Embed Size (px)
Citation preview
0 Ophthalmic Genetics 0167-6784 94
U S $ 3 50 pig menti The blinding mechanisms of incontinentia
Ophthalmic Genetics-- 1994, Phi. 15,
0 Bolus Press Buren (The Netherlundsj 1994
Accepted 24 May 1994
No. z pp. 69 - 76 Morton F. Goldberg
The Wilmer Eye Institute Johns Hopkins University School of Medicine, Baltimore, MD, USA
Abstract The ocular and cerebral abnormalities associated with inconti- nentia pigmenti, an X-linked dominant disease with characteristic cutaneous features, are far worse than the name would indicate. Although some patients have normal vision, total blindness or permanent visual deficiency may occur. Retinal vascular abnormalities, involving the periphery as well as the macula, appear to represent the primary disease process in the eye. Retinal detachment may then ensue, due to mechanisms that seem analogous to those of retinopathy of prematurity. Optic nerve atrophy and occipital lobe infarction are additional causes of severe visual dysfunction in some pa- tients. For the first time, neonatal infarction of the macula is documented in this disease. The purpose of this report is to describe the visually disabling ocular and cerebral manifestations in five selected cases of incontinentia pig- menti.
Key words Incontinentia pigmenti; retinopathy of prematurity; retinal detachment; macular dystrophy: macular dysplasia; cortical blindness; reti- nal neovascularization
Methods The case histories of five patients personally evaluated by the author from I990 through 1993 were reviewed for evidence of severe visual impairment, and the mechanisms of blindness or reduced vision were identi- fied in each case. Four of these patients have had some of their clinical features published previously,’ but the mechanisms of loss of vision were not empha- sized or fully understood. The diagnosis of incontinentia pigmenti was made by a combination of characteristic physical findings, skin biopsy, andlor positive family history.’ Milder cases, some with no visual or other symp- toms whatsoever, were reported previously,’ and are not included here.
Case reports
Case I This patient has previously been reported in part (Case 6 in ref. No.1). Her first retinal examination occurred at seven months of age, and ‘foveal hypoplasia’, consisting of abnormal pigmentation, an absent foveal light reflex and abnormal blood vessels traversing the center of the macula were noted (Fig. 2 in ref. I), primarily in the right eye. Between three months
Thc blinding mechanisms of incontinentia pigmenti
Correspondence to: Morton F. Goldberg, M.D.,The Wilmer Eye Institute, Johns Hopkins University School of Medicine, 727 Maumenee Building, 600 North Wolfe Street, Baltimore, MD 21287, USA
AcknoiLdedgements: The author thanks Thomas Connor, M.D., Michael Repka, M.D., and David Valle, M.D. for referral and care of some of these patients, and the Wilmer Photographic Service for fundus angiograms.
Supported in part by Core Grant P30 EYor765 from the National Eye Institute, Bethesda, Maryland, by an unrestricted research grant from Research to Prevent Blindness, Inc., and by the Guerrieri Retinal Research Fund at Johns Hopkins University
Presentedut the 130th Meeting of the American Ophthalmological Society, Pebble Beach, California, May, 1994
69
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
saka
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

Fig. I. Case I . Fluorescein angiogram at 33 months of age. Notice absence of normal foveal avascular zone (in center of photo) OD.
and twelve months of age, the patient developed constant esotropia OD of 30 to 40 prism diopters. Cycloplegic refraction was +4.50 sph OD and +3.00 sph 0s. Occlusion therapy of the left eye was performed, but, because of poor macular function, there was no visual fixation OD by 17 months of age. The optic nerves appeared normal, and the retinas were attached.The macula OD continued to show angiographic evidence of an abnormally perfused foveal center (Fig. I); ie . , there was no foveal avascular zone. This appeared to be the major cause of severely reduced vision in the right eye.
Caw 2 This patient has previously been reported in part (Case 13, in ref. No. I). At the time of original publication (age one year), foveal abnormal- ities had not been noted by ophthalmoscopy. There had never been any known perception of light in either eye, because extensive infarction of the right and left occipital cortex and other intracranial structures had occurred between day 3 and day 6 of life.' Moreover, both optic nerves were very pale.
A fluorescein angiogram was first done at 20 months of age under general anesthesia. Although the maculas appeared ophthalmoscopically normal, and the retinas were flat and attached, the angiogram, nevertheless, showed an abnormally large zone of avascularity of the perifoveolar area in the left
Fig. 2a. Case 2. Fluorescein angiogram at 20 months of age. Note marked ischemia of left macula (straight arrow) and tuft of neovascularization (curved arrow).
Fig. zh. Case 2. Fluorescein angiogram at 20 months of age. Photographed area is contiguous with Fig. 2a. Curved arrow shows tuft of perifoveolar neovascularization. Straight arrow shows additional extensive zone of nonperfusion in adjacent posterior pole.
M. E Goldberg
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
saka
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.
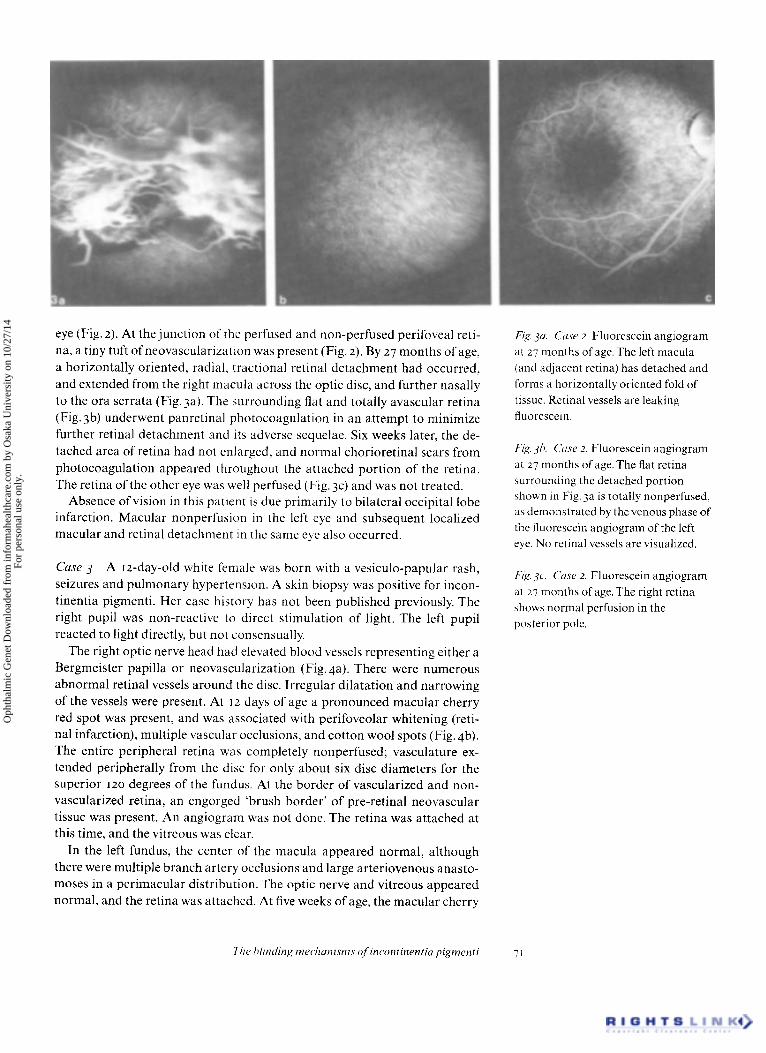
eye (Fig. 2). At the junction of the perfused and non-perfused perifoveal reti- na, a tiny tuft of neovascularization was present (Fig. 2). By 27 months of age, a horizontally oriented, radial. tractional retinal detachment had occurred, and extended from the right macula across the optic disc, and further nasally to the ora serrata (Fig.3a). The surrounding flat and totally avascular retina (Fig. 3b) underwent panretinal photocoagulation in an attempt to minimize further retinal detachment and its adverse sequelae. Six weeks later, the de- tached area of retina had not enlarged. and normal chorioretinal scars from photocoagulation appeared throughout the attached portion of the retina. The retina of the other eye was well perfused (Fig. 3c) and was not treated.
Absence of vision in this patient is due primarily to bilateral occipital lobe infarction. Macular nonperfusion in the left eye and subsequent localized macular and retinal detachment in the same eye also occurred.
Case 3 A 12-day-old white female was born with a vesiculo-papular rash, seizures and pulmonary hypertension. A skin biopsy was positive for incon- tinentia pigmenti. Her case history has not been published previously. The right pupil was non-reactive to direct stimulation of light. The left pupil reacted to light directly, but not consensually.
The right optic nerve head had elevated blood vessels representing either a Bergmeister papilla or neovascularization (Fig. 4a). There were numerous abnormal retinal vessels around the disc. Irregular dilatation and narrowing of the vessels were present. At 12 days of age a pronounced macular cherry red spot was present, and was associated with perifoveolar whitening (reti- nal infarction), multiple vascular occlusions, and cotton wool spots (Fig. 4b). The entire peripheral retina was completely nonperfused; vasculature ex- tended peripherally from the disc for only about six disc diameters for the superior 120 degrees of the fundus. At the border of vascularized and non- vascularized retina, an engorged 'brush border' of pre-retinal neovascular tissue was present. An angiogram was not done. The retina was attached at this time, and the vitreous was clear.
In the left fundus, the center of the macula appeared normal, although there were multiple branch artery occlusions and large arteriovenous anasto- moses in a perimacular distribution. The optic nerve and vitreous appeared normal, and the retina was attached. At five weeks of age, the macular cherry
Fig. jtr. Cctsr 2. Fluorescein angiogram at 27 months of age. The left macula (and adjacent retina) has detached and forms a horizontally oriented fold of tissue. Retinal vessels are leaking fluorescein.
Fig. 3h. Cctsr 2. Fluorescein angiogram at 27 months of age. The flat retina surrounding the detached portion shown in Fig.3a is totally nonperfused, as demonstrated by the venous phase of the fluorescein angiogram of the left eye. No retinal vessels are visualized.
Fig. 3 ~ ' . Crise 2. Fluorescein angiogram at 27 months of age.The right retina shows normal perfusion in the posterior pole.
17ir hlincling mrc~litrnisnis of incontinentia pignzenti 7'
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
saka
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

Fig. 4a. Case 3. Black and white image from color fundus photograph at 12
days of age. Note abnormal vessels on disc (straight white arrow), irregularly dilated vessels (curved white arrows), and a large number of abnormal peripapillary retinal vessels. Black arrows show cotton wool spots (cJ Fig. 4b).
Fig. 46. Case 3. Black and white image from color fundus photograph at 12 days of age is contiguous to that shown in Fig. 4a. Note cherry red spot (‘!’) surrounded by many occluded small vessels. Also note cotton wool spots in papillomacular bundle area (arrows).
Case 4 This patient has previously been published in part (Case 12, in ref. No. I). When first examined at 64 months of age, there was absence of light perception OD and intact fixation and following behavior 0s. A tractional retinal detachment extended from the right disc through the macula to the temporal ora serrata. Within four months, the detachment had become
Fig. 5a. Case 4. Fluorescein angiogram at eight months of age. Red-free fundus photo prior to injection of fluorescein shows vessels traversing region of foveal center.
red spot was no longer visible in the right eye. It would have been virtually impossible to intuit its previous presence, despite the severity of the in- farctive process, Progression of the preretinal neovascularization OD had occurred. Vitreoretinal traction and vitreous hemorrhage were present OD. Panretinal photocoagulation was performed with a diode laser (indirect ophthalmoscope delivery system), and one month later, no active neovas- cularization or retinal detachment was present OD. One month thereafter, however, there was a total inoperable retinal detachment. In the left eye, spontaneous regression of the retinopathy had occurred. At that visit there was no response to light in the right eye and some blepharospasm to light in the left eye. The child would not fixate or follow objects with either eye.
Poor vision in this patient’s right eye is due primarily to macular and reti- nal infarction and, secondarily, to retinal detachment. The explanation for poor vision in the left eye is obscure, but may be related to extensive occipital defects in the brain that were evident on computed tomographic and mag- netic resonance imaging.
Fig. 5b. Case 4. Fluorescein angiogram at eight months of age. Fluorescein angiogram shows absence of foveal avascular zone.
72 M. I; Goldberg
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
saka
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

total, and a retrolental white fibrovascular mass of tissue was present. B-scan ultrasonography showed that the eye had stopped its normal neonatal en- largement and was smaller than the normal left eye (early phthisis bulbi). At 6; months of age, a blunted foveal pit 0s was seen during an examination under anesthesia, and fluorescein angiography showed blood vessels travers- ing the normally avascular foveal center. At 20 months of age, repeat fluor- escein angiography showed an unchanged appearance in the macula. Peri- pheral retinal non-perfusion persisted. Most areas of peripheral preretinal neovascularization had spontaneously regressed.
Loss of vision OD was due to retinal detachment. The visual acuity 0s is expected to be reduced because of the missing foveal avascular zone.
Case 5 This patient has previously been published in part (Case 4, in ref. No. I). She was severely retarded, and had been kept at home, largely in bed, for almost all her life. She was incapable of speech, and visual acuity could not be tested precisely. When first examined at age 33, she had no light perception OD; she fixated and followed a light 0s. Optic disc atrophy and a blunted foveal pit were present OD. In addition, a curvilinear pigmented zone of pe- ripheral retina was present OD from 8 to 11 o’clock, compatible with a spon- taneously re-attached retinal detachment. The fundus of the left eye appeared normal. An angiogram was not done.
Absent vision in the right eye appeared secondarily to optic atrophy, ab- normal macular development, and possibly an antecedent retinal detach- ment that had spontaneously reattached. The intracranial visual pathways could not be accurately assessed.
Discussion Although the neonatal vesicular rash of incontinentia pig- menti is obvious and distressing to both physicians and parents, these cases demonstrate that major, life-long morbidity is more importantly affected by the potential cerebral and retinal abnormalities that appear to be character- istic of this disease. Severe retinal manifestations may be completely inap- parent, however, unless newborn babies with this disease are subjected to routine dilated fundus examinations with scleral depression and, especially, intravenous retinal angiography. All portions of the retinas as well as the optic nerves should be angiographically or angioscopically studied, and the status of the foveal avascular zone should be specifically evaluated. In addi- tion, cerebral complications affecting the visual (and other) pathways may not be obvious unless brain scanning is performed.
Vaso-occlusion in the retina appears to be an early (if not the initial) mani- festation of this disease. Infarction of retinal areas (which can be extensive) can lead to permanent loss of either peripheral or central vision, or both. Optic nerve pallor, observed ophthalmoscopically, possibly may be the result of vascular hypoperfusion in either the optic nerve itself, or in the retina, or may be secondary to pathologic intracranial processes.
In a previous communication,’ the term foveal ‘hypoplasia’ was used to describe an absent or anomalous avascular zone (with retinal vessels travers- ing the foveal center) in young children with incontinentia pigmenti. It was implied that the foveal abnormality was truly congenital, and that its patho- genesis was ‘developmental’ and had probably occurred in utero. Although this scenario may accurately explain some instances of this neonatal (and adult) vasculopathy, the ophthalmoscopic and angiographic appearances of
The blinding mechanism., of incontinentia pigmenti 73
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
saka
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

Case 3 (specifically, a macular cherry red spot and perifoveal vascular non- perfusion at 12 days of age) clearly support the conclusion that remarkable vascular shutdown and macular infarction can occur post-natally within days or weeks of birth in this disease. Subsequent re-modeling of the peri- foveolar vasculature may cause the altered, so-called 'hypoplastic' appear- ance with absence of the normal foveal avascular zone and blunting or absence of the foveal pit. Reduced or absent vision, sometimes with second- ary strabismus, are logical sequelae. Detection of the cherry red spot and the white infarcted macular tissue was fortuitous, and depended exclusively on our examination occurring during the actual, brief, infarctive episode. Such episodes would usually be missed in most infants with this disease. Their prior occurrence would be difficult to intuit, because the retina assumes normal coloration after the acute process has terminated. Ophthalmic consultation, if it occurs at all, usually would take place much later in the evolution of the disease, and the cause of poor vision might therefore be difficult to determine. In some patients, such as Case 2, the macula may appear ophthalmoscopi- cally normal, but angiography may reveal non-perfusion, abnormal perfu- sion, or even neovascularization.
Later effects of retinal non-perfusion are similar and probably analogous to those of retinopathy of prematurity; i.e., pre-retinal neovascularization, intra-vitreal hemorrhage, vitreous traction, combined rhegmatogenous and non-rhegmatogenous retinal detachment^,^,^ and amblyopias with varied pathogeneses. A similar sequence of pathologic events also can occur in vaso-occlusive retinopathies of widely different etiologies, such as diabetes mellitus, sickle cell anemia, retinal branch vein occlusion, dominant exuda- tive vitreoretinopathy, and others. In severe cases, chronic retinal detach- ment can result in cataract, rubeosis, and phthisis bulbi. Previous reports435 implying that abnormalities of the retinal pigmented epithelium (R P E) are responsible for the retinal detachments may not be correct. There have been no opththalmoscopically or angiographically demonstrable abnormalities of the R P E in the patients reported herein, and previously published histologic abnormalities of the R P E probably represent end-stage, rather than primary, pathogenetic mechanisms.435 The ophthalmoscopic and angiographic obser- vations from our cases strongly suggest that ischemia in the sensory retina, with its vasoproliferative sequelae, rather than R P E abnormalities, consti- tutes the primary pathogenesis of eventual retinal detachment in incontinen- tia ~ i g m e n t i . ~ . ~ The cause and time of onset of the retinal vaso-occlusions are not completely clear. It is not known whether absence of retinal vessels is sometimes truly developmental ('Fehlanlage')7 and intrauterine in onset, or secondary to some undefined set of postnatal stimuli. The macular cherry red spot in Case 3, as noted previously, suggests that, at least in some in- stances, retinal vessels do form in utero, but then close after birth.
Whether or not the cerebral manifestations" of incontinentia pigmenti are due to vascular insufficiency analogous to that of the retina remains to be proven. The similar embryologic origins of the retina and the brain make such a pathogenesis quite plausible. Magnetic resonance angiography and other flow studies of intracranial blood vessels should help elucidate this problem, and may offer therapeutic insight for what are now devastating and often untreatable consequences of the underlying disease. For example, attempts in the neonatal period to prevent vascular occlusions in the brain, as well as in the retina, theoretically might have merit.
74 M. E Goldberg
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
saka
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

Therapeutic possibilities for the more advanced retinal manifestations of incontinentia pigmenti include panretinal photocoagulation, cryocoagula- tion, vitrectomy, and scleral buckling. Their proper indications, techniques, and success rates remain to be
The relationships, if any, between the cutaneous manifestations and those of the retina (and possibly the brain) remain obscure. To date, there is little evidence to suggest that the typical inflammatory histopathology in the skin occurs in the retina or brain. Conversely, there is no current histopathologic evidence that vascular non-perfusion occurs in the skin, although the neo- natal blistering implies a possible vascular component. Acquisition of further basic information is necessary if a valid pathogenesis and appropri- ate therapy of this disabling disease are to be promulgated.
Summary Five case histories are utilized to illustrate the disabling visual diseases caused by retinal and cerebral infarction in incontinentia pigmenti. Cortical blindness was definitely present in one baby, who had bilateral ab- sence of light perception, and probably present in a second infant also.
Retinal detachment occurred in three eyes of three patients, one of whom had spontaneous reattachment. In a second patient, a partial tractional reti- nal detachment progressed within four months during infancy to a total, in- operable, retrolental, white fibrovascular mass mimicking Stage V retino- pathy of prematurity. Phthisis bulbi resulted. In a third patient, a localized tractional retinal detachment originated at the non-perfused macula and extended over a seven-month period to the ora serrata. Pre-retinal neovascu- larization waxed and waned in these and other patients.'
Abnormalities of the macula were pronounced, but were sometimes diffi- cult to detect. Their severity and relative frequency have not been previously described in detail. Abnormalities included blunting or absence of the foveal pit and absence of the normal foveal avascular zone. One patient at 12 days of age had an infarcted macula with a cherry red spot. Similar episodes may have occurred in other children and would be sufficient to explain the appear- ance of macular abnormalities and otherwise unexplainable poor visual acuity in older individuals. Well focused macular angiography appears to be highly useful in explaining visual disability due to abnormal foveal anatomy and function. Optic atrophy occurred in several eyes. Its pathogenesis may be multifactorial.
Further research is necessary in order to elucidate the mechanisms of vas- cular closure in the retina as well as the pathogenesis of destructive encepha- lopathy in this exceptionally severe disease. Valid therapeutic possibilities may then become more obvious than they are at present. It is possible that the retina and brain undergo similar disease processes in incontinentia pig- menti.
References Retinal detachments in incontinentia pigmenti. Arch Ophthalmol 1993: 111:
3 Catalan0 RA. Lopatynsky M. Tasman WS. Treatment of proliferative reti- nopathy associated with incontinentia pigmenti. Am J Ophthalmol 1990; IIO:
I Goldberg M E Custis PH. Retinal and 614 - 6 I 7. other manifestations of incontinentia pigmenti (Bloch-Sulzberger syn- drome). Ophthalmology 1993; 100:
1645- 1654. z Wald KJ, Mehta MC, Katsumi 0 et t i / . 701 -702.
The blinding mec.hunism.v of incontinentia pigmenti 75
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
saka
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

4 Rosenfeld SI, Smith ME. Ocular findings in incontinentia pigmenti. Ophthalmology 1985; 92: 543 -546.
5 Mensheha-Manhart 0, Rodrigues M, Shields JA, Shannon GM, Mirabelli RP. Retinal pigment epithelium in incontinentia pigmenti. Am J Ophthalmol 1975; 79: 571-577.
6 Heathcote JG, Schoales BA, Willis NR. Incontinentia pigmenti (Bloch- Sulzberger syndrome): a case report and review of the ocular pathological features. Can J Ophthalmol 1991; 26: 229 - 2.37.
7 Best W, Rentsch F. Uber das Pseudo-
gliom bei der incontinentia pigmenti. Klin Mbl Augenheilk 1974; 164: 19-32.
8 FranGois J. Incontinentia pigmenti (Bloch-Sulzberger syndrome) and retinal changes. Br J Ophthalmol 1984;
9 Spallone A. Incontinentia pigmenti. Br J Ophthalmol 1987; 71: 629 - 634.
10 Triki C, Devictor D, Kah S, Roge- Wolter M, Lacroix C,.Venencie PY, Landrieu P. Complications cerebrales de I’incontinentia pigmenti. Etude clinique et pathologique d u n cas. Rev Neurol 1992; 148: 773 - 776.
68: 19-25,
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
saka
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.













![First IKBKG Gene Mutation Study in Serbian Incontinentia ... · Incontinentia pigmenti (IP; Bloch-Sulzberg-er syndrome; MIM 308300) is a rare X-linked dominant genodermatosis [5]](https://img.pdfslide.net/doc/110x75/5f3bedf5651a4c1377610355/first-ikbkg-gene-mutation-study-in-serbian-incontinentia-incontinentia-pigmenti.jpg)















