Embed Size (px)
Citation preview
11Surgical approachesto the heart
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01448-0 - Wilcox’s Surgical Anatomy of the Heart: Fourth editionRobert H. Anderson, Diane E. Spicer, Anthony M. Hlavacek, Andrew C. Cook and Carl L. BackerExcerptMore information
When we describe the heart in this chapter,and in subsequent chapters, our accountwill be based on the organ as viewed in itsanatomical position1. Where appropriate,the heart will be illustrated as it would beviewed by the surgeon during an operativeprocedure, irrespective of whether thepictures are taken in the operating room, orare photographs of autopsied hearts. Whenwe show an illustration in non-surgicalorientation, this will be clearly stated.
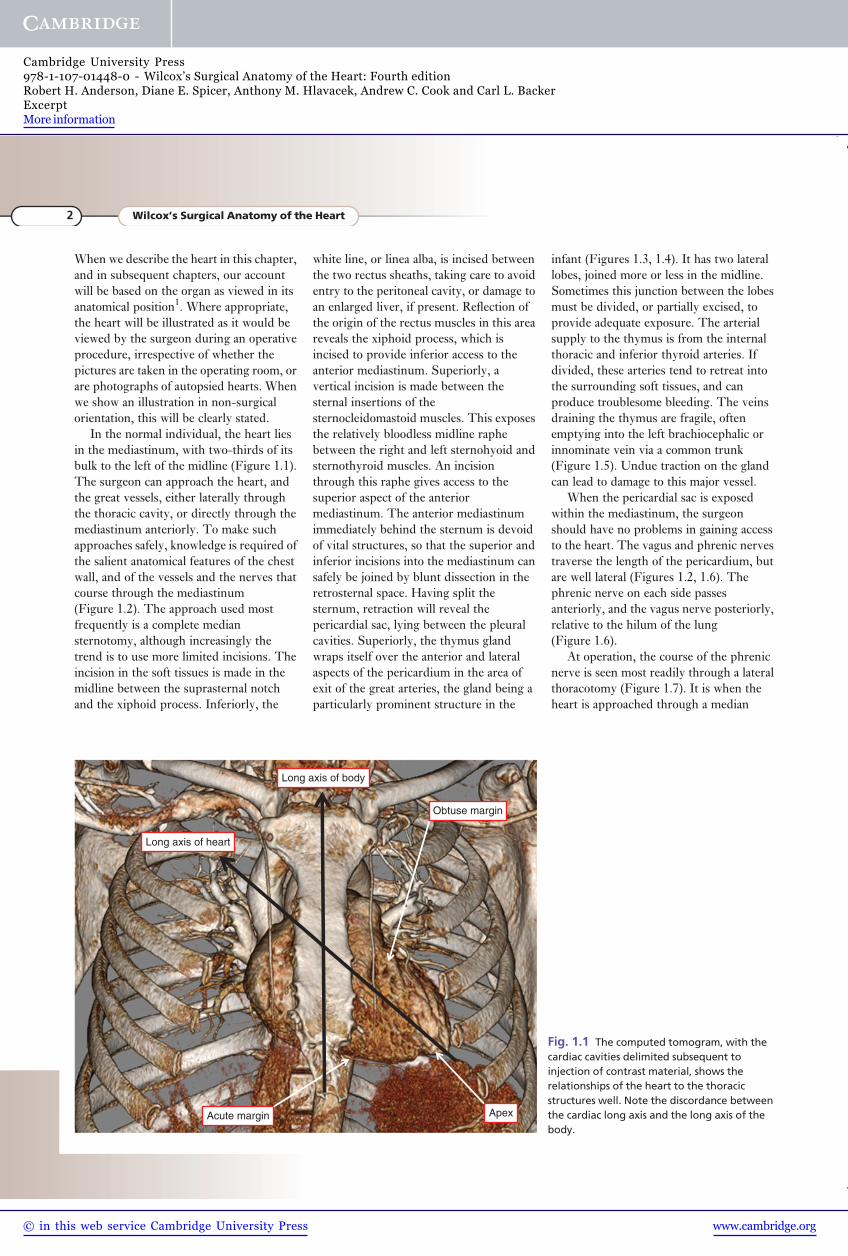
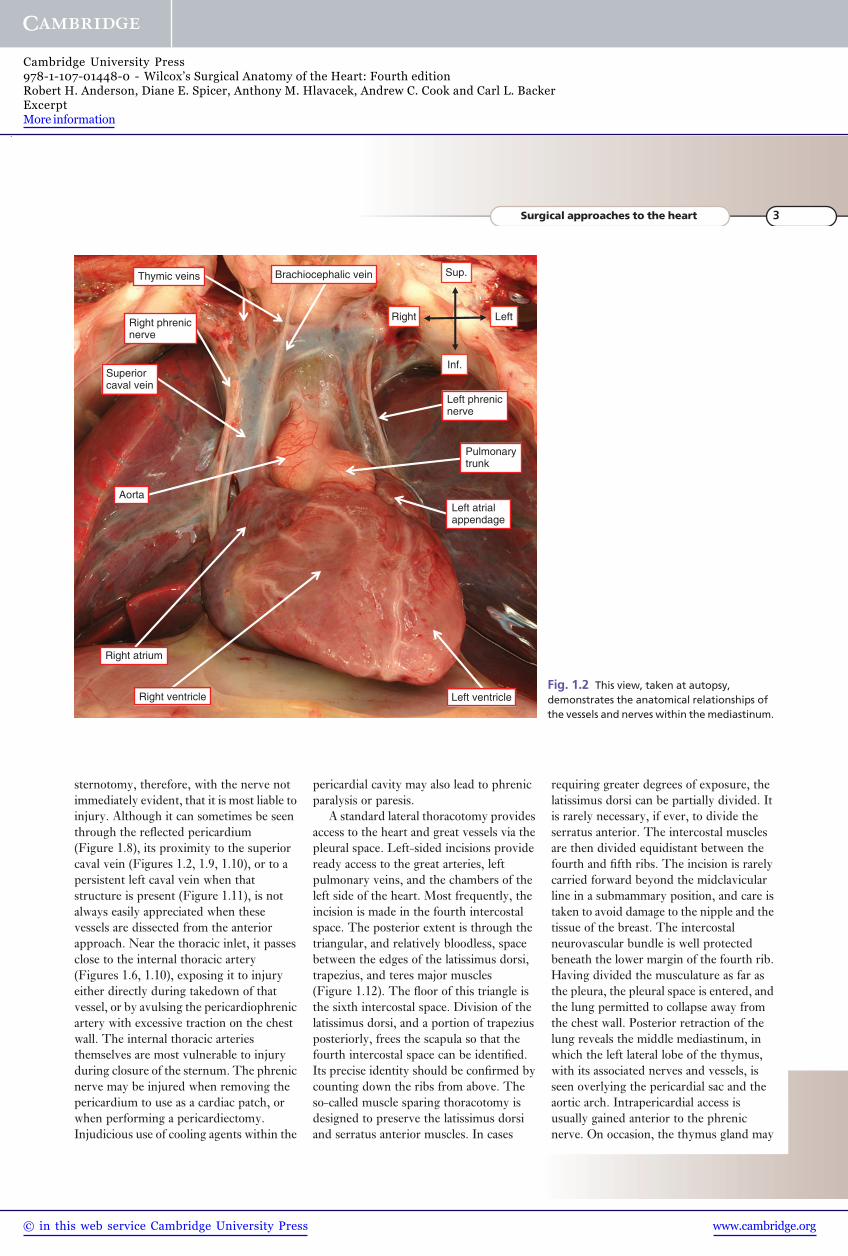
In the normal individual, the heart liesin the mediastinum, with two-thirds of itsbulk to the left of the midline (Figure 1.1).The surgeon can approach the heart, andthe great vessels, either laterally throughthe thoracic cavity, or directly through themediastinum anteriorly. To make suchapproaches safely, knowledge is required ofthe salient anatomical features of the chestwall, and of the vessels and the nerves thatcourse through the mediastinum(Figure 1.2). The approach used mostfrequently is a complete mediansternotomy, although increasingly thetrend is to use more limited incisions. Theincision in the soft tissues is made in themidline between the suprasternal notchand the xiphoid process. Inferiorly, the
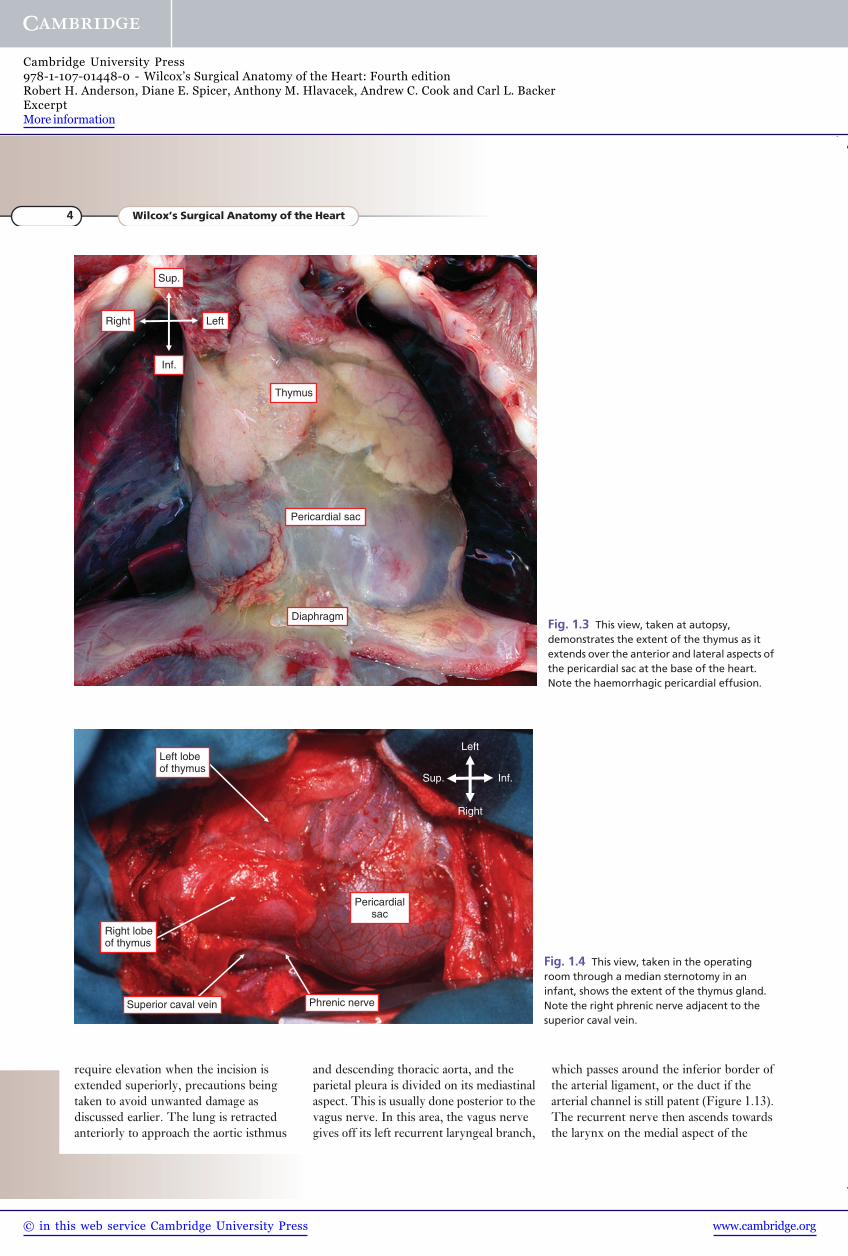
white line, or linea alba, is incised betweenthe two rectus sheaths, taking care to avoidentry to the peritoneal cavity, or damage toan enlarged liver, if present. Reflection ofthe origin of the rectus muscles in this areareveals the xiphoid process, which isincised to provide inferior access to theanterior mediastinum. Superiorly, avertical incision is made between thesternal insertions of thesternocleidomastoid muscles. This exposesthe relatively bloodless midline raphebetween the right and left sternohyoid andsternothyroid muscles. An incisionthrough this raphe gives access to thesuperior aspect of the anteriormediastinum. The anterior mediastinumimmediately behind the sternum is devoidof vital structures, so that the superior andinferior incisions into the mediastinum cansafely be joined by blunt dissection in theretrosternal space. Having split thesternum, retraction will reveal thepericardial sac, lying between the pleuralcavities. Superiorly, the thymus glandwraps itself over the anterior and lateralaspects of the pericardium in the area ofexit of the great arteries, the gland being aparticularly prominent structure in the
infant (Figures 1.3, 1.4). It has two laterallobes, joined more or less in the midline.Sometimes this junction between the lobesmust be divided, or partially excised, toprovide adequate exposure. The arterialsupply to the thymus is from the internalthoracic and inferior thyroid arteries. Ifdivided, these arteries tend to retreat intothe surrounding soft tissues, and canproduce troublesome bleeding. The veinsdraining the thymus are fragile, oftenemptying into the left brachiocephalic orinnominate vein via a common trunk(Figure 1.5). Undue traction on the glandcan lead to damage to this major vessel.
When the pericardial sac is exposedwithin the mediastinum, the surgeonshould have no problems in gaining accessto the heart. The vagus and phrenic nervestraverse the length of the pericardium, butare well lateral (Figures 1.2, 1.6). Thephrenic nerve on each side passesanteriorly, and the vagus nerve posteriorly,relative to the hilum of the lung(Figure 1.6).
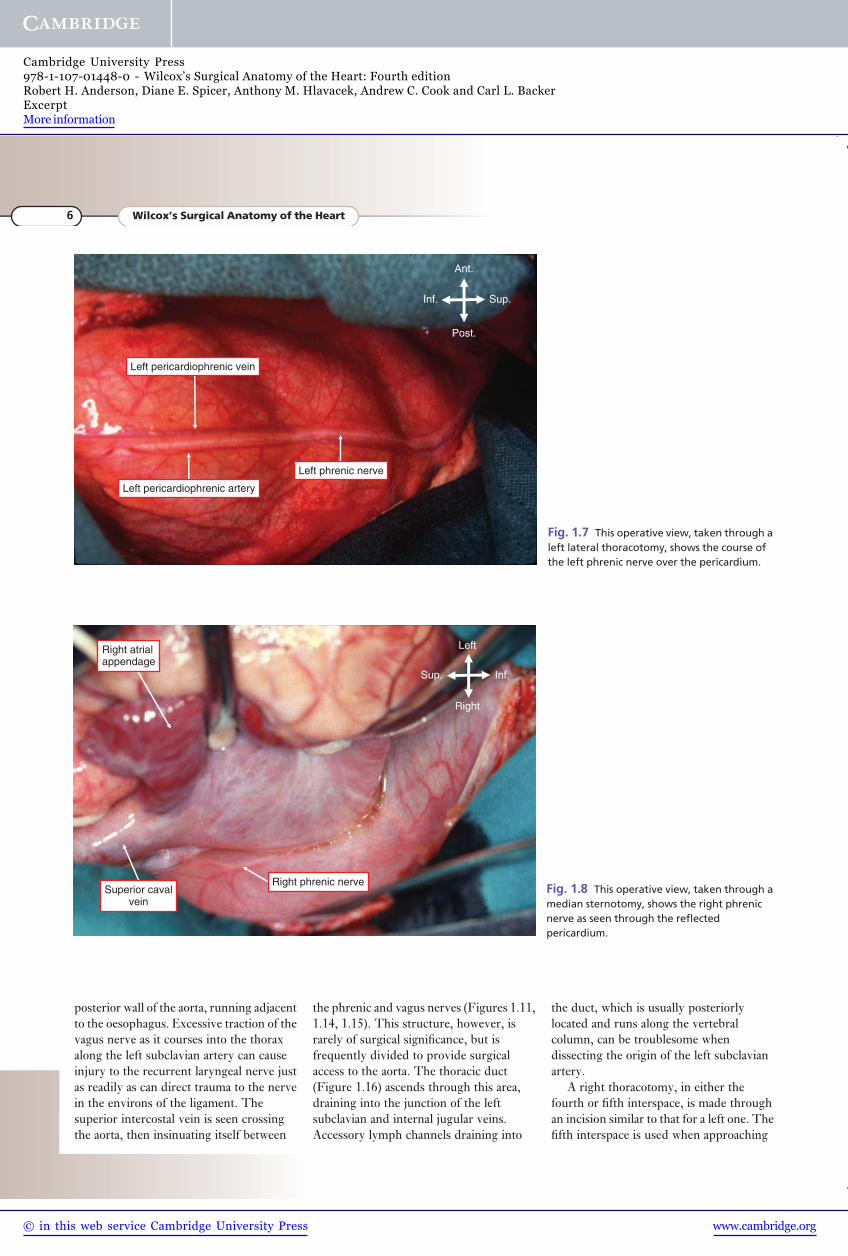
At operation, the course of the phrenicnerve is seen most readily through a lateralthoracotomy (Figure 1.7). It is when theheart is approached through a median
Obtuse margin
Acute margin Apex
Long axis of heart
Long axis of body
Fig. 1.1 The computed tomogram, with thecardiac cavities delimited subsequent toinjection of contrast material, shows therelationships of the heart to the thoracicstructures well. Note the discordance betweenthe cardiac long axis and the long axis of thebody.
2 Wilcox’s Surgical Anatomy of the Heart
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01448-0 - Wilcox’s Surgical Anatomy of the Heart: Fourth editionRobert H. Anderson, Diane E. Spicer, Anthony M. Hlavacek, Andrew C. Cook and Carl L. BackerExcerptMore information
sternotomy, therefore, with the nerve notimmediately evident, that it is most liable toinjury. Although it can sometimes be seenthrough the reflected pericardium(Figure 1.8), its proximity to the superiorcaval vein (Figures 1.2, 1.9, 1.10), or to apersistent left caval vein when thatstructure is present (Figure 1.11), is notalways easily appreciated when thesevessels are dissected from the anteriorapproach. Near the thoracic inlet, it passesclose to the internal thoracic artery(Figures 1.6, 1.10), exposing it to injuryeither directly during takedown of thatvessel, or by avulsing the pericardiophrenicartery with excessive traction on the chestwall. The internal thoracic arteriesthemselves are most vulnerable to injuryduring closure of the sternum. The phrenicnerve may be injured when removing thepericardium to use as a cardiac patch, orwhen performing a pericardiectomy.Injudicious use of cooling agents within the
pericardial cavity may also lead to phrenicparalysis or paresis.
A standard lateral thoracotomy providesaccess to the heart and great vessels via thepleural space. Left-sided incisions provideready access to the great arteries, leftpulmonary veins, and the chambers of theleft side of the heart. Most frequently, theincision is made in the fourth intercostalspace. The posterior extent is through thetriangular, and relatively bloodless, spacebetween the edges of the latissimus dorsi,trapezius, and teres major muscles(Figure 1.12). The floor of this triangle isthe sixth intercostal space. Division of thelatissimus dorsi, and a portion of trapeziusposteriorly, frees the scapula so that thefourth intercostal space can be identified.Its precise identity should be confirmed bycounting down the ribs from above. Theso-called muscle sparing thoracotomy isdesigned to preserve the latissimus dorsiand serratus anterior muscles. In cases
requiring greater degrees of exposure, thelatissimus dorsi can be partially divided. Itis rarely necessary, if ever, to divide theserratus anterior. The intercostal musclesare then divided equidistant between thefourth and fifth ribs. The incision is rarelycarried forward beyond the midclavicularline in a submammary position, and care istaken to avoid damage to the nipple and thetissue of the breast. The intercostalneurovascular bundle is well protectedbeneath the lower margin of the fourth rib.Having divided the musculature as far asthe pleura, the pleural space is entered, andthe lung permitted to collapse away fromthe chest wall. Posterior retraction of thelung reveals the middle mediastinum, inwhich the left lateral lobe of the thymus,with its associated nerves and vessels, isseen overlying the pericardial sac and theaortic arch. Intrapericardial access isusually gained anterior to the phrenicnerve. On occasion, the thymus gland may
Right Left
Inf.
Sup.Brachiocephalic veinThymic veins
Right phrenicnerve
Superiorcaval vein
Aorta
Right atrium
Right ventricle Left ventricle
Left atrialappendage
Pulmonarytrunk
Left phrenicnerve
Fig. 1.2 This view, taken at autopsy,demonstrates the anatomical relationships ofthe vessels and nerves within the mediastinum.
Surgical approaches to the heart 3
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01448-0 - Wilcox’s Surgical Anatomy of the Heart: Fourth editionRobert H. Anderson, Diane E. Spicer, Anthony M. Hlavacek, Andrew C. Cook and Carl L. BackerExcerptMore information
require elevation when the incision isextended superiorly, precautions beingtaken to avoid unwanted damage asdiscussed earlier. The lung is retractedanteriorly to approach the aortic isthmus
and descending thoracic aorta, and theparietal pleura is divided on its mediastinalaspect. This is usually done posterior to thevagus nerve. In this area, the vagus nervegives off its left recurrent laryngeal branch,
which passes around the inferior border ofthe arterial ligament, or the duct if thearterial channel is still patent (Figure 1.13).The recurrent nerve then ascends towardsthe larynx on the medial aspect of the
Diaphragm
Sup.
Inf.
LeftRight
Pericardial sac
Thymus
Fig. 1.3 This view, taken at autopsy,demonstrates the extent of the thymus as itextends over the anterior and lateral aspects ofthe pericardial sac at the base of the heart.Note the haemorrhagic pericardial effusion.
Pericardialsac
Sup. Inf.
Left
Right
Left lobeof thymus
Right lobeof thymus
Superior caval vein Phrenic nerve
Fig. 1.4 This view, taken in the operatingroom through a median sternotomy in aninfant, shows the extent of the thymus gland.Note the right phrenic nerve adjacent to thesuperior caval vein.
4 Wilcox’s Surgical Anatomy of the Heart
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01448-0 - Wilcox’s Surgical Anatomy of the Heart: Fourth editionRobert H. Anderson, Diane E. Spicer, Anthony M. Hlavacek, Andrew C. Cook and Carl L. BackerExcerptMore information
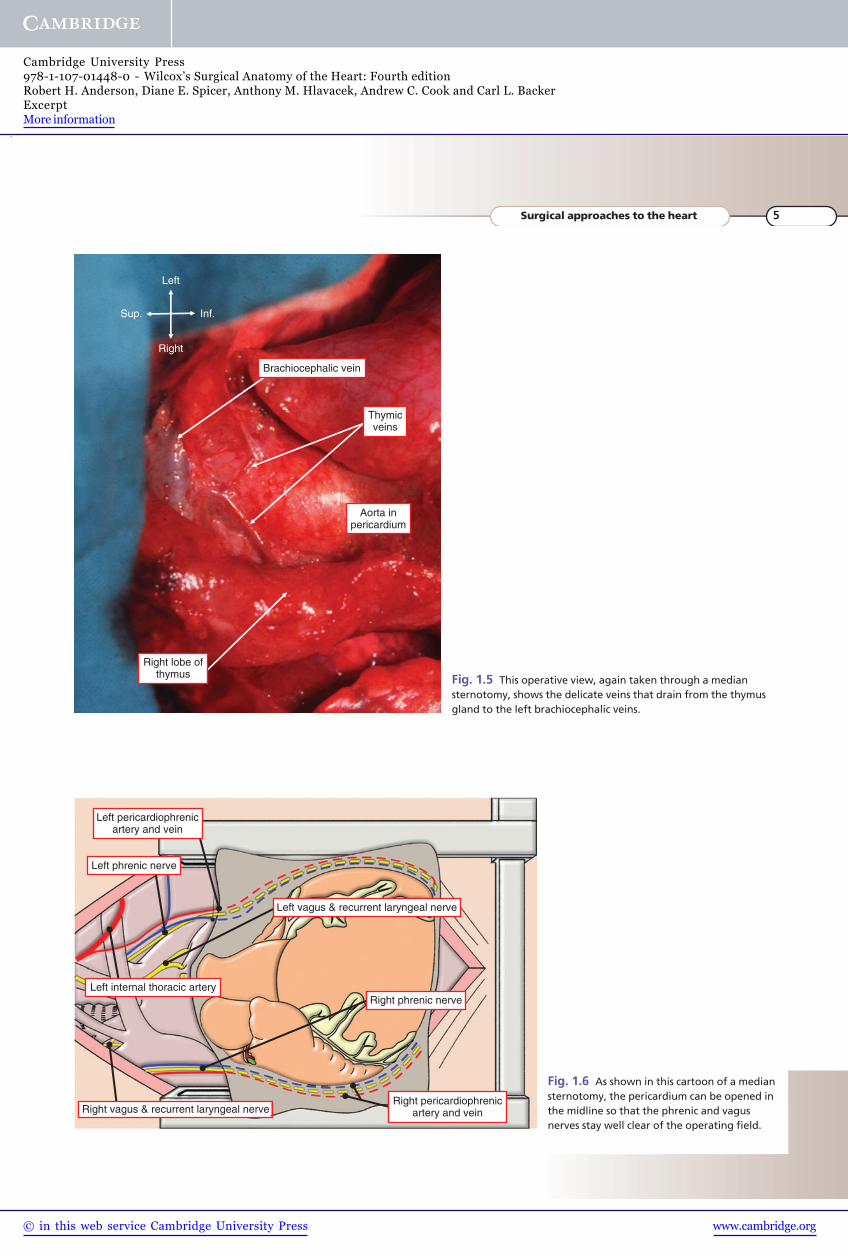
Sup. Inf.
Left
Right
Aorta inpericardium
Right lobe ofthymus
Thymicveins
Brachiocephalic vein
Fig. 1.5 This operative view, again taken through a mediansternotomy, shows the delicate veins that drain from the thymusgland to the left brachiocephalic veins.
Left phrenic nerve
Left pericardiophrenicartery and vein
Left vagus & recurrent laryngeal nerve
Left internal thoracic arteryRight phrenic nerve
Right vagus & recurrent laryngeal nerveRight pericardiophrenic
artery and vein
Fig. 1.6 As shown in this cartoon of a mediansternotomy, the pericardium can be opened inthe midline so that the phrenic and vagusnerves stay well clear of the operating field.
Surgical approaches to the heart 5
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01448-0 - Wilcox’s Surgical Anatomy of the Heart: Fourth editionRobert H. Anderson, Diane E. Spicer, Anthony M. Hlavacek, Andrew C. Cook and Carl L. BackerExcerptMore information
posterior wall of the aorta, running adjacentto the oesophagus. Excessive traction of thevagus nerve as it courses into the thoraxalong the left subclavian artery can causeinjury to the recurrent laryngeal nerve justas readily as can direct trauma to the nervein the environs of the ligament. Thesuperior intercostal vein is seen crossingthe aorta, then insinuating itself between
the phrenic and vagus nerves (Figures 1.11,1.14, 1.15). This structure, however, israrely of surgical significance, but isfrequently divided to provide surgicalaccess to the aorta. The thoracic duct(Figure 1.16) ascends through this area,draining into the junction of the leftsubclavian and internal jugular veins.Accessory lymph channels draining into
the duct, which is usually posteriorlylocated and runs along the vertebralcolumn, can be troublesome whendissecting the origin of the left subclavianartery.
A right thoracotomy, in either thefourth or fifth interspace, is made throughan incision similar to that for a left one. Thefifth interspace is used when approaching
Ant.
Post.
Inf. Sup.
Left pericardiophrenic artery
Left pericardiophrenic vein
Left phrenic nerve
Fig. 1.7 This operative view, taken through aleft lateral thoracotomy, shows the course ofthe left phrenic nerve over the pericardium.
Sup. Inf.
Left
Right
Right atrialappendage
Superior cavalvein
Right phrenic nerveFig. 1.8 This operative view, taken through amedian sternotomy, shows the right phrenicnerve as seen through the reflectedpericardium.
6 Wilcox’s Surgical Anatomy of the Heart
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01448-0 - Wilcox’s Surgical Anatomy of the Heart: Fourth editionRobert H. Anderson, Diane E. Spicer, Anthony M. Hlavacek, Andrew C. Cook and Carl L. BackerExcerptMore information
Sup. Inf.
Left
Right
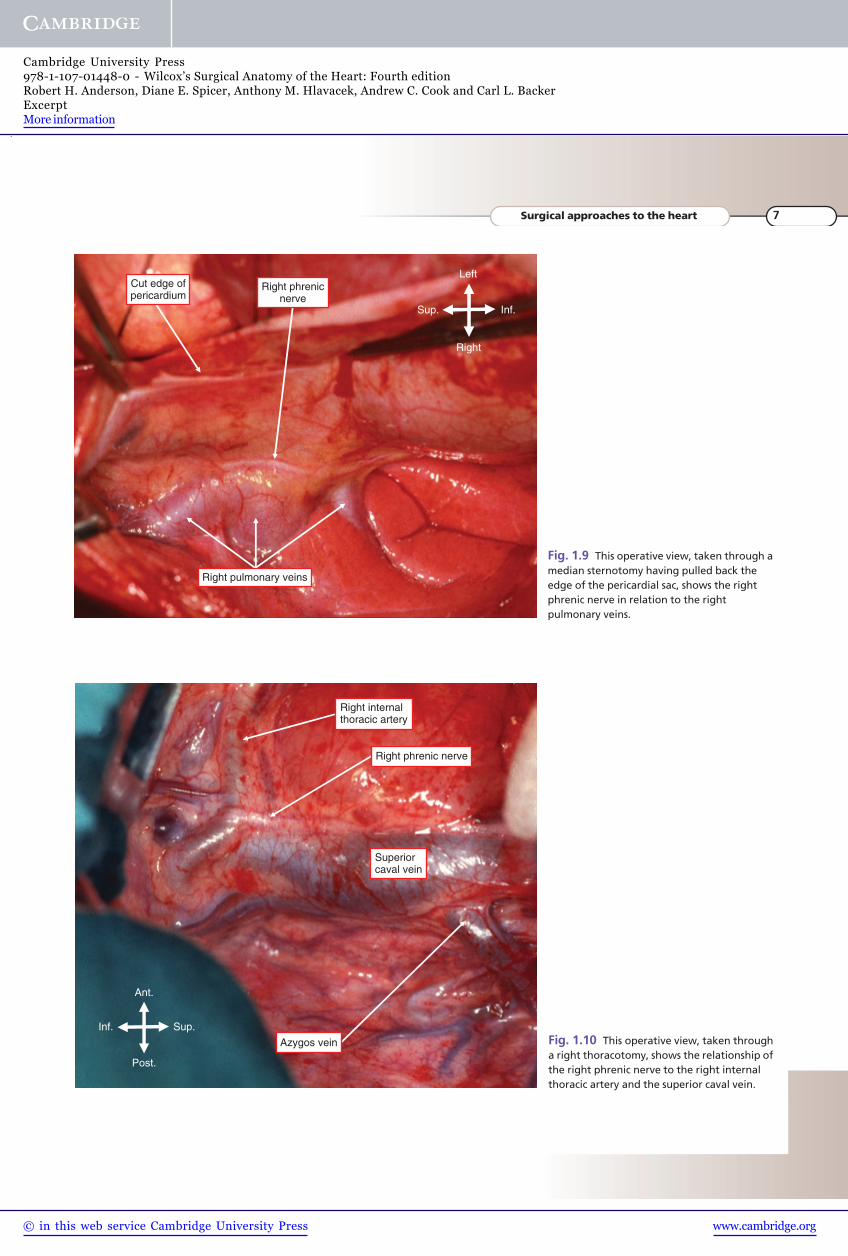
Cut edge ofpericardium
Right phrenicnerve
Right pulmonary veins
Fig. 1.9 This operative view, taken through amedian sternotomy having pulled back theedge of the pericardial sac, shows the rightphrenic nerve in relation to the rightpulmonary veins.
Superiorcaval vein
Ant.
Post.
Inf. Sup.
Right internalthoracic artery
Right phrenic nerve
Azygos vein Fig. 1.10 This operative view, taken througha right thoracotomy, shows the relationship ofthe right phrenic nerve to the right internalthoracic artery and the superior caval vein.
Surgical approaches to the heart 7
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01448-0 - Wilcox’s Surgical Anatomy of the Heart: Fourth editionRobert H. Anderson, Diane E. Spicer, Anthony M. Hlavacek, Andrew C. Cook and Carl L. BackerExcerptMore information
Ant.
Post.
Inf. Sup.
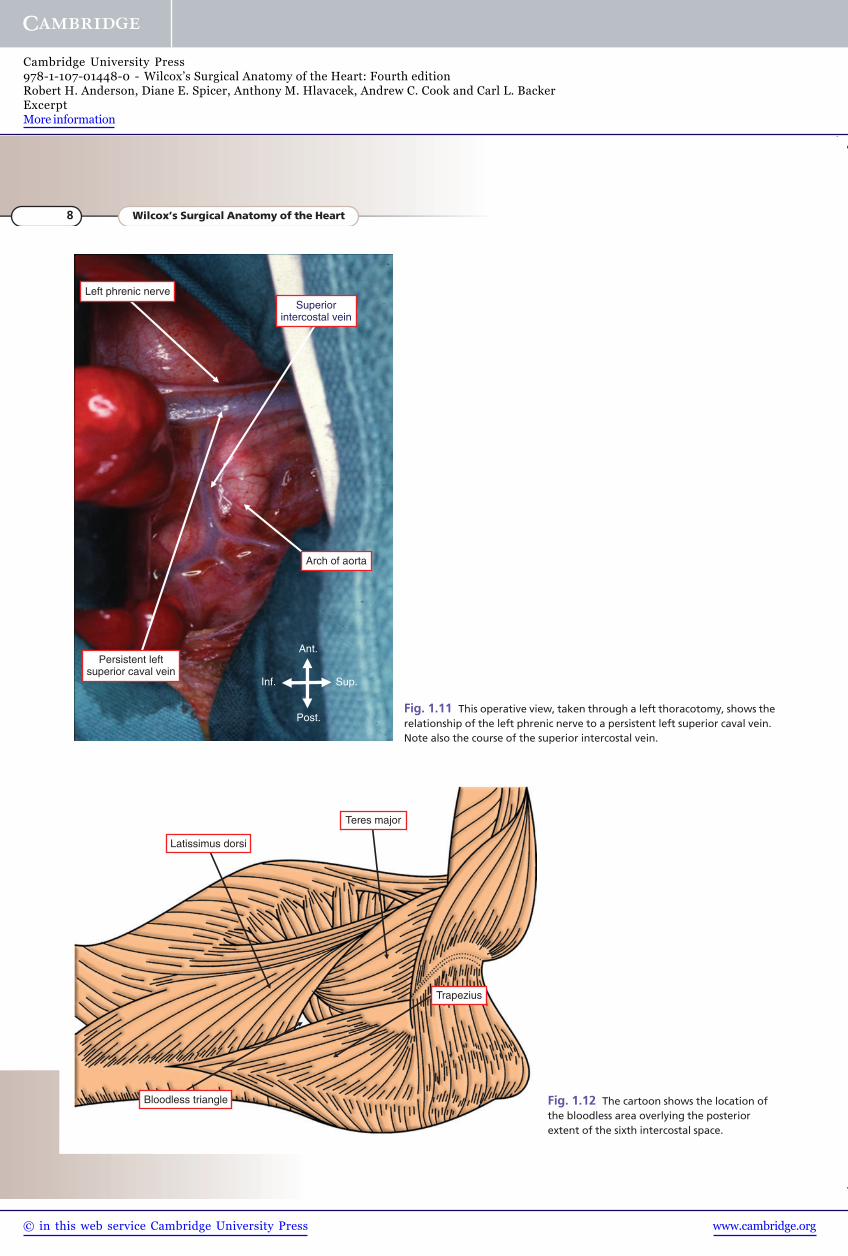
Left phrenic nerve
Arch of aorta
Superiorintercostal vein
Persistent leftsuperior caval vein
Fig. 1.11 This operative view, taken through a left thoracotomy, shows therelationship of the left phrenic nerve to a persistent left superior caval vein.Note also the course of the superior intercostal vein.
Latissimus dorsi
Teres major
Bloodless triangle
Trapezius
Fig. 1.12 The cartoon shows the location ofthe bloodless area overlying the posteriorextent of the sixth intercostal space.
8 Wilcox’s Surgical Anatomy of the Heart
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01448-0 - Wilcox’s Surgical Anatomy of the Heart: Fourth editionRobert H. Anderson, Diane E. Spicer, Anthony M. Hlavacek, Andrew C. Cook and Carl L. BackerExcerptMore information
Ant.
Post.
Inf. Sup.
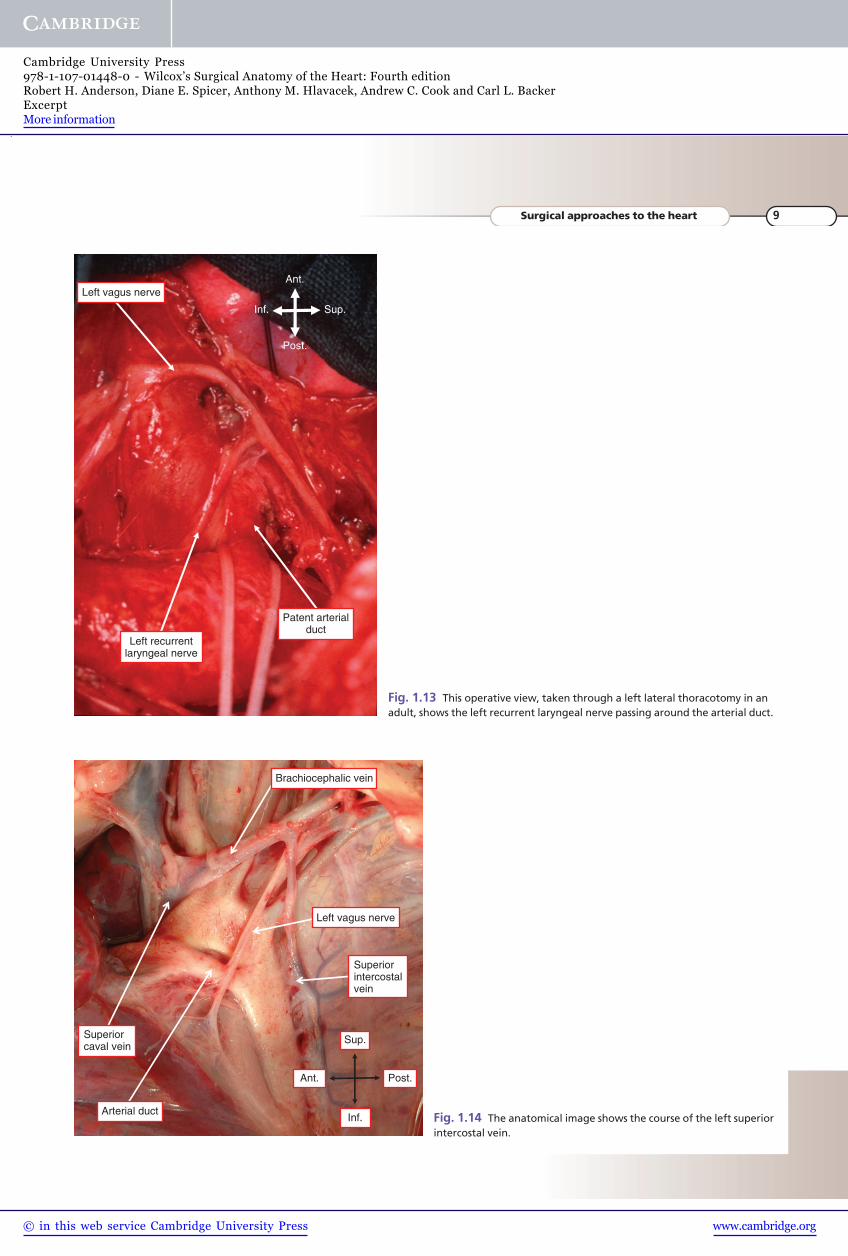
Left vagus nerve
Left recurrentlaryngeal nerve
Patent arterialduct
Fig. 1.13 This operative view, taken through a left lateral thoracotomy in anadult, shows the left recurrent laryngeal nerve passing around the arterial duct.
Brachiocephalic vein
Left vagus nerve
Arterial duct
Superiorcaval vein
Superiorintercostalvein
Sup.
Inf.
Post.Ant.
Fig. 1.14 The anatomical image shows the course of the left superiorintercostal vein.
Surgical approaches to the heart 9
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01448-0 - Wilcox’s Surgical Anatomy of the Heart: Fourth editionRobert H. Anderson, Diane E. Spicer, Anthony M. Hlavacek, Andrew C. Cook and Carl L. BackerExcerptMore information
Ant.
Post.
Inf. Sup.
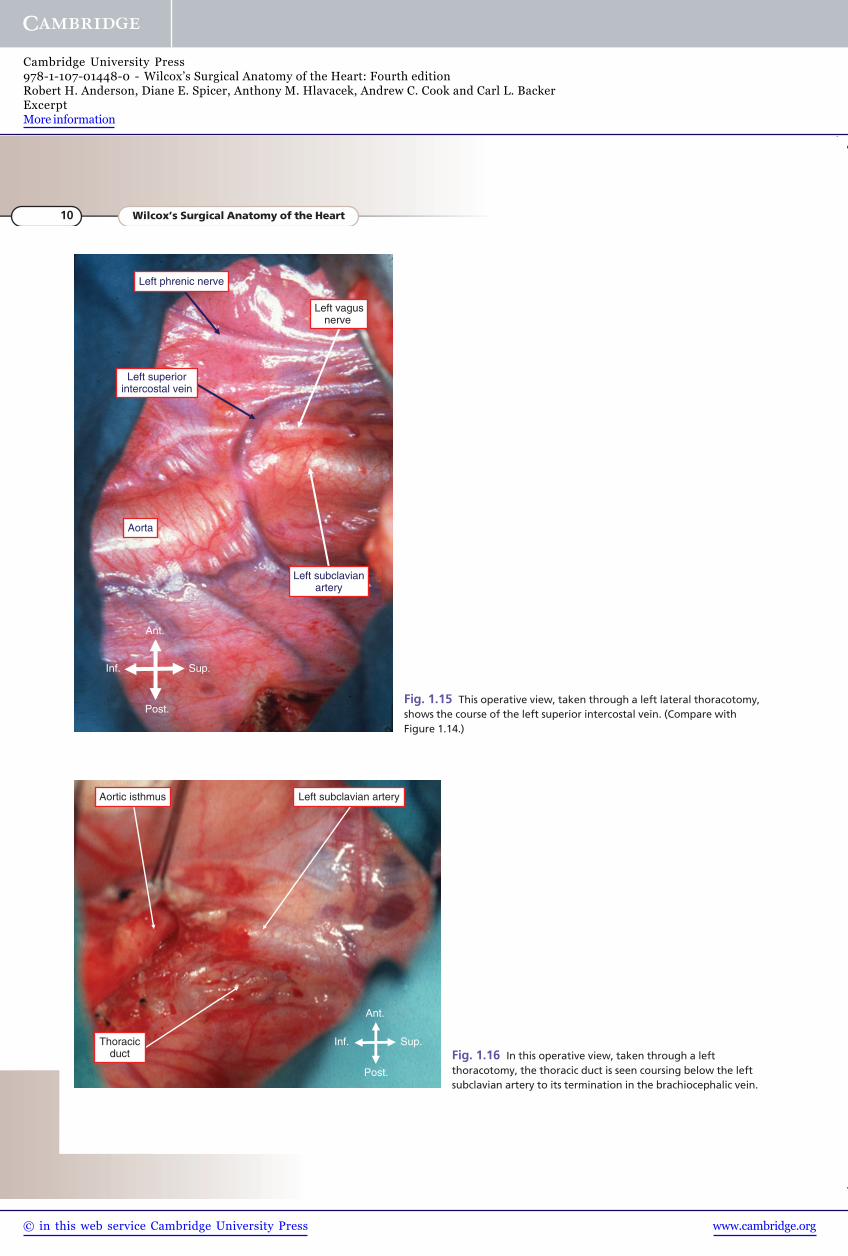
Aorta
Left phrenic nerve
Left superiorintercostal vein
Left subclavianartery
Left vagusnerve
Fig. 1.15 This operative view, taken through a left lateral thoracotomy,shows the course of the left superior intercostal vein. (Compare withFigure 1.14.)
Ant.
Post.
Inf. Sup.
Aortic isthmus Left subclavian artery
Thoracicduct Fig. 1.16 In this operative view, taken through a left
thoracotomy, the thoracic duct is seen coursing below the leftsubclavian artery to its termination in the brachiocephalic vein.
10 Wilcox’s Surgical Anatomy of the Heart
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01448-0 - Wilcox’s Surgical Anatomy of the Heart: Fourth editionRobert H. Anderson, Diane E. Spicer, Anthony M. Hlavacek, Andrew C. Cook and Carl L. BackerExcerptMore information