Embed Size (px)
Citation preview
SCIENTIFIC/CLINICAL ARTICLE
JHT READ FOR CREDIT ARTICLE #244.
The Brachial Plexus Outcome Measure:Development, Internal Consistency, and
Construct Validity
Emily S. Ho, BScOT, OT Reg (Ont), MEdChristine G. Curtis, BScPT, MScDivision of Plastic and Reconstructive Surgery,Department of Rehabilitation Services, The Hospital forSick Children, University of Toronto, Ontario, Canada
Howard M. Clarke, MD, PhDDivision of Plastic and Reconstructive Surgery,Department of Surgery, The Hospital for Sick Children,University of Toronto, Ontario, Canada
Correspondence and reprint requests to Emily S. Ho, BSc OT, OTReg (Ont), MEd, Division of Plastic and Reconstructive Surgery,Department of Rehabilitation Services, The Hospital for SickChildren, 555 University Avenue, Room 5433, Toronto, ON M5G1X8, Canada; e-mail: <[email protected]>.
0894-1130/$ - see front matter � 2012 Hanley & Belfus, an imprintof Elsevier Inc. All rights reserved.
http://dx.doi.org/10.1016/j.jht.2012.05.002
406 JOURNAL OF HAND THERAPY
ABSTRACT:Purpose: The purpose of this article was to report the develop-
ment of a new assessment tool, the Brachial Plexus Outcome Mea-sure (BPOM) and the evaluation of its internal consistency andconstruct validity.
Methods: A retrospective case series of children aged 4e19years with obstetrical brachial plexus palsy (OBPP) was conduct-ed. Intraclass coefficients were calculated for the BPOM ActivityScale items. Correlation between the Active Movement Scale(AMS) and BPOM Activity Scale scores were conducted to deter-mine the convergent validity.
Results: The BPOM Activity Scale items (N¼ 306) had good in-ternal consistency (Cronbach’s a¼ 0.87). A strong correlation be-tween the BPOM Activity Scale and AMS (n¼ 284) was found(r¼ 0.71, p¼ 0.001, a¼ 0.05).
Conclusions: The BPOM Activity Scale demonstrates good in-ternal consistency and construct validity as a discriminative func-tional outcome measure in children with OBPP.
Level of Evidence: IV
J HAND THER. 2012;25:406–17.
Obstetrical brachial plexus palsy (OBPP) is a par-tial or total birth injury to the network of nerves thatoriginate from spinal roots C5eC8 and T1. Fullrecovery of neurological function of the upper limbis possible in an infant if recovery is seen within thefirst month after birth.1 Infants with more severe in-juries will have residual deficits, including loss of ac-tive range of motion (AROM) and joint contracturesin their affected upper extremity. Children with up-per plexus injuries will have more impairment prox-imally, whereas the whole limb may be affected inchildren with total plexus injuries.
Children with OBPP may require secondary sur-gical reconstructive procedures to optimize upperlimb joint integrity, position, and active movement.2
Determining candidacy for such procedures is
influenced by many factors. This includes physicalfactors, such as age, joint integrity, joint active move-ment, balance in muscle groups, and strength of mus-cle donors.2 Consideration of the biomechanics of theupper extremity also plays an important role in deter-mining the optimal joint position when dynamicmovement cannot be achieved. For example, surgicalcorrection of supination contractures to position theforearm at neutral or pronation in this populationhas been described.3e8 In a child with a total plexuspalsy, it is important to consider the biomechanicalrelationship between the forearm and the hand to de-termine which of these two end forearm positions op-timizes function. A child with sufficient radialprehension and individual finger movement wouldbenefit from a pronated end position. In the presenceof weak or absent intrinsics, positioning the forearmin fixed pronation does not position the hand opti-mally for tool use or to act as an assisting hand to cra-dle objects. Such a child would use a crude grasp,such as a transpalmar grasp, with its affected handthat would benefit the most with a forearm posi-tioned at neutral.9 In children with OBPP, it is essen-tial that the quality of upper extremity movement ismeasured from a biomechanical framework.

Evaluation of upper extremity function is critical indetermining candidacy and efficacy of these proce-dures as well as measuring rehabilitation outcomes,including remedial, adaptive, and psychosocial in-terventions.12,13 A comprehensive upper extremityfunctional outcome measure that addresses theseissues must be founded on a theoretical frameworkthat recognizes the multifaceted nature of function.The World Health Organization’s InternationalClassification of Function, Disability and Health(ICF)14 categorizes function into three main domains:body functions and structures, activity, and participa-tion. Body functions and structures are physiologicalfunctions of body systems, including psychologicalfunction. Activity is the execution of a task or anaction by an individual. Participation considers func-tion within the context of the child’s unique lifesituation.14
The outcome measures of body functions andstructures with good psychometric properties havebeen established for children with OBPP. The ActiveMovement Scale (AMS) and Mallet shoulder evalu-ation are reliable and clinically useful measures toevaluate the outcomes in this category of function ininfants and children.15e17 These tools are clinicallyuseful in discriminating the AROM deficit in the up-per limb and provide evaluative information regard-ing the natural history of the injury or postoperativeresults if administered repeatedly.12 However, thesemeasures only evaluate one aspect of function.Children with OBPP may have limitations in theirfunction due to poor self-perception, psychosocialadjustment, or influences of their personal or socialenvironment. These children have been shown tohave a lower self-esteem in relation to participationin motor activities compared with their peers.11
Furthermore, psychosocial factors such as satisfac-tion with the appearance of the limb can also influ-ences decision making regarding the electivesurgical and rehabilitative interventions.10
Measures of activity and participation aim to eval-uate the child’s upper extremity performance duringa task and within the context of their unique environ-ment, respectively. The measures used in the presentstudies on children with OBPP include nonstandar-dized activities of daily living (ADLs) questionnaires,nonstandardized bimanual activities, AssistingHandAssessment (AHA), Pediatric Evaluation of Disa-bility Inventory (PEDI), Pediatric Outcomes DataCollection Instrument (PODCI), Ansula (an adapta-tion of a standardized participation model), andsubjective measures of patient satisfaction.11,13,18e20
Among these assessments, the AHA, PEDI, andPODCI have good psychometric properties.21,22
However, these assessments do not provide qualita-tive information regarding activity or participationdeficits specific to the anatomical impairment of thelimb of a child with OBPP that can help determine
potential interventions at each joint level in thispopulation. Furthermore, the AHA requires video-tape analysis that may be challenging in a busy clini-cal setting. The PEDI is also not sensitive enough todetermine the activity limitations in the self-care abi-lities of children with OBPP without hand impair-ment.19 Therefore, a standardized disease-specificactivity and participation outcomemeasure is neededto evaluate upper extremity function in children withOBPP.
The purpose of this article was to report thedevelopment of a new assessment tool, the BrachialPlexus OutcomeMeasure (BPOM) and the evaluationof the BPOMActivity Scale’s internal consistency andconstruct validity.
MATERIALS AND METHODS
Development Process
The development of the new assessment toolentailed four steps: 1) literature review to determinethe joint movement patterns that are essential forevaluation in children with OBPP, 2) item generationfor the BPOM Activity Scale through compilation ofassessment items used by expert therapists, 3) acti-vity analysis of potential test items using the AMS,and 4) test item reduction.
Literature Review
Medline and CINAHL databases were searched forsurgical outcome studies on childrenwith OBPPwithlevel of evidence one to four23 published between1996 and 2006. Functional assessments were classi-fied using the ICF14 and categorized anatomicallyas one or more of the following: shoulder, elbow, fore-arm, or wrist/hand assessment. Radiographic evalu-ations were excluded as a measure of outcome.Assessments with the highest frequency and clinicalusefulness24 were used to determine the essentialmovements for evaluation in this population.
Forty-six studies were reviewed in the literature todetermine the essential components of evaluation.25
The most common and clinically useful measuresused are listed in Table 1 using the ICF model.Eighty-three percent of these measures are both dis-criminative and evaluative, 50% had specificity toOBPP, and 42% were designed for the entire life ofthe child (i.e., infancy to adulthood). Sixty-seven per-cent used clinical observation and 33% used self- orparental report. Quantitative methods of evaluationwere used in all the measures. Thirty-three percentincluded qualitative methods. Half (50%) of the mea-sures have established components of reliability andvalidity.
Synthesis of the literature on outcomes ofADLs26,27 and bimanual activities18,27,28 in children
OctobereDecember 2012 407

TABLE 1. Most Common OBPP Outcome Measures Used
Outcome MeasuresNumber ofStudies
Body function and structures measuresActive/passive range of motion 21Mallet shoulder evaluation 16Medical Research Council 11Active Movement Scale 6Gilbert shoulder 6Raimondi hand 5
Activity and participation measuresActivities of daily living 5Bimanual activities 3Pediatric Evaluation of Disability Inventory 1Pediatric Outcomes Data Collection Instrument 1Adapted Ansula (Satisfaction Scale) 1Subjective measure of satisfaction 1
OBPP¼ obstetrical brachial plexus palsy.
with OBPP, and the standardized measures listed inTable 1 were used to determine the essential move-ments for evaluation. These movements were labeled‘‘primary movers.’’ The parameters of the AMS29
were used to define the upper extremity movementand later conduct the activity analysis of the itemsgenerated. The AMS is a standardized evaluation ofAROM of 15 movements using an eight-point scale(Table 2). It has established psychometric propertiesin this population.29,30 The 15 AMS movements in-clude: shoulder (abduction, adduction, flexion, exter-nal rotation, and internal rotation), elbow (flexionand extension), forearm (pronation and supination),wrist (flexion and extension), finger (flexion and ex-tension), and thumb (flexion and extension).15 Thefollowing active movements were determined to bethe primarymovers: shoulder external rotation, inter-nal rotation, elbow flexion, forearm supination, fore-arm, pronation, wrist extension, finger flexion, andthumb flexion/adduction. This corresponds withthe essential movements required for basic handfunction and the key AROM deficits in childrenwith OBPP.
TABLE 2. Active Movement Scale
Observation Muscle Grade
Gravity eliminatedNo contraction 0Contraction, no motion 1Motion#½ range 2Motion$½ range 3Full motion 4
Against gravityMotion#½ range 5Motion$½ range 6Full motion 7
Request for permission to reprint pending from Clarke HM andCurtis CG.32
408 JOURNAL OF HAND THERAPY
Item Generation
The BPOM Activity Scale tasks were generatedfrom a retrospective review of the assessment proto-cols and forms used by the six expert therapists at theBrachial Plexus Clinic at the authors’ institution. Thisclinic is a world-leading Brachial Plexus Clinic thatevaluates 60e70 new infants with OBPP annuallyand has seenmore than 1,400 children over the last 20years. All activities used to evaluate function inchildren with OBPP through direct observation orrelying on child/parent report over a 10-year period(1992e2002) were reviewed. A list of 65 potentialtest items was generated. Activity analysis was con-ducted by the first author to determine the keymovement patterns targeted by each test item.
Each activity was divided into components usingthe 15 AMS movements. Table 3 is an illustration ofthematrix used for the activity analysis. The activitiesthat evaluated the same AMS movements weregrouped together into a common movement group.For example, three movement groups are shown inTable 3. Both the activity items, ‘‘combs back ofhead’’ and ‘‘ties ponytail’’ require the use of thesame upper extremity movements and therefore cat-egorized as the samemovement group.Next, each ac-tivity on the item generation list was assigned amaximum of three primary movers.
Item Selection and Reduction
The list of activities was then reviewed for redun-dant items. Items in the same movement group withthe same primary movers were ranked according totheir feasibility in the clinical setting as well asapplicability across gender and age (3e19 yr). Themost clinically useful activity items that measure thesame movements were chosen. The list was reducedto 31 items as a result of this refining process. Theseitemswere then trialed clinically by the first author inthe Brachial Plexus Clinic for six months. During thisperiod, the authors received feedback and reflectionregarding the clinical usefulness and administrationof the activity items from the interprofessional teamat the clinic. After this process, the items of the BPOMActivity Scale were reduced to 11 activities throughconsensus from the expert opinion of the authors.The authors had a combined experience of 50 years inthe assessment and treatment of children with OBPPat the time of review.
The Functional Movement Scale was developed bythe authors to grade the child’s upper extremityfunction in performing the tasks of the BPOMActivity Scale. This scale was defined by: 1) theability to complete the task and 2) the quality anddegree of compensatory movements observed in theaffected upper extremity during the task. TheFunctional Movement Scale is an ordinal scale from
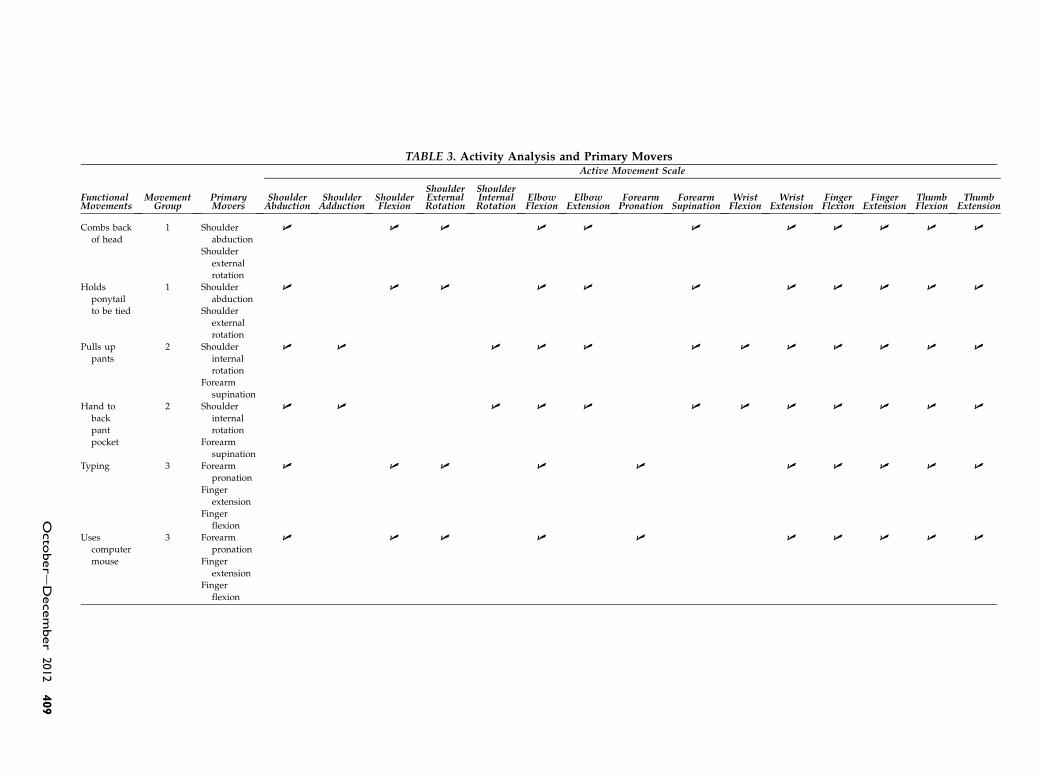
TABLE 3. Activity Analysis and Primary Movers
FunctionalMovements
MovementGroup
PrimaryMovers
Active Movement Scale
ShoulderAbduction
ShoulderAdduction
ShoulderFlexion
ShoulderExternalRotation
ShoulderInternalRotation
ElbowFlexion
ElbowExtension
ForearmPronation
ForearmSupinatio
WristFlexion
WristExtension
FingerFlexion
FingerExtension
ThumbFlexion
ThumbExtension
Combs back
of head
1 Shoulder
abduction
U U U U U U U U U U U
Shoulder
external
rotation
Holds
ponytail
to be tied
1 Shoulder
abduction
U U U U U U U U U U U
Shoulder
external
rotation
Pulls up
pants
2 Shoulder
internal
rotation
U U U U U U U U U U U U
Forearm
supination
Hand to
back
pant
2 Shoulder
internal
rotation
U U U U U U U U U U U U
Forearm
supination
Typing 3 Forearm
pronation
U U U U U U U U U U
Finger
extension
Finger
flexion
Uses
computer
mouse
3 Forearm
pronation
U U U U U U U U U U
Finger
extension
Finger
flexion
Octo
bere
December
2012409
n

one to five. A lower score represents a greater activitylimitation. A child who cannot complete the BPOMActivity item is given a score of one. A score of five isgiven to a child who is able to complete the BPOMActivity item using a normal movement pattern thatis symmetrical to their unaffected upper extremity. Indeveloping the scale, there was a specific challenge ofdefining the difference between minor and majorcompensatory movements that are observed betweengrades 3 and 4 in the scale. Absent active movementin primarymover(s) as defined in the development ofthe tool was used to distinguish the quality ofmovement used to complete the task. At the end ofa trial period of several months, consensus on thedefinition for each level of the Functional MovementScale was made by the authors.
Standardized guidelines for evaluation of eachBPOM activity item were developed. Concurrentadministration of the scale was then tested by ad-ministration of the BPOM Activity Scale by one oftwo student occupational therapists and the firstauthor in the clinic over a four-week period todetermine the preliminary interrater reliability andwhether revisions to the guidelines were required.Consistent administration was achieved at the end ofthe trial period with someminor revisions to the scaleguidelines. A description of the qualifying criteria foreach level of the five-point ordinal scale is providedin the BPOM Activity Scale tool manual.
BPOM Self-evaluation Scale
The BPOM Self-evaluation Scale was developed asan adjunct to the Activity Scale. Historically, severaloutcome measures have been used to capture thechild and family’s functional goals within the contextof their unique life situation. This was an attempt toincorporate a measure of ICF participation into theprotocol for evaluating function. The CanadianOccupational Performance Measure (COPM),31 pre-viously used as a standard measure, was modifiedto improve application and efficiency. The child orparent was asked to identify any functional problemsin ADLs, school, or leisure activities. The perfor-mance and satisfaction of performance on each prob-lem listed was rated on an ordinal scale from one tofour. What transcribed from this assessment wasthe consensus from the expert therapists in the clinicis that a standardized measurement of satisfactionwith upper extremity function was clinically useful.It provided the critical information to help identifywhen psychosocial factors were negatively impactingthe child’s overall function.
After a trial period of using the adapted COPM bytwo expert occupational therapists, the BPOM Self-evaluation Scale was developed. The aim of thisscale is to provide a routine and standardized mea-sure to determine the child’s perception of their arm
410 JOURNAL OF HAND THERAPY
function and appearance. The initial evaluation con-sisted of two visual analog scales that quantified thechild’s satisfaction with their upper extremity func-tional performance and appearance. After a trialperiod, three visual analog scales were developedto measure hand and arm function as well as upperextremity appearance to measure the distinctionbetween upper and total plexus palsy in children.The language used on the scale and for administra-tion was revised and reviewed to ensure comprehen-sion from school-aged children. At the end of the trialperiod, the authors achieved consensus in the devel-opment of three visual analog scales and determinedthat the scale is most reliable for children older than 7years. The BPOM Self-evaluation Scale consists ofthree (100 mm) visual analog scales to evaluate theperceived function of the arm and hand, and the cos-metic appearance of the limb of children (Figure 1).
The BPOM Self-evaluation scale measures a com-ponent of the ICF definition of participation as itconsiders the child’s upper extremity performancewithin their unique life context. The authors wouldnot classify the BPOM Self-evaluation scale as astand-alone measure of participation. Despite theneed for both a standardized activity and participa-tion measure in the literature, the authors feel that itis more important to use an efficient and clinicallyuseful tool in a busy clinic. Clinicians are recom-mended to supplement the BPOM Activity Scale andSelf-evaluation Scale with a global standardized par-ticipation questionnaire when needed. The psycho-metrics of the BPOM Self-evaluation scale is notevaluated in this article.
Construct Validity
The authors’ institution’s research ethics boardapproved the study. A retrospective case series re-search design was used to conduct this study. TheBrachial Plexus Database at the authors’ institutionwas reviewed to find all the brachial plexus clinicvisits in which the AMS and BPOMwere successfullyadministered to children aged 4e19 years betweenApril 1, 2006 and April 1, 2010. The BPOM wasadministered by one therapist or by a student occu-pational therapist under direct supervision of thistherapist during this time period to minimize mea-surement error. Evaluation of the correlation betweenthe AMS and BPOM Activity Scale was performed toexamine the convergent construct validity of theBPOM Activity Scale.
The AMS was used to divide the cohort into twogroups according to the severity of their condition:childrenwithout hand impairment and children withhand impairment (i.e., upper plexus and total plexuspalsy, respectively). Children with hand impairmentare defined as an AMS performance of less than sixon any of the following movements—wrist flexion,
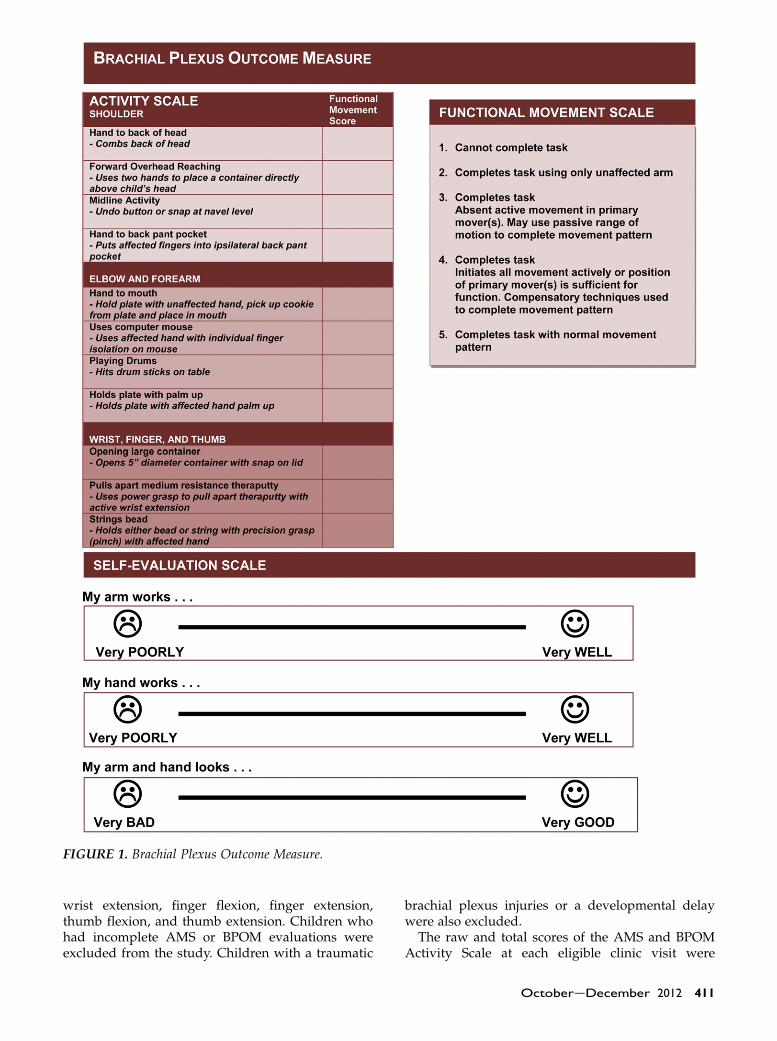
FIGURE 1. Brachial Plexus Outcome Measure.
wrist extension, finger flexion, finger extension,thumb flexion, and thumb extension. Children whohad incomplete AMS or BPOM evaluations wereexcluded from the study. Children with a traumatic
brachial plexus injuries or a developmental delaywere also excluded.
The raw and total scores of the AMS and BPOMActivity Scale at each eligible clinic visit were
OctobereDecember 2012 411

TABLE 4. Demographics
Characteristics Measured (N¼ 306) n (%) or %
Age range (yr)4e6 98 (32)7e9 87 (29)10e12 65 (21)13e15 38 (12)16e18 18 (6)
GenderMale 41Female 59
Affected limbRight 55Left 45
Type of brachial plexus injury (n¼ 284)
collected in a spreadsheet in a password-protected,encrypted document. The total scores of the AMS andBPOM Activity Scale were calculated as the sum ofthe individual scores of the 15 AMS movements andthe 11 BPOM Activity items evaluated per patient,respectively.
Cronbach’s alpha was used to evaluate the internalconsistency of the BPOM Activity Scale. Spearman’scorrelation of the total scores of the BPOM ActivityScale and AMS was conducted using SPSS 17.0statistics software (SPSS Inc., Chicago, IL).33 A nor-mative distribution was determined for the BPOMActivity Scale. Student’s t-tests were used to comparethe BPOM Activity Scale performance among chil-dren with differing severity of brachial plexus palsy.
Upper 60Total 40
Primary microsurgical reconstruction 54
Primary and secondary reconstruction 25
Secondary reconstruction only 7
Operative information unavailable 7
TABLE 5. Internal Consistency: Item-Total Correlation
Activity Items
CorrectedItem-TotalCorrelation
Cronbach’sAlpha if Item
Deleted
Hand to back of head 0.48 0.86Forward reaching 0.49 0.86Midline activity 0.60 0.85Hand to back pocket 0.37 0.87Hand to mouth 0.42 0.87Operates computer mouse 0.72 0.84Plays drums 0.71 0.85Holds plate on palm 0.45 0.86Opens large container 0.78 0.84Pulls apart theraputty 0.57 0.86Strings bead 0.72 0.85
RESULTS
The BPOM is a disease-specific activity assessmentthat was developed through the Brachial PlexusClinic at the authors’ institution (Figure 1). It evalu-ates the quality of upper extremity movement tocomplete 11 activities that measure the key deficientfunctional movement patterns in brachial plexuspalsy. The performances on these items are gradedusing a five-point ordinal scale according to the abil-ity to complete the task and the quality of movementpattern executed.
Three hundred six (N¼ 306) patients were admin-istered the BPOM between April 1, 2006 and April 1,2010. The age range of the patients evaluated wasbetween 4 and 18 years (mean¼ 8.9 yr). The de-mographics of this population are illustrated inTable 4. There were slightly more right affected(n¼ 169) brachial plexus palsy and girls (n¼ 181)represented in this sample. One hundred sixty-four(n¼ 164) patients had microsurgical reconstructionof the brachial plexus in infancy. Of these patients,76 also had secondary reconstructive proceduresthat included surgical procedures on the shoulder, el-bow, forearm, wrist, and the hand. An additional 21patients only had a secondary procedure and didnot have surgery on the nerves of their brachialplexus. Lastly, the operative information was incom-plete for 22 patients in the cohort studied. These pa-tients were referred to the authors’ Brachial PlexusClinic from an external facility after infancy andhad incomplete records.
Using the cohort of 306 patients, the BPOMActivity Scale items demonstrated internal consis-tency reliability of Cronbach’s alpha of 0.87. Item-to-total correlation is shown in Table 5. This measureshow well the BPOM Activity Scale items relate toeach other. All items achieved moderate correlationwith the exception of ‘‘hand to back of pocket.’’
Only 284 patients had both the AMS and BPOMscales administered on the same day. The AMS was
412 JOURNAL OF HAND THERAPY
used to determine children with upper versus totalplexus palsy. Children with impaired AROM onthe AMS in the wrist, fingers, and thumb wereclassified as having a total plexus palsy. Most ofthese children (n¼ 168) had had upper plexus palsy.The BPOMActivity Scale and the AMS demonstrateda strong correlation (Spearman’s rho r¼ 0.71,p¼ 0.001, a¼ 0.05). Comparison of BPOM ActivityScale outcomes according to the severity of injuryfound that the childrenwith upper plexus palsy faredsignificantly better than the childrenwith total plexuspalsy on the BPOM Activity Scale (t-test, p¼ 0.001,a¼ 0.05).
DISCUSSION
The BPOM is a newly developed, disease-specific,functional upper extremity assessment for children
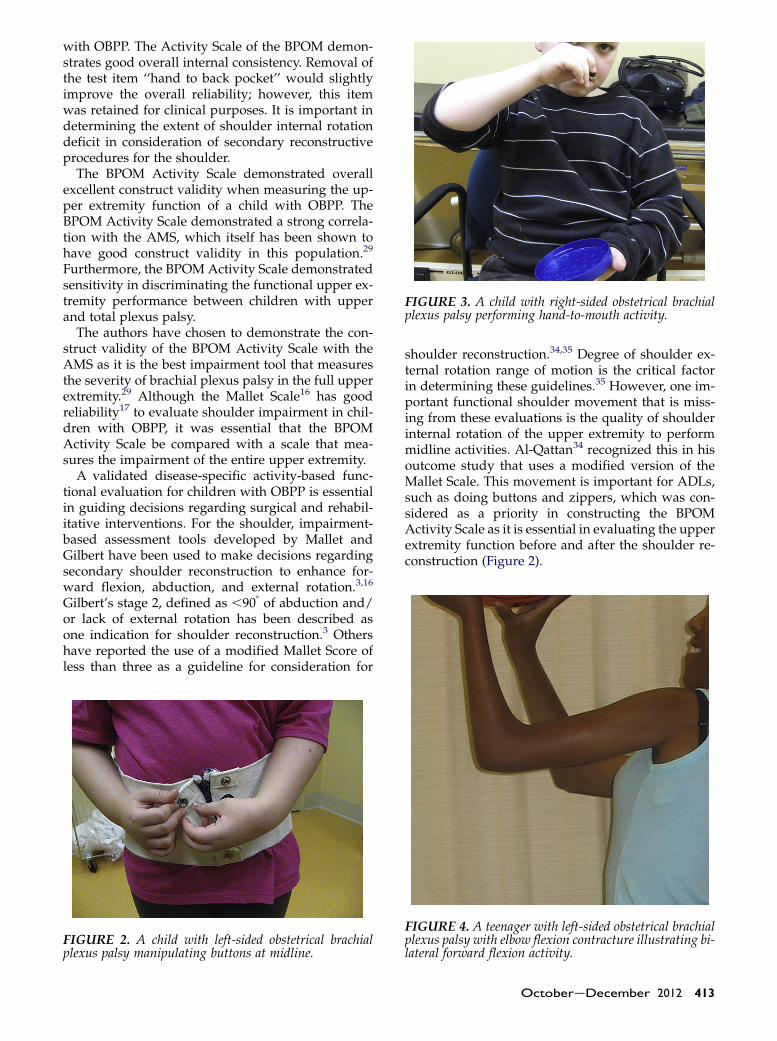
FIGURE 3. A child with right-sided obstetrical brachialplexus palsy performing hand-to-mouth activity.
with OBPP. The Activity Scale of the BPOM demon-strates good overall internal consistency. Removal ofthe test item ‘‘hand to back pocket’’ would slightlyimprove the overall reliability; however, this itemwas retained for clinical purposes. It is important indetermining the extent of shoulder internal rotationdeficit in consideration of secondary reconstructiveprocedures for the shoulder.
The BPOM Activity Scale demonstrated overallexcellent construct validity when measuring the up-per extremity function of a child with OBPP. TheBPOM Activity Scale demonstrated a strong correla-tion with the AMS, which itself has been shown tohave good construct validity in this population.29
Furthermore, the BPOM Activity Scale demonstratedsensitivity in discriminating the functional upper ex-tremity performance between children with upperand total plexus palsy.
The authors have chosen to demonstrate the con-struct validity of the BPOM Activity Scale with theAMS as it is the best impairment tool that measuresthe severity of brachial plexus palsy in the full upperextremity.29 Although the Mallet Scale16 has goodreliability17 to evaluate shoulder impairment in chil-dren with OBPP, it was essential that the BPOMActivity Scale be compared with a scale that mea-sures the impairment of the entire upper extremity.
A validated disease-specific activity-based func-tional evaluation for children with OBPP is essentialin guiding decisions regarding surgical and rehabil-itative interventions. For the shoulder, impairment-based assessment tools developed by Mallet andGilbert have been used to make decisions regardingsecondary shoulder reconstruction to enhance for-ward flexion, abduction, and external rotation.3,16
Gilbert’s stage 2, defined as ,908 of abduction and/or lack of external rotation has been described asone indication for shoulder reconstruction.3 Othershave reported the use of a modified Mallet Score ofless than three as a guideline for consideration for
FIGURE 2. A child with left-sided obstetrical brachialplexus palsy manipulating buttons at midline.
shoulder reconstruction.34,35 Degree of shoulder ex-ternal rotation range of motion is the critical factorin determining these guidelines.35 However, one im-portant functional shoulder movement that is miss-ing from these evaluations is the quality of shoulderinternal rotation of the upper extremity to performmidline activities. Al-Qattan34 recognized this in hisoutcome study that uses a modified version of theMallet Scale. This movement is important for ADLs,such as doing buttons and zippers, which was con-sidered as a priority in constructing the BPOMActivity Scale as it is essential in evaluating the upperextremity function before and after the shoulder re-construction (Figure 2).
FIGURE 4. A teenager with left-sided obstetrical brachialplexus palsy with elbow flexion contracture illustrating bi-lateral forward flexion activity.
OctobereDecember 2012 413

FIGURE 5. Forearm activity evaluation. (A) Child with left-sided obstetrical brachial plexus palsy demonstrating neutralforearm position and transpalmar grasp on drumsticks while playing the drums. (B) Same child demonstrating ability toposition forearm at 458 of pronation to click the mouse with left hand.
FIGURE 6. (A) A child with total plexus palsy with supi-nation contracture. (B) The same child demonstrating iso-lated finger movement when evaluated with BrachialPlexus Outcome Measure activity item ‘‘uses computermouse.’’
Functional evaluation of the elbow in children withOBPP should be conducted in consideration of thetypical shoulder external rotation deficit and elbowflexion contracture in this population. A trumpetsign, which was described by Mallet as the resultantabduction of the shoulder during recruitment ofelbow flexion in the presence of weak shoulderexternal rotation, impacts both the movement andappearance of the limb16 (Figure 3). Elbow flexioncontractures greater than 308 may cause a limb lengthdiscrepancy that impacts bilateral activities thatrequire the child to hold both the arms out-stretched5,10,36 (Figure 4). The BPOM Activity Scaleitems ‘‘hand to back of head’’ and ‘‘forward reach-ing’’ provides this qualitative evaluation of elbowfunction.
Evaluation guidelines specific to forearm functionin OBPP has not been clearly documented.6,37,38 Asillustrated in the introduction of this article, it mustbe emphasized that the determination of the endposition after forearm reconstruction is unique toeach child and their respective hand function.Biomechanically, Strickland9 states that the optimalposition for function is the forearm midway betweenpronation and supination, the wrist dorsiflexed, andthe digits in moderate flexion. This is an ideal posi-tion when a child only has a sufficient hand functionto produce a power grasp in the hand. Boehme39 ar-gues that the most functional position of the forearmis approximately 458 of pronation, as used seen whenwriting. This is an ideal position when a child has ad-equate dexterity in the radial digits for manipulationat tabletop activities. It is with these biomechanicalconsiderations that the BPOM Activity Scale itemsthat evaluate the forearm position, including ‘‘play-ing drums’’ and ‘‘uses computer mouse’’ measured(Figures 5A and 5B). Although, a child with brachialplexus palsy would not typically manipulate a com-puter mouse with its affected limb, this activity is
414 JOURNAL OF HAND THERAPY
designed to assess whether the child has sufficient ra-dial prehension or individual finger movement toconsider reconstruction of the forearm in the pres-ence of a supination contracture (Figures 6A and 6B).

FIGURE 7. Fine motor activity. (A) Gross grasp function.Child demonstrating ability to sufficiently abduct the leftaffected thumb around large objects. (B) Fine grasp func-tion. Child demonstrating fine pincer grasp with the af-fected right hand.
Tendon transfers for wrist extension may berecommended for children with OBPP with wristdrop.40,41 Evaluation of wrist extension is a priority inthis population. Children with hand impairment arepoor candidates for secondary reconstruction of thehand due to lack of appropriate donors and severityof impairment.2 Evaluation of primary movements inthe hand of children with OBPP should include thebasic components of evaluation of hand function inchildren: power grasp, precision grasp, and grossgrasp abilities42 (Figures 7A and 7B). This informa-tion is valuable to the therapist working with a childwith total plexus palsy in providing accommodationsand adaptations for hand function.
The BPOM has demonstrated clinical usefulnessand emerging evaluative properties at the authors’Brachial Plexus Clinic. It has been adopted by severalother clinics outside of the authors’ institution.However, the limitations of the BPOM Activity andSelf-evaluation Scale are that the development of thescale did not undergo the conventional formalizedprocess of item generation and reduction. The use offocus groups or an expert panel that included a
family or child with brachial plexus palsy wouldhave been valuable in the development of the tool.The authors also recognize that it is critical that theBPOM undergo further psychometric evaluation,including the interrater and testeretest reliability.The next step clinically is to also evaluate the tool todetermine the evaluative validity in measuringchanges in upper extremity performance pre- andpostsurgical or rehabilitative interventions. Theseinvestigations are underway and will be presentedin future papers.
The BPOM Activity Scale has good internal con-sistency and construct validity as a discriminativefunctional outcome measure in children with OBPP.The strength of this BPOM Activity Scale is its abilityto discriminate the quality of function of the completeupper extremity in this population. It has high clin-ical utility due to its quick and easy administration,easy-scoring ability, portability, and low cost. This isideal for a busy outpatient clinical setting. This studypresents data to support the clinical use of this tool toevaluate the activity function of children with OBPP.It is best used as an adjunct to an impairmentoutcome measure, such as the AMS, to provide amore comprehensive view of the child’s function.
REFERENCES
1. Waters PM. Comparison of the natural history, the outcome ofmicrosurgical repair, and the outcome of operative reconstruc-tion in brachial plexus birth palsy. J Bone Joint Surg Am. 1999;81:649–59.
2. Waters PM. Update on management of pediatric brachialplexus palsy. J Pediatr Orthop. 2005;25:116–26.
3. Duclos L, Gilbert A. Obstetrical palsy: early treatment and sec-ondary procedures. Ann Acad Med Singapore. 1995;24:841–5.
4. Gilbert A. Obstetrical brachial plexus palsy. In: Tubiana R (ed).The Hand. Philadelphia, PA:WB Saunders Company, 1993. pp.575–601.
5. Price A, Tidwell M, Grossman JAI. Improving shoulder and el-bow function in children with Erb’s palsy. Semin Pediatr Neu-rol. 2000;7:44–51.
6. Price AE. A management approach for secondary shoulderand forearm deformities following obstetrical brachial plexusinjury. Hand Clin. 1995;11:607–17.
7. WangAA, Jacobson-Petrov J, Stubin-Amelio L, Athanasian EA.Selection of fusion position during forearm arthrodesis. J HandSurg Am. 2000;25:842–8.
8. Wang AA, Hutchinson DT, Coleman DA. One-bone forearmfusion for pediatric supination contracture due to neurologicdeficit. J Hand Surg Am. 2001;26:611–6.
9. Strickland JW. Anatomy and kinesiology of the hand. In:Henderson A, Pehoski C (eds). Hand Function in the Child:Foundations for Remediation. St. Louis, MO: Mosby Inc.,2006. pp. 21–44.
10. Ho ES, Roy T, Stephens D, Clarke HM. Serial casting andsplinting of elbow contractures in children with obstetricbrachial plexus palsy. J Hand Surg Am. 2010;35:84–91.
11. Strombeck C, Fernell E. Aspects of activities and participationin daily life related to body structure and function in adoles-cents with obstetrical brachial plexus palsy: a descriptivefollow-up study. Acta Paediatr. 2003;92:740–6.
12. Marcus JR, Clarke HM. Management of obstetrical brachialplexus palsy evaluation, prognosis, and primary surgical treat-ment. Clin Plast Surg. 2003;30:289–306.
OctobereDecember 2012 415
13. Huffman GR, Bagley AM, James MA, Lerman JA, Rab G. As-sessment of children with brachial plexus birth palsy usingthe Pediatric Outcomes Data Collection Instrument. J PediatrOrthop. 2005;25:400–4.
14. World Health Organization. International Classification ofFunctioning, Disability, and Health (ICF). Geneva, Switzer-land: World Health Organization, 2001.
15. Curtis C, Stephens D, Clarke HM, Andrews D. The activemovement scale: an evaluative tool for infants with obstetricalbrachial plexus palsy. J Hand Surg Am. 2002;27:470–8.
16. Mallet J. Obstetrical paralysis of the brachial plexus. Etiopatho-genesis [French]. Rev Chir Orthop Reparatrice Appar Mot.1972;58(Suppl 1):119–23.
17. Bae DS, Waters PM, Zurakowski D. Reliability of three classifi-cation systems measuring active motion in brachial plexusbirth palsy. J Bone Joint Surg Am. 2003;85-A:1733–8.
18. Strombeck C, Krumlinde-Sundholm L, Forssberg H. Func-tional outcome at 5 years in children with obstetrical brachialplexus palsy with and without microsurgical reconstruction.Dev Med Child Neurol. 2000;42:148–57.
19. Ho ES, Curtis CG, Clarke HM. Pediatric Evaluation of Disabil-ity Inventory: its application to children with obstetric brachialplexus palsy. J Hand Surg Am. 2006;31:197–202.
20. Krumlinde-Sundholm L, Eliasson A. Development of the As-sisting Hand Assessment: a rasch-built measure intended forchildren with unilateral upper limb impairments. Scand J Oc-cup Ther. 2003;10:16–26.
21. Reid DT, Bochen K, Wright V. Critique of the Pediatric Evalu-ation of Disability Inventory (PEDI). Phys Occup Ther Pediatr.1993;13:57–87.
22. Pencharz J, Young NL, Owen JL, Wright JG. Comparison ofthree outcomes instruments in children. J Pediatr Orthop.2001;21:425–32.
23. Sackett DL, Strauss SE, Richardson WS, Rosenberg WM, Hay-nes RB. Evidence-Based Medicine: How to Practice and TeachEBM. 2nd ed. Philadelphia, PA: Churchill-Livingstone, 2000.
24. Rudman D, Hannah S. An instrument evaluation framework:description and application to assessments of hand function.J Hand Ther. 1998;11:266–77.
25. Ho ES. Clinical Utility of Functional Assessment in Childrenwith Obsetrical Brachial Plexus Palsy. Triennial Congress ofthe International Federation of Societies for Surgery of theHand (IFSSH). Sydney, Australia: IFSSH, 2007.
26. Hoeksma AF, ter Steeg AM, Nelissen RG, van Ouwerkerk WJ,Lankhorst GJ, de Jong BA. Neurological recovery in obstetricbrachial plexus injuries: an historical cohort study. Dev MedChild Neurol. 2004;46:76–83.
416 JOURNAL OF HAND THERAPY
27. Sundholm LK, Eliasson AC, Forssberg H. Obstetric brachialplexus injuries: assessment protocol and functional outcomeat age 5 years. Dev Med Child Neurol. 1998;40:4–11.
28. Dumont CE, Forin V, Asfazadourian H, Romana C. Function ofthe upper limb after surgery for obstetric brachial plexus palsy.J Bone Joint Surg Br. 2001;83:894–900.
29. Curtis C. The Active Movement Scale: An Evaluative Tool forInfants with Obstetrical Brachial Plexus Palsy. Institute ofMed-ical Sciences. Toronto, Canada: University of Toronto, 2001.
30. Bae DS, Waters PM, Zurakowski D. Correlation of pediatricoutcomes data collection instrument with measures of activemovement in children with brachial plexus birth palsy. J Pe-diatr Orthop. 2008;28:584–92.
31. Law M, Baptiste S, McColl M, Opzoomer A, Polatajko H,Pollock N. The Canadian occupational performance measure:an outcome measure for occupational therapy. Can J OccupTher. 1990;57:82–7.
32. Clarke HM, Curtis CG. An approach to obstetrical brachialplexus injuries. Hand Clin. 1995;11:563–80, discussion 580e1.
33. SPSS. SPSS Statistics. 17.0 ed. Chicago, IL: SPSS Inc., IBM Com-pany, 2010.
34. Al-Qattan MM. Rotation osteotomy of the humerus for Erb’spalsy in children with humeral head deformity. J Hand SurgAm. 2002;27:479–83.
35. Waters PM, Peljovich AE. Shoulder reconstruction in patientswith chronic brachial plexus birth palsy. A case control study.Clin Orthop Relat Res. 1999:144–52.
36. Morrey BF, Askew LJ, Chao EY. A biomechanical study of nor-mal functional elbow motion. J Bone Joint Surg Am. 1981;63:872–7.
37. Bahm J, Gilbert A. Surgical correction of supination deformityin children with obstetric brachial plexus palsy. J Hand Surg Br.2002;27:20–3.
38. Al-QattanMM,Al-Khawashki H. The ‘‘beggar’s’’ hand and the‘‘unshakable’’ hand in children with total obstetric brachialplexus palsy. Plast Reconstr Surg. 2002;109:1947–52.
39. Boehme R. Treatment for Basic Hand Function. Improving Up-per Body Control. Tucson, AZ: Therapy Skill Builders, 1988.pp. 87e118.
40. Duclos L, Gilbert A. Restoration of wrist extension by tendontransfer in cases of obstetrical brachial plexus palsy. AnnChir Main Memb Super. 1999;18:7–12.
41. Al-Qattan MM. Tendon transfer to reconstruct wrist extensionin children with obstetric brachial plexus palsy. J Hand Surg Br.2003;28:153–7.
42. Ho ES. Measuring hand function in the young child. J HandTher. 2010;23:323–8.
JHT Read for CreditQuiz: Article #244
Record your answers on the Return Answer Formfound on the tear-out coupon at the back of thisissue or to complete online and use a credit card,go to JHTReadforCredit.com. There is only onebest answer for each question.
#1. The two properties this study investigated re-garding the BPOM were
a. reliability and validityb. repeatability and predictabilityc. internal consistency and construct validityd. internal validity and construct consistency#2. The subject population was
a. obstetrical brachial plexus palsy patients ages4 to 19b. obstetrical brachial plexus patients ages 2
to 13c. thoracic outlet patients of all agesd. preteen thoracic outlet patients
#3. To determine validity the BPOM was comparedto the
a. BMSb. BPOBc. ABCd. AMS#4. The BPOM is primarily a test of
a. psychological stabilityb. social adjustmentc. functiond. strength and ROM#5. The authors suggest the BPOM unfortunately haslow clinical utility
a. trueb. falseWhen submitting to the HTCC for re-certification,please batch your JHT RFC certificates in groups of 3or more to get full credit.
OctobereDecember 2012 417