Embed Size (px)
Citation preview

Quality in Health Care 1997;6:165-169
Strategies to improve the quality of oral healthcare for frail and dependent older people
J G Steele, AW G Walls
AbstractThe dental profile of the population ofmost industrialized countries is changing.For the first time in at least a century mostelderly people in the United Kingdom willsoon have some oftheir own natural teeth.This could be beneficial for the frail anddependent elderly, as natural teeth areassociated with greater dietary freedom ofchoice and good nutrition. There may alsobe problems including high levels ofdental disease associated with poor hy-giene and diet. New data from a nationaloral health survey in Great Britain is pre-sented. The few dentate elderly people ininstitutions at the moment have poorhygiene and high levels of dental decay. Ifthese problems persist as dentate youngergenerations get older, the burden of carewill be substantial. Many dental problemsin elderly people are preventable or wouldbenefit from early intervention. Strategiesto approach these problems are pre-sented.(Quality in Health Care 1997;6:165-169)
Keywords: dental care; elderly
Department ofRestorative Dentistry,Dental School,Framlington Place,Newcastle upon TyneNE2 4BWJ G Steele, lecturer inrestorative dentistryAW G Walls, professorin restorative dentistry
Correspondence to:Professor AW G Walls,Department of RestorativeDentistry, Dental School,Framlington Place,Newcastle upon TyneNE2 4BW, UK.
Accepted for publication30 June 1997
IntroductionConcerns over the quality of oral health care
for frail or dependent elderly people are notsomething to which industrialised societieshave traditionally been very accustomed. For as
long as institutionalised care of the very old hasbeen a feature of our way of life, being elderlyhas been associated with being toothless.Historically, the dental care required by mostof this population amounted to no more thanoccasional replacement of complete dentures.Disease associated with the soft tissues oc-
curred but, with the exception of oral cancer,did not require complex treatment. For most ofthe population the options were limited, thecosts low, and the results predictable, althoughnot always ideal. The people who retainednatural teeth into advanced age were suffi-ciently few to be manageable within existingframeworks of care, and oral health tended tobe low on a list of priorities for health care inelderly people.However, the need for oral health care in
dependent elderly people will soon be a muchbigger issue. The key to this is the profoundalteration in the dental state of the population,a change which has been shown clearly in Brit-ain and which is being mirrored throughoutmuch of the developed world.' Retention ofsome natural teeth into old age was a rarityuntil recently. In 1968, 88% of the over 75 yearolds in England and Wales had no natural
teeth,2 many having been rendered edentulousbefore the second world war. Since the war, theyounger groups in the population have retainedtheir natural teeth much longer; this is at leastpartly due to the increased availability ofaffordable dental care combined with anincreasing desire to retain natural teeth. Thefirst wave of this group of dentate peoplereached adulthood during the second worldwar and have now been of pensionable age forsome time. We are just starting to see the firstmajor changes in the dental status of the oldestmembers of the United Kingdom population,although some other countries are furtherdown this line.' Predictions from data recordedin 1968, 1978, and 1988 in the UnitedKingdom suggest that there will be at least athreefold increase in the proportion of the 75and over age group who have teeth (from 20%up to 68%) over the 30 year period from 1988to 2018. This is predicted to increase further to81% over the subsequent 20 years.3With planning and awareness, the wide-
spread retention of natural teeth among frailand dependent elderly people could bring con-siderable benefits in terms of health andwellbeing. There is good evidence to show that,when sufficient teeth are retained in a reason-able condition, dietary intake is improved andgeneral health, wellbeing, and satisfaction withoral function tend to be higher than in theedentulous and those with a very limited natu-ral dentition."7 However, the improvements inoral health which have led to the retention ofteeth into old age also have the potential tobring with them a new set of problems whichneed to be solved.There is a substantial and growing body of
evidence to link advanced periodontal diseaseand oral sepsis associated with remaining natu-ral teeth to serious problems with generalhealth. There is evidence suggesting fairlystrong specific associations between coronaryheart disease and perhaps also stroke, and den-tal disease.8"'0 Poor dental state (specificallypoor hygiene) has also been associated withfatal chest infection in frail dependent elderlypeople." Although the evidence for all of theseassociations is, as yet, inconclusive, it isgrowing and looks increasingly convincing.
Natural teeth in the future generations ofvery old people will often be there only by vir-tue of a lifetime of repeated restorativetreatment, such as fillings, root fillings andcrowns. Even with no further disease, themaintenance of existing restorations will be asubstantial undertaking. However, there areadditional concerns about the susceptibility ofelderly people to forms of disease which
165

Steele, Walls
Table 1 Percentage dentate in the United Kingdomnational diet and nutrition survey (NDNS) of adults agede 65
With naturalSample group Weighted base teeth (Oo)
Institution 274 21Free living:
All ages 879 5165-74 y 534 6075-84 y 278 40>85 y 69 23
predominantly affect older people. Foremostamong these is decay of the roots of the teeth, aform of dental caries which is of little relevanceto younger people, but as gums recede rootssusceptible to decay are exposed. This becomesmuch more prevalent in elderly people. In veryold people additional factors, related to use ofmedication and dietary changes, increase therisk of root caries substantially.'2-14Although many of the common conditions
affecting natural teeth are difficult to treat invery old and frail subjects, they may be easier toprevent. Control of diet and good hygienecombined with early detection and simple pre-ventive treatment of early disease may be suffi-cient to prevent or slow down root decay andgood hygiene is essential to the control of peri-odontal disease, 16 but these measures needstrategic planning both at an individual and apopulation level. If there is no strategic aware-ness and no implementation of effectiveprevention, the result will be discomfort andcost to these subjects, logistic problems forcarers who have to organise treatment, and aneconomic burden for the rest of society.
The oral health of frail and dependentelderly people: is there a problem?The evidence we have on the oral health of thisgroup is limited, but what there is suggests thatoral health is poor. Historically, many of thestudies were of those with no natural teeth, asthere were few elderly people in institutionswith natural teeth. These indicated that thequality of dentures and of oral hygiene were notgood.'7 18 Limited data for dentate people sug-gest similar problems of poor hygiene anddisease,'9-23 and this seems to be an inter-national phenomenon.Some of the more recent data for frail and
dependent elderly people come from the oralhealth survey which was part of the recentnational diet and nutrition survey (NDNS)conducted in Britain in 1994-5.24 25 Thissurvey was commissioned by the Departmentsof Health in England, Wales, and Scotland and
Table 2 Percentage of the dentate participants with a functional dentition of 21 or moreteeth
Free living
Institution Total 65-74 75 (¢ 85)
Base (unweighted) 57 405 220 185 (43)Base (weighted) 55 451 323 128 (16)Functional dentition (%) 16 26 32 22 (5)Mean number teeth 10.7 15.5 16.1 13.9 (10.1)Decayed or unsound teeth(mean number) 3.3 1.7 1.7 1.9 (2.5)
Decayed or unsound teeth (%) 31 11 11 14 (25)
the Ministry of Agriculture, Fisheries, andFood. Although detailed data are awaitingpublication, the tables summarise some of thekey findings and give a good indication of theoral health of people in institutions in GreatBritain. The participants in the oral health sur-vey included a nationally representative ran-dom sample of people aged 65 and over livingin residential institutions. There was also alarger sample of free living people aged 65years and over. The samples are weighted toreflect the national population living in institu-tions, and the free living population aged 65 orover respectively. The two samples (free livingand in an institution) should not be compareddirectly as they are not matched for age andsex, both of which are related to oral status;however, even taking into account the differ-ences in the make up of the samples, a numberof trends are evident.
Table 1 indicates very clearly how close weare to having the first generation of dentatevery old people (aged 85 or over) in the UnitedKingdom. The age related trend in thepercentage of dentate people which is showndoes not indicate that teeth are lost rapidly withage. National data have been followed up since1968 and the apparent steep increase in thepercentage with natural teeth with reducingage group represents a cohort effect reflectinghistoric and current patterns of care. Thisincrease in the proportion of the populationwith natural teeth represents the leading edgeof a tidal wave of natural teeth which has nowreached the 75-84 year age band. The dentateproportion in the institution sample (21%) issimilar to the 85 and over age group of free liv-ing people(23%).
Table 2 shows that although there are manydentate older adults, most have a very reduceddentition. More than 20 teeth is often used as athreshold for a dentition which is functionalwithout the need for partial dentures. Evenamong the people with natural teeth, thepercentage with 21 or more is small, even in theyounger group (65-74) it is 32%. Many of therest of those with teeth will rely upon a denturecombined with their natural teeth to give thema functioning dentition. Table 2 also showsclearly that there is a higher rate of tooth decay(including root caries) in frail and dependentelderly people living in institutions than amongfree living people. Nearly a third of all naturalteeth are affected, compared with just over10% of all teeth in free living people aged 65and over. The number of free living very oldpeople (¢ 85) with some teeth is still low, hencethe final base number for this group is small,particularly after weighting. However, the datapresented indicate that there is also a higherlevel of decay in this group than in youngergroups, but less than that found for the samplefrom institutions.
Table 3 gives the data for root decay, andonce again indicates the considerable differ-ence between the institutional and the free liv-ing samples, with the institutional group havingmore than twice the number of decayed orunsound root surfaces than the free living,despite there being far fewer vulnerable teeth.
166
Oral health care forfrail and dependent older people
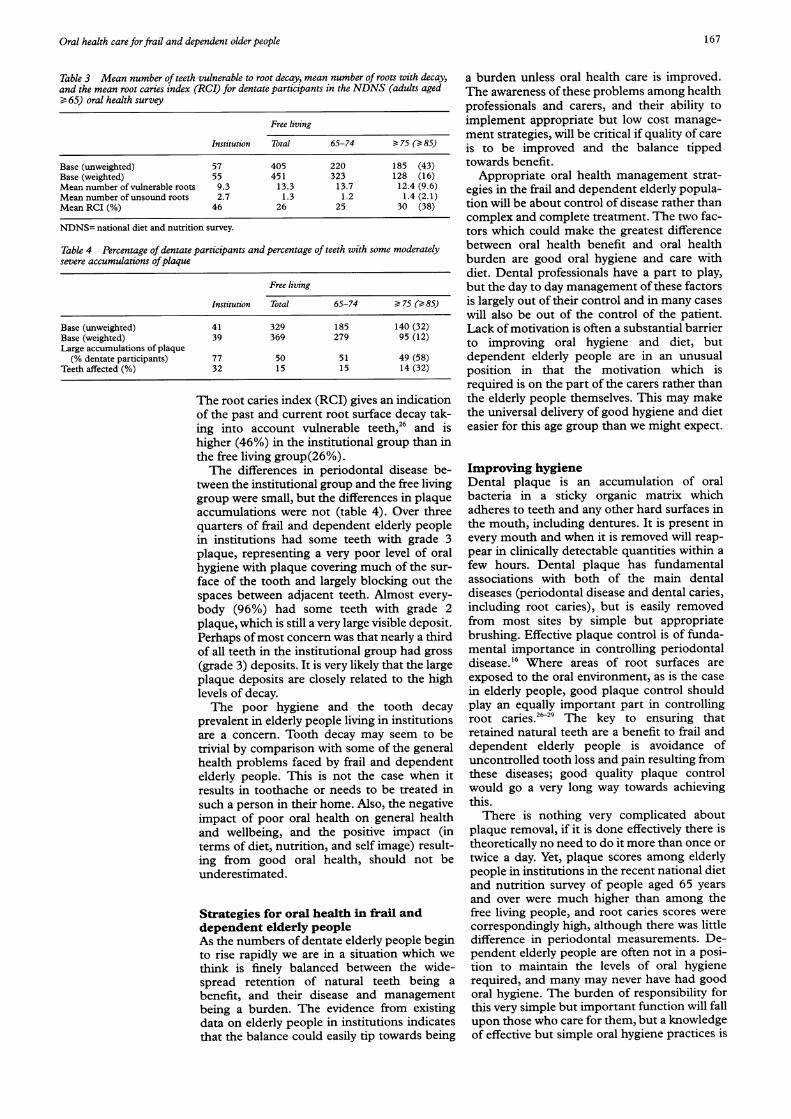
Table 3 Mean number of teeth vulnerable to root decay, mean number of roots with decay,and the mean root caries index (RCI) for dentate participants in the NDNS (adults aged¢ 65) oral health survey
Free living
Institution Total 65-74 > 75 (> 85)
Base (unweighted) 57 405 220 185 (43)Base (weighted) 55 451 323 128 (16)Mean number of vulnerable roots 9.3 13.3 13.7 12.4 (9.6)Mean number of unsound roots 2.7 1.3 1.2 1.4 (2.1)Mean RCI (%) 46 26 25 30 (38)
NDNS= national diet and nutrition survey.
Table 4 Percentage of dentate participants and percentage of teeth with some moderatelysevere accumulations ofplaque
Free living
Institution Total 65-74 75 (> 85)
Base (unweighted) 41 329 185 140 (32)Base (weighted) 39 369 279 95 (12)Large accumulations of plaque(% dentate participants) 77 50 51 49 (58)
Teeth affected (%) 32 15 15 14 (32)
The root caries index (RCI) gives an indicationof the past and current root surface decay tak-ing into account vulnerable teeth,26 and ishigher (46%) in the institutional group than inthe free living group(26%).The differences in periodontal disease be-
tween the institutional group and the free livinggroup were small, but the differences in plaqueaccumulations were not (table 4). Over threequarters of frail and dependent elderly peoplein institutions had some teeth with grade 3plaque, representing a very poor level of oralhygiene with plaque covering much of the sur-
face of the tooth and largely blocking out thespaces between adjacent teeth. Almost every-
body (96%) had some teeth with grade 2plaque, which is still a very large visible deposit.Perhaps ofmost concern was that nearly a thirdof all teeth in the institutional group had gross(grade 3) deposits. It is very likely that the largeplaque deposits are closely related to the highlevels of decay.The poor hygiene and the tooth decay
prevalent in elderly people living in institutionsare a concern. Tooth decay may seem to betrivial by comparison with some of the generalhealth problems faced by frail and dependentelderly people. This is not the case when itresults in toothache or needs to be treated insuch a person in their home. Also, the negativeimpact of poor oral health on general healthand wellbeing, and the positive impact (interms of diet, nutrition, and self image) result-ing from good oral health, should not beunderestimated.
Strategies for oral health in frail anddependent elderly peopleAs the numbers of dentate elderly people beginto rise rapidly we are in a situation which we
think is finely balanced between the wide-spread retention of natural teeth being a
benefit, and their disease and managementbeing a burden. The evidence from existingdata on elderly people in institutions indicatesthat the balance could easily tip towards being
a burden unless oral health care is improved.The awareness of these problems among healthprofessionals and carers, and their ability toimplement appropriate but low cost manage-ment strategies, will be critical if quality of careis to be improved and the balance tippedtowards benefit.
Appropriate oral health management strat-egies in the frail and dependent elderly popula-tion will be about control of disease rather thancomplex and complete treatment. The two fac-tors which could make the greatest differencebetween oral health benefit and oral healthburden are good oral hygiene and care withdiet. Dental professionals have a part to play,but the day to day management of these factorsis largely out of their control and in many caseswill also be out of the control of the patient.Lack of motivation is often a substantial barrierto improving oral hygiene and diet, butdependent elderly people are in an unusualposition in that the motivation which isrequired is on the part of the carers rather thanthe elderly people themselves. This may makethe universal delivery of good hygiene and dieteasier for this age group than we might expect.
Improving hygieneDental plaque is an accumulation of oralbacteria in a sticky organic matrix whichadheres to teeth and any other hard surfaces inthe mouth, including dentures. It is present inevery mouth and when it is removed will reap-pear in clinically detectable quantities within afew hours. Dental plaque has fundamentalassociations with both of the main dentaldiseases (periodontal disease and dental caries,including root caries), but is easily removedfrom most sites by simple but appropriatebrushing. Effective plaque control is of funda-mental importance in controlling periodontaldisease.'6 Where areas of root surfaces areexposed to the oral environment, as is the casein elderly people, good plaque control shouldplay an equally important part in controllingroot caries.""'9 The key to ensuring thatretained natural teeth are a benefit to frail anddependent elderly people is avoidance ofuncontrolled tooth loss and pain resulting fromthese diseases; good quality plaque controlwould go a very long way towards achievingthis.There is nothing very complicated about
plaque removal, if it is done effectively there istheoretically no need to do it more than once ortwice a day. Yet, plaque scores among elderlypeople in institutions in the recent national dietand nutrition survey of people aged 65 yearsand over were much higher than among thefree living people, and root caries scores werecorrespondingly high, although there was littledifference in periodontal measurements. De-pendent elderly people are often not in a posi-tion to maintain the levels of oral hygienerequired, and many may never have had goodoral hygiene. The burden of responsibility forthis very simple but important function will fallupon those who care for them, but a knowledgeof effective but simple oral hygiene practices is
167

Steele, Walls
not inherent, it needs to be delivered, andbrushing somebody else's teeth is a skill thathas to be learned.The first part of a strategy for improving the
oral health care of frail and dependent elderlypeople is to consider the issue of education ofcarers both in relation to the need for and theprovision of health care and monitoring. Suchtraining could be achieved at a relatively lowcost with use of dental hygienists and dentalhealth educators.
Dietary awarenessDental caries occurs when plaque bacteriametabolise dietary sugars to produce acids onthe surface of the tooth. The resultant low pHleads to demineralisation of the mineralcomponent and subsequent softening andcavitation of the tooth surface. The pH gradu-ally recovers after the sugar intake, but frequentsugar intakes maintain a constantly low pH andpersistent damaging caries activity. Whensaliva flow is reduced the recovery of pH aftera sugar intake is further delayed, allowing moretime for demineralisation to occur. When thepH recovers remineralisation and repair ofdamaged surfaces may occur when there is suf-ficient salivary flow.Anybody who has frequent intake of foods
containing sugar is at risk of ongoing cariesactivity."0 Dependent and frail elderly peopleare at additional risk because salivary flow isoften reduced substantially by use of medi-cation or other systemic factors, whereas thereare usually many exposed root surfaces whichare vulnerable sites for new caries.28 29 Plaquecontrol will provide some protection, but evenwhen this is good there are areas which cannotbe easily cleaned. A reduction in the intake ofnon-milk extrinsic sugars, particularly in thefrequency of intake is at the heart of cariescontrol. The worst imaginable dietary regime,from the point of view of dental decay, wouldbe frequent intake of sugar-for example, inthe form of sweetened tea or coffee or as snackssuch as biscuits and confectionery that containsugar. Regrettably this (empirically) seems tobe a perfect description of dietary practicewhich is common in many residential institu-tions. Ironically, many elderly people may beable to manage a more challenging (in terms ofchewing) and less cariogenic diet if naturalteeth are retained in good condition.The second part of our strategy for improv-
ing oral health in frail and dependent elderlypeople is to put into place advisory and moni-toring structures to ensure good dietarypractice in these groups. Once again the dentalprofessional can only provide an advisory role,the real difference could be made by those whoadminister the day to day care of these elderlysubjects.
Professional monitoring and treatmentEven where appropriate preventive strategiesare in place, disease will still occur and dentaldecay can often progress rapidly in elderly peo-ple. Early detection will often lead to simpletreatment which can be delivered quickly in thehome. Early detection means frequent checks
by trained professionals. Ideally this would be adentist, but need not necessarily be so.Auxiliary dental personnel could fulfill themonitoring role, and visiting medical profes-sionals may also be in a position to detectproblems early, although a dentist wouldnormally be required to provide any treatment.Once again, planning and awareness arerequired. By the time dental problems havebecome symptomatic, their management isusually complex, uncomfortable, and in thecase of frail and dependent elderly people,inconvenient and costly.Another strategy for effective and high qual-
ity oral health care for frail and dependent eld-erly people is frequent monitoring of their oralstate to ensure prompt detection and treatmentof dental disease.
Additional preventive measuresA range of additional agents are available whichmay make an important contribution topreventing dental disease in dependent elderlypeople. Fluorides, self administered in the formof mouthwashes, or professionally adminis-tered in the form of varnishes or other topicalapplications can make a substantial differenceto the control of caries, even in older adults.3'There is evidence to show that fluoridation ofthe water supply also results in a significantreduction in root surface caries in olderadults....'. Chlorhexidine mouthwashes arevery effective in plaque control and may provea useful adjunct to conventional oral hygienepractices.'6 Other promising topical chlorhexi-dine applications are also now available andmay provide considerable benefit in terms ofpreventing dental decay.'5 All of these will beuseful, but (with the exception of fluoridationof the water supply) should be used only on thebasis of professional dental advice.
ConclusionsWithin a few years there will be a rapid andprofound alteration in the oral health of theoldest members of society. The change will betowards the retention of natural teeth. Thiscould bring important benefits in terms ofnutrition and general wellbeing, but it couldalso bring with it a great deal of dental diseaseand the need for complex care. Managementstrategies based on prevention, frequent moni-toring, and early treatment ofdental disease areessential if the full benefit of improvements inoral health are to be forthcoming.
We thank the project board of the national diet and nutritionsurvey of people aged 65 years and over for their permission touse some of the data contained within this paper. The nationaldiet and nutrition survey of people aged 65 years and over wasfunded jointly by the Ministry of Agriculture, Fisheries, andFood and the Department of Health and conducted by Socialand Community Planning Research in conjunction with theDunn nutrition unit and the University ofNewcastle, UniversityCollege London, and the University ofBirmingham. Oral healthsurvey grant number MTN12.
1 Ettinger RL. Demography and dental needs, an inter-national perspective. Gerodontology 1993;10:3-9.
2 Gray PG, Todd JE, Slack GL, Bulman JS. Adult dental healthin England and Wales in 1968. London: HMSO, 1970.
3 Todd JE, Lader D. Adult dental health 1988& United Kingdom.London: HMSO, 1991.
168
9ral health care forfrail and dependent older people
4 Chauncey HH, Muench ME, Kapur KK, Wayler AH. Theeffect of the loss of teeth on diet and nutrition. Int Dent Jf1984;34:98-104.
5 Osterberg T, Steen B. Relationship between dental state anddietary intake in 70 year old males and females in Gothen-burg, Sweden: a population study. Jf Oral Rehabil 1982;9:509-21.
6 Osterberg T, Mellstrom D, Sundh V. Dental Health andfunctional ageing. Community Dentistry and Oral Epidemio-logy 1990;18:313-8.
7 Steele JG, Ayatollahi SMT, Walls AWG, Murray JJ. Clinicalfactors related to reported satisfaction with oral function indentate older adults in England. Community Dentistry andOral Epidemiology 1997;25:143-149.
8 DeStefano F, Anda RF, Kahn HS, Williamson DF, RussellCM. Dental disease and risk of coronary heart disease.BMJ 1993;306:688-91.
9 Beck K, Garcia J, Heiss G, Volionas P, Offenbacher S. Peri-odontal disease and cardiovascular disease. Jf Periodontol1996;67:1123-37.
10 Syrjanen J, Peltola J, Valtonen V. Dental Infections in associ-ation with cerebral infarction in young and middle-agedmen. J7 Intern Med. 1989;225:179-84.
11 Scannapieco FA, Mylotte JM. Relationship between peri-odontal disease and bacterial pneumonia. Jf Periodontol1996;13:118-29.
12 Galan D, Lynch E. Epidemiology of root caries. Gerodontol-ogy 1993;10:59-71
13 Vehkalati MM, Rajula M, Tuominen R, Puinio IK.Prevalence of root caries in the adult Finnish Population.Community Dentistry and Oral Epidemiology 1983;11:188-90.
14 Joshi A, Papas AS, Giunta root caries incidence and associ-ated risk factors in middle aged and older adults. Gerodon-tology 1993;10:83-9
15 Lynch E. Antimicrobial management of primary root carieslesions: a review. Gerodontology 1996;13:118-29.
16 Jenkins WMM. The prevention and control of chronic peri-odontal disease. In: Murray JJ, ed. Prevention of oral disease.3rd ed. Oxford: Oxford University Press, 1996:118-38.
17 Ekelund R. The dental and oral condition and the need fortreatment among the residents of municipal old peopleshomes in Finland. Proc Finn Dent Soc 1984;80:43-52.
18 Tobias B, Smith JM. Barriers to dental care and associatedoral status and treatment needs in an elderly populationliving in sheltered accommodation in West Essex. Br DentJ1987;163:293-5.
19 Stuck AE, Chapuis C, Fluiy H, Lang NP. Dental treatmentneeds in an elderly population referred to a geriatric hospi-tal in Switzerland. Community Dentistry and Oral Epidemio-logy 1989;17:267-272.
20 Jokstad A, Ambjornsen E, Eide KE. Oral health ininstitutionalized elderly people. Acta Odontol Scand 1996;54:303-308.
21 Vigild M. Denture status and the realistic need for prostho-dontic treatment among institutionalized elderly in Den-mark. Community Dentistry and Oral Epidemiology 1987;15:128 -133.
22 Vigild M. Dental caries and the need for treatment amonginstitutionalised elderly. Community Dentistry and Oral Epi-demiology 1989;17:102-5.
23 Vigild M. Oral hygiene and periodontal conditions among201 institutionalized elderly. Gerodontics 1988;4: 140-5.
24 Finch S, Doyle W, Lowe C, Bates CJ, Prentice A, SmithersG, Clarke PC. National diet and nutrition survey: people aged65 years or over. Vol 1: report of the diet and nutrition survey.London: Stationary Office, 1997 (in press).
25 Steele JG, Shieham A, Marcenes W, Walls AWG. Nationaldiet and nutrition survey: people aged 65-years or over. Vol 2:report of the oral health survey. London: Stationary Office,1997 (in press).
26 Katz RV. Assessing root caries in populations: the evolutionof the root caries index. _J Public Health Dent 1980;40:7-16.
27 Ravald N, Birkhead D, Hamp SE, Root caries susceptibilityin periodontally treated patients. Results after 12 years. 7Clin Periodontol 1993;13:758-67.
28 Budtz-Jorgensen E, Mojon P, Rentsch A, Roehrich N, vonder Muehll D, Baehni P. Caries prevalence and associatedpredisposing conditions in recently hospitalized elderlypersons. Acta Odontol Scand 1996;54:251-6.
29 Hix JO, O'Leary TJ. The relationship between cementalcaries, oral hygiene status and fermentable carbohydrateintake. J Periodontol 1976;47:394-404.
30 Rugg-Gunn AJ. Diet and dental caries. In: Murray JJ, ed.Prevention oforal disease, 3rd ed. Oxford: Oxford UniversityPress, 1996:3-31.
31 Jones JA. Root caries prevention and chemotherapy. Am JDent 1995;8:353-7.
32 Stamm JW, Banting DW. Comparison of root cariesprevalence in adults with life-long residence in fluoridatedand non-fluoridated communities. Jf Dent Res 1980;59(suppl) :405.
33 Brustman BA. Impact of exposure to fluoride adequatewater on root surface caries in the elderly. Gerodontics1986;2:203-7.
34 Hunt RJ, Eldredge JB, Beck JD. Effect of residence in afluoridated community on the incidence of coronal androot caries in an older population. J Public Health Dent1989;49:138-141
35 Whelton HP, Holland TJ, O'Mullane DM. The prevalenceof root surface caries amongst Irish adults Gerodontology1993;10:72-5.
36 Addy M, Moran J, Wade W. Chemical plaque control in theprevention of gingivitis and periodontitis. In: Lang NP,Karring T, eds. Proceedings of the 1st European workshop onperiodontology (Ittingen 1993). London: Quintessence,1994:244-57.
169





![Implementing Reading Tasks to Improve Students Oral Performance[1]](https://img.pdfslide.net/doc/110x75/577cd7571a28ab9e789eba10/implementing-reading-tasks-to-improve-students-oral-performance1.jpg)