Embed Size (px)
Citation preview

Research Article
Survival of patients with hepatocellular carcinoma treated bytransarterial chemoembolisation (TACE) using Drug Eluting Beads.
Implications for clinical practice and trial design
Marta Burrel1,�, María Reig2,3,�, Alejandro Forner2,3, Marta Barrufet1, Carlos Rodríguez de Lope2,Silvia Tremosini2, Carmen Ayuso1,3, Josep M Llovet2,3,4,5, María Isabel Real1, Jordi Bruix2,3,⇑
1Radiology Department, Barcelona Clinic Liver Cancer (BCLC) Group, Hospital Clinic Barcelona, IDIBAPS, University of Barcelona, Spain; 2LiverUnit, Barcelona Clinic Liver Cancer (BCLC) Group, Hospital Clinic Barcelona, IDIBAPS, University of Barcelona, Spain; 3Centro de InvestigaciónBiomédica en Red de Enfermedades Hepáticas y Digestivas (CIBERehd), Spain; 4Mount Sinai Liver Cancer Program, Division of Liver Diseases,
Mount Sinai School of Medicine, New York, NY 10029, USA; 5Institució Catalana de Recerca i Estudis Avançats, Barcelona, Catalonia, Spain
Background & Aims: Transarterial chemoembolisation (TACE) � 2012 European Association for the Study of the Liver. Published
improves survival of properly selected patients with hepatocellu-lar carcinoma (HCC). Drug eluting beads (DEB) provide a cali-brated and homogenous procedure while increasing efficacy.Outcome data applying this technology is lacking, and this isinstrumental for clinical decision-making and for trial design.We evaluated the survival of HCC patients treated with DEB-TACE following a strict selection (preserved liver function,absence of symptoms, extrahepatic spread or vascular invasion).Methods: We registered baseline characteristics, the develop-ment of treatment-related adverse events, and the overall sur-vival of all HCC patients treated by DEB-TACE from February2004 to June 2010.Results: One hundred and four patients were treated with DEB-TACE. All but one were cirrhotic, 62.5% HCV+, 95% Child-PughA, 41 BCLC-A and 63 BCLC-B. Causes of DEB-TACE treatment inBCLC-A patients were: 35 unfeasible ablation, and six post-treat-ment recurrences. After a median follow-up of 24.5 months, 38patients had died, two patients had received transplantationand 24 had received sorafenib because of untreatable tumourprogression. Median survival of the cohort was 48.6 months(95% CI: 36.9–61.2), while it was 54.2 months in BCLC stage Aand 47.7 months in stage B. Median survival after censoring fol-low-up at time of transplant/sorafenib was 47.7 (95% CI: 37.9–57.5) months.Conclusions: These data validate the safety of DEB-TACE andshow that the survival expectancy applying current selection crite-ria and technique is better than that previously reported. A 50%survival at 4 years should be considered when suggesting treat-ment for patients fitting into controversial scenarios such asexpanded criteria for transplantation/resection for multifocal HCC.
Journal of Hepatology 20
Keywords: Hepatocellular carcinoma; Chemoembolization; Drug eluting beads(DEB); Safety; Survival.Received 5 October 2011; received in revised form 5 December 2011; accepted 9January 2012; available online 5 February 2012⇑Corresponding author. Address: BCLC group, Liver Unit, Hospital Clínic,C/Villarroel 170, 08036 Barcelona, Spain.E-mail address: [email protected] (J. Bruix).
�These authors contributed equally to this work.
by Elsevier B.V. All rights reserved.
Introduction
Transarterial chemoembolisation (TACE) is an established treat-ment for patients diagnosed with hepatocellular carcinoma(HCC) [1]. Optimal candidates for it are asymptomatic patientswith compensated liver disease without extrahepatic spread orvascular invasion. This defines the BCLC-B stage, but TACE is alsoapplied to patients at an earlier stage (BCLC-A) who are not con-sidered for surgery or ablation. This clinical situation is knownas ‘‘treatment stage migration’’ and indicates that each BCLCstage has each first line option. However, according to the indi-vidual patient’s profiling, the treatment selection is tailored foreach patient. Until recently, TACE has been performed using lipi-odol intra-arterial chemotherapy followed by embolisation withGelfoam particles (‘conventional TACE’). This was the techniqueused in most TACE trials that established this treatment as stan-dard. The limitations of the technique are well known. Gelfoamwas prepared manually, arterial obstruction could be heteroge-neous and it lasted less than 72 h. In addition, the time betweenchemotherapy injection and vessel obstruction allowed chemo-therapy to be released to the systemic circulation and inducedtoxicity that impaired the tolerance of the patients. The develop-ment of Drug-Eluting Beads (DEB) represents a major advance-ment. DEB are formed by non-resorbable hydrogel and areloaded with the chemotherapy drug (doxorubicin). This is slowlyreleased upon injection into the blood stream and systemic pas-sage is significantly reduced despite injection of higher doses ofchemotherapy. As a consequence, the treatment efficacy andtolerance are improved [2–5] as compared to conventional TACE[6,7].
The refinement in treatment application has overlapped intime with the improvement of the criteria to select candidates[8]. Most groups do not treat patients with decompensated liverdisease and it is acknowledged that the presence of vascular inva-sion (even segmental) impairs tolerance and outcome [9,10]. As aconsequence, the survival data (median survival below 2 years)
12 vol. 56 j 1330–1335

JOURNAL OF HEPATOLOGY
reported one decade ago are no longer valid [6,7,11]. Thisprompted the current retrospective study that reports thesurvival of HCC patients treated with DEB-TACE in our group.Patients and methods
Patient evaluation
The study population consisted of those patients treated with DEB-TACE at ourinstitution between February 2004 and June 2010, and was followed-up untilJune 2011. After our phase II trial by Varela et al. [2] showing the safety and che-motherapy pharmacokinetics of DEB-TACE, we had to wait for confirmatory stud-ies to have the new material reimbursed for clinical practice. Because of this need,the cohort includes the 22 patients recruited in the Varela et al. study who did notreceive TACE with Gelfoam during follow-up and 82 additional patients that weretreated upon getting the allowance to use DEB. Patients treated by conventionalTACE were excluded.
The inclusion criteria for DEB-TACE were: (1) HCC diagnosed by pathology orby non-invasive criteria according to AASLD guidelines [1,12], (2) patients withearly stage HCC [13] that were not candidates for resection, transplantation, abla-tion or had failed/recurred after resection/ablation or (3) intermediate HCCpatients following the BCLC staging system, (4) normal liver or compensated cir-rhosis with preserved liver function (Child-Pugh score 67 points) [14], (5) perfor-mance status 0 [15], (6) adequate clotting profile (platelet count P60 � 109/L,haemoglobin >8.5 g/dl, and prothrombin time >50%), (7) adequate hepatic func-tion (albumin >2.8 g/dl, bilirubin <3 mg/dl and alanine and aspartate aminotrans-ferase <5 times the upper limit of the normal range), (8) adequate renal function(serum creatinine <1.5 times the upper limit of the normal range).
Exclusion criteria were: (1) portal vein thrombosis (even segmental) or hepato-fugal blood flow, (2) impaired hepatic function, (3) contraindication for arterialendovascular procedure, (4) contraindication for the administration of doxorubicin.
Treatment
All patients received at least one session of DEB-TACE (DC Beads�, Biocompati-bles, UK Ltd.). All tumour sites were treated in a single session even if theyaffected both lobes. Treatment efficacy was assessed at one month. If completeresponse or tumour necrosis was >90% (defined by the absence of contrast uptakein the arterial phase at dynamic imaging) retreatment was considered every6 months. Because of the non-inclusion in a prospective study, some patientshave had their follow-up imaging done in their referring centre.
DEB-TACE sessions were repeated until occurrence of symptomatic progres-sion, extrahepatic spread or vascular invasion, development of liver failure orappearance of severe adverse events [16] . Hence, tumour progression was nottaken as treatment failure and DEB-TACE was repeated if contraindications hadnot appeared. When progression was not treatable by DEB-TACE [16], the patientswere evaluated for second line options that, upon sorafenib proof of efficacy, havehad this agent as the first choice.
No antibiotic prophylaxis [17,18] or anti-inflammatory drugs were adminis-tered prior to treatment. Pain during the procedure was managed individually.Pain and fever attributed to postembolisation syndrome were controlledindividually.
Angiographic technique
The procedure was conducted using the equipment Axiom Artis (Siemens, Ger-many). Diagnostic visceral angiography of the celiac trunk and superior mesen-teric artery was first performed to determine the arterial supply to the liver,the variant arterial anatomy, and the patency of the portal vein. The gastroduode-nal, cystic, and gastric arteries were carefully noted to avoid the backward flow ofchemoembolisation material to these arteries. Selective angiography of the com-mon hepatic artery was then carried out to evaluate tumoural vessels. The mul-tiplanar and maximum intensity projection reconstructions of the 1-mm imagesobtained from the multiphasic CT scan added some information on the tumouralfeeders.
The end point of treatment was to achieve complete tumour devascularisa-tion. Chemoembolisation of all tumoural vessels was performed as distally as pos-sible in one single session. Therefore, we first intended to treat from the tumourfeeder, and if this was not feasible or not enough to ensure complete treatment,we continued from subsegmental or segmental arteries. Patients with unifocal
Journal of Hepatology 2012
lesions were treated selectively from the tumour feeders. Patients with multiplelesions were treated with embolisation from multiple segmental and/or subseg-mental arteries. For this purpose, we always used a coaxial microcatheter 2.7F(Progreat, Terumo Europe, Leuven) and in specific cases a coaxial 2.4F microcath-eter (Excelsior, Boston Scientific, Boston, Massachussets). For cases where supra-selective catheterisation was difficult, a 0.01400 microguidewire (Syncro; BostonScientific, Boston, Massachussets) was used. DEB were loaded at the hospitalpharmacy 12 h before use. Loaded beads were mixed with iodinate contrast ina proportion 1:1 (5 ml of DC Beads in 5 ml of contrast), 5–10 min before injection.During the administration, we added contrast or saline depending on the concen-tration of beads and fluid density. We used 3-ml injection syringes. Beads wereadministered under continuous fluoroscopic monitoring until stagnation of flowwas achieved. Maximum dose administered was 150 mg of doxorubicin (twovials); dose was not tailored according to body surface or weight. The size ofbeads used in the Varela et al. study was 500–700 microns [2] in order to assesssafety and minimise the risk of biliary damage by using smaller beads. Uponestablishing safety when using smaller beads by other authors, we used 300–500 microns in the remaining patients. These are preferred as the potentialmicrocatheter clogging is almost completely avoided. If stagnation of flow wasnot achieved after the injection of two DEB vials, we continued injecting non-loaded spherical particles of 300–500 microns (BeadBlock). A final angiographyto confirm complete tumour devascularisation was performed in all cases.
Clinical and radiological follow-up
Baseline clinical examination, and laboratory and tumour evaluation were per-formed in all patients. Follow-up included clinical examination, laboratory data,tumour evaluation, and registration of serious adverse events following version 3.0Terminology Criteria for Adverse Events (CTCAE), which determines hospitalisation.
The usual policy in patients at the BCLC is to perform follow-up imaging witha multiphasic study (non-enhanced, arterial, portal and late venous phases) usingeither an helical CT or a 64-row multidetector CT scanner with 120 ml of non-ionic contrast agent at a rate of 4 ml/s. Images are reconstructed at 4-mm thick-ness in axial and coronal planes. This protocol is recommended when patients arenot followed at the BCLC, but because of the non-prospective collection of thedata with adequate monitoring, it is not possible to ensure that timing and tech-nology are homogeneous in the whole cohort. Accordingly, assessment ofresponse rate and time to progression has not been evaluated and we onlyfocused on survival. This is a robust end point in terms of validation and registra-tion in any time-to-event analysis.
Same limitation applies to untreatable progression that is defined as develop-ment of HCC progression not amenable for DEB-TACE because of limiting technicalissues, significant disseminated intrahepatic disease, vascular invasion or extrahe-patic spread, clinical intolerance to TACE and/or development of liver failure [16].
Statistical analysis
Quantitative variables were expressed as median and range and categorically ascount and proportions. Patients were classified according to BCLC staging. Differ-ences between subgroups were evaluated by the Chi-squared test or Fisher’s exacttest for categorical variables and by Student t test or non-parametric U-Mann–Whitney test for quantitative variables. Prognostic power of clinical and biochem-ical profile was assessed by dividing parameters according to the median of eachparameters. Univariate analysis was performed on each clinical and biochemistryvariable to examine their influence on patient’s survival. Survival rates and curveswere determined using the Kaplan–Meier method, and compared using the log ranktest. A conventional p value less than 0.05 was considered significant. Last date fordata collection was June 23, 2011. Analysis was done without any censoring andalso censoring survival at the time of liver transplantation or sorafenib treatment.This would rule out the impact of these treatments on the observed survival.
All calculations were done with SPSS package version 18 (SPSS Inc., Chicago,IL).
Results
Baseline characteristics of patients
Between February 2004 and June 2010, 274 patients receivedtreatment with TACE. A total of 104 patients met the inclusioncriteria and are the subject of this study. The excluded patientshad received at least one conventional TACE. The baseline charac-
vol. 56 j 1330–1335 1331

Table 1. Baseline clinical characteristics of patients.
Total cohort (n = 104)
BCLC-A (n = 41)
BCLC-B(n = 63)
p
Age (yr), median 68.2 [34-81] 68.2 [42-81] 66.1 [34-81] n.s. Gender (M/F), n 91/13 34/7 57/6 n.s.HCV/ethanol/HVB/others, n 64/26/7/7 25/11/4/1 39/15/3/6 n.s. Child-Pugh A/B, n (%) 99/4* 40/1 59/3* n.s. BCLC stage, A/B, n 41/63 41/0 0/63 n.a.Performance status, 0/1, n 104/0 41/0 63/0 n.s.ASAT, median (IU/L) 71 [11-409] 79.5 [19-409] 54 [11-366] n.s. ALAT, median (IU/L) 64 [13-451] 69 [21-440] 63 [13-451] n.s. AP, median (IU/L) 227 [67-858] 236 [67-447] 218 [107-858] n.s. GGT, median (IU/L) 100 [23-783] 80 [25-783] 109 [23-509] n.s. PT, median (%) 84 [55-100] 83 [55-100] 88 [57-100] 0.02Bilirubin, median (mg/dl) 0.95 [0.1-2.8] 1.1 [0.1-2.8] 0.85 [0.4-2.4] n.s.Albumin, median (g/dl) 41 [29-64] 40 [31-47] 42 [29-64] n.s. Creatinine, median (g/dl) 0.9 [0.6-1.6] 0.9 [0.6-1.4] 0.9 [0.7-1.6] n.s. AFP, median (IU/ml) 16 [1-78,847] 12 [2-2422] 19.5 [1-78,847] n.s. Hto, median (%/dl) 42 [32-98] 42 [32-51] 43.5 [33-98] n.s. Platelets, median (x 109/L) 130 [39-239] 122 [39-239] 144.5 [46-182] n.s.
HCV, hepatitis C virus; HBV, hepatitis B virus; BCLC, Barcelona Clinic Liver Cancer; ASAT, aspartate aminotransferase; ALAT, alanine aminotransferase; GGT, gamma-glutamyl transpeptidase; AP, alkaline phosphatase; PT, prothrombin time; Hto, haematocrit; AFP, alpha-feto protein; n.s., not significant; n.a., not applicable.⁄One patient presented a non-cirrhotic liver.
Research Article
teristics are summarised in Table 1. All but one patient were cir-rhotic (95% Child-Pugh A). The most frequent etiology of cirrhosiswas HCV (62.5%), followed by ethanol (25%) and HBV (6.7%). Allpatients were asymptomatic (PS 0 100%) and 41 out of 104(39.4%) corresponded to BCLC-A stage. These patients had eithercontraindications to resection/transplantation/ablation or hadfailed them. Table 1 describes the characteristics of the cohortand when divided according to BCLC stage. As expected, theBCLC-A patients presented more frequently with a solitarytumour (n = 13) or two nodules (n = 28). The causes precludingpercutaneous ablation as a curative treatment were non-applica-bility of percutaneous ablation in 35 patients and post-treatmentrecurrence in 6. Radiofrequency is the first line option for abla-tion, and ethanol injection is the second line technique. Its effi-cacy decreases when HCC exceeds 3 cm and this is furtherimpaired in tumours with difficult location. In such instance,the necrotic action of ablation is not different from that achievedby TACE. Thus, some tumours (usually beyond 4 cm in size) wereshifted to TACE following the concept of ‘‘treatment stage migra-tion’’. Reasons for this were a combination of subcapsular loca-tion, vicinity to gallbladder, lung or bowel, together withtumour size in 34 patients. One HCC was not visible at ultraso-nography (US). Patients were not candidates for liver transplanta-tion and/or resection because of co-morbidities and/or portalhypertension.
None of the patients had received previous systemic therapy.The size of the beads was 500–700 microns in 22 patients and300–500 in 82. Median number of DEB-TACE treatments was 2(1–6). Only 46.1% of patients received the full dose of 150 mgof doxorubicin at first TACE, as complete artery obstruction wasachieved prior to injecting the expected vials.
1332 Journal of Hepatology 2012
Overall survival and complications
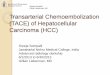
After a median follow-up of 24.5 months (2.6–79.6), 64 patientswere alive, 38 patients had died and two had received transplan-tation. The 1, 3, 4 and 5-year survival of the whole cohort was89.9%, 66.3%, 54.2% and 38.3%, with a median overall survival(OS) of 48.6 months (95% CI: 36.9–61.2) (Fig. 1). The 1, 3, 4 and5-year survival for BCLC-A patients was 89.7%, 67.8%, 50.8% and33.9%, with a median OS of 54.2 months (95% CI: 32.3–76.15),while for BCLC-B patients it was 88.2%, 64.4%, 47.3% and 39.4%,with a median OS of 47.7 months (95% CI: 32.7–62.7) (Figs. 2and 3). Survival after censoring follow-up at the time of trans-plant (n = 2), sorafenib treatment (n = 24) or radioembolisation(n = 1) was 47.7 months (95% CI: 37.9–57.5) for the whole cohort(Fig. 4), 40.6 months (95% CI: 12.8–84.4) for BCLC-A, and42.8 months (95% CI: 27.6–58.0) for BCLC-B.
None of the clinical and biochemical parameters (Table 1)divided the population according to significantly different sur-vival and hence, we could not identify any variable with predic-tive power.
Twenty-five patients were actively treated upon untreatabletumour progression (UTP). Twenty-four patients received sorafe-nib and one radioembolisation. Median time to UTP leading tosorafenib or radioembolisation treatment was 23.3 months(range: 4.9–55.5) and the causes of UTP were: significant intrahe-patic progression (n = 10), biliary dilatation related to tumour(n = 3), extrahepatic spread (n = 5), limiting technical issues(n = 2), DEB-TACE intolerance (n = 1) and increase of lesion sizeafter repeated DEB-TACE sessions (n = 4).
Ten patients presented with major complications after DEB-TACE: three abscesses, two arterial dissections, one cholecystitis,
vol. 56 j 1330–1335

Cum
ulat
ive
surv
ival
1.00
0.80
0.60
0.20
0.00
0.40
Survival functionCensored
Survival (mo)Subjects at risk n = 104
200 40 06 08 100
85 19 47 4
Fig. 1. Overall survival in the whole cohort.
Survival (mo)
Cum
ulat
ive
surv
ival
1.00
0.80
0.60
0.20
0.00
200 40 06 08 100
26 6 12 0
0.40
Survival functionCensored
Subjects at risk n = 41
Fig. 2. Overall survival in patients within BCLC-A.
Cum
ulat
ive
surv
ival
1.00
0.80
0.60
0.20
0.00
0.40
Survival functionCensored
Survival (mo)200 40 60 80 100
43 15 25 0Subjects at risk n = 63
Fig. 3. Overall survival in patients within BCLC-B.
Cum
ulat
ive
surv
ival
1.00
0.80
0.60
0.20
0.00
0.40
Survival functionCensored
Censoring survival (mo)200 40 60 80 100
59 14 35 0Subjects at risk n = 104
Fig. 4. Overall survival in the whole cohort after censoring patients with livertransplantation and sorafenib treatment.
JOURNAL OF HEPATOLOGY
one hepatic subcapsular haematoma, one pancreatitis, one biliarydilatation not related to tumour and one severe pain. One patientwith arterial dissection developed a pseudoaneurysm that wasunsuccessfully treated by surgery, but finally corrected by coilembolisation. The second dissection was self-limited and did
Journal of Hepatology 2012
not prevent further embolisation. The subcapsular bleeding wassuccessfully managed conservatively without need for furtherintervention. Among the three patients with abscesses, 1 dieddue to progressive hepatic failure, and the other two were solvedwith medical treatment. Thus, we had a single treatment-relateddeath (0.96%).
Discussion
Our results provide relevant information for the field of locore-gional treatment of HCC patients. They demonstrate that DEB-TACE has an adequate safety profile and, more importantly, theyshow that the survival assumptions of patients treated with TACEhave to be updated if using adequate selection criteria and state-of-the-art techniques.
The survival figures provide useful information for practiceand research. A 48.6-month median survival represents a majorexpansion if compared with survival data gathered years ago.Obviously, this improvement is the result of an earlier diagnosis,a better staging, and an improved patients’ management,together with a refined treatment application. Whatever the rea-son, the key point is that this is the outcome prediction to be con-sidered when recommending a specific treatment for a givenpatient and also when informing about the life expectancy.Recent cohort studies and registry data also show that the sur-vival of HCC patients treated with TACE has be updated [19–21]. However, while in our study the clinical stage of patients iswell described according to the BCLC strategy, some of the otherstudies do not provide a clear profile of the patients. Treatment ofBCLC-A with TACE reflects real life scenario and the so-called‘‘treatment stage migration’’ concept. It indicates that individua-lised evaluation of a given HCC patient may prompt that the firstline option that would correspond to that stage is not feasible/recommended because of tumour location or co-morbidities.The same phenomenon happens in patients within BCLC-B thathave contraindications for TACE or treatment failure still fittingin the intermediate stage. They are considered for sorafenib andto understand the survival data in the real life clinical setting itwill be key to carefully dissect the population that has ultimatelybeen treated. In that regard, it is important to note that patientstreated with TACE may present objective response, but during
vol. 56 j 1330–1335 1333

Research Article
follow-up they may present with new tumour sites and qualify asdisease progression. Intrahepatic progression may be again trea-ted with TACE, but in some instances contraindications due totumour burden (extrahepatic spread, vascular invasion) or toliver function impairment may argue against treatment repeti-tion. As a consequence, we have two types of disease progression:(i) treatable progression that may again achieve disease control,and (ii) untreatable progression that may prime initiation of sys-temic therapy that now should be sorafenib. We registered suchtransition to sorafenib in 24 patients (it occurred after theapproval of the drug in 2008) and radioembolisation in onepatient. To avoid any confounding survival improvement due totreatment with transplantation, sorafenib or radioembolisation,we performed the survival analysis censoring follow-up at thetime of these treatments. The figures obtained do not signifi-cantly diverge and thus, suggest that the improved survival can-not be attributed to this sequential treatment application. Wealso checked if the survival would be due to the inclusion of BCLCstage A patients, while those at intermediate stage B would nothave such an encouraging survival. As expected, the survival ofBCLC-A patients was slightly better than that of BCLC-B patients,but even so, the median survival of both subgroups exceeds4 years confirming that the improved survival is not a mere con-sequence of a biased selection process.It is important to retain that patients with symptoms related tocancer are considered advanced and not considered for TACE. In ourgroup, this is assessed through the performance status that isequivalent to the Karnofsky score. Asymptomatic patients have abetter life expectancy both if untreated and treated. Survival aftersurgical resection is impaired in patients with symptomatic dis-ease; and in our 2002 trial [6], assessing the survival benefits ofTACE, we described that presence of symptoms was an indepen-dent predictor of therapeutic response and survival. Absence ofsymptoms is always taken as an argument for pushing the limitsto decide treatment when the clinical stage is not optimal for agiven intervention. Frequently, pressure to engage in any availabletreatment option bases the decision on feasibility rather than onsurvival benefit. In a way, all options may be applied but the out-come may not be improved or even impaired. This is the case whenconsidering TACE for patients with vascular invasion. It might bedone, therapeutic response may be obtained, but survival is signif-icantly reduced as reflected by raw data and by the recognition ofvascular invasion as an adverse survival predictor [9,10,22]. Thisis well exemplified in the indication of surgery for large/multifocalHCC or when portal hypertension is already in place. The outcomeof patients is significantly lower than when tumours are small andsolitary, and the liver function is well preserved, but the argumentis frequently based on the survival data of those patients that havebeen operated on after a selective policy and on the outdated TACEsurvival including all sorts of patients.
Our data provide insight about life expectancy that may beachieved with TACE in patients that may be considered for sur-gery or transplantation with expanded criteria because the sur-vival assumptions seem more favourable. The discussion aboutthis issue exceeds the scope of this study, but the major shortageof donors and the need to estimate the survival of patientsaccording to intention-to-treat and equal organ distributionmake our survival figures highly valuable to frame the debateabout expanding the limits or not.
In addition, if research trials with TACE as backbone of treat-ment are designed with survival as an end point, the baseline
1334 Journal of Hepatology 2012
expectancy should no longer be a 2-year median survival, butrather twice as much. Several trials are now ongoing, testingthe combination of molecular targeted agents with TACE or eventhe comparison of conventional TACE vs. DEB-TACE. If the inclu-sion criteria for such trials do not carefully define the target pop-ulation, any positive or negative outcome data may be the resultof an underestimation of the baseline assumptions and events toregister during follow-up.
The confirmation of the safety of DEB-TACE in a large cohort ofHCC patients is worthwhile as the evaluation of any novel devicefor human use requires repeated prospective validation. In thatsense, one of the data that has raised concerns on the use ofDEB is the incidence of hepatic abscess. This complication is wellaccepted for TACE independently of the material used for the pro-cedure. It is due to the fact that necrotic tissue is an optimal cul-ture media for bacteria and if bacteremia occurs after TACE, therisk of infection is obvious. Biliary dilatation increases the risk,but even if excluding such patients, hepatic abscess may develop.Since bacteremia may occur immediately or days after the proce-dure, antibiotic prophylaxis will not be able to prevent it. This isthe basis to not administer any prophylaxis to our patients. It isimportant to note that in the Precision V trial comparing conven-tional TACE with DEB-TACE, the incidence of hepatic abscess wasnot different between arms [5]. The same message can be derivedfrom the studies by other authors in which the incidence rangedbetween 0% - 4.8% [3,4,20,23,24]. The other adverse events areclearly procedure-related and not specific to the agent used forTACE. Indeed, the major advantage of DEB is the capacity to injecta higher dose of chemotherapy without its passage into the sys-temic circulation. This results in a better tolerance due to a lowerchemotherapy-related toxicity, as shown in the Precision V trial[5]. Our study confirmed that the use of higher doxorubicin dos-age is not associated with a higher incidence of major chemother-apy-related adverse events. In addition, it might be that higherdosage of chemotherapy ultimately enhances the therapeuticresponse by overriding the capacity of the multidrug resistancepump that characterises HCC cells. A higher response rate asper imaging techniques was not proven in Precision V [5], butit is important to note that response rate assessment and its com-parison across techniques have not been validated. Intensity ofarterial obstruction and inflammatory changes in the surround-ing tissue may differ between techniques, and if using lipiodolemulsion for drug delivery, the uptake and retention within thetumour may complicate response assessment. In our study, weavoided any assessment of response rate as it would not providemeaningful information because of heterogeneous timing andtechnology. We instead decided to revisit the safety of DEB-TACEand focus the analysis on patients’ survival.
In summary, this study validates the safety of DEB-TACE inpatients with HCC selected according to optimal criteria anddefines the survival expectancy that should be assumed in clini-cal practice. This information is essential to decide between con-troversial surgical indications and TACE, and also to designresearch trials in which TACE is the backbone of treatment.
Conflict of interest
J. Bruix had exerted as consultant or received grants from: Sumi-tomo, Pharmexa, Eisai, Biocompatibles, Biolliance, Bayer Scher-ing, Lilly, Novartis, Arqule, Angiodynamics, Kowa, Imclone.
vol. 56 j 1330–1335

JOURNAL OF HEPATOLOGY
C. Ayuso, M. Burrel, A. Forner, M. Reig, and C. Rodriguez-Lopehad exerted as consultant: Terumo Europe, Bayer Schering.M. Barrufet and M. Real had exerted as consultant: Terumo
Europe.M. Llovet received Research Support from: Bayer Pharmaceuti-
cal, Bristol Myers Squibb and Consultancy Agreements from BayerPharmaceutical, Bristol Myers Squibb, Imclone, Biocompatibles.
Financial support
This study has been supported by a grant from the Instituto deSalud Carlos III (PI 08/0146). CIBERehd is funded by Instituto deSalud Carlos III. Carlos Rodríguez de Lope is supported by a grantof the Instituto de Salud Carlos III (FI09/00510).
Silvia Tremosini was partially supported by a grant from BBVAfoundation. Maria Reig was partially supported by a grant fromthe University of Barcelona (APIF RD63/2006).
Josep M Llovet is supported by grants from the US NationalInstitutes of Diabetes and Digestive and Kidney Diseases(1R01DK076986-01), the European Commission’s FrameworkProgramme 7 (HEPTROMIC, Proposal No: 259744), and theSpanish National Health Institute (SAF-2010-16055).
References
[1] Bruix J, Sherman M. Management of hepatocellular carcinoma: an update.Hepatology 2011;53:1020–1022.
[2] Varela M, Real MI, Burrel M, Forner A, Sala M, Brunet M, et al. Chemoemb-olization of hepatocellular carcinoma with drug eluting beads: efficacy anddoxorubicin pharmacokinetics. J Hepatol 2007;46:474–481.
[3] Poon RT, Tso WK, Pang RW, Ng KK, Woo R, Tai KS, et al. A phase I/II trial ofchemoembolization for hepatocellular carcinoma using a novel intra-arterialdrug-eluting bead. Clin Gastroenterol Hepatol 2007;5:1100–1108.
[4] Malagari K, Chatzimichael K, Alexopoulou E, Kelekis A, Hall B, Dourakis S,et al. Transarterial chemoembolization of unresectable hepatocellular car-cinoma with drug eluting beads: results of an open-label study of 62patients. Cardiovasc Intervent Radiol 2008;31:269–280.
[5] Lammer J, Malagari K, Vogl T, Pilleul F, Denys A, Watkinson A, et al.Prospective randomized study of doxorubicin-eluting-bead embolization inthe treatment of hepatocellular carcinoma: results of the Precision V study.Cardiovasc Intervent Radiol 2010;33:41–52.
[6] Llovet JM, Real MI, Montana X, Planas R, Coll S, Aponte J, et al. Arterialembolisation or chemoembolisation versus symptomatic treatment inpatients with unresectable hepatocellular carcinoma: a randomised con-trolled trial. Lancet 2002;359:1734–1739.
[7] Lo CM, Ngan H, Tso WK, Liu CL, Lam CM, Poon RT, et al. Randomizedcontrolled trial of transarterial lipiodol chemoembolization for unresectablehepatocellular carcinoma. Hepatology 2002;35:1164–1171.
[8] Raoul JL, Sangro B, Forner A, Mazzaferro V, Piscaglia F, Bolondi L, et al.Evolving strategies for the management of intermediate-stage hepatocellu-
Journal of Hepatology 2012
lar carcinoma: available evidence and expert opinion on the use oftransarterial chemoembolization. Cancer Treat Rev 2011;37:212–220.
[9] Luo J, Guo RP, Lai EC, Zhang YJ, Lau WY, Chen MS, et al. Transarterialchemoembolization for unresectable hepatocellular carcinoma with portalvein tumor thrombosis: a prospective comparative study. Ann Surg Oncol2011;18:413–420.
[10] Hu HT, Kim JH, Lee LS, Kim KA, Ko GY, Yoon HK, et al. Chemoembolization forhepatocellular carcinoma: multivariate analysis of predicting factors fortumor response and survival in a 362-patient cohort. J Vasc Interv Radiol2011;22:917–923.
[11] Llovet JM, Bruix J. Systematic review of randomized trials for unresectablehepatocellular carcinoma: chemoembolization improves survival. Hepatol-ogy 2003;37:429–442.
[12] Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatology2005;42:1208–1236.
[13] Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet 2012.doi:10.1016/S0140-6736(11)61347-0. PMID:22353262.
[14] Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transectionof the oesophagus for bleeding oesophageal varices. Br J Surg1973;60:646–649.
[15] Sorensen JB, Klee M, Palshof T, Hansen HH. Performance status assessmentin cancer patients. An inter-observer variability study. Br J Cancer1993;67:773–775.
[16] Bruix J, Reig M, Rimola J, Forner A, Burrel M, Vilana R, et al. Clinical decisionmaking and research in hepatocellular carcinoma: Pivotal role of imagingtechniques. Hepatology 2011;54:2238–2244.
[17] Shelgikar CS, Loehle J, Scoggins CR, McMasters KM, Martin RC, 2nd. Empiricantibiotics for transarterial embolization in hepatocellular carcinoma:indicated? J Surg Res 2009;151:121-124.
[18] Castells A, Bruix J, Ayuso C, Bru C, Montanya X, Boix L, et al. Transarterialembolization for hepatocellular carcinoma. Antibiotic prophylaxis andclinical meaning of postembolization fever. J Hepatol 1995;22:410-415.
[19] Takayasu K, Arii S, Ikai I, Kudo M, Matsuyama Y, Kojiro M, et al. Overallsurvival after transarterial lipiodol infusion chemotherapy with or withoutembolization for unresectable hepatocellular carcinoma: propensity scoreanalysis. AJR Am J Roentgenol 2010;194:830–837.
[20] Malagari K, Pomoni M, Kelekis A, Pomoni A, Dourakis S, Spyridopoulos T,et al. Prospective randomized comparison of chemoembolization withdoxorubicin-eluting beads and bland embolization with BeadBlock forhepatocellular carcinoma. Cardiovasc Intervent Radiol 2010;33:541–551.
[21] Bargellini I, Sacco R, Bozzi E, Bertini M, Ginanni B, Romano A, et al.Transarterial chemoembolization in very early and early-stage hepatocellu-lar carcinoma patients excluded from curative treatment: a prospectivecohort study. Eur J Radiol [3 April 2011, Epub ahead of print]. PMID:21466931.
[22] Takayasu K, Arii S, Ikai I, Omata M, Okita K, Ichida T, et al. Prospective cohortstudy of transarterial chemoembolization for unresectable hepatocellularcarcinoma in 8510 patients. Gastroenterology 2006;131:461–469.
[23] Nicolini A, Martinetti L, Crespi S, Maggioni M, Sangiovanni A. Transarterialchemoembolization with epirubicin-eluting beads versus transarterialembolization before liver transplantation for hepatocellular carcinoma. JVasc Interv Radiol 2010;21:327–332.
[24] Malagari K, Pomoni M, Spyridopoulos TN, Moschouris H, Kelekis A, DourakisS, et al. Safety profile of sequential transcatheter chemoembolization withDC Bead: results of 237 hepatocellular carcinoma (HCC) patients. CardiovascIntervent Radiol 2011;34:774–785.
vol. 56 j 1330–1335 1335