Embed Size (px)
Citation preview
Teaching toolkit formedical studentsAshley Newton and Lucie Wright, The Junior Association for the Study of MedicalEducation, Edinburgh, UK
SUMMARYBackground: From teachingjuniors and peers to educatingpatients, it is imperative for alldoctors to have basic core teachingskills. The Junior Association forthe Study of Medical Education(JASME) felt that a short course inthe fundamentals of teachingwould be well received by students.Context: This article shares thelessons from a one-day teachingcourse aimed at senior medicalstudents. Qualitative feedbackhelped decide which aspects ofthe course were most valued.Intervention: The course waspiloted in London. It combined
interactive plenary sessionson teaching theory withpractical teaching sessions.Each student taught a smallgroup of others a basic clinicalskill, and the student teacherthen received extensive feedbackfrom their peers and an experi-enced clinician with a specialinterest in medical education.There was an opportunity tore-teach part of the skill afterhaving taken the feedback onboard.Implications: Studentscompleted questionnaires at thestart and end of the day toascertain their expectations of
the course and what theyfound most useful. Expectationscan be grouped into threemain areas: students wanted toimprove their teaching skills;gain teaching experience; andreceive feedback on their teach-ing. The most valuable part ofthe course was being able topractise teaching and receivefeedback. Keywords used todescribe the feedback included‘individual’, ‘valuable’, ‘construc-tive’, ‘instant’ and ‘in depth’. Bycontinuing to run similar work-shops we hope that we canfurther encourage the teachersof tomorrow.
It is imperativefor all doctorsto have basiccore teaching
skills
Developingnew teachers
254 � Blackwell Publishing Ltd 2011. THE CLINICAL TEACHER 2011; 8: 254–257
INTRODUCTION
When preparing seniormedical students for theirwork as foundation doc-
tors, much attention is given toequipping them with skills that willhelp them to contribute effectivelyto the clinical environment. Thereappears to be less emphasis placedon their responsibility to develop‘the skills and practices of a com-petent teacher’.1 From teachingjuniors and peers to educatingpatients, it is imperative for alldoctors to have basic core teachingskills. The Junior Association forthe Study of Medical Education(JASME) felt that a short course inthe fundaments of teaching wouldbe well received by students.
JASME is a special interestgroup of The Association for theStudy of Medical Education(ASME). It is run by a group of sixmedical students from across theUK with the support of the ASMEexecutive.
The pilot workshop was run inLondon and it gave a valuableinsight into how students feelabout their role as teachers, andhighlighted the aspects of the daythat they found most useful. It isthese lessons that will be sharedin this article.
Since the pilot workshop, thecourse has been further developedand repeated at further venues inan abbreviated format.
CONTEXT
Existing teaching coursesThere are certainly many coursesin existence at institutions acrossthe UK with the aim of improvingteaching skills, from the funda-mental ‘Teaching the Teachers’course at the University of Shef-field to the rigorous two-dayTeaching Improvement ProjectSystem (TIPS) course used to trainpeer tutors in interdisciplinaryPeer Assisted Learning (PAL).2,3
This present course differed be-
cause it was aimed specifically atstudents, and was designed as acomplete introduction to teach-ing in a clinical setting andassumed no prior experience.
The role of foundation yeardoctors as clinical teachersThe foundation years are theperfect opportunity to harnessenthusiasm and build the confi-dence of new clinical teachers.Many foundation year doctors maybe apprehensive about teachingas they feel that they have not yetbuilt enough of a knowledge base,when in fact it has been demon-strated that in some situations(particularly when teaching clini-cal skills) medical students can bemore effective than experiencedclinicians.4
When should we ‘train’ futureclinical teachers?This workshop was aimed primarilyat final year medical students, aswe feel that the later years of themedical degree is when thisworkshop would be of most bene-fit. The issue of the timing ofwhen to teach teaching skills is animportant one, as being confidentin teaching can have an effect onhow students will behave whenconfronted with teaching oppor-tunities during the foundationyears. One study has focused onthis very issue, trying to determinewhether early training andexperience in teaching influencefoundation doctors’ perception oftheir teaching role, and theirinvolvement in teaching in the
early years of their careers.5
Interestingly, the study high-lighted that doctors who hadexperience of teaching as under-graduates described feeling asense of entitlement to teach,even as foundation doctors, andmoreover a confidence to seek outlearning opportunities.
Description of the courseThe ‘JASME Teaching Toolkit forMedical Students’ was a one-dayclinical teaching course designedto improve students’ teachingskills and equip them with a basicunderstanding of how to lead ateaching session in a clinicalcontext.
Basic theoryThe workshop began with a seriesof interactive plenary sessions.They covered the backgroundtheory behind a variety of teach-ing practices commonly employedin the clinical setting. Throughthe use of case studies, studentswere encouraged to discuss therole of teaching in medicine, theimportance of professionalism,and varying approaches to feed-back. Experienced medical educa-tors facilitated the session tooptimise the exchange of ideasand encourage participation. Anexample of a professionalism casestudy is shown in Box 1.
Factors that impact on learningAn important part of the coursewas to highlight that once stu-dents are clinicians, they may becalled on to teach in a variety of
[This course]was designed asa completeintroduction toteaching in aclinical setting
� Blackwell Publishing Ltd 2011. THE CLINICAL TEACHER 2011; 8: 254–257 255
contexts. As a result they need tohave a certain level of adaptabil-ity, depending on where and whomthey are teaching. To furtherreflect on this point, everyone wasasked to write down factors thatcould affect learning. Theydiscussed the various factors to tryto identify ways in which theteacher can overcome the mostcommon obstructions to learning.
Students were then able tocompare their ideas with modelsfor learning and teaching clinicalskills such as Gagne’s instruc-tional events.6 Many studentswere impressed to see that theyhad identified all of the keyaspects of the theoretical modelfrom their own discussions insmall groups.
Teaching a clinical skillStudents were divided into fivegroups, each of which was allo-cated a different clinical skill thatthey would later teach. They weregiven an hour to discuss the skillwith their group and debate theapproaches to teaching it. Theclinical skills used are shown inBox 2. After lunch the groups weremixed so that each member had adifferent clinical skill to teach therest of the group. An experiencedclinician with a special interest inteaching and medical educationfacilitated every group. Eachmember of the group was given10 minutes to teach the skill, fol-lowed by 15 minutes of writtenand verbal feedback from theirpeers, with an opportunity to re-teach sections implementing therecommendations made. The for-
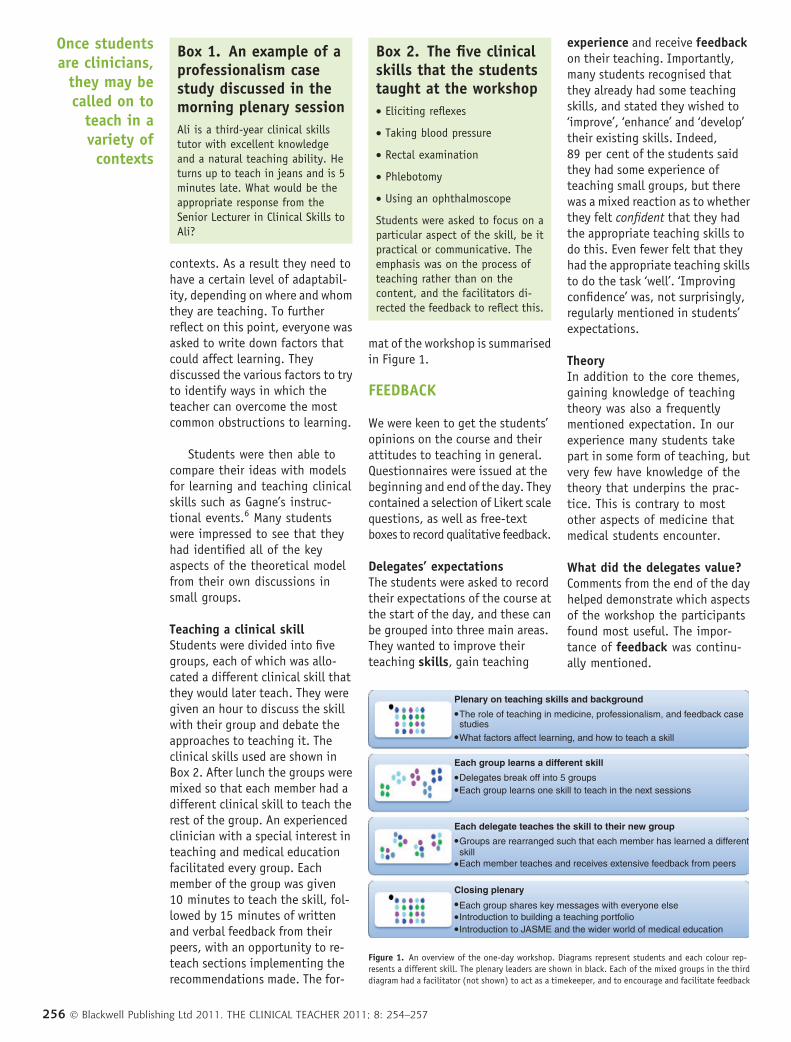
mat of the workshop is summarisedin Figure 1.
FEEDBACK
We were keen to get the students’opinions on the course and theirattitudes to teaching in general.Questionnaires were issued at thebeginning and end of the day. Theycontained a selection of Likert scalequestions, as well as free-textboxes to record qualitative feedback.
Delegates’ expectationsThe students were asked to recordtheir expectations of the course atthe start of the day, and these canbe grouped into three main areas.They wanted to improve theirteaching skills, gain teaching
experience and receive feedbackon their teaching. Importantly,many students recognised thatthey already had some teachingskills, and stated they wished to‘improve’, ‘enhance’ and ‘develop’their existing skills. Indeed,89 per cent of the students saidthey had some experience ofteaching small groups, but therewas a mixed reaction as to whetherthey felt confident that they hadthe appropriate teaching skills todo this. Even fewer felt that theyhad the appropriate teaching skillsto do the task ‘well’. ‘Improvingconfidence’ was, not surprisingly,regularly mentioned in students’expectations.
TheoryIn addition to the core themes,gaining knowledge of teachingtheory was also a frequentlymentioned expectation. In ourexperience many students takepart in some form of teaching, butvery few have knowledge of thetheory that underpins the prac-tice. This is contrary to mostother aspects of medicine thatmedical students encounter.
What did the delegates value?Comments from the end of the dayhelped demonstrate which aspectsof the workshop the participantsfound most useful. The impor-tance of feedback was continu-ally mentioned.
Box 1. An example of aprofessionalism casestudy discussed in themorning plenary session
Ali is a third-year clinical skillstutor with excellent knowledgeand a natural teaching ability. Heturns up to teach in jeans and is 5minutes late. What would be theappropriate response from theSenior Lecturer in Clinical Skills toAli?
Box 2. The five clinicalskills that the studentstaught at the workshop
• Eliciting reflexes
• Taking blood pressure
• Rectal examination
• Phlebotomy
• Using an ophthalmoscope
Students were asked to focus on aparticular aspect of the skill, be itpractical or communicative. Theemphasis was on the process ofteaching rather than on thecontent, and the facilitators di-rected the feedback to reflect this.
Plenary on teaching skills and background
Each group learns a different skill
Each delegate teaches the skill to their new group
Closing plenary
The role of teaching in medicine, professionalism, and feedback case
What factors affect learning, and how to teach a skill
studies
skill
Each group shares key messages with everyone elseIntroduction to building a teaching portfolioIntroduction to JASME and the wider world of medical education
Delegates break off into 5 groupsEach group learns one skill to teach in the next sessions
Each member teaches and receives extensive feedback from peers
Groups are rearranged such that each member has learned a different
Figure 1. An overview of the one-day workshop. Diagrams represent students and each colour rep-resents a different skill. The plenary leaders are shown in black. Each of the mixed groups in the third
diagram had a facilitator (not shown) to act as a timekeeper, and to encourage and facilitate feedback
Once studentsare clinicians,
they may becalled on to
teach in avariety ofcontexts
256 � Blackwell Publishing Ltd 2011. THE CLINICAL TEACHER 2011; 8: 254–257

Attendees were asked whatthey found most useful about thecourse:
I found it useful seeing mypeers teach and learningfrom them; the feedback wasmagnificent.
The best thing was theforum to try out teachingskills and receive construc-tive, useful feedback fromboth peers and facilitators.
Students highlighted what inparticular was useful about thefeedback they had received. Key-words used to describe the feed-back included ‘individual’,‘valuable’, ‘constructive’, ‘instant’and ‘in-depth’. The combination offeedback from peers and experi-enced tutors was also emphasised.
In-depth written feedbackfrom a facilitator and peers.
Outline about medicaleducation and the relevanceof teaching in medicine.
Our facilitator providedgreat depth to feedbackand introduced subtlesuggestions to perfect ourskills.
Another theme was recogni-tion of the importance of thetheory that underpins teaching.Comments such as ‘educationaltheory was useful background’were common.
FINAL REMARKS
In an era where it has become ararity to be in a small teaching
group, the strength of this work-shop lies in its ability to offerstudents individualised andin-depth feedback on theirteaching skills.
Above all, what the workshopachieved is giving a handful ofstudents confidence in their abil-ity as clinical teachers. Althoughit is a small intervention, it maywell have acted as a trigger andprompted some to consider theirfuture roles as teachers. We hopethat for the students attendingthe workshop it is just thebeginning of many years of activeand effective clinical teaching. Bycontinuing to run similarworkshops we hope that we canfurther encourage the teachers oftomorrow.
REFERENCES
1. General Medical Council. Tomorrow’s
Doctors. 2009. Available at http://
www.gmc-uk.org/education/under
graduate/tomorrows_doctors_
2009_responsibilities_doctors.asp.
Accessed on 26 January 2011.
2. Mackinnon R, Haque A, Stark S. Peer
teaching: by students for students.
A student-led initiative. Clin Teach
2009;6:245–248.
3. Gill D, Parker C, Spooner M, Thomas M,
Ambrose K, Richardson J. Tomorrow’s
Doctors and Nurses: Peer assisted
learning. Clin Teach 2006;3:13–18.
4. Graham K, Burke JM, Field M. Under-
graduate rheumatology: can peer-
assisted learning by medical students
deliver equivalent training to that
provided by specialist staff? Rheuma-
tology 2008;47:652–655.
5. Gill D, Richardson J, Parker C.
Tomorrow’s teachers: impact of
teaching in the undergraduate years.
Clin Teach 2008;5:49–55.
6. O’Connor HM. Training undergraduate
medical students in procedural skills.
Emerg Med (Fremantle). 2002;14:
131–135.
Corresponding author’s contact details: Ashley Newton, c ⁄ o ASME, 12 Queen Street, Edinburgh EH2 1SE UK. E-mail: [email protected]
Funding: None.
Conflict of interest: Both authors were members of the JASME Executive Committee at the time of the workshop, and continue to serve
at the time of article submission.
Ethical approval: Formal ethics approval was not sought for this voluntary, supplementary teaching intervention.
The workshopmay well haveprompted somestudents toconsider theirfuture roles asteachers
� Blackwell Publishing Ltd 2011. THE CLINICAL TEACHER 2011; 8: 254–257 257



















![ToolKit for Teaching Beginners[1]](https://img.pdfslide.net/doc/110x75/577d26331a28ab4e1ea0873c/toolkit-for-teaching-beginners1.jpg)









