Embed Size (px)
Citation preview
The changing face of clinical skills
Paul BradleyDirector of Clinical SkillsPeninsula College of Medicine and Dentistry
ASME ConferenceClinical Skills: Fit for Practice
24th April, 2007RIBA, London
What did it look like before?
The traditional learning of clinical skillsl A basic course in clinical methoduHistoryuPhysical examination
l Rotation through clinical specialitiesuObserveuAbsorbuPractise
l Without observation and feedback

Did it work?l Data from traditional course at University of Liverpool
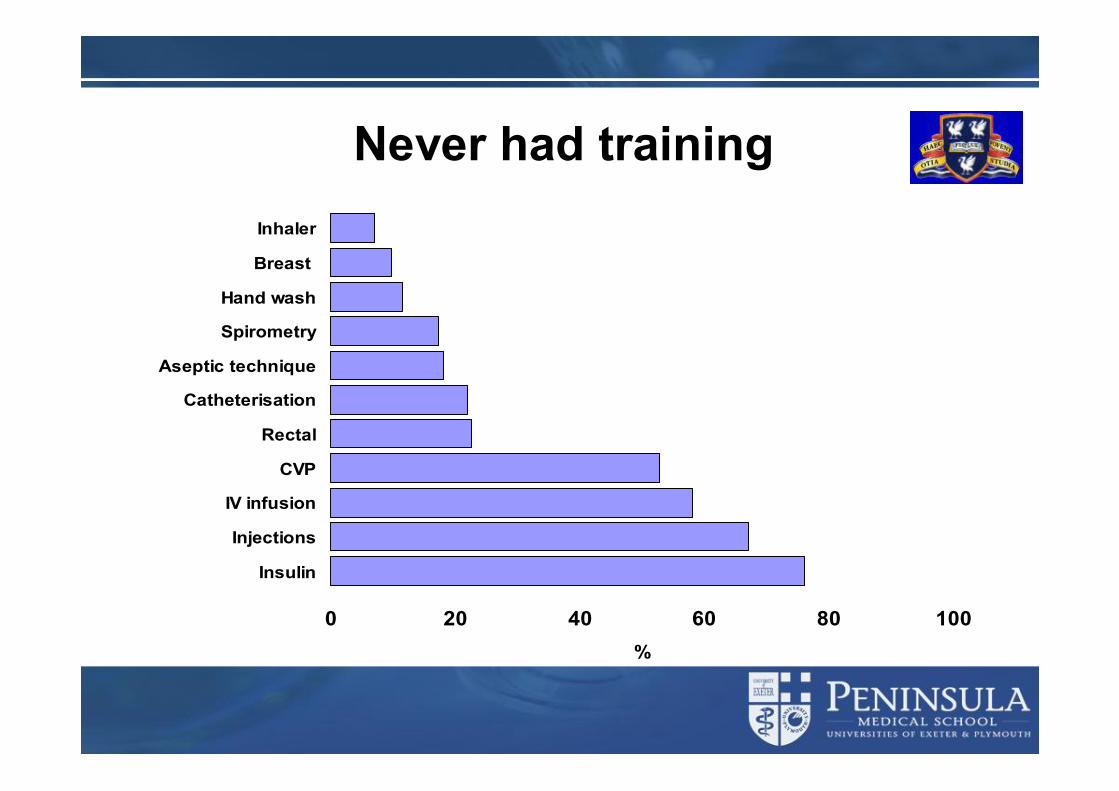
Never had training
0 20 40 60 80 100
Insulin
Injections
IV infusion
CVP
Rectal
Catheterisation
Aseptic technique
Spirometry
Hand wash
Breast
Inhaler
%
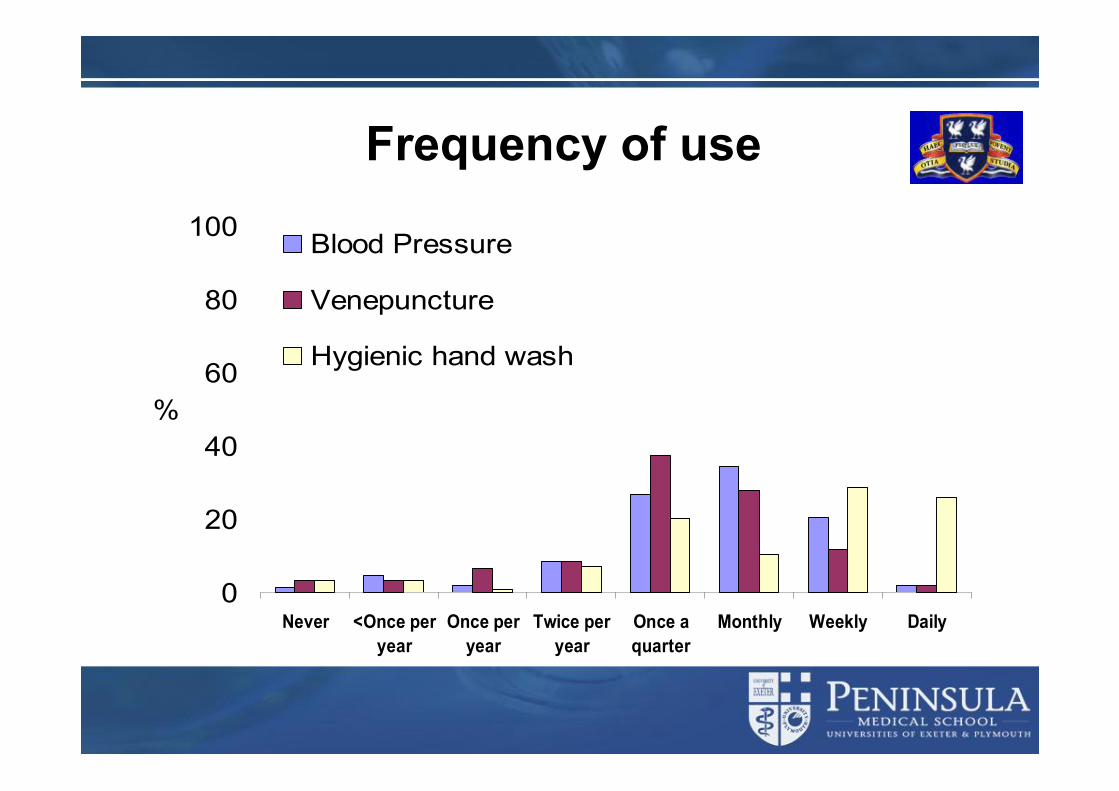
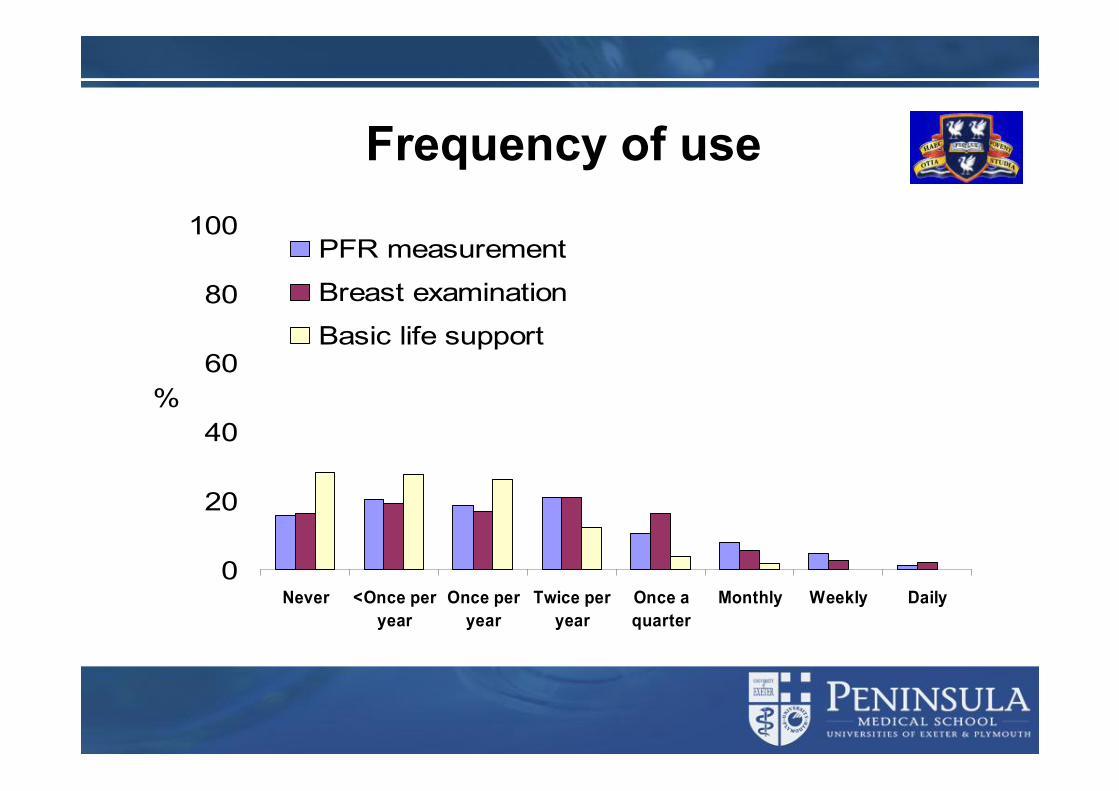
Frequency of use
0
20
40
60
80
100
Never <Once peryear
Once peryear
Twice peryear
Once aquarter
Monthly Weekly Daily
%
Blood Pressure
Venepuncture
Hygienic hand wash
Frequency of use
0
20
40
60
80
100
Never <Once peryear
Once peryear
Twice peryear
Once aquarter
Monthly Weekly Daily
%
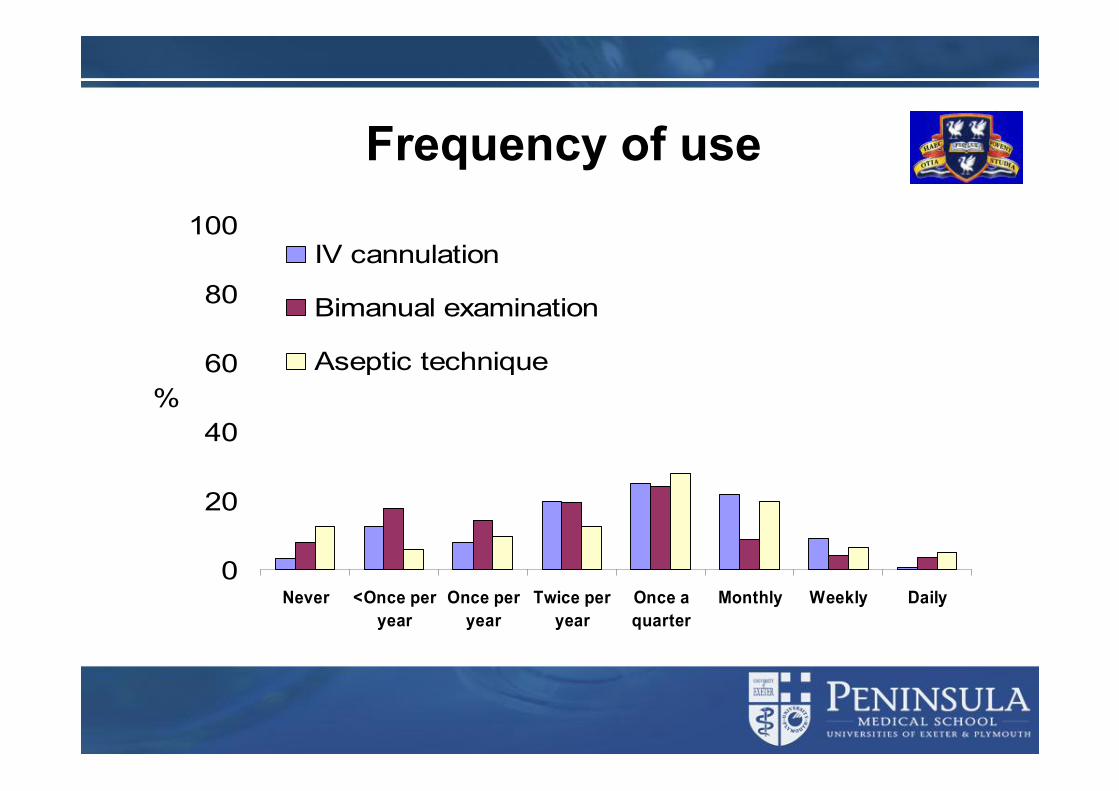
IV cannulation
Bimanual examination
Aseptic technique
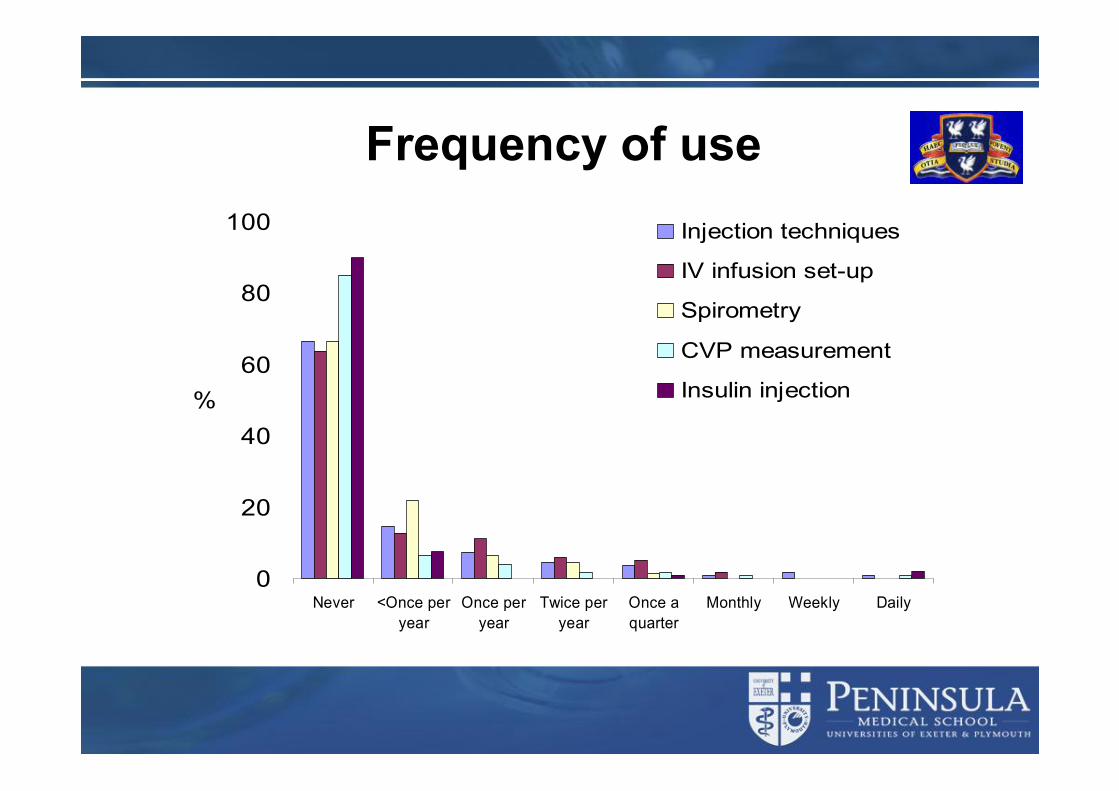
Frequency of use
0
20
40
60
80
100
Never <Once peryear
Once peryear
Twice peryear
Once aquarter
Monthly Weekly Daily
%
PFR measurement
Breast examination
Basic life support
Frequency of use
0
20
40
60
80
100
Never <Once peryear
Once peryear
Twice peryear
Once aquarter
Monthly Weekly Daily
%
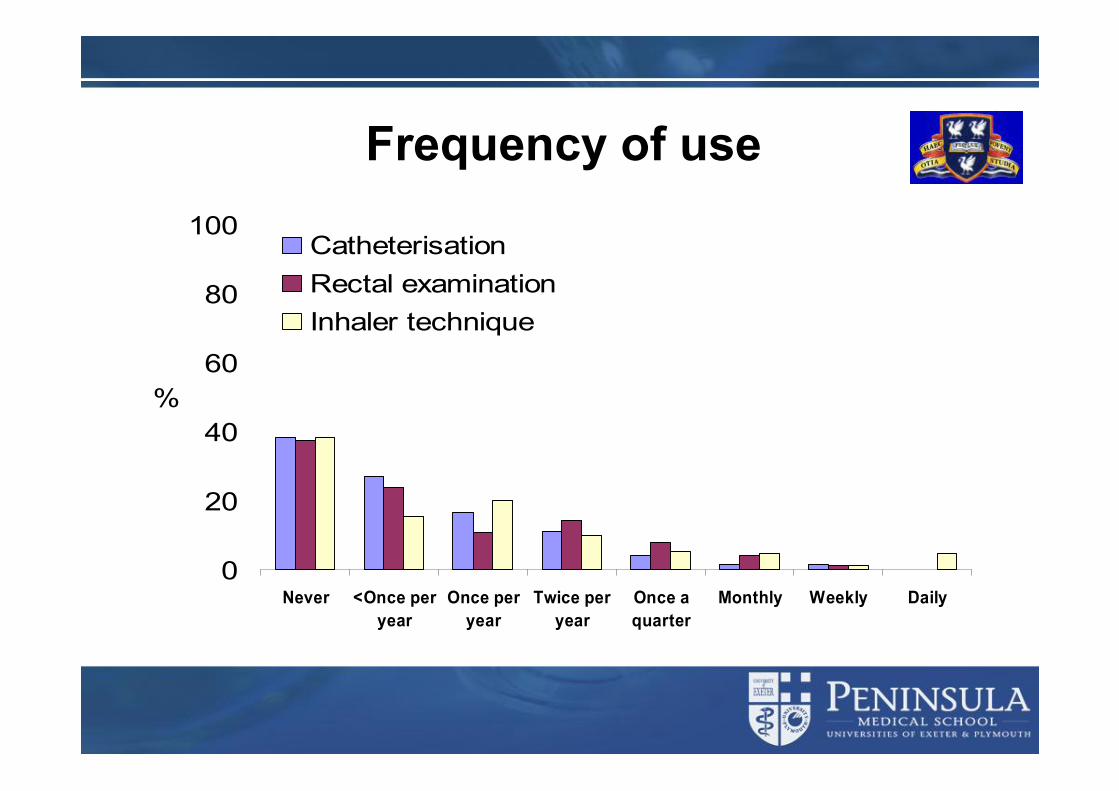
Catheterisation Rectal examination Inhaler technique
Frequency of use
0
20
40
60
80
100
Never <Once peryear
Once peryear
Twice peryear
Once aquarter
Monthly Weekly Daily
%
Injection techniques
IV infusion set-up
Spirometry
CVP measurement
Insulin injection
Blood pressure measurement by junior hospital doctors - a gap in medical education?Feher, M., Harris-St John, K., & Lant, A. (1992). Health Trends, 24(2), 59-61.
And some literature
Cardiopulmonary resuscitation skills of preregistration house officers.Skinner, D. V., Camm, A. J., & Miles, S. (1985). BMJ, 290, 1549-1550.
Senior house officers' work related stressors, psychological distress, and confidence in performing clinical tasks in accident and emergency: a questionnaire study. Williams, S., Dale, J., Glucksman, E., & Wellesley, A. (1997). BMJ, 314, 713-718.
Catheterisation: your urethra in their hands.Carter, R., Aitchison, M., Mufti, G., & Scott, R. (1990). BMJ, 301, 905.
And it isn’t necessarily better yet!
e-mail alert 17th Nov 2006Are Canadian General Internal
Medicine training program graduates well prepared for their
future careers?Card, S. E., Snell, L., & O'Brien, B. D. (2006).
BMC Medical Education, 6(56).
Not just Liverpooll 122 Sheffield students at finals & 84 PRHOsl Of the eight skills studied:uMost performed only a few times by the students u ~50% the current PRHOs could recall any training u There were no significant differences between
teaching hospitals and district general hospitalsu ~2/3rd of PRHOs no recall any training (undergrad
or postgrad about needlestick injury)
Goodfellow, P. B., & Claydon, P. (2001). Students sitting medical finals - ready to be house officers? J R Soc Med, 94(10), 516-520.

Or just the North of Englandl 22/40 PRHOs at Chelsea and Westminsterl 17 station OSCEl Failed a mean of 2.4 OSCE stations (SD 1.8, range 1-8). l No correlations between OSCE result and either self- or
educational supervisor ratings. l The supervisor felt unable to give an opinion on PRHO abilities
in 18% of the skills assessed. l PRHOs seem to have deficiencies in basic clinical skills at the
time they enter the medical register. l Neither PRHOs nor consultants identified these deficiencies.
Fox RA, Ingham Clark CL, Scotland AD, Dacre JE. A study of pre-registration house officers' clinical skills. Medical Education 2000;34(12):1007-12.
Not just the UK and not just studentsl Crotty, M., Ahern, M. J., McFarlane, A. C., & Brooks, P. M. (1993).
Clinical rheumatology training of Australian medical students. A national survey of 1991 graduates. Medical Journal of Australia, 158(2), 119-120.
l Taylor, D. M. (1997). Undergraduate procedural skills training in Victoria: is it adequate? Medical Journal of Australia., 166, 1-3.
l Mangione, S., Burdick, W. P., & Peitzman, S. J. (1995). Physical diagnosis skills of physicians in training: a focused assessment. Academic Emergency Medicine., 2(7), 622-629.
l Chalabian, J., Garman, K., Wallace, P., & Dunnington, G. (1996). Clinical breast evaluation skills of house officers and students. Am Surg, 62(10), 840-845.
l Ringsted, C., Schroeder, T. V., Henriksen, J., Ramsing, B., Lyngdorf, P., Jønsson, V., et al. (2001). Medical students' experience in practical skills is far from stakeholders' expectations. Medical Teacher, 23(4), 412-416.
l Singh, V., Khandelwal, R., Bohra, S., Gupta, R., & Gupta, B. S. (2002). Evaluation of communication skills of physicians about asthma. Journal of the Association of Physicians of India., 50, 1266-1269.
Australia
Australia
N America
N America
Denmark
India
What’s changed?
The health care environment
l Primary care led servicel Shorter periods of hospitalisationl Sicker patients in hospitall Increased service demands on clinical
teachersl Consumer orientated society & patient
rights
Failure of traditional “skills acquisition”
l Serendipity fails to deliver effective skills acquisition
l Evidence ofu Inadequate skillsuStress associated with being unskilled
l Declining number of opportunitiesl Emerging standards and core competencies
Medial education reforml Undergraduate curriculum changeuUK - Tomorrow’s Doctor 1 & 2
l Postgraduate traininguNew F1/F2 programsuShorter traininguWorking time directive
l CPD/CMEuReaccreditation and revalidation
Tomorrow’s doctorsl Take and record a patient’s history,
including their family history.l Perform a full physical examination, and
a mental-state examination.l Interpret the findings from the history,
the physical examination, and the mental-state examination.
l Interpret the results of commonly used investigations.
l Make clinical decisions based on the evidence they have gathered.
l Assess a patient’s problems and form plans to investigate and manage these, involving patients in the planning process.
l Work out drug dosage and record the outcome accurately.
l Write safe prescriptions for different types of drugs.
l Carry out the following procedures involving veins.u Venepuncture.u Inserting a cannula into peripheral
veins.u Giving intravenous injections.
l Give intramuscular and subcutaneous injections.
l Carry out arterial blood sampling.l Perform suturing.l Demonstrate competence in
cardiopulmonary resuscitation and advanced life-support skills.
l Carry out basic respiratory function tests.
l Administer oxygen therapy.l Use a nebuliser correctly.l Insert a nasogastric tube.l Perform bladder catheterisation.
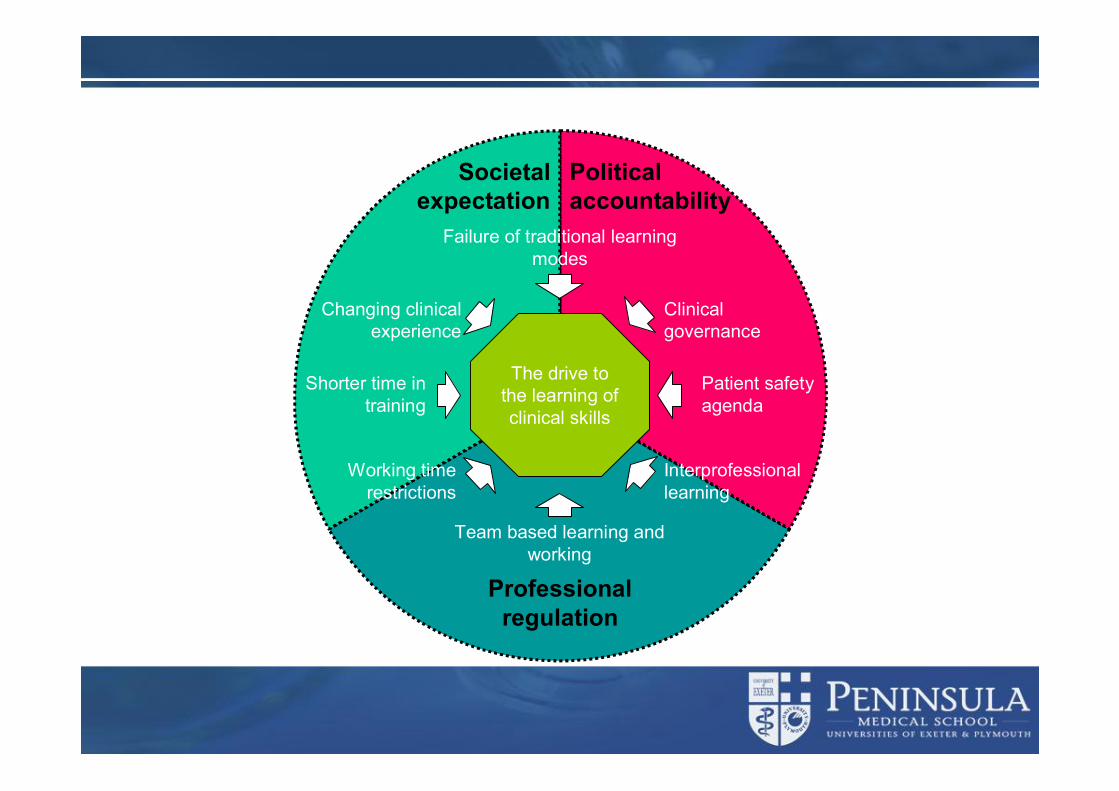
Professionalregulation
Political accountability
Societal expectation
Shorter time in training
Changing clinical experience
Failure of traditional learning modes
Team based learning and working
Interprofessional learning
Patient safety agenda
Working time restrictions
Clinical governance
The drive to the learning of clinical skills
What has been the response?
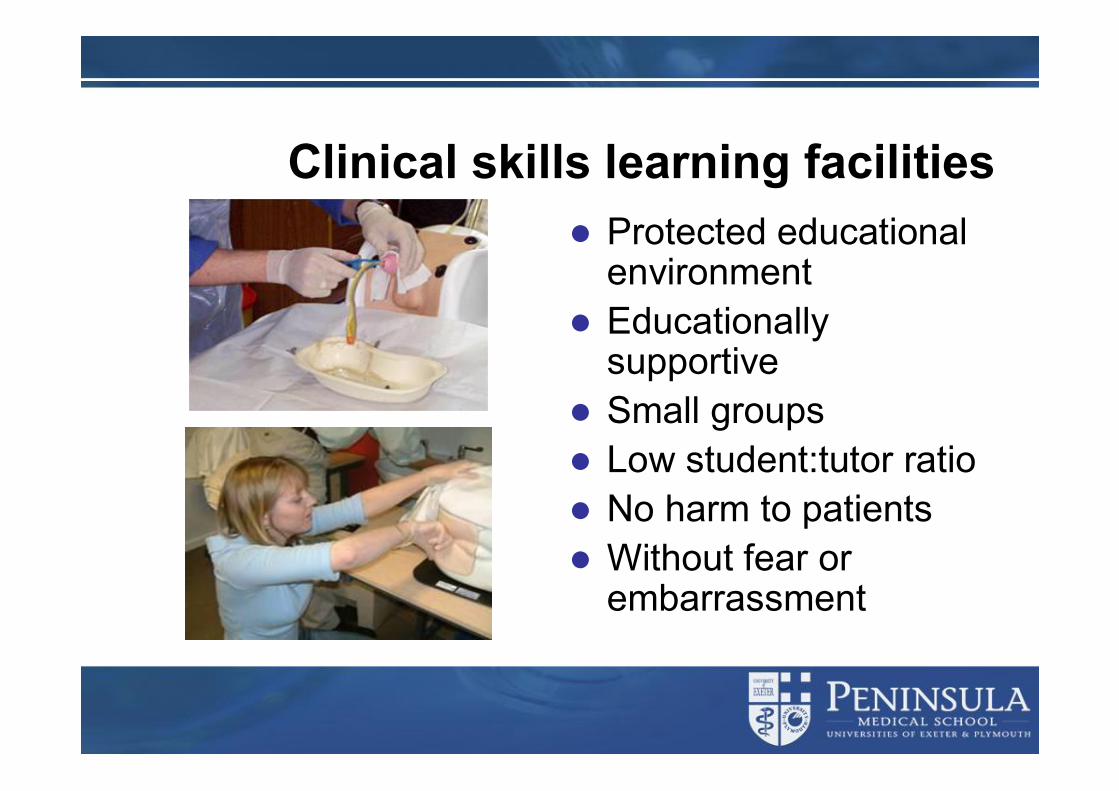
Clinical skills learning facilitiesl Protected educational
environmentl Educationally
supportivel Small groupsl Low student:tutor ratiol No harm to patientsl Without fear or
embarrassment
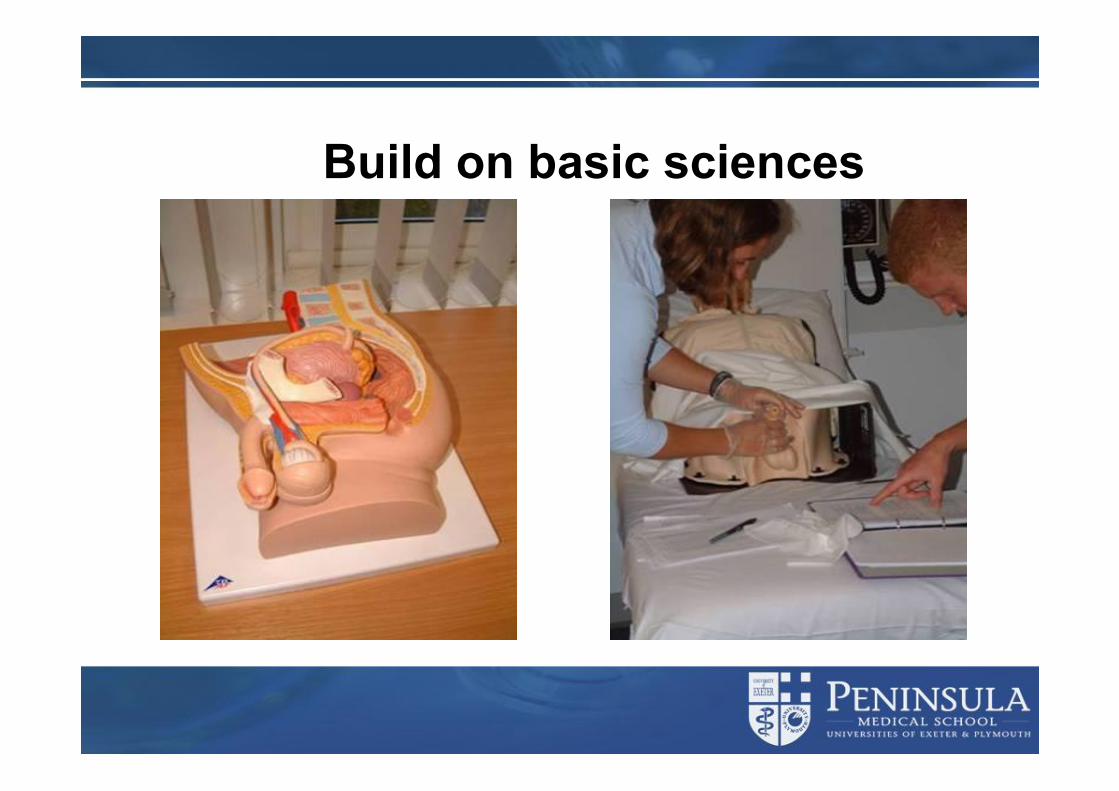
Build on basic sciences
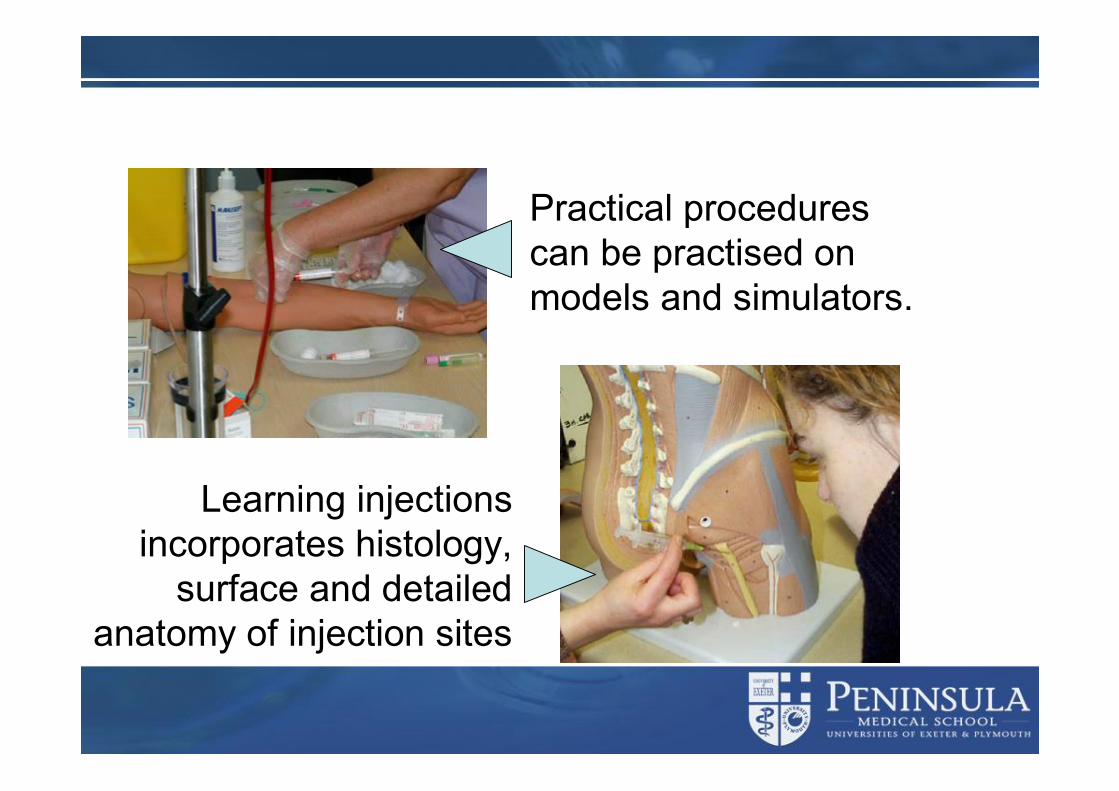
Practical procedures can be practised on models and simulators.
Learning injections incorporates histology,
surface and detailed anatomy of injection sites
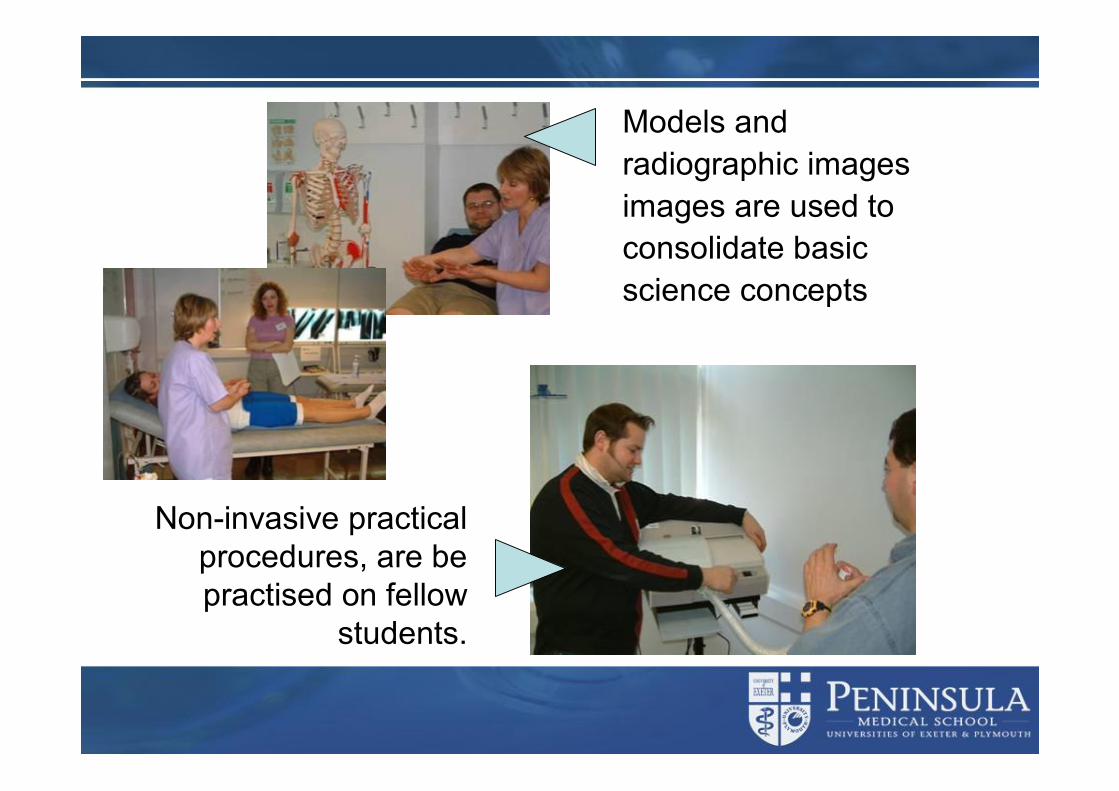
Models and radiographic images images are used to consolidate basic science concepts
Non-invasive practical procedures, are be practised on fellow
students.
Skills progressionl Practice on each other
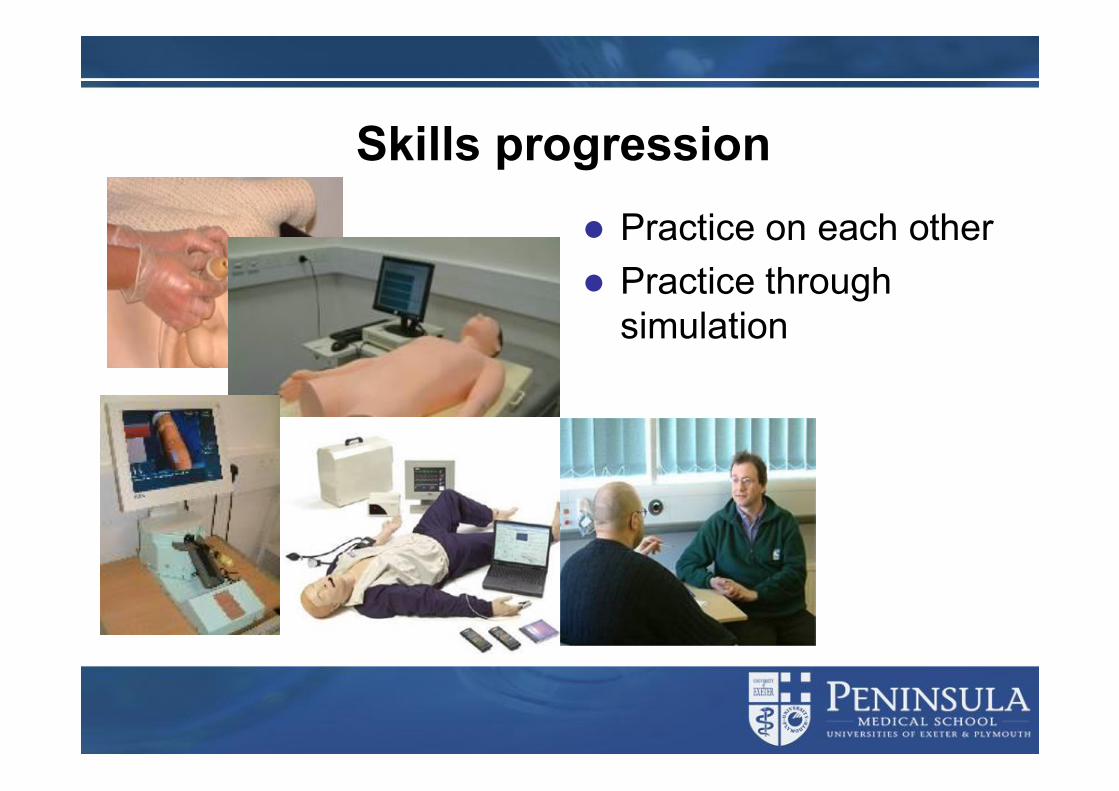
Skills progressionl Practice on each otherl Practice through
simulation
Skills progressionl Practice on each otherl Practice through
simulationl Practice within the real
clinical environment
Words of cautionl Prior teaching and learning in clinical skills does
not deliver a finished productl Prior learning in clinical skills does not preclude
the need for repeated deliberate practice accompanied by observation and feedback on performance
l Prior learning can improve but does not remove the culture shock of real world application of skills
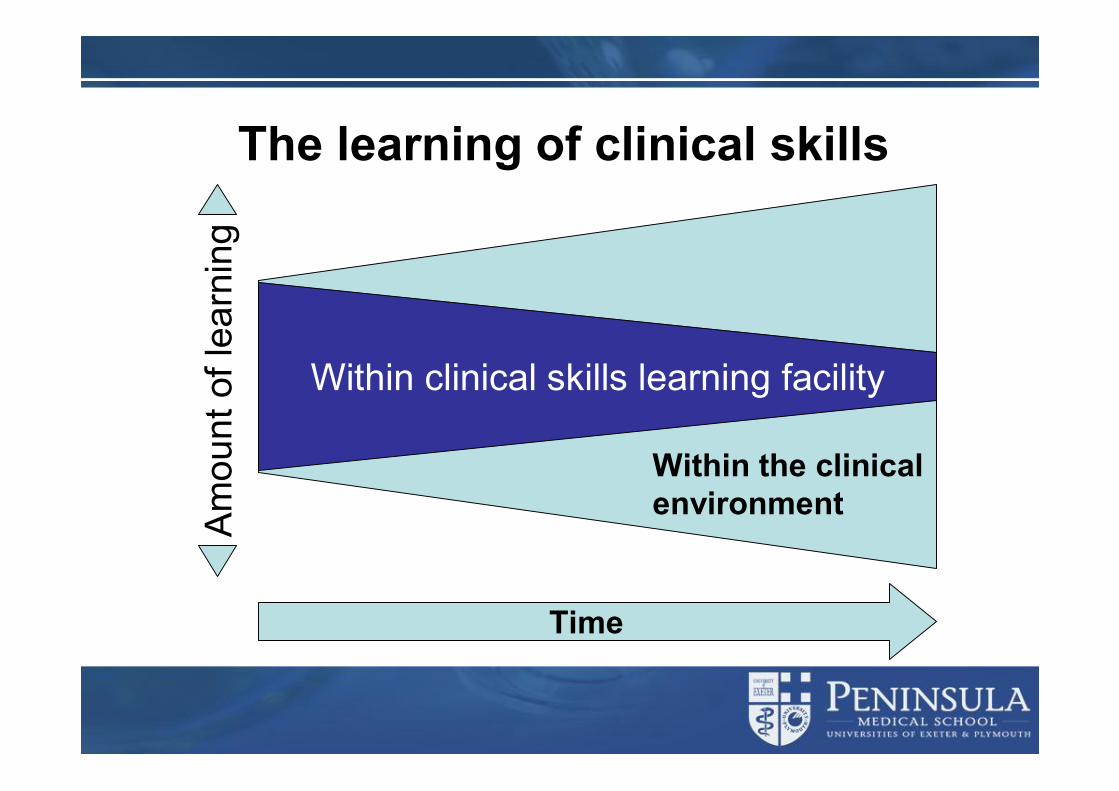
Within the clinical environment
The learning of clinical skills
Within clinical skills learning facility
Time
Am
ount
of l
earn
ing
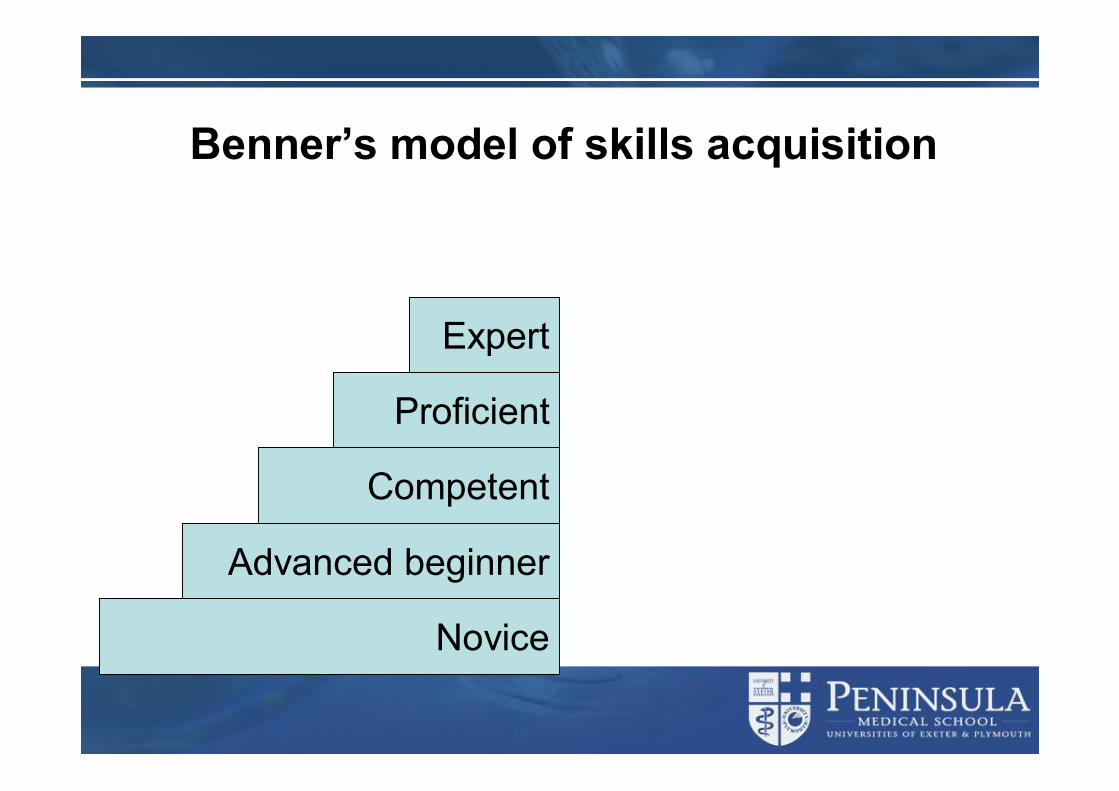
Benner’s model of skills acquisition
Novice
Advanced beginner
Competent
Proficient
Expert

Deliberate practice
Benner’s model and the relation to clinical skills learning
Novice
Advanced beginner
Competent
Proficient
Expert
Foundation learning
Clinically based experience
Transfer of clinical skillsl Clinical skills learning in the CSRC è successful
transfer of clinical skillsl This does not prevent “reality shock”l Students actively seek clinical skills experience in
the clinical environment l Support may be lackingl Students are aware of the need to refresh their
clinical skillsDonnelly, A., Foxall, P., & Bradley, P. (2006). Clinical Skills Resource Centre to a Clinical Environment: 3rd Year Medical Students' experience of clinical skills. Presented at AMEE, Genoa.

The spiral skills curriculum
l Progressivel Iterativel Continuous l Within clinical skills
learning facilities as foundation
l Within clinical setting with increased experience
Year 1Year 1
Year 3Year 3
Year 5Year 5
Year 2Year 2
Year 4Year 4
Clinical skills learningl There has tended to be a narrow focus to clinical
skills learningl A broad perspective of clinical skills is required
Defining clinical skills
“Any action undertaken by a healthcare professional intended to bring about an improvement in patient outcome”
What are clinical skills?l Administrative skillsl Attitudinal awareness and
professionalism l Clinical reasoning skillsl Communication skills l Critical appraisal skills inc
EBMl Documentation skillsl Economic skillsl Ethical/legal considerations l Health and safetyl History skills l ICT
l Investigative skills l Learning skillsl Organisational skillsl Patient managementl Physical examination skillsl Practical proceduresl Presentational skillsl Resuscitation skillsl Self care skillsl Teaching skillsl Team working and leadership
skills Bradley P. Introducing clinical skills training in the undergraduate medical curriculum. Medical Teacher 2002;24(2):209-212.
Spiral skills curriculum - resus
Year 1Year 1
Basic life support
Spiral skills curriculum - resus
Year 1Year 1
Year 2Year 2Defibrillation technique
Spiral skills curriculum - resus
Year 1Year 1
Year 3Year 3
Year 2Year 2
Advanced airways
Spiral skills curriculum - resus
Year 1Year 1
Year 3Year 3
Year 2Year 2
Year 4Year 4
Basic assessment of trauma
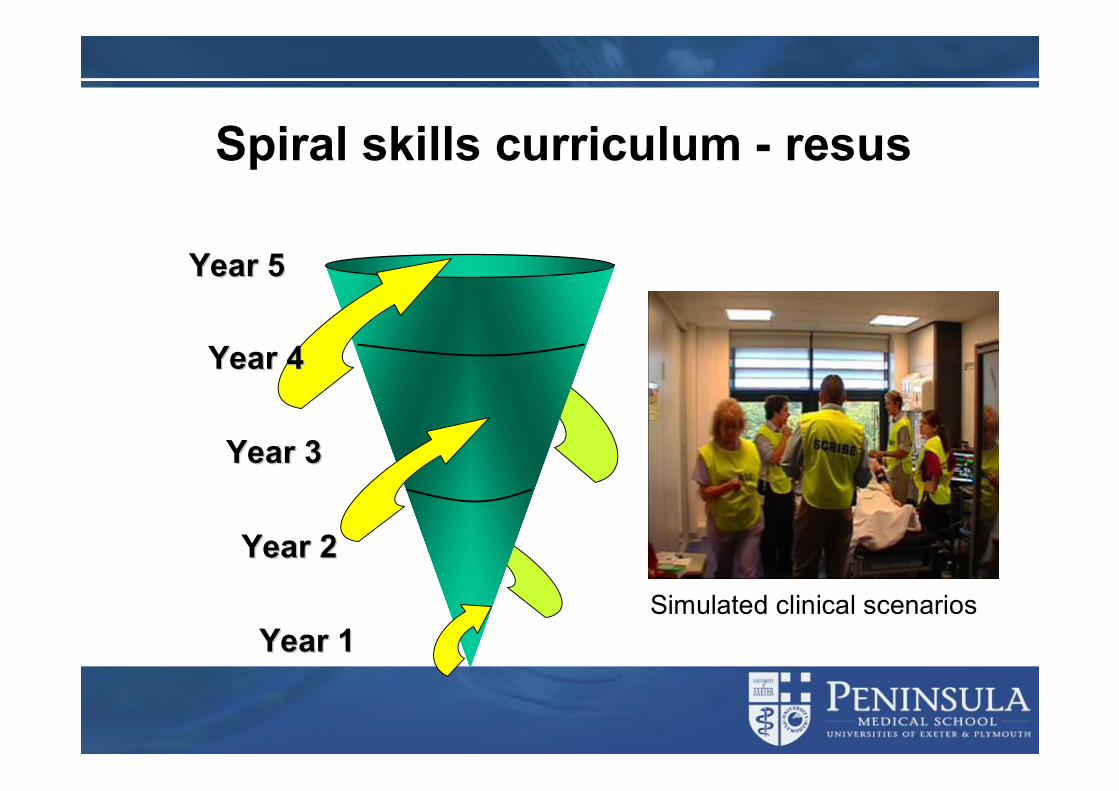
Spiral skills curriculum - resus
Year 1Year 1
Year 3Year 3
Year 5Year 5
Year 2Year 2
Year 4Year 4
Simulated clinical scenarios
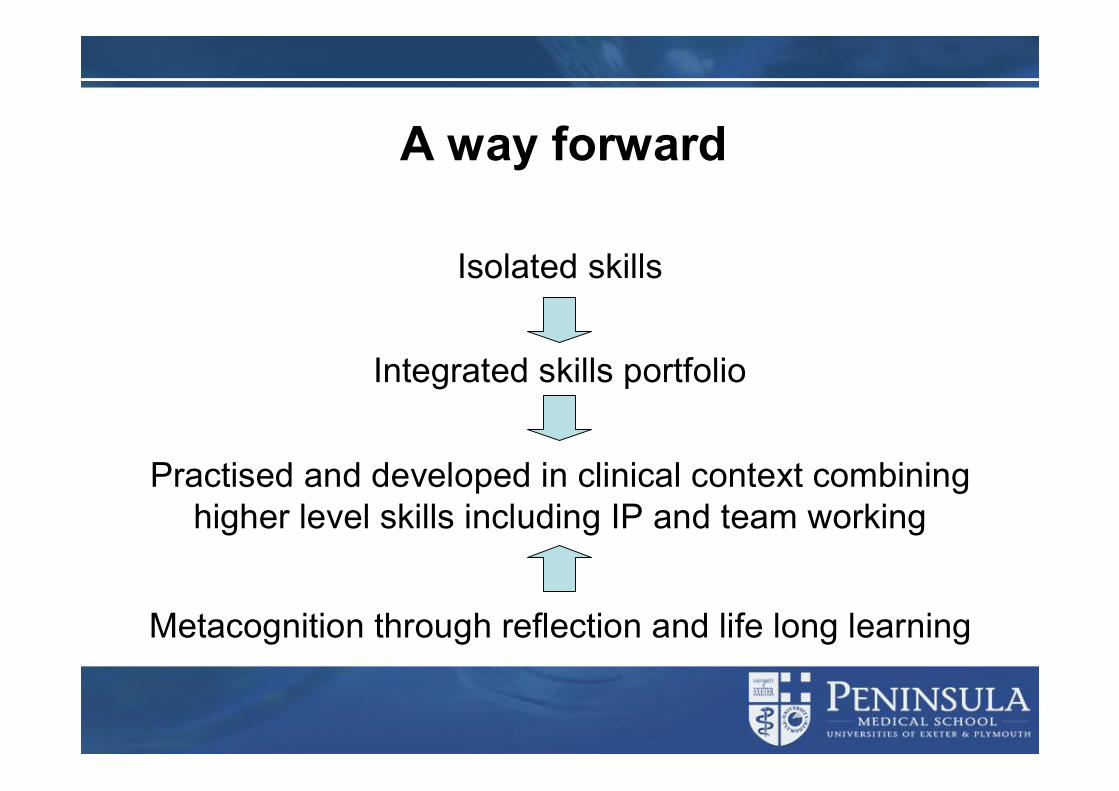
A way forward
Isolated skills
Integrated skills portfolio
Practised and developed in clinical context combining higher level skills including IP and team working
Metacognition through reflection and life long learning
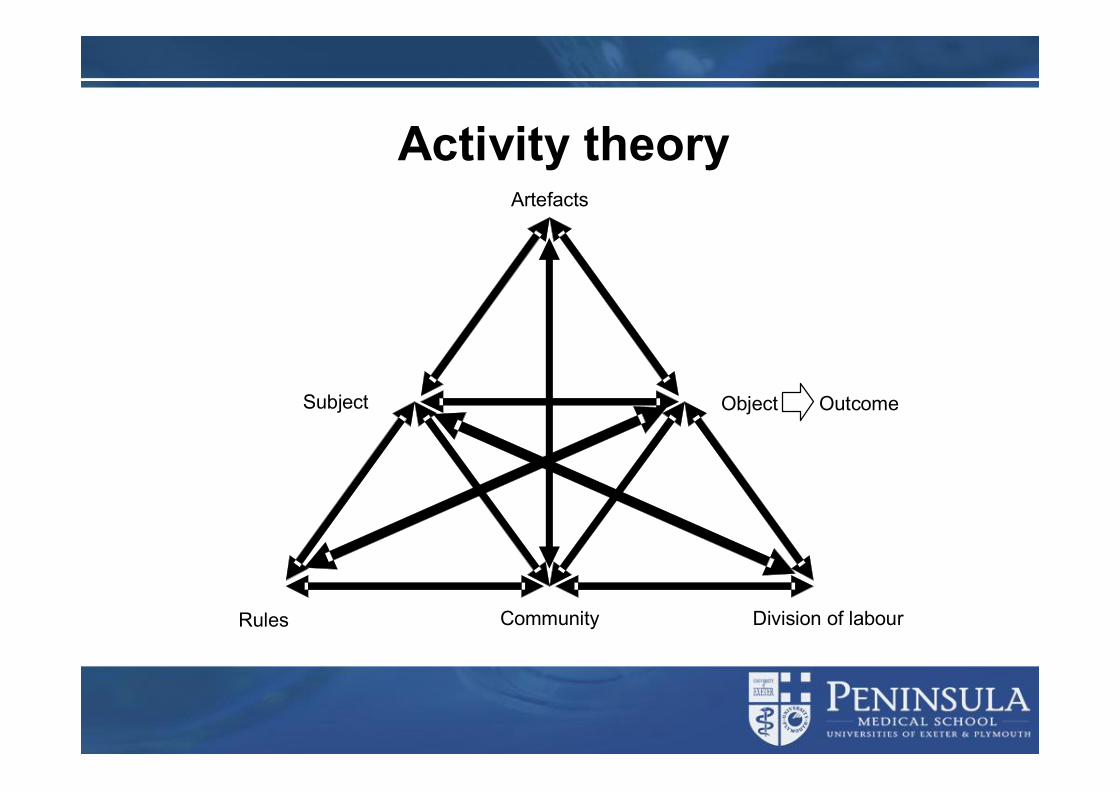
Activity theory
Subject Object Outcome
Community Division of labourRules
Artefacts

From Engeström Y 2001 Expansive learning at work: toward an activity theoretical reconceptualization
Journal of Education and Work 14,2 pp133-156
Simulator Work in operating theatre
Object 1
Rules Community Division oflabour
Subject
Mediating artifacts
Object 1
CommunityDivision oflabour
Subject
Mediating artifacts
Rules
Object 2
Object 2
Object 3
Activity Theory
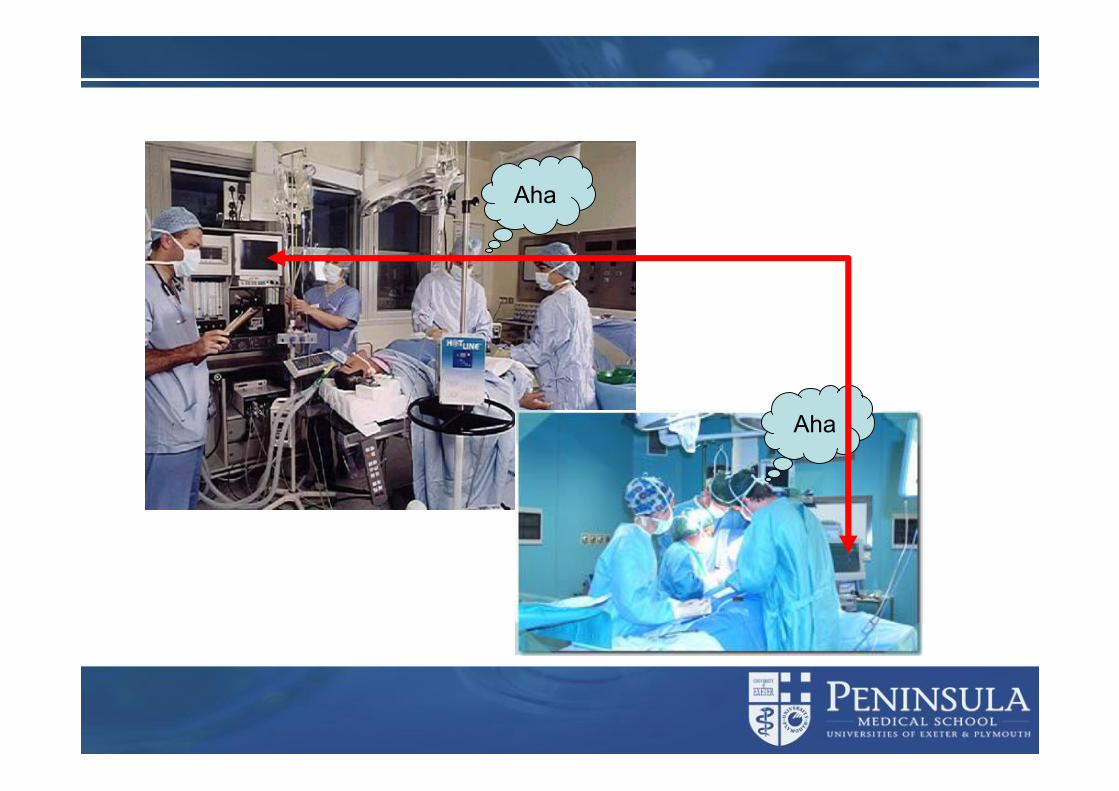
Aha
Aha
So should we concentrate on CSRC teaching and learning?
l The answer is a resounding NO!l Clinical Skills teaching and learning facilities
u Can provide foundation learningu Can ensure teaching and learning of coreu Can ensure consistencyu Can quality assure teaching and learningu Can provide a step up towards clinical learningu Can provide opportunities to learn and do things not
otherwise possibleu CANNOT replace clinical experience
Clinical skills – the research agenda
Building on theories of learningl Medical education and clinical skills learning is a
theory rich educational environmentl Regrettably it is a research poor environment
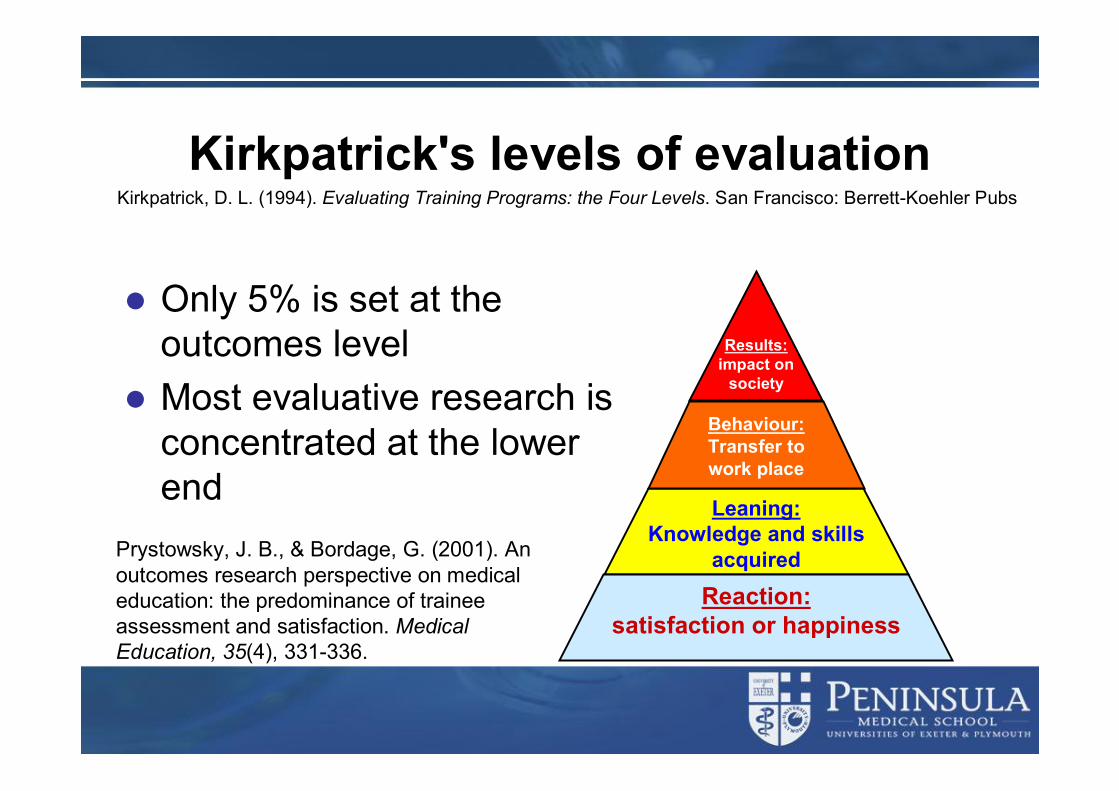
Kirkpatrick's levels of evaluation
l Only 5% is set at the outcomes level
l Most evaluative research is concentrated at the lower end
Reaction:satisfaction or happiness
Leaning:Knowledge and skills
acquired
Results:impact on
society
Behaviour:Transfer to work place
Prystowsky, J. B., & Bordage, G. (2001). An outcomes research perspective on medical education: the predominance of trainee assessment and satisfaction. Medical Education, 35(4), 331-336.
Kirkpatrick, D. L. (1994). Evaluating Training Programs: the Four Levels. San Francisco: Berrett-Koehler Pubs
Learning theoriesl Behaviourisml Constructivisml Social constructivisml Reflective practicel Situated learningl Activity theory
Bradley, P., & Postlethwaite, K. (2003). Simulation in clinical learning. Medical Education, 37(s1), 1-5.
Learning theoriesl Theories can inform our practisel Models of teaching and learning can be
developed that best support our studentsl Theories can be testedl Theories can be revised
Fashions in medical educationl Unexplored assumptions about knowledge underpinning
practice underlie some fashions l Definitions of a topic may be vague or differ l Educational reasoning and justification are implicit at
best and at worst absentl Qualitative information to substantiate empirical data is
often lackingl The feasibility of implementing interventions is ignored
or overlookedTrend spotting: fashions in medical educationJoseph K Campbell, Cindy Johnson - BMJ 1999;318:1272–5
Fashions in medical education
Over reliance on hard science
Over reliance on common sense
Relevance to practise overlooked
Publications about vague concepts
Uncritical use of articles to support position
Fashions in medical education
Over reliance on hard science
Over reliance on common sense
Relevance to practise overlooked
Publications about vague concepts
Uncritical use of articles to support position
Advances in medical education practice
Ways forward} Critical dialogue} Clear definitions} Educational justification} Qualitative and quantitative evidence} Consider utility and feasibility} Look to other disciplines
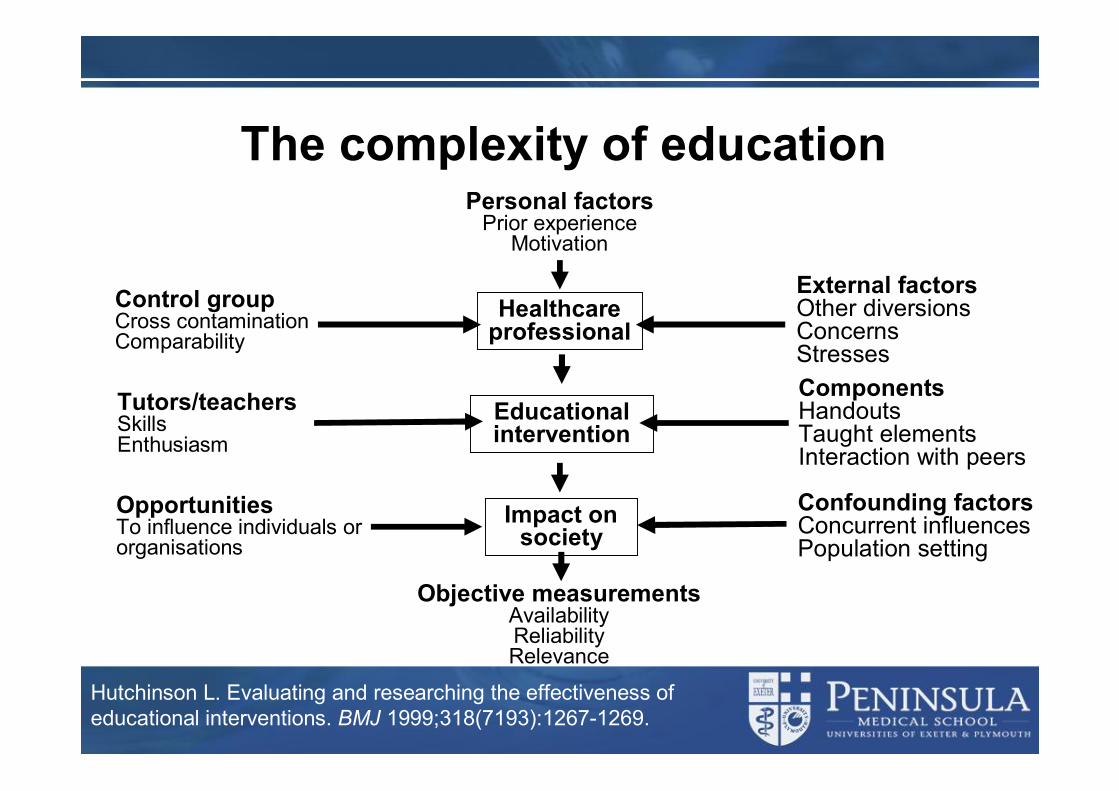
The complexity of education
Hutchinson L. Evaluating and researching the effectiveness of educational interventions. BMJ 1999;318(7193):1267-1269.
Personal factorsPrior experience
Motivation
Objective measurementsAvailabilityReliabilityRelevance
Control groupCross contaminationComparability
Healthcare professional
External factorsOther diversionsConcerns Stresses
Educational intervention
Tutors/teachersSkillsEnthusiasm
ComponentsHandoutsTaught elementsInteraction with peers
Impact on society
OpportunitiesTo influence individuals or organisations
Confounding factorsConcurrent influencesPopulation setting
Research paradigms - Scientificl There is a single tangible ‘reality’, parts of which can be
studied independentlyl The whole is the sum of the partsl It is possible to separate the observer from the observed,
the knower from the knownl What is true at one time and place may well be true at
anotherl Causality is linear – causes lead to effectsl Any enquiry can be value free
Research paradigms - Interpretativel Realities are multiple, and are individually (or socially)
constructed
l The knower cannot be separated from the known
l We can only make statements that are time and context bound
l All entities are continually shaping each other
l Inquiry is inevitably value-bound
Research paradigms - Criticall Oriented toward critiquing and changing society as a
whole
l Directed at the totality of society in its historical specificity
l Knowledge enables human beings to emancipate themselves from forms of domination through self-reflection
l “Teacher as researcher” and action research
A possible way forwardl Encompass the interpretive paradigm
l Make more targeted use of the scientific paradigm to capitalise upon its particular ‘range of convenience’
l Strive for increased theoretical clarity with respect to learning theories
l Together, these ideas could lead to rather different kinds of enquiry
Research in the Scientific paradigml Appropriate for behaviourist learning theories l Use objective data e.g. hi-fid simulator parameters:udata on the actions of the learneru the variables in the underlying mathematical
models as the simulator reacts to the learner’s interventions
Research in the Scientific paradigml Use data u In ways consistent with behaviourist learning
theory, as feedback to reinforce desired behaviour
uTo investigate improvement in students’performance of the skill has improved
l Issues of the validity and reliability of the data would be technical issues related to the adequacy of models, etc.
l Sample size may remain a problemusharing of data across sites?
Research in the Interpretative paradigm
l Appropriate for constructivist learning theory e.g. in the learning of new concepts relevant to an intervention
l Explore and challenge students’ prior thinking about the relevant systems; teach the accepted ideas
l Investigate uChanges in the effectiveness of the
interventions students make

Research in the Interpretative paradigm
l And alsouwhat students say they have learnt –
what their new models areuwhat they say enabled or disrupted that
learninguwhat the learners feel about the learning
experiencel Leads to understanding of a learning experience
in depth from the perspective of the participants
And how should this research be guided?
l International, national and local needsl International, national and local collaborationsl Ask the questionsuSo what?nand
uWho cares?
Summaryl In clinical skills, research has been patchy and poorly
focussedl Methodological weakness has plagued much researchl The field is complex and messy and not an easy research
domainl This should not deter us from pursuing better research in
the futurel Without the evidence we will be going nowhere and may
go backwards

Conclusionsl Clinical skills learning is a key component of modern
medical education l The limitations of learning in educational facilities must be
recognisedl The potential to exploit the learning must also be
recognised and realisedl High quality research using mixed methods is required to
evaluate, justify and develop clinical skills l Collaboration and cooperation between centres are
needed to share best practice and to advance the research agenda
So how should the face changel A reconstruction driven by theoretical stance l Dedicated to innovation in teaching and learningl Shard values, mission and aims amongst
educators in clinical skillsl A drive tou Share best practiceu Evidence based educationu Common research goals