Embed Size (px)
Citation preview

CCR-14-0442; 13/2/2015; 2:45:34
Biology of Human Tumors
Systemic Immune-Inflammation Index Predicts Prognosis ofPatients after Curative Resection for HepatocellularCarcinoma
Bo Hu1, Xin-Rong Yang1, Yang Xu1, Yun-Fan Sun1, Chao Sun1, Wei Guo1,2, Xin Zhang1,Wei-Min Wang1, Shuang-Jian Qiu1, Jian Zhou1,3, and Jia Fan1,3
AbstractPurpose: We developed a novel systemic immune-inflammation index (SII) based on lymphocyte,
neutrophil, and platelet counts and explored its prognostic value in hepatocellular carcinoma (HCC).
Experimental Design: The SII was developed based on a retrospective study of 133 patients with HCC
undergoing resection between 2005 and 2006, and validated in a prospective study of 123 patients enrolled
from 2010 to 2011. The circulating tumor cell (CTC) level in the validation cohort was measured using the
CellSearch system. Prediction accuracy was evaluated with area under the receiver operating characteristic
curve (AUC).
Results:Anoptimal cutoff point for the SII of 330�109 stratified thepatientswithHCC intohigh (�330)
and low SII (<330) groups in the training cohort. Univariate and multivariate analyses revealed the SII was
an independent predictor for overall survival and relapse-free survival, and prognostic for patients with
negative a-fetoprotein and Barcelona Clinic Liver Cancer stage 0þA. The AUCs of the SII for survival and
recurrence were higher than other conventional clinical indices. An SII � 330 was significantly associated
with vascular invasion, large tumors, and early recurrence. CTC levels were significantly higher in the SII�330 group (1.71� 0.34 vs. 4.37� 1.04, P¼ 0.029). In patients with detectable CTCs, those with SII� 330
had higher recurrence rates and shorter survival time than patients with SII < 330.
Conclusion: The SII was a powerful prognostic indicator of poor outcome in patients with HCC and is a
promising tool for HCC treatment strategy decisions. The dismal outcome in patients with high SII scores
might be related to higher CTC levels. Clin Cancer Res; 20(23); 6212–22. �2014 AACR.
IntroductionHepatocellular carcinoma (HCC) is the fifth most com-
mon cancer and has the third highest mortality rate in theworld (1, 2). Currently, surgery remains themain treatmentfor patients with HCC. However, in spite of "curative"resection, approximate 60% to 70% patients experiencerecurrence or distant metastasis within 5 years (3). There-fore, it is important to identify patient subpopulations with
a high risk of recurrence and metastasis to optimize post-operative rational adjuvant treatments and provide thesetreatments to at-risk subpopulations without delay.
The reasons for the high recurrence/metastasis rate inHCCare complex and multifactorial. Hematogenous spread is animportant cause of recurrence and metastasis in HCC, andcirculating tumor cells (CTC) in the bloodstream play animportant role in HCC metastasis (4, 5). In addition to thetumor cells, immune and inflammatory cells such as neu-trophils, platelets, and lymphocytes also contribute to tumorcell invasion into the peripheral blood,where the tumor cellscan survive and reseed distant organs (6).
Several studies have shown that platelets can protectCTCs from shear stresses during circulation, induce CTCepithelial–mesenchymal transition, and promote tumorcell extravasation to metastatic sites (7–10). Neutrophilscan promote adhesion and seeding of distant organ sitesthrough secretionof circulating growth factors such asVEGFand proteases (11–15). Lymphocytes play a crucial role intumor defense by inducing cytotoxic cell death and inhibit-ing tumor cell proliferation and migration (16), therebydictating the host immune response to malignancy (12). Inconsideration of these factors, several inflammation andimmune-based prognostic scores have been developed to
1Department of Liver Surgery, Liver Cancer Institute, Zhongshan Hospital,Fudan University, and Key Laboratory of Carcinogenesis and CancerInvasion, Ministry of Education, Shanghai 200032, P.R. China. 2Depart-ment of Laboratory Medicine, Zhongshan Hospital, Fudan University.3Institute of Biomedical Sciences, Fudan University, Shanghai 200032,P.R. China.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
B. Hu, X.-R. Yang, Y. Xu contributed equally to this article.
Corresponding Author: Jia Fan, Liver Cancer Institute, Zhongshan Hos-pital, Fudan University, 136 Yi Xue Yuan Road, Shanghai 200032, P.R.China. Phone: 8602-1640-41990; Fax: 8602-1640-37181;E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-14-0442
�2014 American Association for Cancer Research.
ClinicalCancer
Research
Clin Cancer Res; 20(23) December 1, 20146212
Research. on June 27, 2020. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2014; DOI: 10.1158/1078-0432.CCR-14-0442

CCR-14-0442; 13/2/2015; 2:45:35
predict survival and recurrence, such as lymphocytecount, neutrophil–lymphocyte ratio (NLR), and plate-let–lymphocyte ratio (PLR; refs. 17–19); however, anintegrated indicator based on peripheral lymphocyte,neutrophil, and platelet counts, which might be betterable to reflect the balance of host inflammatory andimmune status, has not yet been reported in HCC. More-over, the potential effects of peripheral lymphocytes,neutrophils, and platelets on HCC recurrence and metas-tasis have not been elaborated.In this study, a novel index, defined as the systemic
immune-inflammation index (SII), based on lymphocyte,neutrophil, and platelet counts, was developed. The prog-nostic value of the SII in patients with HCCwho underwentsurgery was evaluated in two independent cohorts. Thecorrelation between the SII and CTC levels was alsoexplored. We found that the SII was a promising indepen-dent predictive factor for prognosis of patients with HCCafter surgery and that the high recurrence rate in patientswith high SII scores might be due to increased release ofCTCs from tumor sites.
Patients and MethodsPatients and specimensA retrospective study was conducted in a primary cohort
of patients with HCC who underwent curative resection inour institute from 2005 to 2006 (n¼ 133). From July 2010to June 2011, a validation cohort of patients withHCC (n¼123) undergoing resection was prospectively recruited,which was reported previously (5). The inclusion andexclusion criteria were the same as those previouslydescribed (20). Tumor stage was determined according to
the BarcelonaClinic LiverCancer (BCLC) stage (21). Tumordifferentiation was graded by the Edmondson gradingsystem (22). Liver function was assessed by the Child–Pughscoring system. The blood sample (7.5 mL) used for Cell-Search analysis was collected two days before resection asdescribed inour previous report (5). A secondblood sample(2mL) for platelet, neutrophil, and lymphocyte counts wasobtained at the same time and detected in laboratorydepartment. Ethical approval for the use of human subjectswas obtained from the ZhongshanHospital Research EthicsCommittee, and informed consent was obtained from allpatients. The comparative baseline clinical characteristics ofpatients in both training and validation cohorts aredescribed in Table 1.
Follow-up and treatment for tumor recurrencesPostoperative patient surveillance was performed as
described previously (23). Patients were followed up every2months during the first postoperative year, and then every3 to 4months. All patients were prospectivelymonitored byseruma-fetoprotein (AFP), abdomenultrasonography, andchest X-ray with an interval of 1 to 6 months depending onthe postoperative time. A computed tomography scanof theabdomen was performed every 6 months. Bone scan ormagnetic resonance imaging was done if localized bonepain was reported. If recurrence was suspected, a computedtomography scan or magnetic resonance imaging was doneimmediately. Most of death causes were recurrence, metas-tasis, or complicated liver cirrhosis. Patients with confirmedrecurrence received further treatment, which followed a setprotocol based on the size, site, number of tumor nodules,and liver function. Briefly, if the recurrent tumor was local-ized, a second liver resection, radiofrequency ablation, orpercutaneous ethanol injection was suggested. If the recur-rent tumor was multiple or diffused, transcatheter arterialchemoembolization was administered. External radiother-apy was given if lymph node or bonemetastasis was found.Otherwise, symptomatic treatment was provided. Follow-up was terminated on February 7, 2012, in the trainingcohort and on November 1, 2013, in the validation cohort.Time to recurrence (TTR) and overall survival (OS) weredefined as the interval between the surgery and recurrenceor death, respectively. Using 12 months as the cutoff value,all recurrences were divided into early recurrence and laterecurrence.
Systemic immune-inflammation indexThe SII was defined as follows: SII¼ P�N/L, where P,N,
and Lwere the preoperative peripheral platelet, neutrophil,and lymphocyte counts, respectively.
The X-tile 3.6.1 software (Yale University, New Haven,CT) was used for bioinformatic analysis of the trainingcohort data to determine the cutoff value of SII for tumorrecurrence (24). Results from X-Tile analysis revealed anoptimal cutoff point for the SII at 330� 109 in the trainingcohort (Supplementary Fig. S1). Subsequently, the SIIscores were stratified into <330 � 109 or �330 � 109 forall subsequent analyses.
Translational RelevanceSeveral inflammation and immune-based prognostic
scores have been developed to identify patients at highrisk of recurrence or mortality who may be difficult toidentify using traditional clinicopathologic indexes.However, these scores cannot reflect comprehensivelythe balance of host inflammatory and immune status.Therefore, a novel index, defined as the systemicimmune-inflammation index (SII), based on lympho-cyte, neutrophil, and platelet counts, was developed. Wefound that the SII was a promising independent predic-tive factor for prognosis of patients with hepatocellularcarcinoma (HCC) after surgery. We speculated thepotential mechanism that the elevated SII results in thedissemination of more tumor cells via the circulation,allowing tumor cells to escape immune surveillance, andfinally increasing the peripheral circulating tumor cellslevel. The low cost, easy determination, and reproduc-ibility of a full blood countmake the SII a promising toolfor HCC treatment strategy decisions in future clinicalpractice.
Prognostic Significance of SII in HCC
www.aacrjournals.org Clin Cancer Res; 20(23) December 1, 2014 6213
Research. on June 27, 2020. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2014; DOI: 10.1158/1078-0432.CCR-14-0442

CCR-14-0442; 13/2/2015; 2:45:36
Detection of CTCsEpithelial cell adhesion molecule-positive (EpCAMþ)
CTC analysis was performed before resection using theCellSearch (Veridex)method,without knowledge of patientclinical characteristics (25). Briefly, the semiautomatedCellSearch platform (Janssen Diagnostics) enriches thesample for cells expressing EpCAM with ferromagneticbeads. Fluorescently labeledmonoclonal antibodies specif-ic for cytokeratins and leukocyte (CD45) are used to dis-
tinguish epithelial cells from leukocytes. The identificationand enumeration of CTCs were performed with the use ofthe CellSpotter Analyzer. The CTC results were expressed asthe number of cells per 7.5 mL of blood.
Statistical analysisStatistical analyses were performed using IBM SPSS 19.0
software (SPSS). Continuous variables were summarized asthe median and range or the mean � SEM. The cumulative
Table 1. The clinicopathologic characteristics of patients in the training and validation cohorts
Clinical and pathologicTraining cohort Validation cohort
Indexes N ¼ 133 % N ¼ 123 % P
Age (y)�50 61 45.86 64 52.03 0.324>50 72 54.14 59 47.97
SexFemale 21 15.79 8 6.5 0.019Male 112 84.21 115 93.5
Liver cirrhosisNo 23 17.29 29 23.58 0.212a
Yes 110 82.71 94 76.42Child–PughA 132 99.25 122 99.19 1.000B 1 0.75 1 0.81
HBsAgNegative 24 18.05 12 9.76 0.057Positive 109 81.95 111 90.24
ALT (U/L)�40 69 51.88 75 60.98 0.143>40 64 48.12 48 39.02
AFP (ng/mL)�20 59 44.36 37 30.08 0.164>20 74 55.64 86 69.92
Tumor encapsulationComplete 73 54.89 77 62.6 0.211None 60 45.11 46 37.4
Tumor differentiationI–II 96 72.18 83 67.48 0.413III–IV 37 27.82 40 32.52
Tumor size (cm)�5 98 73.68 80 65.04 0.133>5 35 26.32 43 34.96
Tumor numberSingle 120 90.23 112 91.06 0.820Multiple 13 9.77 11 8.94
Vascular invasionNo 86 64.66 78 63.41 0.835Yes 47 35.34 45 36.59
BCLC0þA 82 61.65 101 82.11 <0.001BþC 51 38.35 22 17.89
Abbreviation: HBsAg, hepatitis B surface antigen.aFisher exact test.
Hu et al.
Clin Cancer Res; 20(23) December 1, 2014 Clinical Cancer Research6214
Research. on June 27, 2020. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2014; DOI: 10.1158/1078-0432.CCR-14-0442

CCR-14-0442; 13/2/2015; 2:45:36
recurrence and survival rates were calculated using theKaplan–Meier method, and the differences between thegroups were assessed by the log-rank test. Univariate andmultivariate analyses were calculated by the Cox propor-tional hazards regressionmodel. The Student t test, Pearsonc2 test, and the Fisher exact test were used to comparegroups. The Pearson c2 test or Fisher exact test was used tocompare qualitative variables; and quantitative variableswere analyzed by the Pearson correlation test. Receiveroperating characteristics (ROC) curves were used to definesensitivity, specificity, and the differences in the area underthe curves (AUC)were detected usingMedCalc version 13.0(MedCalcSoftware). A P value <0.05 was considered statis-tically significant.
ResultsPatient characteristicsThe clinicopathologic characteristics of patients are
shown in Table 1. In the training cohort, OS and recurrencerateswere 87.2%and26.3%at 1 year, 63.2%and36.1%at 3years, and 53.4% and 49.6% at 5 years, respectively. Therewere 71 (53.4%) patients confirmed dead and 70 (52.6%)patients confirmed with tumor recurrence at last follow-up.The mean age of the patients was 64.1 years (range, 32.0–86.0). The median follow-up period was 61.3 months(range, 2.0–86.4).In the validation cohort, 58 of 123 patients presentedwith
tumor recurrence at the final follow-up, with a medianfollow-up time of 28.8 months (range, 1.0–39.5), and 98patientswere still alive at amedian follow-upof 30.4months(range, 3.0–39.5). SII� 330 was present in 39.9% (53/133)of patients in the training cohort and 33.3% (41/123) ofpatients in the validation cohort (Supplementary Table S1).The clinicopathologic characteristics were similar betweenthe two cohorts, with the exception of gender and BCLCstage. The validation cohort included more males, andpatients in the training cohort had a more advanced BCLCstage than those in the validation cohort (Table 1).
Theprognostic significanceof SII in the training cohortResults from our univariate analysis indicated that AFP
level, tumor encapsulation, tumor differentiation, tumorsize, vascular invasion, BCLC stage, NLR, PLR, and SII wereprognostic factors for OS and/or TTR in the training cohort(Table 2), whereas age, gender, cirrhosis, Child–Pugh score,hepatitis history, alanine aminotransferase (ALT) level, andtumor number had no prognostic significance for OS andTTR. A low SII score was significantly associated with bothprolonged TTR [HR, 2.78; 95% confidence interval (CI),1.72–4.48; P < 0.001] and OS (HR, 2.62; 95% CI, 1.63–4.20; P < 0.001).The Kaplan–Meier analysis indicated that the high SII,
NLR, and PLR scores were all associated with shorterOS (P < 0.0001, P ¼ 0.001, and P ¼ 0.010, respectively)and TTR (P < 0.0001, P ¼ 0.001, and P ¼ 0.022,respectively; Fig. 1A; Supplementary Fig. S2A and S2B).The median TTR and OS were 61.3 and 63.3 months forpatients with SII < 330 and 26.4 and 37.3 months for
patients with SII � 330, respectively. In addition, patientswith an NLR < 5 had a median OS and TTR of 62.4 and51.7 months, respectively, whereas patients with an NLR� 5 had a median OS and TTR of 34.5 and 30.4 months,respectively. Patients with a PLR < 150 had a median OSand TTR of 61.3 and 47.1 months, respectively, comparedwith 55.2 and 47.1 months, respectively, for the patientswith a PLR � 150.
On the basis of our multivariate analysis, the SII was anindependent prognostic factor for both TTR (HR, 1.92; 95%CI, 1.04–3.54; P¼ 0.037) andOS (HR, 2.10; 95%CI, 1.14–3.85; P ¼ 0.017; Table 3). The discrimination ability ofinflammation-based prognostic scores and clinical indiceswas compared by the AUC for OS and TTR (Fig. 1C;Supplementary Fig. S2C). The AUC for the SII was 0.66(95% CI, 0.57–0.76) and 0.68 (95% CI, 0.59–0.77), whichwas the strongest factor among indices (NLR, PLR, tumornumber, size, encapsulation, differentiation, vascular inva-sion, AFP, and BCLC stage) for predicting survival andrecurrence in patients with HCC.
Validation of the SII in an independent cohortThe prognostic value of the SII score was further con-
firmed in an independent validation cohort of 123 patients.The results were similar to those obtained from the trainingcohort (Fig. 1B). The SII but not PLR remained associatedwith shorterOS (P¼ 0.003 and P¼ 0.184, respectively) andTTR (P < 0.0001 and P ¼ 0.215, respectively; Fig. 1B;Supplementary Fig. S3B). The NLR also significantly corre-lated with TTR (P ¼ 0.007; Supplementary Fig. S3A). Uni-variate and multivariate analyses demonstrated that the SIIcorrelated was significantly prognostic OS (HR, 2.56; 95%CI, 1.17–5.76;P¼0.019) andTTR (HR, 2.32; 95%CI, 1.28–4.23; P¼ 0.006; Tables 2 and 3). The discrimination abilityof the SII, as assessedbyAUC,was 0.66 (95%CI, 0.53–0.78)and 0.67 (95% CI, 0.58–0.78) for OS and TTR (Fig. 1D)respectively, which was higher than other clinical indexes(Supplementary Fig. S2D).
Association of the SII with clinicopathologicparameters
In the training cohort, we found that patients with an SII� 330 were more likely to have liver cirrhosis (P ¼ 0.006),large tumor size (P < 0.001), presence of vascular invasion(P ¼ 0.020), high BCLC stage (P ¼ 0.002), and earlyrecurrence (P ¼ 0.015; Supplementary Table S1). NLR �5 was associated with elevated ALT (P¼ 0.047); PLR� 150was associated with liver cirrhosis (P ¼ 0.001) and tumorsize (P ¼ 0.009; Supplementary Table S2).
The relationship between the scores and clinicopatho-logic parameters for the validation cohort is shown inSupplementary Tables S1 and S2. An SII � 330 was asso-ciated with liver cirrhosis (P ¼ 0.016), poor tumor differ-entiation (P ¼ 0.021), tumor size >5 cm (P < 0.001), andearly recurrence (P < 0.001). NLR � 5 was associatedwith tumor size >5 cm (P ¼ 0.038) and vascular invasion(P ¼ 0.009). PLR �150 was associated with tumor size >5cm (P ¼ 0.021).
Prognostic Significance of SII in HCC
www.aacrjournals.org Clin Cancer Res; 20(23) December 1, 2014 6215
Research. on June 27, 2020. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2014; DOI: 10.1158/1078-0432.CCR-14-0442
CCR-14-0442; 13/2/2015; 2:45:36
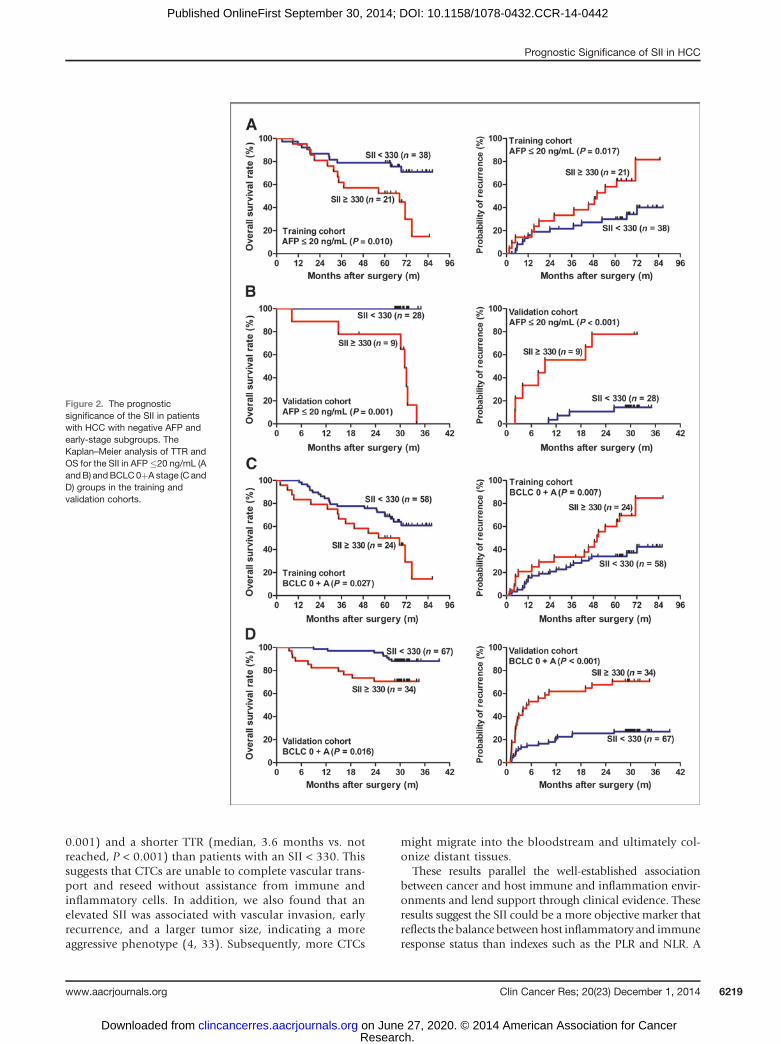
The prognostic significance of the SII in patients withHCC with negative AFP and early-stage subgroups
We investigated the prognostic significance of the SII inthe AFP-negative and early-stage subgroups in greater detail.We found that the SII score was significantly correlated withOS (P ¼ 0.010 and P ¼ 0.027 in AFP-negative and BCLC0þA subgroups of the training cohort, respectively) andTTR(P ¼ 0.017 and P ¼ 0.007 in AFP-negative and BCLC 0þAsubgroups of the training cohort, respectively; Fig. 2Aand C).
In the validation cohort, the prognostic significance forOSand TTRwasmaintained in the BCLC 0þA group (P¼ 0.016and P < 0.001, respectively, Fig. 2D). The SII score also
significantly correlated with OS and TTR in the AFP-negativegroup (P ¼ 0.001 and P < 0.001, respectively, Fig. 2B).
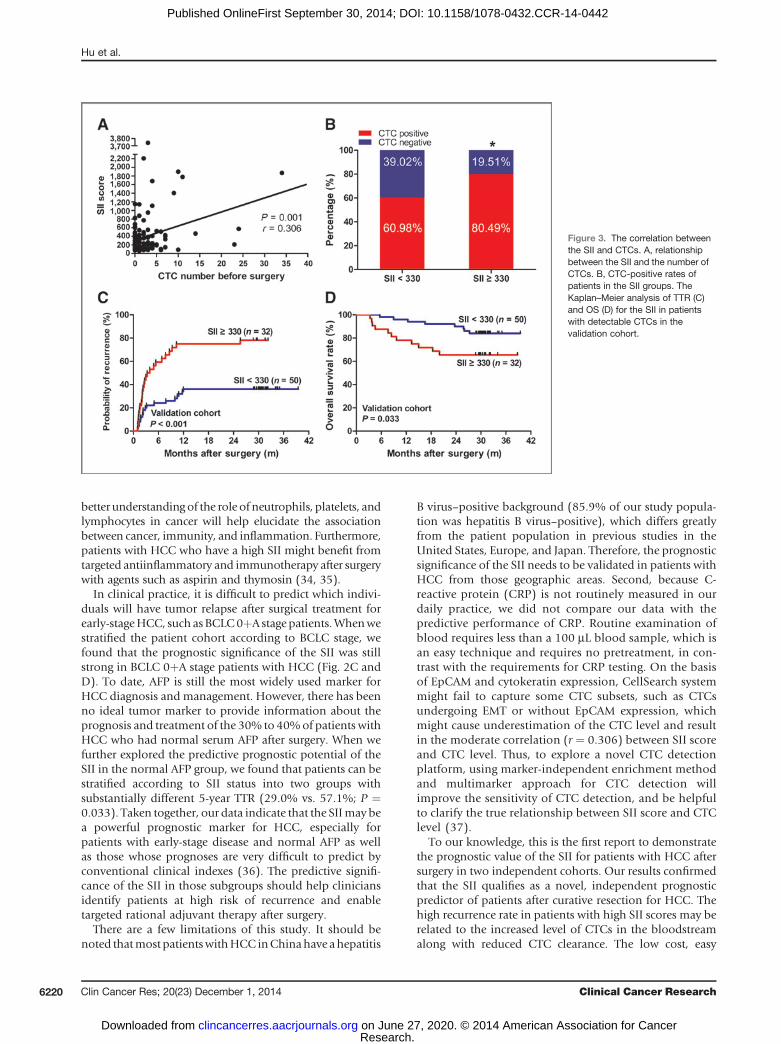
The correlation between the SII and CTCs and itsprognostic significance in patients with HCC who hadCTCs
The correlation between perioperative SII score and CTClevel was further investigated. Scatter plot analyses revealeda significant positive correlation between the SII and CTClevel (r ¼ 0.306; P ¼ 0.001, Fig. 3A). The level of CTCs wassignificantly higher in patients in the SII � 330 group thanthose in the SII<330group (1.71�0.34 vs. 4.37�1.04;P¼0.029, Fig. 3B).
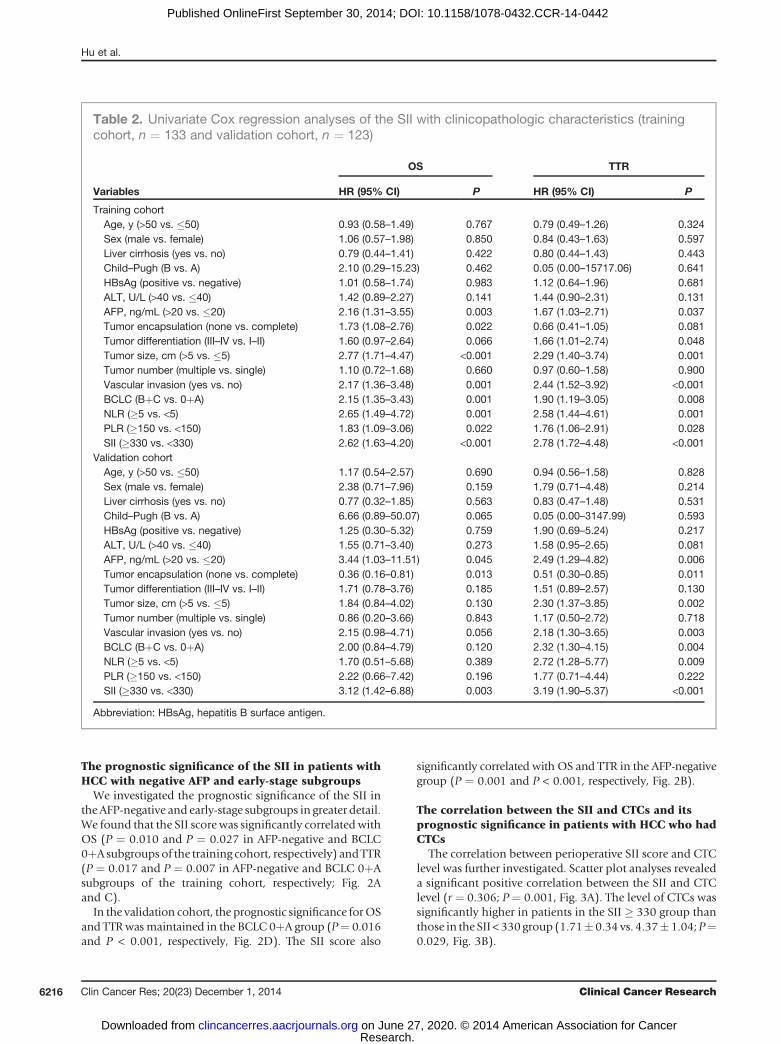
Table 2. Univariate Cox regression analyses of the SII with clinicopathologic characteristics (trainingcohort, n ¼ 133 and validation cohort, n ¼ 123)
OS TTR
Variables HR (95% CI) P HR (95% CI) P
Training cohortAge, y (>50 vs. �50) 0.93 (0.58–1.49) 0.767 0.79 (0.49–1.26) 0.324Sex (male vs. female) 1.06 (0.57–1.98) 0.850 0.84 (0.43–1.63) 0.597Liver cirrhosis (yes vs. no) 0.79 (0.44–1.41) 0.422 0.80 (0.44–1.43) 0.443Child–Pugh (B vs. A) 2.10 (0.29–15.23) 0.462 0.05 (0.00–15717.06) 0.641HBsAg (positive vs. negative) 1.01 (0.58–1.74) 0.983 1.12 (0.64–1.96) 0.681ALT, U/L (>40 vs. �40) 1.42 (0.89–2.27) 0.141 1.44 (0.90–2.31) 0.131AFP, ng/mL (>20 vs. �20) 2.16 (1.31–3.55) 0.003 1.67 (1.03–2.71) 0.037Tumor encapsulation (none vs. complete) 1.73 (1.08–2.76) 0.022 0.66 (0.41–1.05) 0.081Tumor differentiation (III–IV vs. I–II) 1.60 (0.97–2.64) 0.066 1.66 (1.01–2.74) 0.048Tumor size, cm (>5 vs. �5) 2.77 (1.71–4.47) <0.001 2.29 (1.40–3.74) 0.001Tumor number (multiple vs. single) 1.10 (0.72–1.68) 0.660 0.97 (0.60–1.58) 0.900Vascular invasion (yes vs. no) 2.17 (1.36–3.48) 0.001 2.44 (1.52–3.92) <0.001BCLC (BþC vs. 0þA) 2.15 (1.35–3.43) 0.001 1.90 (1.19–3.05) 0.008NLR (�5 vs. <5) 2.65 (1.49–4.72) 0.001 2.58 (1.44–4.61) 0.001PLR (�150 vs. <150) 1.83 (1.09–3.06) 0.022 1.76 (1.06–2.91) 0.028SII (�330 vs. <330) 2.62 (1.63–4.20) <0.001 2.78 (1.72–4.48) <0.001
Validation cohortAge, y (>50 vs. �50) 1.17 (0.54–2.57) 0.690 0.94 (0.56–1.58) 0.828Sex (male vs. female) 2.38 (0.71–7.96) 0.159 1.79 (0.71–4.48) 0.214Liver cirrhosis (yes vs. no) 0.77 (0.32–1.85) 0.563 0.83 (0.47–1.48) 0.531Child–Pugh (B vs. A) 6.66 (0.89–50.07) 0.065 0.05 (0.00–3147.99) 0.593HBsAg (positive vs. negative) 1.25 (0.30–5.32) 0.759 1.90 (0.69–5.24) 0.217ALT, U/L (>40 vs. �40) 1.55 (0.71–3.40) 0.273 1.58 (0.95–2.65) 0.081AFP, ng/mL (>20 vs. �20) 3.44 (1.03–11.51) 0.045 2.49 (1.29–4.82) 0.006Tumor encapsulation (none vs. complete) 0.36 (0.16–0.81) 0.013 0.51 (0.30–0.85) 0.011Tumor differentiation (III–IV vs. I–II) 1.71 (0.78–3.76) 0.185 1.51 (0.89–2.57) 0.130Tumor size, cm (>5 vs. �5) 1.84 (0.84–4.02) 0.130 2.30 (1.37–3.85) 0.002Tumor number (multiple vs. single) 0.86 (0.20–3.66) 0.843 1.17 (0.50–2.72) 0.718Vascular invasion (yes vs. no) 2.15 (0.98–4.71) 0.056 2.18 (1.30–3.65) 0.003BCLC (BþC vs. 0þA) 2.00 (0.84–4.79) 0.120 2.32 (1.30–4.15) 0.004NLR (�5 vs. <5) 1.70 (0.51–5.68) 0.389 2.72 (1.28–5.77) 0.009PLR (�150 vs. <150) 2.22 (0.66–7.42) 0.196 1.77 (0.71–4.44) 0.222SII (�330 vs. <330) 3.12 (1.42–6.88) 0.003 3.19 (1.90–5.37) <0.001
Abbreviation: HBsAg, hepatitis B surface antigen.
Hu et al.
Clin Cancer Res; 20(23) December 1, 2014 Clinical Cancer Research6216
Research. on June 27, 2020. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2014; DOI: 10.1158/1078-0432.CCR-14-0442
CCR-14-0442; 13/2/2015; 2:45:36
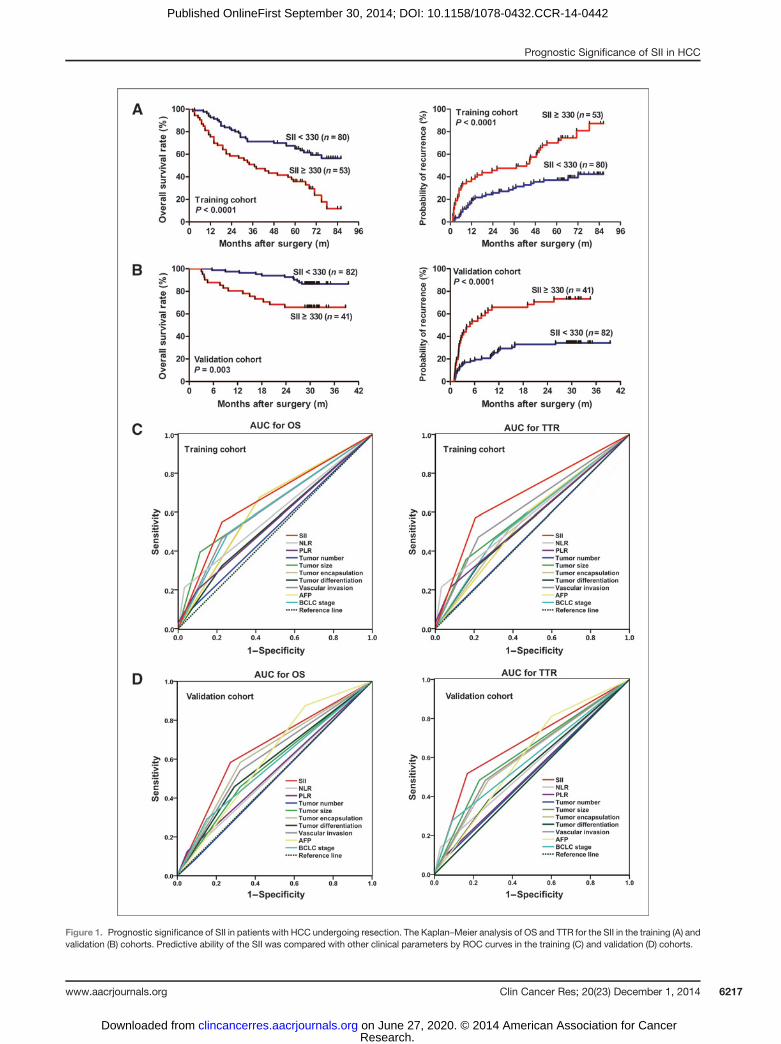
Figure 1. Prognostic significance of SII in patients with HCC undergoing resection. The Kaplan–Meier analysis of OS and TTR for the SII in the training (A) andvalidation (B) cohorts. Predictive ability of the SII was compared with other clinical parameters by ROC curves in the training (C) and validation (D) cohorts.
Prognostic Significance of SII in HCC
www.aacrjournals.org Clin Cancer Res; 20(23) December 1, 2014 6217
Research. on June 27, 2020. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2014; DOI: 10.1158/1078-0432.CCR-14-0442
CCR-14-0442; 13/2/2015; 2:49:6
In light of the close relationship between CTCs and theSII, we further explored the prognostic significance of the SIIin subgroups of patients presenting with CTCs. In patientswith detectable CTCs, patients with an SII� 330 had higherrecurrence rates (78.1% vs. 36.0%; P < 0.001) and a shorterTTR (median, 3.6 months vs. not reached; P < 0.001)compared with patients with SII < 330 (Fig. 3C). In termsofOS, we found that theOS rates were significantly lower inthe SII � 330 group than in the SII < 330 group (65.6% vs.84.0%; P ¼ 0.033, Fig. 3D).
DiscussionSeveral studies have shown the prognostic significance of
NLR, PLR, and percentage of lymphocytes in postsurgerypatients with HCC (26–28). In the present study, a novelimmune-inflammation–based prognostic score (SII) wasconstructed based on lymphocyte, neutrophil, and plateletcounts and was shown to be an independent predictor ofrecurrence and survival for patients with HCC after surgeryin two independent cohorts. Its prediction ability wasshown to be higher than that of the NLR, PLR, and otherconventional parameters such as BCLC staging, tumordifferentiation, and tumor number (Fig. 1C and D). Mean-while, the measure of SII is based on standard laboratorymeasurements of total platelet, neutrophil, and lymphocytecounts, which are routinely performed in the clinical set-ting. Thus, there is a potential for the SII to be used as amarker for tumor recurrence and treatment response sur-veillance, which might provide a powerful test enabling
accurate and early decision making to tailor the mosteffective therapy according to characteristics of individualtumors.
As an integrated indicator based on peripheral lympho-cyte, neutrophil, andplatelets counts, thepredictive valueofthe SII for tumor recurrence and metastasis might be elu-cidated by the function of the three kinds of cells, and thetheir close relationshipwith CTCs, which play an importantrole in the initiation of recurrence and metastases aftersurgery (29–31). The patients with an elevated preoperativeSII usually have thrombocytopenia, neutrophilia, or lym-phopenia, suggesting an elevated inflammatory status andweak immune response in patients. Recent evidence indi-cates that neutrophils can enhance cancer cell invasion,proliferation, and metastasis as well as assist cancer cellswith evading immune surveillance (16, 32). Platelets couldinteract with tumor cells and facilitate tumor cell survivaland metastasis via different mechanisms (8, 9). Activated Tcells and other lymphocytes play a fundamental role in cell-mediated immunologic destruction of host cancer cells.Meanwhile, elevated levels of cytokines released by lym-phocytes, such as IFN-g and TNF-a, that promote tumorcontrol have been associated with an improved prognosisfor patients withmany different cancers. All of these mightcause more tumor cells disseminating into the circulation,escaping immune surveillance, and finally increasing theperipheral CTC level. When analyzed only the subgroupof patients with detectable CTCs, patients with an SII �330 had a higher recurrence rate (78.1% vs. 36.0%, P <
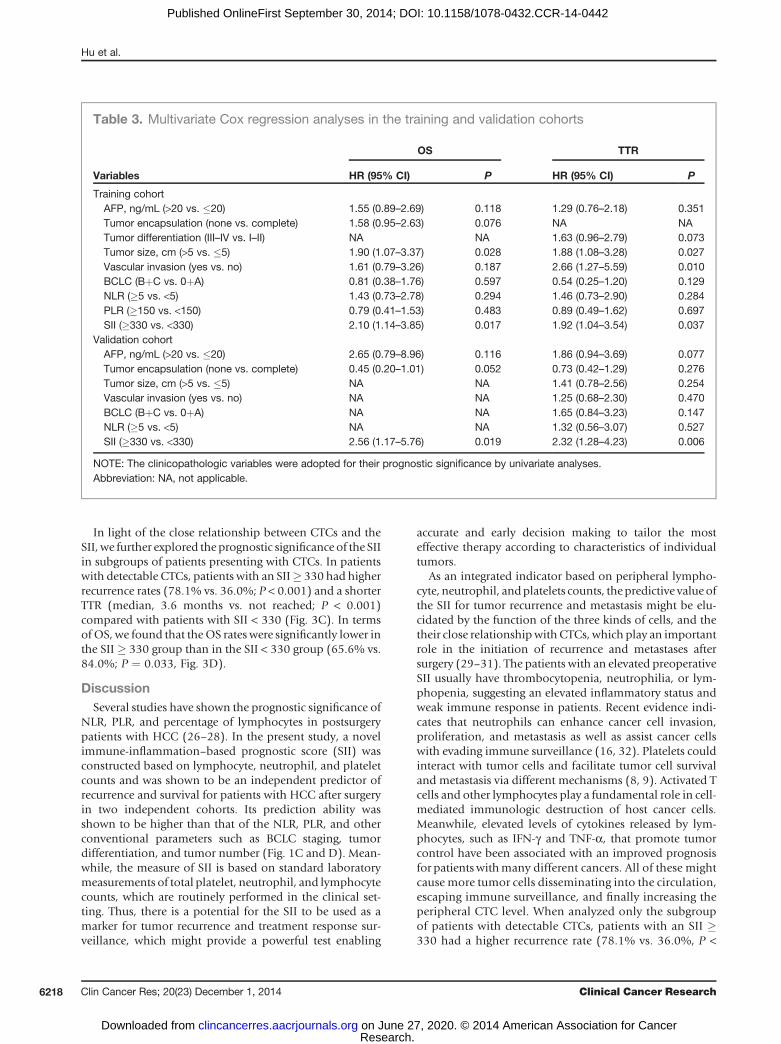
Table 3. Multivariate Cox regression analyses in the training and validation cohorts
OS TTR
Variables HR (95% CI) P HR (95% CI) P
Training cohortAFP, ng/mL (>20 vs. �20) 1.55 (0.89–2.69) 0.118 1.29 (0.76–2.18) 0.351Tumor encapsulation (none vs. complete) 1.58 (0.95–2.63) 0.076 NA NATumor differentiation (III–IV vs. I–II) NA NA 1.63 (0.96–2.79) 0.073Tumor size, cm (>5 vs. �5) 1.90 (1.07–3.37) 0.028 1.88 (1.08–3.28) 0.027Vascular invasion (yes vs. no) 1.61 (0.79–3.26) 0.187 2.66 (1.27–5.59) 0.010BCLC (BþC vs. 0þA) 0.81 (0.38–1.76) 0.597 0.54 (0.25–1.20) 0.129NLR (�5 vs. <5) 1.43 (0.73–2.78) 0.294 1.46 (0.73–2.90) 0.284PLR (�150 vs. <150) 0.79 (0.41–1.53) 0.483 0.89 (0.49–1.62) 0.697SII (�330 vs. <330) 2.10 (1.14–3.85) 0.017 1.92 (1.04–3.54) 0.037
Validation cohortAFP, ng/mL (>20 vs. �20) 2.65 (0.79–8.96) 0.116 1.86 (0.94–3.69) 0.077Tumor encapsulation (none vs. complete) 0.45 (0.20–1.01) 0.052 0.73 (0.42–1.29) 0.276Tumor size, cm (>5 vs. �5) NA NA 1.41 (0.78–2.56) 0.254Vascular invasion (yes vs. no) NA NA 1.25 (0.68–2.30) 0.470BCLC (BþC vs. 0þA) NA NA 1.65 (0.84–3.23) 0.147NLR (�5 vs. <5) NA NA 1.32 (0.56–3.07) 0.527SII (�330 vs. <330) 2.56 (1.17–5.76) 0.019 2.32 (1.28–4.23) 0.006
NOTE: The clinicopathologic variables were adopted for their prognostic significance by univariate analyses.Abbreviation: NA, not applicable.
Hu et al.
Clin Cancer Res; 20(23) December 1, 2014 Clinical Cancer Research6218
Research. on June 27, 2020. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2014; DOI: 10.1158/1078-0432.CCR-14-0442
CCR-14-0442; 13/2/2015; 2:49:6
0.001) and a shorter TTR (median, 3.6 months vs. notreached, P < 0.001) than patients with an SII < 330. Thissuggests that CTCs are unable to complete vascular trans-port and reseed without assistance from immune andinflammatory cells. In addition, we also found that anelevated SII was associated with vascular invasion, earlyrecurrence, and a larger tumor size, indicating a moreaggressive phenotype (4, 33). Subsequently, more CTCs
might migrate into the bloodstream and ultimately col-onize distant tissues.
These results parallel the well-established associationbetween cancer and host immune and inflammation envir-onments and lend support through clinical evidence. Theseresults suggest the SII could be a more objective marker thatreflects the balance between host inflammatory and immuneresponse status than indexes such as the PLR and NLR. A
Figure 2. The prognosticsignificance of the SII in patientswith HCC with negative AFP andearly-stage subgroups. TheKaplan–Meier analysis of TTR andOS for the SII in AFP�20 ng/mL (AandB) andBCLC0þA stage (C andD) groups in the training andvalidation cohorts.
Prognostic Significance of SII in HCC
www.aacrjournals.org Clin Cancer Res; 20(23) December 1, 2014 6219
Research. on June 27, 2020. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2014; DOI: 10.1158/1078-0432.CCR-14-0442
CCR-14-0442; 13/2/2015; 2:51:43
better understanding of the role of neutrophils, platelets, andlymphocytes in cancer will help elucidate the associationbetween cancer, immunity, and inflammation. Furthermore,patients with HCC who have a high SII might benefit fromtargeted antiinflammatory and immunotherapy after surgerywith agents such as aspirin and thymosin (34, 35).
In clinical practice, it is difficult to predict which indivi-duals will have tumor relapse after surgical treatment forearly-stageHCC, such asBCLC0þA stage patients.Whenwestratified the patient cohort according to BCLC stage, wefound that the prognostic significance of the SII was stillstrong in BCLC 0þA stage patients with HCC (Fig. 2C andD). To date, AFP is still the most widely used marker forHCC diagnosis and management. However, there has beenno ideal tumor marker to provide information about theprognosis and treatment of the 30% to 40%of patients withHCC who had normal serum AFP after surgery. When wefurther explored the predictive prognostic potential of theSII in the normal AFP group, we found that patients can bestratified according to SII status into two groups withsubstantially different 5-year TTR (29.0% vs. 57.1%; P ¼0.033). Taken together, our data indicate that the SIImay bea powerful prognostic marker for HCC, especially forpatients with early-stage disease and normal AFP as wellas those whose prognoses are very difficult to predict byconventional clinical indexes (36). The predictive signifi-cance of the SII in those subgroups should help cliniciansidentify patients at high risk of recurrence and enabletargeted rational adjuvant therapy after surgery.
There are a few limitations of this study. It should benoted thatmost patientswithHCC inChinahave ahepatitis
B virus–positive background (85.9% of our study popula-tion was hepatitis B virus–positive), which differs greatlyfrom the patient population in previous studies in theUnited States, Europe, and Japan. Therefore, the prognosticsignificance of the SII needs to be validated in patients withHCC from those geographic areas. Second, because C-reactive protein (CRP) is not routinely measured in ourdaily practice, we did not compare our data with thepredictive performance of CRP. Routine examination ofblood requires less than a 100 mL blood sample, which isan easy technique and requires no pretreatment, in con-trast with the requirements for CRP testing. On the basisof EpCAM and cytokeratin expression, CellSearch systemmight fail to capture some CTC subsets, such as CTCsundergoing EMT or without EpCAM expression, whichmight cause underestimation of the CTC level and resultin the moderate correlation (r ¼ 0.306) between SII scoreand CTC level. Thus, to explore a novel CTC detectionplatform, using marker-independent enrichment methodand multimarker approach for CTC detection willimprove the sensitivity of CTC detection, and be helpfulto clarify the true relationship between SII score and CTClevel (37).
To our knowledge, this is the first report to demonstratethe prognostic value of the SII for patients with HCC aftersurgery in two independent cohorts. Our results confirmedthat the SII qualifies as a novel, independent prognosticpredictor of patients after curative resection for HCC. Thehigh recurrence rate in patients with high SII scores may berelated to the increased level of CTCs in the bloodstreamalong with reduced CTC clearance. The low cost, easy
Figure 3. The correlation betweenthe SII and CTCs. A, relationshipbetween the SII and the number ofCTCs. B, CTC-positive rates ofpatients in the SII groups. TheKaplan–Meier analysis of TTR (C)and OS (D) for the SII in patientswith detectable CTCs in thevalidation cohort.
Clin Cancer Res; 20(23) December 1, 2014 Clinical Cancer Research6220
Hu et al.
Research. on June 27, 2020. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2014; DOI: 10.1158/1078-0432.CCR-14-0442
CCR-14-0442; 13/2/2015; 2:52:58
determination, and reproducibility of a full blood countmake the SII a promising tool for assessing HCC prognosisin future clinical practice.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: B. Hu, X.-R. Yang, Y. Xu, Y.-F. Sun, J. FanDevelopment of methodology: B. Hu, X.-R. Yang, C. SunAcquisitionofdata (provided animals, acquired andmanagedpatients,provided facilities, etc.): B.Hu, Y.-F. Sun, C. Sun,W.Guo, S.-J. Qiu, J. ZhouAnalysis and interpretation of data (e.g., statistical analysis, biosta-tistics, computational analysis): B. Hu, X.-R. Yang, C. Sun, W.-M. WangWriting, review, and/or revision of themanuscript: B. Hu, X.-R. Yang, C.SunAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): X. Zhang, S.-J. Qiu, J. FanStudy supervision: X.-R. Yang, Y. Xu, J. Fan
AcknowledgmentsThe authors thank the participating patients for the source of clinical
blood samples.
Grant SupportThis study was supported by grants from the Major Program of National
Natural Science Foundation of China (81030038), theNational Key Sci-TechProject (2012ZX10002011-002, 2012ZX10002013-005, 2012ZX10002-016, and 2013ZX10002010), the National Natural Science Foundation ofChina (81000927, 81071661, and 81172277), the Research Fund for theDoctoral Program of Higher Education of China (20100071120064), andthe Shanghai New Project for Excellent Youth (XYQ2011020).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received February 22, 2014; revised September 1, 2014; accepted Sep-tember 3, 2014; published OnlineFirst September 30, 2014.
References1. Befeler AS, Di Bisceglie AM. Hepatocellular carcinoma: diagnosis and
treatment. Gastroenterology 2002;122:1609–19.2. JemalA,BrayF,CenterMM,Ferlay J,WardE, FormanD.Global cancer
statistics. CA Cancer J Clin 2011;61:69–90.3. Cha C, Fong Y, Jarnagin WR, Blumgart LH, DeMatteo RP. Predictors
and patterns of recurrence after resection of hepatocellular carcinoma.J Am CollSurg 2003;197:753–8.
4. Chaffer CL, Weinberg RA. A perspective on cancer cell metastasis.Science 2011;331:1559–64.
5. Sun YF, Xu Y, Yang XR,GuoW, Zhang X,Qiu SJ, et al. Circulating stemcell-like epithelial cell adhesion molecule-positive tumor cells indicatepoor prognosis of hepatocellular carcinoma after curative resection.Hepatology 2013;57:1458–68.
6. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation.Cell 2011;144:646–74.
7. Placke T, Salih HR, Kopp HG. GITR ligand provided by thrombo-poietic cells inhibits NK cell antitumor activity. J Immunol 2012;189:154–60.
8. LabelleM,BegumS,HynesRO.Direct signaling between platelets andcancer cells induces an epithelial-mesenchymal-like transition andpromotes metastasis. Cancer Cell 2011;20:576–90.
9. Schumacher D, Strilic B, Sivaraj KK, Wettschureck N, Offermanns S.Platelet-derived nucleotides promote tumor-cell transendothelialmigration and metastasis via P2Y2 receptor. Cancer Cell 2013;24:130–7.
10. Gil-Bernab�e AM, Ferjancic S, Tlalka M, Zhao L, Allen PD, Im JH, et al.Recruitment of monocytes/macrophages by tissue factor-mediatedcoagulation is essential for metastatic cell survival and premetastaticniche establishment in mice. Blood 2012;119:3164–75.
11. Stotz M, Gerger A, Eisner F, Szkandera J, Loibner H, Ress AL, et al.Increased neutrophil-lymphocyte ratio is a poor prognostic factor inpatients with primary operable and inoperable pancreatic cancer. Br JCancer 2013;109:416–21.
12. Halazun KJ, Hardy MA, Rana AA, Woodland DC 4th, Luyten EJ,Mahadev S, et al. Negative impact of neutrophil-lymphocyte ratio onoutcome after liver transplantation for hepatocellular carcinoma. AnnSurg 2009;250:141–51.
13. Dan J, Zhang Y, Peng Z, Huang J, Gao H, Xu L, et al. Postoperativeneutrophil-to-lymphocyte ratio change predicts survival of patientswith small hepatocellular carcinoma undergoing radiofrequency abla-tion. PLoS One 2013;8:e58184.
14. LazovaR, LabergeGS,Duvall E, SpoelstraN, KlumpV,SznolM, et al. Amelanoma brain metastasis with a donor-patient hybrid genomefollowing bone marrow transplantation: first evidence for fusion inhuman cancer. PLoS One 2013;8:e66731.
15. Cools-Lartigue J, Spicer J, McDonald B, Gowing S, Chow S, GianniasB, et al. Neutrophil extracellular traps sequester circulating tumor cellsand promote metastasis. J Clin Invest 2013;123:3446–58.
16. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflamma-tion. Nature 2008;454:436–44.
17. Kobayashi N, Usui S, Kikuchi S, Goto Y, Sakai M, Onizuka M, et al.Preoperative lymphocyte count is an independent prognostic factor innode-negative non-small cell lung cancer. LungCancer 2012;75:223–7.
18. McMillan DC. Systemic inflammation, nutritional status and survivalin patients with cancer. Curr Opin Clin Nutr Metab Care 2009;12:223–6.
19. Gomez D, Farid S, Malik HZ, Young AL, Toogood GJ, Lodge JP, et al.Preoperative neutrophil-to-lymphocyte ratio as a prognostic predictorafter curative resection for hepatocellular carcinoma. World J Surg2008;32:1757–62.
20. Yang XR, Xu Y, Yu B, Zhou J, Li JC, Qiu SJ, et al. CD24 is a novelpredictor for poor prognosis of hepatocellular carcinoma after surgery.Clin Cancer Res 2009;15:5518–27.
21. Bruix J, Llovet JM. Prognostic prediction and treatment strategy inhepatocellular carcinoma. Hepatology 2002;35:519–24.
22. Wittekind C. Pitfalls in the classification of liver tumors. Pathologe2006;27:289–93.
23. Yang XR, Xu Y, Shi GM, Fan J, Zhou J, Ji Y, et al. Cytokeratin 10 andcytokeratin 19: predictive markers for poor prognosis in hepatocellularcarcinoma patients after curative resection. Clin Cancer Res 2008;14:3850–9.
24. CampRL, Dolled-FilhartM, RimmDL. X-tile: a newbio-informatics toolfor biomarker assessment andoutcome-based cut-point optimization.Clin Cancer Res 2004;10:7252–9.
25. Pierga JY, Bidard FC,Mathiot C, Brain E, Delaloge S, Giachetti S, et al.Circulating tumor cell detection predicts early metastatic relapse afterneoadjuvant chemotherapy in large operable and locally advancedbreast cancer in a phase II randomized trial. Clin Cancer Res2008;14:7004–10.
26. Kinoshita A, Onoda H, Imai N, Iwaku A, Oishi M, Fushiya N, et al.Comparison of the prognostic value of inflammation-basedprognosticscores in patients with hepatocellular carcinoma. Br J Cancer2012;107:988–93.
27. Mano Y, Shirabe K, Yamashita Y, Harimoto N, Tsujita E, Takeishi K,et al. Preoperative neutrophil-to-lymphocyte ratio is a predictor ofsurvival after hepatectomy for hepatocellular carcinoma: a retro-spective analysis. Ann Surg 2013;258:301–5.
28. Li C, Wen TF, Yan LN, Li B, Yang JY, Xu MQ, et al. Scoring selectioncriteria including total tumour volume and pretransplant percentage oflymphocytes to predict recurrence of hepatocellular carcinoma afterliver transplantation. PLoS One 2013;8:e72235.
29. Lucci A, Hall CS, Lodhi AK, Bhattacharyya A, Anderson AE, Xiao L,et al. Circulating tumour cells in non-metastatic breast cancer: aprospective study. Lancet Oncol 2012;13:688–95.
30. Fan ZC, Yan J, Liu GD, Tan XY, Weng XF, Wu WZ, et al. Real-timemonitoring of rare circulating hepatocellular carcinoma cells in an
www.aacrjournals.org Clin Cancer Res; 20(23) December 1, 2014 6221
Prognostic Significance of SII in HCC
Research. on June 27, 2020. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2014; DOI: 10.1158/1078-0432.CCR-14-0442

CCR-14-0442; 13/2/2015; 2:52:59
orthotopic model by in vivo flow cytometry assesses resection onmetastasis. Cancer Res 2012;72:2683–91.
31. Karakousis G, YangR, XuX.Circulatingmelanoma cells as a predictivebiomarker. J Invest Dermatol 2013;133:1460–2.
32. Mantovani A, Cassatella MA, Costantini C, Jaillon S. Neutrophils in theactivation and regulation of innate and adaptive immunity. Nat RevImmunol 2011;11:519–31.
33. Schreiber RD, Old LJ, Smyth MJ. Cancer immunoediting: integratingimmunity's roles in cancer suppression and promotion. Science2011;331:1565–70.
34. Sahasrabuddhe VV, Gunja MZ, Graubard BI, Trabert B, Schwartz LM,Park Y, et al. Nonsteroidal anti-inflammatory drug use, chronic liver
disease, and hepatocellular carcinoma. J Natl Cancer Inst 2012;104:1808–14.
35. Sjogren MH. Thymalfasin: an immune system enhancer for thetreatment of liver disease. J Gastroenterol Hepatol 2004;19:S69–72.
36. Qin LX, Tang ZY. Recent progress in predictive biomarkers for met-astatic recurrence of human hepatocellular carcinoma: a review of theliterature. J Cancer Res Clin Oncol 2004;130:497–513.
37. Gervasoni A, Sandri MT, Nascimbeni R, Zorzino L, Cassatella MC,Baglioni L, et al.Comparisonof threedistinctmethods for thedetectionof circulating tumor cells in colorectal cancer patients. Oncol Rep2011;25:1669–703.
Clin Cancer Res; 20(23) December 1, 2014 Clinical Cancer Research6222
Hu et al.
Research. on June 27, 2020. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2014; DOI: 10.1158/1078-0432.CCR-14-0442
2014;20:6212-6222. Published OnlineFirst September 30, 2014.Clin Cancer Res Bo Hu, Xin-Rong Yang, Yang Xu, et al. CarcinomaPatients after Curative Resection for Hepatocellular Systemic Immune-Inflammation Index Predicts Prognosis of
Updated version
10.1158/1078-0432.CCR-14-0442doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2014/10/01/1078-0432.CCR-14-0442.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/20/23/6212.full#ref-list-1
This article cites 37 articles, 9 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/20/23/6212.full#related-urls
This article has been cited by 4 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
SubscriptionsReprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://clincancerres.aacrjournals.org/content/20/23/6212To request permission to re-use all or part of this article, use this link
Research. on June 27, 2020. © 2014 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2014; DOI: 10.1158/1078-0432.CCR-14-0442









![CSF-1 Overexpression Predicts Poor Prognosis in Upper ...downloads.hindawi.com/journals/dm/2019/2724948.pdf · linked to a poor prognosis in pancreatic cancer [26], prostate cancer](https://img.pdfslide.net/doc/110x75/5ed9b1e3385b4c58025dce96/csf-1-overexpression-predicts-poor-prognosis-in-upper-linked-to-a-poor-prognosis.jpg)