Embed Size (px)
Citation preview

This article was downloaded by: [Florida State University]On: 21 October 2014, At: 18:07Publisher: Taylor & FrancisInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Health Communication:International PerspectivesPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/uhcm20
Studying the Process of ClinicalCommunication: Issues of Context,Concepts, and Research DirectionsTerrance L. Albrecht a , Louis A. Penner a , Rebecca J. W. Cline a ,Susan S. Eggly b & John C. Ruckdeschel ba Karmanos Cancer Institute and Department of Family Medicine andPublic Health Sciences , Wayne State University School of Medicine ,Detroit, Michigan, USAb Karmanos Cancer Institute and Department of Internal Medicine ,Wayne State University School of Medicine , Detroit, Michigan, USAPublished online: 15 May 2009.
To cite this article: Terrance L. Albrecht , Louis A. Penner , Rebecca J. W. Cline , Susan S. Eggly& John C. Ruckdeschel (2009) Studying the Process of Clinical Communication: Issues of Context,Concepts, and Research Directions, Journal of Health Communication: International Perspectives,14:S1, 47-56, DOI: 10.1080/10810730902806794
To link to this article: http://dx.doi.org/10.1080/10810730902806794
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &
Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Flor
ida
Stat
e U
nive
rsity
] at
18:
07 2
1 O
ctob
er 2
014

Studying the Process of Clinical Communication:Issues of Context, Concepts, and
Research Directions
TERRANCE L. ALBRECHT, LOUIS A. PENNER, ANDREBECCA J. W. CLINE
Karmanos Cancer Institute and Department of Family Medicine and PublicHealth Sciences, Wayne State University School of Medicine, Detroit,Michigan, USA
SUSAN S. EGGLY AND JOHN C. RUCKDESCHEL
Karmanos Cancer Institute and Department of Internal Medicine,Wayne State University School of Medicine, Detroit, Michigan, USA
Much cancer-related health communication research has involved studies of theeffects of media campaigns and strategies on secondary prevention. Cancer diagno-sis rates, however, continue to affect millions of people. The need exists for commu-nication studies to address the quality of the clinical interaction, the point of actualcare delivery in addressing diagnosis, treatment, and survivorship. Using examplesfrom a 6-year communication and behavioral oncology research program establishedat the Karmanos Cancer Institute (KCI) in Detroit, Michigan, we describe selectedempirical issues; models, particularly the ‘‘convergence model’’ (adapted fromRogers & Kincaid, 1981); and associated constructs that are relevant and promisingfoundations for building future research in cancer clinical settings. Two examplesfrom our empirical research program are described.
Much of the extant cancer-related health communication research (particularly thatwhich has been federally funded) has involved studies of the effects of mediacampaigns and strategies for increasing health promotion and secondary behavioralprevention for screening and early detection. Despite this important work, however,cancer diagnosis rates continue to severely threaten public health in the UnitedStates (Centers for Disease Control and Prevention [CDC], 2006=2007) and Europe(Ferlay et al., 2007) and are disproportionately higher in underserved minoritygroups (Byers et al., 2008). Thus, it is imperative that communication researchefforts expand to more fully address patient, provider and family=companioninteractions in the cancer clinical context. It is in these interactions that oncologistscare for patients and that, in turn, patients and families=companions experienceimportant aspects of the diagnosis and treatment process.
Address correspondence to Terrance L. Albrecht, Ph.D., Professor and Interim AssociateCenter Director—Population Sciences, Karmanos Cancer Institute, 4100 John R. Street –GE00CB, Detroit, MI 48201, USA. E-mail: [email protected]
Journal of Health Communication, 14:47–56, 2009Copyright # Taylor & Francis Group, LLCISSN: 1081-0730 print=1087-0415 onlineDOI: 10.1080/10810730902806794
47
Dow
nloa
ded
by [
Flor
ida
Stat
e U
nive
rsity
] at
18:
07 2
1 O
ctob
er 2
014

Toward that end, this article is a case for clinical communication research as asignificant focus for behavioral medicine. Using examples from a 6-year communica-tion and behavioral oncology research program established at the KCI in Detroit,Michigan, we describe selected empirical issues, models, and constructs that arerelevant and promising foundations for building future research in cancer clinicalsettings. We conclude with two examples from our own on-going research program.
Empirical Issues: Context and Data Capture Methodology
Context
Clinical interactions occur within larger systems that include institutions andcommunities. Oncologists, patients, and family members=companions (Albrecht,Eggly, & Ruckdeschel, in press) do not interact in a vacuum when they meet inthe outpatient and inpatient setting of a cancer center. Studies of clinical interactionsinvolve understanding the influence of multiple encompassing system levels. Forexample, Detroit’s socially and economically challenged urban community-levelcontext affects many of the medical, social psychological and resource aspects ofthe patient–provider–family interaction. Detroit has among the highest unemploy-ment, poverty, obesity, and murder rates nationally; these have potentially strongimpacts on the clinical interaction because of the patient’s stage of diagnosis, pre-senting comorbidity status, and compliance with medical regimens. Blacks in Detroitalso have generally higher cancer mortality and morbidity rates than Whites; cancerrates for Blacks are also higher than for Blacks nationally (Schwartz, 2003). The highschool graduation rate has been reported as less than 25% (Swanson, 2008); the adultilliteracy rate is 47% (Taylor, 2005), with major implications for low health literacy,patients’ and family members’=companions’ understanding of diagnostic and treat-ment information and adherence. As an urban cancer center, the KCI serves thegreatest volume of under-and uninsured cancer patients in its geographical region.This too, has implications for the level of resources available (level of services, space,personnel) to care for patients and address their needs in the clinical encounter.
Data-Capture Methodology
A second important issue relates to the fundamental theoretical premise thatcommunication transactions between and among patients, their family=companions,and physicians are mutual influence processes based on verbal and nonverbal beha-viors (these conceptual issues are described below). Hence, the ability to systemati-cally observe and analyze these transactions necessitates a type of data collectionmethodology that aims to directly capture real time interaction data. The methodol-ogy involves a carefully designed, tested, and assembled strategy for audio and videorecording of medical encounters in the outpatient oncology clinic (for a relatedjustification, see the entire special issue of the Journal of Communication, ‘‘Researchon the Relationship Between Verbal and Nonverbal Communication: EmergingIntegration,’’ 2002; also, Riddle et al., 2002).
The preponderance of physician–patient communication data reported in theliterature, however, involves only audio recording. Thus, in undertaking our researchprogram, we first designed, tested, and established a fully functional and operationalvideo and audio recording system in the outpatient exam rooms throughout our
48 T. L. Albrecht et al.
Dow
nloa
ded
by [
Flor
ida
Stat
e U
nive
rsity
] at
18:
07 2
1 O
ctob
er 2
014

adult and pediatric cancer clinical areas (Albrecht et al., 2005). These include, forexample, 40 multidisciplinary outpatient exam and consult rooms (plus remote,secured monitoring room) in the KCI Wertz Multidisciplinary Cancer Clinic, theeight exam rooms and two procedure rooms in the Pediatric Hematology=Oncology Clinic of Children’s Hospital of Michigan (plus remote, secured mon-itoring room), and in the 12 exam rooms (plus remote secured monitoring room) atthe University Family Physicians Primary Care Clinic (located in northwest Detroit).
Video recording is increasingly viewed as more reliable and valid than audiorecording, because it captures the full range of complex and interdependent verbaland nonverbal behaviors that occur in an interaction. We developed a systemdesigned to video record clinical interactions using mobile cameras that can bequickly and easily moved in and out of different clinical rooms to preserve flexibilityin their use (Albrecht et al., 2005). We have reported data to demonstrate that thesystem is unobtrusive during the interaction and does not produce participant reac-tance (Penner et al., 2007), yet it is fully compatible with institutional review boardguidelines that protect human participants’ privacy and to give them control over therecording process. Human subjects’ protection safeguards have been reviewed andapproved at two NCI-designated comprehensive cancer centers and the universityInstitutional Review Boards associated with both centers.
Importantly, we have empirically demonstrated that coder judgments ofinteractions significantly differed based on whether they were coding video- andaudio-recorded oncologist–patient communication data versus coding audio-onlycommunication data (Riddle et al., 2002). (This investigation was undertaken todemonstrate the added scientific value of capturing video data despite the increasedtime and expense of this complex data collection strategy.) We showed that nonver-bal behavior encompasses critical communication variables that signal meaning (e.g.,parents engaging in supportive touch during distressing pediatric cancer treatmentprocedures; eye contact between physician and patient) and are most often thesource of implicit messages about how to interpret verbal messages and conveyrelational messages, particularly important in interracial interactions (Dovidio,et al., 2008). Without video-recorded data, researchers and coders are forced to relyon verbal content alone, losing critical cues for content and relational information.In short, directly observing clinical interactions as they unfold in the clinical setting isincreasing the validity and reliability of our methods, data, findings, and conclusionsabout physician-patient communication.
Selected Models and Constructs
Definitions
We define cancer clinical communication as a multilevel dynamic process in whichparticipants exchange information that mutually influences their attitudes, behaviors,and relationships regarding cancer prevention, control, diagnosis=treatment, survivor-ship, and related medical and psychosocial health outcomes. Clinical communicationoccurs when physicians, patients, and family=companions attend to one anotherand begin interpreting one another’s verbal and nonverbal, explicit and implicit,obvious and subtle interactional behavior. In the outpatient setting of theexam room, communication consists of messages (verbal and nonverbal communica-tion behavior) and meanings (the attributions made about verbal and nonverbal
Clinical Communication 49
Dow
nloa
ded
by [
Flor
ida
Stat
e U
nive
rsity
] at
18:
07 2
1 O
ctob
er 2
014
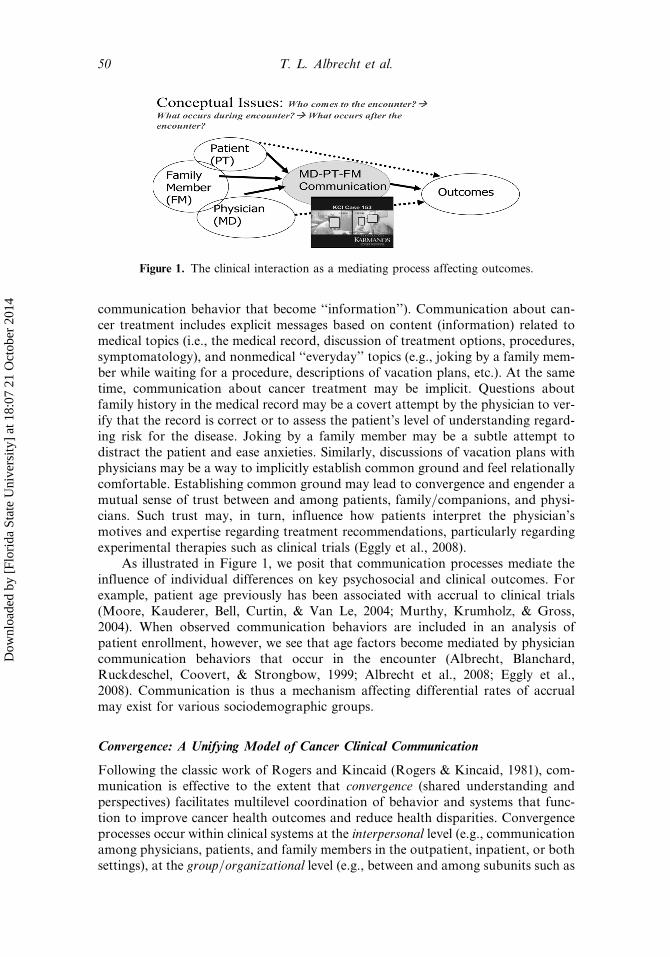
communication behavior that become ‘‘information’’). Communication about can-cer treatment includes explicit messages based on content (information) related tomedical topics (i.e., the medical record, discussion of treatment options, procedures,symptomatology), and nonmedical ‘‘everyday’’ topics (e.g., joking by a family mem-ber while waiting for a procedure, descriptions of vacation plans, etc.). At the sametime, communication about cancer treatment may be implicit. Questions aboutfamily history in the medical record may be a covert attempt by the physician to ver-ify that the record is correct or to assess the patient’s level of understanding regard-ing risk for the disease. Joking by a family member may be a subtle attempt todistract the patient and ease anxieties. Similarly, discussions of vacation plans withphysicians may be a way to implicitly establish common ground and feel relationallycomfortable. Establishing common ground may lead to convergence and engender amutual sense of trust between and among patients, family=companions, and physi-cians. Such trust may, in turn, influence how patients interpret the physician’smotives and expertise regarding treatment recommendations, particularly regardingexperimental therapies such as clinical trials (Eggly et al., 2008).
As illustrated in Figure 1, we posit that communication processes mediate theinfluence of individual differences on key psychosocial and clinical outcomes. Forexample, patient age previously has been associated with accrual to clinical trials(Moore, Kauderer, Bell, Curtin, & Van Le, 2004; Murthy, Krumholz, & Gross,2004). When observed communication behaviors are included in an analysis ofpatient enrollment, however, we see that age factors become mediated by physiciancommunication behaviors that occur in the encounter (Albrecht, Blanchard,Ruckdeschel, Coovert, & Strongbow, 1999; Albrecht et al., 2008; Eggly et al.,2008). Communication is thus a mechanism affecting differential rates of accrualmay exist for various sociodemographic groups.
Convergence: A Unifying Model of Cancer Clinical Communication
Following the classic work of Rogers and Kincaid (Rogers & Kincaid, 1981), com-munication is effective to the extent that convergence (shared understanding andperspectives) facilitates multilevel coordination of behavior and systems that func-tion to improve cancer health outcomes and reduce health disparities. Convergenceprocesses occur within clinical systems at the interpersonal level (e.g., communicationamong physicians, patients, and family members in the outpatient, inpatient, or bothsettings), at the group=organizational level (e.g., between and among subunits such as
Figure 1. The clinical interaction as a mediating process affecting outcomes.
50 T. L. Albrecht et al.
Dow
nloa
ded
by [
Flor
ida
Stat
e U
nive
rsity
] at
18:
07 2
1 O
ctob
er 2
014

groups of physician specialists and auxiliary support services such as the clinicaltrials office) and at the community level (e.g., the extent of engagement betweenthe cancer center and grassroots community groups). Convergence at these levelsis important because shared understanding can increase behavioral coordinationand enable greater patient-centered care We argue that communication processesthat lead to convergence are central to quality cancer care and play an important rolein improving patient outcomes, both large and small, such as affecting adherence toand compliance with medical regimens ( Epstein & Street, 2007; Stewart, 2000), clin-ical trial accrual (Albrecht et al., 2008), adjustment and functioning following a diag-nosis (Gabrijel et al., 2008), reactions to treatment (Cline et al., 2006), racialdisparities in patterns of care (Dovidio et al., 2008), stress (Arora et al., 2003),and the quality of survivorship (Clough-Gorr, 2007).
The Convergence/Nonconvergence Continuum in a Clinical Setting
As physicians, patients, and family=companions simultaneously transact and inter-pret messages during medical encounters, they may converge (share varyingdegrees of meaning regarding the content of information such as the ‘‘diagnosis,’’‘‘medication,’’ ‘‘treatment procedures,’’ ‘‘prognosis’’) or not converge, resulting inmutual misunderstanding and=or disagreement concerning key aspects of apatient’s disease and care. Whether physicians, patients, and family=companionsanions communicate in ways that produce convergent or nonconvergent meaningslikely has consequences for the quality of cancer care provided. The process ofnegotiating convergence is one of assessing and reassessing one’s own and others’views. In Figure 2, convergence (mutual understanding) between and among thepatient, physician, and family member=companion (if present) is depicted byoverlapping portions of circles (Albrecht & Bach, 1997; Laing, Phillipsen, &Lee, 1966; Rogers & Kincaid, 1981; Simmel, 1964). In our view of convergencein the clinical context, the overlapping (converging) segments may expand andcontract throughout the discussion and even afterward depending on the shiftinglevels of mutual understanding and shared perspective that exists at any point intime between and among the parties.
Physicians, patients, and family=companions may agree or disagree aboutmatters discussed, and they may understand or misunderstand (accurately or inaccu-rately perceive) one an others’ views. If they understand that they disagree
Figure 2. Convergence=nonconvergence model of physician–patient–family=companioncommunication (adapted from Rogers & Kincaid, 1981).
Clinical Communication 51
Dow
nloa
ded
by [
Flor
ida
Stat
e U
nive
rsity
] at
18:
07 2
1 O
ctob
er 2
014

(understand that they have different views), they can address and attempt to resolvethat disagreement. If they fail to recognize that they disagree, however, they will pro-ceed as if in agreement, likely resulting in subsequent misunderstandings (and, forexample, errors in administering medication, recognizing symptoms, understandingwhether or not they are enrolled in a clinical trial).
Convergence in clinical communication applies at the level of the physician–patient–family=companion interaction and, as suggested above, to transactionsamong health care providers across departments or subunits in the hospital or clin-ical setting that serves cancer patients and their families, such as between oncologistsand a clinical trials office. Convergence in communication between and among indi-viduals within the same medical institution or even within the same unit most likelyhas the same general characteristics as communication between physicians andpatients (and families=companions if present). The desired outcomes from interper-sonal and organizational communication are degrees of shared understanding lead-ing to coordinated action that benefits the patient and institution. Convergenceduring interactions in face-to-face meetings (e.g., multidisciplinary team meetings)or electronic exchanges (e-mail; videoconferencing) may be influenced by the quality,clarity, usefulness, relevance, and reliability of the new media adopted to facilitatesuch interactions. The desired outcomes of these exchanges, however, are essentiallythe same as the face-to-face exchanges discussed above. That is, members represent-ing differing organizational units need to understand one another’s perspective onthe issue at hand and acknowledge the points about which they have disagreements.The desired outcome is for units to have similar understanding and acceptance fortheir resulting actions to provide high-quality patient care consistent with each unit’sgoals and the goals of the institution (Albrecht & Bach, 1997).
Research Exemplars
The convergence model of clinical communication has guided several of our currentand planned studies. Two examples are briefly described below.
Physician Communication and Clinical Trial Accrual
We have investigated how communication among physicians, patients, and famil-y=companions influences patients’ decision making about participation in clinicaltrials. Using our custom-designed system for capturing video data, we then appliedthe Karmanos Accrual Analysis System (KAAS) to code the interactions (seeAlbrecht et al., 2008).
The KAAS is an observational coding system developed by the authors to assessthe multiparticipant interaction in which a clinical trial is offered. Independent,trained coders judged the interactions using each section of the KAAS. We used agroup consensus process in which three coders independently review and rate eachinteraction. If disagreements occurred, they were resolve during a group discussion.The KAAS was used to assess relational communication (the items are formatted asglobal judgments) rated on 7-point scales with descriptors for the endpoints of eachitem. Separate ratings were applied to judge oncologist–patient and oncologist–family=companion pairs. Principal components exploratory factor analyses withvarimax (orthogonal) rotations showed the items clustered into factors related toalliance behaviors and conversation control behaviors. The KAAS also assesses
52 T. L. Albrecht et al.
Dow
nloa
ded
by [
Flor
ida
Stat
e U
nive
rsity
] at
18:
07 2
1 O
ctob
er 2
014

content messages, and coders used the five comprehensive checklists to measure thetypes of information communicated by the physician to the patient and family=companions. These included legal–informational messages, side effects messages,support messages about the patient’s trial enrollment status, support messagesregarding side effects, and messages about benefits regarding trial participation.
By combining observational analysis of real-time video-recorded observations of235 outpatient interactions (collected at Time 1) with patient self-reports (collectedat Time 2), we showed how direct observations of measurable communication beha-viors during discussions of clinical trial offers influence patients’ accrual decisions(Albrecht et al., 1999; Albrecht et al., 2008). We also found that clinical trials wereexplicitly offered in only 20% of the interactions. When offers were made and patientsperceived they were offered a trial, 77% of patients assented. Thus, contrary to pre-vailing assumptions, patient refusal rates may be less of a problem than low ratesof trial offers. The reasons for these low rates likely include too few trials available,overly stringent eligibility criteria, physicians’ decisions about patient eligibility orappropriateness for open trials, or ineffective physician communication about trialoptions for patients to consider.
Physician–patient–family=companion communication convergence has effectson the patient’s decision-making process. Observed messages (at Time 1) directlyrelated to patients’ self-reports regarding their decisions (2 weeks later) and how theyfelt about their decisions and their physicians. Messages that help build a sense of analliance (among all parties, including the family=companions) provide support (tan-gible assistance and reassurance about managing side effects) and provide medicalcontent in language that patients and family=companions understand are associatedwith the patient’s decision and decision-making process. In addition, we found thatphysician–patient–family=companion convergence moderates the relationshipbetween cancer patients’ initial expectations prior to the visit with the oncologistand their decision to follow their oncologists’ treatment recommendations (Gleasonet al., manuscript). These findings can help increase physician awareness of the waysthat messages and communication behaviors can be observed and evaluated toimprove clinical practice and research.
Pediatric Cancer, Parent–Child Communication, and Treatment Reactions
Many pediatric cancer patients and their parents experience serious psychosocial andbehavioral stressors and problems during and after completion of the course of treat-ment (Patenaude & Kupst, 2005; Schultz et al., 2007). Understanding the origins ofthese stressors and problems (i.e., risk factors) is a prerequisite for designing inter-ventions to improve the pediatric cancer treatment experience and quality of survi-vorship. Convergence appears relatively high between physicians and children andbetween physicians and parents. The greatest problem regarding convergenceappears to occur in a percentage of parents interacting with their children. Thatis, our data (Cline et al., 2006; Peterson et al., 2007) suggest that children’s mostnegative outcomes in response to the treatment situations occur when parent andchild fail to converge around a shared definition of the treatment situation(i.e., complementary roles and rules for how to respond). For example, convergenceoccurs when a child accepts the parents’ proposed definition (acts in character with itby playing at the parents’ encouragement), or when the parents adjust commu-nication to match the child’s situational definition (e.g., by using a supportive
Clinical Communication 53
Dow
nloa
ded
by [
Flor
ida
Stat
e U
nive
rsity
] at
18:
07 2
1 O
ctob
er 2
014

communication pattern when the child is distressed). In contrast, a lack of conver-gence occurs when parents challenge or even ridicule the child’s definition of thesituation, as they do with invalidating communication. Our work has found thatwhen undergoing stressful cancer treatment, children of invalidating parents experi-enced more pain=distress than children whose parents used other communicationpatterns (Penner et al., 2008; Penner & Orom, In press). Thus, the outcomes of par-ent–child treatment-related episodes can be understood in terms of whether parentand child establish patterns of communication exhibiting convergence.
Our present goal is to more precisely identify the variables that affect parent–child interaction in stressful episodes and the processes and mechanisms by whichthese interactions affect subsequent child and parent psychosocial adjustment(Schultz et al., 2007). These findings of convergence=nonconvergence are importantbecause parent and child psychosocial functioning during the course of treatmentpredicts long-term psychosocial outcomes (Kazak & Barakat, 1997; Kusch,Labouvie, Ladisch, Fleischhack, & Bode, 2000), which, in turn, shape the qualityof survivorship.
References
Albrecht, T. L., & Bach, B. W. (1997). Communication in complex organizations: A relationalperspective. Orlando, FL: Harcourt Brace.
Albrecht, T. L., Blanchard, C., Ruckdeschel, J. C., Coovert, M., & Strongbow, R. (1999).Strategic physician communication and oncology clinical trials. Journal of ClinicalOncology, 17(10), 3324–3332.
Albrecht, T. L., Eggly, S., Gleason, M., Harper, F., Foster, T., Peterson, A., et al. (2008).Influence of clinical communication on patients’ decision making on participation inclinical trials. Journal of Clinical Oncology, 26(16), 2666–2673.
Albrecht, T. L., Eggly, S., & Ruckdeschel, J. (In press). Communicating withfamily=companions about cancer care. In D. Kissane, B. Bultz, P. Butow, & L. Finlay(Eds.), Handbook of communication in cancer and palliative care. New York: OxfordUniversity Press.
Albrecht, T. L., Ruckdeschel, J. C., Ray III, F. L., Pethe, B. J., Riddle, D. L., Strohm, J., et al.(2005). A portable, unobtrusive device for videorecording clinical interactions. BehaviorResearch Methods, 37(1), 165–169.
Arora, N. K. (2003). Interacting with cancer patients: The significance of physicians’ commu-nication behavior. Social Science and Medicine, 57(5), 791–806.
Byers, T. E., Wolf, H. J., Bauer, K. R., Bolick-Aldrich, S., Chen, V. W., Finch, J. L., et al.(2008). The impact of socioeconomic status on survival after cancer in the United States:findings from the National Program of Cancer Registries Patterns of Care Study. Cancer,113(3), 582–591.
Centers for Disease Control and Prevention (CDC), Division of Cancer Control and Preven-tion. (2006=2007). Fact sheet: The burden of cancer (pp. 1–4). Atlanta: Author.
Cline, R. J., Harper, F. W., Penner, L. A., Peterson, A. M., Taub, J. W., & Albrecht, T. L.(2006). Parent communication and child pain and distress during painful pediatric cancertreatments. Social Science and Medicine, 63(4), 883–898.
Clough-Gorr, K. M., Ganz, P. A., & Silliman, R. A. (2007). Older breast cancer survivors:Factors associated with change in emotional well-being. Journal of Clinical Oncology,25(11), 1334–1340.
Dovidio, J. F., Penner, L. A., Albrecht, T. L., Norton, W. E., Gaertner, S. L., & Shelton, J.N. (2008). Disparities and distrust: The implications of psychological processes forunderstanding racial disparities in health and health care. Social Science and Medicine,67(3), 478–486.
54 T. L. Albrecht et al.
Dow
nloa
ded
by [
Flor
ida
Stat
e U
nive
rsity
] at
18:
07 2
1 O
ctob
er 2
014

Eggly, S., Albrecht, T. L., Harper, F. W., Foster, T., Franks, M. M., & Ruckdeschel, J. C.(2008). Oncologists’ recommendations of clinical trial participation to patients. PatientEducation and Counseling, 70(1), 143–148.
Ferlay, J., Autier, P., Boniol, M., Heanue, M., Colombet, M., & Boyle, P. (2007). Estimates ofthe cancer incidence and mortality in Europe in 2006. Annals of Oncology, 18(3), 581–592.
Gabrijel, S., Grize, L., Helfenstein, E., Brutsche, M., Grossman, P., Tamm, M., & Kiss, A.(2008). Receiving the diagnosis of lung cancer: Patient recall of information and satisfac-tion with physician communication. Journal of Clinical Oncology, 26(2), 297–302.
Gleason, M. E., Harper, F. W., Eggly, S., Ruckdeschel, J. C., & Albrecht, T. L. (2009). Theinfluence of patient expectations regarding cure on treatment decisions. Patient Educationand Counseling, 75(2), 263–269.
Kazak, A. E., & Barakat, L. P. (1997). Brief report: Parenting stress and quality of life duringtreatment for childhood leukemia predicts child and parent adjustment after treatmentends. Journal Pediatric Psychology, 22(5), 749–758.
Kusch, M., Labouvie, H., Ladisch, V., Fleischhack, G., & Bode, U. (2000). Structuringpsychosocial care in pediatric oncology. Patient Education and Counseling, 40(3),231–245.
Laing, R. D., Phillipsen, H., & Lee, A. R. (1966). Interpersonal perception: A theory andmethod of research. New York: Harper & Row.
Moore, D. H., Kauderer, J. T., Bell, J., Curtin, J. P., & Van Le, L. (2004). An assessment ofage and other factors influencing protocol versus alternative treatments for patients withepithelial ovarian cancer referred to member institutions: A Gynecologic OncologyGroup study. Gynecological Oncology, 94(2), 368–374.
Murthy, V. H., Krumholz, H. M., & Gross, C. P. (2004). Participation in cancer clinical trials:Race-, sex-, and age-based disparities. Journal of the American Medical Association,291(22), 2720–2726.
Patenaude, A. F., & Kupst, M. J. (2005). Psychosocial functioning in pediatric cancer. JournalPediatric Psychology, 30(1), 9–27.
Penner, L. A., Cline, R. J., Albrecht, T. L., Harper, F. W. K., Peterson, A. M., Taub, J. W.,et al. (2008). Parents’ empathic responses and pain and distress in pediatric patients. Basicand Applied Social Psychology, 30, 102–113.
Penner, L. A., & Orom, H. (In press). Enduring goodness: A person by situation perspective onprosocial behaviour. Washington, DC: APA Books.
Penner, L. A., Orom, H., Albrecht, T. L., Franks, M. M., Foster, T. S., & Ruckdeschel, J. C.(2007). Camera-related behaviors during video recorded medical interactions. Journal ofNonverbal Behavior, 31(2), 99–117.
Peterson, A. M., Cline, R. J. W., Foster, T. S., Penner, L. A., Parrott, R. L., Keller, C. M.,et al. (2007). Parents’ interpersonal distance and touch behavior and child pain anddistress during painful pediatric oncology procedures. Journal of Nonverbal Behavior,31(2), 79–97.
Riddle, D. L., Albrecht, T. L., Coovert, M., Penner, L. A., Quinn, G., Ruckdeschel, J. C., et al.(2002). Differences in audiotaped versus videotaped physician-patient interactions.Journal of Nonverbal Behavior, 26, 219–240.
Rogers, E., & Kincaid, D. L. (1981). Communication networks: A paradigm for new research.New York: Free Press.
Schultz, K. A., Ness, K. K., Whitton, J., Recklitis, C., Zebrack, B., Robison, L. L., et al.(2007). Behavioral and social outcomes in adolescent survivors of childhood cancer: Areport from the childhood cancer survivor study. Journal of Clinical Oncology, 25(24),3649–3656.
Schwartz, A. G. (2003). Cancer Statistics in Metropolitan Detroit 2003. Detroit: MetropolitanDetroit Cancer Surveillance System, Surveillance, Epidemiology and End ResultsProgram, Epidemiology Section, Detroit, MI.
Simmel, G. (1964). The sociology of Georg Simmel (K. H. Wolf, trans.). New York: Free Press.
Clinical Communication 55
Dow
nloa
ded
by [
Flor
ida
Stat
e U
nive
rsity
] at
18:
07 2
1 O
ctob
er 2
014

Stewart, M., Brown, J. B., Donner, A., McWhinney, I. R., Oates, J., Weston, W. W., &Jordan, J. (2000). The impact of patient-centered care on outcomes. Journal of FamilyPractice, 49(9), 796–804.
Swanson, C. B. (2008). Cities in crisis. Bethesda, MD: Editorial Projects in Education.Taylor, K. H. (2005). When an idol can’t read. Detroit News. Retrived July 12, 2008 from
http://www.detnews.com/2005/events/0510/12/E01–325560.htm.
56 T. L. Albrecht et al.
Dow
nloa
ded
by [
Flor
ida
Stat
e U
nive
rsity
] at
18:
07 2
1 O
ctob
er 2
014