Embed Size (px)
Citation preview

The effect of a modified functional appliance on obstructive sleep apnea
Paul E. Bonham, DDS, MS,* G. Friins Currier, DDS, MSD, MEd,++ William C. Orr, PhD,*** Joe Othman, MD,**** and Ram S. Nanda, DDS, MS, PhD*“** Tempe, Ariz., Oklahoma City, Okla., Canton, Ohio, and Cumberland, Md.
This study combined the use of cephalometrics and overnight polysomnographic monitoring to analyze the effects of a modified functional appliance on airway, sleep, and respiratory variables in patients with obstructive sleep apnea (OSA). Twelve patients without overt anatomic or pathologic evidence of obstruction were selected on the basis of an initial single night of polysomnographic monitoring, which confirmed the diagnosis of obstructive sleep apnea syndrome. The patients subsequently were fitted with a modified functional appliance designed to securely hold the mandible in an anterior-inferior position. A subsequent overnight polysomnographic study was obtained with each patient wearing the appliance. Lateral cephalometric radiographs with and without the appliance in place were also obtained. The mean vertical and horizontal changes in mandibular position while wearing the appliance were 8.49 mm and 2.28 mm, respectively. The findings indicate that 10 of the 12 patients had decreases in the rate of complete airway obstructions from a mean of 28.86 to 18.69 events per hour, and in the total apnea index from a mean of 53.81 to 35.99 events per hour. A reduction in the rate of obstructive events is attributed to the effect of the appliance on the oropharyngeal structures. Six cephalometric measurements are presented to provide a means of assessing effects of the appliance on the oropharynx and associated structures. The modified functional appliance is a conservative, successful treatment alternative that could benefit patients with obstructive sleep apnea syndrome. (AM J ORTHOD DENTOFAC ORTHOP 1988;94:384-92.)
0 bstructive sleep apnea (OSA) is a condi- tion involving repeated obstruction of the upper airway during sleep. This occlusion of the upper airway may result if sleep-induced physiologic change in muscle activity is superimposed on various structural defects of the upper airway. Macroglossia, micrognathia, ret- rognathia, and decreased airway lumen have all been implicated in OSA. I-7 Although anatomic disturbances commonly lead to obstructed airflow, some patients with OSA have no readily recognizable airway abnor-
This article is based on a thesis submitted to the Faculty of Graduate Studies, University of Oklahoma, in partial fulfillment of the requirements for the degree of master of science. This research project was supported in part by a grant from the Foundation for Orthodontic Research, Pacific Palisades, Calif. *Power resident, Department of Orthodontics, University of Oklahoma. Col- lege of Dentistry; presently in private practice in Tempe, Arizona. **Associate Professor, Department of Orthodontics, University of Oklahoma, College of Dentistry. ***Former Director of the HCA Presbyterian Hospital Sleep Disorders Center, Oklahoma City; presently at the Ohio Institute for Medical Science, Canton, Ohio. ****Formerly of the Department of Neurology, University of Oklahoma Col- lege of Medicine. Oklahoma City; presently in private practice in Cumberland, Md. *****Professor and Chairman, Department of Orthodontics and Division of Developmental Dentistry, University of Oklahoma.
mality. The site of obstruction in these patients has been identified at the level of the oropharynx.R-10 Regardless of the cause, the potential consequences for the patient with untreated OSA are serious. Severe hypoxemia and ventricular and supraventricular cardiac arrhythmias have been noted. “J*
There are a variety of surgical and nonsurgical treat- ment modalities currently available for OSA. Trache- ostomy, the classical surgical treatment, is virtually al- ways successful. However, it is not favorably accepted by most patients. More recently the uvulopalatophar- yngoplasty has achieved widespread use, but suc- cess rates vary and long-term effects are still un- known.‘3v’4 Current nonsurgical treatment methods can be cumbersome and uncomfortable with variable re- sponses. “-”
There is a need for a treatment modality that would benefit patients who are poor surgical risks, reject sur- gery, or have not responded adequately to surgical pro- cedures. It should be more convenient and more pre- dictable than current nonsurgical methods. Treatment should be comfortable and easily accepted, noninva- sive, readily reversible, and cost-effective. Sol1 and George’* and George” have described an easily ac- cepted nonsurgical intervention that uses an intraoral
Volrrme 94 Number 5
Ejfect of modjfied functional appliance on OSA 385
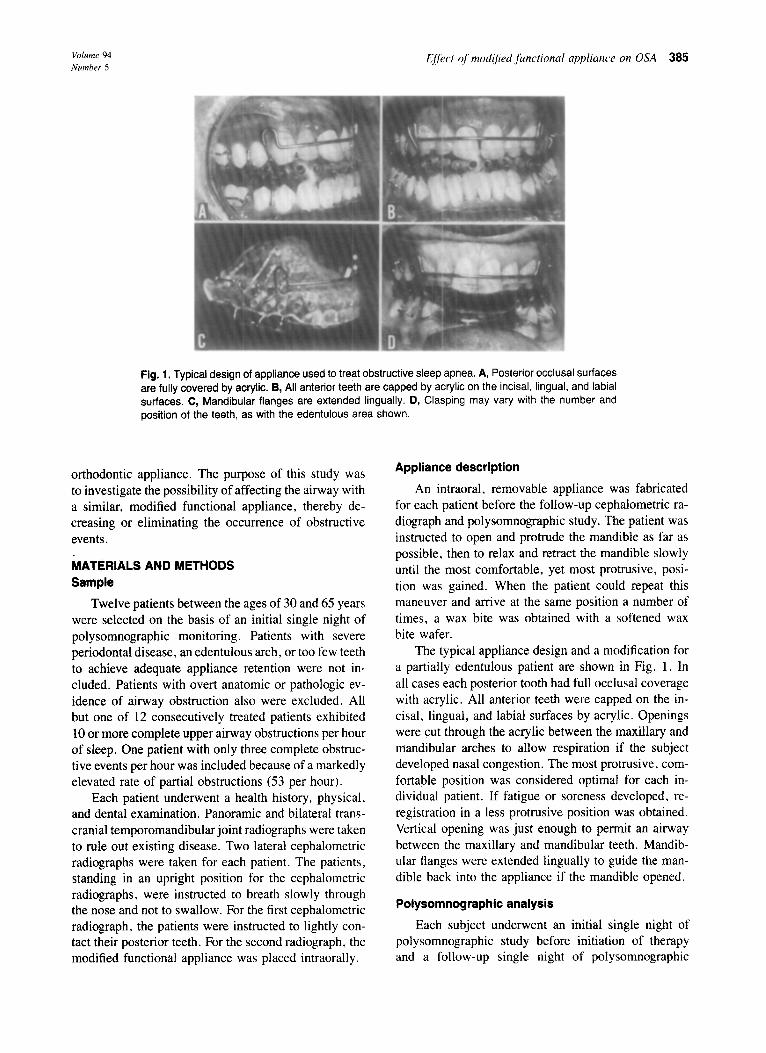
Fig. 1, Typical design of appliance used to treat obstructive sleep apnea. A, Posterior occlusal surfaces are fully covered by acrylic. B, All anterior teeth are capped by acrylic on the incisal, lingual, and labial surfaces. C, Mandibular flanges are extended lingually. D, Clasping may vary with the number and position of the teeth, as with the edentulous area shown.
orthodontic appliance. The purpose of this study was to investigate the possibility of affecting the airway with a similar, modified functional appliance, thereby de- creasing or eliminating the occurrence of obstructive events.
MATERIALS AND METHODS Sample
Twelve patients between the ages of 30 and 65 years were selected on the basis of an initial single night of polysomnographic monitoring. Patients with severe periodontal disease, an edentulous arch, or too few teeth to achieve adequate appliance retention were not in- cluded. Patients with overt anatomic or pathologic ev- idence of airway obstruction also were excluded. All but one of 12 consecutively treated patients exhibited 10 or more complete upper airway obstructions per hour of sleep. One patient with only three complete obstruc- tive events per hour was included because of a markedly elevated rate of partial obstructions (53 per hour).
Each patient underwent a health history, physical. and dental examination. Panoramic and bilateral trans- cranial temporomandibular joint radiographs were taken to rule out existing disease. Two lateral cephalometric radiographs were taken for each patient. The patients. standing in an upright position for the cephalometric radiographs, were instructed to breath slowly through the nose and not to swallow. For the first cephalometric radiograph, the patients were instructed to lightly con- tact their posterior teeth. For the second radiograph, the modified functional appliance was placed intraorally.
Appliance description
An intraoral, removable appliance was fabricated for each patient before the follow-up cephalometric ra- diograph and polysomnographic study. The patient was instructed to open and protrude the mandible as far as possible, then to relax and retract the mandible slowly until the most comfortable, yet most protrusive, posi- tion was gained. When the patient could repeat this maneuver and arrive at the same position a number of times, a wax bite was obtained with a softened wax bite wafer.
The typical appliance design and a modification for a partially edentulous patient are shown in Fig. 1. In all cases each posterior tooth had full occlusal coverage with acrylic. All anterior teeth were capped on the in- cisal, lingual, and labial surfaces by acrylic. Openings were cut through the acrylic between the maxillary and mandibular arches to allow respiration if the subject developed nasal congestion. The most protrusive, com- fortable position was considered optimal for each in- dividual patient. If fatigue or soreness developed, re- registration in a less protrusive position was obtained. Vertical opening was just enough to permit an airway between the maxillary and mandibular teeth. Mandib- ular flanges were extended lingually to guide the man- dible back into the appliance if the mandible opened.
Poiysomnographic analysis
Each subject underwent an initial single night of polysomnographic study before initiation of therapy and a follow-up single night of polysomnographic
386 Bonham et al. Am. J. Orthod. Dentofac. Orthop. November 1988
A 0 c CENTRAL APNEA OBSTRUCTIVE APNEA MIXED APNEA
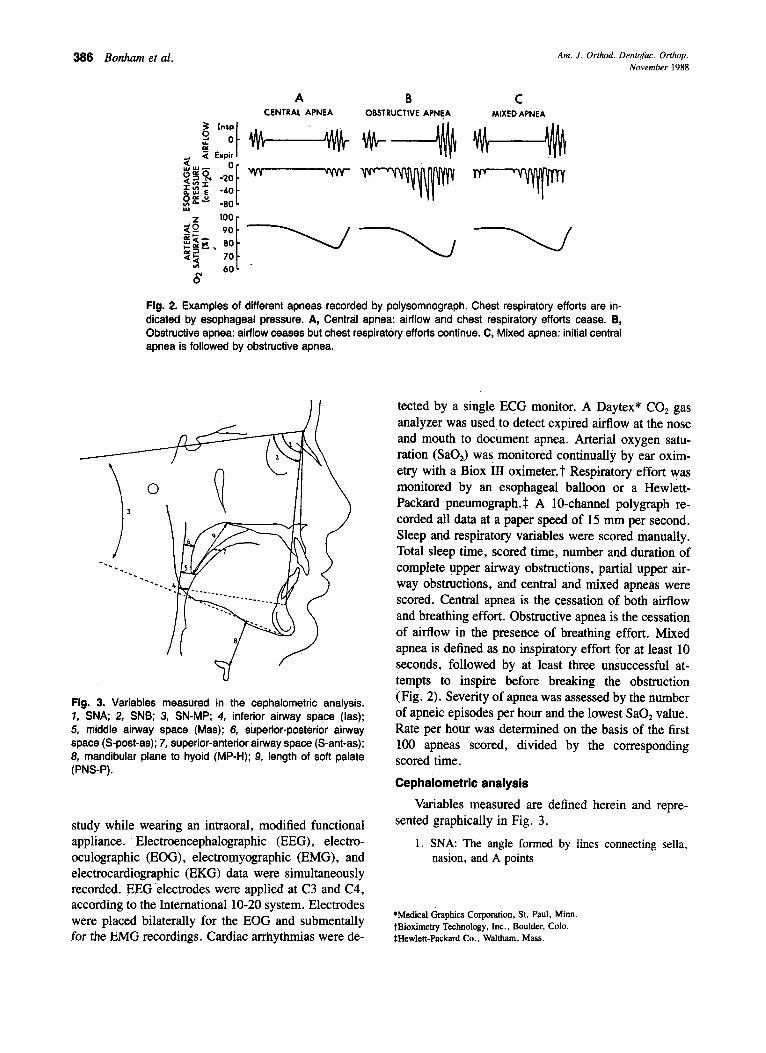
Fig. 2. Examples of different apneas recorded by polysomnograph. Chest respiratory efforts are in- dicated by esophageal pressure. A, Central apnea: airflow and chest respiratory efforts cease. B, Obstructive apnea: airflow ceases but chest respiratory efforts continue. C, Mixed apnea: initial central apnea is followed by obstructive apnea.
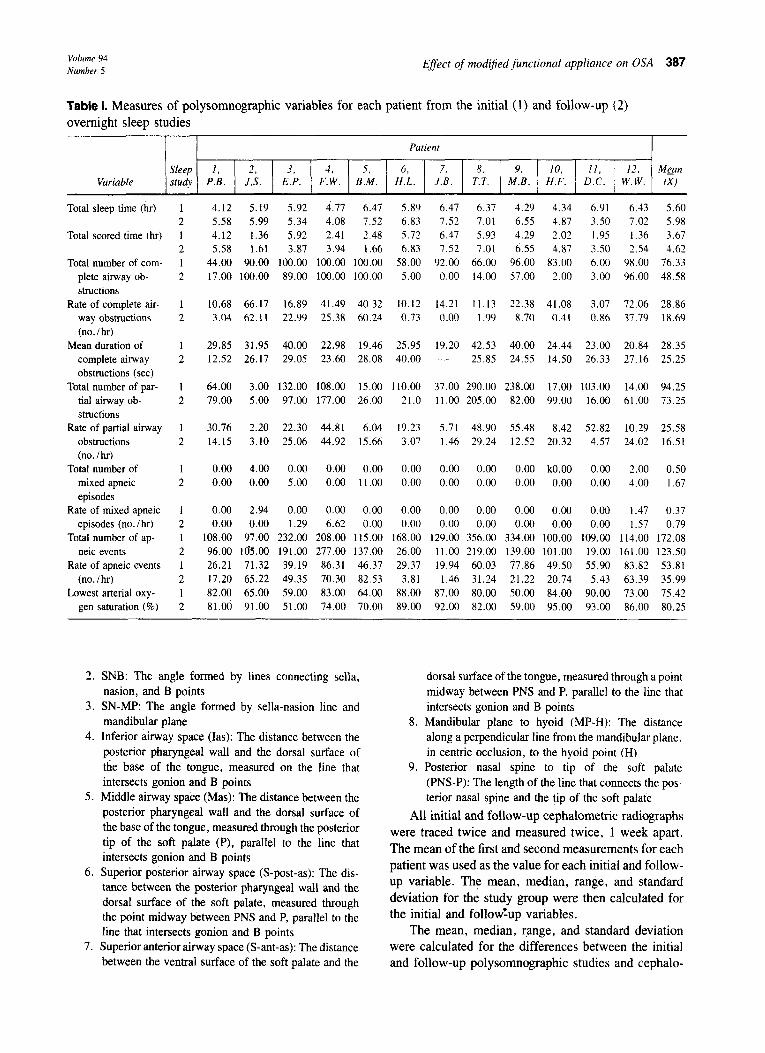
Fig. 3. Variables measured in the cephalometric analysis. 7, SNA; 2, SNB; 3, SN-MP; 4, inferior airway space (las); 5, middle airway space (&las); 6, superior-posterior airway space (S-post-as); 7, superior-anterior airway space (S-ant-as); 8, mandibular plane to hyoid (MP-H); 9, length of soft palate (PNS-P).
study while wearing an intraoral, modified functional appliance. Electroencephalographic (EEG), electro- oculographic (EOG), electromyographic (EMG), and electrocardiographic (EKG) data were simultaneously recorded. EEG .electrodes were applied at C3 and C4, according to the International lo-20 system. Electrodes were placed bilaterally for the EOG and submentally for the EMG recordings. Cardiac arrhythmias were de-
tected by a single ECG monitor. A Daytex* CO, gas analyzer was used to detect expired airflow at the nose and mouth to document apnea. Arterial oxygen satu- ration (SaO,) was monitored continually by ear oxim- etry with a Biox III oximeter:? Respiratory effort was monitored by an esophageal balloon or a Hewlett- Packard pneum0graph.S A lo-channel polygraph re- corded all data at a paper speed of 15 mm per second. Sleep and respiratory variables were scored manually. Total sleep time, scored time, number and duration of complete upper airway obstructions, partial upper air- way obstructions, and central and mixed apneas were scored. Central apnea is the cessation of both airllow and breathing effort. Obstructive apnea is the cessation of airflow in the presence of breathing effort. Mixed apnea is defined as no inspiratory effort for at least 10 seconds, followed by at least three unsuccessful at- tempts to inspire before breaking the obstruction (Fig. 2). Severity of apnea was assessed by the number of apneic episodes per hour and the lowest SaO, value. Rate per hour was deteimined on the basis of the first 100 apneas scored, divided by the corresponding scored time.
Cephalometric analysis
Variables measured are defined herein and repre- sented graphically in Fig. 3.
1. SNA: The angle formed by lines connecting sella, nasion, and A points
*Medical Graphics Corporation, St. Paul, Minn. tBioxim&y Technolcgy, Inc., Boulder, Cola. SHewlett-Packard Co., Waltham, Mass.
Volume 94 Number 5 Effect of mod$ed functional appliance on OSA 387
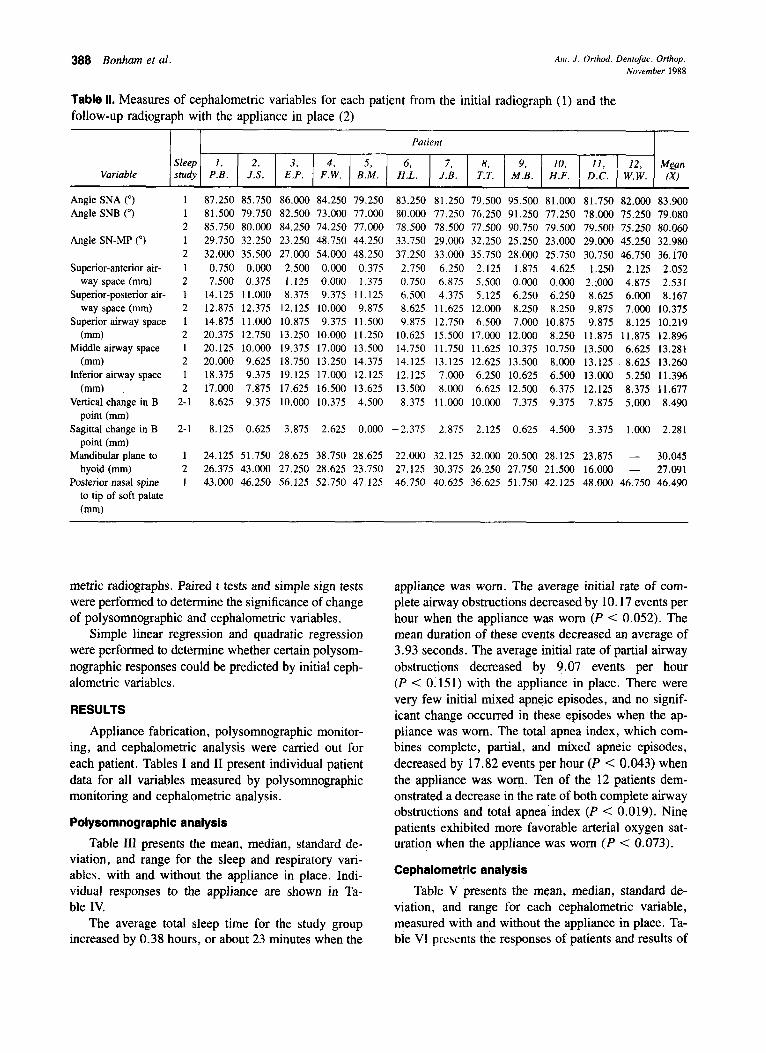
Table I. Measures of polysomnographic variables for each patient from the initial (1) and follow-up (2) overnight sleep studies
Patient
Variable Sleep I, 2, 3, 4. 5. 6, 7. 8. 9. IO. 11, 12. MgltI stud?, P.B. J.S. E.P. F.W. B.M. H.L. J.B. T.T. M.B. H.F. D.C. / W.W. fX1
Total sleep time (hr) 4.12 5.19 5.92 4.71 6.41 5.89 6.47 6.37 4.29 4.34 6.91 6.43 5.60 5.58 5.99 5.34 4.08 7.52 6.83 7.52 7.01 6.55 4.87 3.50 7.02 5.98 4.12 1.36 5.92 2.41 2.48 5.72 6.47 5.93 4.29 2.02 1.95 1.36 3.67 5.58 1.61 3.87 3.94 1.66 6.83 7.52 7 .Ol 6.55 4.87 3.50 2.54 4.62
44.00 90.00 100.00 100.00 100.00 58.00 92.00 66.00 96.00 83.00 6.00 98.00 76.33 17.00 100.00 89.00 100.00 100.00 5.00 0.00 14.00 57.00 2.00 3.00 96.00 48.58
Total scored time (hr)
Total number of com- plete airway ob- structions
Rate of complete air- way obstructions (no. / hr)
Mean duration of complete airway obstructions (set)
Total number of par- tial airway ob- structions
Rate of partial airway obstructions (no./hr)
Total number of mixed apneic episodes
Rate of mixed apneic episodes (no. /hr)
Total number of ap- neic events
Rate of apneic events (no./hr)
Lowest arterial oxy- gen saturation (%)
1 10.68 66.17 16.89 41.49 40.32 10.12 14.21 11.13 22.38 41.08 3.07 72.06 28.86 2 3.04 62.11 22.99 25.38 60.24 0.13 0.00 1.99 8.70 0.41 0.86 37.79 18.69
1 29.85 31.95 40.00 22.98 19.46 25.95 19.20 42.53 40.00 24.44 23.00 20.84 28.35 2 12.52 26.17 29.05 23.60 28.08 40.00 - 25.85 24.55 14.50 26.33 27.16 25.25
1 64.00 3.00 132.00 108.00 15.00 110.00 37.00 290.00 238.00 17.00 103.00 14.00 94.25 2 79.00 5.00 97.00 177.00 26.00 21.0 11.00 205.00 82.00 99.00 16.00 61.00 73.25
1 30.76 2.20 22.30 44.81 6.04 19.23 5.71 48.90 55.48 8.42 52.82 10.29 25.58 2 14.15 3.10 25.06 44.92 15.66 3.07 1.46 29.24 12.52 20.32 4.57 24.02 16.51
1 0.00 4.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 kO.OO 0.00 2.00 0.50 2 0.00 0.00 5.00 0.00 11.00 0.00 0.00 0.00 0.00 0.00 0.00 4.00 1.67
0.00 2.94 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 1.47 0.37 0.00 0.00 1.29 6.62 0.00 0.00 0.00 0.00 0.00 0.00 0.00 1.57 0.79
108.00 97.00 232.00 208.00 115.00 168.00 129.00 356.00 334.00 100.00 109.00 114.00 172.08 96.00 [email protected] 191.00 277.00 137.00 26.00 11.00 219.00 139.00 101.00 19.00 161.00 123.50 26.21 71.32 39.19 86.31 46.37 29.37 19.94 60.03 77.86 49.50 55.90 83.82 53.81 17.20 65.22 49.35 70.30 82.53 3.81 1.46 31.24 21.22 20.74 5.43 63.39 35.99 82.00 65.00 59.00 83.00 64.00 88.00 87.00 80.00 50.00 84.00 90.00 73.00 75.42 81.00 91.00 51.00 74.00 70.00 89.00 92.00 82.00 59.00 95.00 93.00 86.00 80.25
2. SNB: The angle formed by lines connecting sella, nasion, and B points
3. SN-MP: The angle formed by sella-nasion line and mandibular plane
4. Inferior airway space (Ias): The distance between the posterior pharyngeal wall and the dorsal surface of tne base of the tongue, measured on the line that intersects gonion and B points
5. Middle airway space (Mas): The distance between the posterior pharyngeal wall and the dorsal surface of the base of the tongue, measured through the posterior tip of the soft palate (P), parallel to the line that intersects gonion and B points
6. Superior posterior airway space (S-post-as): The dis- tance between the posterior pharyngeal wall and the dorsal surface of the soft palate, measured through the point midway between PNS and P, parallel to the line that intersects gonion and B points
7. Superior anterior airway space (S-ant-as): The distance between the ventral surface of the soft palate and the
dorsal surface of the tongue, measured through a point midway between PNS and P, parallel to the line that intersects gonion and B points
8. Mandibular plane to hyoid (MP-H): The distance along a perpendicular line from the mandibular plane. in centric occlusion, to the hyoid point (H)
9. Posterior nasal spine to tip of the soft palate (PNS-P): The length of the line that connects the pos- terior nasal spine and the tip of the soft palate
All initial and follow-up cephalometric radiographs were traced twice and measured twice, 1 week apart. The mean of the first and second measurements for each patient was used as the value for each initial and follow- up variable. The mean, median, range, and standard deviation for the study group were then calculated for the initial and follow%p variables.
The mean, median, range, and standard deviation were calculated for the differences between the initial and follow-up polysomnographic studies and cephalo-
388 Bonham et al. Am. J. Orthod. Dentofac. Orthop. November 1988
Table II. Measures of cephalometric variables for each patient from the initial radiograph (1) and the follow-up radiograph with the appliance in place (2)
Patient
Variable Sleep I, 2, 3. 4. 5, 6, 7, 8, 9, 10, II, 12, Mean study P.B. J.S. E.P. F.W. B.M. H.L. J.B. T.T. M.B. H.F. D.C. W.W. (x)
Angle SNA (“) Angle SNB (“)
Angle SN-MP to)
Superior-anterior air- way space (mm)
Superior-posterior air- way space (mm)
Superior airway space (mm)
Middle airway space (mm)
Inferior airway space (mm)
Vertical change in B point (mm)
Sagittal change in B point (mm)
Mandibular plane to hyoid (mm)
Posterior nasal spine to tip of soft palate (mm)
1 87.250 85.750 86.000 84.250 79.250 83.250 81.250 79.500 95.500 81.000 81.750 82.000 83.900 1 81.500 79.750 82.500 73.000 77.000 80.000 77.250 76.250 91.250 77.250 78.000 75.250 79.080 2 85.750 80.000 84.250 74.250 77.000 78.500 78.500 77.500 90.750 79.500 79.500 75.250 80.060 1 29.750 32.250 23.250 48.750 44.250 33.750 29.000 32.250 25.250 23.000 29.000 45.250 32.980 2 32.000 35.500 27.000 54.000 48.250 37.250 33.000 35.750 28.000 25.750 30.750 46.750 36.170 1 0.750 0.000 2.500 0.000 0.375 2.750 6.250 2.125 1.875 4.625 1.250 2.125 2.052
2 7.500 0.375 1.125 0.000 1.375 0.750 6.875 5.500 0.000 0.000 2.;000 4.875 2.531 1 14.125 11.000 8.375 9.375 11.125 6.500 4.375 5.125 6.250 6.250 8.625 6.000 8.167 2 12.875 12.375 12.125 10.000 9.875 8.625 11.625 12.000 8.250 8.250 9.875 7.000 10.375 1 14.875 11.000 10.875 9.375 11.500 9.875 12.750 6.500 7.000 10.875 9.875 8.125 10.219
2 20.375 12.750 13.250 10.000 11.250 10.625 15.500 17.000 12.000 8.250 11.875 11.875 12.896 1 20.125 10.000 19.375 17.000 13.500 14.750 11.750 11.625 10.375 10.750 13.500 6.625 13.281 2 20.000 9.625 18.750 13.250 14.375 14.125 13.125 12.625 13.500 8.000 13.125 8.625 13.260 1 18.375 9.375 19.125 17.000 12.125 12.125 7.000 6.250 10.625 6.500 13.000 5.250 11.396 2 17.000 7.875 17.625 16.500 13.625 13.500 8.000 6.625 12.500 6.375 12.125 8.375 11.677
2-l 8.625 9.375 10.000 10.375 4.500 8.375 11.000 10.000 7.375 9.375 7.875 5.000 8.490
2-1 8.125 0.625 3.875 2.625 0.000 -2.375 2.875 2.125 0.625 4.500 3.375 1.000 2.281
1 24.125 51.750 28.625 38.750 28.625 22.000 32.125 32.000 20.500 28.125 23.875 - 30.045 2 26.375 43.000 27.250 28.625 23.750 27.125 30.375 26.250 27.750 21.500 16.000 - 27.091 1 43.000 46.250 56.125 52.750 47.125 46.750 40.625 36.625 51.750 42.125 48.000 46.750 46.490
metric radiographs. Paired t tests and simple sign tests were performed to determine the significance of change of polysomnographic and cephalometric variables.
Simple linear regression and quadratic regression were performed to determine whether certain polysom- nographic responses could be predicted by initial ceph- alometric variables.
RESULTS
Appliance fabrication, polysomnographic monitor- ing, and cephalometric analysis were carried out for each patient. Tables I and II present individual patient data for all variables measured by polysomnographic monitoring and cephalometric analysis.
Polysomnographic analysis
Table III presents the mean, median, standard de- viation, and range for the sleep and respiratory vari- ables. with and without the appliance in place. Indi- vidual responses to the appliance are shown in Ta- ble IV.
The average total sleep time for the study group increased by 0.38 hours, or about 23 minutes when the
appliance was worn. The average initial rate of com- plete airway obstructions decreased by 10.17 events per hour when the appliance was worn (P < 0.052). The mean duration of these events decreased an average of 3.93 seconds. The average initial rate of partial airway obstructions decreased by 9.07 events per hour (P < 0.15 1) with the appliance in place. There were very few initial mixed apneic episodes, and no signif- icant change occurred in these episodes when the ap- pliance was worn. The total apnea index, which com- bines complete, partial, and mixed apneic episodes, decreased by 17.82 events per hour (P < 0.043) when the appliance was worn. Ten of the 12 patients dem- onstrated a decrease in the rate of both complete airway obstructions and total apnea’index (P < 0.019). Nine patients exhibited more favorable arterial oxygen sat- uration when the appliance was worn (P < 0.073).
Cephalometric analysis
Table V presents the mean, median, standard de- viation, and range for each cephalometric variable, measured with and without the appliance in place. Ta- ble VI presents the responses of patients and results of
Volume 94 Number 5
Effect of modijed functional appliance on OSA 389
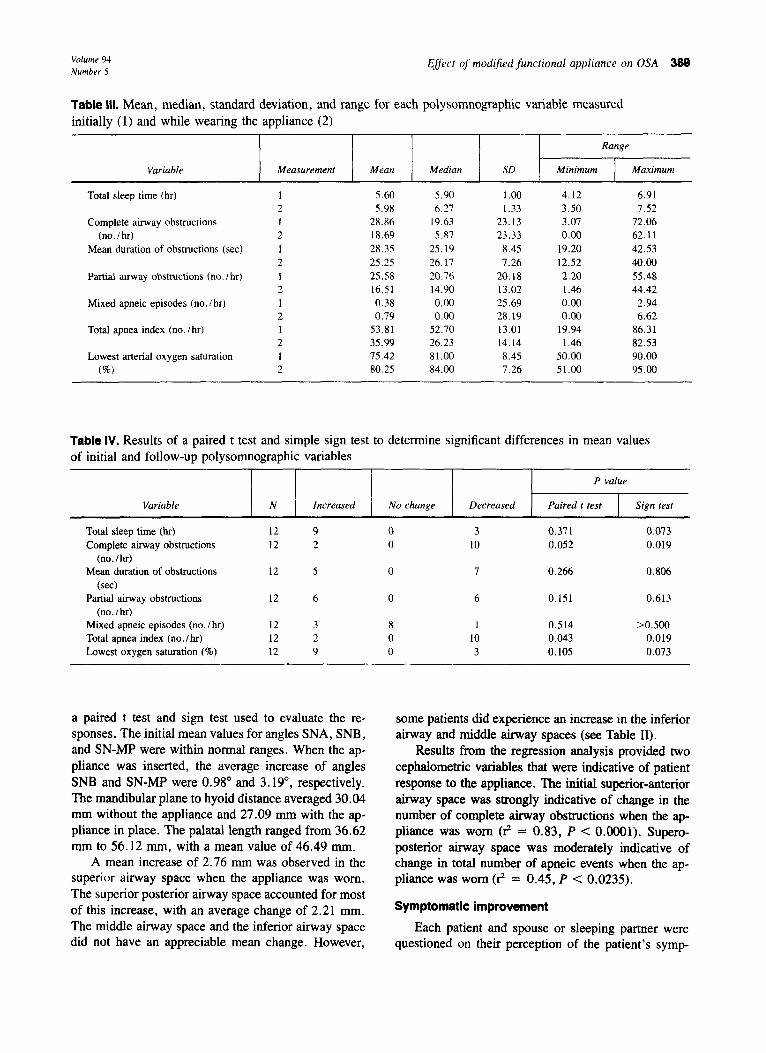
Table III. Mean, median, standard deviation, and range for each polysomnographic variable measured initially (1) and while wearing the appliance (2)
Range
Variable
Total sleep time (hr)
Complete airway obstructions (no./hr)
Mean duration of obstructions (set)
Partial airway obstructions (no. I hr)
Mixed apneic episodes (no. /hr)
Total index (no. I hr) apnea
Lowest arterial saturation oxygen (%6)
Measurement Mean Median SD Minimum Maximum
1 5.60 5.90 1.00 4.12 6.91 2 5.98 6.27 1.33 3.50 7.52 1 28.86 19.63 23.13 3.07 72.06 2 18.69 5.87 23.33 0.00 62.11 1 28.35 25.19 8.45 19.20 42.53 2 25.25 26.17 7.26 12.52 40.00 1 25.58 20.76 20.18 2.20 55.48 2 16.51 14.90 13.02 1.46 44.42 1 0.38 0.00 25.69 0.00 2.94 2 0.79 0.00 28.19 0.00 6.62 1 53.81 52.70 13.01 19.94 86.31 2 35.99 26.23 14.14 1.46 82.53 1 75.42 81.00 8.45 50.00 90.00 2 80.25 84.00 7.26 51.00 95.00
Table IV. Results of a paired t test and simple sign test to determine significant differences in mean values of initial and follow-up polysomnographic variables
P value
Variable
Total sleep time (hr) Complete airway obstructions
(no./hr) Mean duration of obstructions
(set) Partial airway obstructions
(no. / hr) Mixed apneic episodes (no. / hr) Total index (no. /hr) apnea Lowest saturation (%) oxygen
N Increased No change Decreased Paired t test Sign test
12 9 0 3 0.371 0.073 12 2 0 10 0.052 0.019
12 5 0 7 0.266 0.806
12 6 0 6 0.151 0.613
12 3 8 1 0.514 >0.500 12 2 0 10 0.043 0.019 12 9 0 3 0.105 0.073
a paired t test and sign test used to evaluate the re- sponses. The initial mean values for angles SNA, SNB, and SN-MP were within normal ranges. When the ap- pliance was inserted, the average increase of angles SNB and SN-MP were 0.98” and 3.19”, respectively. The mandibular plane to hyoid distance averaged 30.04 mm without the appliance and 27.09 mm with the ap- pliance in place. The palatal length ranged from 36.62 mm to 56.12 mm, with a mean value of 46.49 mm.
A mean increase of 2.76 mm was observed in the superior airway space when the appliance was worn. The superior posterior airway space accounted for most of this increase, with an average change of 2.21 mm. The middle airway space and the inferior airway space did not have an appreciable mean change. However,
some patients did experience an increase in the inferior airway and middle airway spaces (see Table II).
Results from the regression analysis provided two cephalomehic variables that were indicative of patient response to the appliance. The initial superior-anterior airway space was strongly indicative of change in the number of complete airway obstructions when the ap- pliance was worn (rZ = 0.83, P < 0.0001). Supero- posterior airway space was moderately indicative of change in total number of apneic events when the ap- pliance was worn (8 = 0.45, P < 0.0235).
Symptomatic improvement
Each patient and spouse or sleeping partner were questioned on their perception of the patient’s symp-
390 Bonham et al. Am. J. Orthod. Denmfac. Orthop. November 1988
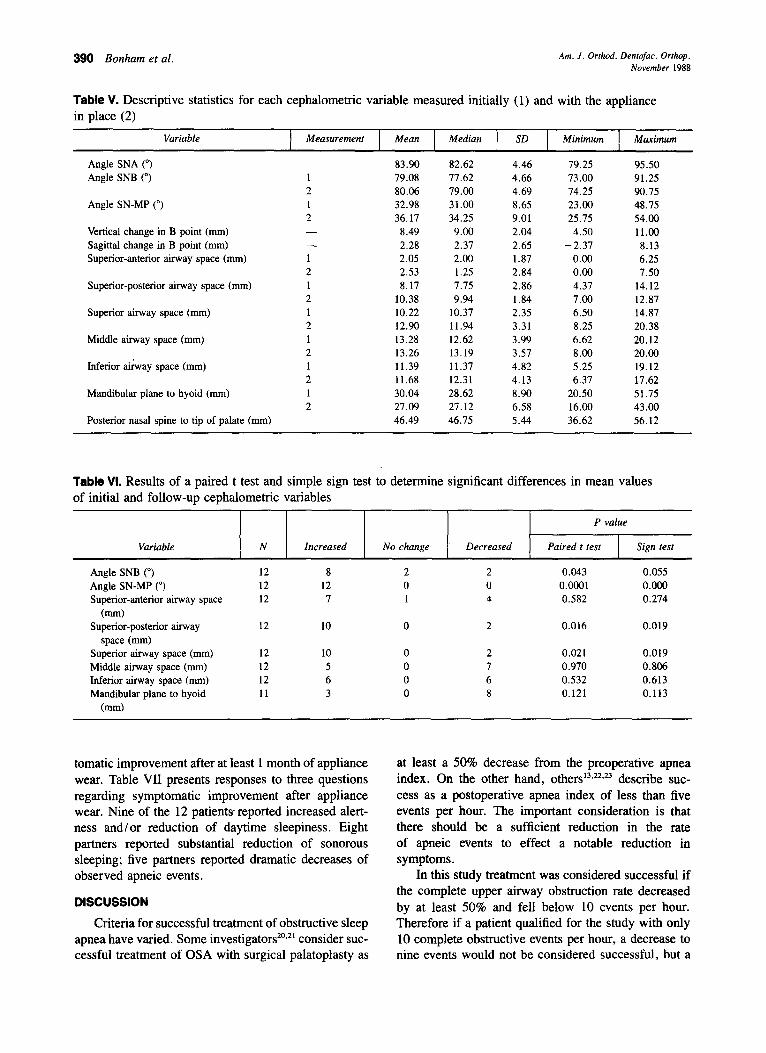
Table V. Descriptive statistics for each cephalometric variable measured initially (1) and with the appliance in place (2)
Variable
Angle SNA (“) Angle SNB (“)
Angle SN-MP (“)
Vertical change in B point (mm) Sagittal change in B point (mm) Superior-anterior airway space (mm)
Superior-posterior airway space (mm)
Superior airway space (mm)
Middle airway (mm) space
Inferior airway (mm) space
Mandibular plane to hyoid (mm)
Posterior nasal spine to tip of palate (mm)
Measurement
1 2 1 2 - - 1 2 1 2 1 2 1 2 1 2 1 2
Mean Median SD Minimum Maximum
83.90 82.62 4.46 79.25 95.50 79.08 77.62 4.66 73.00 91.25 80.06 79.00 4.69 74.25 90.75 32.98 31.00 8.65 23.00 48.75 36.17 34.25 9.01 25.75 54.00
8.49 9.00 2.04 4.50 11.00 2.28 2.37 2.65 -2.37 8.13 2.05 2.00 1.87 0.00 6.25 2.53 1.25 2.84 0.00 7.50 8.17 7.75 2.86 4.37 14.12
10.38 9.94 1.84 7.00 12.87 10.22 10.37 2.35 6.50 14.87 12.90 11.94 3.31 8.25 20.38 13.28 12.62 3.99 6.62 20.12 13.26 13.19 3.57 8.00 20.00 11.39 11.37 4.82 5.25 19.12 11.68 12.31 4.13 6.37 17.62 30.04 28.62 8.90 20.50 51.75 27.09 27.12 6.58 16.00 43.00 46.49 46.75 5.44 36.62 56.12
Table VI. Results of a paired t test and simple sign test to determine significant differences in mean values of initial and follow-up cephalometric variables
P value
Variable
Angle SNB (“) Angle SN-MP (“) Superior-anterior airway space
(mm) Superior-posterior airway
space (mm) Superior airway space (mm) Middle airway (mm) space Inferior airway (mm) space Mandibular plane to hyoid
(mm)
N Increased No change Decreased Paired t test Sign test
12 8 2 2 0.043 0.055 12 12 0 0 0.0001 0.000 12 7 1 4 0.582 0.274
12 10 0 2 0.016 0.019
12 10 0 2 0.021 0.019 12 5 0 7 0.970 0.806 12 6 0 6 0.532 0.613 11 3 0 8 0.121 0.113
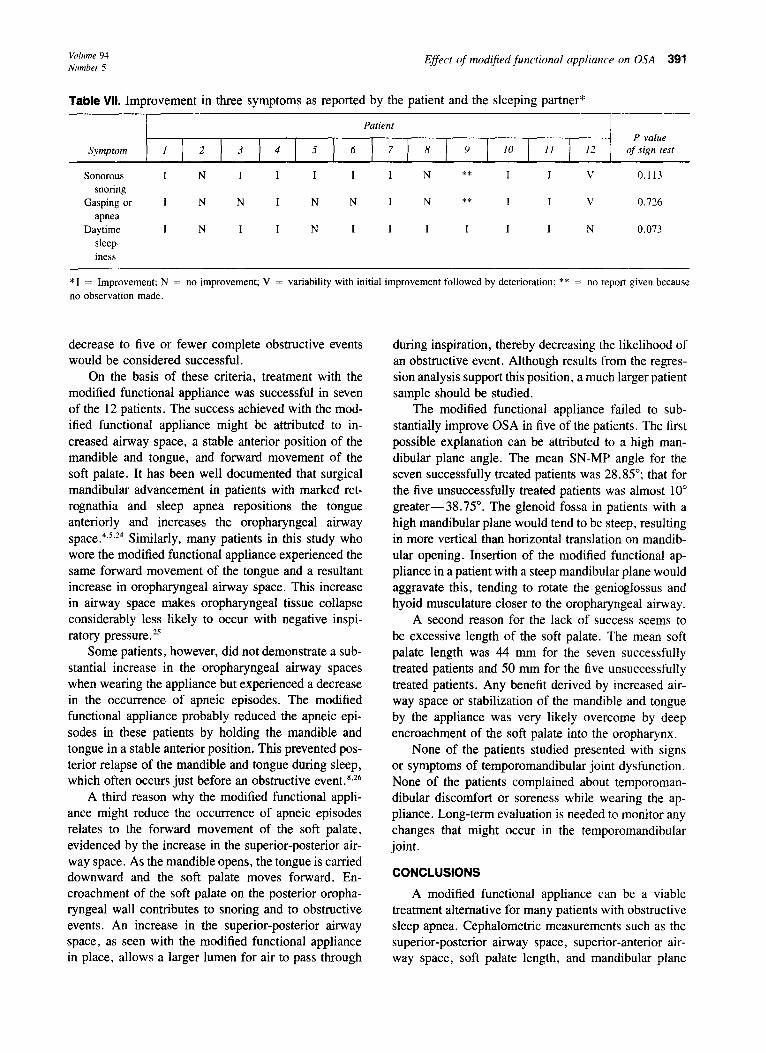
tomatic improvement after at least 1 month of appliance wear. Table VII presents responses to three questions regarding symptomatic improvement after appliance wear. Nine of the 12 patients reported increased alert- ness and/or reduction of daytime sleepiness. Eight partners reported substantial reduction of sonorous sleeping; five partners reported dramatic decreases of observed apneic events.
DISCUSSION
Criteria for successful treatment of obstructive sleep apnea have varied. Some investigators*‘.*l consider suc- cessful treatment of OSA with surgical palatoplasty as
at least a 50% decrease from the preoperative apnea index. On the other hand, others13~22~23 describe suc- cess as a postoperative apnea index of less than five events per hour. The important consideration is that there should be a sufficient reduction in the rate of apneic events to effect a notable reduction in symptoms.
In this study treatment was considered successful if the complete upper airway obstruction rate decreased by at least 50% and fell below 10 events per hour. Therefore if a patient qualified for the study with only 10 complete obstructive events per hour, a decrease to nine events would not be considered successful, but a
Volume 94 Number 5
Effect of modijied functional appliance on OSA 391
Table VII. Improvement in three symptoms as reported by the patient and the sleeping partner*
Patient P value
Symptom I 2 3 4 5 6 7 8 9 10 II 12 of sign test
sonorous I N I I I I I N ** I I \ 0.113 snoring
Gasping or 1 N N I N N I N ** I I V 0.726
apnea Daytime I N I I N I I I I I I N 0.073
sleep- iness
*I = Improvement; N = no improvement; V = variability with initial improvement followed by deterioration; ** = no report given because no observation made.
decrease to five or fewer complete obstructive events would be considered successful.
On the basis of these criteria, treatment with the modified functional appliance was successful in seven of the 12 patients. The success achieved with the mod- ified functional appliance might be attributed to in- creased airway space, a stable anterior position of the mandible and tongue, and forward movement of the soft palate. It has been well documented that surgical mandibular advancement in patients with marked ret- rognathia and sleep apnea repositions the tongue anteriorly and increases the oropharyngeal airway space. 4s~24 Similarly, many patients in this study who wore the modified functional appliance experienced the same forward movement of the tongue and a resultant increase in oropharyngeal airway space. This increase in airway space makes oropharyngeal tissue collapse considerably less likely to occur with negative inspi- ratory pressure.”
Some patients, however, did not demonstrate a sub- stantial increase in the oropharyngeal airway spaces when wearing the appliance but experienced a decrease in the occurrence of apneic episodes. The modified functional appliance probably reduced the apneic epi- sodes in these patients by holding the mandible and tongue in a stable anterior position. This prevented pos- terior relapse of the mandible and tongue during sleep, which often occurs just before an obstructive event.8.26
A third reason why the modified functional appli- ance might reduce the occurrence of apneic episodes relates to the forward movement of the soft palate, evidenced by the increase in the superior-posterior air- way space. As the mandible opens, the tongue is carried downward and the soft palate moves forward. En- croachment of the soft palate on the posterior oropha- ryngeal wall contributes to snoring and to obstructive events. An increase in the superior-posterior airway space, as seen with the modified functional appliance in place, allows a larger lumen for air to pass through
during inspiration, thereby decreasing the likelihood of an obstructive event. Although results from the regres- sion analysis support this position, a much larger patient sample should be studied.
The modified functional appliance failed to sub- stantially improve OSA in five of the patients. The first possible explanation can be attributed to a high man- dibular plane angle. The mean SN-MP angle for the seven successfully treated patients was 28.85”; that for the five unsuccessfully treated patients was almost 10 greater-38.75“. The glenoid fossa in patients with a high mandibular plane would tend to be steep, resulting in more vertical than horizontal translation on mandib- ular opening. Insertion of the modified functional ap- pliance in a patient with a steep mandibular plane would aggravate this, tending to rotate the genioglossus and hyoid musculature closer to the oropharyngeal airway.
A second reason for the lack of success seems to be excessive length of the soft palate. The mean soft palate length was 44 mm for the seven successfully treated patients and 50 mm for the five unsuccessfully treated patients. Any benefit derived by increased air- way space or stabilization of the mandible and tongue by the appliance was very likely overcome by deep encroachment of the soft palate into the oropharynx.
None of the patients studied presented with signs or symptoms of temporomandibular joint dysfunction. None of the patients complained about temporoman- dibular discomfort or soreness while wearing the ap- pliance. Long-term evaluation is needed to monitor any changes that might occur in the temporomandibular joint.
CONCLUSIONS
A modified functional appliance can be a viable treatment alternative for many patients with obstructive sleep apnea. Cephalometric measurements such as the superior-posterior airway space, superior-anterior air- way space, soft palate length, and mandibular plane
392 Bonham et al.
angle might be used in patient selection to improve success rates with this appliance. As more is learned from extended use, this new conservative treatment alternative should achieve a solid position among other treatment modalities.
A team approach to management of the patient with obstructive sleep apnea currently includes the support of the otolaryngologist, pulmonologist, neurologist, and sleep laboratory clinician. More recently, consistent use of cephalometric analysis has been recommended to aid in diagnosis and treatment planning for OSA patients. This, coupled with the new and promising treatment alternative of the modified functional appliance, would suggest that the orthodontist could contribute to the team management of these patients.
We would like to extend thanks to Dr. Donald Parker for assistance with the statistical analysis, and Ms. Claudette Vermillion for valuable assistance with preparation of the manuscript.
REFERENCES 1. Mezon BJ, West P, Maclean JP, Druyger MH. Sleep apnea in
2
3.
4.
5.
6.
I.
8.
9.
10.
acromegaly. Am J Med 1980;69:615-9: Perks WH, Horrocks PM, Cooper RA, et al. Sleep apnea in acromegaly. Br Med J 1980;280:894-6. Imes NK, Orr WC, Smith RO, Rogers RM. Retrognathia and sleep apnea: a life threatening condition masquerading as nar- colepsy. JAMA 1977;237: 1596-7. Bear SE, Priest JH. Sleep apnea syndrome: correction with sur- gical advancement of the mandible. J Oral Surg 1980;38:543-9. Kuo PC, West RA, Bloomquist DS, McNeil RW. The effect of mandibular osteotomy in three patients with hypersomnia sleep apnea. Oral Surg Oral Med Oral Path01 1979;48:385-92. Johnston C, Taussig IM, Koopman C, Smith P, Bjelland J. Ob- structive sleep apnea in Treacher-Collins syndrome. Cleft Palate J 1981;18:39-44. Afzelius L, Elmquist D, Laurin S, Risberg AM, Aberg M. Sleep apnea caused by acromegalia and treatment with reduction plasty of the tongue. ORL J Otorhinolaryngol Relat Spec 1982;42: 142-5.
Remmers JE, DeGroot WJ, Sauerland EK, Anch AM. Patho- genesis of upper airway occlusion during sleep. J Appl Physiol 1978;44:931-8.
Gastaut H, Tassinari CA, Duron B. Polygraphic study of the episodic diurnal and nocturnal (hypnic and respiratory) mani- festations of the Pickwick syndrome. Brain Res 1966;2:167-86. Gastaut H, Duron B, Tassinari CA, Lyagoubi S, Saier J. Mech- anism of the respiratory pauses accompanying slumber in the Pickwickian syndrome. Activ Nerv Sup 1969;11:209-15.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
Am. J. Orthod. Dentofac. Orthop. November 1988
Strohl KP, Saunders NA, Sullivan CE. Sleep apnea syndromes. In: Saunders NA, Sullivan CE, eds. Sleep and breathing. New York: Marcel Dekker Inc., 1984;365-402. Imaizumi T. Arrhythmias in sleep apnea. Am Heart J 1980; 100:513-6. Fujita S, Conway W, Zorick F, Roth T. Surgical correction of anatomic abnormalities in obstructive sleep apnea syndrome: uvulopalatopharyngoplasty. Otolaryngol Head Neck Surg 1981; 891923-34. deBetry-Borowiecki B, Kukwa AA, Blanks RH. Indications for palatophatyngoplasty. Arch Otolatyngol 1985:111:659-63. Sullivan CE, Berthon-Jones M, Issa FG, Eves L. Reversal of obstructive sleep apnea by continuous positive airway pressure applied through the nares. Lancet 1981;1:862-5. Cartwright RD, Samelson CF. The effect of a nonsurgical treat- ment for sleep apnea: the tongue retaining device. JAMA 1982;248:705-9.
Orr WC, Imes NK, Martin RJ. Progesterone therapy in obese patients with sleep apnea. Arch Intern Med 1979;139: 109-l 1. Sol1 BA, George PT. Treatment of obstructive sleep apnea with a nocturnal airway patency appliance. N Engl J Med 1985; 313:386-7. George PT. A modified functional appliance for treatment of obstructive sleep apnea. J Clin Orthod 1987;21:171-5. Zorick R, Roehrs T, Conway W, Fujita S, Wittig R, Roth T. Effect of uvulopalatopharyngoplasty on the daytime sleepiness associated with sleep apnea syndrome. Bull Eur Physiopathol Respir 1983;19:600-3. Simmons F, Guilleminault C, Silvestri R. Snoring and some obstructive sleep apneas can be cured by oropharyngeal surgery. Arch Otolaryngol 1983;109:503-7. Silvestri R, Guilleminault C, Simmons F. Palatopharyngoplasty in treatment of obstructive sleep apneic patients. In: Guillemi- nault C, Lugaresi E, eds. Sleep wake disorders: natural history, epidemiology, and long-term evaluation. New York: Raven Press Inc, 1983. Sher AE, Thorpy MJ. Shprintzen RJ, Spielman AJ, Burack B, McGregor PA. Predictive value of Muller maneuver in selection of patients for uvulopalatopharyngoplasty. Laryngoscope 1985; 95:1483-6. Riley R, Guilleminault C, Powell N, Derman S. Mandibular osteotomy and hyoid bone advancement for obstructive sleep apnea syndrome. Sleep 1984;7:70-82. Rivlin J, Hoffstein V, Kalbfleisch J, McNicholas W, Zamel N, Bryan AC. Upper airway morphology in patients with idiopathic obstructive sleep apnea. Am Rev Respir Dis 1984;129:355-60.
26. Sauerland EK, Orr WC, Hairston LE. EMG patterns of oropha- ryngeal muscles during respiration and sleep. Electromyogr Clin Neurophysiol 1981;21:279-86.
Reprint requests to: Dr. Paul E. Bonham 6200 S. McClintock, Suite 4 Tempe, AZ 85283





























