Embed Size (px)
Citation preview

ORIGINAL RESEARCH
The dissonant care management of illicit drug users in medical wards,
the views of nurses and patients: a grounded theory study
Rob Monks, Annie Topping & Rob Newell
Accepted for publication 2 June 2012
Correspondence to: R. Monks:
e-mail: [email protected]
Rob Monks BSc PhD RGN
Senior Lecturer
School of Health, University of Central
Lancashire, Preston, UK
Annie Topping BSc PhD RGN
Professor, Director
Centre for Health and Social Care Research,
University of Huddersfield, UK
Rob Newell BSc PhD RGN
Professor, Associate Dean
Nursing Research & Knowledge Transfer,
University of Bradford, UK
MONKS R . , TOPP ING A . & NEWELL R . ( 2 0 1 2 ) The dissonant care management
of illicit drug users in medical wards, the views of nurses and patients: a grounded
theory study. Journal of Advanced Nursing 00(0), 000–000. doi: 10.1111/j.1365-
2648.2012.06088.x.
AbstractAims. The aim of this study was to explore how registered nurses manage and
deliver care to patients admitted to medical wards and Medical Assessment Units
with complications of drug use and to elicit the experiences and views of those
receiving that care.
Background. Illicit drug use is a major public health problem worldwide. The
physical complications of problem drug use often result in admission to medical
wards. Registered nurses working in these settings have been reported as
possessing negative attitudes towards patients who use illicit drugs and lacking
preparation to provide problem drug use–related care needs.
Design. Grounded theory.
Methods. A grounded theory approach was used to collect and analyse 41 semi-
structured interviews. Data collection and analysis were undertaken in nine
medical wards in the Northwest of England in 2008. A combination of purposive
and theoretical sampling was adopted to recruit registered nurses (n = 29) and
medical ward patients (n = 12) admitted for physical complications of problem
drug use. Data were subjected to constant comparative analysis.
Findings. Two sub-categories emerged: ‘Lack of knowledge to care’ and ‘Distrust
and detachment’ and these formed the core category ‘Dissonant care’. The
combination of lack of educational preparation, negative attitudes and experience
of conflict, aggression, and untrustworthiness appeared to affect negatively the
nurse–patient relationship.
Conclusions. This study illuminated interplay of factors that complicated the
delivery of care. The complexity of caring for patients who are pre-judged
negatively by nurses appears to engender dissonance and disparities in care
delivery. Better education and training, coupled with role support about problem
drug use may reduce conflict, disruption, and violence and facilitate competent
care for these patients.
Keywords: emotional labour, grounded theory, medical wards, nurse–patient
relationship, problem drug use, social judgement, social reciprocity
© 2012 Blackwell Publishing Ltd 1
JAN JOURNAL OF ADVANCED NURSING

Introduction
Despite the many initiatives to curb drug use, the increasing
rates and range of illicit drug consumption remain a global
problem (EMCDDA 2010). The United Nations Office on
Drugs and Crime [UNODC] suggests that ‘at the core of
drug consumption lie ‘problem drug users’ (PDUs), those
who inject drugs and/or are considered dependent, facing
serious social and health consequences as a result’
(UNODC 2010, p. 16). Many national economies are cur-
rently implementing major financial restraint measures and
those seen as undeserving face an even greater chance of
exclusion (Chan et al. 2008, Hill 2010). Services for drug
users are increasingly threatened by budget cuts (EMCDDA
2010). Consequently, more people who use illicit drugs
may access non-specialist acute hospital services with acute,
possibly life-threatening health problems, as more specialist
services become unavailable (UNODC 2010).
In many countries, like the UK, the price of most illicit
drugs is decreasing while availability and purity is increasing
(UK Focal Point 2004, EMCDDA 2005, 2009). Price and
availability have long been associated with increasing levels
of dependency in populations. Femoral abscesses, cellulitis,
deep vein thrombosis (DVT), and overdose are common
physical complications that often bring PDUs, particularly
those injecting, into contact with acute care services leading
to unplanned admission to Accident & Emergency Depart-
ments (A&E), Medical Admission Units (MAUs), and ulti-
mately medical wards. Emergency admissions through A&
E have increased in the UK as have the number of inpatient
beds. MAUs were introduced to improve throughput,
quality of care, and length of stay. They act as observation
centres for short-term admissions and form part of the filter-
ing process where investigations, testing and imaging, and
urgent treatment are instigated. Most have a 24- to 48-hour
length of stay rule (Cooke et al. 2003).
Physical complications tend to present at the most chal-
lenging stage of a drug-using career. They occur when ‘drug
use is no longer controlled or undertaken for recreational
purposes and where drugs have become a more essential
element of an individual’s life’ (Godfrey et al. 2002, p. 9).
In the UK on admission to hospital, these individuals will
be cared for by registered nurses (RNs) who receive little, if
any, educational preparation about illicit drug use and
addiction (Heyes 2002, Harling et al. 2006, Rassool &
Salman 2008). The Nursing and Midwifery Council
(NMC), the UK professional regulatory, and statutory body
responsible for both registration and quality assurance of
programmes preparing nurses for registration list a range of
standards of proficiency for the four branches (adult, child,
learning disabilities, and mental health) pre-registration
nursing education (See Table 1). These relate to broad
issues rather than specific curriculum uniform content
(Rassool 2008) with the consequence that illicit drug use
receives little attention in the adult nurse curricula (Harling
& Turner 2012). Hence, many adult branch RNs in the UK
are likely to be ill prepared to manage and deliver compe-
tent care to PDUs in acute care settings such as medical
wards and medical admission units.
Background
High bed occupancy, rapid patient throughput, high depen-
dence of patients, and increasing use of technology make
MAUs and medical wards challenging work environments.
Patients with diverse conditions and needs, including those
with acute life-threatening illnesses and those requiring
resource intensive care, are admitted to acute medical ward
settings. A consequence of high activity levels is the prioriti-
zation of patients and related needs. PDUs are often judge
as problematic, difficult to manage, demanding, and disrup-
tive and may be seen as less of a priority (McLaughlin et al.
2000, Happell & Taylor 2001, Boyle et al. 2010). Certain
behaviours may be interpreted by RNs as drug-seeking and
lead to symptoms being ignored or interpreted negatively.
For example, reports of severe pain may be interpreted as a
ploy to receive, or increase, dosage of prescribed methadone
or analgesia (Morrison et al. 2000). Methadone dosage and
non-compliance with acceptable patterns of patient behav-
iour may also create tensions. These conflicts may adversely
affect the smooth running of the clinical environment.
Cumulatively, all these factors may contribute to reinforc-
ing any previously held attitudes leading to loss of trust
between patient and caregiver. In effect, the patient is char-
acterized as unable or unwilling to enter into an appropri-
ate reciprocal exchange relationship with their healthcare
provider (Chan et al. 2008).
Table 1 Standards of proficiency.
Competency framework Five essential skills clusters
Professional values Care, compassion, and
communication
Communication and interpersonal
skills
Medicines management
Nursing practice and decision-
making
Organizational aspects of care
Leadership, management, and
team working
Infection prevention and
control
Nutrition and fluid
management
2 © 2012 Blackwell Publishing Ltd
R. Monks et al.

Attitudes to drug users have been studied across a range
of health professionals including RNs (Carroll 1995, 1996,
Chan et al. 2008); general practitioners (Deehan et al.
1997); healthcare staff generally (McLaughlin et al. 2000,
Happell & Taylor 2001, Boyle et al. 2010); and forensic
nurses (Foster & Onyeukwu 2003). Most of these studies
have focused on determining the dimensions and inherent
contradictions in attitudes held rather than examining
the effect attitudes have on the patient experience of
those with a history of problem drug use in acute hospital
contexts.
Given the unplanned nature of admission to acute ser-
vices, the complex interplay between psychological depen-
dence and lifestyle can create a crisis for the individual.
Inpatients do not normally have access to the drugs that
service dependence and PDUs on admission frequently
experience withdrawal symptoms. This leads them to
demand drugs or leave the ward to ‘score’ drugs to service
their dependence. The combination of negative attitudes
and limited education may produce limited drug misuse
competency in RNs and contribute to a poor care experi-
ence for service users (Happell & Taylor 2001, Rassool &
Rawaf 2008). The rationale underlying this study was to
explore the experiences of RNs and patients to understand
the complex interplay between knowledge and attitudes
and its perceived effect on care delivery better.
The study
Aim
This study aimed to explore how RNs manage and deliver
care to patients admitted to medical wards and MAUs with
complications of drug use and to elicit the experiences and
views of those receiving that care.
Design
A grounded theory approach specifically the techniques and
procedures described by Strauss and Corbin (1998) was
used to direct data collection and analysis including con-
stant comparison, theoretical sampling, open, axial, and
selective coding of the data.
Sample and participants
Purposive sampling was used initially to recruit RNs
(n = 29) working in MAUs and Medical Wards in a large
NHS Acute Hospital in North West England in 2008.
Nurses with different biographical details were recruited to
the study (Table 2). As data collection and analysis pro-
gressed, issues that emerged in the interviews that contrib-
uted developing categories directed theoretical sampling.
For example, most nurse participants in this study
expressed negative views of PDUs. During data collection,
several RN participants identified other RNs (n = 3) who
were ‘known’ in the organization for holding more positive
attitudes towards PDUs. These RNs were actively recruited
as a theoretical sample (Strauss & Corbin 1998) to inform
developing tentative assumptions. Convenience sampling
was used to recruit the patient participants who used illicit
drugs (n = 12). RNs working in MAUs and medical wards
initially approached patients admitted with PDU and fol-
lowed a recruitment schedule (Table 3).
Data collection
Semi-structured interviews (minimum 25; maximum
105 minutes) were undertaken. These were audio recorded
Table 2 Biographical details of the nurse participants.
Interviewee no Age Sex
No of years
experience
Type of
nurse
Interview 1 34 Male 9 RN
Interview 2 50 Male 20 RN
Interview 3 30 Female 0·4 RN
Interview 4 50 Female 21 RN
Interview 5 40 Female 12 RN
Interview 6 23 Male 0·4 RN
Interview 7 30 Female 5 RN
Interview 8 50 Female 22 RN
Interview 9 22 Female 2 RN
Interview 10 30 Female 10·5 RN
Interview 11 30 Female 6 RN
Interview 12 30 Female 2 RN
Interview 13 30 Female 0·4 RN
Interview 14 40 Female 19 RN
Interview 15 30 Female 6 NA
Interview 16 40 Female 0·6 RN/RMN
Interview 17 22 Female 0·6 RN
Interview 18 40 Female 10 RN
Interview 19 41 Female 20 RN
Interview 20 30 Female 10 RN
Interview 21 30 Female 6 RN
Interview 22 30 Male 6 RN/RMN
Interview 23 21 Female 0·6 RN
Interview 24 50 Female 16 RN
Interview 25 34 Female 6 RN
Interview 26 23 Female 2 RN
Interview 27 42 Female 20 RN
Interview 28 22 Female 0·6 RN
Interview 29 30 Female 5 RN
RN, Registered Nurse; RMN, Registered Mental Nurse.
© 2012 Blackwell Publishing Ltd 3
JAN: ORIGINAL RESEARCH Caring for problem drug users in medical wards

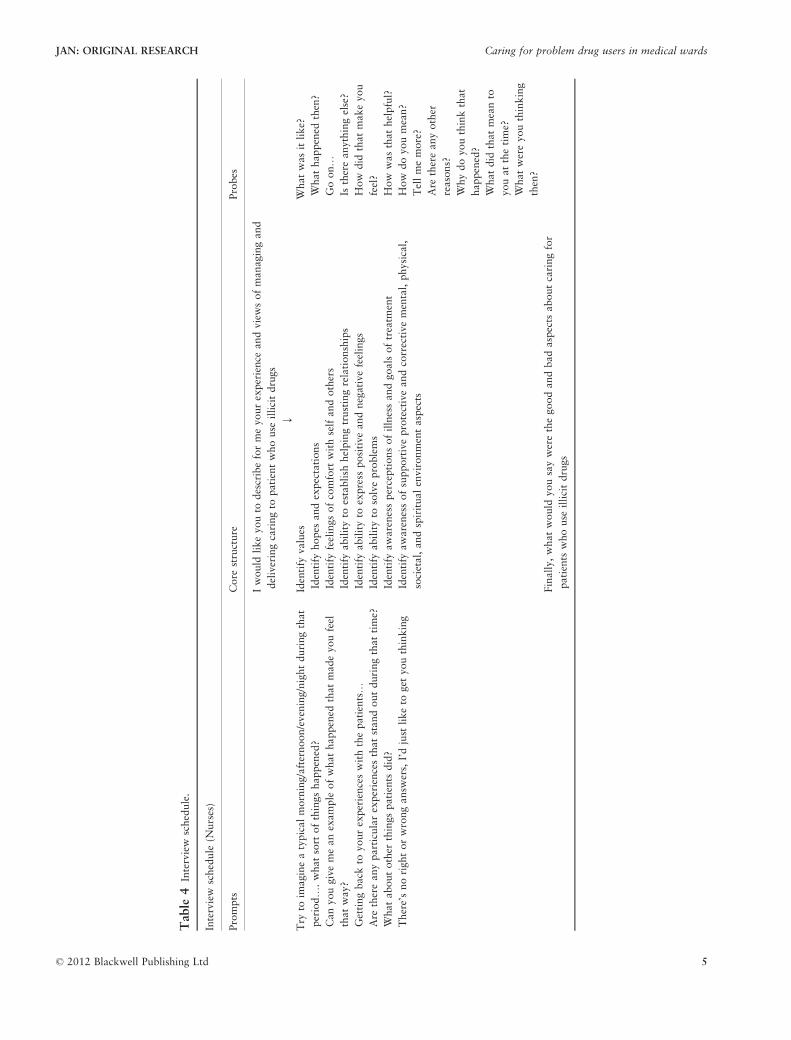
and transcribed prior to analysis. The initial interviews with
RNs began with a request to describe their experiences of
delivering and managing care for patients who were PDUs.
A range of prompts and probes were used in the interview
schedule (Table 4). Patient participants were asked similar
issues about their experience of care delivery in the context
of the medical ward. As conceptual categories began to
emerge from the use of constant comparison, the interview
questions became more focussed. All the nurses interviewed
had been involved in the delivery of direct care to the
patient participants.
Ethical issues
Research Ethics Committee approval was obtained from a
National Health Service (NHS) Local Research Ethics Com-
mittee (LREC) and the University Ethics Committee. Local
governance approval was obtained from the NHS Trust
prior to negotiating access to RNs through unit managers.
Permission to access to the target patient population was
negotiated through the admitting medical consultants and
RNs responsible for their care.
Data analysis
Data analysis was undertaken concurrently with sampling
and data collection. Contemporaneous field notes were kept
to inform analysis and subsequent data collection. Both
transcripts and field notes were analysed manually and sup-
ported with computer-assisted qualitative data analysing
software QSR NVivo 1·3 (Richards 2000). Initially, the
transcripts were examined in detail using memo cards and
different coloured pens for coding. Open coding was used
where sections of data were allocated to tentative categories
that began to form (Strauss & Corbin 1998). As the volume
of data increased, NVivo software was used to manage and
support data handling. This assisted the close detailed anal-
ysis and apportionment of data to the emerging categories.
The properties and dimensions of each category, axial cod-
ing, were explored by comparing how each coded section
of data added to the developing acumen. Data collection
was discontinued when no new properties emerged from
the interviews. As data saturation became evident, selective
coding was undertaken. This process involved integrating
and refining the theory.
Rigour of the study
Several measures were undertaken to enhance the trustwor-
thiness of the data (Denzin & Lincoln 2003). Throughout
data collection and analysis, theoretical and reflexive field
notes were maintained to provide a contemporaneous
account of assumptions, potential biases, and theoretical
explanations. Interview transcripts, where possible, were
returned to the nurse participants to check for accuracy;
this was not possible with the patient participants. No RN
participants chose to amend their account; this was
assumed to indicate accuracy; however, comments were
received about the differences between aural and tran-
scribed accounts. For example, as one RN participant
responded: ‘my comments seem more stark when in a writ-
ten format’. Finally, preliminary findings were presented to
nurse experts in the field and medical ward nurses for feed-
back and as peer review to assess goodness of fit of catego-
rization and overall congruence of the conceptual findings.
Results
Sample characteristics
The RN participants recruited to this study represented a
range of ages (21–58 years), gender (24 females; 5 males)
and experience since qualification (4 months–37 years).
Educational qualifications of the nurses ranged from certifi-
cate level (equivalent to 1 year of undergraduate education)
through Master of Science. All were registered as adult
branch RNs with the Nursing and Midwifery Council
(NMC). All the patient participants reported a history of
poly-drug use including cannabis, amphetamine, ecstasy,
cocaine, crack cocaine, and heroin. All patient participants
reported injecting heroin prior to admission. All were
admitted for acute complications of their drug use and by
definition were ‘problem drug users’ (UNODC 2010,
p. 16).
‘Dissonant care management/delivery’ emerged as the
core category to explain the complexity of the nurse–patient
Table 3 Recruitment process.
Patient admitted to ward declares use of an illicit drug(s)
↓
Inform patient about research study
↓
Give letter of invitation to study + patient information sheet
↓
If patient agrees to participate in study inform researcher (RM,
Tel)
↓
Researcher will come to ward to give further information about
the study, consent the participant, and set up convenient time
for interview
4 © 2012 Blackwell Publishing Ltd
R. Monks et al.
Table
4Interview
schedule.
Interview
schedule
(Nurses)
Prompts
Core
structure
Probes
Iwould
likeyouto
describeformeyourexperience
andviewsofmanagingand
deliveringcaringto
patientwhouse
illicitdrugs
↓
Try
toim
agineatypicalmorning/afternoon/evening/nightduringthat
period….whatsort
ofthingshappened?
Canyougivemeanexample
ofwhathappened
thatmadeyoufeel
thatway?
Gettingback
toyourexperienceswiththepatients…
Are
thereanyparticularexperiencesthatstandoutduringthattime?
Whataboutother
thingspatients
did?
There’snorightorwrongansw
ers,I’djust
liketo
get
youthinking
Identify
values
Identify
hopes
andexpectations
Identify
feelingsofcomfort
withselfandothers
Identify
abilityto
establish
helpingtrustingrelationships
Identify
abilityto
express
positiveandnegativefeelings
Identify
abilityto
solveproblems
Identify
awarenessperceptionsofillnessandgoalsoftreatm
ent
Identify
awarenessofsupportiveprotectiveandcorrectivemental,physical,
societal,andspiritualenvironmentaspects
Whatwas
itlike?
Whathappened
then?
Goon…
Isthereanythingelse?
How
did
thatmakeyou
feel?
How
was
thathelpful?
How
doyoumean?
Tellmemore?
Are
thereanyother
reasons?
Whydoyouthinkthat
happened?
Whatdid
thatmeanto
youatthetime?
Whatwereyouthinking
then?
Finally,whatwould
yousaywerethegoodandbadaspects
aboutcaringfor
patients
whouse
illicitdrugs
© 2012 Blackwell Publishing Ltd 5
JAN: ORIGINAL RESEARCH Caring for problem drug users in medical wards

interaction and relationships involved in the delivery of care
to PDUs in acute MAUs and medical wards. This core cate-
gory was constructed from two sub-categories: ‘Lack of
knowledge to care’ and ‘Distrust and detachment’.
Lack of knowledge to care
Despite repeated calls in the nursing literature to integrate
drug and addiction content into the curriculum for RNs,
none of the nurse participants in this study had received
any formal pre- or post-registration education to prepare
them to deliver care to patients who were admitted with
complications of illicit drug use. The nurses reported feeling
confident and competent to deal with the physical aspects
of problematic drug use such as DVT or septicaemia. They
felt less confident when managing drug-related patient
needs specifically related to drug use, particularly monitor-
ing and managing withdrawals from heroin or other drugs.
This lack of confidence appeared to be translated into inad-
equate care delivery, something recognized by both the
nurses themselves and their patients. Most nurse partici-
pants expressed negative opinions about this patient group
and suggested their views were similar to those held by
most other healthcare professionals:
I think if you ask most nurses and doctors and they were truthful
I’d probably say that nurses’ attitudes towards IV drug abusers and
illicit drug use and, think they’re a waste of space. I think that’s
what they’d say. I think they’re something we have to tolerate.
(Nurse 22)
The patient participants recognized this intolerance and
this seemed to fuel a confrontational mode of communica-
tion as a consequence:
I was coughing up a load of blood, I’d lost a lot of blood and the
doctor said ‘We want to put some blood in you, you’d better come
in.’ ‘No problem, yeah.’ And this nurse came up and was one I had
words with previously ‘Why should we waste a bed on you, you
type of people?’ You know what I mean. So that was it, I went
nuclear! [Became verbally and physically violent] (Patient 12)
The patient participants saw the perceived lack of knowl-
edge of illicit drugs as both a threat to their care and an
opportunity for exploitation. In effect, it afforded an oppor-
tunity to negotiate higher doses of methadone to control
the side effects of withdrawal. Conversely, it appeared to
impact on the care received when symptoms related to
withdrawal went unnoticed. This ‘lack of knowledge’ of
withdrawal management was reportedly well known among
the local community of drug users. A consequence of this
informal knowledge was that patient participants antici-
pated bad withdrawal experiences as a likely consequence
of admission to hospital. Another effect of this informal
knowledge was delaying admission to hospital irrespective
of severity of physical condition(s). The perceived risk of
unsupported withdrawal – ‘cold turkey’ – was seen as a
greater threat than delayed medical intervention.
On admission, patient participants saw the active negotia-
tion of methadone and related medication with healthcare
staff a priority for avoiding withdrawals. The negotiations
about methadone dosage usually began on admission to the
A&E department and if unresolved demands were escalated
on transfer to inpatient care (Medical wards/MAU). Persis-
tence was seen as a strategy for ensuring medication was
administered on time and/or prescriptions dose increased.
Persistence as a tactic was recognized as a risky strategy as it
could lead to conflict with medical and nursing staff. Persis-
tence frequently culminated in the patient being perceived as
a nuisance and interfering with the smooth running of the
ward. Persistence and escalation of demands seemed to serve
to reinforce negative attitudes. The patient participants
reported becoming increasingly discontented when with-
drawal was not managed effectively. This dissatisfaction
often escalated until a point where the patient ‘kicked off’
(Patient 11/Nurse 6). Kicking off involved displaying uncon-
trolled aggression towards the nurse(s) and confirmed the
view that these patients were disruptive and difficult to man-
age.
If these strategies failed, a response was to leave the ward
to ‘score and use’ (Patient 10) and/or take self-discharge:
They’ll (PDUs) come on the ward and 2 hours later they’re gone.
Because all they’re gonna get is DFs (Dihydrocodeine) andmaybe a bit
of Valium (diazepam). You know what I mean. Whereas if they had a
policy where if somebody says they’re on methadone, say somebody
comes in and they say ‘Well, I’m on methadone and I’d like 80 mL of
methadone a day’. ‘Alright, fair enough, I’m prepared to give you
40 mL of methadone today, 40 mL of methadone in the morning and
then we’ll ring your doctor’. You can have half of it. Always half it
because you can guarantee there’ll be a bit of blagging thrown in.
They’re not gonna stay, they’ll just walk off. And the trouble is when
they walk off is the time they (PDUs) drop dead. (Patient 12)
Another aspect of ‘lack of knowledge’ was the absence of
professional understanding of the clinical manifestations of
particular drugs:
I saw a girl come into the department, she’d been smoking crack
cocaine all day. She was screaming, she was really off her face,
she’d had too much crack, too much rock. Screaming, running up
and down the corridors: ‘Help me, help me, help me’. So they
started to put her onto a trolley. But they couldn’t understand
6 © 2012 Blackwell Publishing Ltd
R. Monks et al.

while she wouldn’t keep still and rationally talk, they thought she
was just trying to get a f….ing shot of Valium. Know what I mean?
But she was totally off her face. The nurses and doctors just didn’t
see, they were blind to it. They don’t understand rock (crack
cocaine). (Patient 12)
‘Lack of knowledge’ also had an impact on other aspects
of normal nursing care such as the initiation of supportive
patient education:
Surely we should be doing something while they’re here. You
would with any physical illness which is caused by lifestyle, if it
was an MI, your health promotion, you would be using that. But
with IV drug use, all we do is say, ‘You shouldn’t do it’, But
because we don’t have an understanding, I can’t, I can’t offer nurs-
ing care or information to these people. (Nurse 20)
RNs appeared to be better attuned to patients who could
accurately describe their needs and appeared truthful; in
effect could engage in reciprocal engagement. By contrast,
interactions with patients with a history of illicit drug use
were conducted through a veil of mistrust with the patient
cast as untrustworthy and engaged in ‘blagging’ (Nurse 1).
Blagging was the term used to describe attempts to gain
something, in this case prescribed medication from a nurse
or doctor, by presenting a convincingly truthful explana-
tion. This strategy has been described in other studies, as
has the portrayal of the PDU as a ‘cheater’ (Chan et al.
2008), a foe, socially incompetent, and contemptible (Hill
2010). The perception of PDUs as inherently dishonest
appeared to reinforce negative stereotypes and validate pro-
fessional behaviour.
In the nurse interviews, there was an awareness that a
link existed between poor knowledge and social judgement:
Yeah, helping me to understand a little bit more about their addic-
tion as well because I think we’re all very guilty at times of being
quite judgmental, aren’t we? I think we’re all guilty of judging.
Well, I know I certainly am. (Nurse 25)
Most of the nurses interviewed acknowledged they per-
sonally, and other healthcare staff, held negative attitudes
towards patients who used illicit drugs. This seemed to
cause some dissonance for the nurses a consequence of the
friction between competing values. The RNs expressed
familiarity with the NMC Code of Professional Conduct
(NMC 2008, p. 2). This states that nurses should: ‘make
the care of people your first concern, treating them as indi-
viduals and respecting their dignity’. They also recognized
that their perceptions gained from contact with PDU’s were
incongruent with the professional code as they struggled to
see the person in the patient. This has been described as
‘othering’ patients and significant in obstructing any identi-
fication with patient vulnerabilities or needs (Benner et al.
2008). This dissonance was excused by lack of formal edu-
cation and training and regularly reinforced experientially
through exposure to this patient group. The nurses inter-
viewed in this study expressed a willingness to improve
their knowledge to provide better care and offered a range
of ideas for improving the formal educational preparation
for RNs (Table 5), but none suggested they should take
personal responsibility for acquiring that knowledge.
The absence of ‘knowledge to care’ meant the nurses in
this study seemed unable and sometimes unwilling to
engage in sustained interaction with these patients. Thus,
the behaviours described were at odds with the professional
code, ‘that one must not allow someone’s complaint to pre-
judice the care you provide for them’ (NMC 2008, p. 7).
The nurses seemed to reduce the emotional distress this dis-
sonance caused them by adopting several cognitive and
behavioural strategies. This involved distrust becoming the
assumption underscoring care giving and engaging in
detached manner towards PDUs as strategies to reduce con-
flict. The effectiveness of detachment and distrust went
unquestioned.
Distrust and detachment
Interactions with patients who used illicit drugs were emo-
tionally charged and steeped in mutual feelings of distrust.
This led the nurses in this study to minimize interactions
with PDUs and adopt a disconnected manner. Patient
participants recognized these features in interaction and
reacted by becoming increasingly antagonistic towards the
nurses and others members of the medical team.
Distrust was described as the basis for most interactions
with patients who used illicit drugs, manifesting itself as the
adoption of a detached way of being. Nurses reported limit-
ing the amount of time and interactions with patients who
Table 5 Educational preparation suggested by RNs.
● Understanding of the addiction process
● How the common illicit drugs work and affect people
● Insight into recognizing withdrawals and what to look for
● Courses of managing violence and aggression
● Reflection on case scenarios of previous illicit drug user
admissions
● Insight into the working of the Community Drugs Team
(CDT)
● Understand users’ views of being a patient in the medical ward
● How negative attitudes potentially affect management delivery
● What it is like to be a drug user
© 2012 Blackwell Publishing Ltd 7
JAN: ORIGINAL RESEARCH Caring for problem drug users in medical wards

used drugs in comparison with other inpatients. The conse-
quence of this mutual distrust was an escalation of negative
behaviour, which on occasions ended in conflict involving
verbal or physical abuse directed towards the nurses and
other members of the healthcare team. On other occasions,
it resulted in enforced or self-discharge of patients prior to
resolution of their medical problem(s). Enforced discharge
seemed to be linked to implementation of ‘zero tolerance’
policies used with service users who engage in aggression
and/or violence towards staff (DH 2002). Limiting interac-
tion also meant that the nurses were not as sensitive to
patients’ needs, particularly in relation to their addiction
and associated problems. This detachment was described by
a nurse participant as caring for ‘aliens’ thus asserting their
‘otherness’:
We cannot offer ‘em anything, we can’t give ‘em anything, cos we
don’t know ‘em, to us they’re like ‘aliens’, cos we don’t know ‘em.
(Nurse 18)
Nurses also spoke of their reluctance to discuss issues
related to drugs, or drug use, while undertaking initial assess-
ments on admission to the ward. Lack of understanding of
drug use was offered as a reason for limiting the assessment
process. This reluctance was also recognized by patients who
felt the significance of information they provided went unap-
preciated or was not acted on. Patients described how they
made a rapid appraisal of the knowledge held by the health-
care team; any perceived naivety triggered increased medica-
tion negotiations. Some nurses spoke of purposely keeping
the initial assessment brief and focussed on the physical rea-
sons for admission. This superficial assessment created diffi-
culties for some patients as psychosocial issues related to
their addiction failed to emerge. This was significant as the
chaotic lifestyle of PDUs frequently impacted on individuals
whilst inpatients. Concurrent social and legal problems (e.g.
impending court appearances) often required urgent atten-
tion, and this sometimes led to patients absconding or precip-
itating self-discharge.
Emotionally draining
RNs expressed anxieties about interacting and delivering
care to patients with problematic drug use, particularly the
unpredictability of behaviour. Accounts of hostility and
how this interfered with the smooth running of the ward
contributed to the sub-category of detachment:
It’s hard, it is hard, the ward’s busy anyway and there are certain
people who do have these preconceived ideas and, you know, the
drug abusers are the bottom of heap, they get seen to last… When
they start kicking off and putting other people at risk and being very
very demanding, you do tend,…to detach from them. (Nurse 3)
Most RNs managing the care of patients who used illicit
drugs saw this as an emotional labour (Smith 1992, Smith &
Gray 2001). Nurses spoke of feeling more mentally tired and
drained when patients who use illicit drugs were inpatients.
The working environment was seen as one where intimida-
tion (from patients) was likely to be encountered, where the
RNs felt powerless especially when conflict, disruption, and
violence started to escalate in the confines of the ward:
They’re so unpredictable, you don’t know if they’re gonna sit down
and wait nice and bonny and think, or go off and start ranting and
raving, punching walls, shouting to all the other patients, you
know, like shouting at them as if it’s their fault as well, that
they’ve not got their methadone because they’re the ones that are
being sorted out with. You don’t know what’s gonna happen, it’s
really unpredictable and you fear sometimes, thinking, ‘This is gon-
na get really bad, we might have a really big situation here if we’re
not careful’, …’What do you do? What can we do?’ (Nurse 16)
Seeing the person behind the patient
In contrast, the small number of RNs (n = 3) theoretically
recruited to the study who were recognized in the organiza-
tion as experts in working with inpatient PDUs and drug
user friendly disclosed personal experiences of individuals
(family members or friends) who had used illicit drugs. This
personal biography, as opposed to professionally acquired
understanding, provided them with an insider perspective.
This appeared to positively influence attitudes and became
integrated into their professional way of working. These
RNs appeared to view the patients as people not as drug
users and they seemed more willing and able to interact
and deliver non-judgemental support:
I am interested in them. It’s just a personal thing to me, I have a
friend whose son is a heroin user, so it is interesting to me, but I
know some people, you know, they admit it, they’ve not got time
for them. A couple of times I’ve got involved with the family and
chatted to the family and hear their side of it. (Nurse 4)
The patient participants recognized those nurses who dis-
played emphatic behaviour towards them and responded
positively:
Q: You’ve got some nurses who are nice and they’re okay. And
you are nice and okay to them. (Patient 2)
There’s a young student nurse and she was changing m’bandage
earlier and I were telling her like what happened and that and she
8 © 2012 Blackwell Publishing Ltd
R. Monks et al.

was like really taking interest…and she’s showed more like interest
than what all have ‘em have put together.. She’ll be a good nurse,
definitely. (Patient 4)
When a nurse appeared to show an interest in their prob-
lem, listen, and treat the patient as a ‘person’ not ‘problem
drug user’, interactions with members of the healthcare team
were less charged. The three nurses identified and recruited
to this study appeared to be able to develop rapport, work
with the PDU, and interact in a more recognizably engaged
way. The relationship with patients appeared to other nurses
and the PDUs as less dissonant and more congruent with the
ideology of caring and value of equity of care.
The sub-category ‘distrust and detachment’ illustrates
how in addition to lack of educational preparation and
negative attitudes towards patients who use illicit drugs,
personal experience also served to influence care delivery
and nurse–patient interactions. Seeing the person behind the
patient created an environment where interactions with
PDUs were more positive and harmonious.
Discussion
This study relied solely on interview data and an obvious
limitation is what people ‘say they do’ is not necessarily
‘what they do’ in practice. The nurses and the patients’
accounts confirmed each other and therefore notionally
acted as verification. The likelihood that nurse participants
would present themselves in a negative light if those
accounts were untruthful seems doubtful. Nevertheless, an
observational study would better illustrate how beliefs and
perceptions are transferred into behaviours during care
delivery and would be recommended in future work.
The two sub-categories jointly contribute to the account
of ‘dissonant care management of patients who use illicit
drugs’. The combination of lack of educational preparation
and negative attitudes appeared to act as a barrier to effec-
tive care giving. The RNs functioned in a state of antici-
patory arousal engendered by fears of disruption and
violence. This had the consequence of producing a way of
working that was dissonant with the values more com-
monly associated with nursing: such as competent care giv-
ing and relationships based on mutual trust. The nurses in
this study struggled to avoid the patient’s illness, PDU,
prejudicing the care they provided for them. Dissonance
was not solely a consequence of a relationship between a
lack of knowledge plus negative attitudes. This study
showed experience of caring for PDUs by maintaining them
at a distance as ‘other’ (Benner et al. 2008) appeared to
reinforce negative attitudes and provide knowledge that
constructed and maintained rather than dismantled the bar-
rier between the nurse and PDU.
A distinctive feature of nursing in the UK is that prepara-
tion for initial registration is divided into four branches or
specialities (Adult, Child, Learning Disabilities, and Mental
Health). Adult branch nursing students receive limited edu-
cational input about the health needs of mental ill health. A
potential consequence of specialization is that problem drug
use is categorized as largely falling in the domain of mental
health and positions the PDU outside adult nursing and
very definitely as ‘other’.
That said ‘otherness’ is not necessarily related to stigmati-
zation, exclusion, or demonization yet can result in judge-
ments about the social worth of an individual or group.
Evaluation is an attribute of humanness; hence, nurses are as
likely to make social judgements about a person’s worth as
anyone else. Johnson and Webb (1995) argued that moral
appraisal based on particular attributes, diagnosis, or social
class is more complex than merely labelling and judgements,
as ‘they are flexible and changeable, depending on the social
context’ (p. 471). In this study, the judgement of social worth
of patients admitted with complications of their drug use
seemed to be applied prior to any assessment of the person.
Moreover, such judgements signalled a blanket risk contrib-
uting to perceptions of distrust and use of detachment. How-
ever, this could be specific to this context, where pace and
complexity coupled with efficiency and throughput contrib-
uted to patient objectification, alienation, and constructions
of ‘otherness’.
Although nurses may fight to preserve personhood, it
must be challenging in a rapidly churning acute healthcare
environment (Duffield et al. 2009). Interestingly, those RNs
with personal knowledge gained from exposure to friends
and family members with problems associated with drug
use were able to engage in a different, possibly person-
centred, nurse–patient relationship. They were able to see
the person behind the patient and thus provide a more
caring role expected in the current ideology of nursing.
The primacy of the nurse–patient relationship in care
delivery is central to a contemporary ideology of nursing.
An element of this ideology is the importance placed on
the nurse knowing the patient. Most nurses in this study
spent little time getting to know these patients and, indeed,
minimized interaction as a strategy to reduce opportunities
for conflict and violence, a form of risk management. The
nurses’ spoke candidly of having less concern for patients
who used drugs, seeing their priority as those patients
admitted with supposedly more serious physical conditions
such as myocardial infarction and stroke. These patients
© 2012 Blackwell Publishing Ltd 9
JAN: ORIGINAL RESEARCH Caring for problem drug users in medical wards

were seen as more worthy recipients of their care and
attention. In effect, patients admitted due to complications
of their drug use were prejudged and this impacted on the
care they received. This picture is in stark contrast to
McCance’s (2003) analysis of nurse caring attributes (e.g.
‘showing respect for patients’, ‘Being there’, and ‘being
attentive’); accordingly, the concept of dissonant care
emerged.
Emotional labour, a term first coined by Hochschild
(1983), has been embraced by many commentators (James
1993, Smith & Lorentzon 2007, Gray 2009), as a way of
explaining the trained response used by nurses for managing
and responding to the emotions of patients. It is part of the
labour of nursing work yet can engender feelings of stress,
anxiety, and influence the quality of nurse–patient relation-
ships (Firth-Cozens & Payne 1999). Nurses are obliged, like
many workers, to control their emotional responses within a
narrow range of appropriate behaviours and may feel conflict
between their genuinely felt emotions and those that are pro-
fessionally appropriate to display (Huy 1999). In this study,
most of the RNs consciously chose not to engage in emotional
work with PDUs. Detachment was used as a device for mini-
mizing opportunities. The patient participants recognized
‘part of the gossip’ that they might not receive emotional care
from the majority of RNs they encountered and, perhaps as a
consequence, chose not comply with expectations associated
with the patient role. Thus, a consequence of dissonant care
was neither party fully fulfilled the usual contract of social rec-
iprocity (Molm et al. 1999) in the nurse–patient encounter.
Nurses were aware of this and used several cognitive strategies
such as conflict minimization as a reason for this lack of inter-
action with PDU’s, a form of cognitive dissonance.
Festinger’s (1957) theory of cognitive dissonance suggests
that when behaviours are at odds with beliefs, individuals try
to reduce the psychological distress this causes by adopting
several cognitive and behavioural tactics. Thus, nurses may
seek to reduce their disquiet at being unable to fulfil their core
caring role or engage in emotion work with drug users’ needs
by labelling them as ‘difficult’, ‘problem’, and sometimes
‘alien’ patients.’ This behaviour allows the judgement that
these patients to be appraised as having less social worth and
the cause of their own misfortunes (Johnson 2003). Neverthe-
less, detachment did not seem to be successful defence against
anxiety possibly because of distrust engendered by fears of dis-
ruption and violence.
The findings presented in this study suggest that the con-
ceptual attributes of caring are dissonant to those described
as characterizing most nurse interactions with patients who
are admitted with complications of problem drug use;
moreover, this contributed to poorer outcomes for both the
patients and the nurses.
Conclusion
Findings in this study showed that care management pro-
vided to patients who use illicit drugs was often confused,
chaotic, and disruptive. Early orchestration of appropriate
medication to manage symptoms of withdrawal for PDUs
might offer a stable platform for establishing social
reciprocity as the basis for a person-centred approach.
Better communication between the community drug team
What is already known about this topic
● People with problematic drug use often require
unplanned admission to acute care hospital services
with physical complications of their drug use.
● People with problematic drug use often present with
coexisting psychosocial problems and chaotic social
circumstances that complicate any inpatient stay.
● Registered Nurses, in common with other health pro-
fessionals, often hold negative and stereotypic attitudes
towards patients who use illicit drugs.
What this paper adds
● Registered Nurses in this study recognized they lacked
competencies to manage the problem drug use associ-
ated needs of patients who use illicit drugs.
● Distrust and negative attitudes characterized the nurse
–patient relationship in this study.
● The lack of knowledge to care for problem drug users
coupled with distrust and detachment dominated the
nurse–patient relationship which led to care being
managed and delivered in a vacuum of suspicion and
confrontation.
Implications for practice and/or policy
● Registered Nurses working in acute care settings
require education and training to understand problem
drug use and addiction, to manage withdrawals and
related behaviour, and to initiate appropriate support
for patients who use illicit drugs.
● Understanding the person behind the problem drug
use and addiction may offer a key to care delivery.
● Curriculum development and delivery should involve
services users who have experience of problem drug
use.
10 © 2012 Blackwell Publishing Ltd
R. Monks et al.

and hospital ward staff may aid this. The complexity of
managing and delivering care, the interplay between per-
ceptions, attitudes, and behaviour led to distance and esca-
lation of distrust between the nurses and patients.
According to the nurses’ accounts, education might
improve care management of patients who use illicit drugs
and this need integrating into the Adult branch nurse cur-
riculum in the UK. What was strikingly different in the
accounts provided by the participants was the term
‘expert’ RNs’. These were RNs who gained powerful
learning from personal exposure to people who used illicit
drugs. Arguably non-professional knowledge contributed to
recognizable empathetic professional behaviour and more
positive attitudes towards PDUs. The involvement of ser-
vice users (people who use illicit drugs) in any educational
initiatives may help to expose nurses, to see the person
behind the drugs and ultimately enable RNs to manage
and delivery more competent and empathetic care to this
patient group. Education initiatives alone may not suffice
to rectify the problems encountered when patients who use
drugs clash with the individual nurse; however, such initia-
tives might offer exposure to strategies to de-escalate con-
flict and be more understanding of the plight of PDUs
when they enter the medical ward.
These recommendations may enhance the assessment of
addiction, the management of withdrawals, and the emo-
tional aspects of care provided to patients with problematic
drug use. This could have the effect of reducing the rates of
conflict, unsupported withdrawal from opiate drugs, and
enforced or self-discharge of patients with potentially life-
threatening physical complications.
Funding
This research received no specific grant from any funding
agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
No conflict of interest has been declared by the authors.
Author contributions
All authors meet at least one of the following criteria (rec-
ommended by the ICMJE: http://www.icmje.org/ethi-
cal_1author.html) and have agreed on the final version:
● substantial contributions to conception and design, acqui-
sition of data, or analysis and interpretation of data;
● drafting the article or revising it critically for important
intellectual content.
References
Benner P., Sutphen M., Leonard-Kahn V. & Day L. (2008)
Formation and everyday ethical comportment. American Journal
of Critical Care 17(5), 473–476.
Boyle M.J., Williams B., Brown T., Molloy A., McKenna L.,
Molloy E. & Lewis B. (2010) Attitudes of undergraduate health
science students towards patients with intellectual disability,
substance abuse and acute mental illness: a cross-sectional study.
Medical Education 10(71), 4–8.
Carroll J. (1995) The negative attitudes of some general nurses
towards drug misusers. Nursing Standard 9(34), 36–38.
Carroll J. (1996) Attitudes to drug users according to age of staff.
Professional Nurse 11(6), 401–404.
Chan K.T., Stoove M.A. & Reidpath D.D. (2008) Stigma, social
reciprocity and exclusion of HIV/AIDS patients with illicit drug
histories: a study if Thai nurses’ attitudes. Harm Reduction
Journal 5(28), 1–11.
Cooke M.W., Higgins J. & Kidd P. (2003) Use of emergency
observation and assessment wards: a systematic literature review.
Emergency Medicine 20, 138–142.
Deehan A., Taylor C. & Strang J. (1997) The general practitioner,
the drug misuser and the alcohol misuser: major differences in
general practitioner activity, therapeutic commitment and ‘shared
care’ proposals. British Journal of General Practice 47(424),
705–709.
Denzin N.K. & Lincoln Y.S. (2003) Introduction: The Discipline
and Practice of Qualitative Research. Sage, Thousand Oaks.
Department of Health (2002) Withholding Treatment from Violent
and Abusive Patients in NHS Trusts: NHS zero tolerance zone.
Department of Health, London.
Duffield C., Diers D., Aisbett C. & Roche M. (2009) Churn: patient
turnover and case mix. Nurse Economics 27(3), 185–191.
European Monitoring Centre for Drugs and Drug Addiction (2005)
The State of the Drug Problem in the European Union and
Norway: Annual Report 2005. European Monitoring Centre for
Drugs and Drug Addiction, Lisbon.
European Monitoring Centre for Drugs and Drug Addiction (2009)
The State of the Drug Problem in the European Union and
Norway: Annual Report 2006. European Monitoring Centre for
Drugs and Drug Addiction, Lisbon.
European Monitoring Centre for Drugs and Drug Addiction (2010)
The State of the Drug Problem in the European Union: Annual
Report 2010. European Monitoring Centre for Drugs and Drug
Addiction, Lisbon.
Festinger L. (1957) A Theory of Cognitive Dissonance. Stanford
University Press, Evanston.
Firth-Cozens J. & Payne R. (1999) Stress in health professionals.
Health and Stress 16(5), 327–329.
Foster J. & Onyeukwu C. (2003) The attitude of forensic nurses to
substance using service users. Journal of Psychiatric & Mental
Health Nursing 10(5), 578–584.
Godfrey C., Eaton G., McDougall C. & Culyer A. (2002) The
Economic and Social Cost of Class A Drug Use in England and
Wales, 2000. Home Office, London.
Gray B. (2009) The emotional labour of nursing: defining and
managing emotions in nursing work. Nurse Education Today 29
(2), 168–175.
© 2012 Blackwell Publishing Ltd 11
JAN: ORIGINAL RESEARCH Caring for problem drug users in medical wards
Happell B. & Taylor C. (2001) Negative attitudes towards clients
with drug and alcohol related problems: Finding the elusive
solution. Australian & New Zealand Journal of Mental Health
Nursing 10(2), 87–96.
Harling M. & Turner W. (2012) Student nurses’ attitudes to illicit
drugs: a grounded theory study. Nurse Education Today 32(3),
235–240.
Harling M., Overy C., Beckham G., Denby R., Goddard S.,
O’Connor C., Piotrowski E., Prout T. & Tully D. (2006)
Addressing negative attitudes towards substance use in nursing: a
peer-led approach in nurse education. Drugs and Alcohol Today
6(2), 38–41.
Heyes P.D. (2002) Substance abuse integration in nursing
education: an innovative collaborative model. Substance Abuse
23(1), 67–79.
Hill T.E. (2010) How clinicians make (or avoid) moral judgments
of patients: implications of the evidence for relationships and
research. Philosophy, Ethics and Humanities in Medicine 5(1),
1–14.
Hochschild A. (1983) The Managed Heart. University of California
Press, Berkeley.
Huy Q.N. (1999) Emotional capability, emotional intelligence
and radical change. The Academy of Management Review 24(2),
325–345.
James N. (1993) Divisions of Emotional Labour: Disclosure and
Cancer. In Communication, Relationships and Care (Barett S.,
Komaromy C., Robb M. & Rogers A., eds), Routledge, London,
pp. 259–269.
Johnson M. (2003) Nurses, clients and power. In Sociology as
Applied to Nursing and Health Care, Chapter 8 (Birchenhall M.
& Birchenhall P., eds), Bailliere Tindall, Edinburgh.
Johnson M. & Webb C. (1995) Rediscovering unpopular patients:
the concept of social judgement. Journal of Advanced Nursing
21(3), 466–475.
McCance T.V. (2003) Caring in nursing practice: the development
of a conceptual framework. Research and Theory for Nursing
Practice: An International Journal 17(2), 101–116.
McLaughlin D.F., McKenna H. & Leslie J.C. (2000) The
perceptions and aspirations illicit drug users hold toward health
care staff and the care they receive. Journal of Psychiatric &
Mental Health Nursing 7(5), 435–441.
Molm L.D., Peterson G. & Takahashi N. (1999) Power in
negotiated and reciprocal exchange. American Sociological
Review 64(6), 876–890.
Morrison E.F., Ramsey A. & Synder B.A. (2000) Managing the
care of complex, difficult patients in medical-surgical settings.
MEDSURG Nursing 9(1), 21–26.
Nursing and Midwifery Council (2008) The Code of Professional
Conduct. NMC, London.
Rassool H.G. & Rawaf S. (2008) Predictors of educational
outcomes of undergraduate nursing students in alcohol and drug
education. Nurse Education Today 28(6), 691–701.
Rassool H.G. & Salman R. (2008) Education intervention of
undergraduate nursing students’ confidence skills with alcohol
and drug misusers Education intervention of undergraduate
nursing students’ confidence skills with alcohol and drug
misusers. Nurse Education Today 28(3), 284–292.
Richards L. (2000) Using NVivo in Qualitative Research. QSR
International Pty, Victoria.
Smith P. (1992) The Emotional Labour of Nursing. MacMillan,
London.
Smith P. & Gray B. (2001) Emotional labour of nursing revisited:
caring and learning 2000.Nurse Education in Practice 1(1), 42–49.
Smith P. & Lorentzon M. (2007) Is emotional labour ethical.
Nursing Ethics 16(6), 638–642.
Strauss A. & Corbin J. (1998) Basics of Qualitative Research:
Techniques and Procedures for Developing Grounded Theory.
Sage, Thousand Oaks.
UK Focal Point (2004) United Kingdom Drug Situation 2004:
Annual Report to the European Monitoring Centre for Drugs and
Drug Addiction (EMCDDA). Centre for Public Health, Liverpool
John Moores University and Department of Health. ????.
United Nations Office on Drugs and Crime (2010) World Drug
Report 2010. United Nations, Vienna.
The Journal of Advanced Nursing (JAN) is an international, peer-reviewed, scientific journal. JAN contributes to the advancement of
evidence-based nursing, midwifery and health care by disseminating high quality research and scholarship of contemporary relevance
and with potential to advance knowledge for practice, education, management or policy. JAN publishes research reviews, original
research reports and methodological and theoretical papers.
For further information, please visit JAN on the Wiley Online Library website: www.wileyonlinelibrary.com/journal/jan
Reasons to publish your work in JAN:
• High-impact forum: the world’s most cited nursing journal and with an Impact Factor of 1·540 – ranked 9th of 85 in the 2010
Thomson Reuters Journal Citation Report (Social Science – Nursing). JAN has been in the top ten every year for a decade.
• Most read nursing journal in the world: over 3 million articles downloaded online per year and accessible in over 10,000 libraries
worldwide (including over 3,500 in developing countries with free or low cost access).
• Fast and easy online submission: online submission at http://mc.manuscriptcentral.com/jan.
• Positive publishing experience: rapid double-blind peer review with constructive feedback.
• Rapid online publication in five weeks: average time from final manuscript arriving in production to online publication.
• Online Open: the option to pay to make your article freely and openly accessible to non-subscribers upon publication on Wiley
Online Library, as well as the option to deposit the article in your own or your funding agency’s preferred archive (e.g. PubMed).
12 © 2012 Blackwell Publishing Ltd
R. Monks et al.





























