Embed Size (px)
Citation preview

Postgraduate Medical Journal (November 1982) 58, 716-719
Subcutaneous nodular synovitis following medial arthrotomy in a case of myxoidliposarcoma of the thigh
J. MCCLUREB.Sc., M.D., D.M.J.Path., M.R.C.Path.
PREMA IYERM.B., B.S., F.R.C.P.A.
R. J. BAUZEM.B., B.S., F.R.A.C.S.
T. MUKHERJEEM.B., B.S., D.G.O., M.D.
The Adelaide Bone and Joint Research Unit and the Division of Tissue Pathology IMVS, Frome Road, Adelaide,South Australia
SummaryA lesion of pigmented synovitis appeared as a nodulein the scar one year after arthrotomy and wasremoved one year later. It was clearly distinguishedfrom a concurrent myxoid liposarcoma on clinical andmorphological grounds (light and electron micros-copy).
Introduction
Pigmented synovitis is a well defined disorderaffecting joints, tendons and bursae in a diffuse ornodular form. A variety of names reflect site andmorbid anatomy: giant cell tumour of tendon sheath,localized nodular synovitis (Granowitz and Mankin,1967; Fraire and Fechner, 1972) and pigmentedvillonodular synovitis (Jaffe, Lichtenstein and Sutro,1941). Aetiology and pathogenesis are unknown, butall recognize the lesions to be similar, to be reactive,and very probably to result from repeated haemor-rhage. The changes in the synovium of haemo-philiacs are most often adduced in support of thisargument. We record this very unusual case of asubcutaneous pigmented lesion, arising one year afterarthrotomy, examined by light and electron micros-copy, to add to experience and knowledge of thisuncommon condition. We believe the lesion to havedeveloped in displaced synovium. Difficulty andinterest was added by a concurrent liposarcoma.
Case reportA 28-year-old man injured his left knee. After
several months of persistent pain and swelling, withepisodic collapsing and clicking, a torn left lateralmeniscus was removed. Recovery was uneventful.
Requests for reprints to: Dr J. McClure, C/- IMVS, Box 14,Rundle Street Post Office, Adelaide, South Australia 5001.
One year later he twisted his right knee. Hepresented himself after 14 months because of persist-ing symptoms. During the last 2 months he had alsonoticed a lump on the inner side of his right lowerthigh, which was confirmed by clinical examination.Plain X-rays of the knee were normal. A medialarthrotomy was performed; there was no abnormalityof the meniscus or synovium. The arthrotomy woundwas closed using 3 figure-of-eight vicryl suturesclosing the synovium and capsule in one layer. Acontinuous vicryl suture was placed in the subcutane-ous tissue and the skin was closed by a sub-cuticularprolene suture. The back of the knee was thenexplored: there was a multilobulated, well-encapsu-lated tumour 100x40 mm beneath the adductormagnus muscle belly.
Recovery was uneventful, but he continued to havepain in his knee. Three months after the lastoperation a torn lateral meniscus was removed. Thesynovium was normal.One year later a 3 mm, mobile, painless lump was
noted in the lower end of the medial arthrotomywound of the right knee, attached to the capsule butnot to the skin. A suture granuloma was diagnosed.One year later it was slightly painful, 10 mm indiameter and fairly mobile. The lump plus an ellipseof subcutaneous tissue and skin were excised. Therewas a smaller (3 mm diameter) nodule just beneaththe capsule in the line of the wound. This was alsoexcised together with a segment of capsule. Thewound healed well and recovery has been unevent-ful.
PathologicalfindingsThe tumour from the back of the right knee
exhibited the features of a myxoid variant of liposar-coma (Fig. 1). Lobulated and yellow-pink in colour,
0032-5473/82/1100-0716 $02.00 © 1982 The Fellowship of Postgraduate Medicine
by copyright. on 13 S
eptember 2018 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.58.685.716 on 1 Novem
ber 1982. Dow
nloaded from
Clinical reports 717
::I..~ ~ ~ ~ ~ ~ ~~~iir!~Ikt· ··
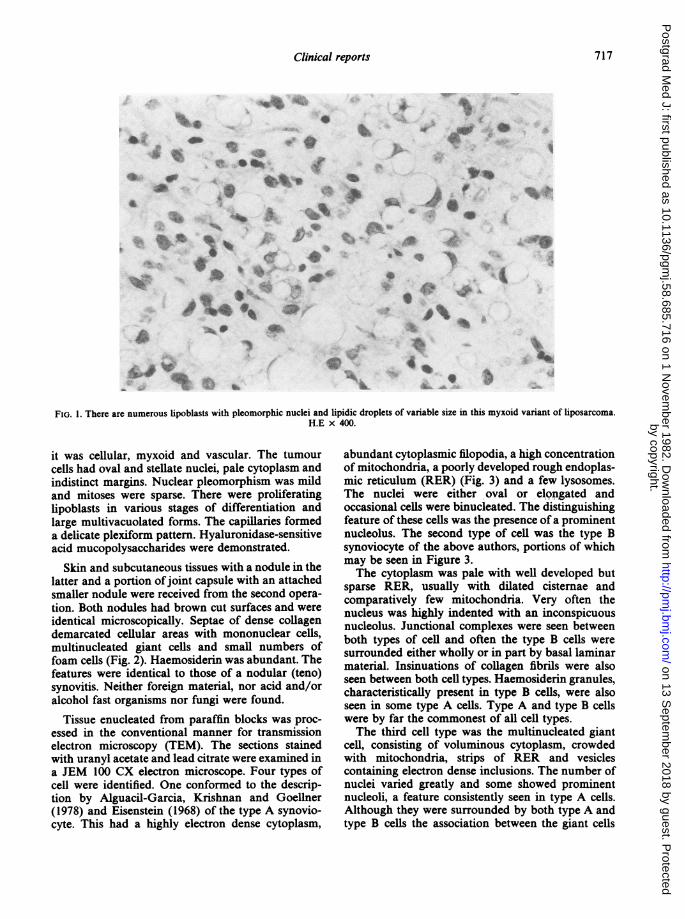
FIG. 1. There are numerous lipoblasts with pleomorphic nuclei and lipidic droplets of variable size in this myxoid variant of liposarcoma.H.E x 400.
it was cellular, myxoid and vascular. The tumourcells had oval and stellate nuclei, pale cytoplasm andindistinct margins. Nuclear pleomorphism was mildand mitoses were sparse. There were proliferatinglipoblasts in various stages of differentiation andlarge multivacuolated forms. The capillaries formeda delicate plexiform pattern. Hyaluronidase-sensitiveacid mucopolysaccharides were demonstrated.
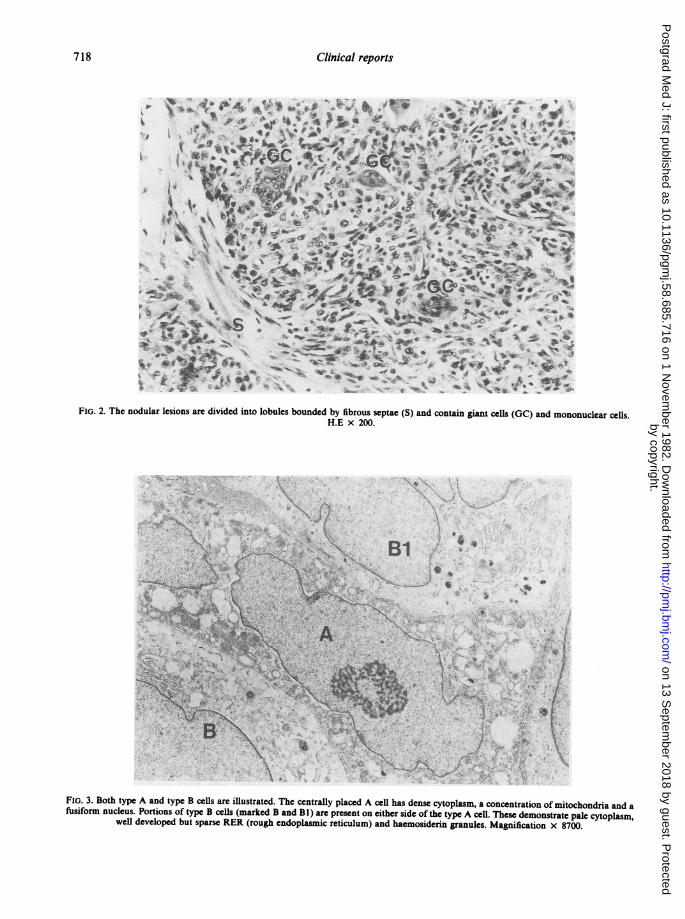
Skin and subcutaneous tissues with a nodule in thelatter and a portion ofjoint capsule with an attachedsmaller nodule were received from the second opera-tion. Both nodules had brown cut surfaces and wereidentical microscopically. Septae of dense collagendemarcated cellular areas with mononuclear cells,multinucleated giant cells and small numbers offoam cells (Fig. 2). Haemosiderin was abundant. Thefeatures were identical to those of a nodular (teno)synovitis. Neither foreign material, nor acid and/oralcohol fast organisms nor fungi were found.
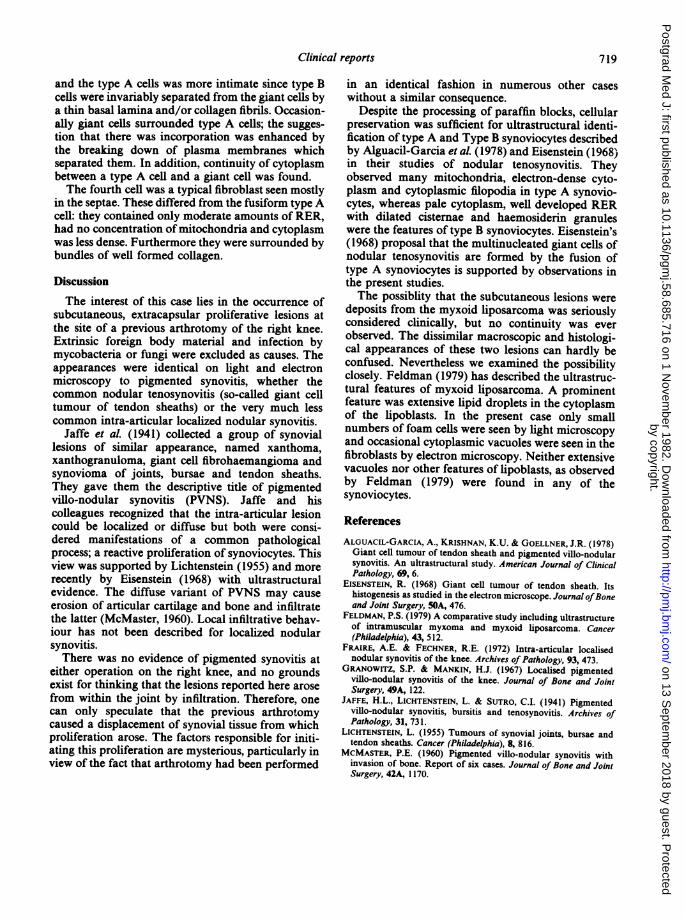
Tissue enucleated from paraffin blocks was proc-essed in the conventional manner for transmissionelectron microscopy (TEM). The sections stainedwith uranyl acetate and lead citrate were examined ina JEM 100 CX electron microscope. Four types ofcell were identified. One conformed to the descrip-tion by Alguacil-Garcia, Krishnan and Goellner(1978) and Eisenstein (1968) of the type A synovio-cyte. This had a highly electron dense cytoplasm,
abundant cytoplasmic filopodia, a high concentrationof mitochondria, a poorly developed rough endoplas-mic reticulum (RER) (Fig. 3) and a few lysosomes.The nuclei were either oval or elongated andoccasional cells were binucleated. The distinguishingfeature of these cells was the presence of a prominentnucleolus. The second type of cell was the type Bsynoviocyte of the above authors, portions of whichmay be seen in Figure 3.The cytoplasm was pale with well developed but
sparse RER, usually with dilated cisternae andcomparatively few mitochondria. Very often thenucleus was highly indented with an inconspicuousnucleolus. Junctional complexes were seen betweenboth types of cell and often the type B cells weresurrounded either wholly or in part by basal laminarmaterial. Insinuations of collagen fibrils were alsoseen between both cell types. Haemosiderin granules,characteristically present in type B cells, were alsoseen in some type A cells. Type A and type B cellswere by far the commonest of all cell types.The third cell type was the multinucleated giant
cell, consisting of voluminous cytoplasm, crowdedwith mitochondria, strips of RER and vesiclescontaining electron dense inclusions. The number ofnuclei varied greatly and some showed prominentnucleoli, a feature consistently seen in type A cells.Although they were surrounded by both type A andtype B cells the association between the giant cells
by copyright. on 13 S
eptember 2018 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.58.685.716 on 1 Novem
ber 1982. Dow
nloaded from
718 Clinical reports
"~f'lfIt'I~B.1
.-mlC·. t~r 1'~~~~~~~~~~~4~~~~~L!~r'..rSp'r x~4~Vq~ *t~~~0i .06#-S.
l'?'.'.-.'I~ ~ 12~~ .· *:~b. 44f1~~I;~~rrF1ci~~~~~~~~~w up~~~~~~~~~~~~~~v1
0~~~~~~~~~~~~~~~~~*~~~~1
!. .b ·..
~~zlC-'4vyt4k.
r3F~~~~~ ,,, ~b/,'~' ~"~~:_~~.~,~ '~'~ '""-""'rF, ~lr,b t~iT ~ ~ 6ja~"_~,:..''St._..., c.. ".-I."..,'- ,,,,~ , -'~ : .~-~f~ -, . ','~ ~~"
iiti~~~~~~~~~~1~~~it~C·~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ . r -.~,. .
FIG. 2. The nodular lesions are divided into lobules bounded by fibrous septae (S) and contain giant cells (GC) and mononuclear cells.H.E x 200.
.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~·':~::·...'" : ~, ·. y.I.. . ',!
'.i?--'(·,~...*'."~:'iC~. , ".'.' ,·~.,I· (,, : .'..-:·:d'<,.. .~·~:' . . ~ . ~~ *~. J·~.,
·~ ~~~·, , , 
Clinical reports 719
and the type A cells was more intimate since type Bcells were invariably separated from the giant cells bya thin basal lamina and/or collagen fibrils. Occasion-ally giant cells surrounded type A cells; the sugges-tion that there was incorporation was enhanced bythe breaking down of plasma membranes whichseparated them. In addition, continuity of cytoplasmbetween a type A cell and a giant cell was found.The fourth cell was a typical fibroblast seen mostly
in the septae. These differed from the fusiform type Acell: they contained only moderate amounts of RER,had no concentration of mitochondria and cytoplasmwas less dense. Furthermore they were surrounded bybundles of well formed collagen.
Discussion
The interest of this case lies in the occurrence ofsubcutaneous, extracapsular proliferative lesions atthe site of a previous arthrotomy of the right knee.Extrinsic foreign body material and infection bymycobacteria or fungi were excluded as causes. Theappearances were identical on light and electronmicroscopy to pigmented synovitis, whether thecommon nodular tenosynovitis (so-called giant celltumour of tendon sheaths) or the very much lesscommon intra-articular localized nodular synovitis.
Jaffe et al. (1941) collected a group of synoviallesions of similar appearance, named xanthoma,xanthogranuloma, giant cell fibrohaemangioma andsynovioma of joints, bursae and tendon sheaths.They gave them the descriptive title of pigmentedvillo-nodular synovitis (PVNS). Jaffe and hiscolleagues recognized that the intra-articular lesioncould be localized or diffuse but both were consi-dered manifestations of a common pathologicalprocess; a reactive proliferation of synoviocytes. Thisview was supported by Lichtenstein (1955) and morerecently by Eisenstein (1968) with ultrastructuralevidence. The diffuse variant of PVNS may causeerosion of articular cartilage and bone and infiltratethe latter (McMaster, 1960). Local infiltrative behav-iour has not been described for localized nodularsynovitis.There was no evidence of pigmented synovitis at
either operation on the right knee, and no groundsexist for thinking that the lesions reported here arosefrom within the joint by infiltration. Therefore, onecan only speculate that the previous arthrotomycaused a displacement of synovial tissue from whichproliferation arose. The factors responsible for initi-ating this proliferation are mysterious, particularly inview of the fact that arthrotomy had been performed
in an identical fashion in numerous other caseswithout a similar consequence.
Despite the processing of paraffin blocks, cellularpreservation was sufficient for ultrastructural identi-fication of type A and Type B synoviocytes describedby Alguacil-Garcia et al. (1978) and Eisenstein (1968)in their studies of nodular tenosynovitis. Theyobserved many mitochondria, electron-dense cyto-plasm and cytoplasmic filopodia in type A synovio-cytes, whereas pale cytoplasm, well developed RERwith dilated cisternae and haemosiderin granuleswere the features of type B synoviocytes. Eisenstein's(1968) proposal that the multinucleated giant cells ofnodular tenosynovitis are formed by the fusion oftype A synoviocytes is supported by observations inthe present studies.The possiblity that the subcutaneous lesions were
deposits from the myxoid liposarcoma was seriouslyconsidered clinically, but no continuity was everobserved. The dissimilar macroscopic and histologi-cal appearances of these two lesions can hardly beconfused. Nevertheless we examined the possibilityclosely. Feldman (1979) has described the ultrastruc-tural features of myxoid liposarcoma. A prominentfeature was extensive lipid droplets in the cytoplasmof the lipoblasts. In the present case only smallnumbers of foam cells were seen by light microscopyand occasional cytoplasmic vacuoles were seen in thefibroblasts by electron microscopy. Neither extensivevacuoles nor other features of lipoblasts, as observedby Feldman (1979) were found in any of thesynoviocytes.
References
ALGUACIL-GARCIA, A., KRISHNAN, K.U. & GOELLNER, J.R. (1978)Giant cell tumour of tendon sheath and pigmented villo-nodularsynovitis. An ultrastructural study. American Journal of ClinicalPathology, 69, 6.
EISENSTEIN, R. (1968) Giant cell tumour of tendon sheath. Itshistogenesis as studied in the electron microscope. Journal ofBoneand Joint Surgery, 50A, 476.
FELDMAN, P.S. (1979) A comparative study including ultrastructureof intramuscular myxoma and myxoid liposarcoma. Cancer(Philadelphia), 43, 512.
FRAIRE, A.E. & FECHNER, R.E. (1972) Intra-articular localisednodular synovitis of the knee. Archives of Pathology, 93, 473.
GRANOWITZ, S.P. & MANKIN, H.J. (1967) Localised pigmentedvillo-nodular synovitis of the knee. Journal of Bone and JointSurgery, 49A, 122.
JAFFE, H.L., LICHTENSTEIN, L. & SUTRO, C.I. (1941) Pigmentedvillo-nodular synovitis, bursitis and tenosynovitis. Archives ofPathology, 31, 731.
LICHTENSTEIN, L. (1955) Tumours of synovial joints, bursae andtendon sheaths. Cancer (Philadelphia), 8, 816.
MCMASTER, P.E. (1960) Pigmented villo-nodular synovitis withinvasion of bone. Report of six cases. Journal of Bone and JointSurgery, 42A, 1170.
by copyright. on 13 S
eptember 2018 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.58.685.716 on 1 Novem
ber 1982. Dow
nloaded from











![Remitting seronegative symmetrical synovitis with … · Remitting seronegative symmetrical synovitis with pitting oedema (RS3PE) is a rare rheumatologic ... [7]. However, cases of](https://img.pdfslide.net/doc/110x75/5adb86477f8b9a4a268b69df/remitting-seronegative-symmetrical-synovitis-with-seronegative-symmetrical-synovitis.jpg)

















