Embed Size (px)
Citation preview

Study on Haptic Feedback Functions for an Interventional Surgical Robot System
Yuan Wang 1, 2 ,Shuxiang Guo1, 2, 3, Ping Guo 1, 2, Nan Xiao 1, 2
1 The Institute of Advanced Biomedical Engineering System, School of Life Science, Beijing Institute of Technology, No.5, Zhongguancun South Street, Haidian District, Beijing 100081, China
2 Key Laboratory of Convergence Medical Engineering System and Healthcare Technology, The Ministry of Industry and Information Technology, Beijing Institute of Technology,
No.5, Zhongguancun South Street, Haidian District, Beijing 100081, China 3 Faculty of Engineering, Kagawa University, 2217-20 Hayashi-cho, Takamatsu, Kagawa 760-8521, Japan
[email protected], [email protected], xiaonan@ bit.edu.cn
Abstract—In medical practice, endovascular treatment has
become increasingly popular. Compared to traditional interventional surgery, robotic surgical system has higher precision and ability to remotely control. However, the existing robotic surgical system dose not provide doctors with real-time effective haptic feelings. This paper presents a novel interventional surgical robot systems. In this design, the robot system will simulate the procedure of the doctor's hand to operate the guide wire, and providing haptic feedback to the doctor. In this paper, the Study of haptic feedback function in the developed interventional surgical robot system was introduced. The advantage of this interventional operation robot system was analyze. And performance improvement of the robot operation system which brought by the haptic feedback function was confirmed. The function of haptic feedback can provide effective support for the doctor in operation.
Index Terms —Interventional surgical robot system, Haptic
feedback, Remotely control
I. INTRODUCTION In medical practice, intravascular intervention has become
more popular, and was accepted by more and more patients and surgeon. Whether for diagnostic or surgical treatment it already is the current mainstream solution. As a branch of technology of minimally invasive surgery, endovascular surgery has a majority of the outstanding characteristics of minimally invasive surgery, such as a small wound, low postoperative pain and faster recovery time. However, it can't like minimally invasive surgery to reduce the risks of surgery. As an emerging technology, it requires a lot of operating skills. In addition, an object of diagnosis and treatment is vascular of patients which are fragility and narrow parts. And the operation is impossible to directly monitor, because tools are motion within the blood vessels. Thus during the catheter is inserted into a patient's blood vessel, any operational errors are likely to cause injury to the patient. Much more skills and experience are required for doctors to insert the catheter. Vascular interventional procedures are divided into cardiovascular interventional surgery and neuro intervention. Cardiovascular intervention includes cardiac ablation procedures, heart stents and valve repair surgery. Neuro intervention including cerebrovascular thrombus ablation, arterial dilation. In operation, the accuracy requirement of neuro intervention is higher than the requirement of interventional cardiovascular surgery. An experienced neurosurgery doctor can
achieve a precision about 1mm in the surgery. Collision parts between the vessel wall and catheter is the main source of danger, collision force will not damage blood vessels is the important condition of safe operation. However, the contact force between the vessels and catheter cannot be detected, it cannot be directly to the doctor for warning. Hence now doctors are combined with the resistance at operated catheter proximal tip, experience and all kinds of medical imaging, is mainly for X optical imaging, to guide their operation. Therefore during the operation process, the X-ray camera is used, long time of irradiation for doctors and patients can cause physical damage. Especially for doctors, after treatment for more patients, his exposure time in X-ray will be much higher than patients. Although the doctor be dressed in protective clothing, it is difficult to effectively protect the doctor’s face and hands which radiated in X-ray. Lead protective clothing has great weight, causing a great challenge of the doctor's stamina. When the fatigue state, the doctor will be very difficult to guarantee the quality of operation. The long-term weight-bearing caused great damage on doctor body especially the spine. To overcome these challenges, we need better technology and mechanism to help and training doctors. So interventional surgical robot system emerge as the times require. But the existing surgical robot system is not adequate to replace conventional surgery. Not only because the machine is not as flexible as hands of human being but also the robot system can not provide accurate haptic feedback to give the doctor operation guide.
The robot system have high accuracy and stability. It can provide the high precision operation for the surgery. And it can be remote control and realize patient isolation. Doctors will is liberated from X ray irradiation environment [1-3]. And the hidden danger of the body caused by long term irradiation with X rays will be solved. However, the current interventional surgical robot system is also not possible to meet all of the operational requirements of intravascular intervention.
When the surgery, the real-time haptic information is very important to guarantee the operation safety [4-10]. However, existing studies have not realize perfect haptic feedback function, which leads to the lack of important guidance information in the operation of the doctor [11-15]. It serious impact on the efficiency and safety of operation. Haptic feedback implementation consists of two key technologies, force
measurement and providing feedback force [16-20]. In order to solve these problems, this paper proposes a new robotic catheter navigation system. The slave side of the system, the catheter manipulator, will simulate the doctor's hand movements to the operation the catheter or guide wire [21-23]. And the use of mechanical sensor integrated in the catheter manipulator complete testing of resistance at catheter. A new type of doctor’s console is designed. The console can be skillful operation. And it can detection accurate operation commands of doctor, and use the reverse driving to generate resistance at the same time, providing haptic feedback effect for the operation of doctors [24-26].
In this article, a complete system was descripted, and using experimental to study the system to provide haptic feedback to enhance the performance of operative intervention. The rest of the paper is organized as follows. The development interventional surgical robot systems was proposed in the next section, method of force measurement and providing force feedback were introduced. Then, design experiments to evaluate the function of haptic feedback effect. Finally is the conclusion part.
II. THE FRAMEWORK OF SYSTEM The research adopts the design idea of the master-slave system, to allow remote operation, completed the doctor-patient separation of functions, will liberation the doctor from the exposure operation environment in X ray [27], operation diagram as Fig 1. The master side is surgeon’s console, the main function is to provide a simulation operation and haptic feedback for the doctor, and collecting control commands of the doctor from the guide wire in the operation. The slave side, catheter manipulator, will be responsible for the control of guide wire in the patient’s intravascular.
Fig. 1 Interventional surgical robot system
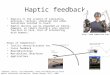
In the endovascular intervention operation, surgeon only need tow manipulation on catheter, rotation and insert. Therefore, there are two basic motions of the catheter, rotation, and go forward and backward. Fig. 2 shows the surgeon’s actions during inserting motion.
In a real operation procedure, surgeon inserts the catheter to the lesion based on the hand’s feeling. For example, the surgeon rotates the catheter when he/she feels more resistance from the catheter. Sometime the surgeon operates the catheter based on the DSA image but most of the time the surgery carries out the operation based on the hand feeling. Haptic is the essential element for surgeons to finish operations.
Fig. 2 Insertion process of the guide wire
A. The guide wire manipulator
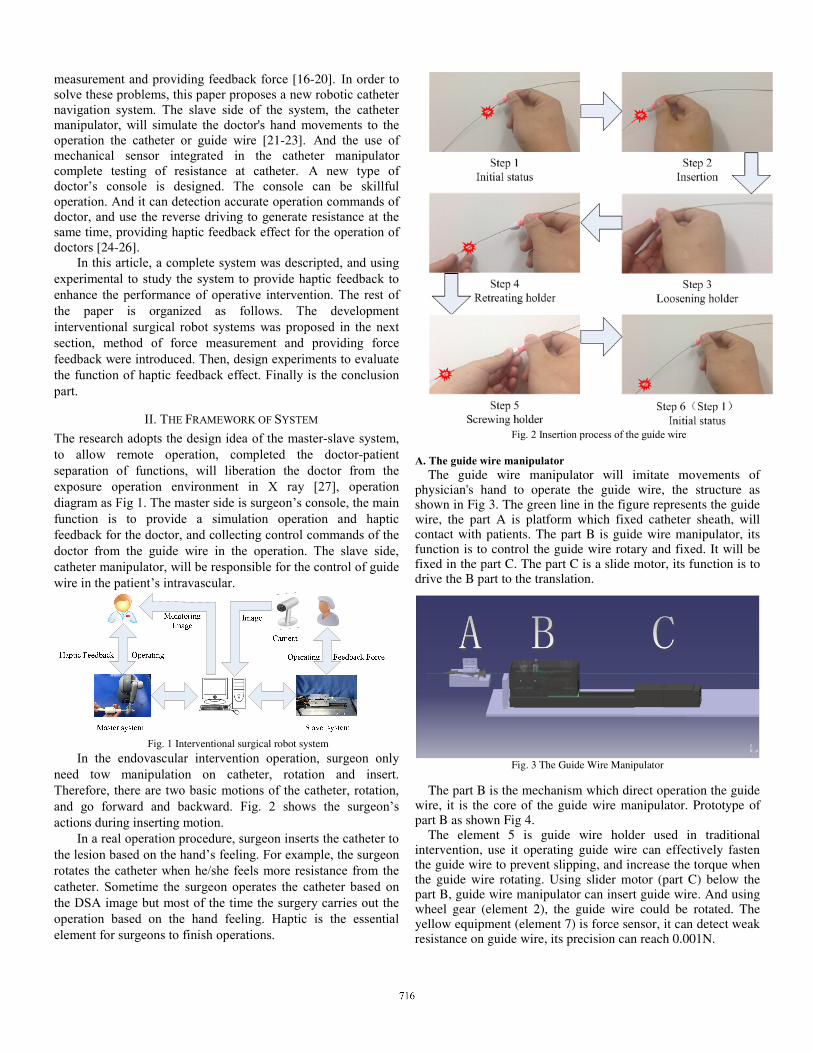
The guide wire manipulator will imitate movements of physician's hand to operate the guide wire, the structure as shown in Fig 3. The green line in the figure represents the guide wire, the part A is platform which fixed catheter sheath, will contact with patients. The part B is guide wire manipulator, its function is to control the guide wire rotary and fixed. It will be fixed in the part C. The part C is a slide motor, its function is to drive the B part to the translation.
Fig. 3 The Guide Wire Manipulator
The part B is the mechanism which direct operation the guide
wire, it is the core of the guide wire manipulator. Prototype of part B as shown Fig 4.
The element 5 is guide wire holder used in traditional intervention, use it operating guide wire can effectively fasten the guide wire to prevent slipping, and increase the torque when the guide wire rotating. Using slider motor (part C) below the part B, guide wire manipulator can insert guide wire. And using wheel gear (element 2), the guide wire could be rotated. The yellow equipment (element 7) is force sensor, it can detect weak resistance on guide wire, its precision can reach 0.001N.
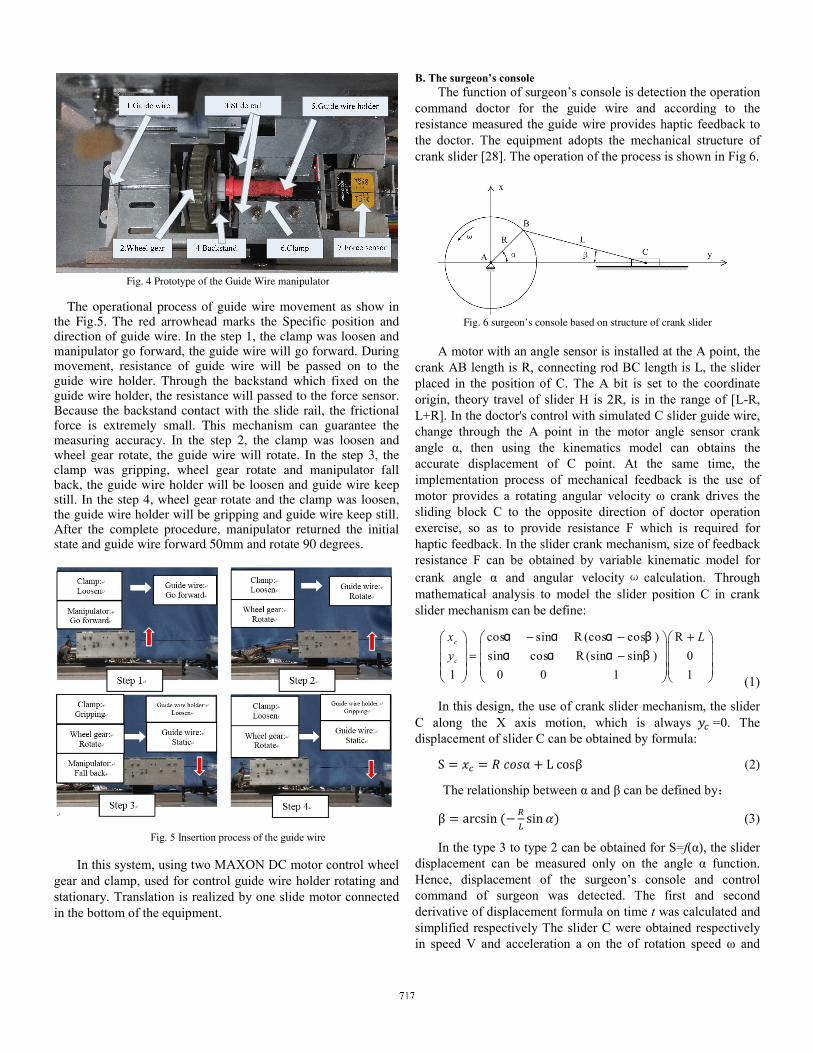
Fig. 4 Prototype of the Guide Wire manipulator
The operational process of guide wire movement as show in the Fig.5. The red arrowhead marks the Specific position and direction of guide wire. In the step 1, the clamp was loosen and manipulator go forward, the guide wire will go forward. During movement, resistance of guide wire will be passed on to the guide wire holder. Through the backstand which fixed on the guide wire holder, the resistance will passed to the force sensor. Because the backstand contact with the slide rail, the frictional force is extremely small. This mechanism can guarantee the measuring accuracy. In the step 2, the clamp was loosen and wheel gear rotate, the guide wire will rotate. In the step 3, the clamp was gripping, wheel gear rotate and manipulator fall back, the guide wire holder will be loosen and guide wire keep still. In the step 4, wheel gear rotate and the clamp was loosen, the guide wire holder will be gripping and guide wire keep still. After the complete procedure, manipulator returned the initial state and guide wire forward 50mm and rotate 90 degrees.
Fig. 5 Insertion process of the guide wire
In this system, using two MAXON DC motor control wheel
gear and clamp, used for control guide wire holder rotating and stationary. Translation is realized by one slide motor connected in the bottom of the equipment.
B. The surgeon’s console The function of surgeon’s console is detection the operation
command doctor for the guide wire and according to the resistance measured the guide wire provides haptic feedback to the doctor. The equipment adopts the mechanical structure of crank slider [28]. The operation of the process is shown in Fig 6.
Fig. 6 surgeon’s console based on structure of crank slider
A motor with an angle sensor is installed at the A point, the
crank AB length is R, connecting rod BC length is L, the slider placed in the position of C. The A bit is set to the coordinate origin, theory travel of slider H is 2R, is in the range of [L-R, L+R]. In the doctor's control with simulated C slider guide wire, change through the A point in the motor angle sensor crank angle α, then using the kinematics model can obtains the accurate displacement of C point. At the same time, the implementation process of mechanical feedback is the use of motor provides a rotating angular velocity ω crank drives the sliding block C to the opposite direction of doctor operation exercise, so as to provide resistance F which is required for haptic feedback. In the slider crank mechanism, size of feedback resistance F can be obtained by variable kinematic model for crank angle α and angular velocity ω calculation. Through mathematical analysis to model the slider position C in crank slider mechanism can be define:
cos sin R (cos cos ) Rsin cos R (sin sin ) 0
1 0 0 1 1
c
c
x Ly
− − +⎛ ⎞ ⎛ ⎞ ⎛ ⎞⎜ ⎟ ⎜ ⎟ ⎜ ⎟= −⎜ ⎟ ⎜ ⎟ ⎜ ⎟⎜ ⎟ ⎜ ⎟ ⎜ ⎟⎝ ⎠ ⎝ ⎠ ⎝ ⎠
α α α βα α α β
(1)
In this design, the use of crank slider mechanism, the slider C along the X axis motion, which is always =0. The displacement of slider C can be obtained by formula: S α L cosβ (2)
The relationship between α and β can be defined by: β arcsin sin (3)
In the type 3 to type 2 can be obtained for S=f(α), the slider displacement can be measured only on the angle α function. Hence, displacement of the surgeon’s console and control command of surgeon was detected. The first and second derivative of displacement formula on time t was calculated and simplified respectively The slider C were obtained respectively in speed V and acceleration a on the of rotation speed ω and

crank angle α formula: v R (4) a Rω (5)
When the sliding block and the guide wire quality simulation is m, can get the reverse driving force feedback mechanism provides F formula: F ma mRω , β arcsin sin (6)
Type 6 to the feedback force F=f (α, ω) to a function capable of measuring angle α with velocity ω.
In the prototype, Phantom omni, a commercial products, was used as the master side. In order to measure the real force of haptic feedback, a novel handle which equipped sensor was design and Instead of the original handle. The prototype of master side is shown in Fig.7.
Fig. 7 surgeon’s console and novel handle
Using the force measured by the sensor, closed-loop control of haptic function can be achieve. The haptic feedback function will be optimized.
III. THE EXPERIMENTAL OF HAPTIC FEEDBACK EFFECT
An insertion experiment was carried out to evaluate the effect of the haptic feedback function. In the experiment, invited 10 volunteers without operation experience. The operation was carried out in simulation environment with and without haptic feedback respectively. Medical training vessel model as treatment object, show in Fig 8, was used to detect operation process of the volunteers.
Each volunteer achieved simulant treatment for 5 different lesions, 10 times operations was carried out at each lesion with and without haptic feedback respectively. Resistance and completion time of each volunteer’s operation was recorded.
Fig. 8 Medical training vessel model
Completion time of operation are show in the Fig 9. The three
sets of data representing average operation time of each volunteers at three different conditions of operation. As can be seen from the graph, completion time of manual operation consumed the least time, completion time of robotic operation without haptic feedback consumed the most time. Hence, compared to the condition of operation without haptic feedback, the condition of operation with force feedback makes the completion of operation are more efficient.
Fig. 9 completion time of operation
The resistance are show in the Fig 10. The resistance was
measured by sensor of slave side and approximate the collision force between guide wire and blood vessel. Smaller resistance means safer operation. Fig 10(a) express the resistance of situation without haptic feedback, the average is 0.0126N and the maximum is 0.0412N. Fig 10(b) express the resistance of situation with haptic feedback, the average is 0.0072N and the maximum is 0.0233N. Two resistance was measured when the guide wire was inserting same lesions. As can be seen from the graph, haptic feedback function improved the safety of operation.
0
50
100
150
200
250
300
350
volunteer 1 volunteer 2 volunteer 3 volunteer 4 volunteer 5
Ave
rage
com
plet
ion
time/
(s)
Completion time of operation
manual operation
Robtic operation with haptic feedback
Robtic operation without haptic feedback
Fig. 10 The resistance of operation
IV. CONCLUSION
This paper introduces a new type of intervention operation robot system simulation hand motion of doctors to operate on the guide wire, the doctor can cast the clinical operation skill fine. The system includes a novel guide wire resistance measurement structure and haptic feedback function. And design experiments to verify the function of haptic feedback has a significant promotion to effect of interventional surgery robot system, and effectively improve the security of the system. In the future, the research group will maintain the same action principle, the structure is improved into a more compact, precise and closed design, to meet the needs of the clinical operation is required for stable, health requirements.
ACKNOWLEDGMENT
T This research is partly supported by the National Natural Science Foundation of China (61375094), National High Tech. Research and Development Program of China (No.2015AA043202).
REFERENCES
[1] P. Kanagaratnam, M. Koa-Wing, D. T. Wallace, A. S. Goldenberg, N. S. Peters, D. W. Davies, “Experience of robotic catheter ablation in humans using a novel remotely steerable catheter sheath,” Journal of Interventional Cardiac Electrophysiology, Vol.21, pp. 19-26, 2008.
[2] J. K. Chun, S. Ernst, S. Matthews, B. Schmidt, D. Bansch, S. Boczor, et al, “Remote-controlled catheter ablation of accessory pathways: results from the magnetic laboratory,” European Heart Journal, Vol. 28, No. 2, pp.190-195, 2007.
[3] C. Pappone, G. Vicedomini, F. Manguso, F. Gugliotta, P. Mazzone, S. Gulletta, N. Sora, S. Sala, A. Marzi, G. Augello, L. Livolsi, A. Santagostino, V. Santinelli, “Robotic Magnetic Navigation for Atrial Fibrillation Ablation,” Journal of the American College of Cardiology, Vol. 47, pp. 1390-1400, 2006.
[4] J. Guo, S. Guo, T. Tamiya, H. Hirata, H. Ishihara, “ A Virtual Reality-based Method of Decreasing Transmission Time of Visual Feedback for a Tele-operative Robotic Catheter Operating System ”, The International Journal of Medical Robotics and Computer Assisted Surgery, DOI: 10.1002/rcs.1642, 2014.
[5] X. Yin, S. Guo, H. Hirata, H. Ishihara, “Design and experimental evaluation of a Teleoperated haptic robot–assisted catheter operating system”, Journal of Intelligent Material Systems and Structures, pp.1-14, DOI:10.1177/1045389X14556167, 2014.
[6] N. Xiao, L. Shi, B. Gao, S. Guo and T. Tamiya, “Clamping Force Evaluation For A Robotic Catheter Navigation System”, Neuroscience and Biomedical Engineering, Vol. 1, No. 2, pp.141-145, 2013.
[7] N. Xiao, J. Guo, S. Guo and T. Tamiya, “A Robotic Catheter System with Real-time Force Feedback and Monitor”, Journal of Australasian Physical and Engineering Sciences in Medicine, Vol.35, No.3, pp. 283-289, 2012.
[8] J. Guo, S. Guo, N. Xiao, B. Gao, “Virtual Reality Simulators based on a Novel Robotic Catheter Operating system for Training in Minimally Invasive Surgery”, Journal of Robotics and Mechatronics, Vol. 24, No. 4, pp. 649-655, 2012.
[9] X. Ma, S. Guo, N. Xiao, J. Guo, S. Yoshida, T. Tamiya and M. Kawanishi, “Development of a Novel Robotic Catheter Manipulating System with Fuzzy PID Control”, International Journal of Intelligent Mechatronics and Robotics (IJIMR) , Vol. 2, No. 2, pp. 58-77, 2012.
[10] J. Guo, S. Guo, N. Xiao, X. Ma, S. Yoshida, T. Tamiya and M. Kawanishi, “A Novel Robotic Catheter System with Force and Visual Feedback for Vascular Interventional Surgery”, International Journal of Mechatronics and Automation, Vol.2, No.1, pp.15-24, 2012.
[11] S. Willems, D. Steven, H. Servatius, B. A. Hoffmann, I. Drewitz, K. Mullerleile, M. A. Aydin, K. W. heider, T. V. Salukhe, T. Meinertz, T. Rostock,“ Persistence of Pulmonary Vein Isolation After Robotic Remote-Navigated Ablation for Atrial Fibrillation and its Relation to Clinical Outcome,” Journal of Interventional Cardiac Electrophysiology,Vol. 21, pp. 1079-1084, 2010.
[12] W. Saliba, V. Y. Reddy, O. Wazni, J. E. Cummings, et.al, “Atrial Fibrillation Ablation Using a Robotic Catheter Remote Control System: Initial Human Experience and Long-Term Follow-Up Results,” Journal of the American College of Cardiology, Vol. 51, pp. 2407-2411, 2008.
[13] M. Tanimoto, F. Arai, T. Fukuda, and M. Negoro, “Augmentation of Safety in Tele-operation System for Intravascular Neurosurgery,” Proceedings of 1998 IEEE International Conference on Robotics and Automation, pp. 2890-2895, 1998.
[14] C. Preusche, T. Ortmaier, G. Hirzinger,“ Tele-operation concepts in minimal invasive surgery,” Control Engineering Practice, Vol. 10, pp. 1245-1250, 2002.
[15] S. Ikeda, F. Arai, T. Fukuda, M. Negoro, K. Irie, and I. Takahashi, et. al, “In Vitro Patient-Tailored Anatomical Model of Cerebral Artery for Evaluating Medical Robots and Systems for Intravascular Neurosurgery,” Proceedings of 2015 IEEE International Conference on Intelligent Robots and Systems, pp. 1558-1563, 2005.
[16] Y. Wang, K. Hu, N. Xiao, S. Guo, “A Force Acquisition Method in A Catheter Navigation System,” Proceedings of IEEE International Conference on Complex Medical Engineering, pp. 633-637, 2013.
[17] Y. Wang, N. Xiao, S. Guo, “Design of a Surgeon's Controller for Catheter Navigation,” Proceedings of IEEE International Conference on Mechatronics and Automation, pp. 974-978, 2013.
[18] F. Arai, R. Fujimura, T. Fukuda, and M. Negoro, “New Catheter Driving Method Using Linear Stepping Mechanism for Intravascular Neurosurgery,” Proceedings of the 2002 IEEE International Conference on Robotics and Automation, pp. 2944-2949,2002.
[19] J. Peirs, J. Clijnen, D. Reynaerts, H. V. Brussel, P. Herijgers, B. Corteville, et. al, “ Amicro optical force sensor for force feedback during minimally invasive robotic surgery”, Sensors and Actuators A: Physical, Vol.115, pp. 447-455, 2004.
[20] N. Xiao, S. Guo, J. Guo, X. Xiao, T. Tamiya, “Development of a Kind of Robotic Catheter Manipulation System,” Proceedings of IEEE International Conference on Robotics and Biomimetics, pp. 32-37, 2011.
[21] Y. Wang, S. Guo, B. Gao, ”Vascular Elastcity Determined Mass-spring Model for Virtual Reality Simulators” International Journal of Mechatronics and Automation, Vol.5, No.1, pp1-10, 2015
[22] N. Xiao, S. Guo, J. Guo, X. Xiao,T. Tamiya, “Development of a Kind of Robotic Catheter Manipulation System,” Proceedings of 2011 IEEE International Conference on Robotics and Biomimetics, pp. 32-37, 2011.
[23] X. Wang, M. Meng, “Perspective of Active Capsule Endoscope: Actuation and Localization,” International Journal of Mechatronics and Automation, Vol.1, No.1, pp. 38-45, 2011.
[24] S. Abdulla, P. Wen, “Robust Internal Model Control for Depth of Anaesthesia,” International Journal of Mechatronics and Automation, Vol.1, No.1, pp. 1-8, 2011.
[25] H. Rafii-Tsri, C. J. Payne, G.Z. Yang,” Current and Emerging Robot-Assisted Endovascular Catheterization Technologies: A Review,” Annals of Biomedical Engineering, Vol. 42, No. 4, pp. 697–715 ,April 2014

[26] Y. Thakui, J. S. Bax, W. David, “Holds worth and Maria Drangova, Design and Performance Evaluation of a Remote Catheter Navigation System,” IEEE Transactions on biomedical engineering, Vol.56, No. 7,pp. 1901-1908, 2009.
[27] W. Saliba, V. Y. Reddy, O. Wazni, J. E. Cummings, et.al, “Atrial Fibrillation Ablation Using a Robotic Catheter Remote Control System: Initial Human Experience and Long-Term Follow-Up Results,” Journal of the American College of Cardiology, Vol. 51, pp. 2407-2411, 2008.
[28] S. J. Chen, J. Hang, “Probability Analysis and Calculation of Kinematic Accuracy for Slider-Crank Mechanism,” Machinery Design and Manufacture, Vol. 7, pp. 203-206, 2013.


![Aalborg Universitet Haptic Feedback for Enhancing Realism ... · E-mail: pabu@itu.dk the haptic feedback in video games was raised by Chang [7] who suggested that haptic technologies](https://img.pdfslide.net/doc/110x75/5e684b66369aa742a847f13b/aalborg-universitet-haptic-feedback-for-enhancing-realism-e-mail-pabuitudk.jpg)