Embed Size (px)
Citation preview

British Journal of Dermatology (1994) 131, 270-274.
The cardio-facio-cutaneous syndrome: a manifestation of theNoonan syndrome?
K.A.WARD, C.MOSS AND C.MCKHOWN*Department of Dermatology. The General Hospital Steelhouse Lane, Birmingham B4 6NH, U.K.'Department ofCIinicat Genetics. Birmingham Maternity Hospitat, U.K.
Accepted for publication 30 December 1993
Summary The cardio-facio-cutaneous (CFC) syndrome has several features in common with the Noonansyndrome, but is distinguished by the presence of hyperkeratotic skin lesions, abnormal hair, and alack of familial cases. We describe a family who clearly satisfy the criteria for the CFC syndrome, andshow other features which have been reported in the Noonan syndrome but not in the CFCsyndrome, namely a haemorrhagic diathesis and ocular abnormalities. This supports the conceptthat the CFC syndrome is a manifestation of the Noonan syndrome.
The cardio-facio-cutaneous (CFC) syndrome is a newlyrecognized syndrome characterized by abnormal facies.mental retardation, congenital heart disease, and ecto-dermal abnormalities.^ Although it has many featuresin common with the Noonan syndrome^ it is distin-guished by the presence of abnormal hair and hyper-keratotic skin lesions, and by its sporadicoccurrence.^^" Recently. Fryer et aL. proposed thatthe CFC syndrome fell within the clinical spectrum of
the Noonan phenotype.support this concept.
The cases reported here
Case reports
Case 1
A 42-year-old woman, the third child of healthy,non-consanguineous Caucasian parents, had facialdysmorphism in childhood suggestive of 'mongolism'.In early infancy she developed erythema and follicularhyperkeratosis of the outer half of the eyebrows, andfollicular hyperkeratosis of the extensor surfaces of thearms. After adolescence, the process became stationary,and then gradually improved. Her general developmentwas normal. She had cardiac surgery for valvularpulmonary stenosis when aged 10 years. VonWillebrand's disease was diagnosed at the age of 29.and platelet dysfunction at the age of 42. She had mildphotophobia.
When seen at the age of 42, her height was 164 cm(50th- 75th centile). and head circumference was58-2cm (well above the 97th centile). She had a high.
bi lai' forehead, long face, curly hair, prominent eyeswith proptosis, full lips, and a wide mouth (Fig. 1).There was erythema, follicular hyperkeratosis. andalopecia of the eyebrows and eyelashes. There was nohypertelorism. and her cars and posterior hairline werenormal. She had pectus excavatum. and a midlinesternotomy scar. Her nails were broad and flat, andshowed koilonychia. The cuticles extended an unusualdistance on to the nail plates (Fig. 2). Ophthalmologicalexamination was normal. Her karyotype was normal.
Case 2
The 13-year-old elder daughter of case 1 was deliveredby caesarean section at 37 weeks' gestation because ofbreech presentation. The neonatal period was com-plicated by feeding difficulties, and she required naso-gastric feeding for the first 5 weeks. Thereafter, sheremained a poor feeder; each feed lasted over 1 h. andwas followed by vomiting. Milestones were otherwisenormal. She sat unsupported at 7 months, and walkedat 15 months. She currently attends a normal school. Aheart murmur was noted at 6 months, and diagnosedas mild aortic stenosis. She has no bleeding tendency,and tests for von Wiilebrand's disease and plateletdysfunction have been negative. She complains ofmild photophobia.
When she was 3 months old she developed erythemaand follicular hyperkeratosis affecting the outer eye-brows. The condition progressed throughout childhood,resulting in erythema of the forehead, cheeks and upperlip, and alopecia of the eyebrows and lashes. There was
270
CARDIO-FACIO-CUTANEOUS AND NOONAN'S SYNDROMES 271
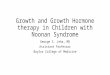
Figure 1. Early photograph of mother (case 1);md elder daughter (case 2). showing sinularfacial features, curly hair, and ulcrythemaophryogenes.
marked follicular hyperkeratosis of the extensor sur-faces of all the limbs.
When examined at 13 years of age, her height was161cm (75th-9Oth centile). and head circumferencewas 56 cm (97th centile). She has a similar facialappearance to her mother, and also has curly hair(Figs 1 and 3). She has pectus carinatum superiorlyand pectus excavatum inferiorly. Her cuticles show thesame abnormality as those of her mother (Fig. 4).Ophthalmological examination revealed prominentcorneal nerves and anterior corneal dystrophy. Karyo-type examination was normal.
Unaffected family members
No other family members had this characteristic facial
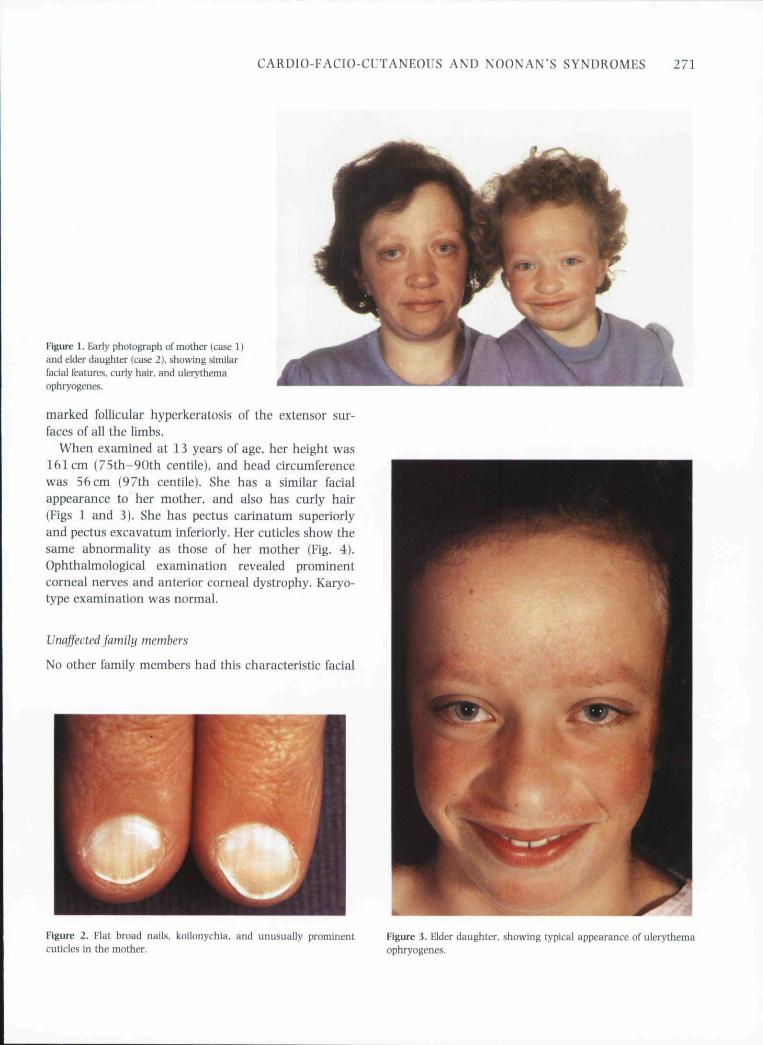
Figure 2. Flat broad nails, koilonychia. and unusually prominentcuticles in the mother.
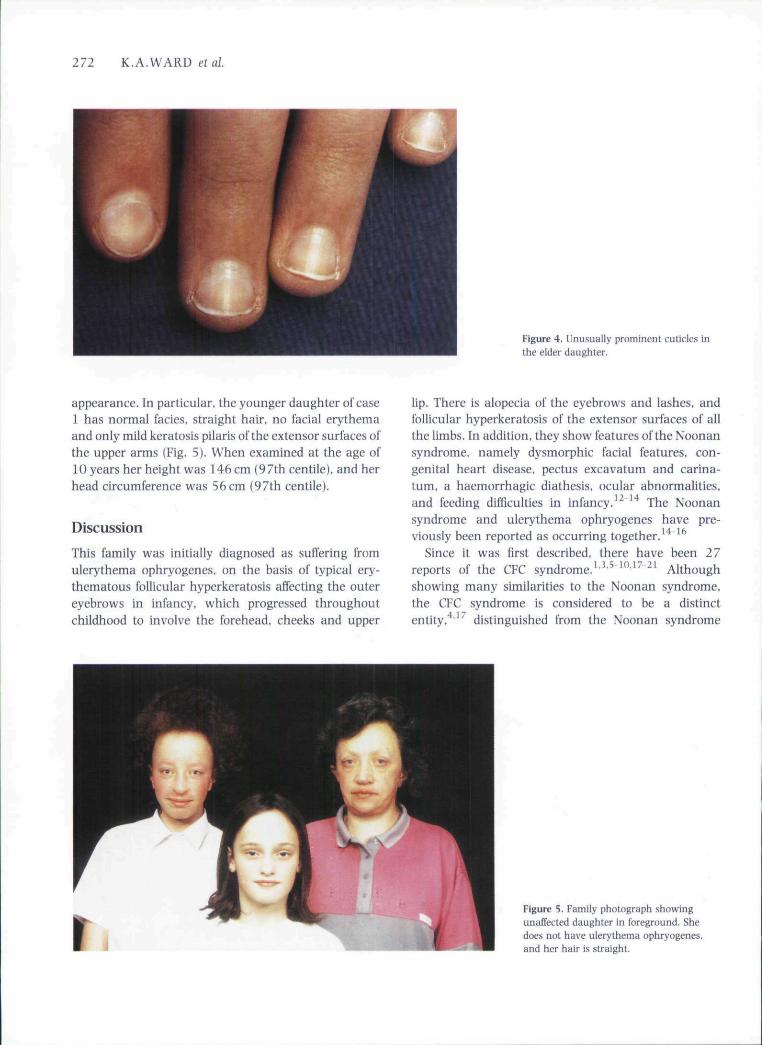
Figure 3. Elder daughter, showing typical appearance of ulcrythemaophryogenes.
272 K.A.WARD etal.
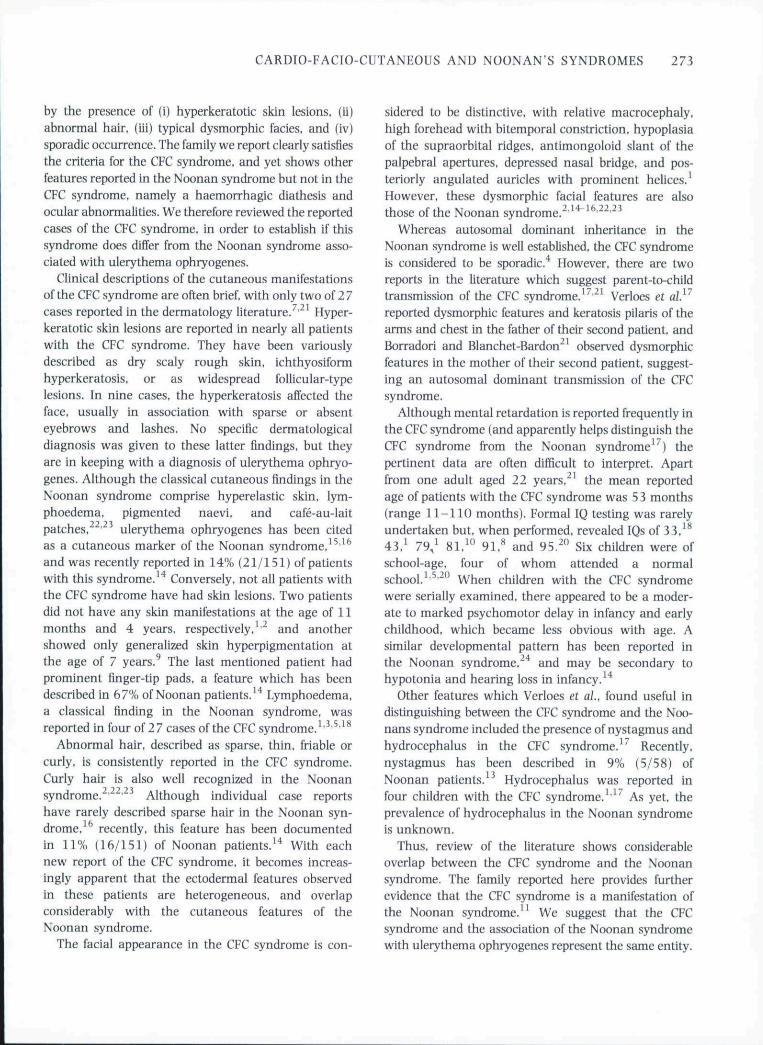
Figure 4. Unusually prominent cuticles inthe elder daugiiter.
appearance. In particular, the younger daughter of case1 has normal facies, straight hair, no facial erythemaand only mild keratosis pilaris ofthe extensor surfaces ofthe upper arms (Fig. 5). When examined at the age of10 years her height was 146 cm (97th centile), and herhead circumference was 56cm (97th centile).
Discussion
This family was initially diagnosed as suffering fromulerythema ophryogenes, on the basis of typical ery-thematous follicular hyperkeratosis affecting the outereyebrows in infancy, which progressed throughoutchildhood to involve the forehead, cheeks and upper
lip. There is alopecia of the eyebrows and lashes, andfollicular hyperkeratosis of the extensor surfaces of allthe limbs. In addition, they show features ofthe Noonansyndrome, namely dysmorphic facial features, con-genital heart disease, pectus excavatum and carina-tum, a haemorrhagic diathesis, ocular abnormalities,and feeding difficulties in infancy. The Noonan
syndrome and ulerythema ophryogenes have pre-viously been reported as occurring together.
Since it was first described, there have been 27reports of the CFC syndrome.^'*'^ '"'^^ ^' Althoughshowing many similarities to the Noonan syndrome,the CFC syndrome is considered to be a distinctentity, distinguished from the Noonan syndrome
Figure 5. Family photograph showingunaffected daughter in foreground. Shedoes not have ulerythema ophryogenes,and her hair is straight.
CARDIO-FACIO-CUTANEOUS AND NOONAN'S SYNDROMES 273
by the presence of (i) hyperkeratotic skin lesions, (ii)abnormal hair, (iii) typical dysmorphic facies. and (iv)sporadic occurrence. The family we report clearly satisfiesthe criteria for the CFC syndrome, and yet shows otherfeatures reported in the Noonan syndrome but not in theCFC syndrome, namely a haemorrhagic diathesis andocular abnormalities. We therefore reviewed the reportedcases of the CFC syndrome, in order to establish if thissyndrome does differ from the Noonan syndrome asso-ciated with ulerythema ophryogenes.
Clinical descriptions of the cutaneous manifestationsof the CFC syndrome are often brief, with only two of 2 7cases reported in the dermatology literature.''^^ Hyper-keratotic skin lesions are reported in nearly all patientswith the CFC syndrome. They have been variouslydescribed as dry scaly rough skin, ichthyosiformhyperkeratosis. or as widespread follicular-typelesions. In nine cases, the hyperkeratosis affected theface, usually in association with sparse or absenteyebrows and lashes. No specific dermatologicaldiagnosis was given to these latter findings, but theyare in keeping with a diagnosis of ulerythema ophryo-genes. Although the classical cutaneous findings in theNoonan syndrome comprise hyperelastic skin, lym-phoedema, pigmented naevi, and cafe-au-laitpatches,^^'^^ ulerythema ophryogenes has been citedas a cutaneous marker ofthe Noonan syndrome. ̂ '̂̂ ^and was recently reported in 14% (21/151) of patientswith this syndrome. Conversely, not all patients withthe CFC syndrome have had skin lesions. Two patientsdid not have any skin manifestations at the age of 11months and 4 years, respectively,^'^ and anothershowed only generalized skin hyperpigmentation atthe age of 7 years.^ The last mentioned patient hadprominent finger-tip pads, a feature which has beendescribed in 67% of Noonan patients.^'* Lymphoedema,a classical finding in the Noonan syndrome, wasreported in four of 27 cases of the CFC syndrome.^'^'^'^^
Abnormal hair, described as sparse, thin, friable orcurly, is consistently reported in the CFC syndrome.Curly hair is also well recognized in the Noonansyndrome.^'^^'^' Although individual case reportshave rarely described sparse hair in the Noonan syn-drome, recently, this feature has been documentedin 11% (16/151) of Noonan patients.^* With eachnew report of the CFC syndrome, it becomes increas-ingly apparent that the ectodermal features observedin these patients are heterogeneous, and overlapconsiderably with the cutaneous features of theNoonan syndrome.
The facial appearance in the CFC syndrome is con-
sidered to be distinctive, with relative macrocephaly.high forehead with bitemporal constriction, hypoplasiaof the supraorbital ridges, antimongoloid slant of thepalpebral apertures, depressed nasal bridge, and pos-teriorly angulated auricles with prominent helices.^However, these dysmorphic facial features are alsothose ofthe Noonan syndrome,^''^"''^^^^
Whereas autosomal dominant inheritance in theNoonan syndrome is well established, the CFC syndromeis considered to be sporadic. However, there are tworeports in the literature which suggest parent-to-childtransmission of the CFC syndrome,^'^'^' Verloes et al}^reported dysmorphic features and keratosis pilaris of thearms and chest in the father of their second patient, andBorradori and Blanchet-Bardon^^ observed dysmorphicfeatures in the mother of their second patient, suggest-ing an autosomal dominant transmission of the CFCsyndrome.
Although mental retardation is reported frequently inthe CFC syndrome (and apparently helps distinguish theCFC syndrome from the Noonan syndrome''') thepertinent data are often difficult to interpret. Apartfrom one adult aged 22 years,^' the mean reportedage of patients with the CFC syndrome was 53 months(range 11-110 months). Formal IQ testing was rarelyundertaken but, when performed, revealed IQs of 33.̂ **43 , ' 7%^ 81,^" 91.^ and 95.^" Six children were ofschool-age, four of whom attended a normalschool.''^'^"^ When children with the CFC syndromewere serially examined, there appeared to be a moder-ate to marked psychomotor delay in infancy and earlychildhood, which became less obvious with age. Asimilar developmental pattern has been reported inthe Noonan syndrome,""* and may be secondary tohypotonia and hearing loss in infancy.'^
Other features which Verloes et al. found useful indistinguishing between the CFC syndrome and the Noo-nans syndrome included the presence of nystagmus andhydrocephaius in the CFC syndrome, ̂ ̂ Recently,nystagmus has been described in 9% (5/58) ofNoonan patients. Hydrocephaius was reported infour children with the CFC syndrome,^^'^ As yet, theprevalence of hydrocephaius in the Noonan syndromeis unknown.
Thus, review of the literature shows considerableoverlap between the CFC syndrome and the Noonansyndrome. The family reported here provides furtherevidence that the CFC syndrome is a manifestation ofthe Noonan syndrome." We suggest that the CFCsyndrome and the association of the Noonan syndromewith ulerythema ophryogenes represent the same entity.

274 K.A.WARD etal
References1 Reynolds IF. Neri G, Herrman JP et al. New multiple congenital
anomalies/mental retardation syndrome with cardio-facio-cutaneous involvement—the CFC syndrome. Am j MedGenet 1986:25:413-27.
2 Noonan JA. Hypertelorism with Turner phenotype. A new syn-drome with associated congenital heart disease. Am ] Dis Child1968: 116: 373-80.
3 Ned G, Sabatino G, Bertini E, Genuardi M. The CFC syndrome-report of the first two cases outside the United States. Am } MedGenet 1987:27: 767-71.
4 Neri G, Zollino M. Reynolds JF. The Noonan-CFC controversy. AmJ Med Genet 1991: 39: 367-70.
5 Sorge G, Di Forti F, Scarano G et al CFC syndrome: report on threeadditional cases. Am ] Med Genet 1989: 33: 476-8.
6 Mucklow ES. A case of ciirdio-facio-cutaneous syndrome. Am jMed Genet 1989: 33:474-5.
7 Pierard GE, Soyer-Broux M, Estrada JA et al Cutaneous presenta-tion of the cardio-facio-cutaneous syndrome. / Am Acad Dermato!1990:22:920-2.
8 Bottani A, Hammerer I, Schinzel A. The cardio-faeio-cutaneoussyndrome: report of a patient and review of the literature. Eur /Pediatr 1991: 150:486-8-
9 Turnpenny PH, IX-an JCS. Auchterlonie IA, Johnston AW. Cardio-faeiocutaneous syndrome with new ectodemiai manifestations./ Med Genet 1992: 29: 428-9.
10 Ghezzi M. Parenti G, de Franchis R et a!. Clinical variability ofcardio-facio-cutaneous syndrome: report of two additional cases.CUnGenet 1992:42: 206-9.
11 Fryer AE, Holt PJ, Hughes HE. The cardio-facio-cutaneous (CFC)syndrome and Noonan syndrome: are they the same.' Am j MedGenet 1991: 38: 548-51.
12 Witt DR, McGillivray BC, Allanscn JK et ai Bleeding diathesis inNoonan syndrome: a eommon association. Am J Med Genet 1988;31: 305-17.
13 Lee NB, Kelly L, Sharland M. Ocular manifestations of Noonansyndrome. Eye 1992: 6: 328-34.
14 Sharland M, Burch M, MeKenna WM, Paton MA. A clinical studyof Noonan syndrome. Arch Dis Child 1992: 67: 178-83.
15 Neild VS, Pegam JS, Wells RS. The association of keratosis pilarisatrophicans and woolly hair, with and without Noonan's syn-drome. BrJDermato! 1984: 110: 357-62.
16 Pierini DO, Pierini AM. Keratosis pilaris atrophicans facici(ulerythema ophryogenes): a cutaneous marker in the Noonansyndrome. BrJDermato! 1979: 100: 409-16.
17 Verloes A, Le Merrer M, Soyeur D et al CFC syndrome: a syndromedistinct from Noonan syndrome. Ann Genet 1988: 31: 230-4.
18 Chrzanowska K, Fryns J-P. Van den Berghe H. Cardio-facio-cutaneous (CFC) syndrome: report of a new patient. Am ] MedGenet 1989: 33:471-3 .
19 Gross-Tsur V, Gross-Kieselstein E, Amir N. Cardio-faeio-cutaneoussyndrome: neurological manifestations, C!in Genet 1990: 38:382-6.
20 Matsuda Y, Murano I, Kondoh 0 et a!, Cardio-facio-cutaneous(CFC) syndrome: report of two patients without hyperkeratoticskin lesions. Am J Med Genet 1991: 39: 144-7.
21 Borradori L, Blanchet-Bardon C. Skin manifestations of cardio-facio-cutaneous syndrome. / Am Acad Dermato! 1993: 28: 8 1 5 -19.
22 Allanson JE. Noonan syndrome. / Med Genet 1987: 24: 9-13.2 3 Wyre HW. Cutaneous manifestations of Noonan's syndrome. Arch
Dermato! 1978; 114: 929-30.24 Money J. Kalus ME. Noonan's syndrome. IQ and specific dis-
abilities. Am J Dis ChUd 1979: 133: 846-50.