Embed Size (px)
Citation preview

Journal of Surgical Research 156, 177–182 (2009)doi:10.1016/j.jss.2009.03.021
Surgical Education in the Internet Era1
Carla M. Pugh, M.D., Ph.D.,* Andrew Watson, M.D.,† Richard H. Bell, Jr, M.D.,‡ Karen J. Brasel, M.D., M.P.H.,§Gretchen Purcell Jackson, M.D., Ph.D.,k Sharon M. Weber, M.D.,{ and Lillian S. Kao, M.D., M.S.#,2
*Department of Surgery, Feinberg School of Medicine, Northwestern University, Chicago, Illinois; †Department of Surgery, University ofPittsburgh, Pittsburgh, Pennsylvania; ‡The American Board of Surgery, Inc., Philadelphia, Pennsylvania; §Department of Surgery, Medical
College of Wisconsin, Milwaukee, Wisconsin; kDepartment of Surgery, Vanderbilt University Medical Center, Nashville, Tennessee;{Department of Surgery, University of Wisconsin, Madison, Wisconsin; and #Department of Surgery, University of Texas Health Science Center,
Houston, Texas
Submitted for publication February 13, 2009
Technological advancements, along with economicand political issues, have resulted in major changesin surgical education. The development of high fidelitysimulators and the widespread availability of the In-ternet have allowed learning to be shifted away fromthe operating room. Furthermore, the Internet pro-vides an opportunity for surgical educators to stan-dardize general surgery training and assessment andto develop collaborations nationally and globally.This paper highlights presentations about the chal-lenges as well as the rewards of surgical education inthe age of the Internet from the 2009 Academic Surgi-cal Congress. � 2009 Elsevier Inc. All rights reserved.
Key Words: surgical education; Internet; curriculum;technology.
INTRODUCTION
Surgical education has experienced a significantparadigm shift over the past decade. The apprentice-ship model originated by William Halstead has beensupplanted by competing models due to a rapidlychanging practice environment and advancingtechnologies [1]. Surgical education has been forced toevolve as a response to work hour restrictions [2],financial constraints [3], shifting practice patterns [4],and public scrutiny regarding patient safety issues
1 This work is a Symposium paper, highlighting presentationsfrom the Committee on Education Session of the Association for Aca-demic Surgery (AAS) and the Society of University Surgeons (SUS).
2 To whom correspondence and reprint requests should be ad-dressed at University of Texas Health Science Center at Houston,5656 Kelley Street, Suite 30S 62008, Houston, TX 77026. E-mail:[email protected].
177
[5]. Additionally, technologic advancements such aselectronic medical records [6], computerized decisionsupport [7], and simulation [8] have altered the faceof surgical practice.
The pervasiveness of the Internet holds significantimplications for surgical patients, learners, and educa-tors. According to the Nielsen ratings, in 2008 over 220million people or 72.5% of the population in the UnitedStates used the Internet [9]. The Internet has been in-corporated into surgical education at all levels, forboth instruction and evaluation. The Internet hasbeen successfully used to provide resources on anatomy[10], problem-based learning [11], clinical examination[12], procedural skills [13], comprehensive course cur-ricula [14], and real-time telementoring [15]. The omni-presence of the Internet, television, and video gameshas resulted not only in a change in the availability ofresources to learners, but also in a change in thelearners themselves. For example, modern-day stu-dents have improved visual-spatial skills, which mayhave implications in laparoscopic surgical training[16] but at the cost of weakened cognitive skills suchas critical thinking [17]. Thus, the goal for surgicaleducators is to capitalize on the widespread availabilityof the Internet and to adapt to the resultant differencesin today’s learners, but not to forget those coreexperiences and skills that must be acquired by moretraditional means.
Successful implementation of Internet-based educa-tional tools into surgical training requires formal needsassessments [18], collaborative efforts by educationaland organizational bodies [19, 20], and rigorous evalua-tion of their effectiveness. These issues were discussedat the4thAnnualAcademicSurgicalCongressby apanel
0022-4804/09 $36.00� 2009 Elsevier Inc. All rights reserved.
JOURNAL OF SURGICAL RESEARCH: VOL. 156, NO. 2, OCTOBER 2009178
convened by the education committees of the Associationfor Academic Surgery and the Society of University Sur-geons. This article highlights the important issues raisedby the panel, including examples of a current nationaland a local initiative to incorporate the Internet into res-ident training and an overview of the evolution of surgi-cal education from the past into the future.
SURGICAL EDUCATION 2009 VERSUS 1999
During the past 10 y, surgical education has beentransformed by a tandem of disruptive forces combinedwith unforeseen enabling. Paper-based medical re-cords, 56 k modems, open cholecystectomies, and expe-riential-based training have been supplanted byelectronic medical records, Fiber-Optic Service (FiOS,Verizon, New York, NY), advanced laparoscopy, andsurgical simulation centers. These changes have hada significant impact on patient care, clinic and operatingroom learning, and the availability of real-time data formedical decision-making. The end result is an unparal-leled potential to formulate a surgical education systemthat is more capable and robust than ever before.
Disruptive Forces
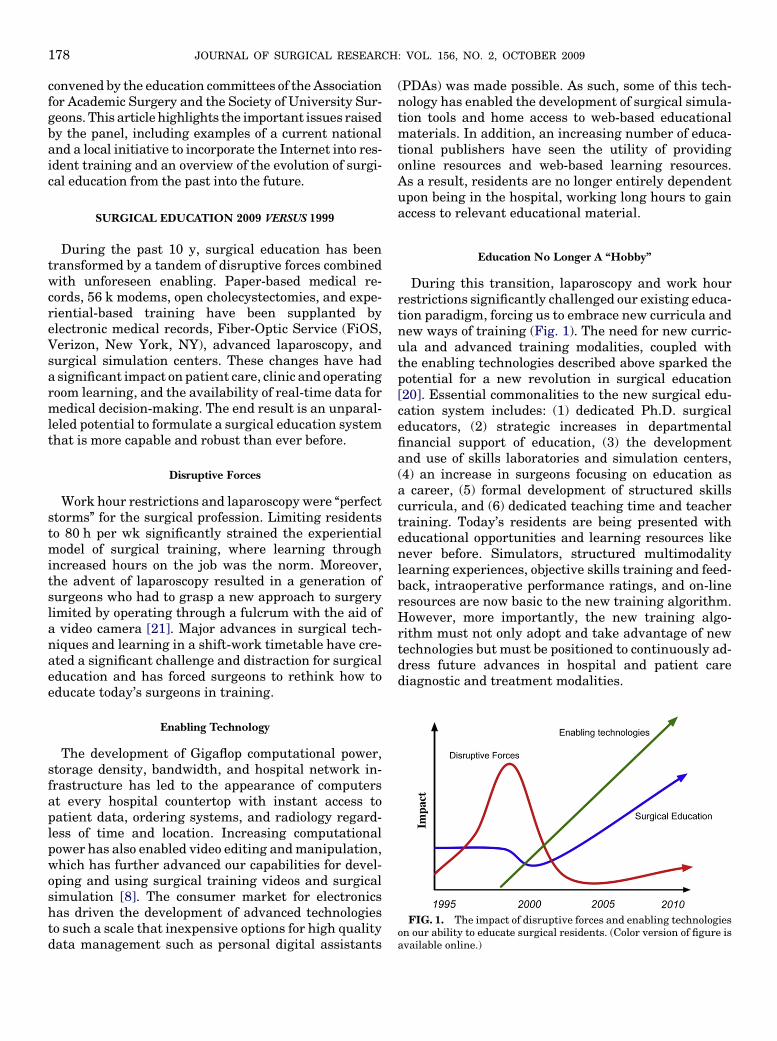
Work hour restrictions and laparoscopy were ‘‘perfectstorms’’ for the surgical profession. Limiting residentsto 80 h per wk significantly strained the experientialmodel of surgical training, where learning throughincreased hours on the job was the norm. Moreover,the advent of laparoscopy resulted in a generation ofsurgeons who had to grasp a new approach to surgerylimited by operating through a fulcrum with the aid ofa video camera [21]. Major advances in surgical tech-niques and learning in a shift-work timetable have cre-ated a significant challenge and distraction for surgicaleducation and has forced surgeons to rethink how toeducate today’s surgeons in training.
FIG. 1. The impact of disruptive forces and enabling technologieson our ability to educate surgical residents. (Color version of figure isavailable online.)
Enabling Technology
The development of Gigaflop computational power,storage density, bandwidth, and hospital network in-frastructure has led to the appearance of computersat every hospital countertop with instant access topatient data, ordering systems, and radiology regard-less of time and location. Increasing computationalpower has also enabled video editing and manipulation,which has further advanced our capabilities for devel-oping and using surgical training videos and surgicalsimulation [8]. The consumer market for electronicshas driven the development of advanced technologiesto such a scale that inexpensive options for high qualitydata management such as personal digital assistants
(PDAs) was made possible. As such, some of this tech-nology has enabled the development of surgical simula-tion tools and home access to web-based educationalmaterials. In addition, an increasing number of educa-tional publishers have seen the utility of providingonline resources and web-based learning resources.As a result, residents are no longer entirely dependentupon being in the hospital, working long hours to gainaccess to relevant educational material.
Education No Longer A ‘‘Hobby’’
During this transition, laparoscopy and work hourrestrictions significantly challenged our existing educa-tion paradigm, forcing us to embrace new curricula andnew ways of training (Fig. 1). The need for new curric-ula and advanced training modalities, coupled withthe enabling technologies described above sparked thepotential for a new revolution in surgical education[20]. Essential commonalities to the new surgical edu-cation system includes: (1) dedicated Ph.D. surgicaleducators, (2) strategic increases in departmentalfinancial support of education, (3) the developmentand use of skills laboratories and simulation centers,(4) an increase in surgeons focusing on education asa career, (5) formal development of structured skillscurricula, and (6) dedicated teaching time and teachertraining. Today’s residents are being presented witheducational opportunities and learning resources likenever before. Simulators, structured multimodalitylearning experiences, objective skills training and feed-back, intraoperative performance ratings, and on-lineresources are now basic to the new training algorithm.However, more importantly, the new training algo-rithm must not only adopt and take advantage of newtechnologies but must be positioned to continuously ad-dress future advances in hospital and patient carediagnostic and treatment modalities.

PUGH ET AL.: SURGICAL EDUCATION IN THE INTERNET ERA 179
NO SURGEON LEFT BEHIND–SCORE AND THE NATIONALSURGICAL CURRICULUM
The Surgical Council on Resident Education(SCORE) [19, 20] is a voluntary consortium of six orga-nizations with a regulatory role and/or interest in gen-eral surgery resident education: the American Board ofSurgery (ABS), the American College of Surgeons(ACS), the American Surgical Association (ASA), theAssociation of Program Directors in Surgery (APDS),the Association for Surgical Education (ASE), and theResidency Review Committee for Surgery (RRC).
The mission of SCORE is to develop a competency-based curriculum for general surgery training. A compe-tency-based curriculum starts with agreement on whatskills, knowledge, and attitudes residents should possessby the time they complete training [22]. In contrast, gen-eral surgery residency has traditionally had primarilya time-based curriculum based on an innate assumptionthat 5 years of association with skilled faculty surgeons issufficient to develop the skills to practice effectively.However, today’s residents see an ever increasing rangeof diseases and conditions, and the surgical profession isfaced with a continuous increase in new technologies andprocedures, making an ill-defined time-based system nolonger applicable to our educational needs.
In defining the competencies expected of a graduateof a general surgery training program, SCORE used asits starting point the six general competencies promul-gated by the Accreditation Council for Graduate Med-ical Education (ACGME): patient care, medicalknowledge, professionalism, communication, practice-based learning, and systems-based practice. To thislist, SCORE added a seventh general competency:technical skill, which, although it is part of patientcare, is so important in surgery as to warrant separaterecognition.
To define the specific patient care competenciesexpected of a graduating general surgery resident,SCORE built on work begun by the General Surgery Res-idency Committee of the ABS and ultimately achievedbroad consensus in the surgical communityabout the dis-eases and the operations that should be included in a res-idency experience. Once these were identified, it wasnecessary to then determine the level of knowledge orskill required; the group recommended that diseases bedivided into two groups, broad and focused, and thatoperations be separated into two categories, essentialand complex. The list of diseases and operations and anexplanation of the methodology, published as the SCOREPatient Care Curriculum Outline, can be found on theABS website, www.absurgery.org.
SCORE is developing a national website available toall residents and faculty, through which educational ma-terials will be delivered that support the teaching and
learning of the patient care topics. The website is orga-nized by disease and operation within an organ system,and for each disease and operation will provide perfor-mance objectives, educational materials and self-assess-ment questions. The website was released in b version inFebruary 2009.
SCORE has made gratifying progress towards defin-ing a curriculum for general surgery residency, butthere are additional domains of competency to address.In medical knowledge, the ABS has focused on the med-ical knowledge competency for a number of years andits resources will be very helpful. For technical skill,the ACS and APDS have jointly developed a skills cur-riculum covering basic skills, specific operations, andteam skills. SCORE will also need to define specificexpected competencies in the areas of professionalism,communication, practice-based learning, and systems-based practice. Collaboration amongst surgical trainingprograms, residents, SCORE and other stakeholders insurgical education will be essential in developing thecurriculum and keeping it relevant and applicable tothe ever changing surgical profession.
WEB-BASED CURRICULA: ONE PROGRAM’S EXPERIENCE
The most important aspect in using a web-based cur-riculum is to view it as an educational resource and toolmeant to enhance teaching and learning. It is not a sub-stitute for a thoughtful educational program, nor is ita substitute for excellent teaching and mentoring.With these principles in mind, the Medical College ofWisconsin’s Department of Surgery developed a ‘pro-tected block’ curriculum for the post-graduate year(PGY) 1 and 2 residents that involves 3 to 4 d of interac-tive learning with homework assignments. During thisprotected block, residents are relieved from all clinicalduties [23]. After a year of curricular planning, thePGY1 curriculum was instituted in 2005–2006, fol-lowed by the PGY2 curriculum in 2006–2007. The fol-lowing year, in addition to institution of a PGY3-5curriculum, the ANGEL learning management systemwas used to incorporate web-based resources into thePGY2 curriculum. This technological effort, done onlyafter the format and content of the protected blockswas initially set, was led by one of our associate pro-gram directors, Dr. Travis Webb.
The curricula are available to all residents and fac-ulty who sign on to the learning management system.Each curricular module contains resources—links totexts, journal articles, videos—that are reference mate-rial or homework. Other websites and resources mayalso be accessed from within the module. The overallschedule as well as the schedule for each protectedblock is easily accessed, as are the evaluations for

JOURNAL OF SURGICAL RESEARCH: VOL. 156, NO. 2, OCTOBER 2009180
each session within the block. Modules may also con-tain quiz material that can be completed on-line.
Another feature of each curricular module is the dis-cussion board, on which residents and faculty can postitems arising from discussion during the block. The dis-cussion board feature is also used by two of the servicesindependent of the curriculum; all residents on thetrauma and critical care services are required to postat least once during their rotation. This feature has sig-nificant advantages, but some fairly obvious pitfalls. Itallows the residents a moderated forum in which theybegin to use available resources to answer questionsbrought up during the course of patient care. For opti-mal educational benefit, it requires a moderator—usu-ally the clinical faculty responsible for the service. Wehave not found faculty involvement in the discussionboard to be an educational time-saver as it requiresadditional time and effort to respond to these postings.As such, it is rare that there is an on-going dialogue es-tablished. Moreover, unlike a real-time discussion, it isnot always clear whether the additional response time isof value. On the contrary, the library of postings areclearly viewed by many of the residents, as it is commonto hear ‘‘there is a nice summary of that on ANGEL’’from residents on service.
Resident use of the web-based learning system (i.e.,accessing articles or old discussion posts) may betracked by the identified administrator of a discussiongroup or course. While we have not incorporateda detailed assessment of resident use into our residents’evaluation, we do note whether or not they participatedin discussion posts during their time on trauma/criticalcare. For the journal club discussion leaders, it is valu-able to know how many of the residents have read thearticles as it helps to facilitate the discussion. Whiletracking resident use of journal articles has been use-ful, ultimately resident journal club is still better appre-ciated face-to-face than in a completely web-basedformat. In the future, as part of our curriculum evalua-tion, the participant tracking function could be used tofacilitate evaluation of the discussion boards and web-based journal clubs as educational tools.
Over the past 4 y, we have found that the more we usethe web-based learning tool the more we like it, hence,the more we use it. It is now used for all communicationfrom the Program Director’s office, for all residentscheduling, and for much of the PGY3-5 curriculum.There are educational resources for residents of alllevels, but the additional potential realized in the dis-cussion boards makes this a living tool. During our firstyears of use, the discussion boards in particularrequired significant faculty effort, and while it stillhas a few major faculty champions, it is easy enoughto use that even the most technologically challengedfaculty can navigate and post with little instruction.
In the end, web-based instruction remains an educa-tional tool that we must learn to harness for maximalteacher and learner benefit.
SURGICAL EDUCATION 2009 VERSUS 2019
The future of surgical education can be informed byprior efforts to understand the fate of academic medi-cine. In 2003, the British Medical Journal and Lancetlaunched an international campaign to reinvent andrevitalize academic medicine [24]. Over 40 journals,medical societies, and funding organizations partici-pated in and supported this effort. As part of the cam-paign, a scenario planning exercise was done foracademic medicine. Scenario planning is a techniquepioneered by the Shell Corporation in the 1970s thathas been used by companies and non-profit groups toimagine and plan for possible futures. The UnitedNations used scenario planning to think about the evo-lution of the acquired immune deficiency syndrome(AIDS) epidemic in Africa. The technique involves ananalysis of present trends, instabilities, and possibledrivers of the future. Participants considered not onlyobvious emerging trends, such as restricted work hoursfor medical trainees, but also unexpected events thatcould radically change the world, such as new diseasesor alternative energy sources that redistributed globalwealth. The aim was not to predict the future but,instead, to broaden thinking about what might be pos-sible and use that information for short-term decisionmaking and long-term planning.
Future Scenarios
Based on these discussions, five possible futures for ac-ademic medicine in 2025 were generated [25]. In the ‘‘Ac-ademic, Inc.’’ scenario, medicine moved completely intothe private sector. Highly competitive institutionsemerged, and academic salaries were higher to recruitthe best and brightest teachers and researchers. How-ever, education and practice were driven by marketforces and, thus, global inequities worsened. Academicmedicine was completely abolished in a second ‘‘Reforma-tion’’ scenario due to frustrations about elite academic in-stitutions as well as research and training that wereirrelevant to the real problems of global health. Medicaleducation and research moved to the mainstream of clin-ical care. Students first learned how to learn, and thenthey learned on the job. Training was shortened and spe-cialized, but innovation was uncommon and slow. In the‘‘Public Eye’’ scenario, academic medicine was trans-formed by a global celebrity culture. Medical practiceand education were conducted under intense media scru-tiny. Successful teachers and academicians receivedgreater recognition for their efforts, and many became

PUGH ET AL.: SURGICAL EDUCATION IN THE INTERNET ERA 181
as famous as actors or musicians. Shows such as ‘‘Amer-ica’s Next Tenured Professor’’ and ‘‘Top Surgeon’’ toppedthe Nielsen television ratings. Funding priorities for ed-ucational and research agendas were driven by popularappeal. In the ‘‘Global Academic Partnership’’ scenario,academic medicine deemed global inequities, especiallyin health, intolerable, based on a greater appreciationthat violence and terrorism were fueled by large gaps be-tweentherichandthepoor.Policymakerscametoappre-ciate that investments in health produced remarkablereturns on economic and social development and, thus,regulated that funding priorities and promotions bedriven by global health interests. The tensions and dis-connects between public priorities and research,research and practice, practice and policy drove a com-mitment of academic institutions to engage stakeholdersin earnest in the final ‘‘Fully Engaged’’ scenario. Mutualunderstanding and acceptance were sometimes difficultwith the involvement of diverse groups, and at times,medicine became dumbed down with compromise to orig-inality and independent thinking.
Projection
The future of academic medicine is unlikely to evolveexactly as described by any of these scenarios, but com-ponents of each have been, and likely will continue tobe, realized. Several themes were common to all scenar-ios. Whether business, media, policy, or principledriven, global thinking was important in all imaginedfutures. Competition among institutions is likely toincrease in the next 10 y, and it will most certainly beinternational given the general trends toward global-ization. In all scenarios, stakeholders, such as ourpatients and payers, played greater roles in activitiesof academic medicine, from direct teaching and re-search functions to agenda setting and policy making.Cutting edge technologies were seen in each of thefutures. There was an increased emphasis on transla-tional research in many scenarios, as the gaps betweenknowledge and practice, or research and practice,became intolerable. Successful academic medical insti-tutions required broader thinking and new skill setswith collaborations from the fields such as law, commu-nications, and economics. Planning for the futurebecame increasingly challenging, but essential, forany academic institution.
The Implications for Surgical Training
These themes have several implications for medicaltraining in the next decade. First, surgical educationwill likely be conducted on an international stage andwill be disseminated across institutions. In pediatricsurgery, we all learn about repair of the broad spectrum
of imperforate anus abnormalities from the world’s ex-pert, Dr. Alberto Pena, and why should not other spe-cialty topics be taught to surgeons by anyone otherthan the world’s leading experts? Next generation sur-gical educators must think about preparing to teach inmultiple languages and having materials appropriateto diverse cultures. The academic surgeon shouldexpect that the teaching requirements for promotionwill require involvement outside of one’s current insti-tution. Futuristic resources, such as WikiSurgery,a free, collaborative, peer reviewed encyclopedia of sur-gery—with greater detail than most atlases and elabo-rate patient resources—is already available online withover 1000 articles provided by an international group ofvolunteers [26].
Second, surgical training is long, and as our specialtymakes progress toward defining competency, ourspecialty might and should move toward incrementalcredentialing. If surgical trainees can demonstrate com-petency in basic procedures, be incrementally creden-tialed to perform procedures, be ultimately responsiblefor patients, and bill for their services—in the middleof the night when surgeons often lose potential reve-nue—the specialty of surgery could solve a lot of theproblems of low trainee salaries, the lack of patient own-ership created by the 80 h work week, and patient aswell as consulting-service satisfaction.
Third, it goes without saying that next generationsurgical educators will be required to use state of theart technologies. Surgical faculty should familiarizethemselves with the latest innovations in communica-tion, simulation, robotics, and telepresence. With re-duced work hours, much of surgical training andfuture patient follow-up may not be done with actualpeople, but instead with simulations and telepresence,respectively. It was just recently reported that a Chris-tian mission worker, David Nott, saved a teenage boy inthe Democratic Republic of Congo after receiving oper-ative instruction on upper extremity forequarter ampu-tation via text messaging from Professor Thomas [27].The information age is here. Simulations will be partof all training environments and evaluation of our com-petency in 2019. It is certain that in 5 or 10 y, educationwill incorporate technologies not yet envisioned today.
Stakeholders—people invested in surgical educationsuch as customers, patients, or payers—will havemore of a say than they currently do about how sur-geons are trained and how competency and qualityare assessed. In the surgical educator role, one mayfind that one must not only address trainees, but alsoeducate patients, families, payers, and referral groups,to an even greater extent in the next decade. Finally,the efforts of both educators and researchers alikemust be collaborative to provide the best education forall surgeons. Current and future technologies will allow
JOURNAL OF SURGICAL RESEARCH: VOL. 156, NO. 2, OCTOBER 2009182
that. Institutions will only be strengthened in reputa-tion and likely funding when engaged in strong part-nerships with other institutions.
CONCLUSIONS
The widespread availability and powerful capabil-ities of the Internet have resulted in rapid incorpora-tion of web-based educational tools into surgicaltraining and practice. Along with other evolving tech-nologies, the Internet holds significant promise foraddressing the current challenges in surgical educationcreated by time constraints and patient safetyconcerns. Furthermore, the Internet removes geo-graphical boundaries, allowing for global sharing ofknowledge, research collaboration, and telementoring.
Surgical educators must be proactive in embracingthe Internet and other evolving technologies. Localefforts have demonstrated the feasibility and utility ofweb-based educational tools for disseminating informa-tion and assessing performance. However, further effi-cient and effective use of the Internet should bepromoted; national and global collaboratives may poolresources, reduce redundancies, and standardize gen-eral surgical training. Further studies are required tovalidate web-based tools and to determine how to opti-mally incorporate them into surgical curricula.
REFERENCES
1. Franzese CB, Stringer SP. The evolution of surgical training:Perspectives on educational models from the past to the future.Otolaryngol Clin North Am 2007;40:1227.
2. Darosa DA, Bell RH, Jr., Dunnington GL. Residency programmodels, implications, and evaluation: Results of a think tankconsortium on resident work hours. Surgery 2003;133:13.
3. Bridges M, Diamond DL. The financial impact of teaching surgi-cal residents in the operating room. Am J Surg 1999;177:28.
4. Dunning K, Liedtke E, Toedter L, Rohatgi C. Outpatient surgerycenters draw cases away from hospitals, impact resident train-ing volume. J Surg Educ 2008;65:460.
5. Barone JE, Tucker JB, Bull SM. The Leapfrog Initiative: Apotential threat to surgical education. Curr Surg 2003;60:218.
6. Chaudhry B, Wang J, Wu S, et al. Systematic review: Impact ofhealth information technology on quality, efficiency, and costs ofmedical care. Ann Int Med 2006;144:742.
7. Moore FA. Evidence-based medical information technology: Thenext generation. J Trauma 2007;63:1195.
8. Scott DJ, Cendan JC, Pugh CM, Minter RM, Dunnington GL,Kozar RA. The changing face of surgical education: Simulationas the new paradigm. J Surg Res 2008;147:189.
9. Internet World Stats. (Accessed Feb 10, 2009, at http://www.Internetworldstats.com/stats14.htm.)
10. Choi AR, Tamblyn R, Stringer MD. Electronic resources for sur-gical anatomy. ANZ J Surg 2008;78:1082.
11. Corrigan M, Reardon M, Shields C, Redmond H. ‘‘SURGENT’’ –student e-learning for reality: The application of interactivevisual images to problem-based learning in undergraduate sur-gery. J Surg Educ 2008;65:120.
12. Criley JM, Keiner J, Boker JR, et al. Innovative web-based mul-timedia curriculum improves cardiac examination competencyof residents. J Hospital Med (Online) 2008;3:124.
13. Chenkin J, Lee S, Huynh T, Bandiera G. Procedures can belearned on the Web: A randomized study of ultrasound-guidedvascular access training. Acad Emerg Med 2008;15:949.
14. Kalet AL, Coady SH, Hopkins MA, et al. Preliminary evaluationof the Web Initiative for Surgical Education (WISE-MD). Am JSurg 2007;194:89.
15. Shimizu S, Nakashima N, Okamura K, et al. Telesurgery systemwith original-quality moving images over high-speed Internet:Expansion within the Asia-Pacific region. J Laparoendosc AdvSurg Tech 2007;17:673.
16. Rosser JC, Jr., Lynch PJ, Cuddihy L, et al. The impact of videogames on training surgeons in the 21st century. Arch Surg2007;142:181. discussion 6.
17. Greenfield PM. Technology and informal education: What istaught, what is learned. Science (NY) 2009;323:69.
18. Pugh CM, DaRosa DA, Glenn D, et al. A comparison of facultyand resident perception of resident learning needs in the operat-ing room. J Surg Educ 2007;64:250.
19. Bell RH. Surgical council on resident education: A new organiza-tion devoted to graduate surgical education. J Am Coll Surg2007;204:341.
20. Sachdeva AK, Bell RH, Jr., Britt LD, et al. National efforts toreform residency education in surgery. Acad Med 2007;82:1200.
21. Kumar U, Gill IS. Learning curve in human laparoscopic sur-gery. Curr Urol Rep 2006;7:120.
22. Prideaux D. ABC of learning and teaching in medicine. Curricu-lum design. BMJ Clinical research ed 2003;326:268.
23. Weigelt JA, Simpson DE, Anderson RC, et al. A PGY1 curricu-lum–meeting a need for changing times. Curr Surg 2006;63:410.
24. Clark J, Smith R. BMJ Publishing Group to launch an interna-tional campaign to promote academic medicine. BMJ 2003;327:1001.
25. Awasthi S, Beardmore J, Clark J, et al. Five futures for academicmedicine. PLoS medicine 2005;2. e207.
26. Wikisurgery—the free surgical encyclopedia. Accessed February9, 2009, at http://www.wikisurgery.com.
27. Nott D. A chance of life. BMJ 2008;337:a2958.