Embed Size (px)
Citation preview

The Current Environment for Hospital Leasing and Financing
March 2012

1
©The Alta Group 2012
TABLE OF CONTENTS
Executive Summary ....................................................................................................... 2
Current Hospital Environment
The Current Situation: Economic and Regulatory ............................................................ 2
Current Size and Scope of the U.S. Hospital Industry ................................................ 3
Current Hospital Operating Environment .................................................................... 5
The Dominant Role of Government ........................................................................... 8
Current Legislative Situation ..................................................................................... 10
Opportunities and Challenges .................................................................................... 11
The Role of Information Technology ......................................................................... 11
Cost Containment Trends ......................................................................................... 12
Forecasts for Medical Equipment Leasing and Financing ....................................... 13
Opportunity ............................................................................................................... 14
Exhibits
Exhibit A-1: Metric Trend by Peer Group .................................................................. 16
Exhibit A-2: Total Operating Profit Margin ................................................................ 17
Exhibit A-3: Days Net Patient Revenue in Accounts Receivable (AR) ...................... 18

2
©The Alta Group 2012
Executive Summary In the 1960s when the modern day equipment leasing industry began to offer non-cancelable, fixed rate, short- and intermediate-term credit products to the commercial sector, a new industry was born. Hospital equipment leasing and financing in the United States has been a mainstay in the larger health services leasing market ever since. Over the next 50 years, the growth and expansion of the national hospital industry outpaced other commercial/industrial sectors. Equipment manufacturers and their captive leasing operations thrived in this sector. Bank-affiliated leasing companies achieved stability and success, and dedicated health care independents prospered and established a permanent presence. It remains a challenge to operate as a lender/lessor in the health care environment. As health care costs have skyrocketed, consuming an ever bigger bite of the GNP, cost controls and government regulations have added complexity to day to day operations. The result is that a successful lender/lessor must have: 1) management personnel who are knowledgeable about the market, 2) an understanding of the complicated regulatory environment, and 3) continued diligence on the part of senior management of the dynamics of the healthcare market. Making fully informed market and credit decisions are of paramount importance if one is to build a portfolio capable of strong performance through industry uncertainty and upheaval. The following study provides an overview of the current hospital environment in the US. The statistics and findings represent the best of the data available from various sources. The dates of the findings from these sources may vary and represent the most current available at the time of this publication. The Current Situation: Economic and Regulatory Background The major economic and regulatory issues that impact today’s leasing and financing environment began in the second half of the 20thcentury and continue in the 21st century. They include rapidly inflating health care costs, affordability, and central government attempts to manage and resolve these problems. This scenario resulted in Congressional approval of Medicare and Medicaid in 1965. In 1973, there was a long series of “Stark legislation” that governed the ethics of physician referral and shaped many aspects of federal medical provider legislation for more than 30 years. In 1985 Medicare shifted to a capitated payment system, allowing only a set reimbursement amount per diagnosis (known as DRGs, or diagnosis-related groups); private health care insurance quickly followed suit. Under this system, Medicare and insurance companies would only reimburse a set amount for each DRG, regardless of other circumstances such as increased cost or new technology. This reimbursement system did not solve the systemic problems,

3
©The Alta Group 2012
and costs continued to escalate. By the 1990s, 16% of Americans were uninsured, mainly because they could not afford the premiums. Currently, the sustainability of both Medicare and employer-based insurance programs are in question and under heated debate. A Medicare Drug Plan (Part D) was approved in 2005, and the Patient Protection and Affordable Care Act was passed in 2010. Current Size and Scope of the U.S. Hospital Industry In its 2009 Annual Survey, the American Hospital Association registered 5,795 hospitals. Of this number, 5,008 were classified as community hospitals. The remaining 787 hospitals are not accessible by the general public and include prison hospitals, college infirmaries, federal government hospitals, non-federal psychiatric hospitals and non-federal long term care hospitals. The 5,008 community hospitals are categorized as follows:
% Segment
58% Non-governmental not-for-profit
22% State or local government
20% Investor-owned, for profit
About 60% of community hospitals are “system hospitals,” which means they may be a multi-hospital institution or a diversified, single hospital system. A multi-hospital system is defined as two or more hospitals owned, leased, sponsored or contract-managed by a central organization. In 2009, community hospitals reported 806,000 staffed (certified) beds and admitted 35,500,000 patients. For the same year, registered hospitals recorded total revenue of approximately $800 billion, with expenses amounting to about $726.7 billion. Hoovers, a Dun & Bradstreet subsidiary, estimates that 30% of the $800 billion was generated by the largest 50 hospitals in the U.S. Statistics for some of the largest hospitals are provided below:
Name Type 2009 Revenues
Kaiser Permanente West coast-based integrated hospital and HMO system
$42 billion
Hospital Corporation of America/HCA
Nationwide, publicly traded proprietary system
$31 billion
Methodist Healthcare Tennessee-based non-profit hospital system
$27 billion
Ascension Health Non-profit hospital system $14 billion

4
©The Alta Group 2012
For 2011, IbisWorld, an independent market research company, estimates relatively flat total revenue of $757 billion, comprised of the products and services noted below:
The Centers for Medicare and Medicaid Services (CMS), the federal agency in charge of administration for Medicare and Medicaid, reports the following breakdown of hospital revenue sources in 2010:
Health Management Partners LLC (HMP), a hospital consulting firm, provides annual hospital metric trends on various peer groups within the hospital industry. This includes investor-owned, not-for-profit, state and local government-owned, children’s, and major teaching hospitals. As expected, the investor-owned total profit margin percentages (including operating margins) and Days Net Patient Revenue in AR (number of days it takes to collect a receivable/liquidity) tend to out-perform the other peer groups. Detailed data is provided in Appendix A.

5
©The Alta Group 2012
CURRENT HOSPITAL OPERATING ENVIRONMENT Not surprisingly, the HMP metric trends for 2008 and 2009 reveal the impact of the Great Recession and the 2009 start of a mixed recovery: Total profit margins for all peer groups dropped 50%. Currently, the industry is still in recovery mode, as demonstrated by the following member statistics recorded by the American Hospital Association in the first quarter of 2010:
2010 Metric % of AHA Members
Lower overall patient volume 70%
Drops in elective procedure volume, as patients deferred or avoided medical care
>70%
Increases in bad debt and uncompensated care
87%
Increased number of patients covered by Medicaid and other public assistance programs
65%
Lower operating margins 75%
Dropping non-operating income, normally dominated by investment income and charitable donations
50%
Reduced access to capital 44%
Reacting to the widespread financial crisis and deep recession, many hospital management teams implemented cost control strategies to stabilize and improve financial performance despite flat volume trends and slow revenue growth. Most in the industry are intensely managing their payables and cash. Many have made significant changes to deal with the recession, including:
Cutting administrative costs: 76%
Delaying capital investments: 73%
Reducing staff: 53%
Cutting services: 25%
Divesting assets: 8%
Merging with another institution: 3%

6
©The Alta Group 2012
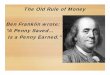
PayNet Statistics: PayNet’s recent data supports the mixed recovery from the recession. Originations trends for the health care equipment type are shown in Figure 1 below. Figure 1
10099
101
107
114115
122
125
133132
123
113
95
91
89
86
90 9191 92 91
80
90
100
110
120
130
140
150
4Q06 1Q07 2Q07 3Q07 4Q07 1Q08 2Q08 3Q08 4Q08 1Q09 2Q09 3Q09 4Q09 1Q10 2Q10 3Q10 4Q10 1Q11 2Q11 3Q11 4Q11
In
de
x 4
Q0
6 =
1
00
Ba
se
d o
n ro
llin
g 1
2 m
on
th
p
erio
ds
Healthcare Originations Indicator
PayNet, Inc.
Figure 1 presents Originations for the Health Care segment. Note health care originations have failed to fully recover from the impact of the recent recession. These trends are unlike equipment leasing for all equipment types, which have shown a healthy recovery. As of December 2011, originations for all equipment types expanded 19% over the prior year according to the Thomson Reuters/PayNet Small Business Lending Index. This marked the 17th monthly consecutive double-digit expansion of equipment leasing. Seasonally adjusted expansion was healthy as well, as December originations grew 5% over November.

7
©The Alta Group 2012
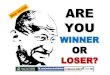
Credit risk for health care as measured by 30 day delinquency shows the level of risk and the risk spectrum of industry players. In Figure 2, the yellow line illustrates the average of the risk spectrum for lenders to the healthcare industry. Figure 2:
PayNet, Inc.
Lenders span a broad range of risk, from the high risk lenders in red to the low risk lenders in green. Note the spread between high risk and low risk lenders narrows during good economic times. It is clear that playing in the high risk space magnifies risk during recessions, as can be seen from the gap that developed between the red and green in 2009. In short, credit risk does matter and companies need to ensure they are paid for the credit risk they are taking.

8
©The Alta Group 2012
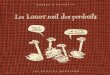
Health care default rates in Figure 3 reinforce the historical attractiveness of this sector. However, according to PayNet’s leading default indicator, defaults of health care providers are forecast to increase by the most of all major equipment groups in 2012. Figure 3
PayNet, Inc.
Defaults on health care equipment are projected to rise to 2.3% by year-end. This represents a 15% increase in defaults of health care deals in 2012. However, even with this latest jump in defaults, health care deals offer some of the lowest defaults of all sectors during times of economic stress. During the latest recession health care deals remained one of the lowest defaults along with the agriculture sector. Given decent pricing, health care deals represent a profitable asset during times of economic stress. The Dominant Role of Government The history of the hospital industry in the second half of the 20th and continuing in the 21st century has been dominated by central government policy. Industry veterans following this heavily regulated industry watch Congress with a wary eye. Examples of government regulation include:
Balanced Budget Act (1997): Following a decade of 10+% annual increases in Medicare spending and out-of-control annual deficits, Congress passed this legislation in 1997.The intention was to balance the federal budget by 2002. To achieve this, Medicare reimbursement levels were severely cut. The government’s Central Budget Office (CBO) originally estimated that, through 2002, Medicare claims reimbursement would be reduced by $112 billion, and hospital inpatient and outpatient payments would be reduced by $44 billion. The industry was significantly impacted in 1998 as perennially profitable

9
©The Alta Group 2012
teaching hospitals lost millions of dollars due to these reductions. Looking backward, the CBO estimated that the act “over shot” the projected cuts by at least $75 billion. With Medicare spending representing 21% of total health care dollars, few medical disciplines were immune from the unintended severity of the cuts. Congress felt the backlash from providers and consumers and eventually restored some reimbursement rates. Deficit Reduction Act (2005): Similarly, the 2005 Deficit Reduction Act (DRA) again targeted the out-of-control growth of Medicare expenditures. Among the significant cuts, Congress seemed to pick winners and losers in the imaging businesses. They approved back-to-back 25% cuts in reimbursement rates for 2006 and 2007 for Outpatient Imaging Centers (OICs) operated principally by investor physicians. Claiming to “level the playing field,” Congress also lowered OIC reimbursement levels to hospital radiology departments, ignoring the fact that non-profit, tax-exempt, charitable donation-accepting competitors operated most of these centers. The DRA has been the death knell for ambulatory OICs, which comprised some 2,000 businesses generating an estimated $10 billion annually. Many were sold to local hospitals seeking to acquire outpatient radiology centers; others were consolidated with bigger, stronger regional operators who frequently operate with larger integrated hospital systems. Many smaller, weaker OICs failed, wreaking havoc on medical equipment lessors targeting this market. Patient Protection and Affordable Care Act (PPACA) (2010): The passage, in 2010, of the controversial PPACA, commonly known as “Obamacare,” carried with it a dramatic shift in health care provisions for all Americans.
PPACA’s key controversial provisions:
-Mandates, beginning in 2014, that everyone under 65 have medical insurance. This will impact approximately 32 million Americans who are currently uninsured -Creates an Independent Payment Advisory Board, starting in 2015, that will set reimbursement -Projects significant cost cutting for Medicare and Medicaid starting in 2015 -Expands Medicaid with revised definitions of income limitations, increasing eligibility to as many as 17 million uninsured Americans, while ultimately reducing funding for the newly eligible.

10
©The Alta Group 2012
Current Legislative Situation A newly invigorated Centers for Medicare and Medicaid Services (CMS) federal agency, administrator for Medicare and Medicaid, is studying perceived loopholes in both Stark legislation and Medicare/Medicaid regulations. The government wants to prohibit “block leasing” arrangements, in which an independent diagnostic testing facility (IDTF) sub-leases its operations to another individual or organization, sharing space, equipment and/or staff. This move targets hospital outsourcing (radiology, emergency room, etc.) and OICs in particular. “Per click” (per use) leases are also on the firing line. Current Stark legislation allows per-click service or lease payments for personal services, space or equipment leases as long as the per-unit charge is fair market value and does not change during the term of the agreement. Accordingly, a physician is permitted to lease a piece of equipment to a hospital at “fair market value” without jeopardizing his patient referral privileges with that hospital. “Not good enough,” CMS maintains. “Such arrangements are inherently susceptible to abuse.” “Under arrangements” between a physician-owned intermediary entity and a hospital or other Medicare certified provider are also targeted. In this scenario, a piece of equipment, owned by the intermediary entity, is leased to the hospital. CMS is considering demanding that the physicians divest themselves of equity in the intermediary entity, or associated Medicare billing will be prohibited. As the independent imaging market is being bought out by hospitals, there are going to be many transactions that will require restructuring and refinancing. The regulatory environment continues to be highly volatile. In late March 2012 the Supreme Court is set to hear the states’ challenge to the “individual mandate” under the Patient Protection and Affordable Care Act (PPACA), the recent major health care reform bill passed by Congress. The outcome will be closely watched and many believe the elimination of the individual mandate will doom the entire PPACA. The failure of the Congressional Super Committee to come to consensus on the $1.2 billion deficit reduction plan in 2011 now forces specific reductions to occur beginning in 2013 thru “sequestration” (arbitrary reductions). Unfortunately the reductions, as laid out by last summer’s Budget Control Act, require specific reductions in entitlement programs as well as the military. The direct impact will be to reduce funding for Medicare by $123 billion over the next ten years. This reduction is separate from any reductions planned for the PPACA. It is expected to have an impact on all types of health care providers to include hospitals, doctors, outpatient providers, home health providers, Medicare part D, Group Plans, and skilled nursing.

11
©The Alta Group 2012
OPPORTUNITIES AND CHALLENGES Rising bad debt, uncompensated care costs and the other negative economic impacts discussed above are due to a weak economy and high levels of unemployment. The result is an increased number of uninsured citizens, including a large segment of the working or retired population who cannot afford today’s high health care fees. The impacted portion of the population is likely deferring or avoiding the doctor or hospital as much as possible. A compounding factor is the capital markets, which remain unengaged and withdrawn from many of their traditional markets, including the health care space. Realistically, the outlook for the health care industry remains uncertain unless there is a national political resolve to implement significant changes to stabilize the business and economics of health care. Many feel that market forces are the best regulators to sort this out. It is likely that, wherever possible, health care providers will continue to defer capital expenditures and table other business initiatives until the uncertainties diminish. They are waiting for a stronger economy and a clearer understanding of the impacts of new federal health care reform legislation. The Role of Information Technology The area of information technology (IT) is included in the numerous examples of recent neglect and/or under-investment by the health care provider community. This situation is changing as the industry scrambles to invest in required information technology, incentivized by available federal subsidies of $27.4B provided in the American Recovery and Reinvestment Act (ARRA) and potential penalties for non-compliance. Vendors serving the industry now consider these shortcomings an opportunity. They expect a considerable positive, spill-over effect once information technology gains a significant foothold in the industry. Many industry observers believe the potential for improved productivity is almost unlimited. The implementation of electronic health records (EHR) alone is estimated to result in reductions of between $50 billion and $200 billion annually. The Medicare Electronic Health Record (EHR) Incentive Program fuels these savings. This federal program provides incentives for early conversion from paper records and, as of 2015, will issue penalties in the form of Medicare disbursement cuts. As previously mentioned, the program was authorized under the American Recovery and Reinvestment Act of 2009 and encourages “eligible hospitals and eligible professionals to acquire and utilize certified EHR technology (certified by CMS) in ways that can be measured significantly in quality and in quantity.”

12
©The Alta Group 2012
The 2012 industry-wide scramble to invest in required information technology is complicated by reduced access to credit and capital plus the additional continuing issue of financing for intangibles. Many hospitals are focused on qualifying under the new “meaningful (technology) user certification” established by the U.S. Department of Health and Human Services (HHS). Implemented in the American Recovery and Reinvestment Act of 2009 as a separate incentive from those offered in the EHR Incentive Program, this certification is necessary to receive federal incentive bonuses and avoid Health Care Finance Administration penalties that have been effective since 2011. Cost Containment Trends More than ever, hospitals and third party payers (including the government and private insurers) are concentrating on cost containment. The following list summarizes current trends:
Increased M&A activity:
Increased M&A activity: There has been a flurry of merger and consolidation
activity. In 2011, a total of $227.4 billion was committed to financing health care merger, acquisition and takeover activity, representing an 11 percent increase over the $205.6 billion spent in 2010, according to a new report from Irving Levin Associates, Inc.
In its “Health Care M&A Report,” Irving Levin Associates notes that based on dollars committed to M&A activity, 2011 is the fourth-largest year of the past 10 years. In terms of deals announced, 2011 saw a total of 980 transactions in 13 sectors of the health care industry, a 3 percent decrease from the 1,007 deals in 2010. However, deal volume is expected to increase to 1,000 and more as new information, such as annual 10-K filings, brings more transactions to light. The four sectors posting the most notable growth in 2011 were hospitals, long-term
care, managed care and physician medical groups. Almost 60% of this activity involved hospitals.
Insurers leading M&A activity: Insurers are the most active seekers of hospital and provider group acquisitions.
Renewed emphasis on reducing costly re-admissions: For a long time, the industry has been concerned about shortening hospital stays and reducing re-admissions. However, there is now a renewed emphasis, because Medicare announced that, as of October 2012, it will no longer pay claims involving “preventable” re-admissions. Currently one out of five elderly patients who is discharged from the hospital is later re-admitted to continue original care. New studies reveal that a number of factors can help reduce these returns, including better use of home health services after hospitalization, heightened patient engagement and the involvement of nursing personnel in planning post-discharge transitional care.

13
©The Alta Group 2012
Accountable Care Organizations (ACOs): These practices include paying providers on patient treatment outcomes rather than care. Currently, there is a great deal of interest in transitioning hospitals to accountable care organizations, although legal challenges to this form of organization may dampen interest.
Comparative Effectiveness Research: This is a controversial approach that applies a time-and-motion study analysis to doctors and other caregivers. The information is then correlated to the quality of patient outcomes. Medical professionals are exerting considerable pushback to this approach.
FORECASTS FOR MEDICAL EQUIPMENT LEASING AND FINANCING Global Industry Analysts Inc. (GIA) estimates that 35-40% of medical equipment in the U.S. is leased. Based on that estimate, medical equipment leasing represents a market opportunity ranging from $133 to $200 billion annually. Medical equipment is the fourth largest category of capital asset investment in the United States, behind software, computers/peripherals and communication equipment. It dwarfs other categories including trucks, trailers, busses, aircraft, rail and marine. Its share of the Gross Domestic Product (GDP) has increased steadily for 51 years since 1960 when it was 5%. CMS estimates that total U.S. health care expenditures in 2010 were approximately $2.8 trillion (17.2% of GDP). CMS forecasts an increase to $4.5 trillion (18.5% of GDP) in 2019. This represents an 80% increase and an average annual growth rate of 8.9%. 2008 health care expenditures (latest year for which data is available) were allocated as follows:
Spending Category %
Hospital care 31%
Research, home health care, over-the-counter medicines, public health and medical equipment*
25%
Physicians and clinical 21%
Prescription drugs 10%
Program administration and related costs 7%
Nursing care 6%
*includes over $500 billion of medical equipment

14
©The Alta Group 2012
The Equipment Leasing and Finance Foundation predicted that the increasing demand for health care services by an aging population, coupled with ever more limited public resources, will positively influence medical equipment expenditures through 2030. The conflicting demands will place tremendous pressure—and a premium—on improved productivity. A wide variety of technology applications will be available to assist in productivity improvements, and a newly receptive and focused health care business sector will adopt a best-practices approach. Many applications will involve investment in cost-saving or labor-saving capital assets that represent significant opportunity for equipment leasing. Opportunity The hospital equipment leasing and financing business represents one of the largest equipment finance opportunities currently available. In spite of the headwinds, the trends and expectations continue to be positive, driven by demographics and the environment. However, it is not without major risks. At a minimum, conducting business in this market requires specific industry expertise, constant monitoring of market dynamics, a strong and disciplined underwriting culture and capability, and experienced senior management.

15
©The Alta Group 2012
The Alta Group is the equipment leasing and finance industry’s preeminent global consultancy, offering clients the unique combination of experience, expertise and executable counsel. Alta’s more than 90 executives worldwide have held senior management positions in public and private equipment leasing companies, manufacturers, banks and other financial services institutions. The Alta Group’s major practice areas include alternative energy financing, captive & vendor programs, government financing, health care financing, legal support services, management consulting, mergers & acquisitions, and professional development. The firm is observing its 20th anniversary. To learn more, please visit www.thealtagroup.com. PAYNET is a data analytics firm providing information on small business credit to increase access to capital, produce economic growth and jobs and significantly reduce the cost of doing business. We collect and track data on small business loans from hundreds of US and Canadian lenders each month turning it into actionable risk intelligence and market insight. Our proprietary database is the richest and largest collection of small business loans and leases encompassing more than $900 billion on over 19 million contracts.

16
©The Alta Group 2012
Exhibit A-1
Source: Hospital Management Partners, LLC October 2010

17
©The Alta Group 2012
Exhibit A-2
Source: Hospital Management Partners, LLC October 2010

18
©The Alta Group 2012
Exhibit A-3
Source: Hospital Management Partners, LLC October 2010