Embed Size (px)
Citation preview

NOTE
THE CONTRIBUTION OF AN IMAGERY CODE TO VERBAL MEMORY
Roy C. Martin1, Kimford J. Meador1, David W. Loring\ Dawn Bowers2 and Kenneth M. Heilman2
('Department of Neurology, Medical College of Georgia; 2Department of Neurology, University of Florida)
Characterization of hemispheric specialization typically includes a dissociation between verbal and visuospatial memory (e.g., Kimura, 1963; Milner, 1968; Whitehouse, 1981). Patients with left. brain lesions have impairments of verbal memory, while right brain lesion patients have reduced memory for visuospatial material (e.g., De Renzi, Faglioni and Spinnler, 1968; Milner, 1971; Corsi, 1972; Novelly et al., 1984; Ojemann and Dodrill, 1985). Although the right hemisphere plays an ascendent role for encoding visuospatial information, the extent to which the left hemisphere contributes to visuospatial memory remains unknown (Benton, 1979). Further, the left hemisphere is dominant for linguistic processing and verbal memory, but the right hemisphere appears to play a role in certain aspects of normal language function such as coherent narrative integration and appropriate emotional responsiveness (Delis et al., 1983; Wapner, Hamby and Gardner, 1981).
Memory often relies on effective verbal encoding of information, even when information consists of visually presented materials. Memory for verbalizable visual material is facilitated by a left hemisphere mediated verbal encoding process which likely enhances properties of the visual information (De Renzi, 1982). Thus, patients with left hemisphere damage exhibit significant memory deficits on some visual memory tasks (Cermak and Moreines, 1976; Cermak and Tarlow, 1978) compared to right brain-injured patients (De Renzi and Spinnler, 1966; Cermak and Butters, 1976; Cremonini, De Renzi and Faglioni, 1980). Although several studies have found immediate recognition deficits for verbalizable pictures in patients with left hemisphere lesions (Boller and De Renzi, 1967; Goodglass, Denes and Calderon, 1974), other studies examining contributions of a verbal code to visuospatial learning have reported differential hemispheric impairment when employing long-term memory paradigms (De Renzi, Faglioni and Villa, 1977; Cremonini et al., 1980). These results suggest that the imagery memory component increases and the verbal component decreases as a function of time.
Research investigating imagery-mediated verbal learning has demonstrated differential performance patterns among left and right unilateral temporal lobectomy (TL) patients (Jones, 1974; Jones-Gotman and Milner, 1978). When left TL patients employed visual imagery during verbal paired-associates tasks, their performance improved. In contrast, the performance of right TL patients was normal when the verbal learning task could easily be encoded using a verbal code. However, when required to use images as mediators in a verbal-learning task, right TL patients performed significantly worse. These results provide evidence that a dual memory code process exists, with each differentially vulnerable to lesions of either the left or right hemispheres (Paivio, 1984). However, the extent to which visual imagery strategies affect subsequent visuo-spatial memory performance has not been directly examined.
The purpose of the present report was to investigate contributions of verbal and imagery-mediated codes on a language-based spatial/imagery memory task. We employed a series of verbally presented prose passages in a free recall paradigm and compared a patient with a large right hemisphere infarction to healthy, education and age equivalent controls. This
Cortex, (1990) 26, 443-450

444 R.C. Martin and Others
patient was unusual because, in spite of the severity of his stroke, he retained superlative language and verbal memory. If imaginal memory becomes more important over time, the effects of the right hemispheric damage should impair delayed recall of the spatial components of the prose passages, while having less effect on the verbal content of delayed recall. In contrast, immediate recall of verbal and spatial items should be comparable to controls due to the initially greater contribution of the verbal code.
MATERIALS AND METHOD
Case Report
The patient was a 33 year old, right-handed man with 16 years of education who experienced acute onset of right ear pain and perforated right tympanic membrane while scuba diving. Two days later, he developed a left hemiparesis which slowly progressed to flaccid hemiplegia and semicoma. CT scan revealed massive right cerebral infarction in the distribution of the internal carotid artery (See Figure 1). Cerebral angiography showed dissection of the right internal carotid artery with distal embolization. Three weeks later, the patient was tested for the present study. At that time, he was alert and oriented. He exhibited a left homonomous hemianopsia, 3/5 to 415 left hemiparesis, left-sided hyperreflexia, and a left Babinski sign. Language and praxis were normal. Post-infarction IQ measures from the WAIS were: VIQ = 130, PIQ = 101, and FSIQ = 118. He performed in the superior to very superior range on all tests of verbal memory and language-related abilities. For example, on the Rey Auditory Verbal Memory Test, the patient recalled all 15 words after the first presentation and again recalled all 15 after a 20 minute delay. Visuospatial abilities were severely impaired for both construction and perception. Profound neglect was present. Patient initially exibited anosognomia which resolved to anisodiaphoria. At the time of experimental testing, the patient consistently bisected lines to right of midline, and neglected all items in left hemispace on a cancellation task. He had left-sided extinction to tactile and auditory double simultaneous stimulation, and a tendency to shave only the right side of his face. The patient's drawings were severely distorted. Because the patient was originally from England and was living in the Carribean at the time of his stroke, a modified verbal geographic orientation task was administered (Benton, Levin and Van Allen, 1974). The patient performed at less than chance level.
Subjects
Ten healthy right-handed adult males (mean age= 31. 7, range= 24-35) were administered identical prose passage given to the patient. Inclusion criteria required at least 16 years of formal education to approximate patient's estimated pre-morbid intellectual level.
Tests
The ability to recall story content and spatial information was tested through the administration of four prose passages. Each story contained narrative descriptions of various settings in which subjects were told to actively imagine themselves in those settings. Subjects were instructed to remember as many individual details as possible, especially those related to right/left spatial orientation. Spatial properties for each story were in the form of descriptive items being presented either in left or right hemispace (see Appendix).
Each story was approximately 300 words in length, and was broken down into units of verbal information (mean units= 50 per story) tagged to left/right spatial orientations (e.g., "At the first set of doorways, to the right he saw a bedroom decorated in dusty blue with a large canopied bed. A dressing robe was thrown carelessly across the foot of the bed"). Scoring was conducted initially on whether a spatially tagged verbal item was recalled independent of its location. Then, for each of the verbal items recalled, it was determined whether the item was correctly placed to either the left or right side. ,
In the above example, eight verbal units associated with spatial location were scored:
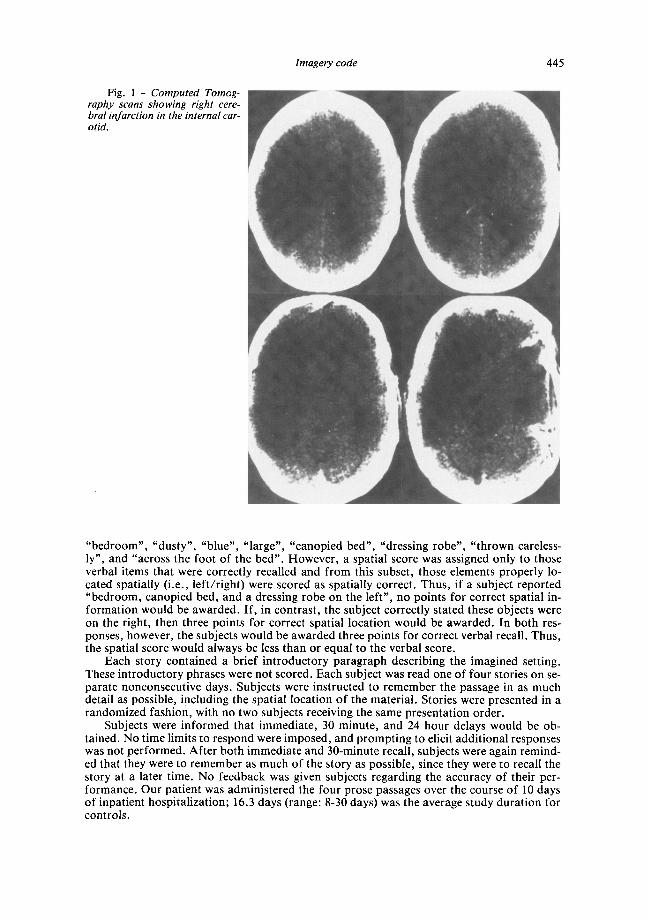
Fig. I - Computed Tomography scans showing right cerebral infarction in the internal carotid.
Imagery code 445
"bedroom", "dusty", "blue", "large", "canopied bed", "dressing robe", "thrown carelessly", and "across the foot of the bed". However, a spatial score was assigned only to those verbal items that were correctly recalled and from this subset, those elements properly located spatially (i.e., left/right) were scored as spatially correct. Thus, if a subject reported "bedroom, canopied bed, and a dressing robe on the left", no points for correct spatial information would be awarded. If, in contrast, the subject correctly stated these objects were on the right, then three points for correct spatial location would be awarded. In both responses, however, the subjects would be awarded three points for correct verbal recall. Thus, the spatial score would always be less than or equal to the verbal score.
Each story contained a brief introductory paragraph describing the imagined setting. These introductory phrases were not scored. Each subject was read one of four stories on separate nonconsecutive days. Subjects were instructed to remember the passage in as much detail as possible, including the spatial location of the material. Stories were presented in a randomized fashion, with no two subjects receiving the same presentation order.
Subjects were informed that immediate, 30 minute, and 24 hour delays would be obtained. No time limits to respond were imposed, and prompting to elicit additional responses was not performed. After both immediate and 30-minute recall, subjects were again reminded that they were to remember as much of the story as possible, since they were to recall the story at a later time. No feedback was given subjects regarding the accuracy of their performance. Our patient was administered the four prose passages over the course of 10 days of inpatient hospitalization; 16.3 days (range: 8-30 days) was the average study duration for controls.
446 R.C. Martin and Others
140 140
120 ..J 120
~ ..J ..J ..J 100 or( 100 or( 0 80
0 80 w w a: a: 60 60
K Patient 40 o Control 40
lmmediate30 minute 24 hour lmmediate30 minute 24 hour
VERBAL RECALL SPATIAL RECALL
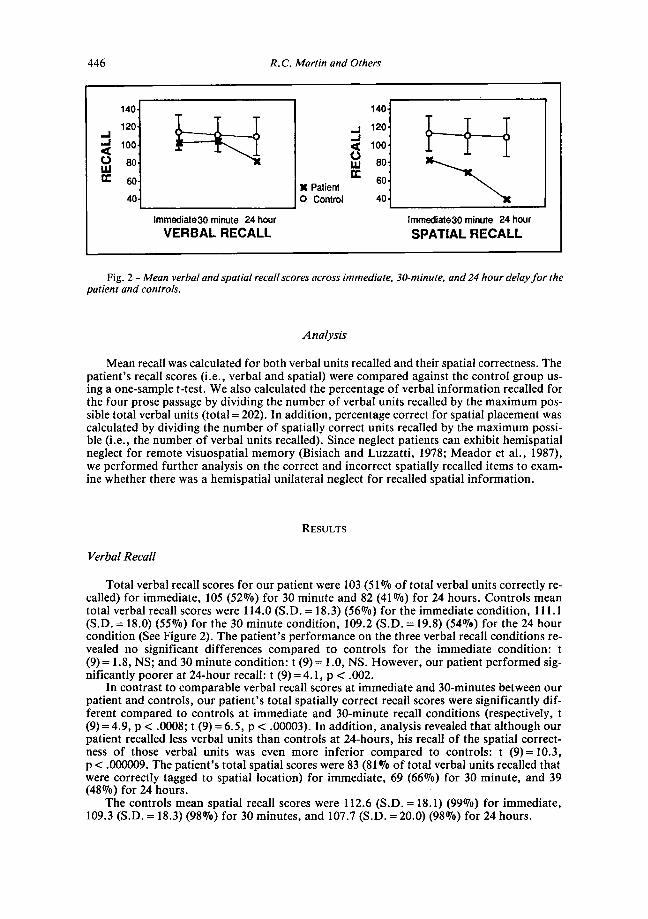
Fig. 2 - Mean verbal and spatial recall scores across immediate, 30-minute, and 24 hour delay for the patient and controls.
Analysis
Mean recall was calculated for both verbal units recalled and their spatial correctness. The patient's recall scores (i.e., verbal and spatial) were compared against the control group using a one-sample t-test. We also calculated the percentage of verbal information recalled for the four prose passage by dividing the number of verbal units recalled by the maximum possible total verbal units (total= 202). In addition, percentage correct for spatial placement was calculated by dividing the number of spatially correct units recalled by the maximum possible (i.e., the number of verbal units recalled). Since neglect patients can exhibit hemispatial neglect for remote visuospatial memory (Bisiach and Luzzatti, 1978; Meador et al., 1987), we performed further analysis on the correct and incorrect spatially recalled items to examine whether there was a hemispatial unilateral neglect for recalled spatial information.
RESULTS
Verbal Recall
Total verbal recall scores for our patient were I 03 (51 OJo of total verbal units correctly recalled) for immediate, 105 (52%) for 30 minute and 82 (41 %) for 24 hours. Controls mean total verbal recall scores were 114.0 (S.D. = 18.3) (56%) for the immediate condition, 111.1 (S.D. = 18.0) (55%) for the 30 minute condition, 109.2(S.D.=19.8) (54%) for the 24 hour condition (See Figure 2). The patient's performance on the three verbal recall conditions revealed no significant differences compared to controls for the immediate condition: t (9) = 1.8, NS; and 30 minute condition: t (9) = 1.0, NS. However, our patient performed significantly poorer at 24-hour recall: t (9) = 4.1, p < .002.
In contrast to comparable verbal recall scores at immediate and 30-minutes between our patient and controls, our patient's total spatially correct recall scores were significantly different compared to controls at immediate and 30-minute recall conditions (respectively, t (9) = 4.9, p < .0008; t (9) = 6.5, p < .00003). In addition, analysis revealed that although our patient recalled less verbal units than controls at 24-hours, his recall of the spatial correctness of those verbal units was even more inferior compared to controls: t (9) = 10.3, p < .000009. The patient's total spatial scores were 83 (81 OJo of total verbal units recalled that were correctly tagged to spatial location) for immediate, 69 (66%) for 30 minute, and 39 (48%) for 24 hours.
The controls mean spatial recall scores were 112.6 (S.D. = 18.1) (99%) for immediate, 109.3 (S.D. = 18.3) (98%) for 30 minutes, and 107. 7 (S.D. = 20.0) (98%) for 24 hours.
Imagery code 447
Comparison of Verbal and Visuospatial recall
To illustrate statistically the disporportional decline in our patient's spatial recall as compared to his verbal recall, we compared verbal/visuospatial ratio scores for our patient to controls. This ratio score was calculated by dividing the percentage of verbal recall by spatial recall to obtain the verbal/visuospatial ratio score for each subject. A repeated measure ANOV A was utilized to compare ratio scores. Analysis revealed a significant time (immediate, 30-minute, 24 hour) x group (patient, controls) interaction, in which our patient's spatial recall declined disproportionately to his verbal recall overtime compared to controls (F = 26.4; d.f. = l, 9; p < .000001).
Unilateral Neglect
No significant differences were found between material recalled in left versus right hemispace for the patient at immediate [t (3) = .53, NS], 30 minute [t (3) = .52, NS], and 24 hour conditions [t (3)= .44, NS]. Similarly, no significant hemispatial differences were found for the control group at immediate [t (9) = .27, NS], 30 minute [t (9) = 1.13, NS], and 24 hour conditions [t (9)= .14, NS].
DISCUSSION
These results suggest that verbal coding is insufficient to adequately consolidate/organize spatial information over time during prose passage recall. Although our patient adequately recalled verbal units on immediate and 30-minute delayed recall, his ability for accurate spatial recall decreased disproportionately over time. The verbal and spatial scores for immediate recall are postulated to result from the patients outstanding verbal memory and language skills that remained intact following right cerebral infarction. However, as the importance of verbal mediation recedes over time, the patient appeared unable to form or retrieve appropriate imaginal components necessary to recall accurately the stories' spatial units. Initially, spatial information may have been encoded directly into linguistic form. Impaired spatial recall over time suggests that structural properties of the information may not have become sufficiently encoded into a spatial imagery system or adequately retrieved from that system. Thus, reliance upon a left hemispheric mediated verbal encoding process may only allow for partial integration of linguistic and visuospatial properties.
These results showed that immediate, 30-minute and 24 hour delayed spatial recall decreased disproportionately compared to controls. Our patients's 24 hour verbal recall score was also lower than controls, suggesting decay of both verbal and visual material over 24 hours. However, spatial memory loss still declined disproportionately. In addition, since the contribution of an imagery code appears to increase over time, its loss may interfere with adequate delayed verbal recall. Therefore, a decreasing reliance upon a verbal memory code over time would result in greater disruption of both verbal and visuospatial delayed memory in our patient. These results are compatible with De Renzi et al. (1981) who investigated the relative contribution of both verbal and visuospatial mediated codes during the course of a visual learning paradigm.
Other lines of evidence indirectly support our patient's failure to encode the spatial properties of the stories. Bisiach and Luzzatti (1978), and Meador et al. (1987) examined remote visuospatial memory in patients with right cerebral infarctions. Their patients exhibited impaired recall for left hemispatial remote visuospatial memories from imagined perspectives of familiar surroundings that were encoded prior to cerebral infarction. In addition to examining verbal and spatial recall in our prose passage, we also examined the possibility that our right brain damaged patient would demonstrate hemispatial neglect for the spatially correct units presented in left hemispace. Our patient did not demonstrate hemispatial neglect for recall of spatial information from the stories, suggesting that he never encoded the information in a visuospatial code. In addition, neuropsychological data indicate that his visual/spatial processing skills were severely impaired. The patient exhibited impaired visual

448 R.C. Martin and Others
constructional deficits as evidenced by inability to adequately copy geometric designs, as well as poor visual spatial perception.
Our results demonstrate significant right hemisphere contribution to imaginal coding in a verbal memory paradigm. However, this does not allow dissociation of interhemispheric for imagery processes (Ehrlichman and Barrett, 1983). Recent conceptualizations regarding imagery system have shifted emphasis towards the hypothesis that imagery is not the exclusive domain of a single hemisphere, but that each hemisphere has specialized imagery functions (Ehrlichman and Barrett, 1983; Farah, 1984). Although a right hemispheric advantage for some types of imagery tasks has been reported (Ratcliff, 1979; Whitehouse, 1981), considerable evidence exists for a left hemisphere contribution to imagery processing (Ehrlichman and Barrett, 1983). Farah (1984) "suggested that the conflicting evidence may be due to a failure to appreciate that there are different components to imagery, each mediated by different neural structures different from those involved in the inspection or transformation of images" (from Corballis and Sergent, 1988, p. 13). Although our results suggest that the influences of a verbal code is more important early in the learning process, and that imagery exerts greater influence over time for auditorially presented verbal material, future reports using a variety of imagery techniques will be necessary to understand each hemisphere's contribution to imagery processing.
ABSTRACT
Free recall for auditorially presented spatial information was examined in a patient with a large right cerebral infarction. Despite normal verbal memory at immediate and 30-minute conditions, the patient exhibited a significant loss in verbal recall at 24 hours and a more severe deficit in the recall of the spatial components of prose passages across all delayed recall conditions. These results suggest that although the verbal code is important early in the learning process, spatial imagery exerts an increasing influence over time. Thus, reliance upon a left hemispheric mediated verbal encoding process may only allow for partial integration of linguistic and visuospatial properties.
Acknowledgements. This study was supported in part by NIA grant KOS AG00314 awarded to KJ. Mand HRS Department of Aging and Adults Services, University of Florida Memory Disorder Clinic, awarded to D.B. We thank Daniel S. Feldman, M.D., and Patricia A. Downs for their assistance with manuscript preparation.
REFERENCES
BENTON, A. L. Visuoperceptive, visuospatial, and visuoconstructive. In K.M. Heilman and E. Valenstein (Eds.), Clinical Neuropsychology. New York: Oxford University Press, 1979, Ch. 8, pp. 186-232.
BENTON, A. L., LEVIN, H. S., and VAN ALLEN, M. W. Geographic orientation in patients with unilateral cerebral disease. Neuropsychologia, 12: 183-191, 1974.
BISIACH, E., and LuzzATTI, C. Unilateral neglect of representational space. Cortex, 14: 129-133, 1978. BOLLER, F., and DE RENZI, E. Relationship between visual memory defects and hemispheric locus of le
sion. Neurology, 17: 1052-1058, 1967. CERMAK, L.S., and BUTTERS, N. The role of language in the memory disorders of brain-damaged pa
tients. Annals ot the New York Academy of Sciences, 280: 857-867, 1976. CERMAK, L.S., and MoREINES, J. Verbal retention deficits in aphasic and amnesic patients. Brain and
Language, 3: 16-27, 1976. CERMAK, L.S., and TARLOW, S. Aphasic and amnesic patients' verbal vs. nonverbal retentive abilities.
Cortex, 14: 32-40, 1978. CoRBALLIS, M.C., and SERGENT, J. Imagery in a commissurotomized patient. Neuropsychologia, 26: 13-
26, 1988. CORSI, P.S. Human memory and the medial temporal lobe of the brain. Unpublished doctoral dissertion,
McGill University, Montreal, 1972. CREMONINI, W., DE RENZI, E., and FAGLIONI, P. Contrasting performance of right and left-hemisphere
patients on short-term and long-term sequential visual memory. Neuropsychologia, 18: 1-9, 1980. DELIS, D.C., WAPNER, w., GARDNER, H., and MOSES, J .A. The contribution of the right hemisphere to
the organization of paragraphs. Cortex, 19: 43-50, 1983.
Imagery code 449
DE RENZI, E. Memory disorders following focal neocortical damage. Philosophical Transactions of the Royal Society of London, B 298: 73-83, 1982.
DE RENZI, E., F AGLIONI, P ., and SPINNLER, H. The performance of patients with unilateral brain damage on face recognition tasks. Cortex, 3: 194-216, 1968.
DE RENZI, E., FAGLIONI, P., PREVIDI, P., SORGATO, P., and VESCOVINI, E. The differential contribution of the verbal code in the course of visual learning: Evidence from hemisphere-damaged patients. Cortex, 17: 447-452, 1981.
DE RENZI, E., FAGLIONI, P., and VILLA, P. Sequential memory for figures in brain-damaged patients. Neuropsychologia, 15: 43-49, 1977.
DE RENZI, E., and SPINNLER, H. The influences of verbal and non-verbal defects on visual memory tasks. Cortex, 2: 322-336, 1966.
EHRLICHMAN, H., and BARRETT, J. Right hemispheric specialization for mental imagery: A review of the evidence. Brain and Cognition, 2: 55-76, 1983.
FARAH, M.J. The neurological basis of mental imagery: A componential analysis. Cognition, 18: 245-272, 1984.
GooDGLASS, H., DENES, G., and CALDERON, M. The absence of covert verbal mediation in aphasia. Cortex, 10: 264-269, 1974.
JONES, M.K. Imagery as a mnemonic aid after left temporal lobectomy: Contrast between material-specific and generalized memory disorders. Neuropsychologia, 12: 21-30, 1974.
JoNES-GOTMAN, M., and MILNER, B. Right temporal-lobe contribution to image-mediated verbal learning. Neuropsychologia, 16: 61-71, 1978.
KIMURA, D. Right temporal-lobe damage. Archives of Neurology, 8: 264-271, 1963. MEADOR, K.J., LORING, D.W., BOWERS, D., and HEILMAN, K.M. Remote memory and neglect syn
drome. Neurology, 37: 522-526, 1987. MILNER, B. Visual recognition and recall after right temporal-lobe excisions in man. Neuropsychologia,
6: 191-210, 1968. MILNER, B. Interhemispheric differences in the localization of psychological processes in man. British
Medical Bulletin, 27: 272-275, 1971. NOVELLY, R.A., AUGUSTINE, E.A., MATTSON, R.H., GLASER, G.H., WILLIAMSON, P.O., SPENCER, 0.0.,
and SPENCER, S.S. Selective memory improvement and impairment in temporal lobectomy for epilepsy. Annals of Neurology, 15: 64-67, 1984.
OJEMANN, G.A., and DODRILL, C.B. Verbal memory deficits after left temporal lobectomy for epilepsy. Journal of Neurosurgery, 62: 101-107, 1985.
PAIVIO, A. The empirical case for dual coding. In J.C. Yuille (Ed.), Imagery, Memory and Cognition: Essay in Honor of Allan Paivio. New Jersey: Lawrence Erlbaum Associates, 1984, Ch. 14, pp. 307-332.
RATCLIFFE, G. Spatial thought, mental rotation and the right cerebral hemisphere. Neuropsychologia, 17: 49-54, 1979.
WAPNER, W., HAMBY, S., and GARDNER, H. The role of the right hemisphere in the apprehension of complex linguistic materials. Brain and Language, 14: 15-33, 1981.
WHITEHOUSE, P.J. Imagery and verbal encoding in left and right hemisphere damaged patients. Brain and Language, 14: 3-15-332, 1981.
David W. Loring, Section of Behavioral Neurology, Department of Neurology, Medical College of Georgia, Augusta, GA 30912-3275, U.S.A.
APPENDIX
Example Story
Introduction
Mr. Holmes arrived at the top of the spiral staircase and gazed down a long hall which had 3 pairs of doorways, one on each side facing a matching doorway across the hall. At the end of the hallway was a dimly lit window in front of which was standing a dark figure in an overcoat. As Mr. Holmes walked slowly down the hall, he never took his eyes off of the man at the far end of the hall, but as he passed each pair of doorways, he paused briefly to glance out of the corner of his eye at the contents of the rooms on each side.
450 R.C. Martin and Others
Scorable contents
At the first set of doorways, to the right he saw a bedroom decorated in dusty blue with a large canopied bed. A dressing robe was thrown carelessly across the foot of the bed. To his left was a sitting room with a large red oriental rug. On the rug was a tobacco pouch with its contents spilled out beside it. From the aroma, Holmes knew that the tobacco was unmistakably a cavendish blend. He moved farther down the hall to the second pair of doorways, never taking his eyes off the figure in the overcoat who he now noticed had his hands concealed. To his right, Holmes saw a office with various papers strewn about the room. To his left was a bathroom with the water still running into an overflowing tub. Holmes moved farther down the hall to the last pair of doorways. This time he gazed first to the left and saw a bedroom decorated in the Queen Ann period. On the floor lay a pearl handled dagger with a crimsonstained blade. To his right was another bedroom and lying face down across the bed was the body of a young man. Holmes slowly walked on and came face to face with the man at the end of the hall.
![Contribution of Borehole Digital Imagery in Core-Log ... · PDF fileSo, digital borehole images (mm-scale) ... of an electrode surrounded by insulation. [B] The Ultrasonic Borehole](https://img.pdfslide.net/doc/110x75/5a793f4a7f8b9aee3b8bf45d/contribution-of-borehole-digital-imagery-in-core-log-digital-borehole-images.jpg)




























