Embed Size (px)
Citation preview

Summary Statistics for Pediatric Psychiatric Visits to USEmergency Departments, 1993–1999
Marion R. Sills, MD, MPH, and Shayne D. Bland, MSc†
ABSTRACT. Objectives. To describe characteristics ofemergency department (ED) encounters for pediatric pa-tients with an acute mental health diagnosis.
Methods. Data are from the National Hospital Ambu-latory Medical Care Survey, which includes abstractsfrom the medical records of a national probability sam-ple of visits to EDs. Analysis was limited to records ofpatients who were younger than 19 years and had adiagnosis of either confirmed or suspected mental disor-der or a suicide attempt.
Results. There was an estimated annual average of434 000 ED pediatric mental health visits from 1993 to1999, an average annual rate of 326.8 visits per 10 000people. Visit rates varied by patient’s region, age, race,and gender. Psychosis was the diagnosis in 10.8% ofthese patients, and suicide attempt was the diagnosis in13.6%. ED pediatric mental health visits accounted for1.6% of all ED visits in this age group.
Conclusions. The significant increase in emergencydepartment pediatric mental health (EDPMH) visits from1993–1999 is greatest among patients who are non-white,teenaged, female, and live in the Northeast or Midwest.This variation in EDPMH visits may reflect variability inthe shortage of mental health providers. The lack ofincrease in the 2 categories of diagnoses mandatorilyseen in EDs—psychoses and suicide attempts—suggeststhat the overall rise in EDPMH visits may have beenattributable to nonurgent complaints more appropriatelymanaged by a primary mental health provider. Pediatrics2002;110(4). URL: http://www.pediatrics.org/cgi/content/full/110/4/e40; emergency services, psychiatric, emergencymedicine, mental disorders diagnosed in childhood, Na-tional Hospital Ambulatory Medical Care Survey.
ABBREVIATIONS. ED, emergency department; EDPMH, emer-gency department pediatric mental health (visit); NHAMCS, Na-tional Hospital Ambulatory Medical Care Survey; PSU, primarysampling unit; ESA, emergency service area; ICD-9-CM, Interna-tional Classification of Diseases, Ninth Revision, Clinical Modification.
Both lay1–3 and trade4–6 publications havedrawn attention to the escalating shortage ofmental health inpatient and outpatient re-
sources, and a Surgeon General’s report has calledthe shortage a “health crisis.”7 The online databases
of the US Department of Health and Human Ser-vices’ Bureau of Primary Health Care (bphc.hrsa.gov/databases/newhpsa/newhpsa.cfm) show that771 health service areas nationwide were designatedas underserved in the first 6 months of 2001.
The Methodology for Epidemiology of Mental Dis-orders in Children and Adolescents study estimatedthat almost 21% of US children ages 9 to 17 had adiagnosable mental or addictive disorder associatedwith at least minimum impairment.8 Between 6 mil-lion and 9 million children and adolescents haveserious emotional disturbances, accounting for 9% to13% of all children.9 There is little in the scientificliterature describing the characteristics of the cohortof US children who present to emergency depart-ments (EDs) with mental health–related diagnoses.
The purpose of this report was to describe thefrequency of emergency medical utilization and thepatient, drug, and visit characteristics for emergencydepartment pediatric mental health (EDPMH) visitsin the United States. We used the National HospitalAmbulatory Medical Care Survey (NHAMCS) to de-scribe the extent and characteristics of emergencymedical utilization for mental health disorders inchildren and adolescents. We examined differencesin utilization and treatment patterns during the pe-riod 1993 to 1999. The data presented here are im-portant for public health, clinical, and academic pur-poses related to disease prevalence, emergencymedicine research, and therapy guidelines and pro-jections.
METHODSData from the 1993–1999 NHAMCS were combined to generate
national estimates of ED visits for pediatric patients with a diag-nosis of either confirmed or suspected mental disorder or a suicideattempt. The NHAMCS is a multistage probability sample of visitsto hospital emergency and outpatient departments conducted an-nually by the National Center for Health Statistics, Centers forDisease Control and Prevention.10 Only the ED data were used forthis study. The survey period was from January 1, 1993, throughDecember 22, 1999.
The NHAMCS uses a 4-stage survey design that involves prob-ability samples of primary sampling units (PSUs), short-stay orgeneral hospitals within PSUs, emergency service areas (ESAs)within hospital EDs, and a systematic sample of approximately 50visits from each ED within the ESAs. The first-stage sample con-sisted of 112 of 1900 geographically defined PSUs that covered the50 states and the District of Columbia. The second-stage sample ofhospitals was from the 1991 SMG Hospital Market Database. Asample of 600 hospitals was randomly divided among 16 subsets,13 of which were used in any survey year. Each sampled hospitalwas inducted once every 15 months. US Bureau of Census fieldrepresentatives inducted the hospitals and formed a list of the
From the Department of Emergency Medicine, Children’s Hospital of Den-ver and University of Colorado Health Sciences Center, Denver, Colorado.Received for publication Apr 11, 2002; accepted Jun 26, 2002.Address correspondence to Marion R. Sills, MD, MPH, Children’s Hospitalof Denver, Department Pediatric Emergency Medicine, 1056 East Ave B251,Denver, CO 80218. E-mail: [email protected]†Deceased.PEDIATRICS (ISSN 0031 4005). Copyright © 2002 by the American Acad-emy of Pediatrics.
http://www.pediatrics.org/cgi/content/full/110/4/e40 PEDIATRICS Vol. 110 No. 4 October 2002 1 of 5 by guest on July 5, 2018www.aappublications.org/newsDownloaded from

emergency ESAs under the direction of the hospital’s ED. Up to 5ESAs from each sampled hospital were included. There were only2 hospitals that had �5 ESAs; in those cases, a sample of 5 wasselected. Only those hospitals with an ED were eligible to partic-ipate in the ED component. In the final stage of sampling, hospitalpersonnel used the daily patient logs during the randomly as-signed 4-week reporting period to identify the sampled cases andpull the appropriate medical records. Hospital staff abstracted thepatient, drug, and visit data from emergency medical records ontothe data collection instrument usually within 1 day of the visit.Because no patients were directly contacted and confidential iden-tifying information was not collected, the NHAMCS is exemptfrom institutional review board approval.
ED data were available from 579 hospitals during the 7 years(yearly range: 374–423), which represented an overall responserate of 96.5%. Abstracted data included up to 3 physician diag-noses; up to 3 reasons for visit or complaints as stated in thepatient’s (or patient surrogate’s) own words; up to 6 medicationsprescribed or provided; and various patient and visit characteris-tics, such as age, race, gender, diagnostic and therapeutic services,and visit disposition. Medications included all new or continueddrugs ordered, supplied, or administered at the visit; immuniza-tion and desensitizing agents; and anesthetics. Diagnoses wereclassified and coded according to the International Classification ofDiseases, Ninth Revision, Clinical Modification (ICD-9-CM).11 Pa-tient’s complaints were coded to the Reason for Visit Classification,12
and medications were assigned a therapeutic class from the Na-tional Drug Code Directory, 1995 Edition.13 All classification andcoding was performed centrally by the National Center for HealthStatistics.
Mental health disorder visits are based on records in which anyof the 3 physician diagnoses were coded 290–314.9. This broadcategory of mental health disorders included cases of psychoticdisorders, neurotic disorders, and personality disorders. Visits forsuicide attempts were identified on the basis of a record in whichany of the 3 reason-for-injury codes was E950 to E959. For pur-poses of this study, visits by patients who were older than 18 yearswere excluded. The sample records included 907 records consid-ered EDPMH visits out of 47 017 ED visits. Because of the absenceof unique patient identifiers in NHAMCS, we could not detectmultiple visits by the same person. We defined visits as “urgent”when they were categorized as “urgent/emergent” in the 1993–1996 surveys or as needing to be seen in �2 hours in the 1994–1999 surveys.
Sample weights were applied using Microsoft Access 97 (Mi-crosoft, Inc, Redmond, WA) to yield national annual estimates ofEDPMH visits. Population rates are based on the average of USBureau of the Census estimates of the civilian, noninstitutional-ized population of the United States as of July 1, 1993–1999, andhave been adjusted for net underenumeration.14 A multivariableregression model containing gender, age (0–6 years, 7–12 years,13–18 years), race (white, nonwhite), and region (Northeast, Mid-west, South, and West) was used. Analysis for trends comparedthe data from each of the 7 years of the study. The outcomevariable was the rate of EDPMH per 10 000 population at risk. Forassessing the significance of the variables in the models, the like-lihood ratio test (�2 statistic) was used. Data were analyzed usingSAS 8.1 Statistical Software (SAS Institute Inc, Cary, NC).
RESULTSAn estimated 3 034 855 EDPMH visits were made
from 1993 to 1999 by individuals who were 18 yearsand younger. The annual average of 433 551 visits(95% confidence interval: 382 407–484 695) providesan annual average rate of 326.8 visits per 10 000people (95% confidence interval: 290.6–363.0). Thesevisits represented 1.6% of all ED visits by people 18years and younger. EDPMH visits accounted for3.2% of all ED visits ending with admission to inpa-tient status for this age group. The chief complaint ofpatients in 9.6% of EDPMH visits was “psychologicaland mental disorder, not elsewhere classified.” Al-though “psychological and mental disorder, not else-where classified” was the predominant chief com-
plaint, “adverse effect of drug abuse,” “depression,”and “headache” accounted for another 15.4% of vis-its.
The percentage distribution of EDPMH visits bypatient characteristics is shown in Table 1 along withpopulation rates. The mean age for EDPMH visitswas 14.6 years. Seventy-one percent were teenagers,50.5% were girls, and 77.8% were white.
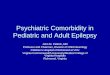
The population-based rates of EDPMH visits byyear from Table 1 are shown in Fig 1. Figure 1 showsa rising slope for all EDPMH visits; however, theslopes are flat for visits with a diagnosis of suicideattempt or self-injury (ICD-9-CM codes E950–E959)and psychotic disorders (ICD-9-CM codes 290–299).
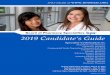
Figure 2 shows the population-adjusted rates ofEDPMHs by age, gender, race, region, and year. Thepopulation rate was greatest among teenagers andleast among children 6 years and younger. Girls were5% more likely to have an EDPMH than were boys,and whites were 2% less likely to have an EDPMHthan were nonwhites. Children and adolescents inthe Northeast region were much more likely to havean EDPMH visit than were people in the West re-gion. Overall, 67.2% of EDPMH visits were consid-ered “urgent”; this percentage rose 2.0 points annu-ally.
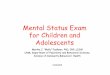
The 3 most common principal diagnoses amongEDPMH visits were “unspecified neurotic disorder,”“depressive disorder,” and “anxiety states,” account-ing for 13.1%, 12.9%, and 11.4% of visits, respec-tively. When grouped by the multiaxial assessmentclassification of the Diagnostic and Statistical Manualof Mental Disorders, Fourth Edition,15 the most com-mon axis I disorders were “substance related disor-ders” (24.2%), “anxiety disorders” (16.6%), and “at-tention deficit and disruptive disorders” (11.3%; Fig
TABLE 1. Number and Annual Rate of EDPMH Visits andOdds Ratio for the Association Among Age, Gender, Race, Region,and Year and Population-Adjusted EDPMH Visits, 1993–1999
Parameter No. ofVisits
Rate per10 000
Population
Odds Ratio Estimate(95% Confidence Interval)
All EDPMH 3 034 855 59.3Age (y)
0–6 318 063 16.3 0.120 (0.119–0.120)7–12 549 351 34.0 0.296 (0.295–0.297)13–18 2 167 441 139.5 Referent
GenderFemale 1 532 708 61.5 1.103 (1.101–1.106)Male 1 502 147 57.2 Referent
RaceWhite 2 360 625 58.5 0.959 (0.956–0.961)Nonwhite 674 230 62.2 Referent
RegionsNortheast 781 038 88.9 1.697 (1.691–1.702)Midwest 795 946 70.1 1.260 (1.256–1.264)South 844 048 50.1 0.907 (0.904–0.910)West 613 823 54.6 Referent
Year1993 305 219 43.3 0.775 (0.772–0.779)1994 425 323 59.5 1.052 (1.048–1.056)1995 438 782 60.6 1.056 (1.051–1.060)1996 404 248 55.1 1.024 (1.020–1.028)1997 474 081 64.0 1.087 (1.083–1.092)1998 527 669 70.6 1.303 (1.298–1.308)1999 459 533 61.0 Referent
2 of 5 PEDIATRIC PSYCHIATRIC EMERGENCY DEPARTMENT VISITS by guest on July 5, 2018www.aappublications.org/newsDownloaded from

3). The 10 most common causes of self-inflicted in-jury or poisoning among EDPMH visits during thestudy period are shown in Table 2.
Among EDPMH visits, 47.1% received at least 1
medication, although only 20.4% received �1 medi-cation. The most commonly given medication wascharcoal, administered in 5.6% of visits (Table 3).Tylenol, Ritalin, and Ativan were the next most com-
Fig 1. Population-adjusted trends inpediatric psychiatric emergencies, sui-cide attempts, and psychotic presenta-tions, 1993–1999.
Fig 2. Population-adjusted rate ofEDPMH visits, 1993–1999.
Fig 3. Most common diagnoses for EDPMH visits, 1993–1999.
http://www.pediatrics.org/cgi/content/full/110/4/e40 3 of 5 by guest on July 5, 2018www.aappublications.org/newsDownloaded from

monly given medications. The mean number of med-ications given was 0.79 per EDPMH visit; for non-EDPMH ED visits, this number was 1.21 per visit.
The disposition data show that 19.4% of EDPMHvisits ended with admission for inpatient care, 8.9%of which were admitted directly to the intensive careunits of the hospital from the ED. In comparison,9.4% of all non-EDPMH ED visits in this age groupended in admission, 4.5 of whom were admitteddirectly to intensive care units. Of all EDPMH visits,15.8% were transferred to other facilities and 33.4%were referred to another clinic. Approximately 3.3%of the EDPMH visits ended with the patient’s deathor death on arrival to the ED. It is possible that someof those patients who were admitted to the hospitalsubsequently died.
DISCUSSIONA significant shift occurred in both the frequency
and the patient characteristics of EDPMHs between1993 and 1999. The increase in EDPMHs during the 7
years is primarily attributable to patients without amore emergent psychiatric diagnosis, such as suicideattempt or psychotic disorder. There is a higher pop-ulation-adjusted rate of EDPMHs in the Northeastand Midwest, as well as among nonwhites, girls, andadolescents. The most common axis I disorders were“substance related disorders,” “anxiety disorders,”and “attention deficit and disruptive disorders.” Themajority of patients received no medications, andonly 35% were either admitted or transferred to an-other facility.
The primary indicator for relative resource utiliza-tion in NHAMCS is rate of hospitalization; length ofED stay and cost information are not included in thedata set. EDPMH patients are admitted to both thegeneral ward and the intensive care unit at a higherrate than are non-EDPMH ED patients in this agegroup, indicating a higher relative resource utiliza-tion rate. Although EDPMHs account for only 1.6%of all ED visits, this suggests that they representresource utilization greater than is predicted by thissmall percentage.
Limitations of using NHAMCS data to describeEDPMH visits include that the NHAMCS does notpermit evaluation of the need for resources used,such as medication or hospitalization, based on clin-ical characteristics such as the results of a psycholog-ical evaluation. In addition, there may be underre-porting of medications or other tests performed inthe ED that are so routine that they are not recorded,such as blood pressure, electrocardiogram, or admin-istration of aspirin. Before the 1997 NHAMCS sur-vey, there was no distinction between suspected andconfirmed diagnoses, which limits the value of ED-PMH figures for survey years before 1997. TheNHAMCS does not include federal hospitals withinthe scope of the survey, although it is doubtful thatthe number of EDPMH visits in the United Stateswould be higher if visits to veteran administrationand military hospitals were considered. The smallsample of hospitals (494 nationally) precludes anequally small standard error for national estimatesfor black patients compared with white patients andfor younger patients compared with adolescent pa-tients. Combining data from multiple years helps butdoes not solve this problem. There may be codingerror as well: the quality control procedure allows forup to a 5% error rate on diagnostic and reason for
TABLE 2. Number and Percentage Distribution of EDPMH Visits by Cause of Injury or Poisoning for Patients With Suicide Attemptor Self-Inflicted Injury or Poisoning: Top 10 Causes Averaged Over 1993–1999
Principal Cause of Self-Inflicted Injury or Poisoning* ICD-9-CMCode
No. ofVisits
Percentageof Visits
Poisoning by unspecified drug or medicinal substance E9505 91 986 3.0Poisoning by analgesics, antipyretics, and antirheumatics E9500 87 840 2.9Poisoning by other specified drugs and medicinal substances E9504 47 905 1.6Injury by cutting and piercing instrument E9560 32 175 1.1Injury by hanging E9530 30 735 1.0Poisoning by tranquilizers and other psychotropic agents E9503 39 245 1.0Injury by other specified means E9588 27 094 0.9Poisoning by other and unspecified solid and liquid substances E9509 23 748 0.8Injury by unspecified means E9589 11 825 0.4Injury by hanging, strangulation, or suffocation of unspecified means E9539 8510 0.3
* Based on the ICD-9-CM, 4-digit E-code.
TABLE 3. Number and Percentage of Visits With the 25 MostCommonly Administered Drugs Mentioned in EDPMH Visits,Averaged Over 1993–1999
Medication No. ofEDPMH Visits
Percentage ofEDPMH Visits
Charcoal 170 633 5.6Tylenol 154 773 5.1Ritalin 92 763 3.1Ativan 85 382 2.8Phenergan 62 422 2.1Albuterol sulfate 62 287 2.1Haldol 61 887 2.0Prozac 56 471 1.9Benadryl 54 659 1.8Xanax 52 453 1.7Vistaril 52 233 1.7Compazine 39 342 1.3Valium 38 113 1.3Naprosyn 32 528 1.1Zoloft 30 358 1.0Ipecac 29 006 1.0Paxil 28 130 0.9Diphtheria tetanus toxoids 27 882 0.9Depakote 27 175 0.9Lithium 25 025 0.8Cogentin 23 654 0.8Doxycycline 23 270 0.8Ibuprofen 22 437 0.7Dilantin 20 380 0.7Narcan 20 054 0.7
4 of 5 PEDIATRIC PSYCHIATRIC EMERGENCY DEPARTMENT VISITS by guest on July 5, 2018www.aappublications.org/newsDownloaded from

visit classification, although the observed coding er-ror rate was �2% overall. Despite the limitationspresented here, these factors do not affect the trenddata because the same limitations apply for all yearsof NHAMCS data.
The ED is only 1 of several clinical settings inwhich children and adolescents may present formental health concerns; other settings include mentalhealth care provider offices (specialty and nonspe-cialty), primary medical care provider offices, com-munity mental health centers, youth crisis centers,and the juvenile justice system. Our data refer only toED utilization and do not reflect all emergent pedi-atric mental health encounters.
CONCLUSIONA significant shift occurred in both the frequency
and the patient characteristics of EDPMHs between1993 and 1999. The increase in EDPMHs during the 7years is greatest among patients who are nonwhite,adolescent, and female and live in the Northeast orMidwest. This variation in EDPMH may reflect vari-ability in the shortage of mental health providers ona regional and/or a local basis. The lack of increase inthe 2 categories of diagnoses mandatorily seen inEDs—psychoses and suicide attempts—suggests thatsome of the overall rise in EDPMH visits was attrib-utable to less urgent mental health complaints andlikely represents decreased access to regular mentalhealth care.
EDs are often poorly staffed for evaluation andtreatment of pediatric mental health problems. Fu-ture research might address factors related to in-creasing utilization of the ED for pediatric mentalhealth problems. An evidence-based approach tochildren’s mental health problems should be di-rected toward guiding the referral process so as toevaluate the impact of care on costs, long-term men-tal health (including adult mental health problems),and impact on other systems, including the juvenilejustice system, schools, and the emergency medicalsystem.
REFERENCES1. Whaley S. Mental health clinics battle staff shortages: state struggling
with recruitment of psychiatrists. Las Vegas Review-Journal. September14, 2001. Available at: www.lvrj.com/lvrj�home/2001/Sep-14-Fri-2001/news/16996880.html
2. Bonfield T. Children’s to expand psychiatric treatment. Cincinnati En-quirer. November 27, 2001. Available at: enquirer.com/editions/2001/11/27/loc�childrens�to�expand.html
3. Richmond E. Lawmakers told mentally ill, drunks crowd LV hospitals.Las Vegas Sun. January 9, 2001. Available at: www.lasvegassun.com/sunbin/stories/archives/2002/jan/09/512865059.html
4. Chamberlin J. Easing children’s psychological distress in the emergencyroom. Monitor Psychol. 2000;31:40–42
5. Sherer R. Mental health care shortages will need creative solutions.Psychiatric Times. 2001;September(suppl 1):1–2
6. Washington State Emergency Medical Services for Children. HospitalEmergency Departments and Children/Adolescents With Mental Health Con-cerns in Washington State. Final Report. Seattle, WA: Department ofHealth and Human Services, Health Resources and Services Adminis-tration Emergency Medical Services for Children; 2001
7. Office of the Surgeon General, Department of Health and HumanServices. Report of the surgeon general’s conference on children’s men-tal health: a national action agenda. Presented at the Surgeon General’sConference on Children’s Mental Health; September 2000; Washington,DC
8. Shaffer D, Fisher P, Dulcan MK, et al. The NIMH Diagnostic InterviewSchedule for Children Version 2.3 (DISC-2.3): description, acceptability,prevalence rates, and performance in the MECA Study. Methods for theEpidemiology of Child and Adolescent Mental Disorders Study. J AmAcad Child Adolesc Psychiatry. 1996;35:865–877
9. Friedman R, Katz-Leavy J, Manderscheid R, Sondheimer D. Prevalenceof serious emotional disturbance in children and adolescents. In:Manderscheid RW, Sonnenschein MA, eds. Mental Health, United States.Washington, DC: US Government Printing Office; 1996:77–112
10. McCaig LF, McLemore T. Plan and operation of the National HospitalAmbulatory Medical Care Survey. National Center for Health Statistics.Vital Health Stat 1. 1994;34:1–78
11. Public Health Service and Health Care Financing Administration. Inter-national Classification of Diseases, Ninth Revision, Clinical Modification. 4thed. Washington, DC: Public Health Service; 1991
12. Schneider D, Appleton L, McLemore T. A reason for visit classificationfor ambulatory care. National Center for Health Statistics. Vital HealthStat 2. 1979;(78):i–vi, 1–63
13. Food and Drug Administration. National Drug Code Directory. Washing-ton, DC: Public Health Service; 1995
14. Public Use Data File Documentation: 1993, 1994, 1995, 1996, 1997, 1998,1999 National Hospital Ambulatory Medical Care Survey. Hyattsville,MD: National Center for Health Statistics; 1994, 1995, 1996, 1997, 1998,1999, 2000
15. American Psychiatric Association. Diagnostic and Statistical Manual ofMental Disorders. 4th ed. Washington, DC: American PsychiatricAssociation; 2000
http://www.pediatrics.org/cgi/content/full/110/4/e40 5 of 5 by guest on July 5, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.110.4.e402002;110;e40Pediatrics
Marion R. Sills and Shayne D. Bland1999−Departments, 1993
Summary Statistics for Pediatric Psychiatric Visits to US Emergency
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/110/4/e40including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/110/4/e40#BIBLThis article cites 5 articles, 0 of which you can access for free at:
Subspecialty Collections
_subhttp://www.aappublications.org/cgi/collection/psychiatry_psychologyPsychiatry/Psychologyfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on July 5, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.110.4.e402002;110;e40Pediatrics
Marion R. Sills and Shayne D. Bland1999−Departments, 1993
Summary Statistics for Pediatric Psychiatric Visits to US Emergency
http://pediatrics.aappublications.org/content/110/4/e40located on the World Wide Web at:
The online version of this article, along with updated information and services, is
1073-0397. ISSN:60007. Copyright © 2002 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on July 5, 2018www.aappublications.org/newsDownloaded from