Embed Size (px)
DESCRIPTION
definiton, causes, treatment
Citation preview

Syncope
MRS SHAGUFTA ISHTIAQRESPIRATORY AND CIRTICAL CARE TECHNOLOGIST.
DIMT-Dow University of Health Sciences

OBJECTIVES
AT THE END OF LECTURE STUDENTS WILL BE ABLE TO
Understand syncope
Know Etiology of syncope
Know the Impact of syncope

Classification of Transient Loss of Consciousness (TLOC)
Syncope• Neurally-mediated reflex
syndromes
• Orthostatic hypotension
• Cardiac arrhythmias
• Structural cardiovascular disease
Disorders Mimicking Syncope• With loss of consciousness, i.e.,
seizure disorders
• Without loss of consciousness, i.e., psychogenic “pseudo-syncope”
Real or Apparent Transient Loss of Syncope (TLOC)
Brignole M, et al. Europace, 2004;6:467-537.

Syncope – A Symptom, Not a Diagnosis
Self-limited loss of consciousness and postural tone
Relatively rapid onset
Variable warning symptoms
Spontaneous, complete, and usually prompt recovery without medical or surgical intervention
Underlying mechanism is transient global cerebral hypoperfusion.
Brignole M, et al. Europace, 2004;6:467-537.

Section I

Causes of True Syncope
Orthostatic CardiacArrhythmia
StructuralCardio-
Pulmonary
1• Vasovagal
syncope (VVS)
• Carotid sinus syndrome (CSS)
• SituationalCoughPost- Micturition
2• Drug-Induced• Autonomic
Nervous System (ANS) Failure
3• Brady
Sinus Node Dysfunction
Atro Ventricular Block
• TachyVent
Tacycardia VT
Sinus VT (SVT)
• Long QT Syndrome
4 • Acute
Myocardial Ischemia
• Aortic Stenosis
• Hypertrophic Cardiomyopathy (HCM)
• Pulmonary Hypertension
• Aortic Dissection
Neurally-Mediated

Section II:
Diagnosis

Diagnostic Objectives
Distinguish true syncope from syncope mimics
Determine presence of heart disease
Establish the cause of syncope with sufficient
• Assessment of prognosis
• effective preventive treatment

A Diagnostic Plan is Essential
Initial Examination• Detailed patient history• Physical exam• ECG• Supine and upright
blood pressure Monitoring
• Holter• Event• Insertable Loop Recorder (ILR)
Cardiac Imaging Special Investigations
• Head-up tilt test• Hemodynamics • Electrophysiology study

Diagnostic Flow Diagram for Transient Loss of Consiousness TLOC
Initial Evaluation
Treatment
Syncope Not Syncope
Certain Diagnosis
Unexplained Syncope
Cardiac Likely
Cardiac Tests
Neurally-Mediated or Orthostatic Likely
Tests for Neurally-Mediated Syncope
Frequent or Severe Episodes
Tests for Neurally-Mediated Syncope
Single/Rare Episodes
No Further Evaluation
Confirm with Specific Test or
Specialist Consultation
Suspected Diagnosis
+ - + - + -
Treatment Treatment
Re-AppraisalRe-Appraisal
Treatment

Initial Exam: Detailed Patient History
Circumstances of recent event• Eyewitness • Symptoms at onset of event• Sequelae• Medications
Circumstances of more remote events
Concomitant disease, especially cardiac
Pertinent family history• Cardiac disease• Sudden death• Metabolic disorders
Past medical history• Neurological history• Syncope
Brignole M, et al. Europace, 2004;6:467-537.

Initial Exam: Thorough Physical
Vital signs
• Heart rate
• Orthostatic blood pressure change
Cardiovascular exam: Is heart disease present?
• ECG: Long QT, pre-excitation, conduction system disease
• Echo: LV function, valve status, HCM—Hypertrophic Cardiomyopathy
Neurological exam
Carotid sinus massage
• Perform under clinically appropriate conditions preferably during head-up tilt test
• Monitor both ECG and BP
Brignole M, et al. Europace, 2004;6:467-537.

Carotid Sinus Massage (CSM)
Method1
• Massage, 5-10 seconds
• Don’t occlude
• Supine and upright posture (on tilt table)
Outcome
• 3 second as ystole and/or 50 mmHg fall in systolic BP with reproduction of symptoms = Carotid Sinus Syndrome
Absolute contraindications2
• Carotid bruit, known significant carotid arterial disease, previous CVA, MI last 3 months
Complications
• Primarily neurological
• Less than 0.2%
• Usually transient
60° - 80°

Other Diagnostic Tests
Ambulatory ECG
• Holter monitoring
• Event recorder− Intermittent vs. Loop
− Insertable Loop Recorder (ILR)
Head-Up Tilt (HUT)
• Includes drug provocation (NTG, isoproterenol)
• Carotid Sinus Massage (CSM)
Adenosine Triphosphate Test (ATP)
Electrophysiology Study (EPS)
Brignole M, et al. Europace, 2004;6:467-537.

Heart Monitoring Options
ILR
Event Recorders(non-lead and loop)
Holter Monitor
12-Lead
2 Days
7-30 Days
Up to 14 Months
10 Seconds
OPTION
TIME (Months)
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Brignole M, et al. Europace, 2004;6:467-537.

Head-Up Tilt Test (HUT)
Protocols vary
Useful as diagnostic adjunct in atypical syncope cases
Useful in teaching patients to recognize prodromal symptoms
Not useful in assessing treatment
Brignole M, et al. Europace. 2004;6:467-537.
60° - 80°

Reveal® Plus ILR
Insertable Loop Recorder (ILR)
Typical Location of theReveal® Plus ILR
Click once on black screen to play video.

Insertable Loop Recorder (ILR)
The ILR is an implantable patient – and automatically – activated monitoring system that records subcutaneous ECG and is indicated for: Patients with clinical syndromes or situations at increased risk of
cardiac arrhythmias
Patients who experience transient symptoms that may suggest a cardiac arrhythmia

Section III:
Specific Conditions and Treatment

Specific Conditions
Cardiac arrhythmia
• Brady/Tachy
• Long QT syndrome
• Torsade de pointes
• Brugada
• Drug-induced
Structural cardio-pulmonary
Neurally-mediated
• Vasovagal Syncope (VVS)
• Carotid Sinus Syndrome (CSS)
Orthostatic

Cardiac Syncope
Includes cardiac arrhythmias
Often life-threatening
May be warning of critical CV disease
• Tachy and brady arrhythmias
• Myocardial ischemia, aortic stenosis, pulmonary hypertension, aortic dissection
Assess culprit arrhythmia or structural abnormality aggressively
Initiate treatment promptly
Brignole M, et al. Europace. 2004;6:467-537.

Syncope Due to Structural Cardiovascular Disease: Principle Mechanisms
Acute MI/Ischemia
• 2° neural reflex bradycardia – Vasodilatation, arrhythmias, low output (rare)
Hypertrophic cardiomyopathy
• Limited output during exertion (increased obstruction, greater demand), arrhythmias, neural reflex
Acute aortic dissection
• Neural reflex mechanism, pericardial tamponade
Pulmonary embolus/pulmonary hypertension
• Neural reflex, inadequate flow with exertion
Valvular abnormalities
• Aortic stenosis – Limited output, neural reflex dilation in periphery
• Mitral stenosis, atrial myxoma – Obstruction to adequate flow
Brignole M, et al. Europace. 2004;6:467-537.

Syncope Due to Cardiac Arrhythmias
Bradyarrhythmias
• Sinus arrest, exit block
• High grade or acute complete AV block
• Can be accompanied by vasodilatation (VVS, CSS)
Tachyarrhythmias
• Atrial fibrillation/flutter with rapid ventricular rate (eg, pre-excitation syndrome)
• Paroxysmal SVT or VT
• Torsade de pointes
Brignole M, et al. Europace. 2004;6:467-537.

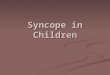
Cardiac Rhythms During Unexplained Syncope-ILR
Seidl K. Europace. 2000;2(3):256-262.Krahn AD. PACE. 2002;25:37-41.Medtronic ILR Replacement Data. FY03, 04. On file.
No Recurrence 36%
(31-48%)
Normal Sinus Rhythm 31%
(17-44%)
Other 11%
Arrhythmia 22%
(13-32%)
Tachycardia 6%(2-11%)
Bradycardia 16%
(11-21%)
Composite: N=133 to 7109

Long QT Syndromes
Mechanism
• Abnormalities of sodium and/or potassium channels
• Susceptibility to polymorphic VT (Torsade de pointes)
Prevalence
• Drug-induced forms – Common
• Genetic forms – Relatively rare, but increasingly being recognized
• “Concealed” forms:
− May be common
− Provide basis for drug-induced torsade
Schwartz P, Priori S. In: Zipes D and Jalife J, eds. Cardiac Electrophysiology. Saunders;2004:651-659.

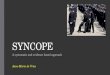
Syncope: Torsade de Pointes
From the files of DG Benditt, MD. U of M Cardiac Arrhythmia Center

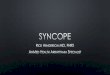
Long QT Syndromes: 12-Lead ECG
From the files of DG Benditt, MD. U of M Cardiac Arrhythmia Center

Drug-Induced QT Prolongation(List is continuously being updated)
Antiarrhythmics
• Class IA
• Class III
Antianginal Agents Psychoactive Agents
Antibiotics
• Erythromycin, Pentamidine, Fluconazole, Ciprofloxacin and its relatives
Nonsedating antihistamines
• Terfenadine*, Astemizole
Others
• Cisapride*, Droperidol, Haloperidol
*Removed from U.S. MarketBrignole M, et al. Europace, 2004;6:467-537.

Syncope Due to Bradyarrhythmia
ACC/AHA/NASPE 2002 Guideline Update. Circ. 2002;106:2145-2161.
nV
0.4
0.2
0.0
-0.2
-0.4
:45:44:43:42:41:40:39:38:37
:37:36:35:34:33:32:31:30:29
:29:28:27:26:25:24:23:22:21
08:23:21
8:23:29
08:23:37
0.4
0.2
0.0
-0.2
-0.4
0.4
0.2
0.0
-0.2
-0.4

Treatment of Syncope Due to Tachyarrhythmia
Atrial tachyarrhythmias
• AVRT due to accessory pathway – Ablate pathway
• AVNRT – Ablate AV nodal slow pathway
• Atrial fib – Pacing, linear/focal ablation for paroxysmal AF
• Atrial flutter – Ablate the IVC-TV isthmus of the re-entrant circuit for ‘typical’ flutter
Ventricular tachyarrhythmias
• Ventricular tachycardia – ICD or ablation where appropriate
• Torsade de pointes – Withdraw offending drug or implant ICD (long QT/Brugada/short QT)
Drug therapy may be an alternative in many cases
Brignole M, et al. Europace. 2004;6:467-537.

Neurally-Mediated Reflex Syncope
Vasovagal Syncope (VVS)
Carotid Sinus Syndrome (CSS)
Situational syncope
• Post-micturition
• Cough
• Swallow
• Defecation
• Blood drawing, etc.
Brignole M, et al. Europace, 2004;6:467-537.

VVSDiagnosis
History and physical exam, ECG and BP
Head-Up Tilt (HUT) – Protocol:
• Fast > 2 hours
• ECG and continuous blood pressure, supine, and upright
• Tilt to 70°, 20 minutes
• Isoproterenol/Nitroglycerin if necessary
• End point – Loss of consciousness
60° - 80°
Benditt D, et al. JACC. 1996;28:263-275.Brignole M, et al. Europace, 2004;6:467-537.

VVS General Treatment Measures
Optimal treatment strategies for VVS are a source of debate
Treatment goals• Acute intervention
− Physical maneuvers, eg, crossing legs or tugging arms
− Lowering head− Lying down
Long-term prevention• Tilt training
• Education
• Diet, fluids, salt
• Support hose
• Drug therapy
• Pacing
Brignole M, et al. Europace, 2004;6:467-537.

VVS Tilt Training Protocol
Objectives
• Enhance orthostatic tolerance
• Diminish excessive autonomic reflex activity
• Reduce syncope susceptibility/recurrences
Technique
• Prescribed periods of upright posture against a wall
• Start with 3-5 min BID
• Increase by 5 min each week until a duration of 30 min is achieved
Reybrouck T, et al. PACE. 2000;23(4 Pt. 1):493-498.

CSSEtiology
Sensory nerve endings in the carotid sinus walls respond to deformation
“Deafferentation” of neck muscles may contribute
Increased afferent signals tobrain stem
Reflex increase in efferent vagal activity and diminution of sympathetic tone results in bradycardia and vasodilatation
Carotid Sinus

Orthostatic Hypotension
Etiology
Drug-induced (very common)
• Diuretics
• Vasodilators
Primary autonomic failure
• Multiple system atrophy
• Parkinson’s Disease
• Postural Orthostatic Tachycardia Syndrome (POTS)
Secondary autonomic failure
• Diabetes
• Alcohol
• Amyloid
Brignole M, et al. Europace, 2004;6:467-537.

Syncope: Diagnostic Testing in Hospital Strongly Recommended
Suspected/known ‘significant’ heart disease
ECG abnormalities suggesting potential life-threatening arrhythmic cause
Syncope during exercise
Severe injury or accident
Family history of premature sudden death
Brignole M, et al. Europace. 2004;6:467-537.

Conclusion
Syncope is a common symptom with many causes
Deserves thorough investigation and appropriate treatment
A disciplined approach is essential
Brignole M, et al. Europace, 2004;6:467-537.

Brief Statement
Indications9526 Reveal® Plus Insertable Loop RecorderThe Reveal Plus ILR is an implantable patient- and automatically activated monitoring system that records subcutaneous ECG and is indicated forPatients with clinical syndromes or situations at increased risk of cardiac arrhythmias Patients who experience transient symptoms that may suggest a cardiac arrhythmia 6191 ActivatorThe Model 6191 Activator is intended for use in combination with a Medtronic Model 9526 Reveal Plus Insertable Loop Recorder.ContraindicationsThere are no known contraindications for the implantation of the Reveal Plus ILR. However, the patient’s particular medical condition may dictate whether or not a subcutaneous, chronically implanted device can be tolerated.Warnings/Precautions9526 Reveal Plus Insertable Loop RecorderPatients with the Reveal Plus ILR should avoid sources of magnetic resonance imaging, diathermy, high sources of radiation, electrosurgical cautery, external defibrillation, lithotripsy, and radiofrequency ablation to avoid electrical reset of the device, and/or inappropriate sensing.6191 ActivatorOperation of the Model 6191 Activator near sources of electromagnetic interference, such as cellular phones, computer monitors, etc., may adversely affect the performance of this device.Potential ComplicationsPotential complications include, but are not limited to, body tissue rejection phenomena, including local tissue reaction, infection, device migration and erosion of the device through the skin.2090 ProgrammerThe Medtronic/Vitatron CareLink programmer system is comprised of prescription devices indicated for use in the interrogation and programming of implantable medical devices. Prior to use, refer to the Programmer Reference Guide as well as the appropriate programmer software and implantable device technical manuals for more information related to specific implantable device models. Programming should be attempted only by appropriately trained personnel after careful study of the technical manual for the implantable device and after careful determination of appropriate parameter values based on the patient's condition and pacing system used. The Medtronic/Vitatron CareLink programmer must be used only for programming implantable devices manufactured by Medtronic or Vitatron.See the device manual for detailed information regarding the implant procedure, indications, contraindications, warnings, precautions, and potential complications/adverse events. For further information, please call Medtronic at 1-800-328-2518 and/or consult Medtronic’s website at www.medtronic.com. To learn more about syncope, visit www.fainting.com.Caution: Federal law (USA) restricts this device to sale by or on the order of a physician.