Embed Size (px)
Citation preview
SWAHS Clinical Redesign Aged & Chronic Complex
Peter StralowResponding to the Challenge Forum 12 September 2007
Background
Improve interfaces between:•Aged Care•Chronic care Cardiac & Respiratory•Community Health•PACC/NOS•GPs•NGOs
Specifically to improve:•patient intake, •triage, •assessment, •and cross referral between service providers.
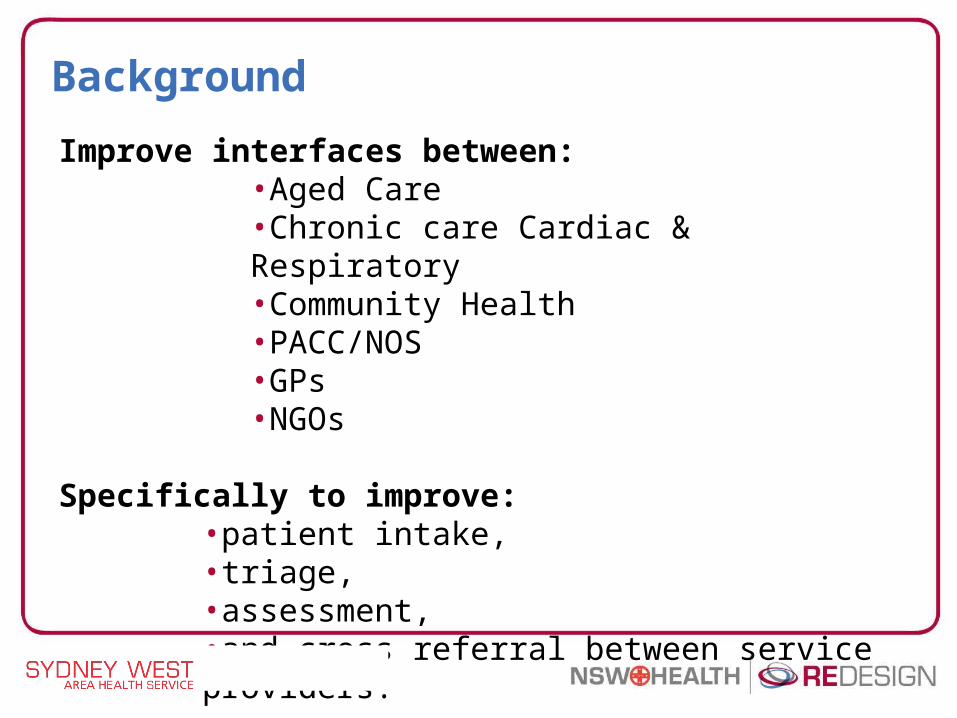
Summary of patient interviews
POSITIVE & NEGATIVE ASPECTS OF PATIENT & CARER EXPERIENCE
12 10 8 6 4 2 0 2 4
No. of Patient nterviewees
Positive / Agree
Negative / Disagree
Fast Access to reliable Health care
Involvement in decisions & respect for patients privileges
Physical comfort and a clean, safe environment
Involvement of, and support for families and carers
Smooth transition to and support for self-care
Effective treatment delivered by staff you can trust
Clear comprehensible information delivered throughout journey
Emotional support, empathy and respect
Coordination and continuity of patient care
6 8 10 12
POSITIVE & NEGATIVE ASPECTS OF PATIENT & CARER EXPERIENCE
12 10 8 6 4 2 0 2 4
No. of Patient nterviewees
Positive / Agree
Negative / Disagree
Fast Access to reliable Health care
Involvement in decisions & respect for patients privileges
Physical comfort and a clean, safe environment
Involvement of, and support for families and carers
Smooth transition to and support for self-care
Effective treatment delivered by staff you can trust
Clear comprehensible information delivered throughout journey
Emotional support, empathy and respect
Coordination and continuity of patient care
6 8 10 12
Patient interviews
The staff sometimes don’t give us information as they think we know it all. I’ve been doing this for 40 years. (carer)
They need co-ordinating in one hit.
I had visits by Nepean outreach and the community nurses. There was a bit of a mix up between NOS and the community nurses-one did not know the other was coming”.
Number of patient interviews attended: 21The tool used was the NSW Health Patient and Carer Experience Discussion Record.
In summary… what did we learn?
There is nothing systemically wrong with current practices, however there is;
• Little to no coordination & standardisation across services & clusters
• SWAHS hospital, outreach and community services operate on a ‘hub and spoke’ model to external services such as GPs, RACFs and NGOs
• Knowledge of services and access to information is disjointed with reliance placed on informal ‘experts’ for advice (rightly or wrongly)
• Intake criteria are inconsistent – but should they be standardised?
In summary… what did we learn?
High commitment among staff and evidence of numerous innovations (e.g. OPERA, HOPE Project, HOME First) in models of care.
There was a clear commitment to move forward to a successful program of cohesive, integrated and aligned solutions.
To facilitate this desired outcome the project team identified the need to develop a framework that would provide coherence and rigour in the solution design process.
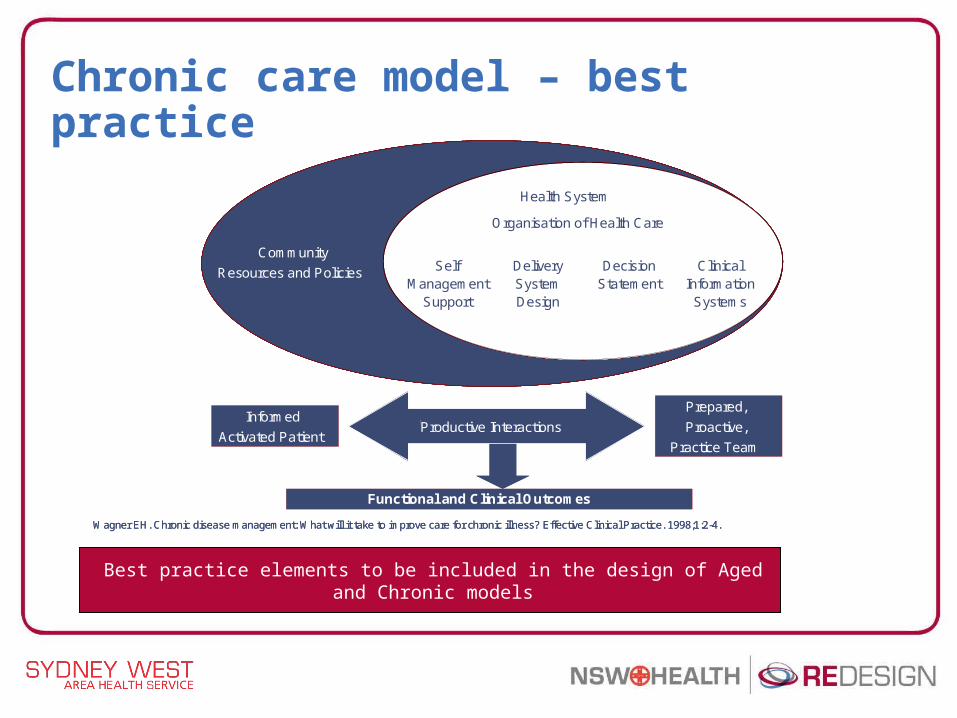
Chronic care model – best practice
Wagner EH. Chronic disease management: What will it take to improve care for chronic illness? Effective Clinical Practice. 1998;1:2-4.
Health System
Organisation of Health Care
Self
Management
Support
Delivery
System
Design
Decision
Statement
Clinical
Information
Systems
Informed
Activated Patient
Prepared,
Proactive,
Practice Team
Functional and Clinical Outcomes
Health System
Organisation of Health Care
Self Management
Support
DeliverySystemDesign
Decision Statement
Clinical Information
Systems
Health System
Organisation of Health Care
Self
Management
Support
Delivery
System
Design
Decision
Statement
Clinical
Information
Systems
Productive InteractionsProductive InteractionsInformed
Activated Patient
Prepared,
Proactive,
Practice Team
Functional and Clinical Outcomes
Community
Resources and Policies
Health System
Organisation of Health Care
Self Management
Support
DeliverySystemDesign
Decision Statement
Clinical Information
Systems
Productive InteractionsProductive InteractionsInformed
Activated Patient
Prepared,
Proactive,
Practice Team
Functional and Clinical Outcomes
Productive InteractionsProductive InteractionsInformed
Activated Patient
Prepared,
Proactive,
Practice Team
Functional and Clinical Outcomes
Wagner EH. Chronic disease management: What will it take to improve care for chronic illness? Effective Clinical Practice. 1998;1:2-4.
Health System
Organisation of Health Care
Self
Management
Support
Delivery
System
Design
Decision
Statement
Clinical
Information
Systems
Informed
Activated Patient
Prepared,
Proactive,
Practice Team
Functional and Clinical Outcomes
Health System
Organisation of Health Care
Self Management
Support
DeliverySystemDesign
Decision Statement
Clinical Information
Systems
Health System
Organisation of Health Care
Self
Management
Support
Delivery
System
Design
Decision
Statement
Clinical
Information
Systems
Productive InteractionsProductive InteractionsInformed
Activated Patient
Prepared,
Proactive,
Practice Team
Functional and Clinical Outcomes
Community
Resources and Policies
Health System
Organisation of Health Care
Self Management
Support
DeliverySystemDesign
Decision Statement
Clinical Information
Systems
Productive InteractionsProductive InteractionsInformed
Activated Patient
Prepared,
Proactive,
Practice Team
Functional and Clinical Outcomes
Productive InteractionsProductive InteractionsInformed
Activated Patient
Prepared,
Proactive,
Practice Team
Functional and Clinical Outcomes
Best practice elements to be included in the design of Aged and Chronic models
Hospital NGO / Others Community Health
Patient / Carer / Client
Specialist
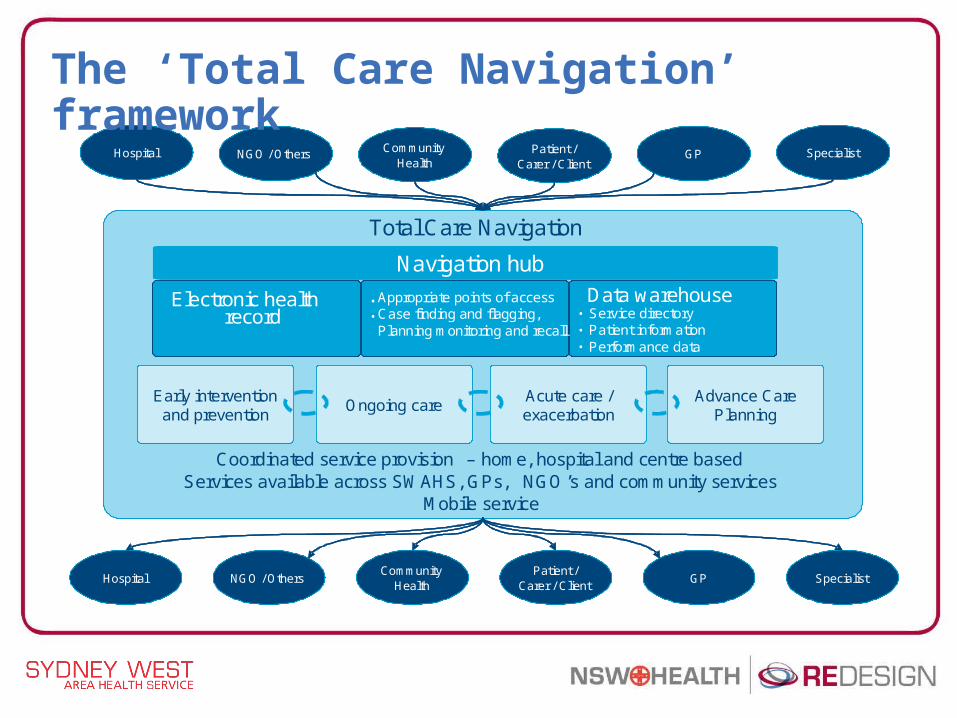
Total Care Navigation
Coordinated service provision – home, hospital and centre based Services available across SWAHS, GPs, NGO’s and community services
Mobile service
•
•Electronic health
recordData warehouse
• Service directory• Patient information• Performance data
Ongoing careAcute care / exacerbation
Advance Care Planning
Early intervention and prevention
Hospital NGO / OthersCommunity
HealthPatient /
Carer / ClientSpecialist
GP
GP
Appropriate points of accessCase finding and flagging, Planning monitoring and recall
Navigation hub
••
Hospital NGO / Others Community Health
Patient / Carer / Client
Specialist
Total Care Navigation
Coordinated service provision – home, hospital and centre based Services available across SWAHS, GPs, NGO’s and community services
Mobile service
•
•Electronic health
recordData warehouse
• Service directory• Patient information• Performance data
Ongoing careAcute care / exacerbation
Advance Care Planning
Early intervention and prevention
Hospital NGO / OthersCommunity
HealthPatient /
Carer / ClientSpecialist
GP
GP
Appropriate points of accessCase finding and flagging, Planning monitoring and recall
Navigation hub
••
The ‘Total Care Navigation’ framework
The ‘Total Care Navigation’ framework
• Reflects the focus on enabling patients to access the right services from the right providers at the right time matched to their level of need.
• It provided a way of cohesively considering solutions, their design, their priority and their interconnections, as part of the larger picture.
• In essence, this served as a guide for solution design with a focus on delivering improved patient journeys
• A key focus of the project has been to ensure that strategies are in place to respond to the challenges of winter 2008.
Solutions
Implementation of a system for care coordination
Care coordination including a strategy that places a person in appropriate programs
Systems that flags clients and provides an understanding of the level of engagement e.g. at risk patients
First point of contact early identification
Solutions
Implementation of a Navigation Hub
Single point of access within SWAHS Access to information and advice for patientsService directory that facilitates the identification of pathways for patient care
Utilise existing systems to provide access to patient information
A system that provides required levels of patient information to relevant service providers across the continuum of care
Solutions
Development and implementation of a self management program
Self management programs (stratify low, medium and high) including opportunities for consumers to self manage using communication tools, e.g. electronic home based care
Enhanced participation of GPs in the core management of these patients
Develop and implement a suite of solutions that enhance GP participation in the core process as well as investigate the functions of GP liaison nurses across SWAHS
Solutions
Service enhancements
Rapid access/response
Enhance hospital in home programs including opening up access points
Advance care planning in SWAHS by utilising a model of expansion of Geriatric Medicine into RACFs (GRACE)
Alignment of aged and chronic care services
Carers program of coordinated
Transport services / car parking
Tele-based medicine























![Magazine [redesign]](https://img.pdfslide.net/doc/110x75/557c8689d8b42a9f578b4f3c/magazine-redesign.jpg)