Embed Size (px)
Citation preview

American Journal of Medical Genetics Part C (Seminars in Medical Genetics) 175C:8–26 (2017)
A R T I C L E
The 2017 International Classification of theEhlers–Danlos SyndromesFRANSISKA MALFAIT,* CLAIR FRANCOMANO, PETER BYERS, JOHN BELMONT,BRITTA BERGLUND, JAMES BLACK, LARA BLOOM, JESSICA M. BOWEN, ANGELA F. BRADY,NIGEL P. BURROWS, MARCO CASTORI, HELEN COHEN, MARINA COLOMBI,SERWET DEMIRDAS, JULIE DE BACKER, ANNE DE PAEPE, SYLVIE FOURNEL-GIGLEUX,MICHAEL FRANK, NEETI GHALI, CECILIA GIUNTA, RODNEY GRAHAME, ALAN HAKIM,XAVIER JEUNEMAITRE, DIANA JOHNSON, BIRGIT JUUL-KRISTENSEN,INES KAPFERER-SEEBACHER, HANADI KAZKAZ, TOMOKI KOSHO, MARK E. LAVALLEE,HOWARD LEVY, ROBERTO MENDOZA-LONDONO, MELANIE PEPIN, F. MICHAEL POPE,EYAL REINSTEIN, LEEMA ROBERT, MARIANNE ROHRBACH, LYNN SANDERS,GLENDA J. SOBEY, TIM VAN DAMME, ANTHONY VANDERSTEEN,CAROLINE VAN MOURIK, NICOL VOERMANS, NIGEL WHEELDON, JOHANNES ZSCHOCKE,AND BRAD TINKLE
*CorresponE-mail: Fransis
DOI 10.100Article first
� 2017 Wil
The Ehlers–Danlos syndromes (EDS) are a clinically and genetically heterogeneous group of heritable connectivetissue disorders (HCTDs) characterized by joint hypermobility, skin hyperextensibility, and tissue fragility. Overthe past two decades, the Villefranche Nosology, which delineated six subtypes, has been widely used as thestandard for clinical diagnosis of EDS. For most of these subtypes, mutations had been identified in collagen-encoding genes, or in genes encoding collagen-modifying enzymes. Since its publication in 1998, a wholespectrum of novel EDS subtypes has been described, and mutations have been identified in an array of novelgenes. The International EDS Consortium proposes a revised EDS classification, which recognizes 13 subtypes.For each of the subtypes, we propose a set of clinical criteria that are suggestive for the diagnosis. However, inview of the vast genetic heterogeneity and phenotypic variability of the EDS subtypes, and the clinical overlapbetween EDS subtypes, but also with other HCTDs, the definite diagnosis of all EDS subtypes, except for thehypermobile type, relies onmolecular confirmation with identification of (a) causative genetic variant(s). We alsorevised the clinical criteria for hypermobile EDS in order to allow for a better distinction from other jointhypermobility disorders. To satisfy research needs, we also propose a pathogenetic scheme, that regroups EDSsubtypes for which the causative proteins function within the same pathway. We hope that the revisedInternational EDS Classification will serve as a new standard for the diagnosis of EDS and will provide aframework for future research purposes. © 2017 Wiley Periodicals, Inc.
KEYWORDS: classification; Ehlers–Danlos syndromes; genetic basis; collagen
How to cite this article: Malfait F, Francomano C, Byers P, Belmont J, Berglund B, Black J, Bloom L,Bowen JM, Brady AF, Burrows NP, Castori M, Cohen H, Colombi M, Demirdas S, De Backer J,
De Paepe A, Fournel-Gigleux S, Frank M, Ghali N, Giunta C, Grahame R, Hakim A, Jeunemaitre X,Johnson D, Juul-Kristensen B, Kapferer-Seebacher I, Kazkaz H, Kosho T, Lavallee ME, Levy H,
Mendoza-Londono R, Pepin M, Pope FM, Reinstein E, Robert L, Rohrbach M, Sanders L, Sobey GJ,Van Damme T, Vandersteen A, van Mourik C, Voermans N, Wheeldon N, Zschocke J, Tinkle B. 2017.The 2017 international classification of the Ehlers–Danlos syndromes. Am J Med Genet Part C Semin
Med Genet 175C:8–26.
INTRODUCTION
The Ehlers–Danlos syndromes (EDS)are a heterogeneous group of heritable
dence to: Fransiska Malfait, [email protected]/ajmg.c.31552published online in Wiley Online Lib
ey Periodicals, Inc.
connective tissue disorders (HCTDs)characterized by joint hypermobility,skin hyperextensibility, and tissuefragility. The clinical and genetic
for Medical Genetics, Ghent University Hospital, D
rary (wileyonlinelibrary.com).
heterogeneity of this condition haslong been recognized. The 1988 “BerlinNosology” recognized 11 subtypes,defined by Roman numerals, based on
e Pintelaan 185, B-9000 Ghent, Belgium.

ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 9
clinical findings and mode of inheri-tance [Beighton et al., 1988]. Thesubjective interpretation of several semi-quantitative clinical signs, such as jointhypermobility, skin hyperextensibility,tissue fragility and bruising, however, ledto clinical uncertainty, diagnostic con-fusion regarding the type of EDS and theinclusion of phenotypically similar con-ditions under the broad diagnosis ofEDS. With the elucidation of thebiochemical and molecular basis ofmany of these EDS types, a revisedclassification, the “Villefranche Nosol-ogy,” was published in 1998 [Beightonet al., 1998]. This classification delin-eated six subtypes, for which majorand minor clinical criteria were defined,andwhich included the biochemical andmolecular basis, when known. TheRoman numerals were substituted by adescriptive name, which capturedthe characteristic manifestations ofeach type. One underlying assumptionwas that most, if not all, of these typesof EDS were a consequence of alter-ations in fibrillar collagen genes orin genes that encoded collagenmodifiers.
With the elucidation of thebiochemical and molecularbasis of many of these EDStypes, a revised classification,the “Villefranche Nosology,”was published in 1998. Thisclassification delineated sixsubtypes, for which majorand minor clinical criteriawere defined, and whichincluded the biochemicaland molecular basis, when
known.
Over the past two decades theVillefranche Nosology has served itspurpose and has been widely used as thestandard for the clinical diagnosis of
EDS, and for clinical research on variousaspects of these conditions. However,since its publication, a whole spectrumof novel EDS subtypes has beendescribed, and with the advent ofnext-generation sequencing (NGS)facilities, mutations have been identifiedin an array of new genes, that arenot always, at first sight, involved incollagen biosynthesis and/or structure.As such, the Villefranche classificationis showing its age. Furthermore, inthe persistent lack of a genetic defect,there is a dire need for a betterclinical definition of the hypermobiletype of EDS and its delineation fromother hypermobility disorders. There-fore, we undertook a comprehensivereview of the EDS-related literature,and, based on our findings, revised theEDS Classification.
THE 2017 INTERNATIONALCLASSIFICATION FOR THEEHLERS–DANLOSSYNDROMES
The new classification recognizes 13subtypes, as outlined in Table I. Aftercareful discussions whether to maintaina clinically orientated classificationversus a genetic classification, we pro-pose to maintain a clinical classification,in which the previously establisheddescriptive names are maintained, sincethey are generally accepted andwidely used in the medical, scientificand patient community. For newlydefined EDS phenotypes, we proposea novel descriptor that captures thecharacteristic manifestations of thephenotype.
We included all phenotypes thatpresent the basic clinical hallmarks ofEDS, that is joint hypermobility, skinhyperextensibility and tissue fragility. Inparticular, such features should distin-guish the redefined hypermobile type(hypermobile EDS, hEDS) from otherjoint hypermobility disorders (See also “Aframework for the classification of JointHypermobility and Related Conditions”by Castori et al., this issue). Some ofthe phenotypes clinically overlap withother HCTDs, such as “myopathicEDS,” which is caused by heterozygous
or biallelic mutations in COL12A1(mEDS) and which clinically overlapswith Bethlem Myopathy, and “
spondylodysplastic EDS” caused by bial-lelic B3GALT6 mutations (spEDS-B3GALT6), which clinically overlapswith spondylo-epimetaphyseal dysplasiawith joint laxity type I (SEMD-JL1).Since several patients with these con-ditions are clinically suspected to have aform of EDS,we believe that inclusion inthe EDS classification is justified. This isalso the case for Brittle Cornea Syn-drome. We currently did not retain thefilaminA-related periventricular nodularheterotopia (PVNH) with EDS-featureswithin the classification, as the majorityof patients primarily present with aneurological phenotype. A minority ofpatients has varying features of a HCTD,which may include life-threateninganeurysms, however, there is insufficientpublished data to reliably differentiateand prognosticate PVNH from PVNH-EDS. We recommend that in- or exclu-sion of these conditions in the EDSclassification is reviewed in future years,when more information becomesavailable.
In line with the 1997 VillefrancheNosology, we propose a set of majorand minor clinical criteria for eachEDS subtype. A major criterion hashigh diagnostic specificity because it ispresent in the vast majority of theaffected individuals and/or it is char-acteristic for the disorder and allowsdifferentiation from other EDS sub-types and/or other HCTDs. A minorcriterion is a sign of lesser diagnosticspecificity, but its presence supports thediagnosis. For each of the subtypes, wedefined minimal major�minor clini-cal criteria that are suggestive for thediagnosis of a specific subtype. How-ever, in view of the vast geneticheterogeneity and phenotypic variabil-ity of the EDS subtypes, and theclinical overlap between many of thesesubtypes, but also with other HCTDs,the definite diagnosis relies for all sub-types, except hEDS, on molecular confir-mation with identification of (a)causative variant(s) in the respectivegene. A molecular diagnosis is ex-tremely important for counseling

TABLE I. Clinical Classification of the Ehlers-Danlos Syndromes, Inheritance Pattern, and Genetic Basis
Clinical EDS subtype Abbreviation IP Genetic basis Protein
1 Classical EDS cEDS AD Major: COL5A1, COL5A1 Type V collagenRare: COL1A1 Type I collagen
c.934C>T, p.(Arg312Cys)
2 Classical-like EDS clEDS AR TNXB Tenascin XB
3 Cardiac-valvular cvEDS AR COL1A2 (biallelic mutations that lead to COL1A2NMD and absence of pro a2(I) collagen chains)
Type I collagen
4 Vascular EDS vEDS AD Major: COL3A1 Type III collagenRare: COL1A1 Type I collagen
c.934C>T, p.(Arg312Cys)c.1720C>T, p.(Arg574Cys)c.3227C>T, p.(Arg1093Cys)
5 Hypermobile EDS hEDS AD Unknown Unknown
6 Arthrochalasia EDS aEDS AD COL1A1, COL1A2 Type I collagen
7 Dermatosparaxis EDS dEDS AR ADAMTS2 ADAMTS-2
8 Kyphoscoliotic EDS kEDS AR PLOD1 LH1FKBP14 FKBP22
9 Brittle Cornea syndrome BCS AR ZNF469 ZNF469PRDM5 PRDM5
10 Spondylodysplastic EDS spEDS AR B4GALT7 b4GalT7B3GALT6 b3GalT6SLC39A13 ZIP13
11 Musculocontractural EDS mcEDS AR CHST14 D4ST1DSE DSE
12 Myopathic EDS mEDS AD or AR COL12A1 Type XII collagen
13 Periodontal EDS pEDS AD C1R C1rC1S C1s
IP, inheritance pattern; AD, autosomal dominant; AR, autosomal recessive, NMD, nonsense-mediated mRNA decay.
10 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE
purposes, as it allows confirmation ofthe precise diagnosis and gives infor-mation on inheritance pattern, recur-rence risk and prognosis, and it mayguide management. Moreover, itallows for the formation of homoge-neous cohorts for research purposes,and future therapeutic interventions.Since the genetic basis of hEDS isstill unknown, the diagnosis of thissubtype rests on clinical findings, asdelineated in the revised criteria forhEDS.
In view of the vast geneticheterogeneity and phenotypic
variability of the EDSsubtypes, and the clinical
overlap between many of thesesubtypes, but also with other
HCTDs, the definitediagnosis relies for all
subtypes, except hEDS, on
molecular confirmation withidentification of (a) causativevariant(s) in the respective
gene.
Molecular diagnostic strategiesshould rely on NGS technologies,which offer the potential for parallelsequencing of multiple genes. Targetedresequencing of a panel of genes,for example, COL5A1, COL5A2,

1Skin extensibility should be measured bypinching and lifting the cutaneous and subcu-taneous layers of the skin on the volar surface atthe middle of the non-dominant forearm asdescribed in Remvig et al. [2009]. Skin ishyperextensible if it can be stretched over astandardized cut-off in three of the followingareas: 1.5 cm for the distal part of the forearmsand the dorsum of the hands; 3 cm for neck,elbow, and knees.2Abnormal scarring can range in severity. Mostpatients have extensive atrophic scars at anumber of sites (Fig. 1). These can sometimesbe haemosiderotic. A minority of patients aremore mildly affected.3GJH is evaluated according to the Beightonscore; a Beighton score of �5 is consideredpositive for the presence of GJH (Fig. 2). Sincelaxity decreases with age, patients with aBeighton score <5/9 may be consideredpositive based on their historical observations(see “five-point questionnaire (5PQ)” (TableIII).4Easy bruising can occur anywhere on the body,including unusual sites. The pretibial area oftenremains stained with hemosiderin from previ-ous bruises.5Subjective abnormality of the skin texture isappreciable by touching the skin.6Molluscoid pseudotumors are fleshy lesionsassociated with scars, found over pressure points(e.g., elbow, fingers).7Subcutaneous spheroids (Fig. 1F) are smallspherical hard bodies, frequently mobile, andpalpable on the forearms and shins. Spheroidsmay be calcified and detectable radiologically.8Epicanthal folds are often seen in childhoodbut may also be seen in adults.
ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 11
COL1A1 and COL1A2, is a time- andcost-effective approach for the molecu-lar diagnosis of the genetically hetero-geneous EDS.When no mutation (or incase of an autosomal recessive conditiononly one mutation) is identified, thisapproach should be complemented witha copy number variant (CNV) detectionstrategy to identify large deletions orduplications, for example MultiplexLigation-dependent Probe Amplifica-tion (MLPA), qPCR, or targeted arrayanalysis. Alternatively, or in a secondphase, whole exome sequencing(WES) or whole genome sequencing(WGS) and RNA sequencing techni-ques can be used, with data-analysisinitially focusing on the genes of interestfor a given EDS subtype. In absence ofthe identification of a causal mutation,this approach allows to expand theanalysis to other genes within thegenome. This is particularly interestingin view of the clinical overlap betweenEDS subtypes and with otherHCTDs, and the observation that inan important proportion of EDS-patients, no pathogenic variants areidentified in any of the known EDS-associated genes.
The interpretation of variants ofuncertain significance (VUS), espe-cially missense variants, should includecorrelation with the complete clinicalphenotype. In keeping with theACMG guidelines, variants that aresupported by some evidence of patho-genicity (e.g., high in silico scores,presence in a functionally active do-main) can be considered “likely patho-genic.” Familial segregation studiesmay help to interpret the pathogenicityof the variant, and for some genes,ultrastructural, biochemical and/orfunctional protein assays are available,as outlined below. Individuals harbor-ing such a “likely pathogenic” variantshould be followed clinically. Initialcounseling for such patients shouldpoint out that the true significance ofthe variant will not be known untilthese additional tests are completed.In the longer term, assignment ofpathogenicity is likely to be facilitatedby data from large-scale genome-sequencing projects in patient and
control cohorts [Weerakkody et al.,2016].
For patients who fulfill the set ofminimal clinical requirements for aspecific EDS subtype, but (i) who haveno access to molecular confirmation;(ii) in whom one or more VUS is/areidentified in one the EDS subtype-specific genes; or (iii) in whom nocausative variants are identified in any ofthe EDS-subtype-specific genes, a “pro-visional clinical diagnosis” of an EDSsubtype can be made, and patientsshould be followed clinically. However,alternative diagnoses and hence ex-panded molecular testing should beconsidered.
PATHOGENETICMECHANISMSUNDERLYING THEEHLERS–DANLOSSYNDROMES
While the proposed clinically orien-tated classification aims to be user-friendly for the EDS non-specialist,and offers the affected patients andtheir family members a “descriptive”diagnosis that he or she can identifywith, a genetic classification provides abetter framework for research purposesand for the development of futuretreatment strategies. To satisfy bothclinical and research needs, we propose,in addition to the clinical classification,a pathogenetic scheme, that regroupsEDS subtypes for which the proteins,coded by the causative genes, functionwithin the same pathway, and whichare likely to have shared pathogenicmechanisms, based on current knowl-edge (Table II). A similar regrouping ofosteogenesis imperfecta (OI) subtypesby gene function was proposed and iswidely adapted in clinical and inresearch settings.
CLASSIFICATION OF EDS
Classical EDS (cEDS)
•
Inheritance Autosomal dominantMajor criteria
• 1. Skin hyperextensibility1 and atro-phic scarring2
2. Generalized joint hypermobility
(GJH)3•
Minor criteria 1. Easy bruising42. Soft, doughy skin5
3. Skin fragility (or traumatic splitting)4. Molluscoid pseudotumors6
5. Subcutaneous spheroids7
6. Hernia (or history thereof)7. Epicanthal folds8
8. Complications of joint hyper-mobility (e.g., sprains, luxation/subluxation, pain, flexible flatfoot)
9. Family history of a first degree
relative who meets clinical criteria
TABLEII.Reg
roupingoftheEhlers-D
anlosSyn
dromes
Accordingto
UnderlyingGen
etic
andPathogen
etic
Mechan
isms
Form
erno
menclatureandother
names
Villefranche
nomenclature
New
Nom
enclature
OMIM
cond
ition
Locus
Gene
OMIM
gene
Protein
IP
GROUPA:Disordersofco
llage
nprimarystructure
andco
llage
nprocessing
Gravis/EDSI
Classicaltype
ClassicalEDS(cEDS)
130000
9q34.3
COL5A
1120215
Type
Vcollagen
AD
Mitis/EDSII
130010
2q32.2
COL5A
2120190
Type
Vcollagen
17q21.33
COL1A
1120150
Type
Icollagen(p.Arg312C
ys)
Arterial-Ecchymotic
EDS
Vasculartype
Vascular
EDS(vEDS)
130050
2q32.2
COL3A
1120180
Type
IIIcollagen
AD
EDSIV
17q21.33
COL1A
1120150
Type
Icollagen
p.(Arg312C
ys)
p.(Arg574C
ys)
p.Arg1093Cys)
Arthrochalasis
Multip
lexCon
genita
Arthrochalasia
type
Arthrochalasia
EDS(aEDS)
130060
17q21.33
COL1A
1120150
Type
Icollagen
AD
130060
7q21.3
COL1A
2120160
EDSVIIA
EDSVIIB
Hum
anderm
atosparaxisEDSVIIC
Dermatosparaxistype
DermatosparaxisEDS(dEDS)
225410
5q35.3
ADAMTS2
604539
ADAMTS-2
AR
Cardiac-valvularEDS
/Cardiac-valvularEDS(cvE
DS)
225320
7q21.3
COL1A
2120160
Type
Icollagen
AR
Totalabsenceof
proa2(I)collagen
chains
GROUPB:Disordersofco
llage
nfoldingan
dco
llage
ncross-linking
Ocular-Scoliotic
EDS
Kypho
scoliosis
type
Kypho
scoliotic
EDS
(kEDS-PL
OD1)
225400
1p36.22
PLOD1
153454
Lysylhydroxylase
1AR
EDSVI
EDSVIA
//
Kypho
scoliotic
EDS
(kEDS-FK
BP1
4)
614557
7p14.3
FKBP1
4614505
FKBP2
2AR
GROUPC:Disordersofstructure
andfunctionofmyo
matrix,
theinterfacebetweenmuscle
andECM
Classical-likeEDS(clEDS)
606408
6p21.33-p21.32
TNXB
600985
Tenascin
XB
AR
//
Myopathic
EDS(m
EDS)
616471
6q13-q14
COL12
A1
120320
CollagenXII
AD/A
R
GROUPD:Disordersofglyc
osaminoglyc
anbiosynthesis
EDSProgeroid
EDSProgeroidtype
Spon
dylodysplastic
EDS
(spE
DS-B4G
ALT7)
130070
5q35.3
B4G
ALT7
604327
GalactosyltransferaseI
b4G
alT7
AR
EDSProgeroidtype
1
EDSProgeroidtype
2b3G
alT6-deficient
EDS
Spon
dylodysplastic
EDS
(spE
DS-B3G
ALT6)
615349
1p36.33
B3G
ALT6
615291
GalactosyltransferaseII
b3G
alT6
AR
b3G
alT6-deficient
EDS
AdductedThu
mbClubfoo
tsynd
rome
MusculocontracturalEDS
(mcE
DS-CHST
14)
601776
15q15.1
CHST
14608429
Dermatan-4
sulfo
transferase-1
AR
EDSKosho
type
MusculocontracturalEDS
(mcE
DS-DSE
)
615539
6q22.1
DSE
605942
Dermatan
sulfate
epim
erase-1
AR
EDSMusculocontracturaltype
D4ST1-deficient
EDS
12 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE

TABLEII.(Continued)
Form
erno
menclatureandother
names
Villefranche
nomenclature
New
Nom
enclature
OMIM
cond
ition
Locus
Gene
OMIM
gene
Protein
IP
GROUPE:Disordersofco
mplemen
tpathway
EDSV
III
EDSperiod
ontitis
Period
ontalEDS(pEDS)
130080
12p13.31
C1R
613785
C1r
AD
C1S
120580
C1s
GROUPF:Disordersofintracellularprocesses
a
Spon
dylocheirodysplastic
EDS
Spon
dylodysplastic
EDS
(spE
DS-SL
C39
A13
)
612350
11p11.2
SLC39
A13
608735
ZIP13
AR
Brittle
CorneaSynd
rome
Brittle
CorneaSynd
rome(BCS)
229200
16q24
ZNF4
69612078
ZNF4
69AR
614170
4q27
PRDM5
614161
PRDM5
AR
Unresolved
form
sofEDS
Hypermob
ileHypermob
ility
type
Hypermob
ileEDS(hEDS)
130020
??
?AD
EDSIII
Conditionsnotincluded
inEDSspectrum
anym
ore
Occipitalho
rnsynd
rome
//
304150
Xq21.1
ATP7
A300011
ATP7
AX-L
Fibron
ectin
-deficient
(EDSX)
//
AD
FamilialArticular
hyperm
obility
(EDSXI)
//
AD
X-linkedEDSwith
musclehematom
a(EDSV)
//
X-L
Filamin
ArelatedEDSwith
periventricular
nodu
larheterotopia
//
300049
Xq28
FLNA
300017
Filamin
AX-L
IP,inh
eritancepattern;
AD,autosom
aldo
minant;AR,autosomalrecessive;
X-L,X
-linkedrecessive.
a For
EDSsubtypes
implem
entedin
thiscategory,the
underlying
pathop
hysio
logicalm
echanism
isno
treadily
understood
,and
classificationwith
inthissubgroup
isprovision
ary,un
tilfurtherfunctio
nalinformationbecomes
available.
ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 13
•
Minimal criteria suggestive for cEDS: – Major criterion (1): skin hyperexten- sibility and atrophic scarringPlus
– Either major criterion (2): GJH– And/or: at least three minor criteria Confirmatory molecular testing isobligatory to reach a final diagnosis.•
Molecular basisMore than 90% of cEDS patients harbora heterozygous mutation in one of thegenes encoding type V collagen(COL5A1 and COL5A2) [Symoenset al., 2012; Ritelli et al., 2013; Zoppiet al., 2015] (see also “Ehlers–DanlosSyndrome, Classical Type,” by Bowenet al., this issue). Rarely, specific muta-tions in the genes encoding type Icollagen can be associated with acEDS-phenotype. These include theheterozygous COL1A1 c.934C>T,p.(Arg312Cys) substitution [Malfaitet al., 2007a]. Patients harboring thismutation are particularly at risk forvascular rupture, whereas patients har-boring other COL1A1 arginine-to-cys-teine substitutions are associated withother specific phenotypes (see also “Eh-lers–Danlos Syndromes, Rare Types,” byBrady et al., this issue). Sodium DodecylSulfate PolyAcrylamide Gel Electropho-resis (SDS PAGE) demonstrates themigration of an extra band in the cellfraction, and sometimes also in themedium fraction. This band, whichdisappears after reduction with b-mer-captoethanol, consists of disulfide-bonded a chains [Malfait et al., 2007b].Furthermore, biallelic COL1A2 muta-tions that lead to complete absence of theproa2(I) collagen chain may also presentwith a classical EDS-like phenotype, butthese patients are at risk for developingsevere cardiac-valvular problems. More-over, inheritance of this condition isautosomal recessive (see also “Cardiac-valvular EDS,” below, and “Ehlers–DanlosSyndromes,RareTypes,” byBrady et al., thisissue). SDS PAGE demonstrates completeabsence of (pro-)a2 chains of type I (pro)collagenextracted fromdermis [Schwarzeet al., 2004; Malfait et al., 2006].• Verification of clinical diagnosisMolecular screening by means oftargeted resequencing of a gene panel

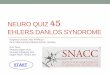
Figure 1. The atrophic skin/widened scars seen in hypermobile EDS as comparedto classic EDS. Hypermobile EDS. Post-traumatic, atrophic, and widened scar in ayoung man (A). Skin stretching between the examiner’s fingers discloses mild atrophy ofthe underlying dermis (B). A further atrophic and widened scar due to wound healingdelay after excision of a melanocytic nevus in a youngwoman (C). Classical EDS. Typicalpapyraceous and hemosideric scar after repetitive wound re-opening and molluscoidpseudotumor in an adult man (D). Papyraceous, but not hemosideric scar and acquiredcutis laxa in a young woman (E). Subcutaneous spheroid (F). Huge molluscoidpseudotumor of the elbow (G).
More than 90% of cEDSpatients harbor a heterozygousmutation in one of the genesencoding type V collagen(COL5A1 and COL5A2). 9For definitions of GJH and skin hyperexten-
sibility, see criteria for “Classical EDS.”
14 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE
that includes at least the COL5A1,COL5A2, COL1A1, and COL1A2genes, or by WES or WGS, isindicated. When no mutation isidentified, this approach should becomplemented with a CNV detectionstrategy to identify large deletions orduplications.
In case of unavailability of genetictesting, transmission electron micros-copy (TEM) findings of collagenflowers on skin biopsy can supportthe clinical diagnosis, but cannotconfirm it.Absence of these confirmatory
findings does not exclude the diagno-sis, as specific types of mutations (e.g.,deep intronic mutations) may goundetected by standard diagnosticmolecular techniques; however, alter-native diagnoses should be consideredin the absence of (a) COL5A1,COL5A2, COL1A1, or COL1A2mutation(s).
Classical-Like EDS (clEDS)
•
Inheritance Autosomal Recessive Major criteria • 1. Skin hyperextensibility,9 with vel-vety skin texture and absence ofatrophic scarring
2. GJH9 with or without recurrentdislocations (most commonly shoul-der and ankle)
3. Easy bruisable skin/spontaneous
ecchymoses•
Minor criteria 1. Foot deformities: broad/plump fore-foot, brachydactyly with excessiveskin; pes planus; hallux valgus;piezogenic papules
2. Edema in the legs in absence ofcardiac failure
3. Mild proximal and distal muscleweakness
4. Axonal polyneuropathy5. Atrophy of muscles in hands and
feet6. Acrogeric hands, mallet finger(s),
clinodactyly, brachydactyly7. Vaginal/uterus/rectal prolapse
Minimal criteria suggestive for clEDS: • – All three major criteria AND a familyhistory compatible with autosomalrecessive transmission.Confirmatory molecular testing isobligatory to reach a final diagnosis.

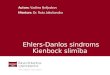
Figure 2. The Beighton scoring system. Each joint is measured using a goniometer and each side is scored independently as outlined[Juul-Kristensen et al., 2007]. (A) With the palm of the hand and forearm resting on a flat surface with the elbow flexed at 90°, if themetacarpal-phalangeal joint of the fifth finger can be hyperextended more than 90° with respect to the dorsum of the hand, it is consideredpositive, scoring 1 point. (B) With arms outstretched forward but hand pronated, if the thumb can be passively moved to touch theipsilateral forearm it is considered positive scoring 1 point. (C)With the arms outstretched to the side and hand supine, if the elbowextendsmore than 10°, it is considered positive scoring 1 point. (D) While standing, with knees locked in genu recurvatum, if the knee extendsmore than 10°, it is considered positive scoring 1 point. (E) With knees locked straight and feet together, if the patient can bend forward toplace the total palm of both hands flat on the floor just in front of the feet, it is considered positive scoring 1 point. The total possible score is9. Figure courtesy of Dr. Juul-Kirstensen.
ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 15
•
Molecular basisclEDS is caused by a complete lack ofTenascin XB (TNX) due to biallelicTNXBmutations, that lead to nonsense-mediated mRNA decay, or biallelicdeletion of TNXB. As a result theTNX protein is completely absent.TNXB is the only gene associated withclEDS.•
Verification of diagnosisMolecular analysis of the TNXB geneshould be used as the standard confir-matory test. Difficulties in DNA testingare related to the presence of apseudogene (TNXA), which is morethan 97% identical to the 30 end ofTNXB (exons 32–44). With the onlyexception of exon 35, which partiallyshows a TNXB-specific sequence,exon and intron sequences in thisregion are identical or almostidentical in both the gene and thepseudogene. This has implicationsboth for sequencing and deletion/duplication analysis.For sequence analysis of TNXB, twoapproaches are recommended. 1. Sanger sequencing of the entireTNXB gene.2. Next-generation sequencing of
TNXBþ Sanger sequencing of the
10The cardiac-valvular problems were reportedpseudogene region.
in all affected adult individuals, but were absentin the two reported children (both<10 years ofage).11For definition of skin hyperextensibility, seecriteria for “Classical EDS.”
Both approaches will requiresequence analysis of the pseudogene-homolog region in a few large multi-exons amplicons.
If no or only one causativemutationis identified by classic sequencing,additional methods that allow detectionof large deletions/duplications shouldbe added. So far no method is able tospecifically detect TNXB CNVs in thehighly homologous exons 32–34 and36–44. CNV analysis of exon 35 iscurrently used to detect deletions inthis region, including the 30 kb deletionpreviously described by Schalkwijket al. [2001].
TNX, a large 450 kDa extracel-lular matrix glycoprotein, secretedby skin fibroblasts, can be detectedwith antibodies directed against itscarboxyterminal end. Patients withclEDS are completely depleted of theTNX protein in serum. We refer tothe paper of Schalkwijk et al. [2001]for more detailed information con-cerning the used method to detectTNX.
Absence of these confirmatoryfindings does not exclude the diagnosis,as specific types of mutations (e.g., deepintronic mutations) may go undetectedby standard diagnostic molecular tech-niques; however, alternative diagnosesshould be considered in the absence of aTNXB mutation.
Cardiac-Valvular EDS (cvEDS)
•
Inheritance Autosomal recessive•
Major criteria 1. Severe progressive cardiac-valvularproblems (aortic valve, mitralvalve)10
2. Skin involvement: skin hyperexten-sibility,11 atrophic scars, thin skin,easy bruising
3. Joint hypermobility (generalized or
restricted to small joints)•
Minor criteria 1. Inguinal hernia2. Pectus deformity (especiallyexcavatum)3. Joint dislocations4. Foot deformities: pes planus, pes
planovalgus, hallux valgus
• Minimal criteria suggestive for cvEDS:– Major Criterion (1): severe progres-sive cardiac-valvular problems
– AND a family history compatible
with autosomal recessive inheritancePlus
– Either: one other major criterion– And/or: at least two minor criteria Confirmatory molecular testing isobligatory to reach a final diagnosis.•
Molecular basiscvEDS is caused by a complete lack ofthe proa2-chain of type I collagen dueto biallelic COL1A2 mutations, that
16 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE
lead to nonsense-mediated mRNAdecay. COL1A2 is the only geneassociated with cvEDS.
•
A family history of thedisorder, arterial rupture, or
Verification of diagnosisMolecular screening by Sanger se-quencing of COL1A2, or targetedresequencing of a gene panel thatincludes COL1A2 is indicated. Whenno mutation is identified, this approachshould be complemented with a CNVdetection strategy to identify largedeletions or duplications.
In case of unavailability of genetictesting, SDS PAGE demonstratestotal absence of (pro-) a2(I) collagenchains.
Whereas absence of these confirma-tory biochemical findings allows toexclude the diagnosis of cvEDS, absenceof confirmatory genetic findings doesnot exclude the diagnosis, as specifictypes of mutations (e.g., deep intronicmutations) may go undetected by stan-dard diagnostic molecular techniques.
dissection in individuals less
Vascular EDS (vEDS) than 40 years of age,unexplained sigmoid colon
• Inheritance rupture, or spontaneous Autosomal dominantMajor criteria
pneumothorax in the presence •of other features consistentwith vEDS should all lead todiagnostic studies to determineif the individual has vEDS.
1. Family history of vEDS withdocumented causative variant inCOL3A1
2. Arterial rupture at a young age3. Spontaneous sigmoid colon perfora-
tion in the absence of knowndiverticular disease or other bowelpathology
4. Uterine rupture during the thirdtrimester in the absence of previousC-section and/or severe peripartumperineum tears
5. Carotid-cavernous sinus fistula (CCSF)
formation in the absence of trauma•
Minor criteria 1. Bruising unrelated to identifiedtrauma and/or in unusual sitessuch as cheeks and back
2. Thin, translucent skin with in-creased venous visibility
3. Characteristic facial appearance4. Spontaneous pneumothorax5. Acrogeria6. Talipes equinovarus7. Congenital hip dislocation
8. Hypermobility of small joints9. Tendon and muscle rupture10. Keratoconus11. Gingival recession and gingival
fragility12. Early onset varicose veins (under
age 30 and nulliparous if female)
• Minimal criteria suggestive for vEDS:A family history of the disorder, arterialrupture or dissection in individualsless than 40 years of age, unexplainedsigmoid colon rupture, or spontaneouspneumothorax in the presence of otherfeatures consistent with vEDS should alllead to diagnostic studies to determine ifthe individual has vEDS. Testing forvEDS should also be considered in thepresence of a combination of the other“minor” clinical features listed above.Even for experienced clinicians theclinical diagnosis of vEDS may bedifficult. Because of implications fortreatment, natural history, and recur-rence risk, the diagnosis of vEDS restson the identification of a causativevariant in one allele of COL3A1.
•
Molecular basisPatients with vEDS typically harbor aheterozygous mutation in theCOL3A1gene, encoding type III collagen, withthe rare exception of specific heterozy-gous arginine-to-cysteine substitutionmutations in COL1A1 (c.934C>T, p.Arg312Cys; c.1720C>T, p.Arg574Cysand c.3277C>T, p.Arg1093Cys) thatare also associated with vascular fragility,mimicking COL3A1-vEDS [Malfaitet al., 2007b], (see also “Ehlers–DanlosSyndrome, Rare Types,” by Brady et al.,this issue).
In very rare instances, biallelic path-ogenic variants in COL3A1 may beidentified.
•
Verification of clinical diagnosisMolecular screening by Sanger se-quencing of COL3A1, or targetedresequencing of a gene panel thatincludes COL3A1 and COL1A1 (thelatter to identify the above-listed argi-nine-to-cysteine substitution muta-tions) is indicated. When no mutationis identified, this approach should becomplemented with a CNV detectionstrategy to identify large deletions orduplications.Absence of these confirmatory find-ings does not exclude the diagnosis, asspecific types of mutations (e.g., deepintronic mutations) may go undetectedby standard diagnostic molecular tech-niques; however, alternative diagnosesshould be considered in the absence of aCOL3A1 or COL1A1 mutation.
Hypermobile EDS (hEDS)
•
Inheritance Autosomal dominant Molecular basis • Unknown Clinical diagnosis • The diagnosis of hEDS remains clinicalas there is yet no reliable or appreciablegenetic etiology to test for in the vastmajority of patients. This, in part, likelyreflects genetic heterogeneity. In addi-tion, the syndromic presentation mayvary according to age and gender. Thereis also a clinical spectrum rangingfrom asymptomatic joint hypermobility,through “non-syndromic” hypermo-bility with secondary manifestations,to hEDS (see “A Framework for theClassification of Joint Hypermobility andRelated Conditions” by Castori et al., thisissue). A diagnosis of hEDS should beassigned only in those who meet all ofthe criteria described below, whichshould help to reduce heterogeneityand facilitate efforts to discover the
ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 17
underlying genetic cause(s) of thesyndrome which, in turn, may helpclinical management. Since there iscurrently no “gold standard” laboratorytest to confirm or refute the diagnosis,we anticipate that future research willlead to further revisions of these clinicalcriteria necessitating regular review ofthe relevant medical literature. It is alsoimperative, as this is a clinical diagnosis,to be relatively confident that thepatient’s presentation does not repre-sent one of the many other disorders ofconnective tissue. Therefore, the clini-cian should be experienced at thephysical examination described hereinas well the historical and clinicalpresentation of other HCTD and theirdiagnoses.
The clinical diagnosis of hEDS needsthe simultaneous presence of criteria 1AND 2 AND 3. Specific annotationsand further explanations (i.e., footnotes[FN]) are reported for select features.
TABLE III. The Five-Point Questionnaire. Adapted From[Grahame and Hakim, 2003]
1. Can you now (or could you ever) place your hands flat on the floor without bendingyour knees?
2. Can you now (or could you ever) bend your thumb to touch your forearm?3. As a child, did you amuse your friends by contorting your body into strange shapesor could you do the splits?
4. As a child or teenager, did your shoulder or kneecap dislocate on more than oneoccasion?
5. Do you consider yourself “double-jointed”?A “yes” answer to two or more questions suggests joint hypermobility with 80–85%sensitivity and 80–90% specificity
Criterion 1: Generalized JointHypermobility (GJH)
To date, the Beighton score (Fig. 2) isthe most recognized tool for assessingGJH (see “Measurement Properties ofClinical Assessment Methods for ClassifyingGeneralized Joint Hypermobility—a Sys-tematic Review” by Juul-Kristensen et al.,this issue). According to the originaldefinition of the Beighton score and itssubsequent incorporation into the Vil-lefranche nosology for the hEDS, thecut-off for the definition of GJH is �5points out of 9. However, joint range ofmotion decreases with age [Soucie et al.,2011;McKay et al., 2016] and there is aninverse relationship between age atascertainment and the Beighton score[Remvig et al., 2007], so the cut-off offive may prompt an over-diagnosis inchildren and an under-diagnosis amongadults and elders. As GJH is considered aprerequisite for the diagnosis of hEDSand GJH is a constitutional trait stronglyinfluenced by acquired and inheritedconditions (e.g., sex, age, past-traumas,co-morbidities, etc.), some minor adap-tations to the cut-off of five shouldbe considered for the diagnosis ofhEDS. The Committee on behalf of
the International Consortium on theEhlers–Danlos Syndromes proposes�6 for pre-pubertal children and ado-lescents, �5 for pubertal men andwomen up to the age of 50, and �4for those >50 years of age for hEDS.This may vary from other types of EDSbut such types have confirmatorytesting.
According to the originaldefinition of the Beightonscore and its subsequentincorporation into the
Villefranche nosology for thehEDS, the cut-off for thedefinition of GJH is �5points out of 9. However,
joint range of motion decreaseswith age and there is an
inverse relationship betweenage at ascertainment andthe Beighton score, so the
cut-off of five may prompt anover-diagnosis in children andan under-diagnosis among
adults and elders.
In individuals with acquired jointlimitations (past surgery, wheelchair,
amputations, etc.) affecting theBeighton score calculation, the assess-ment of GJH may include historicalinformation using the five-point ques-tionnaire (5PQ) (Table III) [Hakim andGrahame, 2003; Mulvey et al., 2013],although this has not been validated inchildren (see “Measurement Properties ofClinical Assessment Methods for ClassifyingGeneralized Joint Hypermobility—a Sys-tematic Review” by Juul-Kristensen et al.,this issue). If the Beighton score is 1 pointbelow the age- and sex-specific cut-offAND the 5PQ is ‘positive’ (¼ at leasttwo positive items), then a diagnosis ofGJH can be made.
For patients with lower Beightonscores, the assessment of other joints isoften considered, including temporo-mandibular joint, shoulder, hip, foot,wrist, ankle, and other digits. Increasedankle and wrist dorsiflexion, increasedinternal and external hip rotation, andpes planus have been correlated withBeighton score [Smits-Engelsman et al.,2011] However, similar concerns aboutage, gender, and environmental influ-ences as well as measurement method-ology and reliable cut-off values, limitsuch analysis as too subjective in thedetermination of GJH. Therefore, theuse of such measurements cannot befactored into a diagnostic algorithm atthis time. Obviously, more informationregarding the assessment methodology(ies) in the determination of GJH isneeded (see “Measurement Properties ofClinical Assessment Methods for ClassifyingGeneralized Joint Hypermobility—a

12If marfanoid features are present, considerother conditions such as: Marfan syndrome,Loeys–Dietz syndrome, congenital contracturalarachnodactyly, Shprintzen–Goldberg syn-drome, Stickler syndrome, Homocystinuria,multiple endocrine neoplasia type 2B, and thefamilial thoracic aortic aneurysmal disorders[Pyeritz and Loeys, 2012].Molecular testing formany of these conditions is clinically available.13While skin softness and texture remainsubjective, it is often very notable in someindividuals and useful when present but notquantifiable; we therefore recommend a highthreshold for positivity.14Skin extensibility as measured by pinchingand lifting the cutaneous and subcutaneouslayers of the skin on the volar surface at themiddle of the non-dominant forearm asdescribed in Remvig et al. [2009]. Skinextensibility of>1.5 cm is considered the upperend of normal. It is likely that the hyper-extensibility of the skin in hEDS overlapssignificantly with that of “normal” skin.Therefore, extensibility of more than 1.5 cmis “positive.” If extensibility >2.0 cm is presentespecially in combination with other cutaneousfeatures, such as papyraceous scars, molluscoidpseudotumors and/or subcutaneous spheroids,consider other EDS types as possible alternativediagnoses (mainly cEDS and classical-likeEDS).
16Atrophic scarring is defined as scars fromlinear traumatic lacerations or single-surgerythat are unusually shallow (i.e., thin and sunken)and/or wider than the original wound due toimpaired repair and subsequent dermal hypo-trophy. Atrophic scars as the result of multipleincisions, wound infections, or inflammatoryconditions (such as viral infections, cystic acne,etc.) are not to be considered. Ellipticalincisions (e.g., for removal of nevi) may bedifficult to assess without knowing the size ofthe original wound. True skin fragility, such asthe propensity to have an open wound due totrivial trauma, is not a typical feature of hEDS.Atrophic scarring in hEDS is mildly tomoderately different from that usually consid-ered typical of cEDS (Fig. 1).17Includes history of dental crowding ororthodontic intervention(s) to correct suchproblems. Both conditions must be positive tomeet this criterion.
18 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE
Systematic Review” by Juul-Kristensenet al., this issue).
Lastly, the use of the Beightonscoring system is meant to be adiagnostic screening method. It isunderstood that gender, age, ethnicity,strength training, stretching exercises,and warming up all affect JH andtherefore GJH. However, muscularovercompensation, injury and surgerycan cause either joint hypermobility orhypomobility. Muscular overcompensa-tion, such as tight hamstrings, can affectthe degree of knee extension and lumbarflexion negatively, while stretching ex-ercises andwarming up affects positively.Injury can destabilize a joint or alterna-tively reduce movement. Surgery cansimilarly affect a joint. For example, aperson with lumbar spine fusion maynot be able to have a “positive” forwardspinal flexion for Beighton scoring.There is a temptation by clinicians toconsider this a positive score but withoutcurrent ability or historical demonstra-tion, it should be scored negative. Anargument could be made to invalidatespinal flexion scoring thus the total scorewould be eight and not nine. However,it is not known if the numerator(determinant of GJH) should be ad-justed in this situation. In theory, thismakes sense but what is the appropriatecut-off? Therefore, like any clinical tool,there is some subjectivity and this is aguideline not to replace the judgment ofthe experienced clinician; however,standardization of performance proce-dures is required. One may want tolabel such persons as having “probableGJH” but at the present time, “probableGJH” should not be considered analternative of the objectively diagnosedGJH (as described above) into thediagnostic flow-chart of hEDS. Strongerscrutiny of phenocopies should becontemplated.
15Piezogenic papules are herniations of subcu-taneous fat often demonstrable in the heel uponstanding (Fig. 3). It is considered uncommon inchildren but can be found in adults with historyof prolonged standing (occupational), mara-thon runners, or weightlifters [Poppe andHamm, 2013] However, in a sex- and age-matched study of 29 Dutch EDS patients,piezogenic papules were found in 34.5% butnone in the control group [Kahana et al., 1987].
18Some studies show no increase in thefrequency of clinically significant MVP [Dolanet al., 1997; McDonnell et al., 2006; Atzingeret al., 2011] and others show an MVPfrequency of 28–67% among hEDS patients[Camerota et al., 2014; Kozanoglu et al., 2016].This feature is included in the diagnosticcriteria because it can be a marker of connectivetissue laxity, but is usually not clinicallysignificant in patients with hEDS.
Criterion 2: Two or More Amongthe Following Features (A–C)MUST Be Present (for Example:A and B; A and C; B and C;A and B and C)
Feature A: systemic manifestations of amore generalized connective tissue
disorder (a total of five must bepresent)12
1.
Unusually soft or velvety skin132.
Mild skin hyperextensibility143.
Unexplained striae such as striaedistensaeor rubrae at the back, groins,thighs, breasts and/or abdomen inadolescents, men or prepubertalwomen without a history of signifi-cant gain or loss of body fat or weight4.
Bilateral piezogenic papules of theheel155.
Recurrent or multiple abdominalhernia(s) (e.g., umbilical, inguinal,crural)6.
Atrophic scarring involving at leasttwo sites and without the formation oftruly papyraceous and/or hemosidericscars as seen in classical EDS167.
Pelvic floor, rectal, and/or uterineprolapse in children, men or nullipa-rous women without a history ofmorbid obesity or other known pre-disposing medical condition8.
Dental crowding and high or narrowpalate179.
Arachnodactyly, as defined in one ormore of the following: (i) positivewrist sign (Steinberg sign) on bothsides; (ii) positive thumb sign (Walkersign) on both sides10.
Arm span-to-height �1.05 11. Mitral valve prolapse (MVP) mild orgreater based on strict echocardio-graphic criteria18
12.
Aortic root dilatation with Z-score>þ2Feature B: positive family history,with one or more first degree relatives

ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 19
independently meeting the currentdiagnostic criteria for hEDS.
Feature C: musculoskeletal com-plications (must have at least one):
1.
19“
bopotheof20Rexacoandusi
Musculoskeletal pain in two or morelimbs, recurring daily for at least 3months
2.
Chronic, widespread pain for �3months3.
Recurrent joint dislocations or frankjoint instability, in the absence oftrauma (a or b)19a. Three or more atraumatic disloca-tions in the same joint or twoormoreatraumatic dislocations in two differ-ent joints occurring at different times
b. Medical confirmation of joint insta-bility at two or more sites not related
Disnesitiopatheefmpunt
dng
to trauma20
Criterion 3: All the FollowingPrerequisites MUST Be Met
1.
Absence of unusual skin fragility, whichshould prompt consideration of othertypes of EDS2.
Exclusion of other heritable and acquiredconnective tissue disorders, includingautoimmune rheumatologic conditions.In patients with an acquired connectivetissue disorder (e.g., lupus, rheumatoidarthritis, etc.), additional diagnosis ofhEDS requires meeting both Features Aand B of Criterion 2. Feature C ofCriterion 2 (chronic pain and/or insta-bility) cannot be counted towards adiagnosis of hEDS in this situation.3.
Exclusion of alternative diagnoses thatmay also include joint hypermobilityby means of hypotonia and/or connec-tive tissue laxity. Alternative diagnosesand diagnostic categories include, butare not limited to, neuromuscularlocation” is defined as displacement of aout of the joint socket (or out of normaln in the case of sesamoid bones such astella), sufficiently severe to limit motionjoint and requiring manual reduction.ers to sites regardless of laterality. Forle, right and left patellar instability wouldas two. Instability should be evaluatedetermined by a qualified practitionerrecommended guidelines.
21Abilmohav[By
disorders (e.g., myopathic EDS, Beth-lem myopathy), other HCTD (e.g.,other types of EDS, Loeys–Dietzsyndrome, Marfan syndrome), andskeletal dysplasias (e.g., OI). Exclusionof these considerations may be basedupon history, physical examination,and/or molecular genetic testing, asindicated.• General commentMany other features are described inhEDS but most are not sufficientlyspecific nor sensitive at the moment tobe included in formal diagnostic crite-ria (see “Hypermobile Ehlers–DanlosSyndrome (a.k.a. Ehlers–Danlos Syn-drome Type III and Ehlers–Danlos syn-drome hypermobility type): ClinicalDescription, and Natural History” byTinkle et al., this issue). These includebut are not limited to: sleep distur-bance, fatigue, postural orthostatictachycardia, functional gastrointestinaldisorders, dysautonomia, anxiety, anddepression. These other systemic man-ifestations may be more debilitatingthan the joint symptoms, often impairfunctionality and quality of life, andshould always be determined duringclinical encounters. While they are notpart of the diagnostic criteria, thepresence of such systemic manifesta-tions may prompt consideration ofhEDS in the differential diagnosis.Future research will need to focus onsuch symptoms to validate any associa-tion with hEDS, describe sub-groupsor sub-phenotypes, and be focused onevidence-based management of thesymptoms in the context of hEDS.
Arthrochalasia EDS (aEDS)
•
Inheritance Autosomal dominant Major criteria • 1. Congenital bilateral hip dislocation21llateleceer
reported aEDS patients had congenitalral hip dislocation. One unreportedularly proven aEDS patient is known tohad congenital unilateral hip dislocations et al., personal communication].
22
“C
2. Severe GJH, with multiple disloca-tions/subluxations22
3. Skin hyperextensibility22
Forlas
Minor criteria
• 1. Muscle hypotonia2. Kyphoscoliosis3. Radiologically mild osteopenia4. Tissue fragility, including atrophicscars5. Easy bruisable skin
Minimal criteria suggestive for aEDS: • – Major criterion (1): Congenital bilateral hip dislocationPlus
– Either major criterion (3): skinhyperextensibility– Or major criterion (2): severe GJHwithmultipledislocations/subluxations
and at least two other minor criteriaConfirmatory molecular testing isobligatory to reach a final diagnosis.
•
Molecular basisaEDS is caused by heterozygous muta-tions in either COL1A1 or COL1A2,that cause entire or partial loss of exon 6of the respective gene. No other genesare associated with aEDS.•
Verification of diagnosisMolecular screening by Sanger sequenc-ing of COL1A1 and COL1A2, ortargeted resequencing of a gene panelthat includes these genes, is indicated.When no mutation is identified, thisapproach should be complemented witha CNV detection strategy to identifylarge deletions or duplications.In case of unavailability of genetictesting, SDS PAGE of the pepsin-digested collagen in the medium orcell layer of cultured dermal fibroblastsdemonstrates the presence of a mutantpNa1(I) or pNa2(I) chain (precursorprocollagen chains in which the carboxy(C)-but not the amino (N)-propetide iscleaved off).TEMof skin specimens shows loosely
and randomly organized collagen fibrilswith a smaller and more variable diame-ter, and an irregular outline. Thesefindings may support the diagnosis, butcannot confirm it.Absence of a causative mutation in
COL1A1 or COL1A2 that leads to
definition of GJH, see criteria forsical EDS.”

23
prlidfoscsuhy24
coskblne25
“C26
sefirco
20 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE
complete or partial deletion of the exon6 of either gene excludes the diagnosis ofaEDS.
Dermatosparaxis EDS (dEDS)
•
Inheritance Autosomal recessive Major criteria: • 1. Extreme skin fragility with congeni-tal or postnatal skin tears2. Characteristic craniofacial features,
which are evident at birth orearly infancy, or evolve later inchildhood23
3. Redundant, almost lax skin, withexcessive skin folds at the wrists andankles
4. Increased palmar wrinkling5. Severe bruisability with a risk of
subcutaneous hematomas andhaemorrhage
6. Umbilical hernia7. Postnatal growth retardation8. Short limbs, hand and feet9. Perinatal complications due to con-
Craotus alds,leraturepopRepnneulle uonaForlasMoverestndi
nective tissue fragility24
•
Minor criteria 1. Soft and doughy skin texture2. Skin hyperextensibility3. Atrophic scars4. GJH255. Complications of visceral fragility(e.g., bladder rupture, diaphrag-matic rupture, rectal prolapse)
6. Delayed motor development26
7. Osteopenia
nbn
e,slocfrmt
sist
mti
iofacial features include: prominent anderant eyes with puffy, oedematous eye-d excessive periorbital skin, epicanthaldownslanting palpebral fissures, bluelarge fontanels and/or wide cranial
, delayed closure of fontanels andastic chin.rted perinatal complications due totive tissue fragility include: congenitalactures, intracerebral hemorrhage, fria-bilical cord, congenital skin tears,
al pneumothorax.definition of GJH, see criteria forcal EDS.”patients identified to date display a
phenotype, recognizable from birth oronths of life. Milder forms of theon have recently been described.
8. Hirsutism9. Tooth abnormalities10. Refractive errors (myopia,
astigmatism)11. Strabismus
Minimal criteria suggestive for dEDS: • – Majorcriterion (1): extremeskin fragility– AND major criterion (2): character- istic craniofacial featuresPlus
– Either: one other major criterion– And/or: three minor criteria Confirmatory molecular testing isobligatory to reach a final diagnosis.•
Molecular basisdEDS is caused by biallelic mutationsin ADAMTS2, the gene encodingADAMTS-2, the main procollagen IN-proteinase. It is the only geneassociated with dEDS.•
27Muscular hypotonia can be very pronouncedand lead to delayed gross motor development.This condition should be considered in theinitial differential diagnosis of a floppy infant.Neuromuscular work-up is however normal.28Kyphoscoliosis is usually present at birth ordevelops in infancy. In patients with biallelicPLOD1 mutations, it may be absent through-out adulthood.29For definitions of GJH and skin hyper-extensibility, see criteria for “Classical EDS.”30Scleral and ocular fragility were removed from
Verification of diagnosisMolecular screening by Sanger sequenc-ing of targeted resequencing of a genepanel that includes ADAMTS2 is indi-cated. When no, or only one, causativemutation is identified, this approachshould be complemented with a CNVdetection strategy to identify largedeletions or duplications.
In case of unavailability of genetictesting, SDS PAGE demonstrates pres-ence of pNa1(I) and pNa2(I) chains oftype I procollagen extracted fromdermisin the presence of protease inhibitors ordetected in fibroblast cultures.
TEMshows collagen fibrils in affectedskin specimens with a hieroglyphicpattern. These ultrastructural findingsare usually typical but may be almostindistinguishable from those observed inaEDS. As such, they are not sufficient toconfirm the diagnosis.
Absence of these confirmatory find-ings does not exclude the diagnosisof dEDS, as specific types of mutations(e.g., deep intronic mutations) may goundetected by standard diagnostic mo-lecular techniques; however, alternativediagnoses should be considered in theabsence of ADAMTS2 mutations.
the major clinical criteria of kEDS-PLOD1, asrupture of the eye globe following minimaltrauma has only been reported in five individuals,
Kyphoscoliotic (kEDS) including one patient with both eyes affected.31Facial dysmorphic features include: low-setears, epicanthal folds, down-slanting palpebral • Inheritance fissures, synophrys, and high palate. Autosomal recessiveMajor criteria
• 1. Congenital muscle hypotonia272. Congenital or early onset kypho-scoliosis (progressive or non-progressive)28
3. GJH29 with dislocations/subluxa-tions (shoulders, hips, and knees in
particular)•
Minor criteria: 1. Skin hyperextensibility292. Easy bruisable skin3. Rupture/aneurysm of a medium-
sized artery4. Osteopenia/osteoporosis5. Blue sclerae6. Hernia (umbilical or inguinal)7. Pectus deformity8. Marfanoid habitus9. Talipes equinovarus10. Refractive errors (myopia,
hypermetropia)
• Gene-specific minor criteria1. PLOD11. Skin fragility (easy bruising, fria-
ble skin, poor wound healing,widened atrophic scarring)
2 Scleral and ocular fragility/rupture30
3. Microcornea4. Facial dysmorphology31
2. FKBP141. Congenital hearing impairment
(sensorineural, conductive, ormixed)
2. Follicular hyperkeratosis3. Muscle atrophy4. Bladder diverticula

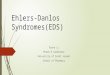
Figure 3. Piezogenic papules of the feet which are subcutaneous fat herniationsthrough the fascia. They often appear as blanching white nodules only while bearingweight.
ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 21
•
Minimal criteria suggestive for kEDS: – Major criterion (1): congenital mus-cle hypotonia– AND major criterion (2): congenital
or early-onset kyphoscoliosisPlus
– Either major criterion (3): GJH– And/or three minor criteria(either general or gene-specific criteria)Confirmatory molecular testing isobligatory to reach a final diagnosis.
•
Molecular basisThe majority of patients with kEDSharbor biallelic mutations in PLOD1,the gene encoding the collagen-modifying enzyme procollagen-ly-sine, 2-oxoglutarate 5-dioxygenase 1(PLOD1 or LH1 [lysylhydroxylase1]).LH1 plays an important role as apost-translational modifying enzymein collagen biosynthesis through(i) hydroxylation of helical lysylresidues in—Xaa-Lys-Gly-collagensequences to hydroxy-lysyl residueswhich serve as sites of attachmentfor carbohydrate units (either galactoseor glucosyl-galactose) and (ii) inthe formation of intra- and inter-molecular collagen cross-links. LH1deficiency results in underhydroxy-lation of lysyl residues and underglyco-sylation of hydroxylysyl residues incollagens and, hence, impaired cross-link formation with consequent me-chanical instability of the affectedtissues.The majority of patientswith kEDS harbor biallelicmutations in PLOD1, thegene encoding the collagen-
modifying enzymeprocollagen-lysine, 2-
oxoglutarate 5-dioxygenase1 (PLOD1 or LH1[lysylhydroxylase1]).
Recently, biallelic mutations havebeen identified in FKBP14, encodingFKBP22, a member of the F506-binding family of peptidyl-prolyl cis-trans isomerases, in patients displaying aphenotype that clinically largely over-laps with kEDS-PLOD1 [Baumannet al., 2012].
•
Verification of diagnosisLaboratory confirmation of kEDSshould start with the quantification ofdeoxypyridinoline (Dpyr or LP forlysyl-pyridinoline) and pyridinoline(Pyr or HP for hydroxylysyl-pyridino-line) cross-links in urine quantitated bymeans of high-performance liquidchromatography (HPLC). An increasedDpyr/Pyr ratio is a highly sensitive andspecific test for kEDS caused by biallelicPLOD1 mutations (kEDS-PLOD1),but is normal for biallelic FKBP14mutations (kEDS-FKBP14).The normal ratio of Dpyr/Pyr cross-
links is approximately 0.2, whereas inkEDS-PLOD1 the ratio is significantlyincreased (approximately 10–40 timesincrease, range 2–9). This method is fastand cost-effective and it can also be usedto determine the pathogenic status of aVUS in PLOD1.SDS–PAGE may detect faster migra-
tion of underhydroxylated collagenchains and their derivatives in kEDS-PLOD1 but not in kEDS-FKBP14.However, abnormalities in migrationcan be subtle.
Molecular analysis for kEDS-PLOD1 may start with MLPA analysisof PLOD1, for the evaluation of thecommon intragenic duplication inPLOD1 caused by an Alu-Alu recom-bination between introns 9 and 16 (themost common mutant allele) [Hautalaet al., 1993].
Molecular screening by means oftargeted resequencing of a gene panelthat includes PLOD1 and FKBP14, isindicated when MLPA of PLOD1 failsto identify the common duplication.Such a gene panel my also include othergenes associated with phenotypes thatclinically overlap with kEDS, such asZNF469, PRDM5, B4GALT7,B3GALT6, SLC39A13, CHST14,and DSE. Alternatively, WES may beperformed. When no, or only one,causative mutation is identified, thisapproach should be complementedwith a CNV detection strategy toidentify large deletions or duplicationsin these genes.
TEM on skin specimens has shownvariable diameters and abnormal con-tours of the collagen fibrils and irregularinterfibrillar space, but these abnormal-ities are not unique to this condition. Assuch, whereas TEM on a skin biopsy cansupport diagnosis, it cannot confirm it.
Whereas absence of an abnormalurinary LP/HP ratio excludes thediagnosis of kEDS-PLOD1, absence ofthe confirmatory genetic findings doesnot exclude the diagnosis of kEDS, asspecific types of mutations (e.g., deepintronic mutations) may go undetected

22 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE
by standard diagnostic molecular tech-niques and/or other, yet to be discov-ered, genes, may be associated with thisphenotype; however, alternative diag-noses should be considered in theabsence of PLOD1 or FKBP14mutations.
Brittle Cornea Syndrome (BCS)
•
Inheritance Autosomal recessive Major criteria • 1. Thin cornea, with or without rup-ture (central corneal thickness often<400mm)
2. Early onset progressive keratoconus3. Early onset progressive keratoglobus4. Blue sclerae
Minor criteria •33Characteristic craniofacial features associatedwith biallelic B4GALT7 mutations include:triangular face, wide-spaced eyes, proptosis,narrow mouth, low-set ears, sparse scalp hair,abnormal dentition, flat face, wide forehead,blue sclerae, and cleft palate/bidif uvula.
1. Enucleation or corneal scarring as aresult of previous rupture
2. Progressive loss of corneal stromaldepth, especially in central cornea
3. High myopia, with normal ormoderately increased axial length
4. Retinal detachment5. Deafness, oftenwithmixed conduc-
tive and sensorineural components,progressive, higher frequencies of-ten more severely affected (“slop-ing” pure tone audiogram),
6. Hypercompliant tympanicmembranes
7. Developmental dysplasia of the hip8. Hypotonia in infancy, usually mild
if present9. Scoliosis10. Arachnodactyly11. Hypermobility of distal joints12. Pes planus, hallux valgus13. Mild contractures of fingers (espe-
cially 5th)14. Soft, velvety skin, translucent skin
34Reported radiographic findings associated
Minimal criteria suggestive for kEDS: • with biallelic B4GALT7 mutations include:include radioulnar synostosis, metaphysealflaring, osteopenia, radial head subluxation or– Major criterion (1): thin cornea,with or without rupture (centralcorneal thinckness often < 100
dislocation, and short clavicles with broad
micrometer) medial ends.35 Plus Characteristic craniofacial features associatedwith biallelic B3GALT6 mutations include:midfacial hypoplasia, frontal bossing, proptosis,or prominent eyes, blue sclerae, downslanting
– Either: at least one other majorcriterion
– And/or three other minor criteria
32For definitions of GJH and skin hyper-extensibility, see criteria for “Classical EDS.”
palpebral fissures, depressed nasal bridge, longupperlip, low-set ears, micrognathia, abnormaldentition, cleft palate, sparse hair.
Confirmatory molecular testing isobligatory to reach a final diagnosis
•
Molecular basisBCS is caused by biallelic mutations ineither ZNF469, encoding ZNF469, azinc finger protein of unknown func-tion, or PRDM5, encoding a DNA-binding transcription factor of the PR/SET protein family that lacks theintrinsic histon methyltransferase activ-ity. At least one family with a clinicalBCS phenotype did not harbor muta-tions in these genes, suggesting that atleast one other gene might be associatedwith BCS [Rohrbach et al., 2013].•
Verification of diagnosisMolecular screening by means of tar-geted resequencing of a gene panel thatincludes ZNF469 and PRDM5 isindicated. Such a gene panel my alsoinclude other genes associated withphenotypes that clinically overlap withBCS, such as PLOD1, FKBP14,B4GALT7, B3GALT6, SLC39A13,CHST14 and DSE. Alternatively,WES may be performed. When no,or only one, causative mutation isidentified, this approach should becomplemented with a CNV detectionstrategy to identify large deletions orduplications in these genes.Absence of these confirmatory find-ings does not exclude the diagnosis, asspecific types of mutations (e.g., deepintronic mutations) may go undetectedby standard diagnostic molecular tech-niques, and other, yet unknown genes,might be associated with BCS.
Spondylodysplastic EDS (spEDS)
•
Inheritance Autosomal recessive Major criteria • 1. Short stature (progressive inchildhood)2. Muscle hypotonia (ranging from
severe congenital, to mild later-onset)
3. Bowing of limbs
Minor criteria • 1. Skin hyperextensibility,32 soft,doughy skin, thin translucent skin2. Pes planus
3. Delayed motor development4. Osteopenia5. Delayed cognitive development
Gene-specific minor criteria • – B4GALT7– Radioulnar synostosis– Bilateral elbow contractures orlimited elbow movement
– GJH32
– Single transverse palmar crease– Characteristic craniofacialfeatures33
– Characteristic radiographicfindings34
– Severe hypermetropia– Clouded cornea
– B3GALT6– Kyphoscoliosis (congenital or earlyonset, progressive)
– Joint hypermobility, generalized orrestricted to distal joints, with jointdislocations
– Joint contractures (congenital orprogressive) (especially hands)
– Peculiar fingers (slender, tapered,arachnodactyly, spatulate, withbroad distal phalanges)
– Talipes equinovarus– Characteristic craniofacialfeatures35
– Tooth discoloration, dysplasticteeth

36
wplshtabphmtuosanon37
bimosprra
ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 23
– Characteristic radiographicfindings36
– Osteoporosis with multiple spon-taneous fractures
– Ascending aortic aneurysm– Lung hypoplasia, restrictive lungdisease
– SLC39A13:– Protuberant eyes with bluishsclerae
– Hands with finely wrinkled palms– Atrophy of the thenar muscles, andtapering fingers
– Hypermobility of distal joints– Characteristic radiologic findings37
Reithatyortulysalabuteod reRealleodteooxl n
pobspoilareallignlatipoadpatpolicerapeimeck
Minimal criteria suggestive for spEDS:
• – Major criterion (1): short stature– AND major criterion (2): muscle hypotoniaPlus
– Characteristic radiographic abnor-malities and at least three other minor criteria (general or type-specific)Confirmatory molecular testing isobligatory to reach a final diagnosis
•
Molecular basisspEDS is caused by either: – Biallelic mutations in B4GALT7,encoding galactosyltransferase I(b1,4-galactosyltransferase 7 orb4GalT7), which catalyzes the trans-fer of the first galactose to thexylose residue in tetrasaccharidelinker region of glycosaminoglycans(GAGs).– Biallelic mutations in B3GALT6,encoding galactosyltransferase II(b1,3-galactosyltransferase 6 orb3GalT6), which catalyzes the
rted radiographic features associatediallelic B3GALT6 mutations include:ndyly, anterior beak of vertebral body,ium, prominent lesser trochanter, ace-dysplasia, metaphyseal flaring, meta-dysplasia of femoral head, elbowment, radial head dislocation, over-on, bowing of long bones, generalizedrosis, healed fractures. Craniosynostosisioulnar dysostosis has been reported inient.rted radiologic findings associated withSLC39A13mutations include: mild tote platyspondyly, mild to moderatenia of the spine, small ileum, flatal femoral epiphyses, short, wide femo-s.
transfer of the second galactose to thefirst galactose residue in tetrasacchar-ide linker region of GAGs.
– Biallelic mutations in SLC39A13,encoding the homodimeric trans-membrane Zrt/irt-like protein 13(ZIP13) protein, a member of theSLC39A/ZIP family that regulates
the influx of Zn into the cytosol.•
38Characteristic craniofacial features include:large fontanelle, hypertelorism, short anddownslanting palpebral fissures, blue sclerae,short nose with hypoplastic columella, low-setand rotated ears, high palate, long philtrum,thin upper lip vermilion, small mouth, micro-retrognathia.39For definition of skin hyperextensibility, seecriteria for “Classical EDS.”40The phenotypic features in the three reportedpatients with EDS caused by DSE deficiencyseem to be milder than those in patients withEDS caused by D4ST1-deficiency, but identi-fication of additional patients with DSE-deficiency is needed to confirm this correlation.
Verification of diagnosisMolecular screening by means of tar-geted resequencing of a gene panel thatincludes B4GALT7, B3GALT6, andSLC39A13 is indicated. Such a genepanel may also include other genesassociated with phenotypes that clini-cally overlap with spEDS, such asPLOD1, FKBP14, ZNF469,PRDM5, CHST14, andDSE. Alterna-tively, WES may be performed. Whenno, or only one, causative mutation isidentified, this approach should becomplemented with a CNV detectionstrategy to identify large deletions orduplications in these genes.
For definite proof of GAG deficiency(B4GALT7 and B3GALT6mutations),biochemical methods to assess GAGsynthesis in patients’ cultured fibroblastsare currently available in many special-ized laboratories [Talhaoui et al., 2010].
The laboratory measurement of uri-nary pyridinolines, lysyl-pyridinoline(LP) and hydroxylysyl-pyridinoline(HP) quantitated by HPLC allowsthe detection of an increased ratio LP/HP to approximately 1, (compared to anormal values of approximately 0.2) inpatients with mutations in SLC39A13[Giunta et al., 2008]. This fast and cost-effective method can also be used todetermine the pathogenic status of aVUS (see also “verification of diagno-sis” in kEDS-PLOD1).
Absence of confirmatory geneticfindings does not exclude the diagnosisof spEDS, as specific types of mutations(eg deep intronic mutations) may goundetected by standard diagnosticmolecular techniques, and still other,yet to be discovered, genes may beassociated with these phenotypes. Incase no B4GALT7, B3GALT6, orSCL39A13 mutations are identified,alternative diagnoses should however beconsidered.
Musculocontractural EDS(mcEDS)
•
Inheritance Autosomal recessive Major criteria • 1. Congenital multiple contractures,characteristically adduction-flexioncontractures and/or talipes equino-varus (clubfoot)
2. Characteristic craniofacial features,which are evident at birth or in earlyinfancy38
3. Characteristic cutaneous features in-cluding skin hyperextensibility39,easy bruisability, skin fragility withatrophic scars, increased palmar
wrinkling•
Minor criteria 1. Recurrent/chronic dislocations402. Pectus deformities (flat, excavated)3. Spinal deformities (scoliosis,
kyphoscoliosis)4. Peculiar fingers (tapering, slender,
cylindrical)5. Progressive talipes deformities (val-
gus, planus, cavum)6. Large subcutaneous hematomas7. Chronic constipation8. Colonic diverticula9. Pneumothorax/
pneumohemothorax10. Nephrolithiasis/cystolithiasis11. Hydronephrosis12. Cryptorchidism in males13. Strabismus14. Refractive errors (myopia,
astigmatism)15. Glaucoma/elevated intraocular
pressure

24 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE
•
Minimal criteria suggestive for mcEDS: – At birth or in early childhood: Majorcriterion (1): Congenital multiplecontractures AND (2) characteristiccraniofacial features– In adolescence and in adulthood:Major criterion (1): Congenital mul-tiple contractures AND (3) charac-
teristic cutaneous featuresConfirmatory molecular testing isobligatory to reach a final diagnosis.
•
Molecular basismcEDS is caused by biallelic mutationsin CHST14, encoding D4ST1, asingle-exon gene encoding carbohy-drate sulfotransferase 14 or dermatan 4-O-sulfotransferase 1, an enzyme in-volved in the biosynthesis of the GAGdermatan sulfate. It catalyzes 4-O-sulfation of N-acetylgalactosamine(GalNAc) in the sequence “L-iduronicacid (IdoA)-GalNAc,” immediately af-ter epimerization of D-glucuronic acid(GlcA) to IdoA by dermatan sulfateepimerase (DSE).41So far, five families have been reported: fourwith an autosomal dominant condition and onewith an autosomal recessive condition. Theaffected siblings from the family with theautosomal recessive condition have a moresevere form of the condition than patients withautosomal dominant inheritance [Zou et al.,2014].42
mcEDS is caused bybiallelic mutations in
CHST14, encoding D4ST1,a single-exon gene encodingcarbohydrate sulfotransferase
14 or dermatan 4-O-sulfotransferase 1, anenzyme involved in thebiosynthesis of the GAG
dermatan sulfate.
Muscle biopsy and skin fibroblast culturestudies: the diagnosis can be suspected in
patients that undergo a muscle biopsy and/orin whom a fibroblast line is established. In theautosomal recessive form in which there is noA fewmutations have been identified inthe DSE gene, encoding DSE, inpatients with a similar phenotype.
collagen XII produced, immunostaining has
• shown absence of collagen XII staining. Inmissense mutations that lead to autosomaldominant forms, collagen XII may be abnor-mally secreted. The myopathic pattern onmuscle biopsy may be suggestive, but is notdiagnostic. Recently, muscle MRI has beendeveloped as an alternative, non-invasivetechnique to study muscle involvement, how-ever it is not specific enough to confirm thediagnosis.Verification of diagnosisMolecular screening by means of tar-geted resequencing of a gene panel thatincludes CHST14 and DSE is indi-cated. Such a gene panel my also includeother genes associated with phenotypesthat clinically overlap with mcEDS,such as PLOD1, FKBP14, ZNF469,PRDM5, B4GALT7, B3GALT6, andSLC39A13. Alternatively,WESmay be
performed. When no, or only one,causative mutation is identified, thisapproach should be complementedwith a CNV detection strategy toidentify large deletions or duplicationsin these genes.
Absence of these confirmatory find-ings does not exclude the diagnosis ofmcEDS, as specific types of mutations(e.g., deep intronic mutations) may goundetected by standard diagnosticmolecular techniques. In case noCHST14 or DSE mutations are iden-tified, alternative diagnoses should beconsidered.
Myopathic EDS (mEDS)
•
Inheritance Autosomal dominant or autosomal recessive•
Major criteria 1. Congenital muscle hypotonia, and/or muscle atrophy, that improveswith age41
2. Proximal joint contractures (knee,hip, and elbow)42
3. Hypermobility of distal joints
Minor criteria • 1. Soft, doughy skin2. Atrophic scarring3. Motor developmental delay4. Myopathy on muscle biopsy
Minimal clinical criteria suggestive for • mEDS: – Major criterion (1): congenital mus- cle hypotonia that improves with agePlus
– Either: one other major criterion– And/or: three minor criteria Confirmatory molecular testing isobligatory to reach a final diagnosis.•
Molecular basismEDS is caused by heterozygous orbiallelic mutations in COL12A1, en-coding type XII collagen. The clinicalphenotype highly overlaps with colla-gen type VI-related myopathies, that is,Bethlem Myopathy, and Ullrich Con-genital Muscular Dystrophy. It is cur-rently unknown whether other, yet tobe discovered genes, are associated withthis phenotype.•
Verification of diagnosisMolecular screening by means of tar-geted resequencing of a gene panel thatincludes COL12A1 is indicated. Such agene panel my also include other genesassociated with phenotypes that clini-cally overlap with mEDS, such asCOL6A1, COL6A2, COL6A3. Alter-natively, WES may be performed.When no, or only one, causativemutation is identified, this approachshould be complemented with a CNVdetection strategy to identify largedeletions or duplications in thesegenes.Absence of these confirmatoryfindings does not exclude the diag-nosis, as specific types of mutations(eg deep intronic mutations) may goundetected by standard diagnosticmolecular techniques, and other,yet to be discovered, genes may beassociated with this phenotype. Incase no COL12A1 mutations areidentified alternative diagnoses, espe-cially collagen VI-related UllrichCongenital Muscular Dystrophy andBethlem Myopathy, should beconsidered.
Periodontal EDS (pEDS)
•
Inheritance Autosomal dominant
ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) 25
Major criteria
• – Severe and intractable periodontitisof early onset (childhood oradolescence)– Lack of attached gingiva– Pretibial plaques– Family history of a first-degree rela-
tive who meets clinical criteria•
Minor criteria – Easy bruising– Joint hypermobility, mostly distaljoints– Skin hyperextensibility43 and fragil-ity, abnormal scarring (wide oratrophic)
– Increased rate of infections– Hernias– Marfanoid facial features– Acrogeria– Prominent vasculature
Minimal criteria suggestive for pEDS: • – Major criterion (1): severe andintractable periodontitis of early on-set (childhood or adolescence)– OR major criterion (2): lack of
attached gingivaPlus
– At least two other major criteria and one minor criterionConfirmatory molecular testing isobligatory to reach a final diagnosis.
•
Molecular basispEDS is caused by heterozygous gain-of-function mutations in C1R or C1S,encoding subunits C1r and C1s of thefirst component of the classical comple-ment pathway.•
Verification of diagnosisIdentification of known or compatiblemutations by sequence analysis ofC1R and C1S. Large deletions or nullmutations that completely remove C1ror C1s protein function do not causepEDS.At present it cannot be statedwhether absence of a C1R or C1Smutations excludes the diagnosis be-cause the experience with the molecu-lar diagnosis is limited.
CONCLUDING REMARKS
We hope that the revised InternationalEDS criteria will serve as a new, albeitprovisional, standard for the diagnosisof EDS. Our proposal has the aim of
facilitating accurate and timely diagno-sis, and improve the diagnostic unifor-mity for clinical and research purposes,genetic counseling, management, natu-ral history studies, and identification ofpotential areas of research. Future revi-sion of this EDS Classification will beplanned within the framework of theInternational EDS Consortium and theEhlers–Danlos Society.
ACKNOWLEDGMENTS
We are very grateful for the cooperationof many patients and their families allover the world. We thank ProfessorStephen Robertson and PVNH supportfor their help with PVNH-EDS. Wealso wish to acknowledge the contribu-tions of many professionals and laypersons alike to this endeavour. Wewould like to thank our generoussponsors including, but not limited to,The Ehlers–Danlos National Founda-tion, the Ehlers–Danlos Support UK,and the Ehlers–Danlos Society. Fran-siska Malfait is Senior Clinical Investi-gator at the Fund for Scientific ResearchFlanders.
REFERENCES
Atzinger CL, Meyer RA, Khoury PR, Gao Z,Tinkle BT. 2011. Cross-sectional and lon-gitudinal assessment of aortic root dilationand valvular anomalies in hypermobile andclassic Ehlers-Danlos syndrome. J Pediatr158:826–830e821.
Baumann M, Giunta C, Krabichler B, Ruschen-dorf F, Zoppi N, Colombi M, Bittner RE,Quijano-Roy S, Muntoni F, Cirak S,Schreiber G, Zou Y, Hu Y, Romero NB,Carlier RY, Amberger A, Deutschmann A,Straub V, Rohrbach M, Steinmann B,Rostasy K, Karall D, Bonnemann CG,Zschocke J, Fauth C. 2012. Mutations inFKBP14 cause a variant of Ehlers-Danlossyndrome with progressive kyphoscoliosis,myopathy, and hearing loss. Am J HumGenet 90:201–216.
Beighton P, de Paepe A, Danks D, Finidori G,Gedde-Dahl T, Goodman R, Hall JG,Hollister DW, Horton W, McKusick VA,et al. 1988. International nosology ofheritable disorders of connective tissue,Berlin, 1986. Am J Med Genet 29:581–594.
Beighton P, De Paepe A, Steinmann B, TsipourasP, Wenstrup RJ. 1998. Ehlers-Danlos syn-dromes: Revised nosology, villefranche,1997. ehlers-Danlos national foundation(USA) and ehlers-Danlos support group(UK). Am J Med Genet 77:31–37.
Camerota F, Castori M, Celletti C, Colotto M,Amato S, Colella A, Curione M, Danese C.2014. Heart rate, conduction and ultrasoundabnormalities in adults with joint hypermo-bility syndrome/Ehlers-Danlos syndrome,hypermobility type. Clin Rheumatol33:981–987.
Dolan AL,MishraMB,Chambers JB, GrahameR.1997. Clinical and echocardiographic surveyof the Ehlers-Danlos syndrome. Br JRheumatol 36:459–462.
Giunta C, ElScioglu NH, Albrecht B, Eich G,Chambaz C, Janecke AR, Yeowell H, WeisM, Eyre DR, Kraenzlin M, Steinmann B.2008. Spondylocheiro dysplastic form of theEhlers-Danlos syndrome—An autosomal-recessive entity caused by mutations in thezinc transporter gene SLC39A13. Am JHum Genet 82:1290–1305.
Hakim AJ, Grahame R. 2003. A simple question-naire to detect hypermobility: An adjunct tothe assessment of patients with diffusemusculoskeletal pain. Int J Clin Pract57:163–166.
Hautala T, Heikkinen J, Kivirikko KI, Myllyla R.1993. A large duplication in the gene forlysyl hydroxylase accounts for the type VIvariant of Ehlers-Danlos syndrome in twosiblings. Genomics 15:399–404.
Kahana M, Feinstein A, Tabachnic E, Schewach-Millet M, Engelberg S. 1987. Painfulpiezogenic pedal papules in patients withEhlers-Danlos syndrome. J Am Acad Der-matol 17:205–209.
Kozanoglu E, Coskun Benlidayi I, Akilli R, TasalA. 2016. Is there any link between jointhypermobility and mitral valve prolapse inpatients with fibromyalgia syndrome? ClinRheumatol 35:1041–1044.
Malfait F, Symoens S, Coucke P, Nunes L, DeAlmeida S, De Paepe A. 2006. Total absenceof the alpha2(I) chain of collagen type Icauses a rare form of Ehlers-Danlos syn-dromewith hypermobility and propensity tocardiac valvular problems. J Med Genet 43:e36.
Malfait F, Symoens S, De Backer J, Hermanns-LeT, SakalihasanN, LapiereCM,Coucke P, DePaepe A. 2007a. Three arginine to cysteinesubstitutions 4 in the pro-alpha (I)-collagenchain cause Ehlers-Danlos syndrome with apropensity to arterial rupture in earlyadulthood. Human Mutation 28:387–395.
Malfait F, Symoens S, De Backer J, Hermanns-LeT, SakalihasanN, LapiereCM,Coucke P, DePaepe A. 2007b. Three arginine to cysteinesubstitutions in the pro-alpha (I)-collagenchain cause Ehlers-Danlos syndrome with apropensity to arterial rupture in earlyadulthood. Hum Mutat 28:387–395.
McDonnell NB, Gorman BL, Mandel KW,Schurman SH, Assanah-Carroll A, MayerSA, Najjar SS, Francomano CA. 2006.Echocardiographic findings in classical andhypermobile Ehlers-Danlos syndromes. AmJ Med Genet A 140A:129–136.
McKay MJ, Baldwin JN, Ferreira P, Simic M,Vanicek N, Hiller CE, Nightingale EJ,Moloney NA, Quinlan KG, Pourkazemi F,Sman AD, Nicholson LL, Mousavi SJ, RoseK, Raymond J, Mackey MG, Chard A,Hubscher M, Wegener C, Fong Yan A,Refshauge KM, Burns J, Norms Project C.2016. 1000 Norms Project: Protocol of a

26 AMERICAN JOURNAL OF MEDICAL GENETICS PART C (SEMINARS IN MEDICAL GENETICS) ARTICLE
cross-sectional study cataloging human vari-ation. Physiotherapy 102:50–56.
Mulvey MR, Macfarlane GJ, Beasley M, Sym-mons DP, Lovell K, Keeley P, Woby S,McBeth J. 2013. Modest association of jointhypermobility with disabling and limitingmusculoskeletal pain: Results from a large-scale general population-based survey. Ar-thritis Care Res (Hoboken) 65:1325–1333.
Poppe H, Hamm H. 2013. Piezogenic papulesin Ehlers-Danlos syndrome. J Pediatr 163:1788.
Pyeritz RE, Loeys B. 2012. The 8th internationalresearch symposium on the Marfan syn-drome and related conditions. Am J MedGenet A 158A:42–49.
Remvig L, Duhn PH, Ullman S, Kobayasi T,Hansen B, Juul-Kristensen B, Jurvelin JS,Arokoski J. 2009. Skin extensibility andconsistency in patients with Ehlers-Danlossyndrome and benign joint hypermobilitysyndrome. Scand J Rheumatol 38:227–230.
Remvig L, Jensen DV, Ward RC. 2007. Arediagnostic criteria for general joint hyper-mobility and benign joint hypermobilitysyndrome based on reproducible and validtests? A reviewof the literature. J Rheumatol34:798–803.
Ritelli M, Dordoni C, Venturini M, Chiarelli N,Quinzani S, TraversaM, Zoppi N, VascellaroA, Wischmeijer A, Manfredini E, GaravelliL, Calzavara-Pinton P, Colombi M. 2013.Clinical and molecular characterization of40 patients with classic Ehlers-Danlos syn-drome: Identification of 18 COL5A1 and 2COL5A2 novel mutations. Orphanet J RareDis 8:58.
Rohrbach MSH, Porter LF, Burkitt-Wright EM,B€urer C, Janecke A, Bakshi M, Sillence D,Al-Hussain H, Baumgartner M, SteinmannB, Black GC, Manson FD, Giunta C. 2013.ZNF469 frequently mutated in the brittlecornea syndrome (BCS) is a single exon genepossibly regulating the expression of severalextracellular matrix components. MolGenet Metab 109:289–295.
Schalkwijk J, ZweersMC, Steijlen PM,DeanWB,Taylor G, van Vlijmen IM, van Haren B,Miller WL, Bristow J. 2001. A recessiveform of the Ehlers-Danlos syndrome causedby tenascin-X deficiency. N Engl J Med345:1167–1175.
Schwarze U, Hata R, McKusick VA, Shinkai H,Hoyme HE, Pyeritz RE, Byers PH.2004. Rare autosomal recessive cardiacvalvular form of Ehlers-Danlos syndromeresults from mutations in the COL1A2gene that activate the nonsense-mediatedRNA decay pathway. Am J Hum Genet74:917–930.
Smits-Engelsman B, Klerks M, Kirby A. 2011.Beighton score: A valid measure for gener-alized hypermobility in children. J Pediatr158:119–123123 e111-114.
Soucie JM,WangC, Forsyth A, Funk S, DennyM,Roach KE, Boone D, Hemophilia Treat-ment Center N. 2011. Range of motionmeasurements: Reference values and adatabase for comparison studies. Haemo-philia 17:500–507.
Symoens S, Syx D, Malfait F, Callewaert B, DeBacker J, Vanakker O, Coucke P, De PaepeA. 2012. Comprehensive molecular analysisdemonstrates type V collagen mutations inover 90% of patients with classic EDS and
allows to refine diagnostic criteria. HumMutat 33:1485–1493.
Talhaoui I, Bui C, Oriol R, Mulliert G, GulbertiS, Netter P, Coughtrie MW, Ouzzine M,Fournel-Gigleux S. 2010. Identification ofkey functional residues in the active site ofhuman {beta}1, 4-galactosyltransferase 7: Amajor enzyme in the glycosaminoglycansynthesis pathway. J Biol Chem 285:37342–37358.
Weerakkody RA, Vandrovcova J, Kanonidou C,Mueller M, Gampawar P, Ibrahim Y,Norsworthy P, Biggs J, Abdullah A, RossD, Black HA, Ferguson D, Cheshire NJ,Kazkaz H, Grahame R, Ghali N, Vanders-teen A, Pope FM, Aitman TJ. 2016.Targeted next-generation sequencing makesnew molecular diagnoses and expandsgenotype-phenotype relationship inEhlers-Danlos syndrome. Genet Med 18:1119–1127.
Zoppi N, Chiarelli N, Cinquina V, Ritelli M,Colombi M. 2015. GLUT10 deficiencyleads to oxidative stress and non-canonicalalphavbeta3 integrin-mediated TGFbetasignalling associated with extracellular ma-trix disarray in arterial tortuosity syndromeskin fibroblasts. Hum Mol Genet 24:6769–6787.
Zou Y, Zwolanek D, Izu Y, Gandhy S, SchreiberG, Brockmann K, Devoto M, Tian Z, Hu Y,Veit G,MeierM, Stetefeld J, Hicks D, StraubV, Voermans NC, Birk DE, Barton ER,Koch M, Bonnemann CG 2014. Recessiveand dominant mutations in COL12A1 causea novel EDS/myopathy overlap syndrome inhumans and mice. Hum Mol Genet 23:2339–2352