Embed Size (px)
Citation preview

2004;113;1735PediatricsL. Kaplan and Mary L. Brandt
Karen D. Schultz, Leland L. Fan, Jay Pinsky, Lyssa Ochoa, E. O'Brian Smith, SheldonManagement
The Changing Face of Pleural Empyemas in Children: Epidemiology and
http://pediatrics.aappublications.org/content/113/6/1735.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2004 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at UNIV OF CHICAGO on May 29, 2013pediatrics.aappublications.orgDownloaded from

The Changing Face of Pleural Empyemas in Children: Epidemiologyand Management
Karen D. Schultz, MD*; Leland L. Fan, MD*; Jay Pinsky, BA‡; Lyssa Ochoa, MD‡; E. O’Brian Smith, PhD§;Sheldon L. Kaplan, MD�; and Mary L. Brandt, MD‡
ABSTRACT. Objective. Empyema remains a signifi-cant cause of morbidity in children. This study evaluatesthe changes that have affected the outcome in childrenwith pleural empyema, including the emergence of resis-tant organisms, the introduction of the pneumococcalconjugate vaccine, and earlier treatment with video-as-sisted thoracoscopy (VATS).
Methods. A retrospective chart review was performedon all patients who were discharged with a diagnosis ofempyema and community-acquired pneumonia over a10-year period (1993–2002) at Texas Children’s Hospitalin Houston, Texas. Data collected included demographicinformation, clinical presentation, radiographic studies,laboratory data including culture results, and hospitalcourse.
Results. A total of 230 charts were available for re-view. The mean age of the patients was 4.0 � 3.6 years. Ofthe pleural fluid cultures performed, 32% (69 of 219) werepositive. An additional 27 patients had a cause identifiedby blood culture. The first penicillin-nonsusceptibleStreptococcus pneumoniae was identified in 1995, and thefirst methicillin-resistant Staphylococcus aureus wasidentified in 1998. After the universal use of the pneu-mococcal conjugate vaccine, 3 major changes have oc-curred (1999–2000 vs 2001–2002): 1) the number of pa-tients admitted with empyema (per 10 000 admissions)has decreased from 23 to 12.6; 2) the prevalence of Spneumoniae has decreased from 66% (29 of 44) to 27% (4of 15); and 3) S aureus has become the most commonpathogen isolated (18% vs 60%), with 78% of those beingmethicillin resistant. The use of early VATS (<48 hoursafter admission) versus late VATS (>48 hours after ad-mission) significantly decreased the length of hospital-ization (11.49 � 6.56 days vs 15.18 � 8.62 days).
Conclusions. The microbiologic cause of empyemahas changed with an increasing incidence of S aureus,particularly methicillin-resistant S aureus. The use ofVATS for initial therapy of empyema results in de-creased duration of fever and length of hospitalization.Pediatrics 2004;113:1735–1740; empyema, community-ac-quired pneumonia, video-assisted thoracic surgery, chil-dren, microbiology.
ABBREVIATIONS. CTD, chest tube drainage; VATS, video-as-sisted thoracic surgery; PCN-NS, penicillin nonsusceptible; MIC,minimum inhibitory concentration; LOS, length of stay; MRSA,methicillin-resistant Staphylococcus aureus; PCN-S, penicillin sus-ceptible; MSSA, methicillin-susceptible Staphylococcus aureus.
Pleural effusions and empyemas are knowncomplications of bacterial pneumonia. Effu-sions occur in at least 40% of bacterial pneu-
monias, with up to 60% of effusions resulting in theformation of empyema in all age groups.1,2 Recentstudies have noted an increase in the incidence ofempyemas in children.3–6 Other reports have sug-gested a change in the cause of empyemas in chil-dren, including an increase in resistant organisms aswell as a decline in the incidence of Streptococcuspneumoniae.7–10
Multiple nonantibiotic treatment modalities existfor pleural effusions and empyemas, including tho-racentesis, chest tube drainage (CTD), instillation offibrinolytic therapy into the pleural cavity, and de-cortication. With the advent of video-assisted tho-racic surgery (VATS), pleural debridement, or “lim-ited decortication,” has become more common. Theless invasive nature of VATS, as well as excellentpublished results, has led many experts to recom-mend an early surgical approach to drain the pleuralspace, rather than thoracentesis, chest tube place-ment, or antibiotics alone.11,12 This study was per-formed to document the changes in microbiologiccauses and therapeutic procedures during the past 10years in patients with empyema associated withcommunity-acquired pneumonia at Texas Children’sHospital.
METHODSMedical records of all patients who were discharged with a
diagnosis of empyema associated with community-acquiredpneumonia from 1993 to 2002 from Texas Children’s Hospital inHouston, Texas, a tertiary referral hospital, were reviewed retro-spectively. Cases were identified through International Classifica-tion of Diseases, Ninth Revision codes of 510.0 (empyema withfistula) or 510.9 (empyema without fistula). Coding of the diag-nosis of empyema was at the discretion of the discharge physician.The annual number of patients admitted was obtained from theInformation Services Department. For our study, an empyemawas defined as a loculated or septated effusion by radiographicstudy or findings of pus or loculated effusion at the time ofsurgical intervention. Patients were excluded when they had sig-nificant neurologic abnormalities predisposing to aspiration, im-munosuppression, or a significant underlying disease that wouldnot be associated with community-acquired pathogens (eg, tra-cheostomy, cystic fibrosis).
Organisms defined as pathogens included S pneumoniae, Staph-
From the *Department of Pediatrics, Pulmonology Section, Baylor Collegeof Medicine Houston, Texas; ‡Michael E. DeBakey Department of Surgery,Department of Pediatrics, Baylor College of Medicine Houston, Texas;§Department of Pediatrics, Nutrition Section, Baylor College of MedicineHouston, Texas; and �Department of Pediatrics, Infectious Diseases Section,Baylor College of Medicine Houston, Texas.Received for publication Aug 18, 2003; accepted Mar 1, 2004.Reprint requests to (M.L.B.) Texas Children’s Hospital, 6701 Fannin, CC650.00, Houston, TX 77030. E-mail: [email protected] (ISSN 0031 4005). Copyright © 2004 by the American Acad-emy of Pediatrics.
PEDIATRICS Vol. 113 No. 6 June 2004 1735 at UNIV OF CHICAGO on May 29, 2013pediatrics.aappublications.orgDownloaded from

ylococcus aureus, group A streptococcus, and Haemophilus influen-zae. Penicillin-nonsusceptible (PCN-NS) S pneumoniae was definedas a penicillin minimum inhibitory concentration (MIC) �0.1 �g/mL, penicillin-intermediate MIC �0.1 to 1.0 �g/mL, and penicil-lin-resistant MIC �2 �g/mL by E-test. Duration of fever wasdefined as the length of time until the patient was afebrile(�100.5°F) for 24 hours. Length of hospitalization was defined asthe number of days that the patient was hospitalized at ourinstitution.
A standardized data form was completed retrospectively foreach patient with empyema. Information collected included de-mographic, preadmission, microbiologic, radiographic, manage-ment, and complication data. The study was approved by theInstitutional Review Board of Baylor College of Medicine. Datawere entered in to a Microsoft Access (Redmond, WA) database.Data analysis was performed with Minitab (State College, PA)statistical software. Analysis of covariance was used to assess theeffects of VATS timing and differences between resistant andsusceptible bacteria on length of stay (LOS) and length of feverwhile adjusting for potential confounding variables. �2 was usedto compare incidence rates over time. Results are presented asmean � standard deviation. A t test was used to compare baselinecharacteristics of the early versus late VATS intervention groups.
RESULTSA total of 230 charts were reviewed. A complete
analysis could not be performed on 18 charts. How-ever, limited data were available through the hospi-tal computer system (demographic data, laboratoryand culture data, and radiographic data). Proceduredata were not available on these patients. The aver-age age of the 230 patients was 4.0 � 3.6 years (range:3 weeks to 16.6 years). The male to female ratio was1.3:1. The ethnic breakdown was similar to that ofoverall admissions to the hospital except that signif-icantly more white children were admitted with em-pyema compared with overall hospital admissions (P� .05).
During the study period, the number of admis-sions for empyema initially increased, with a peak of23.0 cases/10 000 admissions during 1999–2000 (P �.06 for 1997–1998 vs 1999–2000, and P � .007 for1993–1998 vs 1999–2000). However, the number ofcases decreased during the following 2-year period(12.6 cases/10 000 admissions; P � .06) to a similarrate to that seen in 1997–1998 (Table 1). Of the pleuralfluid cultures performed, 32% (69 of 219) were pos-itive. An additional 27 patients had a cause identifiedby blood culture (overall yield: 43%). There were nopositive blood cultures for S aureus during the studyperiod. The number of positive cultures did not sig-nificantly change during the 10-year study period.However, there was a significant decrease in theproportion of positive cultures during the last 2-yearperiod (44 [50%] of 88 in 1999–2000 and 15 [32%] of47 in 2001–2002; P � .04; Table 1).
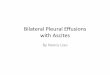
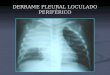
The first PCN-NS S pneumoniae was identified in1995, and the first methicillin-resistant S aureus(MRSA) was identified in 1998. The number of Spneumoniae cases also increased during the first 8years of the study, with a peak incidence of 29 cas-es/44 isolates in 1999–2000. During 2001–2002, thenumber of cases of S pneumoniae decreased signifi-cantly (4 cases/15 isolates; P � .03). The absolutenumber of cases of empyema caused by S aureusincreased substantially during the entire period ofthe study, although the proportion of isolates thatwere S aureus did not change significantly (�2 fortrend, P � .09) However, the proportion of casescaused by S aureus increased significantly during1999–2000 versus 2001–2002 (8 of 44 vs 9 of 15; P �.03; Table 1, Fig 1). The percentage of PCN-NS Spneumoniae did not change significantly during thestudy period. Thirteen of 52 pneumococcal isolateswere resistant to erythromycin; only 4 of 52 isolateswere resistant to clindamycin. Among the positivecultures, the proportion that was MRSA increasedsignificantly during the course of the study (P �.00016, �2 for trend). The number of cases of empy-ema based on causative organism and age is pre-sented in Fig 2. The empyema cases caused by Saureus occurred primarily in children who wereyounger than 1 year (14 S aureus isolates/28 positivecultures for children younger than 1 year vs 10 Saureus isolates/197 positive culture for children olderthan 1 year; P � .001).
The LOS was not significantly different betweenthe patients with infection caused by PCN-NS Spneumoniae versus penicillin-susceptible (PCN-S) Spneumoniae (8.92 � 1.31 days vs 9.64 � 1.42 days; P �.158). However, it did approach significance whencorrected for age with the PCN-S S pneumoniae grouphaving a longer LOS (14.70 � 2.18 days vs 20.88 �2.42 days; P � .07). In contrast, comparing empyemacases caused by MRSA versus methicillin-susceptibleS aureus (MSSA), the MRSA group had a significantlylonger LOS (18.83 � 1.66 days vs 14.00 � 1.66 days;P � .05). Duration of fever was similar in thePCN-NS versus PCN-S S pneumoniae (8.92 � 1.31days vs 9.64 � 1.42 days; P � .71) groups as well asthe MRSA versus MSSA (7.10 � 1.55 days vs 10.09 �1.47 days; P � .18) groups.
Information on therapeutic interventions wasavailable for 212 patients. Of those, 4 received anti-biotics only, 19 had a thoracentesis and/or had achest tube placed, and 189 underwent some type ofsurgical intervention: VATS (n � 125), minithora-
TABLE 1. Culture Data Based on Time Period
1993–1994 1995–1996 1997–1998 1999–2000 2001–2002 P Value*
Total admissions for empyema 19 24 48 88 51Empyema admissions/10 000 hospital admissions 5.8 6.7 13 23 12.6 .06Proportion of positive cultures (blood or pleural fluid) 7/19 8/15 20/48 44/88 15/47 .04S pneumoniae isolates 5 3 11 29 4 .03PCN-NS S pneumoniae isolates 0 2 4 11 2 NSS aureus isolates 1 3 3 8 9 .03MRSA isolates 0 0 1 4 7 NS
NS indicates not significant.* P value compares 1999–2000 and 2001–2002.
1736 EMPYEMAS IN CHILDREN at UNIV OF CHICAGO on May 29, 2013pediatrics.aappublications.orgDownloaded from

cotomy (n � 31), or open thoracotomy (n � 32).Complications, including lung abscess, pneumato-cele formation, bronchopleural fistula formation, re-spiratory failure, requirement of a blood transfusion,and air leak �24 hours, were not statistically signif-icant between the nonsurgical and surgical groups.Eight patients required lobectomy during the studyperiod. There were no deaths from empyema asso-ciated with community-acquired pneumonia duringthe study period.
A total of 125 patients underwent VATS. Of those,49 patients had the procedure performed within 48hours of admission (early VATS) versus 76 who un-derwent the procedure �48 hours after admission(late VATS). Baseline characteristics of the 2 groupsare presented in Table 2. The only significant differ-ences were previous hospitalization and admissionservice, with more patients in the early interventiongroup being admitted to the surgical service. TheLOS was significantly shorter in the early VATSgroup compared with the late VATS group (11.49 �6.56 days vs 15.18 � 8.62 days; P � .008). Adjustmentfor age, race, gender, admission service, fever, and
cough duration before hospitalization, duration ofpresumed viral illness before hospitalization, atten-dance at child care, smoking in the home, use ofnonsteroidal anti-inflammatory agents and antibiot-ics before hospitalization, bacterial cause, and previ-ous hospitalization both individually and combineddid not alter the significance of the decreased LOS inthe early intervention group (11.12 � 2.82 days vs13.94 � 2.74 days; P � .013). The length of fever after
Fig 1. Number of cases of empyema caused by S aureus from 1993 to 2002 at Texas Children’s Hospital. MSSA versus MRSA.
Fig 2. Distribution of empyema cases based on age and cause from 1993 to 2002 at Texas Children’s Hospital.
TABLE 2. LOS and Baseline Characteristics of Early VersusLate VATS
Early VATS Late VATS P Value
LOS (all patients) 11.49 � 6.56 15.18 � 8.62 .008Age 5.01 � 4.23 3.78 � 3.24 NSAdmission service, % .04
General pediatrics 51 67Pulmonary 26 20Surgery 12 1Other 10 12
LOS (Texas Children’sHospital admissiononly)
9.91 � 2.95 12.34 � 2.80 .027
ARTICLES 1737 at UNIV OF CHICAGO on May 29, 2013pediatrics.aappublications.orgDownloaded from

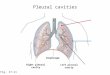
hospitalization was significantly shorter for earlyversus late VATS (7.1 � 5.6 days vs 9.4 � 5.5 days;P � .046). Forty-five percent of patients in the earlyVATS group remained febrile on day 5, with 10% stillfebrile on day 15 (Fig 3). There were no significantdifferences in complication rates between the earlyand late VATS groups, including lung abscess, pneu-matocele formation, bronchopleural fistula forma-tion, respiratory failure, requirement of a bloodtransfusion, air leak �24 hours, and need for lobec-tomy (Table 3).
DISCUSSIONPneumonia is a common childhood disease. with
an incidence of between 1.0 and 4.5 cases per 100children per year.13 Although most cases of pneumo-nia are viral in cause, bacteria are the causative agentin 20% to 30% of patients.14 Bacterial pneumonia canbe severe and life-threatening, accounting for �3million pediatric deaths per year worldwide, primar-ily in resource-poor countries.15 Our study confirmsthe observations of others that there has been anincrease in the incidence of empyema in children.3–6
However, the routine administration of the pneumo-coccal conjugate vaccine to infants beginning at 2months of age has resulted in a significant decreasein the number of cases of empyema caused by Spneumoniae. This observation affirms the recent find-ings of Whitney et al16 indicating a decrease in theincidence of invasive pneumococcal disease amongchildren in the United States after universal vaccina-tion. Our study also confirms the findings of Bying-ton et al6 with an increased rate of admission ofwhite children in patients with empyema comparedwith the general hospital population. The reason forthis increase is unclear; however, it may be attribut-able to better access of care by white children whoare treated with inadequate outpatient therapy.
Identification of the causative agent in childrenwith empyema is often difficult, necessitating the useof empiric rather than specific therapy.13,14 Reporteddiagnostic yield from pleural and/or blood cultures
ranges from 60% to 70%.6,17 Only 43% of our pedi-atric patients had a cause established by either bloodor pleural cultures. Campbell et al18 suggested thatblood cultures have limited usefulness in adults withcommunity-acquired pneumonia. Our yield fromblood cultures was higher before 2001, with a largedecrease in the incidence of positive blood culturesduring the past 2 years, related both to a decline inpneumococcal infections and to an increase in theincidence of S aureus empyema that was associatedwith negative blood cultures. However, in patientswith a positive culture, 28% had a cause identified byblood culture only.
The most common pathogens that cause effusionsor empyemas associated with community-acquiredpneumonia in children are S pneumoniae, S aureus,and group A streptococcus.2 From 1995 to 1998, therewas a significant increase in the proportion of Spneumoniae isolates resistant to penicillin, cefotaxime,erythromycin, and trimethoprim-sulfamethoxazolerecovered from invasive infections in the UnitedStates. Multidrug resistance also increased.9 Patientswho were at an increased risk of having S pneumoniaeisolates with antibiotic resistance were younger than5 years, of white race, or hospitalized.9 However,multiple studies have not demonstrated an increasein adverse outcomes of pneumonia caused byPCN-NS versus PCN-S S pneumoniae. Hardie et al8demonstrated no difference in the LOS, days of fever,
Fig 3. Proportion of patients with empyema becoming afebrile in early versus late VATS.
TABLE 3. Complications for Early Versus Late VATS
Early(n � 46)
Late*(n � 79)
Lung abscess 3 4Pneumatocele 2 7Bronchopleural fistula 1 1Respiratory failure (before
or after procedure)5 6
Blood transfusion 9 18Air leak �24 h 3 5Lobectomy 3 3
* There were no significant differences found.
1738 EMPYEMAS IN CHILDREN at UNIV OF CHICAGO on May 29, 2013pediatrics.aappublications.orgDownloaded from

days of hypoxia, or need for lobectomy betweenthese 2 groups. Furthermore, Tan et al10 showedno difference in the development of complicated ver-sus uncomplicated effusions with PCN-S versusPCN-NS S pneumoniae. In fact, Byington et al6 foundan increase in the percentage of PCN-NS organismsin patients with simple pneumonia as comparedwith those who developed an empyema.
During 1999–2000, there was an increase in thenumber of cases of S pneumoniae at our institution.However, our data from the 2001–2002, which fol-lows the initiation of routine use of the pneumococ-cal conjugate vaccine, demonstrate a significant de-crease in the number of cases of empyema caused byS pneumoniae. We found no significant difference inthe LOS or duration of fever in the PCN-NS andPCN-S groups of S pneumoniae, with a trend towarda longer LOS in the PCN-S group. We did find a lowrate of resistance of S pneumoniae to clindamycin,suggesting that this antibiotic may be a useful optionin the treatment of pneumonia caused by PCN-NS Spneumoniae. Buckingham et al19 recently demon-strated an increase in the number of cases of compli-cated parapneumonic effusions caused by S aureus;however, they only accounted for 30% of the overallcases. Our absolute number of cases of empyemacaused by S aureus has increased during the 10 yearsof the study; the proportion of cases of empyemacaused by S aureus has significantly increased duringthe last 4 years of the study. S aureus has now becomethe most common causative agent of empyema iden-tified in our institution. The majority of these isolatesare MRSA (78% in 2001–2002).
The LOS for patients with empyema caused byMRSA was significantly longer than for those withpneumonia caused by MSSA; however, the durationof fever was similar in the 2 groups. Empiric therapyof empyema and pleural effusions associated withcommunity-acquired pneumonia should coverMRSA in communities in which at least 10% of com-munity S aureus isolates are MRSA. Vancomycin isthe gold standard therapy for treating serious infec-tions caused by MRSA. Clindamycin is a valuableagent for treating less severe pneumonia/empyemacaused by susceptible community-acquired MRSAisolates, but the laboratory must screen for the in-ducible form of macrolide-lincosamide-strepto-gramin resistance.20
The management of empyema in children remainscontroversial. The use of antibiotics alone is effectivetherapy in patients with simple pneumonia andthose with early effusion. However, drainage of thepleural space is often necessary in later stages ofparapneumonic effusions and empyemas. Nonsurgi-cal methods to drain the pleural space include tho-racentesis, single or repeated; small-caliber, flexibledrainage catheters; and large-bore CTD, with orwithout the use of fibrinolytics.21–28 Historically,CTD has been the mainstay of therapy; however, theother methods are gaining favor. Thoracentesis isgenerally easy to perform and can provide informa-tion on the causative agent as well as be therapeutic.Historically, surgical debridement or decortication inpatients with empyema has been reserved for those
with disease refractory to medical management.However, as early as 1990, some authorities advo-cated early surgical intervention in the treatment ofempyema, especially in patients with severe dis-ease.12 With the increased use of the minimally in-vasive surgery in the mid-1990s, VATS has beenproposed as a first-line therapy in patients with em-pyema, especially those with more advanced disease.A number of retrospective reviews have demon-strated that VATS decreases the length of CTD andhospitalization.11,12,29,30 One study demonstrated notonly a shorter LOS but also a decrease in the cost ofhospitalization in patients who were treated withprimary VATS.31
In our institution, most of the children who requirea thoracostomy tube are taken to the operating roomfor placement under more controlled and less psy-chologically traumatic circumstances. In the past sev-eral years, VATS has been generally performed inthese patients as they were usually placed undergeneral anesthesia. In the past 10 years, the majorityof our patients (189 of 212) have had surgical inter-vention at some point in their hospital course. There-fore, it is impossible for us to compare conservativemanagement (ie, antibiotics � thoracentesis/chesttube) with antibiotics plus surgical intervention.However, of the 125 patients who underwent VATS,those who were treated earlier (within 48 hours ofadmission) had a significantly shorter LOS. The onlysignificant baseline differences between these 2groups were previous hospitalization and admissionservice, with more patients in the early interventiongroup being admitted to the surgical service. Becauselength of hospitalization before admission at ourhospital was not taken into account in calculatingLOS, the additional days of hospitalization couldbias the total length of hospitalization of these pa-tients transferred to our hospital and thus affect thedifference between these 2 groups. However, therewas no significant interaction between LOS and pre-vious hospitalization on analysis. When the LOS wascorrected for previous hospital admissions (n � 43patients), it remained significantly shorter for pa-tients who were treated with early VATS (Table 2).The 4-day reduction in hospitalization that we ob-served is clinically significant, especially in the cur-rent era of managed care. Patients who underwentearly VATS also had a decreased length of feveroverall. However, although most patients in theearly VATS group were afebrile by day 5, 10% re-mained febrile on day 15, with 1 patient febrile onday 28. Therefore, persistently febrile patients shouldbe watched closely with no additional interventionunless there is a change in the patient’s status. On thebasis of our results, we believe that early VATS is aneffective and safe method of treating empyema inchildren and should be considered a treatment ofchoice.
In summary, the bacterial cause of empyema inchildren is changing. Since the routine administra-tion of the pneumococcal conjugate vaccine, we haveseen a significant decrease in the number of cases ofempyema caused by S pneumoniae and, for reasonsthat are not clear, an increase in the number of cases
ARTICLES 1739 at UNIV OF CHICAGO on May 29, 2013pediatrics.aappublications.orgDownloaded from

caused by S aureus, with the majority being MRSA.Clindamycin should adequately cover both MRSAand PCN-NS S pneumoniae in almost all outpatientinstances. Either clindamycin or vancomycin shouldbe included in the regimen of inpatients, the specificchoice depending on the severity of illness. Earlyintervention with VATS seems to decrease the lengthof hospitalization and should be considered for pa-tients with empyema.
REFERENCES1. Strange C. Pathogenesis and management of parapneumonic effusions
and empyema. In: Feigin RD (ed). UpToDate Pediatrics. Wellesley, MA:UpToDate; 2001
2. Givan DC, Eigen H. Common pleural effusions in children. Clin ChestMed. 1998;19:363–371
3. Rees JH, Spencer DA, Parikh D, Weller P. Increase in incidence ofchildhood empyema in West Midlands, UK. Lancet. 1997;349:402
4. Playfor SD, Smyth AR, Stewart RJ. Increase in incidence of childhoodempyema. Thorax. 1997;52:932
5. Thompson A, Reid A, Shields M, Steen H, Taylor R. Increased incidencein childhood empyema thoracis in Northern Ireland. Ir Med J. 1999;92:438
6. Byington CL, Spencer LY, Johnson TA, et al. An epidemiological inves-tigation of a sustained high rate of pediatric parapneumonic empyema:risk factors and microbiological associations. Clin Infect Dis. 2002;34:434–440
7. Sarihan H, Cay A, Aynaci M, Akyazici R, Baki A. Empyema in children.J Cardiovasc Surg (Torino). 1998;39:113–116
8. Hardie WD, Roberts, NE, Reising, SF, Christie CDC. Complicated para-pneumonic effusions in children caused by penicillin-nonsusceptibleStreptococcus pneumoniae. Pediatrics. 1998;101:388–392
9. Whitney CG, Farley MM, Hadler J, et al. Increasing prevalence ofmultidrug-resistant Streptococcus pneumoniae in the United States.N Engl J Med. 2000;343:1917–1924
10. Tan TQ, Mason EO, Wald ER, et al. Clinical characteristics of childrenwith complicated pneumonia caused by Streptococcus pneumoniae.Pediatrics. 2002;110:1–6
11. Grewal H, Jackson RJ, Wagner CW, Smith SD. Early video-assistedthoracic surgery in the management of empyema. Pediatrics. 1999;103(5).Available at: pediatrics.org/cgi/content/full/103/5/e63
12. Hoff SJ, Neblett WW, Edwards KM, et al. Parapneumonic empyema inchildren: decortication hastens recovery in patients with severe pleuralinfections. Pediatr Infect Dis J. 1991;10:194–199
13. Chin TW, Nussbaum E, Marks M. Bacterial pneumonia. In: Hilman BC(ed). Pediatric Respiratory Disease. Philadelphia, PA: WB Saunders; 1993:271–281
14. Correa AG, Starke JR. Bacterial pneumonias. In: Chernick V, Boat TF(eds). Kendig’s Disorders of the Respiratory Tract in Children. Philadelphia,PA: WB Saunders; 1998:485–503
15. Miller MA, Ben-Ami T, Daum RS. Bacterial pneumonia in neonates andolder children. In: Tuassig LM, Laundau LI (eds). Pediatric RespiratoryMedicine. St Louis, MO: Mosby; 1999:644–647
16. Whitney CG, Farley MM, Hadler JH, et al. Decline in invasive pneu-mococcal disease after the introduction of protein-polysaccharide con-jugate vaccine. N Engl J Med. 2003;348:1737–1746
17. Vuori-Holopainen E, Salo E, Saxen H, et al. Etiologic diagnosis ofchildhood pneumonia by use of transthoracic needle aspiration andmodern microbiological methods. Clin Infect Dis. 2002;34:583–589
18. Campbell SG, Marrie TJ, Anstey R, Dickinson G, Ackroyd-Stolarz S. Thecontribution of blood cultures to the clinical management of adultpatients admitted to the hospital with community-acquired pneumonia.Chest. 2003;123:1142–1150
19. Buckingham SC, King MD, Miller ML. Incidence and etiologies ofcomplicated parapneumonic effusions in children, 1996 to 2001. PediatrInfect Dis J. 2003;22:499–504
20. Martınez-Aguilar G, Hammerman WA, Mason EO Jr, Kaplan SL. Clin-damycin treatment of invasive infections caused by community-acquired, methicillin-resistant and methicillin-susceptible Staphylococ-cus aureus in children. Pediatr Infect Dis J. 2003;22:593–598
21. Shoseyov D, Bibi H, Shatzberg G, et al. Short-term course and outcomeof treatments of pleural empyema in pediatric patients: repeated ultra-sound-guided needle thoracentesis vs chest tube drainage. Chest. 2002;121:836–840
22. Mitri RK, Brown SD, Zurakowski D, et al. Outcomes of primary image-guided drainage of parapneumonic effusions in children. Pediatrics.2002;110(3). Available at: pediatrics.org/cgi/content/full/110/3/e37
23. Pierrepoint MJ, Evans A, Morris SJ, Harrison SK, Doull IJ. Pigtailcatheter drain in the treatment of empyema thoracis. Arch Dis Child.2002;87:331–332
24. Krishnan S, Amin N, Dozor AJ, Stringel G. Urokinase in the manage-ment of complicated parapneumonic effusions in children. Chest. 1997;112:1579–1583
25. de Benedictis FM, De Giorgi G, Niccoli A, Troiani S, Rizzo F, Lemmi A.Treatment of complicated pleural effusions with intracavity urokinasein children. Pediatr Pulmonol. 2000;29:438–442
26. Kornecki A, Sivan Y. Treatment of loculated pleural effusions withintrapleural urokinase in children. J Pediatr Surg. 1997;32:1473–1475
27. Barbato A, Panizzolo C, Monciotti C, Marcucci F, Stefanutti G, GambaPG. Use of urokinase in childhood pleural empyema. Pediatr Pulmonol.2003;35:50–55
28. Thomson AH, Hull J, Kumar MR, Wallis C, Balfour Lynn IM. Random-ised trial of intrapleural urokinase in the treatment of childhood empy-ema. Thorax. 2002;57:343–347
29. Kercher KW, Attorri RJ, Hoover D, Morton D Jr. Thoracoscopic decor-tication as first-line therapy for pediatric parapneumonic empyema.Chest. 2000;118:24–27
30. Doski JJ, Lou D, Hicks BA, et al. Management of parapneumoniccollections in infants and children. J Pediatr Surg. 2000;35:265–270
31. Meier AH, Smith B, Raghavan A, Lawrence Moss R, Harrison M,Skarsgard E. Rational treatment of empyema in children. Arch Surg.2000;135:907–912
1740 EMPYEMAS IN CHILDREN at UNIV OF CHICAGO on May 29, 2013pediatrics.aappublications.orgDownloaded from

2004;113;1735PediatricsL. Kaplan and Mary L. Brandt
Karen D. Schultz, Leland L. Fan, Jay Pinsky, Lyssa Ochoa, E. O'Brian Smith, SheldonManagement
The Changing Face of Pleural Empyemas in Children: Epidemiology and
ServicesUpdated Information &
tmlhttp://pediatrics.aappublications.org/content/113/6/1735.full.hincluding high resolution figures, can be found at:
References
tml#ref-list-1http://pediatrics.aappublications.org/content/113/6/1735.full.hat:This article cites 25 articles, 6 of which can be accessed free
Citations
tml#related-urlshttp://pediatrics.aappublications.org/content/113/6/1735.full.hThis article has been cited by 26 HighWire-hosted articles:
Subspecialty Collections
diseasehttp://pediatrics.aappublications.org/cgi/collection/infectious_Infectious Disease & Immunitythe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2004 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at UNIV OF CHICAGO on May 29, 2013pediatrics.aappublications.orgDownloaded from