Embed Size (px)
Citation preview
Susan Roberts, MS, RD, CNSC
Andrea JeVenn, RD, LD, CNSC
ABDOMINAL EXAMINATIONAND THE
ASSESSMENT OF FLUID ACCUMULATION
THEABDOMINAL EXAMINATION
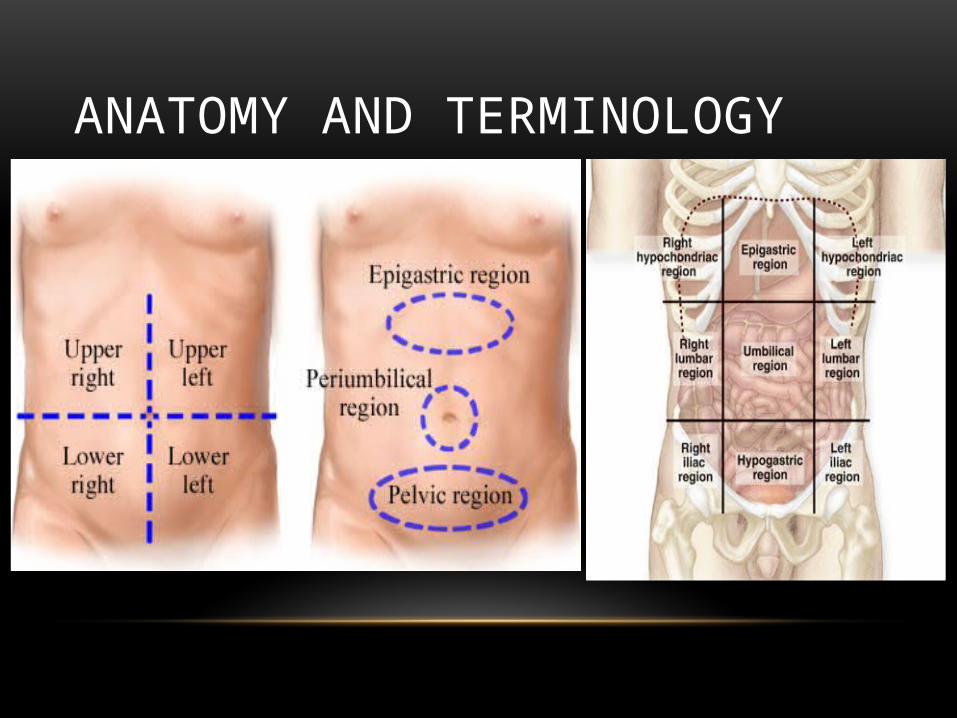
ANATOMY AND TERMINOLOGY
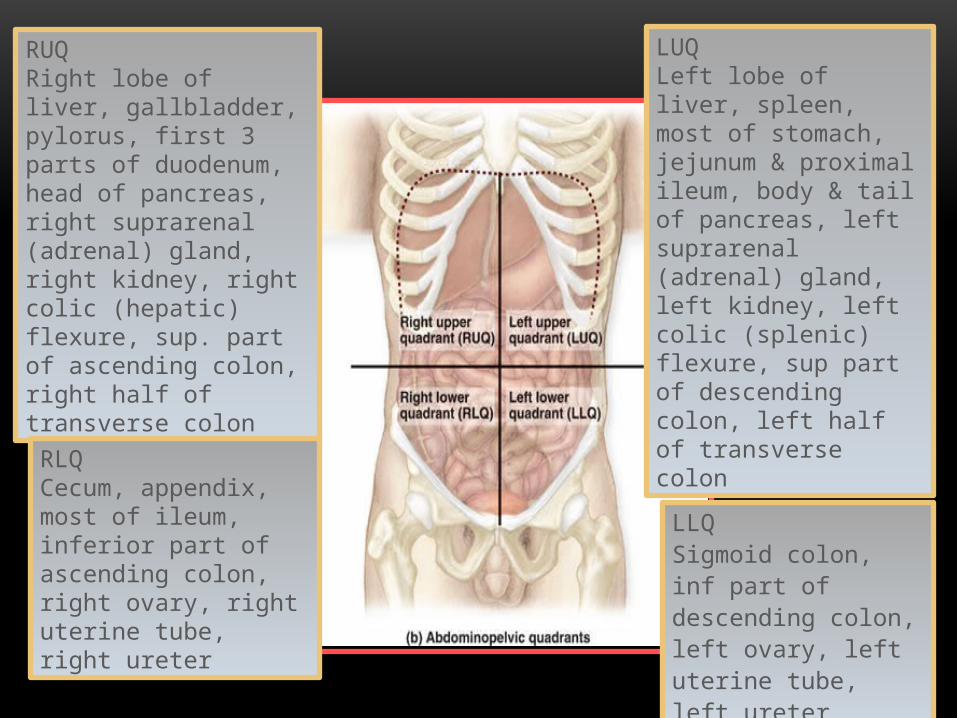
RUQ Right lobe of liver, gallbladder, pylorus, first 3 parts of duodenum, head of pancreas, right suprarenal (adrenal) gland, right kidney, right colic (hepatic) flexure, sup. part of ascending colon, right half of transverse colon
RLQ Cecum, appendix, most of ileum, inferior part of ascending colon, right ovary, right uterine tube, right ureter
LLQ Sigmoid colon, inf part of descending colon, left ovary, left uterine tube, left ureter
LUQ Left lobe of liver, spleen, most of stomach, jejunum & proximal ileum, body & tail of pancreas, left suprarenal (adrenal) gland, left kidney, left colic (splenic) flexure, sup part of descending colon, left half of transverse colon
COMPONENTS OF EXAM
Inspection• Visual review
• Assess symmetry and contour
Auscultation• Assess bowel and vascular sounds
• Done prior to palpation
Percussion• assess location & density of underlying body
masses/organs, gas/fluid patterns
AUSCULTATION
Use diaphragm of stethoscope
Begin in RLQ (ileo-cecal valve)
Listen in each quadrant• What are bowel sounds?
• Gas and fluid movement• Active
• Hypoactive
• Absent
BOWEL SOUNDSHyperactive
• Increased motility
• Stenosis
• Early SBO
• Resolving ileus
• Gastroenteritis
Hypoactive• Decreased motility
• Inflammation
• Paralytic ileus
• Peritonitis
• Surgical manipulation
• Late SBO
• Lower lobe pneumonia
PERCUSSION
Light tapping on abdomen• Assess size and position of solid organs
• Differentiate gas versus liquid vs solids
Tympany
Dullness
ILEUSAbsence of peristalsis or function
• Lack of mechanical issue
Causes• Peritonitis• Sepsis• Medications, especially narcotics• Metabolic disturbances
• Hyperglycemia and hypokalemia
Absent or hypoactive BS
Abdominal distention
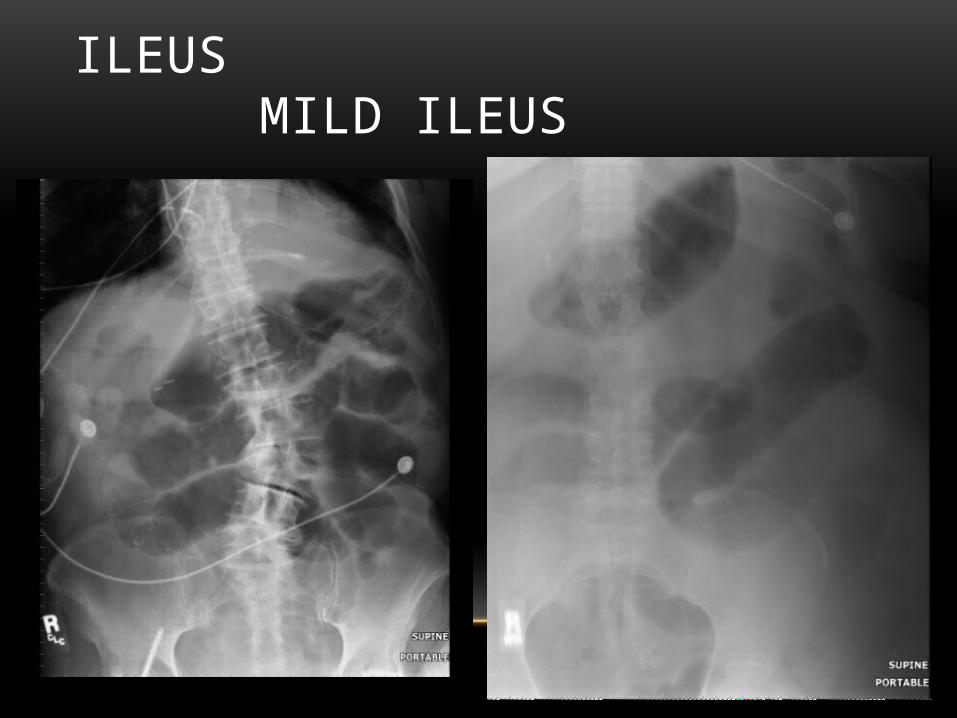
ILEUS MILD ILEUS
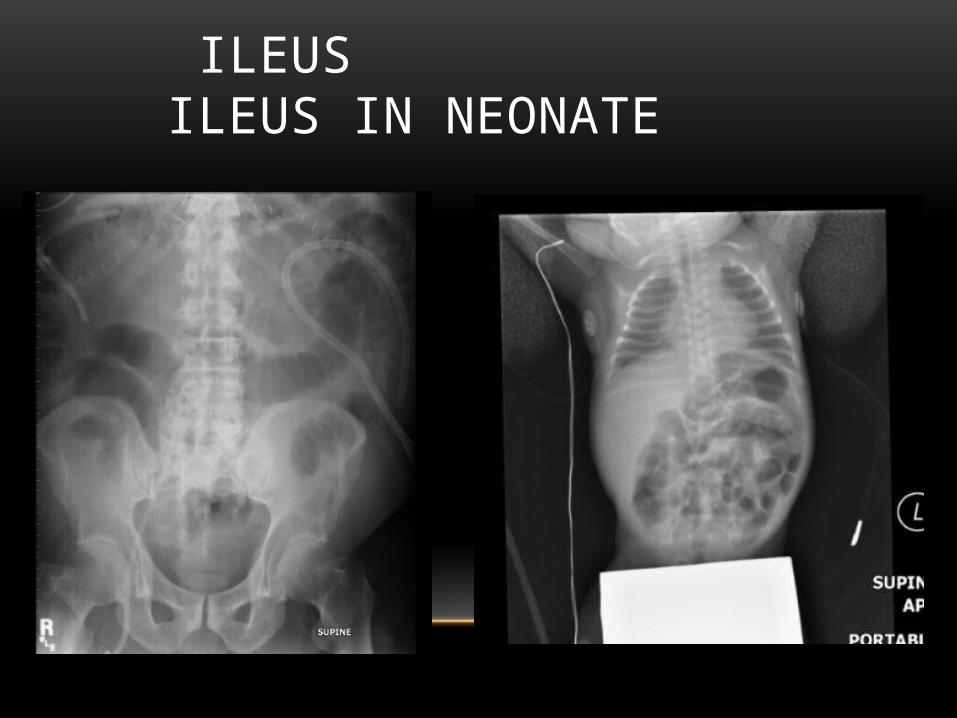
ILEUS ILEUS IN NEONATE
BOWEL OBSTRUCTIONDefined as a partial or complete blockage
Causes
• Extrinsic
• Adhesions, volvulus, or hernias
• Intrinsic
• Tumor, stricture, stenosis
• Intraluminal
• Bezoars, fecal material, gallstones
BOWEL OBSTRUCTIONGeneral signs & symptoms
• Distention• Hyperactive or high
pitched BS• Minimum rebound• Crampy pain
Tests• Abdominal film• CT• UGI and/or small
bowel series
SITE OF OBSTRUCTION
Proximal• Acute onset
• Greater vomiting
• Bilious emesis
• Less distention
Distal• Less vomiting
• Greater explosive diarrhea
• Greater distention
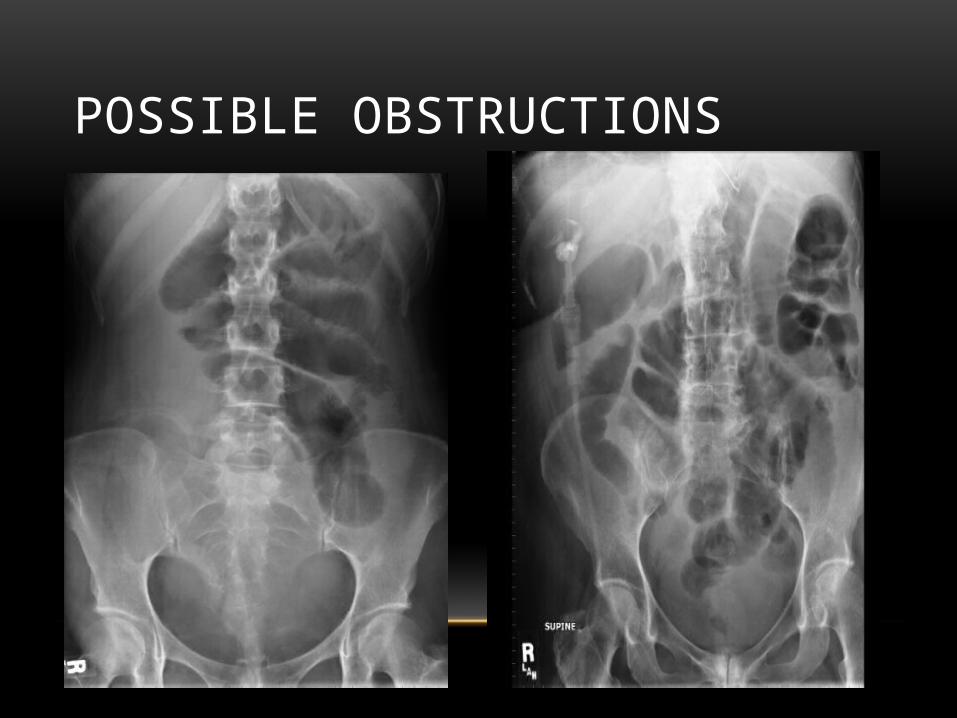
POSSIBLE OBSTRUCTIONS
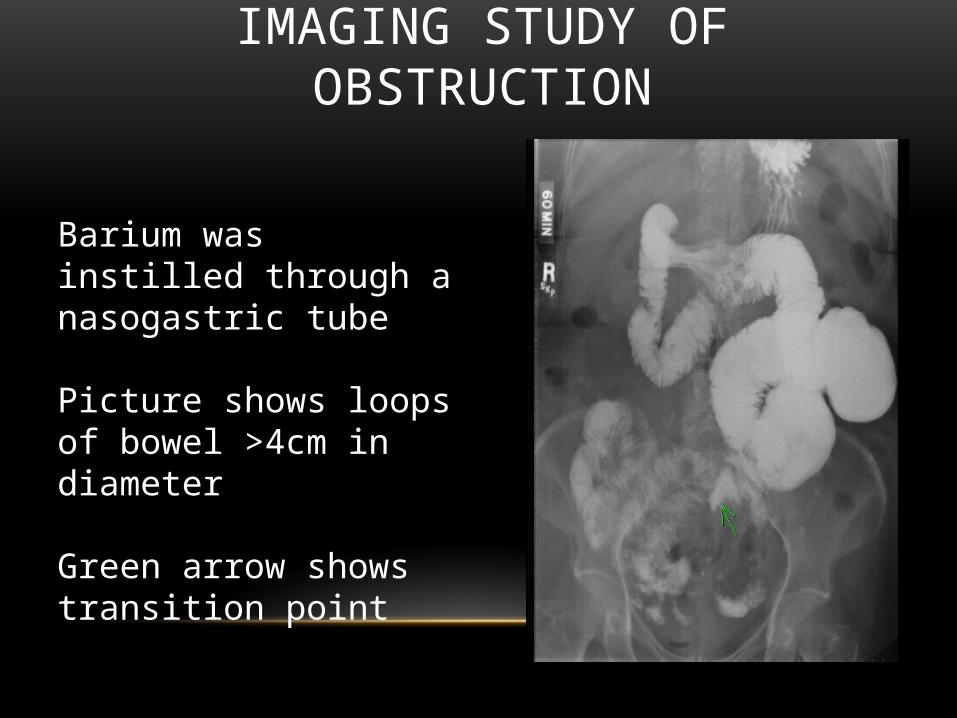
IMAGING STUDY OF OBSTRUCTION
Barium was instilled through a nasogastric tube
Picture shows loops of bowel >4cm in diameter
Green arrow shows transition point
ILEUS VS OBSTRUCTION
Ileus• No source of obstruction
• Gas in colon/rectum
• Distention but without pain
• May have bowel sounds
ASSESSING FLUID ACCUMULATION
WHAT IS FLUID RETENTION?
Abnormal retention of fluid in interstitial spaces and cavities (e.g., peritoneal/abdominal cavity)
• may not clinically manifest until it accounts for at least 10% of body weight or fluid volume is increased by 2.5-3 liters
• fluid accumulation around the heart, in the lungs, small pockets of ascites, or hematomas may only be seen on imaging studies
Braunwald, Loscalzo. Ch 36: Edema. In: Longo DL, Kasper DL, et al. Harrisons Principles of Internal Medicine; 2012 Epocrates: Evaluation of Peripheral Edema; accessed 11/26/14Sterns RH. Clinical manifestations and diagnosis of edema in adults; UpToDate 1/30/14 Ch 15: I have a patient with edema. How do I determine the Cause? In: Symptom to Diagnosis: An Evidence-Based Guide; 2009
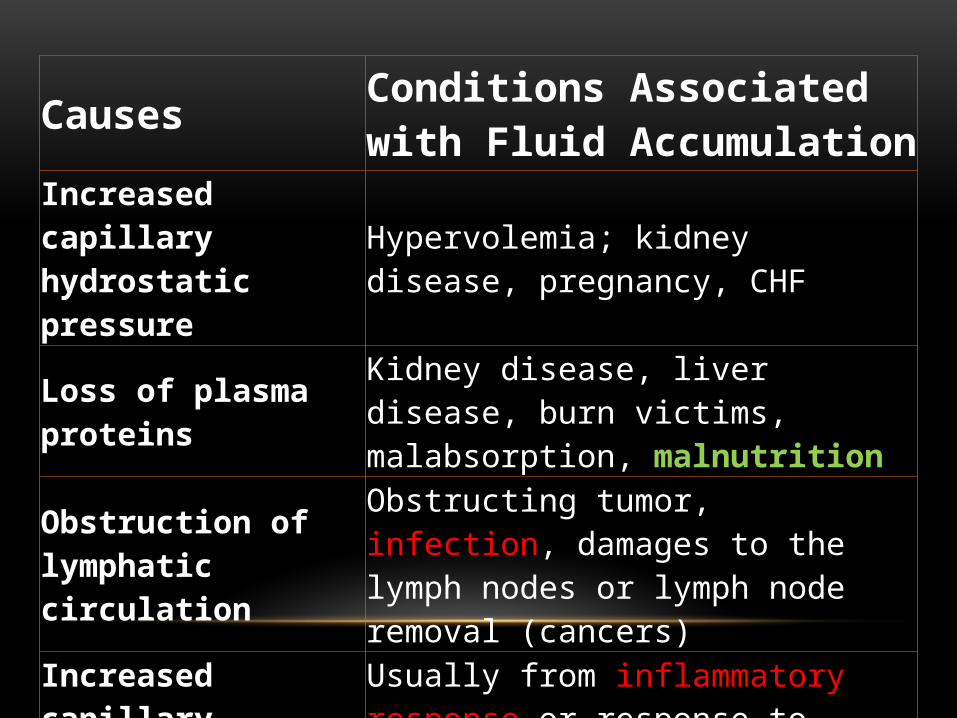
Causes Conditions Associated with Fluid Accumulation
Increased capillary hydrostatic pressure Hypervolemia; kidney disease, pregnancy, CHF
Loss of plasma proteins Kidney disease, liver disease, burn victims, malabsorption, malnutrition
Obstruction of lymphatic circulation
Obstructing tumor, infection, damages to the lymph nodes or lymph node removal (cancers)
Increased capillary permeability
Usually from inflammatory response or response to infections
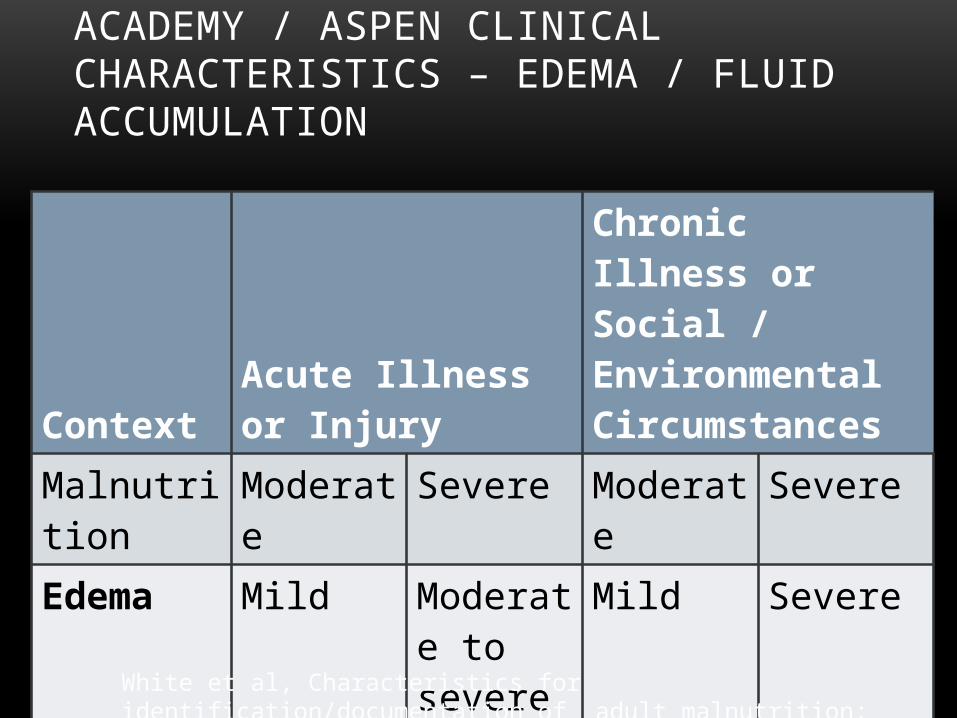
ACADEMY / ASPEN CLINICAL CHARACTERISTICS – EDEMA / FLUID ACCUMULATION
Context Acute Illness or Injury
Chronic Illness or Social / Environmental Circumstances
Malnutrition Moderate Severe Moderate Severe
Edema Mild Moderate to severe
Mild Severe
White et al, Characteristics for identification/documentation of adult malnutrition; JPEN 2012
• Weight loss is frequently masked by fluid retention and weight gain may be present
• If severe, can also mask evaluation of muscle/fat loss
• Usually SUPPORTIVE evidence
- RARELY ever directly related to malnutrition
White et al, Characteristics for identification/documentation of adult malnutrition; JPEN 2012
ACADEMY / ASPEN CLINICAL CHARACTERISTICS – EDEMA / FLUID ACCUMULATION
ASSESSING FLUID RETENTION
• Primarily found in dependent areas such as the sacrum, ankles, feet, calves, scrotum, vulva
• The clinician may evaluate generalized or localized fluid accumulation during a physical exam
• Localized:
• extremities, abdomen (ascites), vulva/scrotal area
• Generalized:
• if severe, is referred to as anasarca

DEPENDENT EDEMA – AMBULATORY PATIENTS: LEGS, ANKLES, FEET
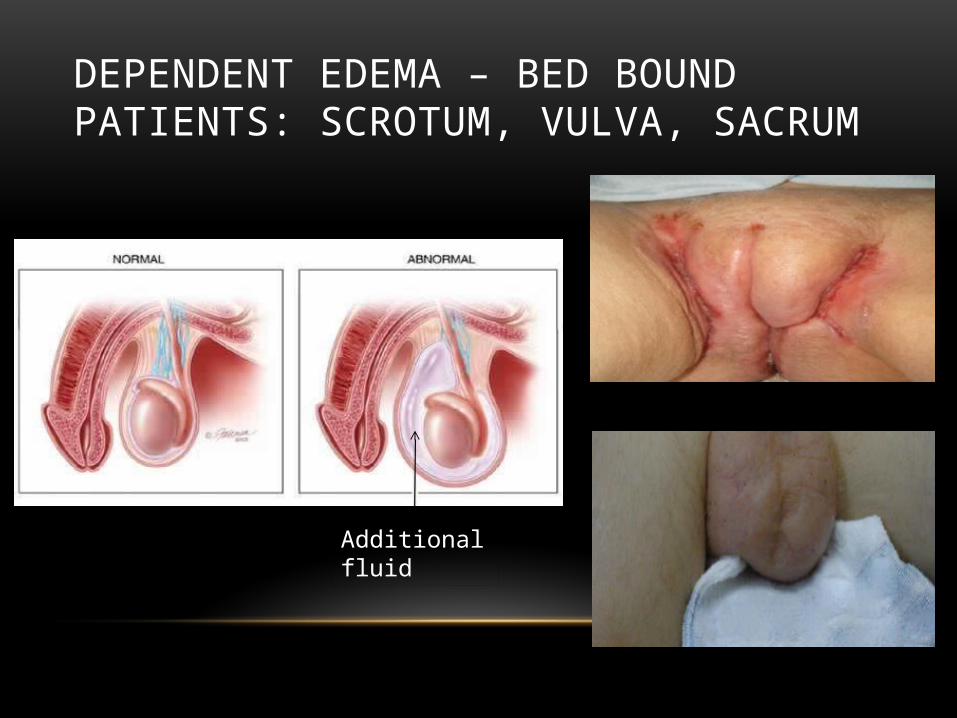
DEPENDENT EDEMA – BED BOUND PATIENTS: SCROTUM, VULVA, SACRUM
Additional fluid
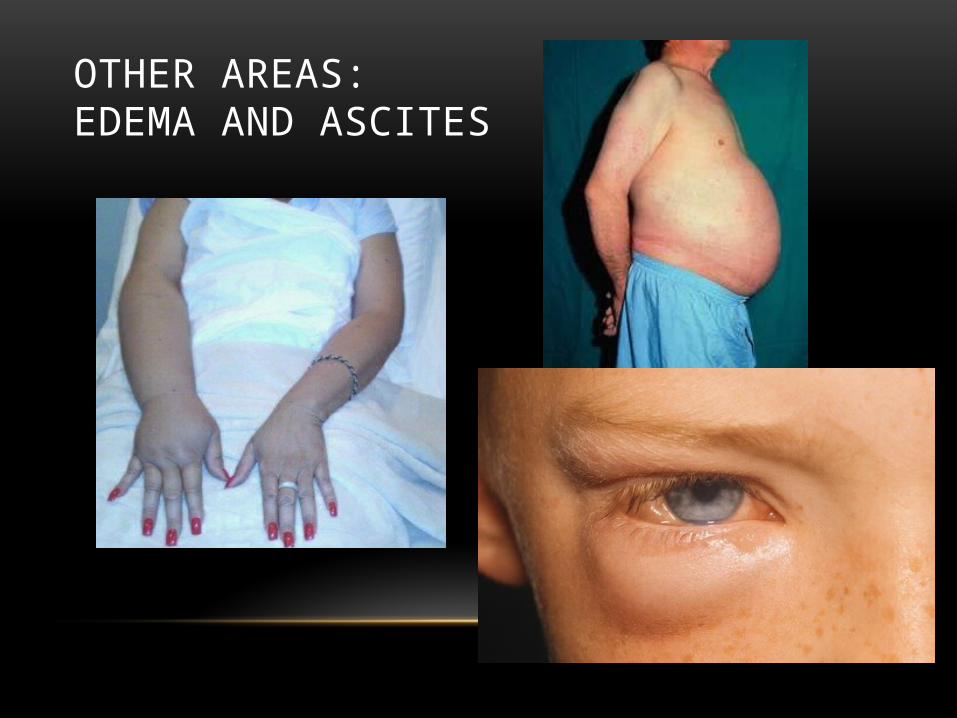
OTHER AREAS:EDEMA AND ASCITES
ASSESSMENT STRATEGY
• Perform general survey, then head-to-toe
• Use inspection and palpation• gloves optional
• Determine if onset is acute vs chronic• Acute: < 72 hours
• Chronic: better? worse? same?
• Correlate physical findings of fluid accumulation with other evidence • vital signs, input/output records, labs, weight, history,
imaging studies
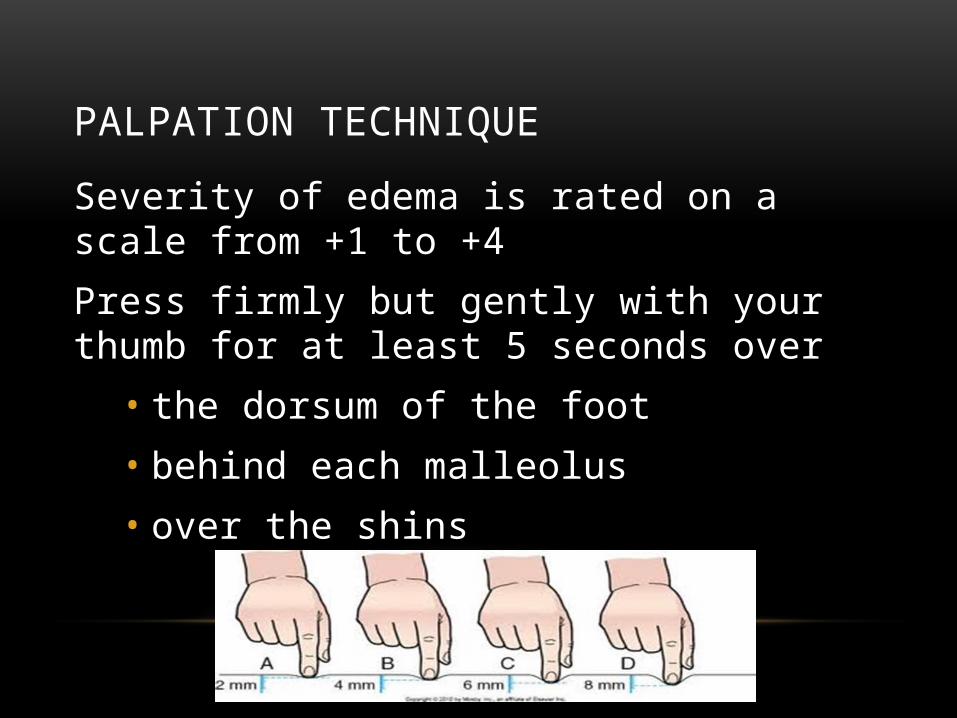
Severity of edema is rated on a scale from +1 to +4
Press firmly but gently with your thumb for at least 5 seconds over
• the dorsum of the foot
• behind each malleolus
• over the shins
PALPATION TECHNIQUE
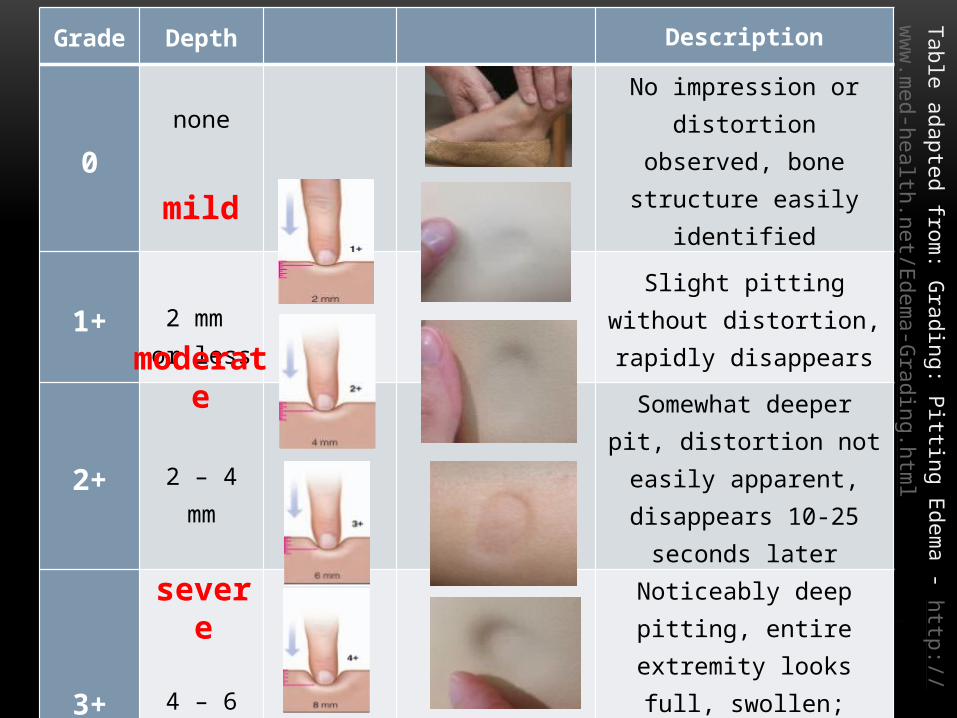
Grade
Depth
Description
0none No impression or distortion
observed, bone structure easily identified
1+ 2 mm or less
Slight pitting without distortion, rapidly disappears
2+ 2 – 4 mm
Somewhat deeper pit, distortion not easily apparent, disappears
10-25 seconds later
3+ 4 – 6 mm
Noticeably deep pitting, entire extremity looks full, swollen;
indentation can last longer than 1 minute
4+ 6 – 8 mmVery deep pitting, extremity is
grossly misshapen, indentation lasts 2-5 minutes
Table adapted from: G
rading: Pitting Edema - http://
www.med-health.net/Edem
a-Grading.htm
l
mild
severe
moderate
FEASIBILITY OF ACCESSING DATA IN HOSPITALIZED PATIENTS…
• Cross-sectional survey at 4 different hospitals: 2 tertiary teaching,1 urban, 1 rural; included 262 adults
• Determined availability of data to support the proposed Academy/ASPEN malnutrition characteristics
• Data on edema available at time of nutrition assessment
• All patients – 84.4%, Non-ICU – 85.9%, ICU – 82.7%
• Edema used as one of the characteristics to define malnutrition
• All patients – 26.6%, Non-ICU – 16.2%, ICU – 39.1%
Nicolo et al. JPEN 2013
SUMMARY
• Nutritional and medical history, & current medical picture must be considered before determining whether fluid accumulation is a relevant characteristic to use in identifying malnutrition
• Many patients have fluid accumulation but not all are malnourished
• RARELY a direct result of malnutrition
• Fluid accumulation may not always be readily visible
• Fluid accumulation will falsely increase weight / mask weight loss and can prevent muscle mass / SQ fat assessment
• Continue to partner with nurses, physicians and other health care team members to enhance assessment of fluid status





























