Embed Size (px)
Citation preview
The 39th
Congress of theRomanian Society of Neurosurgery with
International Participation
ABSTRACT BOOK
www.rsn.ro
September 18th - 21th, 2013
Table of ConTenTs
GENERAL INFORMATION 6
scIENTIFIc pROGRAMME 13
INVITED spEAKERs 25
ABsTRAcT pApERs 41
INDEX 103
General InformationGeneral Information
5
WelCoMe MessaGe
Dear colleagues,It is for me a great pleasure to invite you to participate to the 39th cONGREss OF THE ROMANIAN sOcIETY OF NEUROsURGERY with International participation to be held between 19.09 and 21.09.2013 at the palace of the National Military.The chosen topics are of great neurosurgical interest.The 2013 Neurosurgical congress is preceded by the 18th French course of Neurosurgery in Romania, organized
by the French speaking society of Neurosurgery that will also enjoy highly in-teresting topics.
We would be extremely honored to have you as guests in 2013 at Bucharest!
Welcome to Romania!
sincerely,prof. R. M. GORGAN, MD, phD
president of the congresspresident of the RsN
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
6
GENERAL INFORMATION
Official LanguageEnglish for the congress. French for the course. No simultaneous translation will be provided.
Organizing Committee:Prof. R. M. GORGAN, MD, PhD (congress president)Assoc. Prof. Ligia TATARANU, MD, PhD (congress secretary)Prof. G. IACOB, MD, PhD (French course president)F. GRAMADA, MD, PhD (French course secretary)V. CIUBOTARU, MD, PhD (Treasurer)V. Pruna MDAssist. Prof. F. BREHAR MD, Ph.D
Scientific Committee:Prof. R.M. GORGAN, MD, PhD (President)Assoc. Prof. Ligia TATARANU, MD, PhDProf. G. IACOB, MD, PhDProf. I. POEATA, MD, PhD
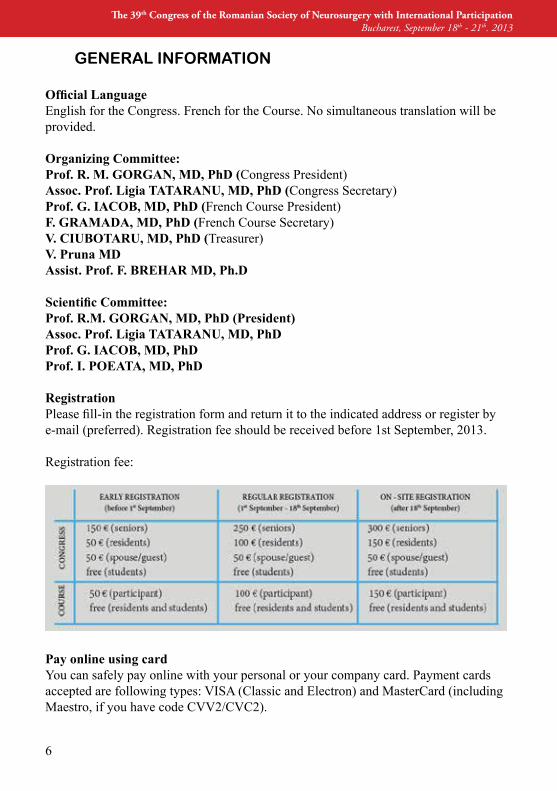
RegistrationPlease fill-in the registration form and return it to the indicated address or register by e-mail (preferred). Registration fee should be received before 1st september, 2013.
Registration fee:
Pay online using cardYou can safely pay online with your personal or your company card. payment cards accepted are following types: VIsA (classic and Electron) and Mastercard (including Maestro, if you have code cVV2/cVc2).
General InformationGeneral Information
7
Bank wire transferpayment in €uros by bank transfer in the bank account IBAN: RO-10BREL0002000694020200, LIBRA INTERNET BANK sA - sucursala BERcENI, Bucharest, for the Romanian society of Neurosurgery. It is mandatory that you specify on the transfer documents your full name and the string “For the 2013 RsN congress” or “For the 18th French course”. All bank transfer fees have to be supported by the participant.Romanian participants will pay in RON in the bank account IBAN: RO-91BREL0002000694020100, opened at the same bank.
DEADLINE FOR ABsTRAcT sUBMIssION is 25th August 2013.
No payment, no paper admission.
Accreditation Statement- The 39th conference of RsN with International participation, was accredited by the National council of Romanian college of physicians with 18 points.
- The 18th French course of Neurosurgery in Romania, was accredited by the National council of Romanian college of physicians with 6 points.
The Registration Covers- participation at the congress meetings/workshops; all written materials of the con-gress; attendance certificate;- coffee breaks- lunches- Welcome party.
Topics- Gliomas- Arteriovenous Malformations- Varia
Presentation Conditionspresentation: oral or poster.Oral presentations: computer assisted (powerpoint) on video projector display.poster presentations: 90x120 cm format.
The Scientific Committee reserves its right to accept or reject the submitted abstracts and to select abstracts for oral presentation (10 minutes) or poster.
ClothingDuring the entire meeting, attire will be casual and informal.
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
8
CurrencyThe Romanian Leu (RON) is the official national currency.
Mobile PhonesAs a courtesy to speakers and other participants, all mobile phones and pagers must be silenced before entering the scientific sessions.
Official site: www.rsn.ro/index.php/39th-congres-of-rsn
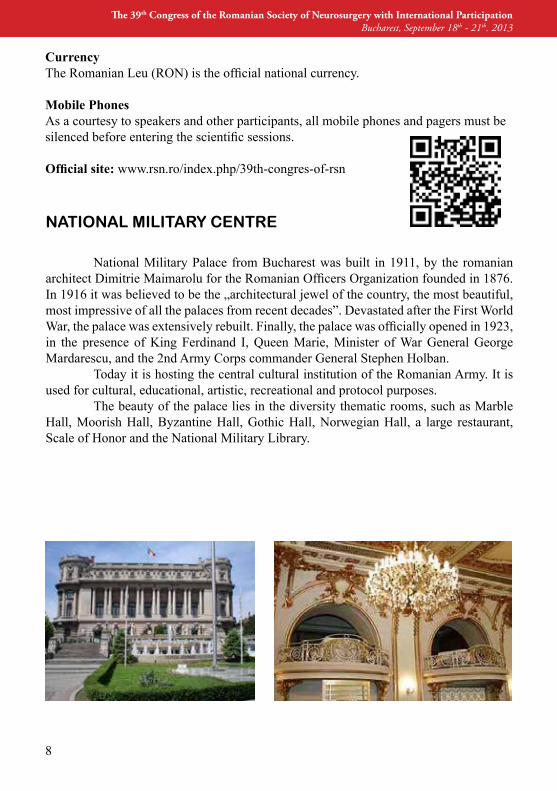
National Military palace from Bucharest was built in 1911, by the romanian architect Dimitrie Maimarolu for the Romanian Officers Organization founded in 1876. In 1916 it was believed to be the „architectural jewel of the country, the most beautiful, most impressive of all the palaces from recent decades”. Devastated after the First World War, the palace was extensively rebuilt. Finally, the palace was officially opened in 1923, in the presence of King Ferdinand I, Queen Marie, Minister of War General George Mardarescu, and the 2nd Army corps commander General stephen Holban. Today it is hosting the central cultural institution of the Romanian Army. It is used for cultural, educational, artistic, recreational and protocol purposes. The beauty of the palace lies in the diversity thematic rooms, such as Marble Hall, Moorish Hall, Byzantine Hall, Gothic Hall, Norwegian Hall, a large restaurant, scale of Honor and the National Military Library.
NATIONAL MILITARy CENTRE
General InformationGeneral Information
9
Location:Address: 21, Blvd. Regina ElisabetaTel: +40.21.313.86.80
GRAND HOTEL CONTINENTAL
Address: calea Victoriei 56, Bucharest 010083Phone: 0372 010 300
Grand Hotel continental is a 5 star hotel in Bucharest that combines the details of an exceptional architecture with a vast aray of personalized services, dedicated to an elite clientele. The building nested in a historical monument has an excellent lo-cation on Victoriei Avenue, a place full of history, the center of the Bucharest high-life, since the 1800′s. Recently opened in 2009, after a 4 years restoration and redec-oration process, Grand Hotel continental awaits its guests for a history journey. It offers an unforgetful accommodation in Bucharest right next to the main tourist at-tractions.

THANK YOU FOR YOUR SUPPORT!

Carl Zeiss – noua generatie
de microscoape neurochirurgicale
Pentru informatii despre
oferta speciala ZEISS,
contactati-ne la adresa de
mai jos!
OPMI Pentero 900 Lupe EyeMag Pro
Carl Zeiss Instruments SRL
E-mail: [email protected]
Tel.: 031- 425 3000
Fax: 031- 425 3370
OPMI Vario 700

SCIENTIFIC PROGRAMME

The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th, 2013
14
18EME COURS FRANCOPHONE DE NEUROCHIRURGIE18.09.2013
09:00 - 10:00 Craniosténoses (Prof. Patrick Dhellemmes)
10.00 - 12:00 Myélo-Méningocèles et autres dysraphies cranio-spinales (Prof. Patrick Dhellemmes)
12:00 - 12:15 Comments
12:15 - 13:30 LUNCH (MILITARY CENTER RESTAURANT)
13:30 - 14.30 Médulloblastomes de l’enfant (Prof. Olivier Klein)
14.30 - 15:30 Tumeurs intramédullaires, ouvertures et fermetures de la FCP (Prof. Olivier Klein) 15:30 - 16:30 Artères et veines de l’insula (Prof. Philippe Mercier) 16:30 - 17:30 Perforantes du tronc cérébral et angle pontocérébelleux (Prof. Philippe Mercier)
17:30 - 17:45 Comments
17:45 - 18:00 CLOSING REMARKS
Wed
nesd
ay, S
epte
mbe
r 18t
h, 2
013
Scientific Programme
15
20:00 WELCOME PARTY (NATIONAL MILITARY CENTER, MARBLE HALL)
09:00 - 10:00 OFFICIAL OPENING
Eugen Nicolaescu (Minister of Health)Prof. G. Iana (President of CAS Bucharest)Prof. I. Sinescu (Rector of UMF “Carol Davila”)Prof. I. Lascar (President of CMB)Acad. C. Popa (Romanian Academy)Gen. C. Zisu (Romania)Col. Dr. A. Ranetti (Romania)Prof. Prof. M.R Gorgan (President of RSN)Prof. I. Florian (Past President of RSN)Prof. I. Poeata (Vice President of RSN)Prof. G. Iacob (Vice President of RSN)
Thursday, September 19th, 2013
THE 39TH CONGRESS OF THE ROMANIAN SOCIETY WITH INTERNATIONAL PARTICIPATION
10:00 - 10:30 CREATIVITY IN NEUROSURGERY. TRIBUTE TO LADISLAU STEINER A ROMANIAN AM BASSADOR TO INTERNATIONAL NEURO SURGERY A.V. Ciurea, D. Mohan, D.A. Nica, I. Luca-Husti, H. Moisa
Thursday, September 19th, 2013
Wednesday,
September 18th, 2013
OPENING CONFERENCESTRATEGY OF TREATMENT FOR CRANIOVERTEBRAL AND SPINAL INSTABILITYProf. Atul GOEL (India)
10:30 - 11:00
11:00 - 11:15 COMMENTS

The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th, 2013
16
ARTERIOVENOUS MALFORMATIONS SESSION
11:45 - 12:15 SURGERY FOR ARTERIOVENOUS MALFORMATIONProf. Atul GOEL (India)
12:15 - 12:35 INTRACRANIAL VASCULAR MALFORMA TION A SURGICAL POINT OF VIEW I.S. Florian1, S.V. Trifoi, P. Kiss
11:15 - 11:45 COFFEE BREAK
Chairmen: Prof. Atul GOEL (India), Prof. M.R. GORGAN (Romania)
12:35 - 12:55 CURRENT ASPECTS IN THE SURGI CAL TREATMENT OF AVMS – ANALYSIS OF A PERSONAL SERIES OF 26 CASES TREATED SURGICALLY AND PATHOLOGICALLY CONFIRMED IN 3 YEARS I. Poeata, Al. Chiriac, F. Ziyad, N. Dobrin, Smaranda Predoaica, Antonia Nita
12.55 - 13:15 MICROSURGICAL MANAGEMENT OF BRAIN ARTERIOVENOUS MALFORMATIONS: LONG-TERM OUTCOME AND RESULTS M.R. Gorgan, Narcisa Bucur, Angela Neacsu, Aurelia Mihaela Sandu, F.M. Brehar, V.M. Pruna, D. Martin, A. Giovani, O. Zamfir, Anamaria Gheorghiu
13.30 - 14:30 LUNCH (MILITARY CENTER RESTAURANT)
14:30 - 14:45 IMRT - VMAT IN TUMORILE CEREBRALE (AMETHYST)
14:45 - 15:00 CEREBROLYSIN (EVER NEURO PHARMA)
13:15 - 13:30 COMMENTS
Thur
sday
, Sep
tem
ber 1
9th,
201
3
Scientific Programme
17
GLIOMAS SESSION (PART ONE)
15:00 - 15:15 CURRENT PROTOCOL OF BRAIN GLIOMA TREATMENT IN THE NEUROSURGERY CLINIC OF IASI – A RETROSPECTIVE STUDY OF 341 CASES B. Iliescu, D. Rotariu, C. Apetrei, F. Ziyad, I. Poeata
15:15 - 15:30 LOW GRADE GLIOMAS SURGERY- HOW I DO IT I.S. Florian, A. Baritchii, A. Iosif, Z. Andrasoni15:30 - 15:45 CURRENT SURGICAL TREATMENT AND PROGNOSIS OF SUPRATENTORIAL LOW GRADE GLIOMAS IN ADULTS V. Ciubotaru, D. Paunescu, Ligia Tataranu, M. Chelsoi, Anica Dricu
15:45 - 16:00 SUPRATENTORIAL LOW GRADE GLIOMAS NEW ACHIEVMENTS IN DIAGNOSTIC AND TREATMENT A.V. ciurea, V. ciubotaru, I. Ogrezeanu, M. Lisievici, I. Luca-Husti, H. Moisa
Chairmen: Prof. St. FLORIAN (Romania), Prof. A.V. CIUREA (Romania)
Thursday, September 19th, 2013
16:00 - 16:15 CoMMenTs
16:15 - 16:45 COFFEE BREAK
Chairmen: Prof. I. POEATA (Romania), H. PLES (Romania)
16:45 - 17:00 THERAPEUTICAL DECISION IN PEDIATRIC LOW GRADE GLIOMAS; OUR OPINION BASED ON 408 CASES A. Tascu, L. Nuteanu, R.E. Rizea, A. Iliescu, C. Pascal, Iulia Vapor, A. Enache
17:00 - 17:15 CEREBELLAR PILOCYTIC ASTROCYTO MAS IN CHILDREN – A CONTINOUS CHALLENGE A. Tascu, Iulia Vapor, Mihaela Florea, L. Nuteanu, C. Pascal, A. Iliescu

The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th, 2013
18
17:15 - 17:30 ANALYSIS OF 136 PATIENTS WITH INTRA CRANIAL GLIOBLASTOMA: CLINICAL CHARACTERISTICS, MANAGEMENT AND PROGNOSTIC FACTORS Ligia Tataranu, Adriana Dediu, V. Ciubotaru, Alisa Popescu, Anica Dricu
17:30 - 17:45 PROGNOSTIC FACTORS AND SURVIVAL FOLLOWING SURGERY FOR MALIGNANT GLIOMA c. Toader, M. stroi
17:45 - 18:00 PROGNOSTIC FACTORS OF THE MICRO SURGICAL TREATMENT FOR RECURRENT GLIOBLASTOMAS F. M. Brehar, R.M. Gorgan, Narcisa Bucur, Angela Neacsu, V.M. Pruna, Aurelia Mihaela Sandu
18:00 - 18:15 COMMENTS
20:00 SPECIAL ROMANIAN EVENING (Military Center Restaurant)
Thur
sday
, Sep
tem
ber 1
9th,
201
3
Friday, September 20th, 2013
09:00 - 09:15 NESTIN ExPRESSION IN BIOPSY SAMPLES CORRELATES WITH THE INVASIVE PHENO TYPE OF CEREBRAL GLIOMAS F. M. Brehar, D. Arsene, M. Lisievici, M. R. Gorgan
09:15 - 09:30 SURGICAL APPROACHES IN LATERAL VENTRICLE TUMORS M. Radoi, L. Danaila, F. Stefanescu, R. Vakilnejad, D.A. Petrescu, S. Suditu
GLIOMAS SESSION (PART TWO)
Chairmen: Prof. G. IACOB (Romania) Assoc. Prof. Ligia TATARANU (Romania)
Frid
ay, S
epte
mbe
r 20t
h, 2
013
Scientific Programme
19
09:30 - 09:45 MANAGEMENT OF INTRAMEDULLARY ASTROCYTOMAS D. Serban, F. Exergian, C. Zamfir, N. Calina, G. Checiu, M. Podea
09:45 - 10:00 COMMENTS
10:00 - 10:30 COFFEE BREAK
Friday, September 20th, 2013
VARIA
Chairmen: Prof. G. ZAPUHLIH (Moldova), Prof. D. ADAM (Romania)
10:30 - 10:45 THE FIRST YEAR ExPERIENCE IN THE SPINAL INSTRUMENTATION NEUROSURGERY - FROM MICRONEUROSURGERY TO THE SPINAL NEUROSURGERY G. Zapuhlih, S. Borodin, Al. Bostan, M. Andronic, V. Frumusachi, A. Marin
10:45 - 11:00 POSTERIOR CERVICAL APPROACH IN CERVICAL DISCHERNIATION: ANATOMY, TECHNIqUE, RESULTS B. Chirita
11.00 - 11:15 INCIDENTAL DUROTOMY IN LUMBAR SPINE SURGERY: INCIDENCE, RISK FACTORS AND MANAGEMENT D. Adam, T. Papacocea, R. Iliescu, Ioana Hornea, Cristina Moisescu
11.15 - 11.30 LUMBAR L4-L5 GANGLION CYST WITH CAUDA EqUINA SYNDROME. REPORT OF A Case G. Iacob11:30 - 11:45 THE VALUE OF DIFFUSION TENSOR MR IMAGING IN CERVICAL TRAUMA assessMenT M. Dabija, B. Iliescu, B. Chirita, D. Andronic, I. Poeata

The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th, 2013
20
11:45 - 12:00 TRAUMATIC PATHOLOGY OF THE THORACIC AND LUMBAR SPINE T. Maior
12:00 - 12:15 TREATMENT OF TRAUMATIC SPINAL CORD INJURIES TESTED BY CSF PHOS PHRYLATED NEUROFILAMENT SUBUNIT NF-H (pNF-H) LEVELS St. M. Iencean, A. Tascu, A. St. Iencean, I. Poeata
12:15 - 12:30 OUR ExPERIENCE WITH CEREBRAL HEMANGIOBLASTOMAS: NEUROSURGI CAL MANAGEMENT AND RESULTS M.R. Gorgan, Narcisa Bucur, Angela Neacsu, Aurelia Mihaela Sandu, F.M. Brehar, V.M. Pruna, D. Martin
14:00 - 14:15 THE ROLE OF THE MICROSURGICAL TREATMENT WITHIN THE MULTIMODAL THERAPY OF BRAIN METASTASES FROM LUNG CANCER R.M. Gorgan, Narcisa Bucur, Angela Neacsu, Aurelia Mihaela Sandu, V.M. Pruna, F. M. Brehar
14:15 - 14:30 SURGERY IN SUPERIOR SAGITTAL SINUS MENINGIOMATOSIS - CASE REPORT A. St. Iencean, B. Secara, F. Ziyad, St. M. Iencean, I. Poeata
14:30 - 14:45 INTRACRANIAL PRESSURE MONITORING IN SEVERE TRAUMATIC BRAIN INJURY c. Apetrei
12:45 - 14:00 LUNCH (MILITARY CENTER RESTAURANT)
12:30 - 12:45 COMMENTS
Chairmen: Prof. St. FLORIAN (Romania), Al. LUPSA (Romania)
Frid
ay, S
epte
mbe
r 20t
h, 2
013

Scientific Programme
21
14:45 - 15:00 SIxTH NERVE PALSY SECONDARY TO CRANIOCEREBRAL TRAUMA - OPTIONS OF TREATMENT Violeta Ioana Pruna, Ligia Tataranu, Daniela Cioplean, V.M. Pruna, M.R. Gorgan
Chairmen: Prof. A.V. CIUREA (Romania), Assoc. Prof. C. TOADER (Romania)
15:45 - 16:00 NORMAL PRESSURE HYDROCEPHALUS - ACTIVE AND PASSIVE PATHOGENETIC MECHANISMS St. M. Iencean, A. Tascu, I. Poeata, A. St. Iencean, M.R. Gorgan
16:00 - 16:15 PRELIMINARY RESULTS IN EPILEPSY SURGERY J. Ciurea, Ioana Mandruta, Teodora Coman, Nicoleta Diaconu, A. Rasina, Mirela Renta, Ana Ciurea, G. Gari, A. Barborica
15:15 - 15:45 COFFEE BREAK
15:00 - 15:15 COMMENTS
Friday, September 20th, 2013
16:15 - 16:30 NEUROSURGICAL MASTERCLASS – ADVANCED THEORETICAL COURSE FOR STUDENTS AND RESIDENTS C. C. Aldea, V. Volovici, I. S. Florian
16.30 - 16:45 A COMPARISSON BETWEEN THE qUALITY OF HEALTHCARE IN PUBLIC HOSPITALS VS PRIVATE HOSPITALS. STANDARDS OF TREATMENT AND qUALITY OF LIFE A.V. Ciurea, I. Luca-Husti, M. Dăncescu, G. David, H. Moisa16:45 - 17:00 COMMENTS
16:00 - 17:00 POSTER SESSION
17:00 - 18:30 RSN BUSINESS MEETING
20:00 GALA DINNER (GRAND HOTEL CONTINENTAL, CONCERTO HALL)

The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th, 2013
22
Saturday, September 21th, 2013
Chairmen: Prof. H. BERTALANFFY (Germania) Prof. L. RASULIC (Serbia)
09:00 - 09:30 SELECTION OF THE SUGICAL APPROACH IN BRAINSTEM CAVERNOMA Prof. Helmut BERTALANFFY (Germany)
09:30 - 10:00 INDICATION FOR SURGERY IN BRAIN STEM GLIOMAS Prof. Helmut BERTALANFFY (Germany)
10:00 - 10:30 MANAGEMENT OF MALIGNANT PERIPHERAL NERVE SHEAT TUMORS Prof. Lukas RASULIC (Serbia)
10:45 - 11:15 COFFEE BREAK
11:15 - 11:35 ACTUAL TENDENCIES IN THE MANAGEMENT OF SPONTANEOUS INTRACEREBRAL HEMATOMA – ANALYSIS OF A SERIES OF 100 CASES AND REVIEW OF THE LITERATURE I. Poeata, C. Apetrei, B. Iliescu, Z. Fayad, S. Predoaica, Al. Chiriac
10:30 - 10:45 COMMENTS
Chairmen: Prof. M.R. GORGAN (Romania) Prof. I. POEATA (Romania)
11:35 - 11:55 NEUROSURGICAL MANAGEMENT OF ANTERIOR CIRCULATION CEREBRAL ANEURYSMS c. Toader, M stroi
Satu
rday
, Sep
tem
ber 2
1th,
201
3
Scientific Programme
23
11:55 - 12:10 SUPERIOR CEREBELLAR ARTERY RUPTURED ANEURYSMS TREATED BY ENDOVASCULAR OR SURGICAL TECHNIqUES – CASE DISCUSSION M. Radoi1, St. Dima1, F. Stefanescu1, L. Marginean2
12:10 - 12:25 COMMENTS
12:25 - 12:40 CLOSING REMARKS prof. M.R. GORGAN (Romania) prof. st. FLORIAN (Romania) prof. I. pOEATA (Romania) prof. G. IAcOB (Romania) Assoc. prof. Ligia TATARANU (Romania)
Saturday, September 21th, 2013

Aesculap 146 de ani de excelenta in chirurgie si neurochirurgie
Aplicatoare si Clipuri anevrism Yasargil
peste 40 de ani de traditie si dezvoltare in domeniul neurovascular, alaturi de renumiti neurochirugi;
peste 170 de modele de clipuri anevrism din Titan; 24 de modele de aplicatoare si 4 modele de extractoare clipuri anevrism peste 120 de modele de clipuri anevrism din Phynox(Cobalt) 28 de modele de aplicatore clipuri anevrism
Substituenti Dura Mater Neuro-Patch: substituent non-absorbabil, sintetic, din polyester-uretan; Lyoplant: substituent absorbabil, colagen din pericard bovin;
INVITED SPEAKERS
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th, 2013
26
Prof. Dr. med. Helmut BERTALANFFY
Dr. Bertalanffy is professor of Neurological surgery and Director of the center for Vascular Neurosurgery at the International Neuroscience Institute, Hannover, Germany. He received his neurosurgical training from the Albert-Ludwigs University of Freiburg im Breisgau, Germany, where he completed with honors a Medical Doctorate in 1986 and obtained the qualification as board certified neurosurgeon in 1990. Dr. Bertalanffy spent more than 2 years from 1990 to 1992 at the Department of Neurosurgery of the Keio University, Tokyo, Japan, as a Scientific Fellow of the Alexander-von-Humboldt Foundation, Bonn, Germany, and the Japan Society for the Promotion of Science, Tokyo, Japan, working in the fields of cerebral and spinal microcirculation and skull base surgery. He served as vice chairman of the Department of Neurosurgery of the Technical University of Aachen, Germany from 1992 to 1997. In 1997 Dr. Bertalanffy was appointed to professor on a permanent basis by the state of Hessen, Germany, and served as professor and chairman of the Depart ment of Neurosurgery of the philipps University of Marburg for 10 years. In July 2007 he was appointed to chairman of the Department of Neurosurgery of the University of Zurich, switzerland, where he served three and a half years in that position. In November 2010 he accepted the new position of Director of the center for Vascular Neurosurgery at the prestigious International Neuroscience Institute in Hannover, Germany. Dr. Bertalanffy is a member of the German and swiss societies of Neurosurgery, the German Academy of Neurosurgery, the American Academy of Neurological surgery (corresponding member), the World Academy of Neurosurgery, the skull Base and the Nominating committees of the World Federation of Neurological surgeons (former chairman of the Nominating committee), the International Advisory Board of the American Association of Neurological surgeons, the Academia Eurasiana, and an honorary member of the Romanian society of Neurosurgery. He is the Editor-in-Chief of the scientific journal Neurosurgical Review and lends his expertise to the Editorial Boards of Neurosurgery, Acta Neurochirurgica, Techniques in Neurosurgery, Neurologia Medico-chirurgica and Zentralblatt für Neurochirurgie.
Invited Speakers
27
Prof. Atul GOEL
Job Title professor and Head of DepartmentDepartment Department of NeurosurgeryInstitution/Affiliation Seth G.S. Medical College and K.E.M. Hospitalcountry India
Education1982 ~ 1987 M.ch. (Neurosurgery), Bombay University, India, 1987.1976 ~ 1981 MBBs, Government Medical college, Nagpur, India, 1976-81.
Professional Affiliations1998 ~ 2013 professor and Head: Department of Neurosurgery, King Ed-ward Memorial Hospital and seth G.s. Medical college, parel, Mumbai, India, 1998 – present1999 ~ 2013 consultant Neurosurgeon: TATA Memorial Hospital and can-cer Research Institute, 1999 – present.2004 ~ 2013 Hon. consultant Neurosurgeon, Lilavati hospital and research centre, December 2004.
Academic Interestsskull Base surgery, complex neurosurgery, craniovertebral junction, spine, Vascular Neurosurgery.
publications summary Book Kobayashi s, Goel A, Hongo K. Neurosurgery of complex Tumors and Vascular Lesions. churchill Livingstone, New York/London, 1997. IsBN 044-3078-70X.
Goel A, cacciola F: The craniovertebral Junction: Diagnosis, pathology, surgi-cal Techniques. 2011, Georg Thieme Verlag, stuttgart, Germany. IsBN 978-3-13-149071-1 chapters, Academic papers, etc. Fifty chapters in various books and periodicals on Neurosurgery Number of publications in peer reviewed journals - 425 One hundred and fifty original and personal surgical techniques published in various international journals.

The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th, 2013
28
Memberships: Member: World federation of neurological surgery: skull base section- 2001 till date, Ethics & medicolegal affairs ethics committee- 2006 till date, Brain tumor section.
president Asia-Oceanian skull Base surgery society
president: Indo-Japan society of neurosurgery. 2014
Invited Speakers
29
Prof. Lukas RASULIC
personal data:Name: LukasSurname: Rasulić Age: 47Date of birth: 18. 03. 1965.place of birth: priština.Marital status: Married, two childrenOccupation: NeurosurgeonAdress: Institute for neurosurgery, clinical centre of serbia, Visegradska 26,11000 Belgrade, Department B
Education & continuous Medical Education• 2010, INI 10th Anniversary Hands-On Cadaver Course & Live Surger-ies Minimal Invasive skull Base Approaches, Microsurgical and Endoscopic professional Training course, July 18-19, 2010 INI-Hannover, Germany con-tinuing Medical Education project of World Federation of Neurosurgical societ-ies 25th International course • 2010, Skull Base Live Surgery July 20-21, 2010 INI-Hannover, Germa-ny continuing Medical Education project of World Federation of Neurosurgical societies 25th International course• 2010, 10 years Anniversary Meeting of International Neuroscience In-stitute, Hannover, Germany July 21-25 , 2010, Impact of technologies and methods for advances in neurosurgery,Influence of interdisciplinary cooperation for the progress in neurosurgery, Con-tribution of medical industry for the development of neurosurgery• Stručni skup Neurohirurško lečenje refrakterne epilepsije, Prof. Dr Jo-hann Schramm, Medicinski fakultet Univerziteta u Beogradu, Klinički Centar Srbije, Centar za naučno-istraživački rad, 26.03.2011, Beograd, 2 CME • Continuous Medical Education, Novine u neurohirurgiji, Klinika za neurohirurgiju, Klinički Centar Srbije, Centar za naučno-istraživački rad,, 26.03.2011, Beograd, 5 cME • 26th International Hands-On Cadaver Course & Skull Base Live Sur-gery February 26-March 1, 2011 INI-Hannover, Germany continuing Medical Education project of World Federation of Neurosurgical societies 26th Interna-tional course,• 12th Dubai Spine Conference, Challenges in Spine Surgery and Periph-eral Nerve surgery, Dubai, May 10-12, 2011, 19 cME hours
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th, 2013
30
• University Neurosurgical Clinic, Department for Brachial Plexus and peripheral nerve surgery, Buenos Aires, Argentina, 04-11-09- 2011, prof. Dr Mariano sokolovsky.• 14th WFNS Interim Meeting 2011 and the 15th Congress of Continuous Education of the Brazilian society of Neurosurgery, september 14 to 17, 2011, summerville Beach Resort in porto de Galinhas, pernambuco, Brasil, septem-ber 13th, 2011 Activity: symposium: cONTROVERsIEs IN pERIpHERAL NERVE sURGERY panel III – Adult brachial plexus injury • WFNS Educational Course, February 10-11. 2012, Skopje, Macedonia, session 1-How I do it/Techical note, Decision making in brachial plexus sur-gery: viability of the proximal stump. • 27th International Hands-On Cadaver Course & Skull Base Live Sur-gery February 18-21, 2012, INI-Hannover, Germany, continuing Medical Edu-cation project of World Federation of Neurosurgical societies, 27th International course, Minimal Invasive skull Base Approaches, Microsurgical and Endoscop-ic professional Traininig course, Live surgeries.• 1st International Congress on Minimally Invasive Neurosurgery, 20-23 March 2012, Florence, Italy, pre-congress course: Innovative Tools and Ap-proaches For Everyday Neurosurgery, Tuesday, 20 March 2012.• 1st International Congress on Minimally Invasive Neurosurgery, 20-23 March 2012, Florence, Italy, pre-congress course: Neuroendoscopy (Basic course), Tuesday, 20 March 2012.• 1st International Congress on Minimally Invasive Neurosurgery, 20-23 March 2012, Florence, Italy, pre-congress course: Mininvasive Lumbar poste-rior Motion preservation Tuesday, 20 March 2012.
Academic status:1998 Assistant professor of Medical school University of Belgrade, election2002 Assistant professor of Medical school University of Belgrade, reelection 2006 Assistant professor of Medical school University of Belgrade, reelection 2007 Associate professor of Medical school University of Belgrade election
Work experience1991 Institute of neurosurgery, clinical center of serbia volonteer.992 Institute of neurosurgery, clinical center of serbia, resident1998 Institute of neurosurgery, clinical center of serbia, specialist2009 Institute for neurosurgery, clinical center of serbia, Head of the depart-ment B.
Invited Speakers
31
ETAT CIVIL
DHELLEMMES PatrickNé le 18 juin 1943Marié 5 enfants
FONCTION:professeur des universités en Neurochirurgie depuis 1981 49ème section - 2ème sous-section du conseil National des Universités
ADRESSE PROFESSIONNELLE:clinique neurochirurgicaleHopital Roger salengroRue Emile LAINEcHRU59037 LILLE cedex
SERVICE MILITAIREEffectué en 1980-1981 dans le service de Neurochirurgie du Val de Grâce à paris
TITRESTITRES UNIVERSITAIRES Diplôme de Médecine du travail 1968 Docteur en Médecine - Mention très honorable 1973 chef de clinique à la Faculté de Médecine de Lille 1973 Médecin Spécialiste qualifié en Neurochirurgie 1981 professeur des Universités 1983 professeur des Universités, 1ère classe 1999
TITRES HOSPITALIERS Externe des Hôpitaux de Lille 1964 Interne des Hôpitaux de Lille 1968 Assistants des Hôpitaux de Lille 1973 praticien du cadre hospitalier- Neurochirurgien au cHRU de Lille 1979 chef du service de Neurochirurgie c - cHRU de Lille de 1984 à 2008 coordonnateur de la clinique neurochirurgicale - cHRU de Lille de 1999 à 2008 Membre de la cME du cHRU de Lille de mars 1999 à mars 2003• Neurochirurgien vacataire du centre de référence en malformations cranio-fa-ciales attaché au cHRU de LILLE après avoir validé ses droits à la retraite depuis septembre 2008.
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th, 2013
32
ACTIVITES ADMINISTRATIVES ET DE SOINS Responsable de l'unité fonctionnelle de Neurochirurgie pédiatrique depuis 1974. chef du service de Neurochirurgie pédiatrique depuis 1984 Membre permanent du bureau de la clinique de Neurochirurgie Responsable du fonctionnement (équipement médical, personnel) du bloc opératoire de la clinique Neurochirurgicale de 1992 à 1999. Responsable médical de la stérilisation centrale de l'Hôpital Roger salengro de 1992 à 1998.• Membre de la Sous-commission des équipements médicaux de la CME de 1999 à 2003• Copilote du « Réseau Traumatisés Crâniens du Nord-Pas de Calais » depuis 2000. ACTIVITES D’ENSEIGNEMENTECOLES PARAMEDICALES
cours de Neurochirurgie dans les écoles suivantes : école d’infirmières du CH d’Armentières de 1974 à 1984 école d'infirmières du CHRU de Lille en 1972-75-76-77. école d’infirmières du CH de Lens en1973. école d’infirmières de bloc opératoire en 1973-74.
école de puériculture du cHRU de Lille de 1988 à 2008. Institut de formation en masso-kinésithérapie du Nord de la France enseignement en 3ème année de 1995 à 2008. Enseignement au Diplôme Universitaire d'Etudes complémentaires de "Rééducation périnéale à visée uro-génitale" depuis 1990. Enseignement de neuro-psychologie clinique de 1980 à 1987.
ETUDIANTS EN MEDECINE DE DEUxIEME ET TROISIEME CYCLE
Initiation clinique des étudiants, pcEM2 et DcEM1 Formation des étudiants hospitaliers et internes affectés dans mon service lequel est validant pour la Neurochirurgie et la pédiatrie (enseignement quoti-dien au lit du malade symposium le samedi matin - réunion hebdomadaire de dossiers communs à la Neurochirurgie pédiatrique, la Neuroradiologie et la Neuro-pédiatrie .) cours de sémiologie neurochirurgicale en DcEM1 depuis 1981. Certificat de Neurologie-Neurochirurgie en DCEM3 au CHRU de LILLE depuis 1977 et à la Faculté libre de Médecine de Lille depuis 1981. Enseignement dirigé de médecine générale en 1996.
Invited Speakers
33
ENSEIGNEMENT AU DES - DIS
participation à l'enseignement du DEs-DIs de: Neurochirurgie Région Nord, pédiatrie de Lille depuis 1976, neurologie en 1982, chirurgie générale en 1999.
participation au Diplôme d'Université de Médecine Fœtale depuis 1990.participation à l'attestation d'Etude sur l'Enfance Maltraitée depuis 1996.participation à l’enseignement du DIU de Neuro-pédiatrie en 2004.participation à l’enseignement du DU de médecine d’urgence depuis 1999.participation à la formation post-universitaire de neurochirurgie au cambodge depuis 2008.participation à la formation neurochirurgicale des étudiants du DEs de chirurgie générale du cambodge dans le cadre de l’Université des sciences et de la santé de phnom penh depuis 2010.
ACTIVITES DE RECHERCHE
Modélisation en éléments finis des craniosténoses (plagiocéphalies) Acquisition par cT et IRM en collaboration avec p. Kulik - ph. pellerin - p. Villon - R. Assaker participation au mémoire de D.E.A. (1993) Docteur J.p. Hladky coagulation au Laser cO2 de la dure mère dans la prévention des récidives de craniosténoses après craniectomie : étude expérimentale chez le lapin.
SOCIETES Membre de la société de Médecine du Nord 1975 Membre correspondant de la société de Neurochirurgie de Langue Française 1975 Membre titulaire 1980 Membre de la société Française de Neurochirurgie 1976 Membre de "European society for paediatric Neurosurgery" 1976 Membre de la "société Française de pédiatrie" - section Nord 1976 Membre de la "société de chirurgie de Lille" 1979 Membre de "l'International society for paediatric Neurosurgery" 1985 Membre fondateur et trésorier de la "société Française de neurochirurgie pédiatrique (sFNcped.)" 1997 secrétaire puis vice-président 1998 président de la sFNcped. 2005
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th, 2013
34
A. ETAT CIVIL
KLEIN OlivierNé le 07 octobre 1970 à METZ (Moselle)
situation de famille : séparé, 5 enfants
B. SCOLARITEBaccalauréat c mention AB : 1989Etudes de Médecine à la faculté de Médecine de Nancy
C. TITRES HOSPITALIERSInterne des Hôpitaux (Interne de spécialités chirurgicales), concours 1996 : Novembre 96 – Octobre 97:service de Neurochirurgie, pr. Hepner, cHU NancyNovembre 97 – Avril 98service de chirurgie Orthopédique, Dr. MétaizeauHôpital Belle-Isle, MetzMai 98 – Avril 99:service de Neurochirurgie, pr. Hepner, cHU NancyMai 99 – Octobre 99:service de chirurgie Orthopédique, Dr. MétaizeauHôpital Belle-Isle, MetzNovembre 99 – Octobre 00:Département de Neurochirurgie, pr. Auque, cHU NancyNovembre 00 – Avril 01: stage Hors subdivision :service de Neurochirurgie pédiatrique, pr. pIERRE-KAHNHôpital Necker – Enfants Malades, parisMai 01 – Octobre 01:Département de Neurochirurgie, pr. Auque, cHU Nancy
D. SITUATION ACTUELLENeurochirurgien des Hôpitauxprofesseur des Universités, praticien Hospitalier
E. TITRES UNIVERSITAIRESDiplôme d’Enseignement supérieur (DEs) de Neurochirurgie : octobre 2001.chef de clinique – Assistant des Hôpitaux (Département de Neurochirurgie - cHU Nan-cy) : Novembre 2001 – Juin 2004.DIU de pédagogie médicale (année 2008-2009)Mémoire : « construction d’une évaluation des pratiques professionnelles (EPP) : la déri-
Invited Speakers
35
vation ventriculaire externe ». DOcTEUR DE L’UNIVERsITE HENRI pOINcARE, NANcY 1Doctorat UHp ENVIRONNEMENT ET sANTE « Hydrocéphalie – Mesure du débit extériorisé du liquide cérébrospinal chez l’adulte hydrocéphale porteur d’une dérivation ventriculaire externe (DVE). Relations pression et Résistance en fonction du débit des systèmes de DVE ». soutenance de thèse le 06 Novembre 2009
HABILITATION A DIRIGER DES RECHERCHES (HDR)Version de diplôme : HDR Aspects Moléculaires et cellulaires BiologieEcole Doctorale : Biologie santé Environnement (266)Titre des travaux : Hydrocéphalie et liquide cérébro spinalFormation doctorale : sciences de la vie et de la santésoutenue le 16 Décembre 2010.
F. SOCIETES SAVANTESMembre titulaire de la société Française de NeurochirurgieMembre titulaire de la société Française de Neurochirurgie pédiatrique (depuis 2007)Membre titulaire de la société de Neurochirurgie de Langue Française (depuis 2008)Membre du collège de Neurochirurgie (depuis 2010)Membre de la société Européenne de Neurochirurgie pédiatrique (en cours)
G. THESE DE DOCTORAT EN MEDECINELes astrocytomes pilocytiques diencéphaliques de l’enfant : A propos de 7 observations.Faculté de Médecine de Nancy, Université Nancy I (Henri poincaré).soutenue publiquement le 11 octobre 2001 (Mention très honorable).
H. AUTRES DIPLOMESCertificat d’ANATOMIE et ORGANOGENESE (C1 de la Maîtrise de Sciences Bi-ologiques et Médicales) : juin 1993.Certificat d’ANATOMIE SPECIALISEE : NEUROANATOMIE (C2 de la Maîtrise de sciences Biologiques et Médicales) : septembre 1993.MAITRIsE DE scIENcEs BIOLOGIQUEs ET MEDIcALEs : septembre 1996.FIFTH EUROpEAN pOsT-GRADUATE cOURsE IN pEDIATRIc NEUROsUR-GERY (3 ans): validation en 2001 (Fait partie de la qualification de Neurochirurgie Pédi-atrique)
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th, 2013
36
Philippe MERCIER
Date of birth : 21th June 1951
Address for correspondence: centre Hospitalier et Universitaire d’ANGERs Department of Neurosurgery rue Larrey 49045 cedex ANGERs – FRANcE
Medical Education: • D.E.R.B.H. 1985• Habilitation à diriger les recherches 1986• ph.D. Anatomy 1983• specialist in Neurosurgery 1983• Medicine, Lyon University 1971 -1980• Medicine, Limoges University 1969 -1971
Positions Held: Head of Anatomy (1995 - )Head of Neurosurgery (2003 -2007 )professor of Anatomy, University of Angers (1986 - )First class (2001) Exceptional class (2011)Assistant in Neurosurgery, Angers (1980-1986)Assistant in Anatomy (1980-1986)
Academic offices• Reviewer Interventional Neuroradiology, surgical Radiological Anatomy, Neuro-
chirugie • Member of the French Neurosurgical society since 1985• Member of the French pediatric Neurosurgical society since 1990 • Member of the French Neurosurgical society since 1980• Member of the French Microsurgical group since 1980• Member of the European society of pediatric Neurosurgery since 1986• Member of the European society for stereotactic and Functional Neurosurgery
since 1987• Member of the European Association of clinical Anatomy since1997• Member of the French Morphologist Association since 1980• Member of the Anatomical society of paris since 1980
Awards• French Neurosurgical Society Thesis Price (1982)
Invited Speakers
37
• Palmes Académiques Chevalier (1997) Officier (2010)• Expert près le tribunal d’Angers (2003 -)
Publications• Invited speaker International conferences 35• Scientific presentations 212• publications in peer reviewed journals 188• chapters in multi-authors books 37
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th, 2013
38
Grigore Vasile ZAPUHLîH
Dr. Zapuhlîh Grigore Vasile, was born on the 24th of December 1958, in Mascauti, criuleni, citizen of the Republic of Moldova
30 years experience in neurosurgery
professor&chairman, Department of Neurosurgery, Institute of Neurology and Neurosurgery,Medical Director of the German Diagnostic center, chairman of Neurosurgical Deparment of the International Hospital MedparkMembership in International Neurosurgical Organisations1. World Academy of Neurosurgery – phoenix, Arizona, UsA 20122. Board of World Federation of Neurosurgical societies, Marrakesh, Morocco, 20053. German society of Neurosurgery, Koln, 20044. American Asociation of Neurological surgery, san Diego, UsA, 2009
Education
1976 – 1982 Faculty of General Medicine, state Medical University “Nicolae Testemi-tanu”, chisinau, Republic of Moldova1982-1983 – Internship in Neurosurgery, Department of Neurosurgery, state Medical University “Nicolae Testemitanu”, chisinau, Republic of Moldova1990 – Defended his MD dissertation, topic: “compression neuropathies of peripheral nerves”, at the Specialized Scientific Council,Burdenko Neurosurgical Insititute, Mos-cow, Russian Federation1998 – Defended his phD dissertation, topic: “cervical spondiloticmielopathy (clini-cal manifestations, diagnosis and microsurgery)”, at the Specialized Scientific Council, state Medical University “NicolaeTestemitanu”, chisinau, Republic of Moldova.2000 – chairman of chair of Neurosurgery, state Medical University “Nicolae Testemi-tanu”, chisinau, Republic of Moldova2002 – president of the Association of Neurosurgeons of Moldova (ANM)2004 – University professor of chair of Neurosurgery, state Medical University “Nico-lae Testemitanu”, chisinau, Republic of Moldova
Training courses and exchange of experiencein Russia, Ukraine, Romania, UsA, canada, Japan, south Korea, Germany, France, Is-rael, Austria, Holland, Belgium, poland, India, Morocco, spain, Italy, Finland, switzer-land, Hawaii, Brasilia , Taiwan
Dă viaţă ideilor tale!
Contribuim împreună la modernizarea Spitalului Clinic de Urgenţă “Bagdasar – Arseni” şi ne îndreptăm zilnic atenţia spre alte unităţi sanitare. Însă, tot zilnic, ne lovim de probleme precum completarea nevoilor curente ale spitalului, achiziţia de medicamente sau materiale sanitare.
Cu sprijinul vostru am putea reda oamenilor bolnavi demnitatea şi calitatea vieţii pe care o merită. Prin fondurile donate de voi (de la minimul de 2% din impozitul anual pe salariu, până la o suma oricât de mare), putem deschide calea atâtor oameni, indiferent de categorie socială sau situaţie materială, către servicii medicale de calitate.
Nu vi se pare absurd să nu putem
face nimic pentru noi şi cei apropiaţi nouă?
Mai multe urgenţe rezolvate, mai multă sănătate, mai multă sevă într-un creier capabil, dar amorţit, în aşteptarea motivului de a se reactiva.
Ne propunem să încurajăm medicii tineri, să le oferim mai multe motive să rămână în ţară prin posibilităţi de a participa la cursuri, simpozioane şi congrese. Însă ne lipseşte sprijinul financiar.
Avem medici talentaţi, dar avem şi mulţi, mulţi oameni bolnavi, poate chiar şi în rândul vostru sau al rudelor voastre.
Contact:Str. Sfânta Vineri nr. 29, sector 3, Bucureşti,cod 030203
Telefon/ Fax: +4021 316 4822
www.fundatianeurolife.ro
FUNDAŢIANEUROLIFE
Coordonate pentru efectuarea donaţiilor:
Banca: BANCA ROMANEASCA – SMBCont în LEI: RO11BRMA0999100046778537Cont în EURO: RO11BRMA0999100050792397Cod Swift: BRMAROBUCIF: 28837916
ABSTRACT PAPERS
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
42
ARTERIOVENOUS MALFORMATIONSAVM1. INTRACRANIAL VASCULAR MALFORMATION A SURGICAL POINT OF VIEW
I.S. Florian1,2, S.V. Trifoi2, P. Kiss2
1University of Medicine and Pharmacy “Iuliu Hatieganu” Cluj-Napoca, Department of Neurosurgery 2Cluj County Emergency Hospital, Department of Neurosurgery
INTRODUCTION: In this paper we want to describe our surgical experience and strat-egy in the field of intracranial vascular malformation and the current management of these lesions, in the absence of endovascular preoperative embolisation or neuronaviga-tion facilities.
PATIENTS AND METHODS: The retrospective analysis of 192 intracranial vascular malformations admitted and surgically treated in our department between June 1996 and November 2012. From all intracranial vascular malformations 66% (127) are arteriove-nous malformations, and 34% are cavernomas (65 cases). The diagnosis was established based on clinical findings, CT, MRI, angiography, and confirmed with pathological find-ings. We recorded a minor male preponderance (54% for AVMs and 58% for caverno-mas). The peak incidence has been found in the 5th decade.
RESULTS: The major clinical findings were: hemorrhage, seizures, progressive neu-rological deficit, and headache and according to Spetzler-Martin grading system most cases of AVMs were grade II and III (65%). All the cases included in the study ware treated surgically. For arteriovenous malformation, postoperative complications were: transient neurolog-ical deficits (11%), hydrocephalus (9%), and re-bleeding (9%). The outcome was GOS 5 and 4 in 86% of the cases. In 20% of the cases, the AVMs had associated aneurisms, treated in the same operatory session.For cavernomas, postoperative complications were predominantly seizures and neuro-logic deficits (each 11%), and then hydrocephalus, and re-bleeding. The outcome was good (GOs 5 and 4) in 77% of the cases. The mortality rate for the entire series was 1.53% (meaning a case with multiple cavernomas).
CONCLUSIONS: The best treatment of an intracranial vascular malformation is surgi-cal resection, subtotal resection being in our opinion not a good option in surgery.
Keywords: intracranial vascular malformation, surgical resection.
Abstract Papers
43
AVM2. CURRENT ASPECTS IN THE SURGICAL TREATMENT OF AVMS – ANALYSIS OF A PERSONAL SERIES OF 26 CASES TREATED SURGICALLY AND PATHOLOGICALLY CONFIRMED IN 3 YEARS
I. Poeata1,2, Al. Chiriac1, F. Ziyad1, N. Dobrin1, Smaranda Predoaica1, Antonia Nita1
1Emergency Prof. Dr. N. Oblu Hospital, Neurosurgery III, Iasi, Romania2Gr.T. Popa University of Medicine and Pharmacy, Neurosurgery, Iasi, Romania
INTRODUCTION: Microsurgical treatment of AVMs changed in the last years due to access to Gamma-Knife and the development of endovascular techniques in our depart-ment in Iasi.
PATIENTS AND METHODS: We analyze 26 cases of AVM treated surgically and confirmed by imagistic and anatomo-pathological studies in the 07.2010-06.2013 period.
RESULTS: We looked at: spetzler grade, presentation, previous treatments, localization, preop and postoperative clinical status, pre- and postoperative imagistic, complications.
CONCLUSIONS: Microsurgical resection plays still a major role in the definitive treat-ment of AVMs either as a single treatment or in conjunction with endovascular tech-niques or Gamma-Knife radiosurgery in complex cases.
Keywords: AVM, microneurosurgery, treatment
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
44
AVM3. MICROSURGICAL MANAGEMENT OF BRAIN ARTERIOVENOUS MALFORMATIONS: LONG-TERM OUTCOME AND RESULTS
M.R. Gorgan1,2, Narcisa Bucur2, Angela Neacsu2, Aurelia Mihaela Sandu2,3, F.M. Bre-har1,2, V.M. Pruna2,3, D. Martin2, A. Giovani2, O. Zamfir2, Anamaria Gheorghiu2
1Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bucharest2Fourth Department of Neurosurgery, Emergency Clinical Hospital Bagdasar-Arseni3Ph.D. Student in Neurosurgery University of Medicine and Pharmacy “Carol Davila”, Bucharest
INTRODUCTION: Brain arteriovenous malformations (AVMs) are congenital com-plex network of dysplastic vessels.
MATERIAL AND METHOD: We retrospectively reviewed medical records of patients with brain AVMs operated from 1998 to 2013, in the Fourth Department of Neurosur-gery, Emergency clinical Hospital Bagdasar-Arseni.
RESULTS: Fifty-three patients with brain AVMs underwent surgery. Mean age was 37.58 years, varying from 17 to 85 years. Eight patients (15.1%) had AVMs spetzler-Mar-tin grade I, 12 patients (22.6%) grade II, 21 patients (39.6%) grade III, 7 patients (13.2%) grade IV and 5 patients (9.4%) grade V. Fourty-six patients (86.8%) had supratentorial and 7 (13.2%) had infratentorial lesions. We performed total resection of AVMs in 39 cases (73.6%). Fourteen patients (26.4%) had residual nidus. patients with residual nidus were referred to stereotactic radiosurgery with good outcome.Thirty-four patients (64.2%) presented increased modified Rankin Score (mRS) follow-ing surgery, in 6 cases (11.3%) mRs remained unchanged and 13 patients (24.5%) pre-sented decreased mRs. Mortality rate was 9.4%. Long term follow-up showed excellent quality of life in 22 patients (45.8%), good quality of life 10 cases (20.8%), mediocre quality of life in 8 patients (16.7%) and a poor quality of life in 8 cases (16.7%).
CONCLUSIONS: Microsurgery is the treatment of choice in AVMs. surgical results are excellent, with low morbidity rate. patients with poor surgical results belonged to the group admitted with severe altered state of consciousness, massive hematomas, acute brainstem dysfunction. If for any reason part of the nidus cannot be safely surgical re-sected, stereotactic radiosurgery can provide definitive cure.
Keywords: arteriovenous malformation, microsurgery, outcome

Abstract Papers
45
GLIOMASG1. CURRENT PROTOCOL OF BRAIN GLIOMA TREATMENT IN THE NEUROSURGERY CLINIC OF IASI – A RETROSPECTIVE STUDY OF 341 CASES
B. Iliescu, D. Rotariu, C. Apetrei, F. Ziyad, I. Poeata”Gr. T. Popa” University of Medicine and Pharmacy, Iasi, Neurosurgery, Romania
INTRODUCTION: Multidisciplinarity, multimodality, and maximal safe resection are the current standard in the therapeutic approach towards brain glioma. Although an increasing body of biological data raises promising new possibilities for targeted treatment microsurgical resection, radiotherapy, and chimiotherapy still represent the main line of defense against this pathology. However, new technical developments and clinical evidence impose significant changes in the protocols and therapeutic approach.
PATIENTS AND METHODS: We have analyzed a series of 341 cases of gliomas which were diagnosed and surgically treated between March 2010 and March 2013 following the current diagnostic and therapeutic protocols, including functional imag-ing, microsurgical resection, intraoperative neuronavigation and ultrasound, and awake surgey for eloquent areas tumors. We have excluded the patients without histological confirmation and patients with infratentorial lesions or the age under 18.
RESLUTS: In our series we have observed a slight predominance in males 55.4 %. The main symptom besides headache was the impairment of the motor function observed in 36.3 % cases and seizures in 30.9% cases. The preponderant age group was between 51 and 60 years of age (31% ). The complete resection was obtained in 35.4% of cas-es and in other 61.8% of cases radical surgery was not possible because of the tumor infiltration in basal ganglia (21.8%), eloquent areas (49%), and invasion of vascular structures (13.6%). The main complications were: hemorrhage in the tumoral resection bed (13.6%). All patients were directed, after recovery from surgery, to the oncology department for adjuvant therapy (Rxt/cht). In 36 patients there was a second operation for recurrence and the average time for re-intervention was 15,6 months.
CONCLUSIONS: Early imaging diagnosis, using high sensitive MRI exams, and max-imal safe microsurgical resection are in our series the factors that significantly improve the outcome of brain gliomas aided by a coherent adjuvant therapy plan. Nonetheless, complete cure is difficult to assess and needs long periods of follow-up. We present the most interesting cases of our series and discuss the advantages and disadvantages of our current therapeutic and surveillance protocol for brain gliomas.
Keywords: glioma, microsurgery, treatment
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
46
G2. LOW GRADE GLIOMAS SURGERY- HOW I DO IT
I.S. Florian1,2, A. Baritchii1, A. Iosif2, Z. Andrasoni3
1University of Medicine and Pharmacy “Iuliu Hatieganu” Cluj-Napoca, Department of Neurosurgery2Cluj county Emergency Hospital, Department of Neurosurgery
INTRODUCTION: Low grade gliomas include numerous histopathological types with varying peculiarities considering evolution, diagnosis, imaging and treatment. Despite their slow growing nature, they are not in most of the cases benign tumors, malignant transformation being described in all histopathological types.The aim of this study is to highlight some of the elements concerning the role of surgery in the treatment of low grade gliomas
PATIENTS AND METHODS: We present a retrospective study of 400 low grade glio-mas, representing 40,1 % of 997 operated by the main author (prof. Dr Florian) between 01.01.2000 and 31.12.2012, accounting for 33,18% out of the total of 3004 tumors oper-ated within the same interval. 224 cases of low grade gliomas met the inclusion criteria for multivariate statistical analysis in order to define the role of radical surgery in low gliomas treatment.
RESULTS: From a total of 400 low grade gliomas cases pilocytic astrocitomas represent 23,5 % (94 cases), grade II gliomas (astrocitomas, mixed gliomas) represent 44,5% (178 cases), oligodendrogliomas 10,7% (43 cases) and ependimomas (grade I and II) 15,25% (61 cases). Gross total removal was achieved in 88% of the cases. The improvement of the KPS scale is significantly higher (p< 0,05) in patients with gross total removal of the tumor.
CONCLUSION: The extent of removal independently influences the outcome, but no correlation with malignant transformation could be established. Radical surgery must be the goal of the treatment of all cerebral gliomas.
Keywords: low grade gliomas, radical surgery, outcome, prognosis
Abstract Papers
47
G3. CURRENT SURGICAL TREATMENT AND PROGNOSIS OF S U -PRATENTORIAL LOW GRADE GLIOMAS IN ADULTS
V. Ciubotaru1, D. Paunescu1,2, Ligia Tataranu1,2, M. Chelsoi1, Anica Dricu3
1 Neurosurgical Clinic, “Bagdasar-Arseni” Clinical Hospital, Bucharest, Romania2 “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania3 Division of Biochemistry, University of Medicine and Pharmacy, Craiova, Romania
INTRODUCTION: The importance of surgical resection for adult patients with supra-tentorial low-grade glioma (LGG) remains controversial.
MATERIAL AND METHODS: From June 2003 to June 2013, 84 adult patients with supratentorial low-grade gliomas were treated at “Bagdasar-Arseni” clinical Hospital (Neurosurgery clinic III). All patients underwent surgical intervention: gross total re-section in 24 patients (>90%), subtotal resection (<90%) in 53 patients and biopsy in 7 patients. This retrospective study assessed whether the extent of resection was associated with improved of survival and malignant transformation. The challenge for an optimal management of these patients is to find the balance between an optimal survival and the preservation of neurological function including cognition.
RESULTS: In our group, histological subtypes were as follows: oligoastrocytoma in 22 patients (26 %), diffuse astrocytoma in 26 patients (31 %) and oligodendroglioma in 36 patients (43 %). Median preoperative tumor volumes were 46.2 cm3 (between 8.3 and 174 cm3) and postoperative 5.8 cm3 (between 0 and 132.2 cm3). patients were divided into two groups by the resection grade: ≥90% and <90%. Overall survival and malig-nant transformation were analyzed. Better survival rate was correlated with increased excision for diffuse astrocytoma but not for oligodendroglioma (which are sensitive to chemotherapy). Malignant transformation occurred in 11 patients (9 of the patients given post-operative radiotherapy) of subtotal resection group (9 male and 2 female).
CONCLUSIONS: Overall survival is significantly better and malignant transformation is reduced in patients with excision higher then 90%.
Keywords: low-grade glioma, biopsy, surgery, overall survival, malignant transforma-tion
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
48
G4. SUPRATENTORIAL LOW GRADE GLIOMAS NEW ACHIEV-MENTS IN DIAGNOSTIC AND TREATMENT
A.V. ciurea1, V. ciubotaru2, I. Ogrezeanu2, M. Lisievici3, I. Luca-Husti1, H. Moisa4
*sanador Medical center, Department of Neurosurgery,**“Bagdasar-Arseni” clinical Hospital, Department of Neurosurgery ***“Bagdasar-Arseni” clinical Hospital, Department of Neuropathology****„carol Davila” University of Medicine and pharmacyBucharest, Romania, Av. Berceni 10-12, sector 4, cod 041915, Bucharest
INTRODUCTION: Low grade gliomas (LGG) are slow growing tumors. The aim of the treatment is to simultaneously combine an optimal extension of resection by preser-vation of functional integrity with correct grading of tumor malignancy and the adequate adjuvant therapies in order to achieve a long survival, with a good postoperative quality of life. There are some important questions regarding LGG: What is the delimitation of LGG? What are the therapeutical decisions: observation, surgical removal or biopsy? Does surgical removal alone ever cure LGG? If recurrences appear, is another surgery recommended? What is the efficiency of radiotherapy and chemotherapy in LGG recur-rences? What are the indications of Gamma Knife surgery (G.K.s.)?
MATERIALS AND METHOD: Our experience in a series of 160 adult patients with supratentorial LGG, operated over a period of 11 years (January 2002 - December 2012) is presented, focusing on the newest achievements in the diagnosis of gliomas (neuro-imaging, immunohistochemical analysis of tumor specimens), surgical treatment (intra-operative electrophysiology) and adjuvant therapies (oncological protocols). preoper-ative diagnosis was based on 1T MRI images. Microsurgical resection was performed in all cases: total removal 79 cases (49,3 %), partial removal 81 cases (50,6 %), with no perioperative mortality. The outcome at 6 month (GOs): good recovery 135 cases (84,3%), moderate disability 21 cases (13,1%), severe disability 4 cases (2,5%). The follow-up period was between 12 months – 9 years with the medium range of 4,5 years. Histological grading was assessed by classical pathologic examination and showed: fi-brilary astrocytomas in 102 cases, oligodendriogliomas in 26 cases, oligoastrocytomas in 21 cases, dysembryoplastic neuroepithelial tumor in 5 cases, protoplasmic astrocy-toma in 4 cases, ganglioglioma in 2 cases. In our data at 5 years postoperative we find: 11 patients were lost, recurrences to grade III-IV in 49 cases, regrowth grade II-III in 53 cases and 47 cases remain in evidence (grade II). The total number of regrowth-recur-rences cases is 102 (63,8%). It is very important to perform a check-up MRI exam every 6 months. LGG causing long-standing and medically refractory epilepsy are more likely to be associated with multiple epileptogenic foci, therefore intraoperative electrocorti-cography was used for tailoring the resection, together with intraoperative localization of central sulcus using somatosensory evoked potentials in tumors localized around the central area. Intraoperative electrophysiological monitoring was performed in 31 cases. Because actually, the final diagnosis requires immunohistochemistry and also, study of
Abstract Papers
49
the molecular biology of these tumors is an important step for understanding the genesis and biological behavior of these diseases, in the last years of the study we have per-formed also immunohistochemical analysis of the tumor specimens. We have studied in order to identify, quantify and compare, in a series of 37 cases of glioma surgical specimens (low grade and high grade gliomas), previously classified concerning their histological grade (WHO), the following immunohistochemical markers: Ki-67 proteins and pcNA (markers of the cellular proliferation), p53 (product of the tumor suppressor gene Tp53), cD 34, VEGF, VEGFR2, bFGF (markers for angiogenesis). surgical speci-mens were immunostained for p53 (clona DO-7, Biogenex UsA); Ki-67 (MIB-1; 1:50, DAKO- Glostrup, Denmark) and proliferating cell nuclear antigen (pcNA; 1:10, pc10 Dakote). proliferative activity (nuclear immunostain) was measured. p53 immunoreac-tivity was positive in all grade III and IV gliomas, and in 50% of low grade gliomas. With a median of 12% and 24% for MIB-1 and pcNA respectively, for all neoplasms in the study, the mean percentage positive nuclear area for MIB-1 and pcNA was 3.06% and 13.11% in low-grade (II) astrocytomas, 14.34% and 29.68% in highgrade (III) as-trocytomas, and 18.77% and 44.11% in glioblastoma multiforme (grade IV). One-way analysis of variance showed a significant correlation between the histological grade and MIB-1 and between the histological grade and pcNA. Isolated cases of low grade gliomas with high MIB and pcNA percentage were noticed. cD34, VEGF, VEGFR2 and bFGF expression were determined by immunohistochemistry (cD34, clone Q band, Immunotech; VEGF, sc-152, santa cruz Bioth.; VEGFR2, sc-7269, santa cruz Bioth; bFGF, bFGF88, Biogenex). Immunoreactivity for cD34 was positive in all types of the tumors. Immunoreactivity for VEGF, VEGFR2 and bFGF was seen in both endothelial cells and tumor cells, with increased levels in more aggressive tumors, comparing with normal tissue where immunoreactivity was present only in endothelial cells.
CONCLUSIONS: LGG could be treated only surgically. We advocate the idea, that patients with LGG and medically refractory epileptic seizures, may undergo tailored resections. Incompletely resected tumors may be managed with irradiation in the tumor bed, or by observation alone. proliferation in gliomas, measured as MIB-1 and pcNA, correlates significantly with histological grade, providing useful additional information for diagnosis evaluation of the tumor recurrence susceptibility. Angiogenesis markers could indicate the invasiveness tendency of the tumor. correlated with the proliferation markers, they express the aggressive tendency of the tumor and consequently, the prog-nosis. As a result, the correct treatment and prognosis of the case could be evaluated, es-pecially in LGG where the indication of radiotherapy is debatable. Despite the optimism associated with prognostic in LGG, these tumors usually recur, having a higher grade of malignancy. We consider that new, even more aggressive treatment protocols are needed for their management.
Key words: low grade gliomas, supratentorial, microsurgery, intraoperative electro-physiology, immunohistochemistry, neuro-oncology, Gamma Knife Surgery (G.K.S.)
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
50
G5. THERAPEUTICAL DECISION IN PEDIATRIC LOW GRADE GLIOMAS; OUR OPINION BASED ON 408 CASES
A. Tascu1,2, L. Nuteanu1, R.E. Rizea1,2, A. Iliescu1, C. Pascal1, Iulia Vapor1, A. Enache1
11-st Neurosurgery Clinic- Pediatric Department, Emergency Hospital „Bagdasar-Arse-ni”, Bucharest, Romania, Av Berceni 10-122Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bucharest
INTRODUCTION: Low grade gliomas (LGG) are slow growing tumors. surgery real-ise citoreduction and establish the tumoral grading. There are some important points: de-limitation of LGG; therapeutical decision: observation, surgery or biopsy; in recurrences, surgery ? radiotherapy (Gamma-Knife ?) ? chemotherapy ? Our goals are to evaluate the necessary factors for the therapeutical decision.
PATIENTS AND METHODS: Department’s 408 cases of LGG (including spinal) and literature were used. We consider: pilocytic astrocytoma (62.99 %), fibrillary astrocyto-ma (15.44 %), ganglioglioma (11.03 %), gangliocytoma (1.71 %), oligodendroglioma (1.96 %), oligoastrocytoma (4.9 %), pleomorphic xanthoastrocytoma (0.49 %), dysem-brioplastic neuroepithelial tumor (1.23 %), ependimoma (0.24 %); 0 central neurocyto-mas, subependymal giant cell astrocytomas, choroid gliomas of the third ventricle.
RESULTS: In our serie, GOs was: GR 87.25 %, MD 9.55 %, sD 2.2 %, D 0.98 %. Re-currencies at 5 years were 7.35 % and at 10 years 7.59 %. surgical resection was 49.26 % total and 50.73 % subtotal.
CONCLUSIONS: We advocate as much as possible surgical resection, without new deficits, even in critical areas (for focal tumors). Observation or biopsy is indicated only for particular cases. In recurrences, surgery, radiotherapy and chemotherapy should be considered. In the future, molecular biology will help the prognosis and therapy.
Keywords: low grade gliomas, pediatric, therapy
Abstract Papers
51
G6. CEREBELLAR PILOCYTIC ASTROCYTOMAS IN CHILDREN – A CONTINOUS CHALLENGE
A. Tascu1,2, Iulia Vapor1, Mihaela Florea3, L. Nuteanu1, C. Pascal1, A. Iliescu1
11-st Neurosurgery Clinic- Pediatric Department, Emergency Hospital „Bagdasar-Arse-ni”, Bucharest, Romania, Av Berceni 10-122Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bucharest3 Student of University of Medicine and Pharmacy “Carol Davila”, Bucharest
INTRODUCTION: posterior fossa piloctytic astrocytomas represent approximately 27-40% of pediatric posterior fossa tumors. These are benign tumors with a natural his-tory of slow growth, this leading to a delay of diagnosis. Usually at the time when the child is referred to the neurosurgeon the tumor has big dimensions, usually accompanied by hydrocephalus.
MATERIAL AND METHOD: We present our experience in 107 cases of pediatric posterior fossa pilocytic astrocytomas treated in our department from January 2003 to December 2012. The average age at the time of diagnosis was 9,05 years. The period from the setting of signs and symptoms until the moment of diagnosis was 1day to 2 years (mean period 2 months).
RESULTS: Hydrocephalus was present in 87% of cases. Gross total resection was ac-complished in 80,38% of cases (evaluation based on postoperative IRM). Outcome was favorable in 95,33% of cases.
CONCLUSIONS: According to the benign course of most cases of pediatric posterior fossa pylocitic astrocytomas, the goal of surgery is achieving maximum resection of tumor without producing new neurological deficits.
Keywords: piloctytic astrocytoma, posterior fossa, child
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
52
G7. ANALYSIS OF 136 PATIENTS WITH INTRACRANIAL GLIOBLASTOMA: CLINICAL CHARACTERISTICS, MANAGEMENT AND PROGNOSTIC FACTORS
Ligia Tataranu1,2, Adriana Dediu1,2, V. Ciubotaru1, Alisa Popescu3, Anica Dricu4
1 Neurosurgical Clinic, “Bagdasar-Arseni” Clinical Hospital, Bucharest, Romania2 “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania3 Neurological Department, University of Medicine and Pharmacy, Craiova, Romania4 Division of Biochemistry, University of Medicine and Pharmacy, Craiova, Romania INTRODUCTION: Gioblastomas are the most common primary brain tumours in adults. These tumours have an aggressive behaviour with a median survival after di-agnosis about one year. The main therapeutic methods for this pathology are surgical resection, radiotherapy and chemotherapy.
MATERIAL AND METHODS: Between June 2010 and July 2013, 136 consecutive patients were diagnosed with intracranial glioblastoma and surgically treated in our neu-rosurgical department from Emergency clinical Hospital “Bagdasar – Arseni” Bucha-rest, Romania. Adequate follow-up was obtained for all patients of the study. There were 54 women (39.8%) and 82 men (60.2%) with age between 30 and 78 years old. The mean age at admission was 56.4 years.
RESULTS: There were 133 supratentorial tumors, 2 brainstem tumors and one tumor located in the left cerebellar hemisphere. From the 133 supratentorial tumors, 26 were frontal (19.1%), 28 in the temporal lobe (20.5%), 6 in the parietal lobe (4.4%), 3 in the occipital lobe (2.2%), 8 in the basal nucleus (5.8%), 62 tumors were located in more than one lobe, sometimes with invasion in the corpus callosum. Of the 129 supratentorial tumors that were lateralized, 44.1% were located in the left hemisphere (60 patients) and 50.7% in the right hemisphere (69 patients). In two patients we found another associated tumors: one had a meningioma diagnosed and treated 2 years before the glioblastoma was diagnosed and the other patient had a tumor in the left ponto-cerebellar angle. Four-teen patients had needle biopsy, one patient had biopsy during open surgery, for 118 the tumor was resected during surgery and 3 patients were untreated surgically. The histo-pathological examination confirmed the diagnosis of glioblastoma in operated patients; in one case sarcomatos elements were also observed.
CONCLUSIONS: patients with glioblastoma who underwent radical excision of the tu-mour followed by adjuvant radiotherapy and temozolomide have an improved survival compared to patients undergoing biopsy or subtotal resection. In conclusion, younger age, small tumors, gross or near total resection, radiotherapy and temozolomide therapy are factors that predicte prolonged survival. The findings of this study may help guide treatment and prognosticate survival for patients with glioblastomas.Keywords: glioblastoma, biopsy, surgery, radiotherapy, chemotherapy

Abstract Papers
53
G8. PROGNOSTIC FACTORS AND SURVIVAL FOLLOWING SURGERY FOR MALIGNANT GLIOMA
c. Toader1,2, M. stroi2
1Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bucharest2National Institute of Neurology and Neurovascular Diseases - Bucharest, Neurosurgery, Romania
INTRODUCTION: Despite the remarkable advances in surgical techniques, adjuvant treatment strategies and the use of the operating microscope, malignant brain glioma remains a serious disease that is never cured. Even if the modern diagnostic and surgi-cal procedures contributed to the reduction of the perioperative morbidity and mortality rates in malignant gliomas, the odds of significant long term survival has remained poor and stable for the last three decades.
PATIENTS AND METHODS: A retrospective study evaluated 120 consecutive pa-tients diagnosed with malignant supratentorial glioma who underwent surgery at the Vas-cular Neurosurgical Department of the National Institute of Neurology and Neurovascu-lar Diseases between april 2008-july 2012.There were 72 women and 48 men; age range 21-78 years, mean 52 years.patient were followed-up until death or up to 14 months after enrollment in the study and survival data were correlated with the histopathological grade and location of the tumor, the extent of surgery, the patient”s performance status, the applied adjuvant therapies, complications, tumor recurrences, the time interval from the onset of symptoms to diagnosis and surgical treatment.The postoperative quality of life was assessed with the help of the Kps.survival curves were calculated by the Ka-plan-Meyer method to account for varying periods of follow-up.
RESULTS: In multivariate analyses, the extent of resection, age 65 years or younger and a Kps score of 70 or great, and anaplastic oligodendroglioma were associated with a prolonged survival time for patients with malignant gliomas.Multifocal glioblastoma and anaplastic glioma apparently arose de novo are associated with poor prognostic.
CONCLUSIONS: This study provide evidence to support tumor grade, the extent of resection, patient” age and patient”s functional status as prognostic factors for survival in patient with malignant glioma.
Keywords: malignant glioma,survival, resection, prognostic
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
54
G9. PROGNOSTIC FACTORS OF THE MICROSURGICAL TREATMENT FOR RECURRENT GLIOBLASTOMAS
F. M. Brehar1,2, R.M. Gorgan1,2, Narcisa Bucur1, Angela Neacsu1, V.M. Pruna1,3, Aurelia Mihaela Sandu1,3
1Clinical Hospital “Bagdasar-Arseni”, Bucharest2Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bu-charest3Ph.D. Student in Neurosurgery University of Medicine and Pharmacy “Carol Davila”, Bucharest
INTRODUCTION: Glioblastoma is the most common malignancy of the central ner-vous system with a poor outcome because of its tendency for recurrences. There are divergent opinions regarding the management of glioblastoma recurrence.
PATIENTS AND METHODS: The authors of this study present a series of 198 surgical procedures performed for glioblastoma recurrences in 156 patients admitted in our clinic between January 1998 and July 2013. The majority of patients (126 cases) underwent one operation for recurrences, 21 patients have been operated for two times (first and second recurrence), 6 patients for three times and 3 patients for four times.
RESULTS: The surgical mortality in this series was 1,2 % and morbidity (new neu-rological deficits postoperatively) was 9,5%. The medium survival time for recurrent glioblastoma was 30 weeks. The authors correlated the medium survival time, mortality and morbidity with the following preoperative parameters: age, Karnofsky performance status (Kps) preoperative score, tumor location (dominant or nondominat hemisphere) and extension (lobar vs multilobar). several preoperative criteria were found to be pre-dictive for a better outcome in operated recurrences of glioblastoma: age<70 years, KPS score>80 and location in non-dominant hemispheres.
CONCLUSIONS: Tumor resection should be considered for the following cases of glioblastoma recurrences: age<70 years, tumor location in non-dominant hemispheres and symptoms related to tumor mass-effect. careful selection of the patients, based on analysis of several specific preoperative criteria (age, KPS score, location, mass-effect), is important in order to obtain a better outcome and a good quality of life.
Key words: Recurrent glioblastoma, prognostic criteria, mortality, morbidity
Abstract Papers
55
G10. NESTIN ExPRESSION IN BIOPSY SAMPLES CORRELATES WITH THE INVASIVE PHENOTYPE OF CEREBRAL GLIOMAS
F. M. Brehar1,2, D. Arsene3, M. Lisievici1, M. R. Gorgan2
1Clinical Hospital “Bagdasar-Arseni”, Bucharest2Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bu-charest3Institute of Cerebro-Vascular Diseases, Bucharest
INTRODUCTION: New evidences suggest that cancer stem cells (cscs) play an im-portant role in malignant gliomas invasion. Nestin is one of the most used markers for cscs. The aim of this report was to analysis the relation between nestin expression in biopsy samples and gliomas invasion.
PATIENTS AND METHODS: serial stereotactic biopsies have been performed for 49 patients, admitted in our institution between september 2010 and April 2013 with cerebral gliomas, using Leksell stereotactic system (Elekta, sweden). All tissue samples included in study were from brain-tumor interface and were formalin fixed and paraffin embedded. Immunohistochemistry was performed using the EnVision+ Dual Link sys-tem peroxidase kit (Dako, carpinteria, cA, UsA) and primary antibodies anti nestin (santa cruz Biotechnology, cA, UsA, dilution 1:50). statistic analysis was performed using spss version 19.
RESULTS: In forty cases (81,6%) the tissue samples presented three distinct areas: tu-mor area, intermediate area and distant areas. In nine cases (18,4%) only tumor tissue could be identified. There was a statistically significant correlation between the invasive-ness of tumors (assesed by preoperative MR investigations) and the intensity of nestin expression for each area of the samples, as follows: nestin in tumor area (p=0,046), nes-tin in intermediate area (p=0,001) and nestin in distant area (p=0,011).
CONCLUSIONS: Our results support the hypothesis that cscs promote gliomas inva-sion. Moreover, nestin could be a clinically relevant marker associated with the infiltra-tive phenotype of cerebral gliomas.
ACKNOWLEDGMENTS: This work was supported by grant no.28487/30.10.2012 of University of Medicine and pharmacy “carol Davila”, Bucharest, Romania.
Keywords: nestin, gliomas, stereotactic biopsy, invasion.
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
56
G11. SURGICAL APPROACHES IN LATERAL VENTRICLE TUMORS
M. Radoi, L. Danaila, F. Stefanescu, R. Vakilnejad, D.A. Petrescu, S. SudituNational Institute of Neurology and Neurovascular Diseases - Bucharest, Neurosurgery, Romania
INTRODUCTION: Tumors of the lateral ventricle are rare lesions including a large va-riety of benign or malignant tumors and cyst formations. The purpose of this study is to discuss the factors that affected the preference for transcallosal or transcortical approach.
PATIENTS AND METHODS: It was a retrospective series that comprised 26 consec-utive patients who underwent operation for lateral ventricle tumors between 2006-2013. The main clinical symptoms and signs were associated with the localization and size of the tumors. cerebral computed tomography and magnetic resonance imaging were used to determine the location and expansion of each tumor. The transcortical approach was used in 15 patients and the transcallosal approach was used in 11 patients.
RESULTS: Total tumor resection was achieved in 19 patients. Most frequent histologic tumor’s type were glioblastoma (5), choroid plexus papilloma (5), ependymoma (4) and meningioma (4). signs of increased intracranial pressure were most dominant. One pa-tient died because of postoperative intraventricular hemorrhage. Additional neurological deficits were seen in 3 patients and postoperative seizure occurred in one patient. Two patients, one with postoperative hydrocephalus and the other with postoperative epidural hematoma required reoperation. 15 of 26 patients received postoperative radiotherapy. The mean duration of postoperative evaluation was 24,32 (range 5-92). We reoperated 2 patients due to recurrence.
CONCLUSIONS: The nature, size, location and vascularization of intraventricular tu-mors are the most important elements influencing the choice of surgical approach. Sur-geons must evaluate all these factors and prefer the short and safe way to remove the tumor.
Keywords: transcortical approach, transcallosal approach, prognostic factors
Abstract Papers
57
G12. MANAGEMENT OF INTRAMEDULLARY ASTROCYTOMAS
D. Serban, F. Exergian, C. Zamfir, N. Calina, G. Checiu, M. PodeaClinical Hospital “Bagdasar-Arseni”, Spine Surgery, Bucharest, Romania
INTRODUCTION: primitive IMT represent 8-10% of all primary tumors of the spinal cord. Only 2- 4% of all cNs tumors in adults are IMT. sc tumors are much less common than intracranial tumors with an overall prevalence of approximately an intramedullary tumor for four intracranial tumors, with variations depending on the type of tumor. For example, the location intracranial/spinal for astrocytomas is approximately 10/1, while the same ratio for ependymomas varies from 3/1 to 20/1 depending on the histological type of ependymoma. In particular, mixo-papillary ependymomas are found more fre-quently in the sc (1).
PATIENTS AND METHODS: patients enrolled in the study were hospitalized and operated in the period 2003-2009 in Neurosurgery I clinic, Ward II, “Bagdasar-Arseni” clinical Emergency Hospital for IMT in various locations. 59 patients were included in the study, age between 15 and 70 years, 40% female sex ratio = 1.5. 62 surgeries were performed. All patients were operated on by the same surgical team, same main operator.
RESULTS: We prospectively analyzed clinical, imaging and pathological data from all consecutive patients operated for intramedullary tumors in our department (Neurosur-gery I clinic, Ward II) between January 2003 and August 2009 (80 months). All surgical interventions were performed by the same surgical team. We emphasized the technical difficulties raised by ablation of IMT depending on the type of the tumor and postoper-ative neurological outcome.
CONCLUSIONS: Astrocytomas grade I could be completely or partially ablated. Total or almost total ablation is due to the cleavage plane between IMT and normal medullary tissue. In low-grade astrocytomas, where there plane cleavage is present, total or almost total ablation is the goal. - Astrocytomas grade III and IV and part of grade II astrocyto-mas (with anaplastic cells elements) were subtotally ablated because of their infiltrative nature. - There were no major intraoperative complications, postoperative immediately and/or delayed. - All cases of grade III and IV astrocytomas have clear indication for postoperative radiotherapy.
Keywords: intramedullary astrocytomas, surgery, postoperative neurological outcome

The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
58
VARIAV1. CREATIVITY IN NEUROSURGERY. TRIBUTE TO LADISLAU STEINER A ROMANIAN AMBASSADOR TO INTERNATIONAL NEUROSURGERY
A.V. Ciurea1, D. Mohan2, D.A. Nica3, I. Luca-Husti1, H. Moisa4
1Sanador Medical Center Hospital, Department of Neurosurgery, Bucharest, Romania.2Bihor County Emergency Hospital, Department of Neurosurgery, Oradea, Romania. 3St. Pantelimon Emergency Hospital, Department of Neurosurgery, Bucharest, Romania.4”Carol Davila” University School of Medicine, Bucharest, Romania.
INTRODUCTION: The incredible personality of professor Ladislau steiner represents an example of total commitment to science and the progress of international neurosur-gery.
MATERIAL: Ladislau steiner was born in the small town of Fagaras in August 1920 in a modest family. He graduated the “King Ferdinand” University of cluj-Napoca and afterwards committed himself to neurosurgery in the clinic of prof. Dr. stefan T. Iacob. After getting some experience in neurosurgery both in cluj and Bucharest, he passed through checkpoint charlie and into West Berlin from where he travelled to the Mecca of Neurosurgery at the Institute of Karolinska in stockholm, under the supervision of prof. H. Olivecrona.After learning a new language he climbed all the steps of hierarchy and became a pro-fessor of neurosurgery and the chief of the 2nd neurosurgical unit at the Institute of Karolinska. He became involved in various scientific researches and became a collaborator of Pro-fessor Lars Leksell. soon afterwards, the efforts of the two scientists led to the birth of Gamma Knife surgery. Although aged 67, after an incredible career in neurosurgery, Ladislau steiner became chief of the Gamma Knife surgery (GKs) department at the University of charlottesville in Virginia, UsA. At his new location he performed more than 15.000 Gamma Knife interventions on patients from more than 57 countries from 6 continents. His personality became that of a titan of neurosurgery and in 2010 he moves once more, but this time to the INI center of Hannover at the invitation of prof. Madjid M. samii. Having the soul of a true Romanian, Ladislau Steiner was one of the first to accept the invitation to participate at the congress of neurosurgery in 1994 in Timisoara. From then on he participated at all the important conferences and congresses of neurosurgery or-ganized in Romania, and showed the traits of a true friend and supporter of Romanian Neurosurgery. Various professors of neurosurgery from Romania have profited by Pro-fessor steiner’s invitations to Virginia at neurosurgical events and conferences. professor Ladislau steiner was the mentor of the Gamma Knife surgery Department of Bucharest. professor Ladislau steiner had impressed the auditorium of the EANs con-
Abstract Papers
59
gress of portugal in 2003 when, after having received the Medal of Honor of the WFNs clearly mentioned he was a Romanian and that his first contact with neurosurgery took place in cluj-Napoca. He presented with an homage to all his colleagues and mentors.His regretfull passing away in February of 2013 filled with sorrow the whole internation-al neurosurgical community. The Romanian ambassador to international neurosurgery passed away with the same warm smile and his constant love to human beings and Ro-manian soil. May he rest in peace.
Keywords: Ladislau Steiner, Gamma Knife Surgery, Karolinska Institute, University of Virginia, Madjid Samii.
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
60
V2. THE FIRST YEAR ExPERIENCE IN THE SPINAL INSTRUMEN-TATION NEUROSURGERY - FROM MICRONEUROSURGERY TO THE SPINAL NEUROSURGERY
G. Zapuhlih1, S. Borodin1, Al. Bostan1, M. Andronic1, V. Frumusachi2, A. Marin3
1Department of Neurosurgery, Institute of Neurology and Neurosurgery, Chisinau, Mol-dova2Department of Neurology, Institute of Neurology and Neurosurgery, Chisinau, Moldova3Department of Neuroradiology, Institute of Neurology and Neurosurgery, Chisinau, Moldova
INTRODUCTION: Increasing incidence of spinal column pathology as trauma, tumor and degenerative disease led to “explosion” of spinal fusion surgery in our country.Anal-ysis of own experience in diversity of spinal fusions using same company implants and screws.
PATIENTS AND METHODS: Retrospectively, we analyzed 18 spinal fusion cases, performed in the Neurosurgical clinic of the Institute of Neurology and Neurosurgery, chisinau, Moldova from November 2012 to september 2013.
RESULTS: Results: From all spinal column pathology 8 cases were traumatic and 10 were degenerative. Topographical level of the lesion was: lumbar spine pathology - 13 cases, of which 10 cases were nontraumatic pathology, 3 cases traumatic one. In cervical and thoracic segment all cases were exclusively traumatic, 2 case at cervical level, 3 cases at lower thoracic level. Depending on the type of spinal fusion were performed: 10 cases of transpedicular isolated fusion, of which 6 cases with fixation in 2 levels, 1 case of spinal fixation in 3 levels and 3 cases with fixation in 4 levels.. Exclusively in neurosurgical practice from Republic of Moldova were performed cervical fusion with ADD plus and intersomatica Golden Gate plates.
CONCLUSIONS: In all cases we obtained good anterior and posterior compartments fusion.
Keywords: Spinal instrumentation surgery
Abstract Papers
61
V3. POSTERIOR CERVICAL APPROACH IN CERVICAL DISCHERNIATION: ANATOMY, TECHNIqUE, RESULTS
B. ChiritaEmergency Prof. Dr. N. Oblu Hospital, Neurosurgery III, Iasi, Romania
INTRODUCTION: Even if anterior cervical approach is the most common technique for cervical disc herniation, posterior cervical approach has still some clear indications. This paper presents some anatomic details, technical notes and illustrated cases.
PATIENTS AND METHODS: Outcome follow up of 2012-2013 cases with cervical disc herniation operated using posterior approach.
RESULTS: we did not noticed any technique complications. During hospitalization all patients had a good evolution with neurological improvement.
CONCLUSIONS: in selected cases this is the optimal technique. It provides a good de-compression with less possible technical complications then anterior cervical approach.
Keywords: posterior cervical approach, anterior cervical approach, cervical disc her-niation.
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
62
V4. INCIDENTAL DUROTOMY IN LUMBAR SPINE SURGERY: INCI-DENCE, RISK FACTORS AND MANAGEMENT
D. Adam1,2, T. Papacocea1,2, R. Iliescu1, Ioana Hornea1, Cristina Moisescu1
1“Carol Davila” University of Medicine and Pharmacy Neurosurgery, Bucharest, Ro-mania2Emergency Clinical “St. Pantelimon” Hospital, Neurosurgery, Bucharest, Romania
INTRODUCTION: Incidental durotomy is a common complication of lumbar spine operations for degenerative disorders. Its incidence varies depending on several risk fac-tors and regarding the intra and postoperative management, there is no consensus. The aim is to present our experience with incidental durotomy in patients who were operated on for lumbar disc herniation, lumbar spinal stenosis and revision surgeries.
METHODS: Between 2009-2012, 1259 patients were operated on for degenerative lumbar disorders. For primary operations, the surgical approach was mini-open, inter-lamar, uni- or bilateral, as for recurrences, the removal of the compressive element was intended: the epidural scar and the disc fragment. There were operated on 863 patients (67.7%) for lumbar disc herniation, 344 patients (27.3%) for lumbar spinal stenosis, and 52 patients (5%) for recurrences. The operations were performed by neurosurgeons with the same professional degree but with different operative volume.
RESULTS: Unintentional durotomy occurred in 20 (2.3%) of the patients with herni-ated disc, in 14 (4.07%) with lumbar spinal stenosis and in 12 (23%) with recurrences. The most frequent risk factors were: obesity, revised surgery and the physician’s low operative volume. Intraoperative dural fissures were repaired through suture (8 cases), by applying muscle, fat graft or curaspon, tachosil, fibrin glue. Four cerebro-spinal fluid (CSF) fistulas were repaired at reoperation.
CONCLUSIONS: Incidental dural fissures during operations for degenerative lumbar disorders must be recognized and immediately repaired to prevent complications such as CSF fistula, osteodiscitis and increased medical costs. Preventing, identifying and treating unintentional durotomies can be best achieved by respecting a neat surgical tech-nique and a standardized treatment protocol.
Keywords: durotomy, dural tear, CSF fistula
Abstract Papers
63
V5. LUMBAR L4-L5 GANGLION CYST WITH CAUDA EqUINA SYN-DROME. REPORT OF A CASE
G. IacobClinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bucha-rest, SUUB, Bucharest, Romania
INTRODUCTION: Although juxtafacet cysts are lesions noted as incidental findings associated with spinal facet joints on imaging studies of the spine (computed tomogra-phy - cT and magnetic resonance imaging – MRI); in some patients, they may produce symptoms
METHODS: A female aged 47 years old was admitted for an acute cauda equina syn-dome induced by a ganglion facet cyst. Diagnosis was sustained on spinal lumbar MRI and dynamic flexion/extension X-rays.
RESULTS: The patient got benefit from microsurgery, with excellent outcome, with no surgery-related complications six months after operation and no fusion.
CONCLUSIONS: Mostly associated with degenerative facet joints and spondylolisthe-sis, symptomatic lumbar juxta facet cysts - ganglion and synovial cysts are uncommon lesions of the spine. They can mimic herniated discs, causing low back pain, radiculopa-thy or even cauda equina syndrome.
Keywords: ganglion cyst, synovial cyst, juxtafacet cyst, spinal fusion, degenerative spine disease, cauda equine syndrome
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
64
V6. THE VALUE OF DIFFUSION TENSOR MR IMAGING IN CERVI-CAL TRAUMA ASSESSMENT
M. Dabija, B. Iliescu, B. Chirita, D. Andronic, I. Poeata”Prof. Dr. N. Oblu” Clincial Emergency Hospital, 1st Neurosurgery, Iasi, Romania
INTRODUCTION: MR imaging, with its high soft-tissue resolution, has been estab-lished as the gold standard in evaluating the extent of spinal cord structural damage in cases with spinal cord trauma. However, the conventional MR imaging offers poor data concerning the microstructure of the spinal cord, such as fiber tracts of the white matter. The advent of diffusion tensor imaging made it possible to analyze the level of integrity of functional structures represented by the white matter tracts.
PATIENTS AND METHODS: We present our initial experience of using a complex imaging protocol that includes DTI sequences in the cases with cervical spine trauma. We analyze the clinical and imaging characteristics of 17 patients that suffered traumatic injuries of the cervical spine from various causes.
RESULTS: clinically we established the AsIA score for each individual case. From the imaging data we studied the T2 and FLAIR-weighted images and looked at the signal intensity abnormalities. correlations were established between the three different mea-sures. We discuss the prognostic value of each measure separately and in conjunction.
CONCLUSIONS: Our current data suggest that DTI has a better correlation with the clinical status of the patient, offers a better explanation for the degree of neurological deficit, and, most importantly has a much better prognostic value.for the outcome of the cervical spine trauma that affects the spinal cord.
Keywords: cervical, trauma, diffusion tensor MRI, outcome
Abstract Papers
65
V7. TRAUMATIC PATHOLOGY OF THE THORACIC AND LUMBAR SPINE
T. MaiorCluj County Emergency Hospital Department of Neurosurgery, Cluj-Napoca, Romania
INTRODCUTION: Traumatic pathology of the thoracic and lumbar spine is easy to be surgically solved. surgery itself does not represent a real surgical challenge, but the true challenge regarding this pathology is related to the decision making process. The paper presents the surgical treatment protocol in trauma pathology located in dorsal and lumbar spine area. Aspects related to vertebral body surgery, lengths and type of instrumenta-tion, reason of treatment, and pitfalls in trauma surgery are discussed.
METHODS: 180 of cases were studied with at least one year post-op follow-up, oper-ated according to the same criteria. The treatment algorithms area presented, including some representative cases of posterior approaches, and of combined (anterior and poste-rior) approaches. All presented cases are from the author’s personal archive and under-went surgery using the same system of stabilization and the same technique.
RESULTS: Obvious advantages of the transpedicualr stabilization, ligamentotaxis and the reconstruction of the vertebral body. Images of illustrated cases are present-ed.
CONCLUSIONS: Based on our expereince short intrsumentations, good restoration of the sagital balance, vertebral body reconstruction are key facts in order to obtain good long term results in spine traumatic pathology.
Keywords: transpedicular posterior instrumentation, ligamentotaxis, short instrumen-tations
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
66
V8. TREATMENT OF TRAUMATIC SPINAL CORD INJURIES TEST-ED BY CSF PHOSPHRYLATED NEUROFILAMENT SUBUNIT NF-H (pNF-H) LEVELS
St. M. Iencean1, A. Tascu2, A. St. Iencean1,3, I. Poeata1,3
1Gr.T. Popa University of Medicine and Pharmacy, Iasi, Neurosurgery, Iasi, Romania2Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bucharest3Emergency Prof. Dr. N. Oblu Hospital, Neurosurgery III, Iasi, Romania
INTRODUCTION: several studies showed that the phosphorylated form of the neuro-filament subunit NF-H ( pNF-H) are related to neuronal injuries and its detection pro-vide information about the degree of neuronal loss. The phosphorylated neurofilament subunit NF-H ( pNF-H ) is present into CSF in significant amounts following neuronal injury and may be detected. The pNF-H could be a biomarker of the neuronal injuries and its detection might provide prognosis in humans.
METHODS: We used a pNF-H ELIsA test capable of detecting the levels of phosphor-ylated NF-H (pNF-H) to patients with spinal cord injury. We studied the pNF-H levels in csF in patients with spinal cord injury (scI) and for normal values of pNF-H we deter-mined the csF pNF-H level from individuals without neurological damage.
RESULTS: The normal values were: 0 to 0.9 ng/mL and the pathological values were till 10.9 ng/mL. The pNF-H values of csF from the patients with scI were 6 - 10 times higher than the normal and its higher values were related to an unfavorable outcome.
CONCLUSIONS: In conclusion the phosphorylated form of the neurofilament subunit NF-H ( pNF-H) is biomarker in scI in humans and its increased values are consistent with an unfavorable outcome.
Keywords: biomarker, phosphorylated neurofilament subunit pNF-H, spinal cord injury
Abstract Papers
67
V9. OUR ExPERIENCE WITH CEREBRAL HEMANGIOBLASTO-MAS: NEUROSURGICAL MANAGEMENT AND RESULTS
M.R. Gorgan1,2, Narcisa Bucur1, Angela Neacsu1, Aurelia Mihaela Sandu1,3, F.M. Bre-har1,2, V.M. Pruna1,3, D. Martin1, A. Giovani1, O. Zamfir1, Anamaria Gheorghiu1
1Clinical Hospital “Bagdasar-Arseni”, Bucharest2Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bu-charest3Ph.D. Student in Neurosurgery University of Medicine and Pharmacy “Carol Davila”, Bucharest
BACKGROUND: Hemangioblastomas are highly vascular, well-defined, cystic, cys-tic with mural nodule or solid, benign tumors, occurring sporadically or in von Hip-pel-Lindau disease.
MATERIAL AND METHOD: We retrospectively reviewed medical records of adult patients, admitted and operated into the Fourth Department of Neurosurgery, Emergency clinical Hospital Bagdasar-Arseni with positive histopathological diagnosis of hema-gioblastoma.
RESULTS: From 1998 to 2013, 39 patients with brain hemangioblastomas were admit-ted in our department. In 31 patients hemangioblastoma (79.5%) occurred sporadically and 8 cases (20.5%) had von Hippel-Lindau disease. There were 22 males (56.4%) and 17 females (43.6%). Mean age was 44.38, varying from 18 to 73 years. In 33 patients (84.6%) the tumor was located into the posterior fossa and in 6 cases (15.4%) the tumor was supratentorial. The tumor was intraaxial in 35 patients (89.74%) and extraaxial in 4 cases (10.26%). patients underwent 67 surgical procedures: 39 underwent primary tumor surgical resec-tion, 10 patients underwent second surgery for tumor recurrence, 4 patients underwent third surgery for tumor recurrence, 8 patients required a ventriculoperitoneal shunt for hydrocephalus, 2 patients underwent shunt revision and 4 patients required surgery for complications, posterior fossa compressive cyst requiring cystic-ventriculoperitoneal shunt, cerebral abscess, extradural hematoma and intraparenchymatal hematoma. All 10 patients (25.6%) with tumor recurrence had subtotal resection. Morbidity rate was 12.82% and mortality was 2.56%. Twenty eight (71.79%) patients had favorable long-term outcome.
CONCLUSIONS: The most common location for hemangioblastomas was posterior fossa. subtotal resection is associated with tumor recurrence. Total resection ensures a favorable long-term and a recurrence-free outcome. Hydrocephalus is the most frequent associated pathology.
Keywords: hemangioblastoma, posterior fossa tumor, surgery
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
68
V10. THE ROLE OF THE MICROSURGICAL TREATMENT WITH-IN THE MULTIMODAL THERAPY OF BRAIN METASTASES FROM LUNG CANCER
R.M. Gorgan1,2, Narcisa Bucur1, Angela Neacsu1, Aurelia Mihaela Sandu1,3, V.M. Pru-na1,3, F. M. Brehar1,2
1Clinical Hospital “Bagdasar-Arseni”, Bucharest2Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bu-charest3Ph.D. Student in Neurosurgery University of Medicine and Pharmacy “Carol Davila”, Bucharest
INTRODUCTION: cerebral metastases of pulmonary origin represent a pathology with an increasing incidence and a severe prognosis. Often patients come to the neuro-surgeon with multiple cerebral metastases and a surgical decision has to be taken based on the benefits and the risks of the microsurgical treatment.
PATIENTS AND METHODS: The authors present a series of 78 patients with cerebral metastases with pulmonary origin operated in our clinic between 2006 and 2012 and detailed the therapeutic strategies in relation with the location and number of metastases.
RESULTS: There were 20 women (25, 6 %) and 58 men (74, 4%) with a mean age of the series of 55,44 years (±sD 10,46). There was no surgical mortality in this series and no additional neurological deficits postoperatively. 62 patients had one metastasis. The surgical resection was total for all cases with single cerebral metastases. 10 patients had 2 cerebral metastases. In 3 patients both cerebral metastases have been removed by a sin-gle-stage surgical approach. In 7 patients the larger metastasis has been totally removed and for the smaller one the Gamma-knife has been performed. six patients had three or more metastases. In all these cases the largest, life threatening metastasis has been removed and for smaller lesions, Gamma-knife has been performed.
CONCLUSIONS: single symptomatic cerebral metastases have the following surgi-cal indications: age<75 years, Karnofsky performance status (KPS)>70, stable primary cancer, midline-shift and the presence of a perilesional hypodens area on cT scan of minimum 3 cm. patients with multiple cerebral metastases and one symptomatic and surgical accessible lesion have also the same neurosurgical indications. In these cases, neurosurgical procedure removed the life-threatening lesion, while Gamma-knife thera-py provided a long term control of the remaining smaller lesions.
Key words: cerebral metastases, microsurgical treatment, mortality
Abstract Papers
69
V11. SURGERY IN SUPERIOR SAGITTAL SINUS MENINGIOMATO-SIS - CASE REPORT
A. St. Iencean1, B. Secara1, F. Ziyad1, St. M. Iencean1,2, I. Poeata1,2
1Emergency Prof. Dr. N. Oblu Hospital, Neurosurgery III, Iasi, Romania2Gr.T. Popa University of Medicine and Pharmacy, Neurosurgery, Iasi, Romania
INTRODUCTION: Multiple meningiomas attract a lot of interest because of their rel-ative rarity, unclear aetiology and the problems related to proper management strategy.
PATIENTS AND METHODS: We describe a case of 58 years old female that presented with slowly progressive right hemiparesis for 2 years, aphasia for 2-3 months that im-proved under medical treatment, left crural paresis for 10 days and signs of intracranial hypertension. The MRI imaging showed multiple nodules: right parasagital precoronar, right paracentral, bilateral parasagital pre-lambdoidal. Also, the seldinger angiography show total obstruction of sinus at the level of pre-coronar nodule and partial at the level of pre-lambdoidal nodules and the possibility of venous drainage through venous ducts in the periphery of lambdoidal tumors. the surgey consisted in parasagittal bilateral bone flap, mainly on the right side, resection of the pre-coronar and paracentral nodules; intra-capsular resection of the pre-lambdoidal nodules with keeping some patent venous ducts in the thickness of tumoral capsule and partial resection of the nodule invading the sss.
RESULTS: The patient had a very good postoperative evolution (Karnofsky 70 to 90), the signs of intracranial hypertension dissapeared and she improved the hemiparesis and the walking ability.
CONCLUSIONS: Radical resection of meningiomas invading the superior sagittal sinus (sss) presents several hazards. some surgeons consider sss invasion a contraindication for complete resection, and others advocate total resection with venous reconstruction.
Keywords: meningiomatosis, surgical approach, superior sagittal sinus
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
70
V12. INTRACRANIAL PRESSURE MONITORING IN SEVERE TRAUMATIC BRAIN INJURY
c. ApetreiEmergency Prof. Dr. N. Oblu Hospital, Neurosurgery III, Iasi, Romania
INTRODUCTION: Intracranial pressure management is still a challenge despite neu-rotraumatology development. That’s why intracranial pressure monitoring is extremely important in this pathology for choosing the right therapeutical method. We will present some illustrated cases, our technique and results.
PATIENTS AND METHODS: We had followed evolution of patients with severe trau-matic brain injury monitored with camino Integra system.
RESULTS: Medical and surgical treatment guided by intracranial pressure monitoring seems to be more effective then without invasive captors.
CONCLUSIONS: Monitoring intracranial pressure is a crucial technique in leading ce-rebral edema treatment.
Keywords: intracranial pressure, brain swelling

Abstract Papers
71
V13. SIxTH NERVE PALSY SECONDARY TO CRANIOCEREBRAL TRAUMA - OPTIONS OF TREATMENT
Violeta Ioana Pruna1,5, Ligia Tataranu2,3, Daniela Cioplean1, V.M. Pruna2,4, M.R. Gor-gan2,3
1Oftapro Clinic, Bucharest, Romania2Clinical Hospital “Bagdasar-Arseni”, Bucharest3Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bu-charest4Ph.D. Student in Neurosurgery University of Medicine and Pharmacy “Carol Davila”, Bucharest5Ph.D. Student in Ophtalmology University of Medicine and Pharmacy “Carol Davila”, Bucharest
INTRODUCTION: Due to it’s long intracranial course, sixth nerve is one of the most common affected cranial nerves in cranial - cerebral trauma. It may be damaged either by direct mechanism (skull base fractures) or indirectly, by raised intracranial pressure, which compress the nerve at the angle over the tip of the petrosum bone. Neuromuscular dysfunction may be partial (paresis) or complete (palsy) and significantly reduces the quality of the patient’s life, by diplopia and confusion. A waiting period of 6 months to one year prior to strabismus surgery must be considered, in order to assess the chance of spontaneous recovery. Treatment may be conservative or surgical, depending on the residual neuromuscular function and time elapsed from the injury.
MATERIAL AND METHODS: Authors reviewed the files of 17 patients admitted into Oftapro clinic with sixth nerve palsy, secondary to cranial cerebral trauma, produced by car crash (13 cases) and falls from height (4 cases). 12 patients had unilateral, and 5 pa-tients had bilateral sixth nerve paralysis. In terms of neural muscular dysfunction degree, 12 patients manifested complete sixth nerve palsy, and in 5 cases, the deficit was partial. 9 of the patients underwent surgery alone, botulinum toxin injection alone worked in one case, 5 cases needed combined therapy (surgical, BTX-A, and prismatic correction) and 2 cases showed spontaneous recovery in time.
RESULTS: Good ocular alignment or slightly under correction, with restoration of binocular vision (with or without prismatic correction) was obtained in all cases, except one, in whom ocular misalignment persisted, despite surgery and BTX-A injection (the patient refuses the idea of reintervention). Surgical success was defined as orthoptic ocu-lar alignment in primary position or residual esotropia less than 12 pD (prism diopters), with ability of the eye to move at least at the median line (abduction – 4), associated with binocular vision recovery.

The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
72
CONCLUSIONS: sixth nerve palsy has multiple therapeutic options, depending pri-marily on the degree of residual neuromuscular function. Good functional results can be obtained if different procedures are applied specifically for each case. A good interdisci-plinary collaboration is mandatory for functional recovery of these patients.
Keywords: Sixth nerve palsy, cranial cerebral trauma, binocular vision, diplopia
Abstract Papers
73
V14. NORMAL PRESSURE HYDROCEPHALUS - ACTIVE AND PAS-SIVE PATHOGENETIC MECHANISMS
St. M. Iencean1, A. Tascu2, I. Poeata1,3, A. St. Iencean3, M.R. Gorgan2
1Gr.T. Popa University of Medicine and Pharmacy, Iasi, Neurosurgery, Iasi, Romania2Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bucharest3Emergency Prof. Dr. N. Oblu Hospital, Neurosurgery III, Iasi, Romania
INTRODUCTION: Normal pressure hydrocephalus (NpH) is characterized by normal csF pressure, less than 18 cm H2O, classical clinical triad: gait disturbance, dementia and incontinence in patients with communicating hydrocephalus on cT or MRI..
PATIENTS AND METHODS: We analyzed retrospectively the NpH hospitalized pa-tients in three neurosurgical centers between January 2008 and December 2011. There were only 41 selected cases of patients with NpH, including 24 patients with secondary NpH and 17 patients with idiopathic NpH.
RESULTS: Ventriculoperitoneal shunt was performed in all 24 patients with secondary NpH and at 9 patients with IdNpH. The short-term and long-term results were good and very good for cases of secondary NpH and good in 60% and poor in 40% in cases of IdNpH.
CONCLUSIONS: We can consider that secondary NpH and some cases of idiopathic NpH with repeated small increases of Icp, with transependymal migration of csF and hydrocephalus causes clinical triad because of the open glial-ependymal barrier, as an Active Normal pressure Hydrocephalus and the shunt has good results ; and other cases of IdNpH have not increases of intracranial pressure, no transependymal migration of csF and there are pre-existing periventricular deep lesions that causes clinical triad, as a passive hydrocephalus, this is a passive Normal pressure Hydrocephalus.
Keywords: normal pressure hydrocephalus, idiopathic normal pressure hydrocephalus
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
74
V15. PRELIMINARY RESULTS IN EPILEPSY SURGERY
J. Ciurea1, Ioana Mandruta2, Teodora Coman1, Nicoleta Diaconu1, A. Rasina1, Mirela Renta1, Ana Ciurea1, G. Gari1, A. Barborica3
15th Dept. of Functional Neurosurgery , Clinical Hospital “Bagdasar-Arseni”, Bucha-rest2 Univ. Mun. Hospital, Neurology, Epilepsy Center, Bucharest, Romania3 Univ. of Physics, Magurele, Romania
INTRODUCTION: The objective is to investigate results after electrophysiologial di-agnosis and resective epilepsy surgery in Department of Functional Neurosurgery.
PATIENTS AND METHODS: All patients were referred to our center after careful assessment by a dedicated epilepsy team from another hospital. The first step was im-plantation of deep brain electrodes for a tailored well planed resection. There were 12 procedures. Identification of vessels was performed by MR enhancement studies in ded-icated IDL environment. cT scans were used for postoperative assessment. A total of 40 procedures were performed in the last 2 years of which there were 4 lobectomies 7 lezionectomie with electrocorticography, 5 supraselective amigdalohypocampectomies, and one reposition of electrodes. All patients had been prospectively followed in the dedicated Epilepsy center.
RESULTS: In the short term, all patients were seizure-free or improved significantly postop, One patient developed an ischemia. The fusion of preoperative and postoperative images aloud confirmation of precision electrode placement. The resection was selective due to electrophysiology and the final results were analyzed on pre and post operative imaging.
CONCLUSIONS: Almost all patients are seizure-free or improved since surgery. Many patients who gain seizure freedom can successfully discontinue antiepileptic drugs in future.
Keywords: Epilesy, Surgery Deep Brain Electrodes
Abstract Papers
75
V16. NEUROSURGICAL MASTERCLASS – ADVANCED THEORETICAL COURSE FOR STUDENTS AND RESIDENTS C. C. Aldea1, V. Volovici2, I. S. Florian1
1“Iuliu Hatieganu” University of Medicine and Pharmacy, Cluj-Napoca, Romania2 Erasmus University Medical Center, Rotterdam, The Netherlands
The first edition of the Neurosurgical Masterclass took place in July 2013 in Cluj-Napoca. It was organised by the Students’ Scientific Circle of Neurology and Neurosurgery under the patronage of the Neurosurgical Department of the cluj-county Emergency Hospital. The course was aimed at students who express a strong desire and capability to pursue a neurosurgical career and to residents in this field. The Masterclass was designed in such a way as to offer participants not only fundamental theoretical information, but also clarify where and who to learn from. Bearing in mind that we were analysing a surgical subject, we divided the course into 2 days: first day – neuroanatomy at the highest theoretical level possible, second day- neurosurgical patology. During day 1 we covered the anatomy of the cranial fossae, the cerebral me-ninges and ventricles, the major cerebral arteries and veins, the dural venous sinuses. We analysed the macroscopic and most importantly the microsurgical anatomy of these structures. We demonstrated that a thorough knowledge of anatomy is indispensable for anyone willing to enter a surgical career. In the last day we discussed neurosurgical approaches (pterional, retrosigmoid-ian, posterior fossa approaches) relying on the anatomical knowledge covered on the previous day. We also focused our attention on neurotrauma (going from the essentials- mechanisms of cerebral trauma, posttraumatic intracranial haematomas and working ourselves up to the latest in the neurosurgical community- discussing the results of the latest trials), vascular and tumoral neurosurgical pathology. Here, again we went from the fundaments to the latest developments in the treatment of aneurysms, gliomas, me-ningiomas. Our participants were from 3 major university centres from Romania. The goal of the course, to give participants the key to theoretical mastering of the field of neurosurgery was accomplished. Given the high quality of information pro-vided and the results, further editions are justified. Also, this Masterclass paved the way for a future hands-on course, preparing the participants with all the theoretical knowl-edge needed to fully focus on acquiring the much needed practical skills.

The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
76
V17. A COMPARISSON BETWEEN THE qUALITY OF HEALTHCARE IN PUBLIC HOSPITALS VS PRIVATE HOSPITALS.STANDARDS OF TREATMENT AND qUALITY OF LIFE
A.V. Ciurea1, I. Luca-Husti1, M. Dăncescu2, G. David3, H. Moisa4
1Sanador Medical Center, Hospital, Department of Neurosurgery, Bucharest, Romania.2”St. Constantin” Hospital, Brasov3”Queen Mary” Emergency Military Hospital Brasov, Romania4”Carol Davila” University School of Medicine, Bucharest
INTRODUCTION: Nowadays physicians find more and more involved in the constant debate whether public healthcare is better than private healthcare. It goes without saying that small private practices have always been around for dentistry, cardiology and many more, however, the situation is entirely different in what concerns private hospitals. At such a level things are much more complicated as disputes are generated by the necessity of financial covering of the treatment by the state. The authors wish to underline that private healthcare does not interfere with public healthcare services. On the contrary, private healthcare comes as an adjuvant and and a stimulant, thus ensuring a viable alter-native that patients have, for the bennefit of public healthcare in Romania.
MATERIALS: In contemporary medical literature, authors show that the European tendencies regarding healthcare systems are globally poised to reducing differences be-tween national systems. In this respect a series of measures were undertaken – improving financing, increasing the efficiency of public healthcare providers, promoting prevention rather than treatment, finding appropriate payment means for healthcare and last but not least, developing of private healthcare services. The improvement of quality in health-care can be achieved easier and faster by stimulating private healthcare systems and private healthcare insurances in a way that can insure transparency and optimal funding. In Romania, the relationship between public and private healthcare providers is not one of adversity, rather one of complementarity and “competitivity” as some analysts might say. The arguments for the development of private healthcare were freedom of choice – some patients wished for higher treatment standards and hospital facilities; ballancing demand and supply and thus reducing the discrepancies between western healthcare systems and the national one; assuming risks the state had until now- by ac-cepting patients, private healthcare systems have lowered the costs of national healthcare – smaller risk for certain diseases, fewer buildings needed, cheaper utility bills, etc, and last but not least, ensuring that patients have access to modern treatment means at a better cost – compared to western countries. There are public hospitals known for their efficient management strategies – such as Moinesti city Hospital or Alba county Hospital as well as private hospitals known to provide an efficient treatment and an improved quality of service such as MedLife Hospital, sanador Medical center, IccO of Brasov, AKH of Vienna or INI center of Hannover.
Abstract Papers
77
CONCLUSIONS: We observe signifiant diferences between public and private health-care. What is common between the two is the constant search of maximum results. We have to admit that both systems offer increased performance, however, the satisfaction of the patient is mandatory. If we are to pursue quality in all fields of interest – treatment, accommodation, logistics etc we tend to think of private systems. If we’re to refer to access to services and basic healthcare we tend to think of public healthcare. The two systems therefore have to coexist as together they provide the most reasonable formula of effectiveness and improved quality of treatment. A crucial difference between the two is the absence of informal payment in private healthcare systems while in public health-care this represents a serious downfall. The relationship between the two systems – private and public has to be characterized equally by competitivity and complementaruty. The introduction of private healthcare systems shouldn’t be an objective per se. The true objective should be recording benefits for national healthcare and the social-economic system of Romania.
Keywords: Health insurances, public hospital, private hospital, neurosurgery.
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
78
V18. ACTUAL TENDENCIES IN THE MANAGEMENT OF SPONTA-NEOUS INTRACEREBRAL HEMATOMA – ANALYSIS OF A SERIES OF 100 CASES AND REVIEW OF THE LITERATURE
I. Poeata1, C. Apetrei2, B. Iliescu2, Z. Fayad2, S. Predoaica2, Al. Chiriac2, 1Gr.T. Popa University of Medicine and Pharmacy, Iasi, Neurosurgery, Iasi, Romania2Emergency Prof. Dr. N. Oblu Hospital, Neurosurgery III, Iasi, Romania
INTRODUCTION: Non-traumatic intracerebral hematoma may be the result of an AVM rupture discoverable n routine angiography. In other cases the clinical and imag-istic data suggest the possibility of hematoma in the context of hypertension of amyloid angiopathy. Besides these there are a number of other possible causes: anticoagulation, hemorrhagic infarction, hemorrhagic tumors, cryptic AVMs.
PATIENTS AND METHODS: The goal of this paper is to analyze the shifts in the di-agnosis and therapeutic approach with the advent of MRI as the main diagnostic tool, in the context of multiple angiographic diagnosis options, continuous improvement of neu-roanesthesiology and intensive care, improved surgical techniques, better intraoperative localization and hemostasis. In the same time we look at the change in attitude in favor of a more conservative approach for a vast portion of these cases, while the complexity of the cases increased due to an aging population and the increased life expectancy with additional comorbidities. We analyzed retrospectively 100 consecutive cases with IcH admitted recently in the Department of Neurosurgery in Iasi.
RESULTS: The following pathologies were encountered: hypertension in 74 cases, rup-tured intracranial aneurysms in 7 cases, cavernomas in 5 cases, AVM in 2 cases, amy-loid hematoma in 2 cases, anticoagulation in 2 cases, hemorrhagic infarction in 2 cases, hemorrhagic tumor in 1 case, while 5 cases had no discoverable cause. surgical remov-al of the hematoma was performed in 28 cases, 12 of which were treated in the same procedure for the underlying vascular lesion (aneurysm clipping, cavernoma or AVM nidus resection). In one case the aneurysm was embolyzed and the hematoma treated conservatively. 3 cases had a EVD performed and one case necessitated decompressive craniectomy.
CONCLUSIONS: In the diagnosis the main dilemma consists in how far the investiga-tions should go in order to discover a etiology underlying the hemorrhage. The treatment is constrained by the decision of surgical evacuation of the hematoma. Whilst additional data was made available it is still a multifactorial decision and it is more often than not influenced by the personal preference of the surgeon in charge of the case.
Keywords: intracerebral hematoma, spontaneous, treatment, diagnosis
Abstract Papers
79
V19. NEUROSURGICAL MANAGEMENT OF ANTERIOR CIRCULA-TION CEREBRAL ANEURYSMS
c. Toader1,2, M stroi2
1Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bucharest2National Institute of Neurology and Neurovascular Diseases - Bucharest, Neurosurgery, Romania
INTRODUCTION: Ruptured intracranial aneurysms are major neurosurgical urgencies that have a poor natural history with regard to rebleeding and should be treated as soon as possible.
PATIENTS AND METHODS: We present our surgical experience in 83 patients who presented 99 anterior circulation cerebral aneurysms , who underwent surgery at the Vas-cular Neurosurgical Department of the National Institute of Neurology and Neurovascu-lar Diseases between july 2010- august 2013. There were 38 male and 51 women.Age range 26-78 years, mean 54 years. Anterior communicating artery aneurysms were en-countered the most frequent( 32 patients).24 patients were diagnosed with middle cere-bral artery aneurysms.One patient had unruptured ophthalmic artery aneurysm.11 patient harbored posterior communicating artery aneurysms.The rest of the patients presented anterior circulation intracranial aneurysms as follows: anterior choroidal aneurysms(2 patients), carotid artery bifurcation aneurysms( 4 patients), distal anterior cerebral artery aneurysms(6 patients ), cavernous carotid artery aneurysms( 3patients ).Large and giant aneurysms were encountered in 13 patients.16 patients harbored multiple aneurysms. Two patients had 5 aneurysms.
RESULTS: We analised the rate of morbidity and mortality and complications related to each type of eneurysm.The overall mortality was 9% and the morbidity was 27%.
CONCLUSIONS: Aneurysms surgery is and should remain an important element of neurosurgical culture, even as endovascular techniques advance in popularity and so-phistication. Modern aneurysms techniques offer excellent solutions and must be saved for those aneurysms that require them.
Keywords: aneurysms, clipping, subarachnoid hemorrhage, outcome
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
80
V20. SUPERIOR CEREBELLAR ARTERY RUPTURED ANEURYSMS TREATED BY ENDOVASCULAR OR SURGICAL TECHNIqUES – CASE DISCUSSION
M. Radoi1, St. Dima1, F. Stefanescu1, L. Marginean2
1National Institute of Neurology and Neurovascular Diseases - Bucharest, Neurosurgery, Romania 2Nova Vita Hospital Tg Mures, Angiography, Tg. Mures, Romania
INTRODUCTIONIn the last decade, aneurysms of the cerebral posterior circulation were more feasible to endovascular treatment due to the challenging position of these aneurysms for surgical clipping. We reported two particular cases of a distal superior cerebellar artery ruptured aneurysm treated by endovascular and, respectively, surgical techniques.
METHODSOcclusion of the aneurysms was achieved by endovascular placement of two stents, and, in the other case, by surgical clipping.
RESULTSIn both cases, the aneurysm was excluded from circulation. six months, and respectively, twelve months follow-up control angiography demonstrate complete occlusion of the aneurysms. No focal neurological deficits of the both patients were recorded.
CONCLUSIONSIn experienced hands and in selected cases surgery of aneurysms developed in challeng-ing surgical positions could be as successful and efficient as endovascular therapy.
Keywords: aneurysm, endovascular, surgery

Abstract Papers
81
POSTERS SESSIONP1. OUR LAST 10 YEARS ExPERIENCE IN TREATMENT OF TUBERCULUM SELLAE MENINGIOMAS
Ligia Tataranu1,2, V. Ciubotaru1, B. Dumitrescu1, Anica Dricu3
1 Neurosurgical Clinic, “Bagdasar – Arseni” Clinical Hospital, Bucharest, Romania2 “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania3 University of Medicine and Pharmacy, Craiova, Romania
INTRODUCTION: Tuberculum sellae meningiomas present a close relationship with anterior visual pathways, the arteries of the anterior circulation and the hypothalamus. The authors report on a series of surgically treated tuberculum sellae meningiomas, re-section being achieved by different approaches.
MATERIAL AND METHODS: A retrospective study was conducted on 24 consecu-tive patients with tuberculum sellae meningiomas, operated on at the 3rd Neurosurgical clinic, “Bagdasar – Arseni” clinical Hospital Bucharest, between January 2002 and July 2012. The mean age of the 19 women and 5 men enrolled in the study was 51 years (range 21 – 75 years). The follow-up period ranged from 3 to 85 months (median: 46 months).
RESULTS: The main presenting symptom was visual compromise in 83.3 % of the patients (20 cases). In addition, preoperative hormonal abnormalities were highlighted in 25 % of the patients (6 cases). MRI and angio MRI were the main radiological exams. In terms of surgery, a frontolateral approach was used in 21 patients (87.5 %) and an endoscopic endonasal extended transsphenoidal approach for the rest of the 3 patients (12.5 %). Quick access to the tumor was achieved through these approaches; they were also minimally invasive with less brain exposure, therefore complications were being kept to a minimum. Radical tumor removal was possible in all but 2 patients (91.7 %). postoperatively, vision improved in 19 patients (79.2 %), did not change in 4 patients (16.7 %) and worsened in one patient (4.2 %). No perioperative mortality was recorded.
CONCLUSION: The surgical treatment’s goal in the majority of patients with tubercu-lum sellae meningiomas is total resection. Usually, this can be safely accomplished, with minimal postoperative complications and morbidity. The most important factors that in-fluence the treatment strategies are the extent and duration of visual symptoms, the size of the tumor and the encasement of the anterior cerebral artery complex.
Keywords: tuberculum sellae meningiomas, frontolateral approach, endoscopic endona-sal extended transsphenoidal approach.
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
82
P2. GASSERIAN CYSTIC SCHWANOMA WITH INTRACAVERNOUS ExTENSION AND SKULL BASE DESTRUCTION. A MICROSCOPIC ExTRADURAL MIDDLE FOSSA APPROACH V. Munteanu, R. StanescuNeurosurgical Clinic, “Bagdasar – Arseni” Clinical Hospital, Bucharest, Romania
BACKROUND: Trigeminal schwannomas account for less than 8% of intracranial schwannomas. They originate within the ganglion, nerve root, or 1 of the 3 divisions of the trigeminal nerve. About 50% of these tumors are limited to the middle fossa, while 30% extend into the posterior fossa and 20% are dumbbell-shaped and extend into both fossae. Diagnosis is best established with MRI. The differential diagnosis includes me-ningioma, vestibular schwannoma, epidermoid lesions, and primary bone tumors of the skull base.
METHODS: A 60 years old female pacient was admitted for numbness in the left tri-geminal V b region. IRM study revealed an extranevraxial left temporal tumor invading the cavernous sinus, cavum Mecheli and the sphenoidal sinus. Ophtalmologic examam-ination showed papiledema.
RESULTS: surgery was performed and a predominent chystic tumor with solid com-ponent was identified and resected. Postoperative neurological evolution was favorable marked only by a CSF fisutla has been treated by instaling a lumbar drainage for 5 days. After the microdecompresion the pain has completely dissapear . Histophatological exam was schwanoma Antoni A.
CONCLUSION: Extranevraxial skull baze schwanomas can be surgically removed safelly. CSF fisula can be a compication that can be treated conservatively.
Keywords: schwanoma, skull base, middle fossa approach
Abstract Papers
83
P3. SURGICAL TREATMENT IN HUGE FORAMEN MAGNUM TU-MOR IN CHILDREN – CASE REPORT
B. Secara1, A. St. Iencean1, F. Ziyad1, St. M. Iencean1,2 I. Poeata1,2
1Emergency Prof. Dr. N. Oblu Hospital, Neurosurgery III, Iasi, Romania2Gr.T. Popa University of Medicine and Pharmacy, Neurosurgery, Iasi, Romania
INTRODUCTION: We present the clinical, imagistic, surgical findings and the out-come at a 12-years old girl with huge foramen magnum tumor.
PATIENTS AND METHODS: A 12-years old girl presented with progressive proximal upper right extremity paresis for 3 weeks and spastic tetraparesis mainly on the right side for 3 days. MRI imaging showed a huge foramen magnum gadolinium-enhancing lesion that compressed and displaced the spinal cord. The surgery consisted in suboccipital craniectomy with c1 laminectomy, c2 laminoplasty and microsurgical resection of the tumor.
RESULTS: After surgery the patient made good neurological improvements, and the postoperative MRI showed the resolution of spinal cord compression at cervical level. The anatomopathological report was meningothelial meningioma with many psamoma-tous bodies.
CONCLUSIONS: Meningiomas are relatively uncommon in childhood. The intraoper-ative appearance of the tumor with the extent in the c2 foramen suggested a neurinoma. The recent onset and rapid progression are discordant with the tumoral size and the fast recovery.
Keywords: meningioma, foramen magnum tumor, children
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
84
P4. RADIO-INDUCED NEUROSURGICAL BRAIN LESIONS
M.R. Gorgan1,2, Narcisa Bucur1, Angela Neacsu1, Aurelia Mihaela Sandu1,3, F.M. Bre-har1,2, V.M. Pruna1,3, D. Martin1, A. Giovani1, O. Zamfir1, Anamaria Gheorghiu1
1Clinical Hospital “Bagdasar-Arseni”, Bucharest2Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bu-charest3Ph.D. Student in Neurosurgery University of Medicine and Pharmacy “Carol Davila”, Bucharest
INTRODUCTION: Radio-induced neurosurgical brain lesions occur inside previous-ly radiation area, are not present at the time of radiotherapy, occur after a sufficiently long period of time following radiotherapy, have different histopathological diagnosis compare with the primary tumor and patients lack genetic predisposition for second tu-mor occurrence. Radio-induced neurosurgical brain lesions are: meningiomas, vestibular schwannomas, gliomas, cavernomas, etc.
MATERIAL AND METHOD: We report 4 cases with radio-induced brain lesions, ad-mitted into the Fourth Department of Neurosurgery, Emergency clinical Hospital Bag-dasar-Arseni.
RESULTS: All 4 patients were males. primary disease was third ventricle tumor in 3 cases and scalp trichophytia in one case. Three patients underwent surgery with tumor resection and were referred to adjuvant conventional whole-brain radiotherapy. One patient suffered from scalp trichophytia and was treated with scalp radiation. Time to diagnosis of radio-induced brain lesion was 13, 17, 17, and 30 years following radiother-apy. Two patients presented supratentorial meningiomas and two presented cerebellar hemisphere cavernomas. patients with meningiomas, were symptomatic, presented large tumors and required life-saving surgery. Other imaging findings were diffuse brain atro-phy and leukoencephalopathy.
CONCLUSIONS: Radiotherapy can cause long-term complications and can induce new brain lesions development inside the radiation area. Meningiomas and cavernomas may be radio-induced brain lesions and may occur following previous radiotherapy. Me-ningiomas grow to large size, requiring surgery.
Keywords: radiotherapy, long-term complications, meningioma, cavernoma

Abstract Papers
85
P5. ENDOSCOPIC TRANSNASAL APPROACH FOR PITUITARYADENOMA – PRELIMINARY ExPERIENCE
D. Rotariu, F. Ziyad, I. Poeata”Gr. T. Popa” University of Medicine and Pharmacy, Iasi, Neurosurgery, Romania
INTRODUCTION: pituitary adenomas account for 10-15% of all brain tumors. The current approach to this sellar lesion is the transnasal endoscopic approach. We present our preliminary experience and results using this approach in the treatment of sellar region tumor.
METHODS: We have included all patients with pituitary adenoma operated on using the endoscopic transnasal approach in the 3rd Neurosurgical Department of Neurosur-gery at “prof Dr N Oblu” clinical Emergency Hospital, Iasi, Romania since the introduc-tion of the technique (May 2013).
RESULTS: 6 cases (3 males and 3 females) were operated on using the endoscopic transnasal approach in the last 3 months. 4 of the patients had non secreting pituitary adenoma and 2 of them had prolactinomas with signs of pituitary apoplexy. The mean volume of the lesions was 13.52 cm3 (range 3.85-28.6cm3). cavernous sinus was invad-ed in 4 cases, 3 cases had type C supraselar extension and in 4 cases the sellar floor was invaded. All the patients had single nostril approach (right side) and 3 of them had a de-viated nasal septum on the side of the approach. The sphenoid sinus had a simple struc-ture (one single septum) in 4 cases and 2 had complex structure (3 septum). The mean time of procedure was 181 minutes (range 145 - 230). One single case, the first one, needed reconversion to microsurgery in order to control bleeding. Gross total removal was achieved in one case and subtotal in the other 5 (but with no signs of compression on the adjacent structures). The pituitary gland was identified intra operatively and pre-served in 5 cases, postoperatively no patient had new endocrine insufficiency. The main complication was represented by transitory diabetes insipidus in 2 cases, with no cases of infection or csF leak.
CONCLUSIONS: The transnasal endoscopic approach is a safe and efficient procedure for treatment of pituitary adenomas, with a low rate of surgical complication, and with high rates of endocrine function preservation given the high optics, which permit the identification and preservation of the normal pituitary gland. Anyhow the duration of surgery is comparable to the microsurgical trans sphenoidal approach and will continue to lower with further gain of experience.
Keywords: pituitary adenoma, endoscopic transsphenoidal approach

The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
86
P6. APOPLExY IN A RECURRENT PITUITARY ADENOMA - CASE REPORT
Adriana Dediu1,2, Ligia Tataranu1,2, V. Ciubotaru1, Violeta Pruna3, M.R. Gorgan1,2
1 Neurosurgical Clinic, “Bagdasar-Arseni” Clinical Hospital, Bucharest, Romania2 “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania3 “Oftapro” Clinic, Bucharest, Romania
BACKGROUND: pituitary apoplexy is a clinical syndrome characterized by abrupt onset of severe signs of intracranial hypertension, visual impairment, restriction of visual fields, paresis of ocular muscles, nausea, vertigo, meningismus, and/or decreased level of consciousness. The clinical syndrome is consequent to subarachnoid extravasation of blood and dural irritation, cranial nerve and hemispheric compression from lateral or su-perior extention of necrotic and/or hemorrhagic material, endocrine abnormalities from acute pituitary dysfunction. standard therapy of pituitary apoplexy includes decompres-sion via transsphenoidal route and high-dose steroid treatment.
CASE REPORT: We report a case of a 29-year old woman with a history of transsphe-noidal hypophysectomy for a prolactinoma 7 years ago and currently on bromocriptine and glucocorticoid and thyroid hormone replacement, who presented with galactorrhea, sudden severe headache, nausea, vomiting, diplopia and visual impairment on both eyes. computer tomography and contrast-enhanced magnetic resonance imaging of the head proved a large sellar tumor with extension to the suprasellar region with intratumoral hemorrhagic zones. The treatment of choice was resection of the sellar mass by trans-sphenoidal approach. Histological examination revealed a pituitary adenoma mostly acidophil, with intratumoral hemorrhage, highly suggestive for pituitary apoplexy. The outcome was favorable and the patient was discharged in a good condition but with ne-cessity for hormonal replacement as a treatment of pituitary insufficiency.
CONCLUSIONS: pituitary apoplexy remains a potentially life-threatening disease. This case demonstrates that apoplexy can occur and should be suspected even in a patient with a previous history of hypophysectomy.
Keywords: pituitary adenoma, pituitary apoplexy, transsphenoidal approach
Abstract Papers
87
P7. COLLOID CYST – AN UNUSUAL LOCATION. CASE REPORT
D. Păunescu1,2, Ligia Tataranu1,2, V. Ciubotaru1, M.R. Gorgan1,2
1 Neurosurgical Clinic, “Bagdasar-Arseni” Clinical Hospital, Bucharest, Romania2 “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
BACKGROUND: colloid cysts represents 0.2 - 2% of brain tumors and less than 1% of symptomatic brain tumors. They are found throughout the neuroaxis but over 99% of them develop in the third ventricle. colloid cysts of the pituitary gland are very rare pathological lesions occurring in sellar region.
CASE PRESENTATION: A 67-year-old woman presented to the endocrinology de-partment with a 3-months history of frontal and retroocular persistent headache. No focal neurological deficits and no signs of intracranial hypertension were present and hormon-al biomarkers were in normal range. Magnetic resonance imaging (MRI) of the brain showed a relatively homogeneous sellar mass extended superiorly into the suprasellar cistern and impinge on the optic chiasm. Visual field examination shows optochiasmatic syndrome. Tumor removal proceeded in a standard way by transsphenoidal approach and the pathologic examination confirmed the diagnosis of colloid cyst. At the 3rd month fol-low-up visit the patient did not show any endocrinological or focal neurological deficits. MRI brain images revealed total resection of colloid cyst and no compression on opic chiasma.
CONCLUSIONS: The absolute differentiation of pituitary macroadenomas from rare non-pituitary origin sellar tumours is often not possible prior to invasive therapeutic or diagnostic procedures.
Keywords: colloid cyst, transsphenoidal approach

The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
88
P8. GLUCOSE AND INSULIN ExPRESSION IN VARIOUS TYPES AND GRADES OF BRAIN TUMORS
Oana Alexandru1, L. Ene1, Ligia Tataranu2, V. Ciubotaru2, Alisa Popescu1,3, Ada Maria Georgescu4, V. Pruna2, Anica Dricu3
¹ Department of Neurology, University of Medicine and Pharmacy, Craiova, Romania2 Neurosurgical Clinic, „Bagdasar-Arseni” Clinical Hospital, „Carol Davila” Universi-ty of Medicine and Pharmacy, Bucharest, Romania3 Division of Biochemistry, University of Medicine and Pharmacy, Craiova, Romania4 „Medico Science” SRL, Craiova, Romania
INTRODUCTION: In the last years, many authors suggest the existence of an associ-ation between different components of metabolic syndrome and various cancers. Two important components of metabolic syndrome are hyperglycemia and hyperinsulinemia. Both of them had already been linked to increased risk of cancers: pancreas, breast, endometrial or prostate. However the correlation of the glucose and insulin level with various types and grades of brain tumors remains unclear.
MATERIAL AND METHODS: In this article we analyzed the values of plasma gly-cemia and insulin in 267 patients consecutively diagnosed with various types of brain tumors.
RESULTS: Our results showed no correlation between the glycemia and brain tumor types or grades. High plasma levels of insulin were found in brain metastasis and as-trocytomas while the other types of brain tumors (meningiomas and glioblastomas) had lower levels of the peptide. The expression of insulin was also higher in brain metastasis and grade 3 brain tumors compared with the grades 1, 2 and 4 brain tumors.
Keywords: insulin level, brain tumor, astrocitoma, glioblastoma, meningioma, brain me-tastasis
Abstract Papers
89
P9. SPINAL ASSOCIATED WITH VON RECKLINGHAUSEN’S DISEASE
K. IstvanClinical Emergency Hospital, Neurosurgery, Tg. Mures, Romania
INTRODUCTION: The neurofibromatosis type 1 (NF1) was first described by Von Recklinghausen and Festscher, and has been known as the Von Recklinghausen’s disease also. It is inherited as an autosomal dominant trait, therefore, is a hereditary condition. At least eight forms of neurofibromatosis have been recognized, but the most common is the (NF1), with a prevalence of 1:2200 to 3000 births. When associated with Von Reck-lighausen’s disease, the tumors are usually multiple, and may occur at numerous levels of the spinal cord. The signs and symptoms of this condition vary widely among affected people. The most common sign on the skin are multiple neurofibromas that can occur anywhere in the body. Another highly characteristic feature on the skin is the presence of café au lait (coffee with milk) pigmentation. Lisch nodules (pigmented hamartomas of the iris), translucent brown-pigmented spots on the iris, are found in nearly all affect-ed individuals. Bone lesions, cardiovascular and neurological abnormalities are others manifestations of this disease. Abnormalities that involve neurological system includes central nervous system tumours, macrocephaly, mental deficiency, seizures, short statute and scoliosis.
PATIENTS AND METHODS: A 32 years-old female patient was referred to our de-partment, due to full motor loss (immobilized to bed), localized at the level of the inferior members and urinary and defecation disfunctions. In general physical examination we notice the presence of papules, subcutaneous nodules and café au lait pigmentation in many parts of the body. After MRI-examinaton we observed the presence, of subdural tumoral lesions at the L2-L5 levels. complete resection of the lesions was performed, through a L2-L5 laminectomy, confirming the initial diagnosis. Thoracic and abdominal cT also showed multisistemic involvance. The general clinical, imagistic and intraopera-tive findings, completed with the histopathological examination confirmed the diagnosis of Von Recklinghausen’s disease. A modest neurological improvement was observed during the initial postoperative course. The patient could walk independently 5 days later, with the preservation of urinary and defecation functions. postoperative follow-up was difficult in this case, she came back to our institute one year after surgery. Clinical signs were bilateral cervicobrachialgia, paraparesis, bilateral sensitive radiculopathy c3-c7 levels. MRI showed multiple subdural, extramedullary tumoral masses at the c2-c6 levels, with intraforaminal extension. A c2-c6 laminectomy was performed with the microscopical resection of the tumoral masses. After surgery the patient had favorable outcome with the remission of preoperative clinical signs.
RESULTS: The best results are obtained with patients showing minimal neurological
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
90
deficits during the pre-operative period. Little improvement may be expected from the patients who develop complete transection syndrome during the postoperative period.
CONCLUSIONS: Is one of the few genetic diseases, which requires neurosurgical im-plications. Prenatal diagnosis is possible, but difficult. There is about a 5% increase in risk for various cancers, including brain tumor. Plexiform neurofibromas can become malignant. There is also an increased rate of scoliosis in NF1, with progresses around the time of pubert.
Keywords: Von Recklinghausen’s disease, neurofibromatosis 1, neurofibroma
Abstract Papers
91
P10. CEREBRAL AVM-RELATED INTRACRANIAL HEMORRHAGE-CLINICAL CONSIDERATIONS
Anca Smaranda Natalia Predoaica1, B. Iliescu2, Z. Fayad1, Al. Chiriac1, D. Rotariu1, I. Poeata1,2
1Emergency Prof. Dr. N. Oblu Hospital, Neurosurgery III, Iasi, Romania2Gr.T. Popa University of Medicine and Pharmacy, Neurosurgery, Iasi, Romania
INTRODUCTION: Arteriovenous malformations (AVMs), part of intracranial vascular malformations group, are leading cause of intracerebral haemorrhage in young adults and the most common presenting symptom for patients with AVMs is brain hemorrhage that can cause devastating neurological deterioration.
PATIENS AND METHODS: Between 2009 and 2013, medical records of 44 patients reffered to University Hospital “N. Oblu” Iasi, presented with intracranial hemorrhage caused by cerebral arteriovenous malformation (AVM), which was diagnosed by cT scan Factors followed in terms of their influence on the level of consciousness at admis-sion were: volume of intraventricular hematoma, acute hydrocephalus, intraparenchymal hematoma.
RESULTS: Diagnosis of AVMs was confirmed with MRA, angio CT scan, and/or Seldinger angiogram. Nineteen patients had intraparenchymal supratentorial, five had intraparenchymal posterior fossa, twenty had intraventricular hemorrhage clinical status ranged from mild impairment to profound coma.
CONCLUSIONS: All factors we follow significantly contributed to the development of serious disturbance of consciousness in the acute stage following intracranial hemor-rhage. Left untreated, can cause a progression of symptoms that can lead to permanent disabilities or death.
Keywords: Cerebral arteriovenous malformations, Intracranial hemorrhage
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
92
P11. SUPRATENTORIAL ARTERIOVENOUS MALFORMATIONS: CLINICAL ARTICLE
c. Toader1,2, M stroi1
1Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bucharest2National Institute of Neurology and Neurovascular Diseases - Bucharest, Neurosurgery, Romania
INTRODUCTION: Because of their complex nature and varied locations, treatment strategies must take into account both the directs effect of the AVMs on the surrounding structures as well as the dependence of these structures on its blood supply.Even the AVMs can pose formidable surgical challenges, surgical resection continues to be the treatment modality of choice. The most common presentation of a patient harboring AVMs is with an intracranial hemorrhage.
PATIENTS AND METHODS: We present our surgical experience in 6 patients with supratentorial cerebral arteriovenous malformations, who underwent surgery at the Vas-cular Neurosurgical Department of the National Institute of Neurology and Neurovascu-lar Diseases between jan. 2011-july 2013 .Three of them were associated with intranidal or remote, flow-related aneurysms and one complex AVM was associated with dural arteriovenous fistula.There were 5 male and 1 women.Age range 42-77 years, mean 58 years.All patients presented with intracranial hemorrhage and all were investigated with DsA.We used the most widely accepted grading system Martin –spetzler scale. The clinical outcome was evaluated in terms of neurological deterioration attributable to treatment.
RESULTS: The cure rate was based on angiography. The eradication of the AVMs was achieved in 5 of 6 patients, with 1 AVM being partially resected.The rate of complica-tions were strongly associated with Martin-spetzler scale.
CONCLUSIONS: Direct surgical excision of small and medium sized AVMs remains possible and with an acceptable risk, even in eloquent areas, provided their acces is simple.Direct excision of large AVMs remains a formidable procedure, full of dangers intra-and postoperatively.
Keywords: AVM, resection, complications, prognostic
Abstract Papers
93
P12. ASPECTS OF EARLY SURGERY IN SEVERE CRANIO-CERE-BRAL TRAUMA
I. streltov1, I. poeata1,2, Marcela Nour1
1Emergency Prof. Dr. N. Oblu Hospital, Neurosurgery III, Iasi, Romania2Gr.T. Popa University of Medicine and Pharmacy, Neurosurgery, Iasi, Romania
INTRODUCTION: The goal of the study was to evaluate the outcome of patients with severe traumatic brain injuries according to the time of surgical treatment.
PATIENTS AND METHODS: We studied the clinical, radiologic findings and outcome of patients with severe traumatic brain injuries that were operated between 2012-2013 in our hospital. The patients were followed postoperatively with several cranio-cerebral cT exams. The outcome was assessed by Glasgow Outcome scale.
RESULTS: 259 patients were diagnosed with severe traumatic brain injuries and they were operated for that in our department between 2012-2013.
CONCLUSIONS: In our opinion the best results were achieved at the patients whose surgical treatment was initiated immediate after trauma.
Keywords: severe cranio-cerebral trauma

The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
94
P13. POSTTRAUMATIC EPICRANIAN ARTERIO-VENOUS FISTULA –CASE REPORT
M.R.Gorgan, F.M. Brehar, Aurelia Mihaela Sandu, V.M. Pruna, Anamaria GheorghiuFourth Department of Neurosurgery, Emergency Clinical Hospital Bagdasar-Arseni
Posttraumatic arterio-venous fistulas are rare lesions which occur at various periods of time after the initial traumatic injury. Epicranian locations are usually related to open wound injuries of the scalp which involve major feeding arteries of the scalp.The authors of this presentation report the case of a 28 year-old male which presented an open injury of the scalp with the involvement of the right superficial temporal artery. The wound was treated in another department. At one month after the initial injury, patient presented tinnitus and right hemicrania. patient was admitted in our department and local exam revealed a subcutaneous pulsatile right temporal mass and right temporal bruit. Patient had no neurological deficits.cerebral angiography (which included external carotid catheterization) showed an ar-teriovenous fistula between right superficial temporal artery and right external jugular vein. We chose to treat surgically this lesion due to its superficial and accessible loca-tion. A linear right temporal preauricular incision was performed and after subcutaneous dissection, an arterioven ous fistula with feeders from right superficial temporal artery was found, located superficial to temporal muscle fascia. Total resection was performed.postoperative cerebral angiography showed total removal of the lesion. patient was dis-charged with no neurological deficits. Tinnitus and bruit remitted completely.Posttraumatic epicranian arteriovenous fistulas are rare lesions which are suitable to sur-gical resection due to their superficial and accessible location.
Keywords: arteriovenous fistula, posttraumatic, surgical resection
Abstract Papers
95
P14. COMPLICATIONS RELATED TO SEVERE CEREBRAL VASO-SPASM AFTER ANEURYSMAL SUBARACHNOID HEMORRHAGE
D.A. Petrescu, L. Danaila, St. Dima, Otilia Petrescu, C. Preoteasa, S. SudituNational Institute of Neurology and Neurovascular Diseases - Bucharest, Neurosurgery, Romania
INTRODUCTION: Vasospasm is a common complication that may occur after aneu-rysmal subarachnoid hemorrhage. Irritating blood breakdown products cause the walls of an artery to contract and spasm. The prolonged smooth muscle contraction involves some alteration in the structure of the arterial wall (hypertrophy, fibrosis, degeneration), that reduces blood flow to a specific vascular territory causing a secondary stroke.
PATIENTS AND METHODS: Our study includes 1294 cases of cerebral aneurysms, diagnosed angiographic (38,64%), out of 3348 cerebral angiographies, performed in Neurosurgical Department of National Institute of Neurology and Neurovascular Dis-eases, during a period of 5 years. Of all discovered aneurysms, 1186 (91,65%) were broken and they started with subarachnoid and/or cerebral hemorrhage. The remain-ing 108 (8,35%), were incidentally detected during investigations for other diseases. 1242 (95,98%) of all detected aneurysms were treated with surgical clipping and only 28 (0,84%), were treated with endovascular procedures. The remaining 24 (0,71%) were not treated, either because of refusal, or because bad conditions that resulted in death. A total of 423 cases with broken aneurysms (35,66%) had a deterioration of awareness and neurological deficits, secondary outbreaks of cerebral hemorrhage and/or angiographic demonstrated vasospasm. The vasospam was present in a number of 318 cases (26,81%). The meaning of the present paper, we have defined the severe vasospasm, that change of vascular diameter, angiographic, demonstrable, responsible exclusively for major neu-rological deficits, stable and irreversible after the conventional therapy applied in accor-dance with medical protocols, which led to the invalidity or death.
RESULTS: 129 patients (10,88%) had a good recovery, after correct treatment of vaso-spasm with nimodipine in continuous intravenous perfusion or local intra arterial, 113 (9,53%) survived with a minimal disability, 50 (4,21%) survived with major focal neu-rological deficits and 26 (2,19%) died. Both, the correct treatment of aneurysms and the postoperative presence of vasospasm were angiographic demonstrated in all cases.
CONCLUSIONS: Recovery and prognosis are highly variable and largely dependent on the severity of the initial vasospasm.
Keywords: cerebral aneurysm, subarachnoid hemorrhage, vasospasm, cerebral angi-ography
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
96
P15. SUBARACHNOID HAEMORRHAGE IN MULTIPLE INTRACRA-NIAL ANEURYSMS
V. Munteanu, R. Stanescu, Diaconu NicoletaNeurosurgical Clinic, “Bagdasar – Arseni” Clinical Hospital, Bucharest, Romania
BACKROUND: Intracranial aneurysms are common and are located on the large arter-ies of the circle of Willis and its branches. Autopsy series uncover them in 0.4–3.6% of individuals, whereas cerebral angiography documents incidental aneurysms in 3.7–6.0% of patients. Therefore, roughly 2% of all individuals harbor aneurysms. Approximately 80–85% of these lesions are in the anterior cerebral circulation, and the rest are in the posterior circulation. cerebral aneurysms are multiple in 25% of cases
METHODS: case A – a 51 years old woman was admitted for headache, dysarthria, severe episthaxis, and balance disorder. case B- a 64 years old man was admitted for headache, neck pain, balance disorder and vomiting. Results- case A - Four-vessel angiography disclosed sacular aneurysm at the bifurcation of the left McA, with maximum diameter of 4.46 mm and neck of 2.36, and another one aprox. 3mm distance from the first aneurysm anterior oriented with maximum diame-ter of 4.73mm , neck of 2.27mm. case B- Four vessel angiography disclosed ruptured aneurysm with daughter sac inserted at the origin of the left pericalosal artery, with 3,9/3.5mm diameter, 2mm neck. In both cases cT scan revealed sAH.
CONCLUSION: Familial aneurysms are generally larger at time of rupture and morelikely to be multiple than sporadic aneurysms. The development of largeand multiple aneurysms may be related to genetic factors that determinedefects of the arterial wall.
Keywords: Intracranial ruptured aneurysms, four-vessel angiography, SAH, genetic fac-tors.

Abstract Papers
97
P16. SURGICAL TREATMENT OF BASILAR APEx ANEURYSM-CASE PRESENTATION
A. Spatariu1, C. Pascal1, P. Petrescu1, Barari1, Al. Tascu1,2
11st Neurosurgical Department Bagdasar Arseni Hospital Bucurest. Romania2Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bucharest
posterior circulation aneurysms represent a special challenge to neurosurgeons because of the deep location and intimate reports with brainstem, cranial nerves and perforating arteries.Despite progress in neurosurgical techniques, neuroanastesiology, neuroradiology, the surgical treatment of basilar apex aneurysms shows a higher morbidity and mortality than aneurysms of anterior circulation.The inability to perform microsurgical clipping of basilar apex aneurysms has led to the development of other treatment modalities such as endovascular therapy. However, en-dovascular coil occlusion is less durable than microsurgery, as shown by its higher rates of aneurysm recanalization and regrowth and microsurgery provided better outcome in some specific basilar apex aneurysms.In this paper we present the case of a patient with subarachnoid hemorrhage Hunt & Hes-s1becouse of a rupture of basilar apex aneurysm susccessfuly treated by microsurgical clipping using a subtemporal route. Outcome was assessed by Glasgow Outcome scale : GOs-GR.
Bibliography:Angiographic and clinical results in 316 coil-treated basilar artery bifurcation aneurysms.Henkes H, Fischer s, Mariushi W, Weber W, Liebig T, Miloslavski E, Brew s, Kühne DJ Neurosurg. 2005 Dec; 103(6):990-9.schievink WI, Wijdicks EF, piepgras DG, chu cp, O'Fallon WM, Whisnant Jp.The poor prognosis of ruptured intracranial aneurysms of the posterior circulation. J Neurosurg. 1995 May; 82(5):791-5.Bavinzski G, Killer M, Gruber A, Reinprecht A, Gross cE, Richling B.Treatment of basilar artery bifurcation aneurysms by using Guglielmi detachable coils: a 6-year experience. J Neurosurg. 1999 May; 90(5):843-52.Eskridge JM, song JK. Endovascular embolization of 150 basilar tip aneurysms with Guglielmi detachable coils: results of the Food and Drug Administration multicenter clinical trial.J Neurosurg. 1998 Jul; 89(1):81-6.Vallee JN, Aymard A, Vicaut E, Reis M, Merland JJ. Endovascular treatment of basilar tip aneurysms with Guglielmi detachable coils : predictors of immediate and long-term results with multivariate analysis 6-year experience. Radiology. 2003;226:867–879.
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
98
P17. RARE CASE OF ANEURYSM ASSOCIATED WITH PORPHYRIA
Mihaela Cosman1, A. Iordache1, N. Dobrin1, Al. Chiriac1, I. Poeata1,2
1Emergency Prof. Dr. N. Oblu Hospital, Neurosurgery III, Iasi, Romania2Gr.T. Popa University of Medicine and Pharmacy, Neurosurgery, Iasi, Romania
INTRODUCTION: Association between porphyria and cerebral aneurysm is a rare situation. The initial presentation of our patient is atypical: vertigo, bradycardia and de-pression.
PATIENTS AND METHODS: The patient known with acute intermittent porphyria was examined initially by neurologist and sent to psychiatry and cardiology. The patient came back to neurosurgery : the cT scan showed subarachnoid hemorrhage and angiocT showed an aneurysm of the M1 on the right side. Due to her history we decided to use an endovascular approach.
RESULTS: The procedure was successful we have obtained an initial obliteration of more than 90%.
CONCLUSIONS: Although there were many discussions about the treatment the endo-vascular coilling was suitable for this patient.
Keywords: aneurysm, porphyria, endovascular coilling
Abstract Papers
99
P18. VOLUMETRIC ASSESSMENT OF INTRACRANIAL ANEURYSMS FROM 3D ROTATIONAL ANGIOGRAPHY
Al. Chiriac, B. Iliescu, F. Ziyad, I. Poeata"Gr. T. Popa" University of Medicine and Pharmacy, Iasi, Neurosurgery, Romania
INTRODUCTION: The 3D rotational angiography is an increasingly used method for cerebral aneurysms treatment planning. Volume measurement techniques of intracranial aneurysms from 3D rotational angiography vary on different factor settings and, there-fore, are operator-dependent.
METHODS: In this study we evaluate the application and the precision of ellipsoidal approximation (mathematics and computer technique) and software methods to measure intracranial aneurysms volume starting from planar (DR and sD) and 3-dimensional (3D) angiographic images. Retrospective assessment of aneurysm volume was achieved with two measurement methods by using two-dimensional copies or 3D reconstruction images (digital or printed form in sagittal and coronal angiography section) obtained with a siemens Artis Angiograph with rotational digital subtraction possibilities. The re-liability of the methods was statistically compared in a clinical setting of 42 angiograms and 100 measurements performed by the same users.
RESULTS: Based on statistical analysis obtained from the Friedman test we found sta-tistically significant differences at p £ 0,05 threshold between the three techniques of analysis [?2 (2) = 8.714, p = 0.013]
CONCLUSIONS: This study suggests that both techniques could be used for clinical applications with similar efficiency results.
Keywords: aneurysm, 3D rotational angiography
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
100
P19. THE EFFECT OF EPIDURAL INSTILLATION OF DExAMETHA-SONE ON LOCAL SCARING TISSUE AFTER LUMBAR MICRODISCECTOMY
G. Vasilescu, V. Ciubotaru, B. Ghinguleac, A. SpatariuNeurosurgical Clinic, “Bagdasar – Arseni” Clinical Hospital, Bucharest, Romania
BACKGROUND: Lumbar disc herniation is a pathological condition that appears in 1% to 3% of the general population, being influenced by age, usually between 30 and 50 years, gender, male to female ratio is higher in male (2:1), working conditions, with higher incidence on patient who have an intense physical work, professional drivers etc. In the literature the overall recurrence rate is around 7 to 12% of the total cases operated by microdiscectomy. In the senior authors series the recurrence rate is 3.5%.
METHODS: The authors have analyzed the incidence of local compressive tissue af-ter lumbar disc herniation microdiscectomy requiring surgical removal comparing the patients where Dexamethasone was used intraoperative and those where corticoid instil-lation was not performed. Length of the surgical procedure, difficulty of dissection and the volume of the compressive/adherent epidural tissue were chosen as the comparison criteria.
RESULTS: As a result of corticoid epidural instillation after microdiscectomy the ad-herential scaring process is reduced dramatically with the condition of performing a proper foraminectomy when the genuine microdiscectomy is done. The overall volume of compressive scar requiring surgical removal after microdiscectomy was not influ-enced by the use of dexamethasone and may depend on personal factors. The duration of the surgical procedure, the ease of the dissection process itself and the much lower occurrence of dural tear are the main benefits of the epidural corticoid instillation.
CONCLUSION: The epidural instillation of one vial of dexamethasone after microdis-cectomy represents a simple gesture devoid of risk that is useful for those cases where a second surgical decompressive procedure is needed.
Keywords. epidural instillation, Dexamethasone, microdiscectomy
Abstract Papers
101
P20. LUMBAR-PELVIC STABILIZATION USING ILIAC SCREWS IN A CASE OF A LUMBAR-SACRAL GIANT TUMOR
M. Catana1, V.M. Prună1,2, M.R. Gorgan1,3
1Clinical Hospital “Bagdasar-Arseni”, Bucharest, Romania2Ph.D. Student in Neurosurgery University of Medicine and Pharmacy “Carol Davila”, Bucharest3Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bu-charest
INTRODUCTION: The first lumkmbar-pelvic stabilization was described in 1982 by Allen and Ferguson. Indications for sacroiliac fixation include lumbosacral destructive processes (tumors, infections, trauma), pseudoarthrosis L5-s1, L5-s1, high grade spon-dylolisthesis, symptomatic lumbar spine deformities. symptoms consist in pain (in about 96% of cases), radiculopathy or cauda equine syndrome. The investigation of choice is the MRI with sagittal, coronal and axial acquisitions.
CASE PRESENTATION: A 58 y.o. woman, with breast cancer, was admitted in our clinic with low back pain, bilateral L5-s1 sciatica and cauda equina syndrome, Frankel D. Lumbar spine MRI shows a spinal tumor that destroyed the L5, s1 vertebral bodies, causing severe L5, s1 nerve roots and dural compression. The surgical treatment was performed by a total L5 vertebrectomy and partial s1 (involved by tumor) and the spinal canal and the neuroforamina was decompressed. spinal reconstruction was achieved using acrylic cement with contention in vertebral body L4 and s2 segment of the sacrum. surgical stabilization was performed with titanium polyaxial screws into L3-L4-s1 bilat-eral pedicles and two titanium screws (with a length of 90 mm) in both iliac wings. We used the Zodiac spinal Fixation system by Alfa Tech.The technique of the placement of iliac screwsAfter the posterior superior iliac spines (PSIS) were identified, the iliac screws insertion points were located at about 1 cm inferior to the psIs and 1 cm proximal to the distal edge of psIs. The screws were about 90 mm in length and 8.5 mm in diameter. The two iliac screws were connected to the system via two connectors. postoperative outcome was favorable and local pain disappeared. Neurological deficits begin to improve and the spinal stability was achieved. No postoperative complications. Hystological examina-tion: metastasis of adenocarcinoma (possible breast cancer).The patient was discharged 8 days postoperatively.
CONCLUSIONS: The lumbar-pelvic fixation is a relatively easy technique, and sta-bilisation with transiliac screws is sometimes necessary, when the tumor invades the lumbar-sacral junction and the spinal stability was definitely compromised.
Key words: lumbar-sacral junction, vertebral tumor, lumbar-pelvic fixation
The 39th Congress of the Romanian Society of Neurosurgery with International ParticipationBucharest, September 18th - 21th. 2013
102
P21.TITANIUM ExPANDABLE CAGE – AN ExCELENT CHOICE FOR THE SURGICAL TREATMENT OF CERVICAL SPINAL METAS-TASIS
M. Catana1, V.M. Prună1,2, M.R. Gorgan1,3
1Clinical Hospital “Bagdasar-Arseni”, Bucharest, Romania2Ph.D. Student in Neurosurgery University of Medicine and Pharmacy “Carol Davila”, Bucharest3Clinic of Neurosurgery - University of Medicine and Pharmacy “Carol Davila”, Bu-charest
INTRODUCTION: spinal metastases are the most common malignant lesions of the spine (over 94 %). clinical symptoms consist in neck pain (90%) and various degrees of motor deficits (over 50% of patients). The most common type are osteolytic when osse-ous destruction can lead to fracture of the vertebral body, spinal instability and deformity of the spine. Because the majority of cervical metastases develops in the vertebral body, the anterior cervical approach is most suitable for surgery. The surgery goals are: de-compression of spinal cord, spinal reconstruction and spinal stability. cervical spine re-construction after corporectomy can be done using several methods, such as: bone graft, bone cement, titanium Mash, expandable cage. The expandable cages are cylindrical devices, with different shapes and sizes which facilitates stability of the spine. The cage can be filled with bone allograft or bone substitute.
CASE PRESENTATION: A 69 y. o. woman, was admitted in our clinic for neck pain, incomplete tetraplegia, with c6 level (Frankel D). cervical MRI reveals a c6 vertebral body tumor, with spinal cord compression and vertebral collapse. No history of neoplas-tic disease, but the cT scan of the thorax showed an expansive process in the right infe-rior lobe. No other lesions - in the brain or abdominal cavity. The surgery was performed by an anterior cervical approach with c6 corporectomy, spinal cord decompression and spinal reconstruction using titanium expandable cage (CAGE-LOC by BIOTEK), filled with bone substitute (synthetic phosphocalcic Hydroxyapatite - Nanogel). Extension mechanism was secured by 2 screws that block the mechanism extension. pathological examination found metastatic adenocarcinoma, probably pulmonary origin. postopera-tively the patient's evolution was favorable, drainage was suppressed at 24 hours after surgery. second day, she was mobilized. she was discharged at 7 days after surgery.
CONCLUSIONS: Fully ablation of the cervical spinal metastasis can be easily per-formed through a cervical anterior approach. Once the corporectomy was done, recon-struction of the vertebral body and spine stabilization are mandatory. The expandable cages represent an excellent and safe option for the vertebral reconstruction.
Keywords: spinal metastasis, cervical vertebral body, expandable cage
INDEXAAdam D. 62Aldea C. C. 75Alexandru Oana 88Andrasoni Z. 17, 46Andronic D. 19, 64Andronic M. 19, 60Apetrei C. 17, 22, 45, 70, 78Arsene D. 18, 55
BBarborica A. 21, 74Baritchii A. 17, 46Borodin S. 19, 60Bostan Al. 19, 60Brehar F.M. 16, 20, 44, 54, 55, 68, 84, 94Bucur Narcisa 16, 18, 20, 44, 54, 67, 68, 84
CCalina N. 19, 57Catana M. 101, 102C. C. Aldea 75Checiu G. 19, 57Chelsoi M. 17, 47Chiriac Al. 16, 22, 43, 78, 91, 98, 99Chirita B. 19, 61, 64Cioplean Daniela 21, 71Ciubotaru V. 17, 18, 47, 48, 52, 81, 86, 87, 88, 100Ciurea Ana 21, 74Ciurea A.V. 48, 58, 76Ciurea J. 74Coman Teodora 21, 74Cosman Mihaela 98
DDabija M. 64Danaila L. 18, 56, 95Dăncescu M. 21, 76David G. 21, 76
Dediu Adriana 18, 52, 86Diaconu Nicoleta 21, 74, 96Dima St. 23, 80, 95Dobrin N. 16, 43, 98Dricu Anica 17, 18, 47, 52, 81, 88Dumitrescu B. 81
EEnache A. 50Ene L. 88Exergian F. 19, 57
FFlorea Mihaela 17, 51Florian I.S. 21, 42, 46, 75Frumusachi V. 19, 60
GGari G. 21, 74Gheorghiu Anamaria 16, 44, 67, 84, 94Ghinguleac B. 100Giovani A. 16, 44, 67, 84Gorgan M.R. 18, 20, 21, 44, 54, 55, 67, 68, 71, 73, 84, 86, 87, 94, 101, 102
HHornea Ioana 19, 62
IIacob G. 63Iencean A. St. 20, 21, 66, 69, 73, 83Iencean St. M. 20, 66, 69, 73, 83Iliescu A. 17, 50, 51Iliescu B. 19, 22, 45, 64, 78, 91, 99Iliescu R. 19, 62Iordache A. 98Iosif A. 17, 46I. Poeata 17, 45Istvan K. 89
KKiss P. 16, 42
LLisievici M. 17, 18, 48, 55Luca-Husti I. 15, 17, 21, 48, 58, 76
MMaior T. 65Marginean L. 23, 80Marin A. 19, 60Martin D. 16, 20, 44, 67, 84Mohan D. 15, 58Moisa H. 15, 17, 21, 48, 58, 76Moisescu Cristina 19, 62Munteanu V. 82, 96
NNeacsu Angela 16, 18, 20, 44, 54, 67, 68, 84Nita Antonia 16, 43Nour Marcela 93Nuteanu L. 17, 50, 51
OOgrezeanu I. 17, 48
PPapacocea T. 19, 62Pascal C. 17, 50, 51, 97Paunescu D. 17, 47, 87Petrescu D.A. 18, 56, 95Petrescu Otilia 95Petrescu P. 97Podea M. 57Poeata I. 17, 19, 20, 21, 43, 45, 64, 66, 69, 73, 78, 83, 85, 91, 93, 98, 99Popescu Alisa 18, 52, 88Predoaica Smaranda 16, 22, 43, 78, 91Preoteasa C. 95Pruna Violeta Ioana 71, 86Pruna V.M. 16, 18, 20, 21, 44, 54, 67, 68, 71, 84, 94, 101, 102
RRadoi M. 56, 80Rasina A. 21, 74
Renta Mirela 21, 74Rizea R.E. 17, 50Rotariu D. 17, 45, 85, 91
SSandu Aurelia Mihaela 16, 18, 20, 44, 54, 67, 68, 84, 94Secara B. 20, 69, 83Serban D. 57Spatariu A. 97, 100Stanescu R. 82, 96Stefanescu F. 18, 23, 56, 80Streltov I. 93Stroi M. 18, 22, 53, 79, 92Suditu S. 18, 56, 95
TTascu A. 20, 21, 50, 51, 66, 73, 97Tataranu Ligia 17, 21, 47, 52, 71, 81, 86, 87, 88Toader C. 53, 79, 92Trifoi S.V. 16, 42
VVakilnejad R. 18, 56Vapor Iulia 17, 50, 51Vasilescu G. 100Volovici V. 21, 75V. Volovici2 21, 75
ZZamfir C. 19, 57Zamfir O. 16, 44, 67, 84Zapuhlih G. 60Ziyad F. 16, 17, 20, 22, 43, 45, 69, 78, 83, 85, 91, 99