 74 70 4 31.2 29.5 1.7 0.87 0.83 0.04 180.4 178.0 2.4 176.6 160.4 16.2 28 514 74 70 4 31.2 29.5 1.7 0.87 0.83 0.04 213.3 200.2 13.1 132.5 130.4 2.1 29 530 83 80 3 34.5 33.3 1.2 0.83 0.80 0.03 240.6 180.1 62.5 125.3 109.4 15.9 30 608 92 87 4 36.5 34.5 2 1.05 0.99 0.06 248.9 209.1 39.8 196.7 234.3 -37.6
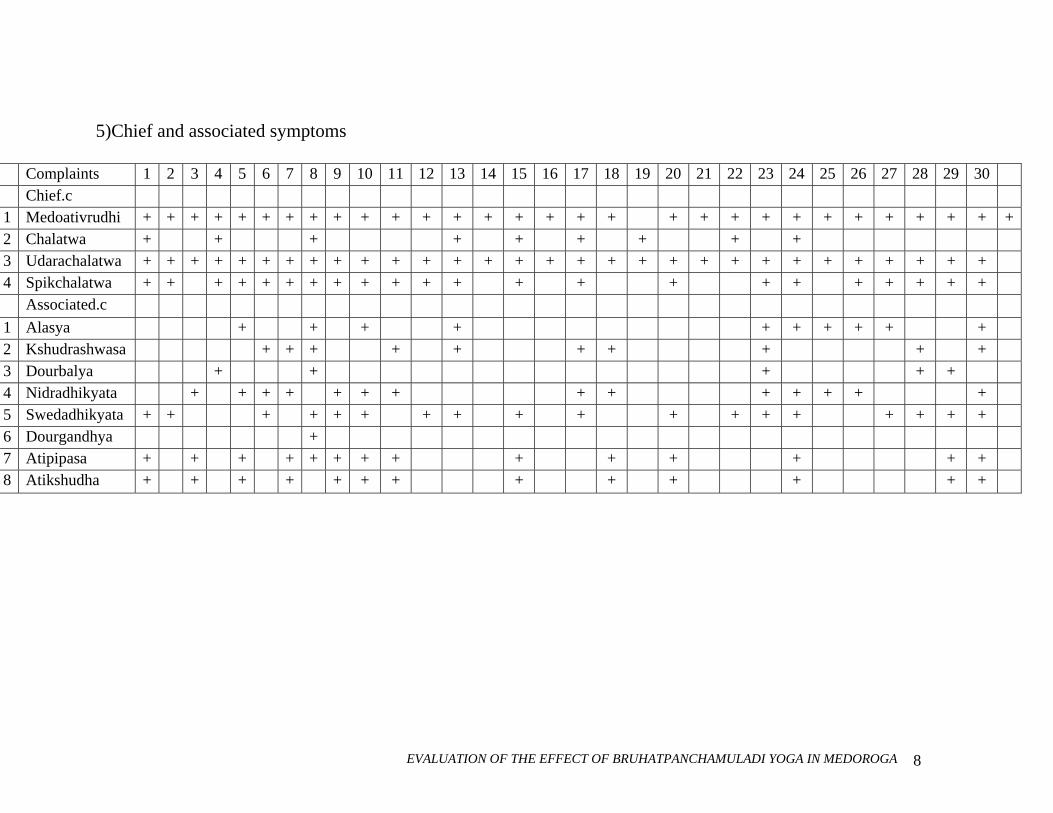
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA 8
5)Chief and associated symptoms
Complaints 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 Chief.c 1 Medoativrudhi + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + 2 Chalatwa + + + + + + + + + 3 Udarachalatwa + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + 4 Spikchalatwa + + + + + + + + + + + + + + + + + + + + + + Associated.c 1 Alasya + + + + + + + + + + 2 Kshudrashwasa + + + + + + + + + + 3 Dourbalya + + + + + 4 Nidradhikyata + + + + + + + + + + + + + + 5 Swedadhikyata + + + + + + + + + + + + + + + + + + 6 Dourgandhya + 7 Atipipasa + + + + + + + + + + + + + + 8 Atikshudha + + + + + + + + + + + + +
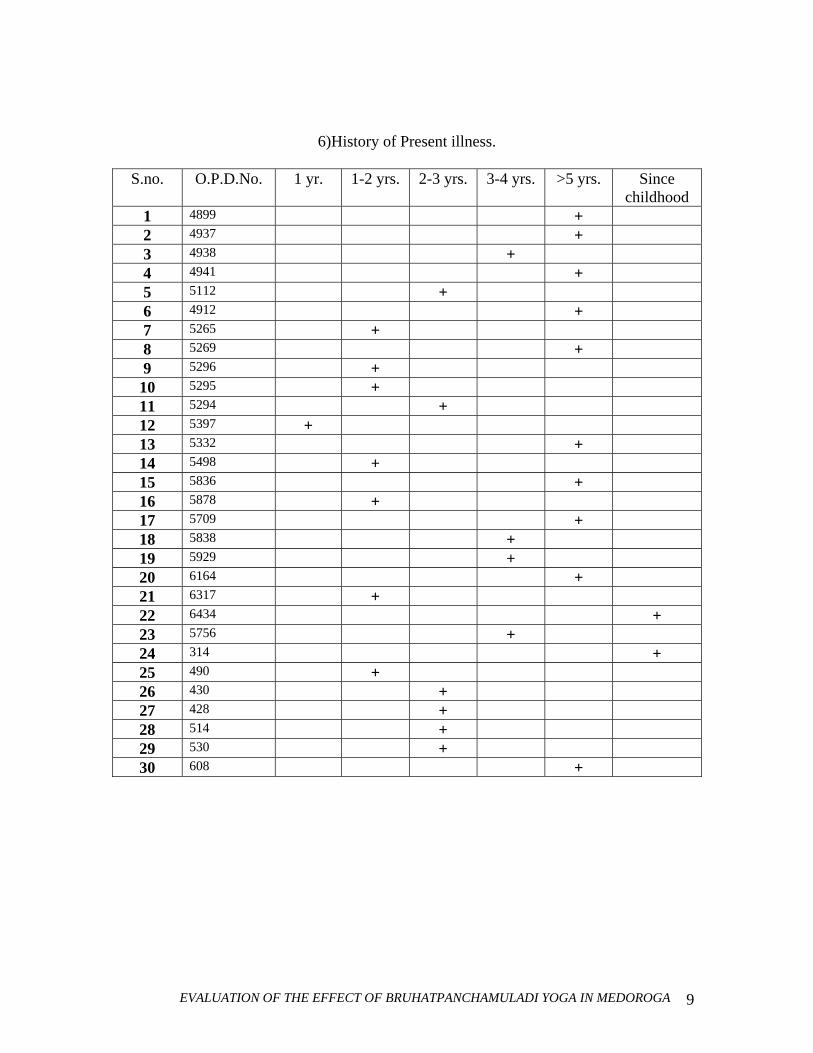
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA 9
6)History of Present illness.
S.no. O.P.D.No. 1 yr. 1-2 yrs. 2-3 yrs. 3-4 yrs. >5 yrs. Since childhood
1 4899 + 2 4937 + 3 4938 + 4 4941 + 5 5112 + 6 4912 + 7 5265 + 8 5269 + 9 5296 + 10 5295 + 11 5294 + 12 5397 + 13 5332 + 14 5498 + 15 5836 + 16 5878 + 17 5709 + 18 5838 + 19 5929 + 20 6164 + 21 6317 + 22 6434 + 23 5756 + 24 314 + 25 490 + 26 430 + 27 428 + 28 514 + 29 530 + 30 608 +
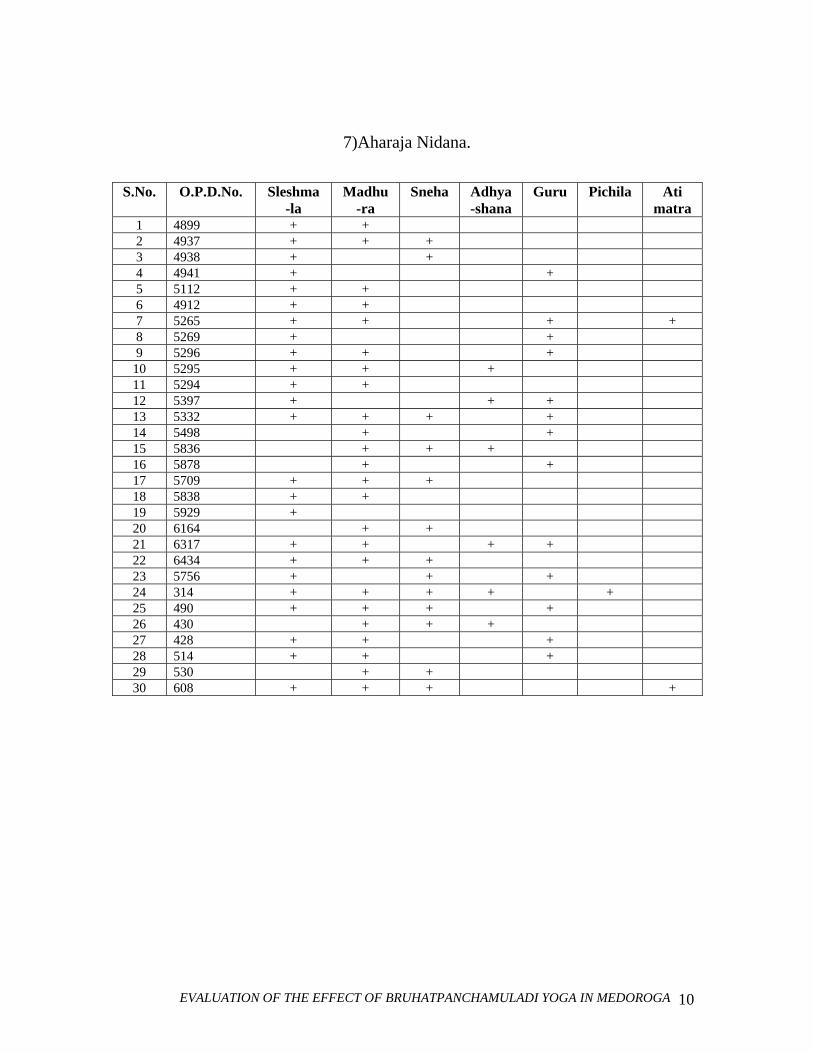
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA 10
7)Aharaja Nidana.
S.No. O.P.D.No. Sleshma -la
Madhu -ra
Sneha Adhya -shana
Guru Pichila Ati matra
1 4899 + + 2 4937 + + + 3 4938 + + 4 4941 + + 5 5112 + + 6 4912 + + 7 5265 + + + + 8 5269 + + 9 5296 + + +
10 5295 + + + 11 5294 + + 12 5397 + + + 13 5332 + + + + 14 5498 + + 15 5836 + + + 16 5878 + + 17 5709 + + + 18 5838 + + 19 5929 + 20 6164 + + 21 6317 + + + + 22 6434 + + + 23 5756 + + + 24 314 + + + + + 25 490 + + + + 26 430 + + + 27 428 + + + 28 514 + + + 29 530 + + 30 608 + + + +
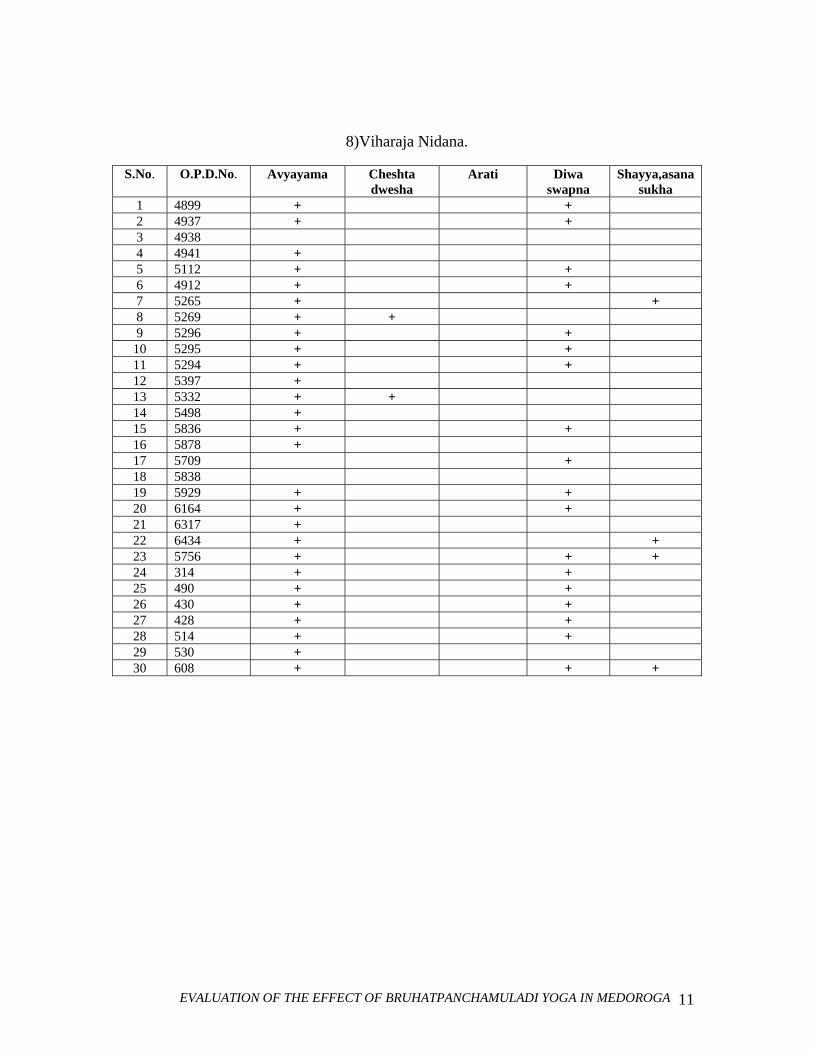
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA 11
8)Viharaja Nidana.
S.No. O.P.D.No. Avyayama Cheshta dwesha
Arati Diwa swapna
Shayya,asanasukha
1 4899 + + 2 4937 + + 3 4938 4 4941 + 5 5112 + + 6 4912 + + 7 5265 + + 8 5269 + + 9 5296 + +
10 5295 + + 11 5294 + + 12 5397 + 13 5332 + + 14 5498 + 15 5836 + + 16 5878 + 17 5709 + 18 5838 19 5929 + + 20 6164 + + 21 6317 + 22 6434 + + 23 5756 + + + 24 314 + + 25 490 + + 26 430 + + 27 428 + + 28 514 + + 29 530 + 30 608 + + +
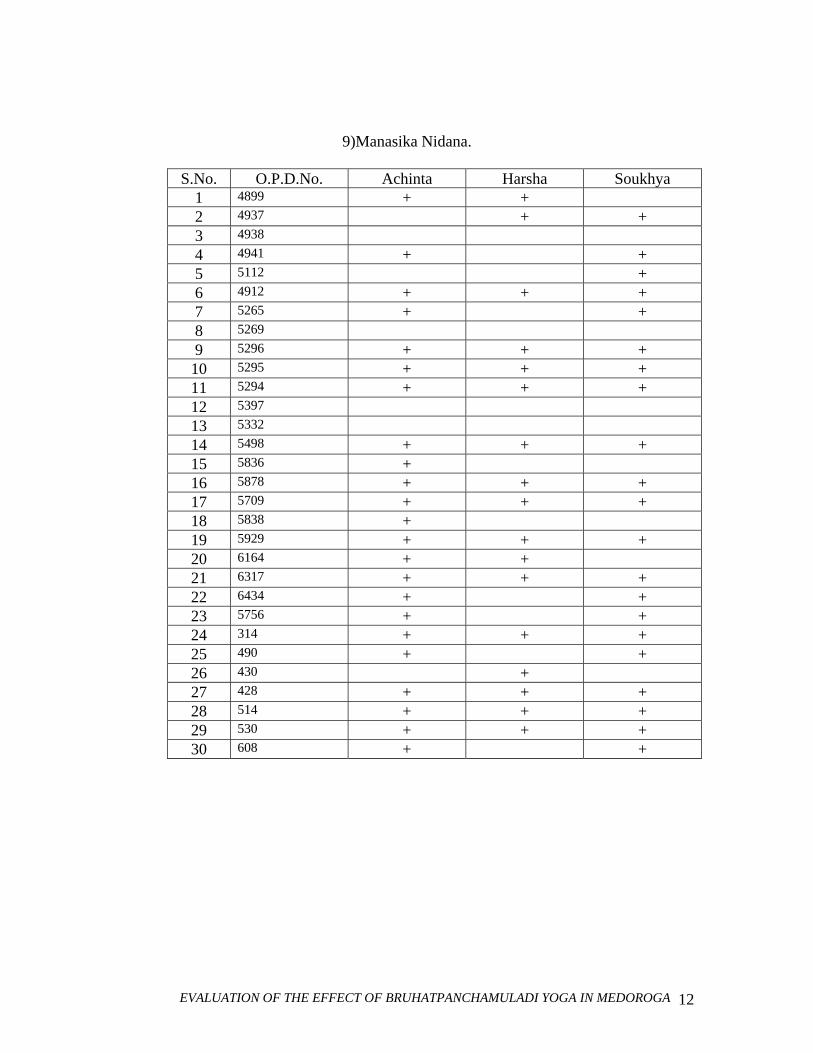
EVALUATION OF THE EFFECT OF BRUHATPANCHAMULADI YOGA IN MEDOROGA 12
9)Manasika Nidana.
S.No. O.P.D.No. Achinta Harsha Soukhya 1 4899 + + 2 4937 + + 3 4938 4 4941 + + 5 5112 + 6 4912 + + + 7 5265 + + 8 5269 9 5296 + + + 10 5295 + + + 11 5294 + + + 12 5397 13 5332 14 5498 + + + 15 5836 + 16 5878 + + + 17 5709 + + + 18 5838 + 19 5929 + + + 20 6164 + + 21 6317 + + + 22 6434 + + 23 5756 + + 24 314 + + + 25 490 + + 26 430 + 27 428 + + + 28 514 + + + 29 530 + + + 30 608 + +
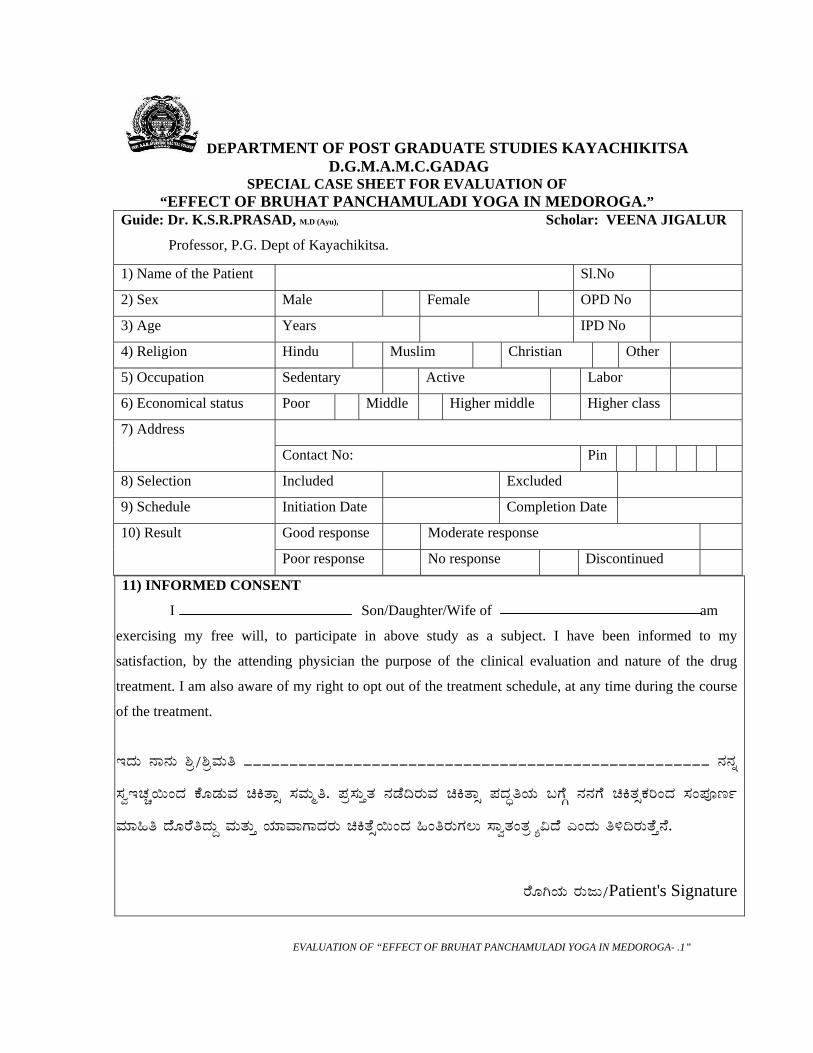
DEPARTMENT OF POST GRADUATE STUDIES KAYACHIKITSA D.G.M.A.M.C.GADAG
SPECIAL CASE SHEET FOR EVALUATION OF “EFFECT OF BRUHAT PANCHAMULADI YOGA IN MEDOROGA.”
Guide: Dr. K.S.R.PRASAD, M.D (Ayu), Scholar: VEENA JIGALUR
Professor, P.G. Dept of Kayachikitsa.
1) Name of the Patient Sl.No
2) Sex Male Female OPD No
3) Age Years IPD No
4) Religion Hindu Muslim Christian Other
5) Occupation Sedentary Active Labor
6) Economical status Poor Middle Higher middle Higher class
7) Address
Contact No: Pin
8) Selection Included Excluded
9) Schedule Initiation Date Completion Date
Good response Moderate response 10) Result
Poor response No response Discontinued
11) INFORMED CONSENT
I Son/Daughter/Wife of am
exercising my free will, to participate in above study as a subject. I have been informed to my
satisfaction, by the attending physician the purpose of the clinical evaluation and nature of the drug
treatment. I am also aware of my right to opt out of the treatment schedule, at any time during the course
of the treatment.
EzÀÄ £Á£ÀÄ ²æ/²æªÀÄw ___________________________________________________ £À£Àß
¸ÀéEZÀѬÄAzÀ PÉÆqÀĪÀ aQvÁì ¸ÀªÀÄäw. ¥Àæ¸ÀÄÛvÀ £ÀqÉ¢gÀĪÀ aQvÁì ¥ÀzÀÞwAiÀÄ §UÉÎ £À£ÀUÉ aQvÀìPÀjAzÀ ¸ÀA¥ÀÇtð
ªÀiÁ»w zÉÆgÉwzÀÄÝ ªÀÄvÀÄÛ AiÀiÁªÁUÁzÀgÀÄ aQvÉì¬ÄAzÀ »AwgÀÄUÀ®Ä ¸ÁévÀAvÀæ÷å«zÉ JAzÀÄ w½¢gÀÄvÉÛ£É.
gÉÆVAiÀÄ gÀÄdÄ/Patient's Signature
EVALUATION OF “EFFECT OF BRUHAT PANCHAMULADI YOGA IN MEDOROGA- .1”
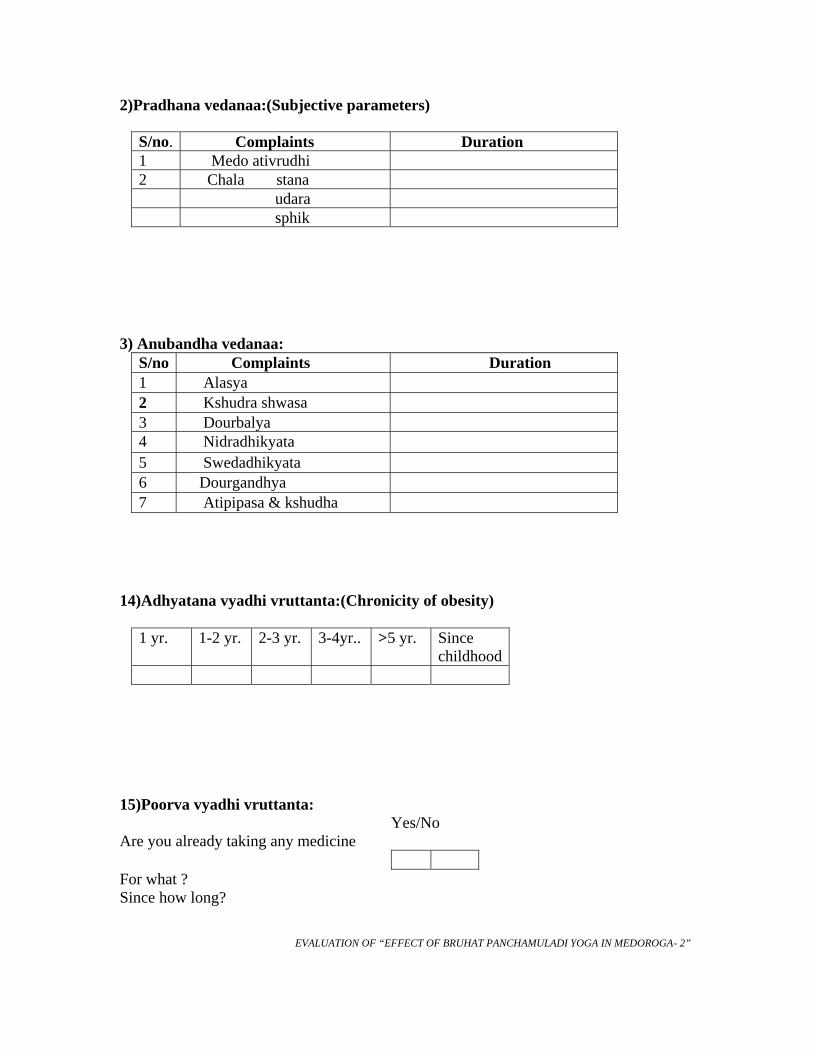
2)Pradhana vedanaa:(Subjective parameters)
S/no. Complaints Duration 1 Medo ativrudhi 2 Chala stana udara sphik
3) Anubandha vedanaa:
S/no Complaints Duration 1 Alasya 2 Kshudra shwasa 3 Dourbalya 4 Nidradhikyata 5 Swedadhikyata 6 Dourgandhya 7 Atipipasa & kshudha
14)Adhyatana vyadhi vruttanta:(Chronicity of obesity)
1 yr. 1-2 yr. 2-3 yr. 3-4yr.. >5 yr. Since childhood
15)Poorva vyadhi vruttanta: Yes/No Are you already taking any medicine
For what ? Since how long? EVALUATION OF “EFFECT OF BRUHAT PANCHAMULADI YOGA IN MEDOROGA- 2”
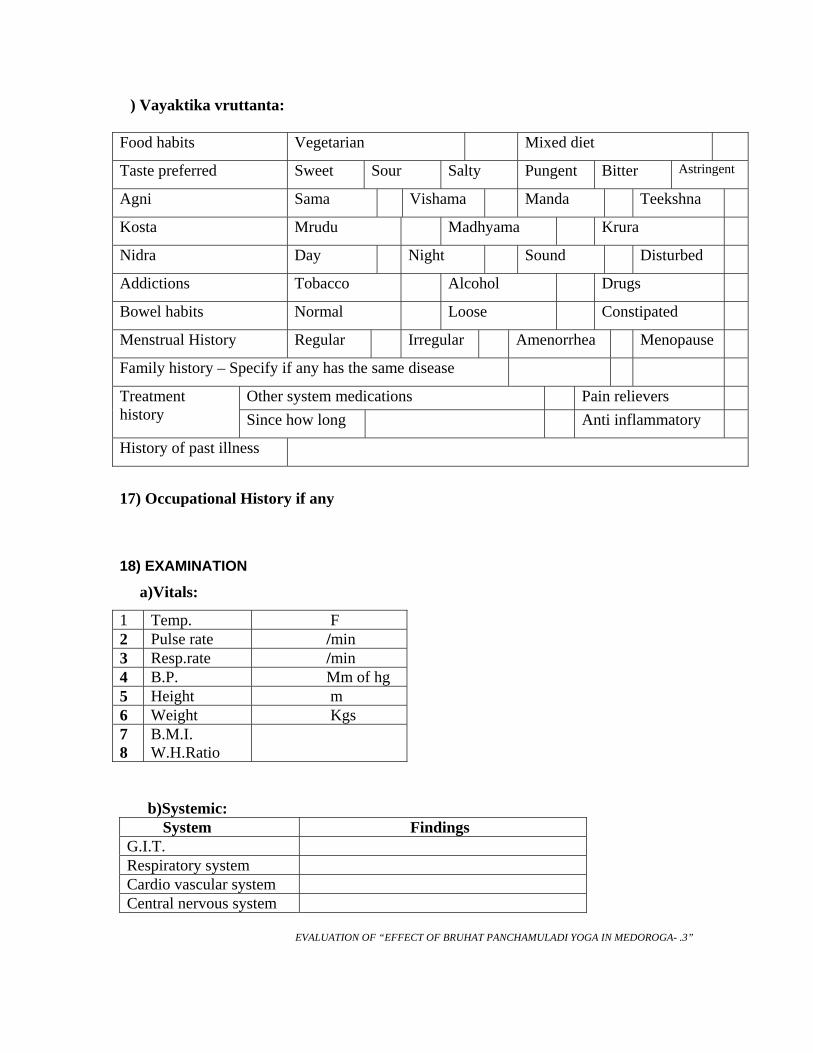
) Vayaktika vruttanta: Food habits Vegetarian Mixed diet
Taste preferred Sweet Sour Salty Pungent Bitter Astringent
Agni Sama Vishama Manda Teekshna
Kosta Mrudu Madhyama Krura
Nidra Day Night Sound Disturbed
Addictions Tobacco Alcohol Drugs
Bowel habits Normal Loose Constipated
Menstrual History Regular Irregular Amenorrhea Menopause
Family history – Specify if any has the same disease
Other system medications Pain relievers Treatment history Since how long Anti inflammatory
History of past illness
17) Occupational History if any
18) EXAMINATION
a)Vitals:
1 Temp. F 2 Pulse rate /min 3 Resp.rate /min 4 B.P. Mm of hg 5 Height m 6 Weight Kgs 7 8
B.M.I. W.H.Ratio
b)Systemic: System Findings G.I.T. Respiratory system Cardio vascular system Central nervous system
EVALUATION OF “EFFECT OF BRUHAT PANCHAMULADI YOGA IN MEDOROGA- .3”
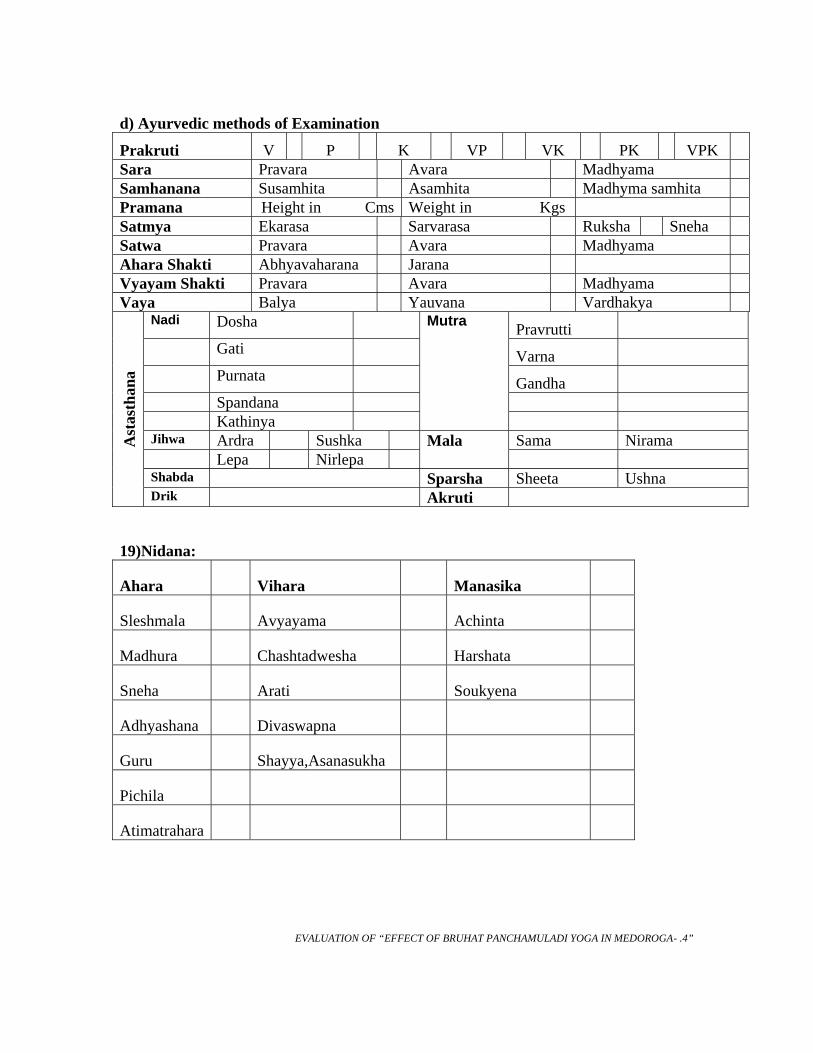
d) Ayurvedic methods of Examination
Prakruti V P K VP VK PK VPK
Sara Pravara Avara Madhyama Samhanana Susamhita Asamhita Madhyma samhita Pramana Height in Cms Weight in Kgs Satmya Ekarasa Sarvarasa Ruksha Sneha Satwa Pravara Avara Madhyama Ahara Shakti Abhyavaharana Jarana Vyayam Shakti Pravara Avara Madhyama Vaya Balya Yauvana Vardhakya
Nadi Dosha Pravrutti Gati Varna Purnata Gandha Spandana Kathinya
Mutra
Jihwa Ardra Sushka Sama Nirama Lepa Nirlepa
Mala
Shabda Sparsha Sheeta Ushna
Ast
asth
ana
Drik Akruti
19)Nidana:
Ahara Vihara Manasika
Sleshmala Avyayama Achinta
Madhura Chashtadwesha Harshata
Sneha Arati Soukyena
Adhyashana Divaswapna
Guru Shayya,Asanasukha
Pichila
Atimatrahara EVALUATION OF “EFFECT OF BRUHAT PANCHAMULADI YOGA IN MEDOROGA- .4”
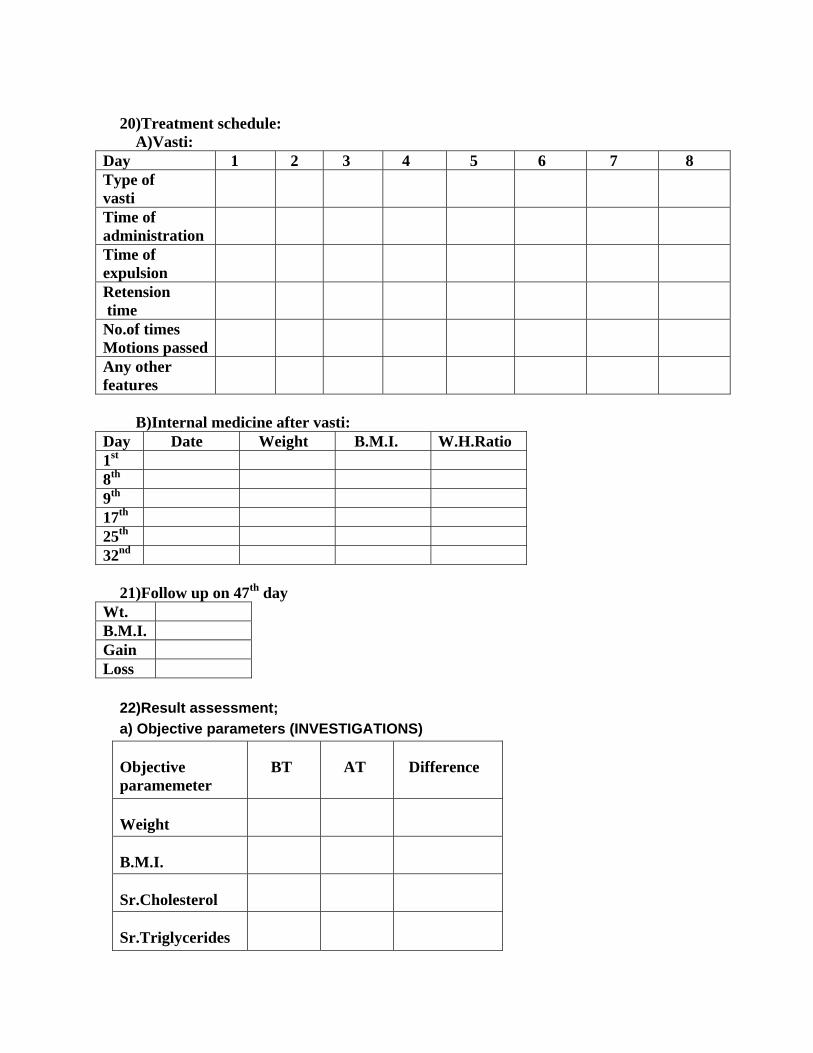
20)Treatment schedule: A)Vasti:
Day 1 2 3 4 5 6 7 8 Type of vasti
Time of administration
Time of expulsion
Retension time
No.of times Motions passed
Any other features
B)Internal medicine after vasti:
Day Date Weight B.M.I. W.H.Ratio 1st 8th 9th 17th 25th 32nd
21)Follow up on 47th day
Wt. B.M.I. Gain Loss
22)Result assessment; a) Objective parameters (INVESTIGATIONS)
Objective paramemeter
BT AT Difference
Weight
B.M.I.
Sr.Cholesterol
Sr.Triglycerides
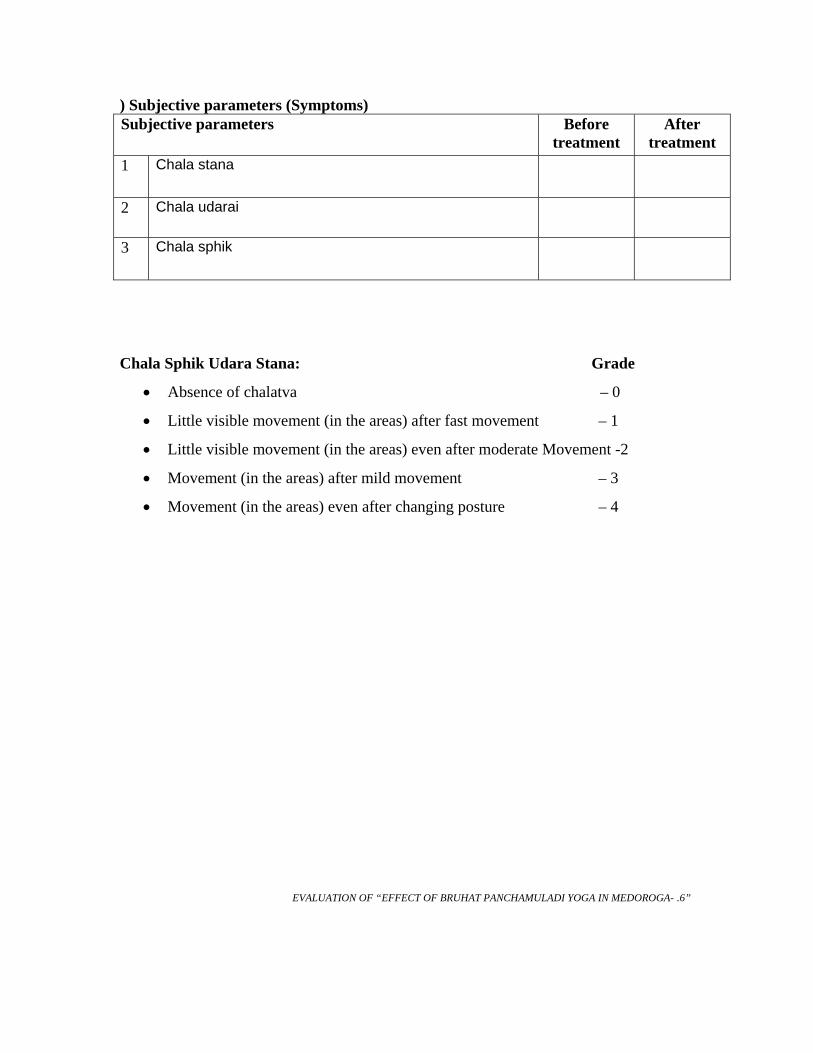
) Subjective parameters (Symptoms) Subjective parameters Before
treatment After
treatment 1 Chala stana
2 Chala udarai
3 Chala sphik
Chala Sphik Udara Stana: Grade
• Absence of chalatva – 0
• Little visible movement (in the areas) after fast movement – 1
• Little visible movement (in the areas) even after moderate Movement -2
• Movement (in the areas) after mild movement – 3
• Movement (in the areas) even after changing posture – 4
EVALUATION OF “EFFECT OF BRUHAT PANCHAMULADI YOGA IN MEDOROGA- .6”





























