Embed Size (px)
Citation preview

The Effect of Emergency DepartmentCrowding on Education: Blessing or Curse?Philip Shayne, MD, Michelle Lin, MD, Jacob W. Ufberg, MD, Felix Ankel, MD, Kelly Barringer, MD,Sarah Morgan-Edwards, MD, Nicole DeIorio, MD, and Brent Asplin, MPH, MD
AbstractEmergency department (ED) crowding is a national crisis that contributes to medical error and systeminefficiencies. There is a natural concern that crowding may also adversely affect undergraduate andgraduate emergency medicine (EM) education. ED crowding stems from a myriad of factors, and indi-vidually these factors can present both challenges and opportunities for education. Review of the medi-cal literature demonstrates a small body of evidence that education can flourish in difficult clinicalenvironments where faculty have a high clinical load and to date does not support a direct deleteriouseffect of crowding on education. To provide a theoretical framework for discussing the impact of crowd-ing on education, the authors present a conceptual model of the effect of ED crowding on educationand review possible positive and negative effects on each of the six recognized Accreditation Council forGraduate Medical Education (ACGME) core competencies.
ACADEMIC EMERGENCY MEDICINE 2009; 16:76–82 ª 2008 by the Society for Academic EmergencyMedicine
Keywords: emergency medicine, emergency department, crowding, education
E mergency department (ED) crowding is anational crisis. Between 1992 and 2003, the num-ber of ED visits rose by 27% nationally, or close
to 2 million visits each year.1,2 Concurrently, there was anet loss of more than 1,100 EDs between 1998 and 2002.3
In addition, the patients presenting to our EDs are olderand present with more complex medical issues with eachpassing year, further stressing the national emergencycare system.
Emergency department crowding is a complicatedphenomenon that encompasses multiple causes and hasmany manifestations.4 Crowding is not just a factor ofthe influx of new patients or the number of patients onED gurneys, in hallways, and in waiting areas, but alsoof patients’ time waiting to be seen by a health careprofessional, ED length of stay (LOS), turnaround timesof essential tests and studies, and time waiting to beadmitted to a hospital bed or an operating room.Ambulance diversion time may or may not limit theimpact of additional patients on the ED, but passes thestresses to other hospitals in the region. For this report,we will adopt the American College of Emergency Phy-sicians’ definition of crowding: ‘‘Crowding occurs whenthe identified need for emergency services exceedsavailable resources for patient care in the emergencydepartment, hospital, or both.’’5
As our hospitals become more crowded, admittedand often critically ill patients ‘‘board’’ in the ED untilan inpatient bed becomes available.6 In one survey ofnational EDs, 91% of 575 respondents reported thatcrowding was a problem, and 40% reported a problemwith crowding on a daily basis.7 With crowding beingsuch a pervasive problem across many EDs in theUnited States, the concern is that this may negatively
ISSN 1069-6563 ª 2008 by the Society for Academic Emergency Medicine76 PII ISSN 1069-6563583 doi: 10.1111/j.1553-2712.2008.00261.x
From the Department of Emergency Medicine, Emory Univer-sity (PS), Atlanta, GA; the Department of Emergency Medicine,University of California San Francisco and San FranciscoGeneral Hospital (ML), San Francisco, CA; the Department ofEmergency Medicine, Temple University (JWU), Philadelphia,PA; the Department of Emergency Medicine, Regions Hospital(FA, KB, BA), St. Paul, MN; the Department of EmergencyMedicine, University of New Mexico (SME), Albuquerque, NM;and the Department of Emergency Medicine, Oregon Healthand Science University (ND), Portland, OR.The Society for Academic Emergency Medicine (SAEM)Crowding Taskforce Education Workgroup consists of LouisBinder, MD, James Creel, MD, Susan Farrell, MD, JonathanFisher, MD, Sean Kelley, MD, and Peter Sokolove, MD.Received April 23, 2008; revision received June 29, 2008;accepted July 16, 2008.Presented at the SAEM Academic Assembly in Washington,DC, May 31, 2008.This manuscript has been reviewed and approved by the SAEMBoard of Directors, April 2008.Address for correspondence and reprints: Philip Shayne, MD;e-mail: [email protected] related commentary appears on page 56.

impact the ability of emergency care providers tomanage the growing numbers of ED patients in a safeand efficient manner. Furthermore, crowding may alsoimpact the educational environment of the ED.
The ED provides a wealth of clinical educationalopportunities for medical students, residents, and otherlearners. Clinical education, as defined by the Associa-tion of American Medical Colleges (AAMC) encom-passes the acquisition of medical knowledge, skills, andattitudes needed to achieve competency.8 The ED is anideal environment to provide learners with a uniqueexposure to undifferentiated patients, a variety of acutepresentations, multitasking experience, skill develop-ment, an interdisciplinary team approach to patientcare, and a basic set of technical procedures. This isaccomplished through clinical experiences tied to bed-side teaching9–12 and feedback.13–16 Emergency medi-cine (EM) also has the natural advantage of the 24 · 7presence of faculty in the ED. While current educa-tional trends have focused on learner competencyassessment tools to measure educational outcomes17
and healthy learning environments,18 little is knownabout the effects of ED crowding on undergraduateand graduate EM education.
The Society for Academic Emergency Medicine(SAEM) ED Crowding Taskforce was given an objectiveof reviewing the current evidence on the effects of EDcrowding on clinical education and providing a frame-work for future research. In this article, we attempt tosummarize the existing evidence regarding the effect ofcrowding on EM education, discuss the current EMlearning environment, and present a conceptual modelof the effect of ED crowding on education. This concep-tual model helps to provide a theoretical framework fordiscussions regarding the impact of ED crowding oneducation.
STATE OF THE ART
Although there is ample anecdotal experience that hos-pital crowding negatively impacts education, there islittle evidence examining ED crowding’s impact on edu-cation. A major reason for this paucity of data lies inthe difficulty in objectively measuring ED crowding, thediversity in teacher and student learning styles, and thelack of reliable methods for measuring educational out-comes. Heins et al.19 conducted an extensive literaturesearch in 2005 on ED crowding’s impact on education.Their search methodology used ‘‘emergency medicine’’in three of their four literature search approaches. Weaimed to conduct a broader search to also includepublications based outside of and within the field ofEM. Our literature search strategy involved a PubMedsearch for the 10-year period of 1998–2008. Nine pairedkeyword searches were used, with one of the keywordsfrom Group A (crowding, overcrowding, productivity)and one of the keywords from Group B (education,teaching, learning). These paired keyword searcheswere ‘‘crowding AND education’’ (505 citations),‘‘crowding AND teaching’’ (369 citations), ‘‘crowdingAND learning’’ (78 citations), ‘‘overcrowding AND edu-cation’’ (85 citations), ‘‘overcrowding AND teaching’’(82 citations), ‘‘overcrowding AND learning’’ (12 cita-
tions), ‘‘productivity AND education’’ (4,078 citations),‘‘productivity AND teaching’’ (3,483 citations), and‘‘productivity AND learning’’ (1,773 citations). Individualpublications were reviewed and assessed for relevancyto the topic of ED crowding and their impact onmedical education. References within the relevantpublications were reviewed to find additional articlesnot discovered in the electronic search. A small body ofevidence shed some light on aspects of the potentialchallenges and benefits to bedside teaching andfeedback that result from ED crowding.
A major component of education in the ED stemsfrom focused bedside teaching. It would seem logicalthat time spent on bedside teaching may be compro-mised if ED crowding results in EM faculty having tofocus more on patient care and flow. We found no ED-based studies supporting this perspective, but foundtwo prospective studies outside of the field of EM thatsuggest that characteristics associated with crowdingmay negatively impact the educational value of the clin-ical experience. In pediatric subspecialty clinics, surveysof 30 residents demonstrated that less efficient clinics,as defined by prolonged patient stays and delayedworkups, directly correlated with a lower educationalvalue score.20
A second study evaluated the quantity of teachingperformed by anesthesia faculty in the operating roomsetting, as assessed by an independent observer. Basedon 1,558 operative cases, there was a 33% decrease inteaching interactions between the faculty and the resi-dent when the faculty member concurrently directedcare in more than one room. Decreased faculty-to-patient ratios correlated with decreased teachingtime.21
These studies shed light on crowding’s potentialimpact on education in the ED. Because multiple stud-ies have demonstrated that ED crowding results indelayed patient care and operational inefficiencies,22–24
the first study might suggest that ED crowding detractsfrom the educational experience. Similarly, the latterstudy might suggest that a crowded, high census EDswith low faculty-to-patient ratios would result in lessteaching and thus detract from the overall quality ofthe educational experience in the ED.
However, in contrast to these findings, two prospec-tive survey studies that were conducted in the ED sug-gest that crowding did not affect the learners’perception of faculty teaching quality. Kelly et al.25
found that skilled EM faculty received high teachingevaluation scores from EM residents independent ofthe faculty members’ clinical work load and ED census.Similarly Berger et al.26 demonstrated that highly ratedEM faculty received excellent medical student teachingevaluations regardless of the faculty members’ clinicalproductivity, indirectly measured by the relative valueunits (RVU) generated per hour.26 Based on the out-come measure of learner perception regarding teachingquality, these two studies suggest that excellent educa-tors will remain excellent educators independent ofclinical productivity, contrary to the aforementionedpediatric and anesthesia studies.20,21
More robust studies are needed to characterize therelationship between education and crowding in the ED,
ACAD EMERG MED • January 2009, Vol. 16, No. 1 • www.aemj.org 77

using more rigorous educational measures. Additionally,the relationship of clinical productivity as defined byRVU generated to degree of crowding is unclear.
CONCEPTUAL MODELING OF ED CROWDINGAND EDUCATION
There is a concern within the academic EM communitythat strained conditions in the clinical setting mayimpact the quality of education for EM learners. Inaddition to EM residents, the ED is a valuable trainingenvironment for residents from other specialties, medi-cal students, nursing students, allied health students,and military personnel. The ED is also a natural drawfor nonmedical personnel first considering a career inmedicine. Factors that impact ED function, such as per-formance and efficiency, can influence those drawnthere to learn.
The multifactorial challenges to ED capacity, suchas patient volume, patient illness acuity, LOS, andboarding, can be considered to be both additive anddetrimental to education. Medical education dependsheavily on experiential learning and thus relies onadequate clinical opportunities and exposure. Theaccrediting authority for U.S. and Canadian medicalschools, the Liaison Committee for Medical Education(LCME), has published ‘‘Functions and Structure of aMedical School’’ that emphasizes the importance ofproviding medical students with the depth andbreadth of clinical exposure necessary to obtain com-petency for graduation.27 Similarly, the AccreditationCouncil for Graduate Medical Education (ACGME)Resident Review Committee for Emergency Medicine(RRC-EM), in their special program requirements,places threshold minimums on ED patient populationencounters for learners. For institutions wishing tohost accredited residency training programs, programdirectors are required to report admission rates andacuity levels.28 Accreditation is also contingent uponachieving certain threshold numbers of core proce-dures and participation in resuscitations. The educa-tional assumption has been that these minimums areobjective benchmarks for training experience and thereal-life exposure to emergency care that is necessaryto obtain competence in an apprentice model of med-ical education. It is the excess of these very importantand necessary opportunities that in turn can causeconditions of ED crowding.
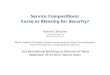
The instinctive concern is that crowding and strainedED capacity brings too much of a ‘‘good thing.’’ Whileincreasing clinical opportunities might bring a compa-rable increase in competency, is there some break-pointwhere increased clinical loads disrupt the educationalprocess? We can hypothesize three conceptual modelscenarios with a ‘‘Starling curve’’–type relationshipbetween the factors that contribute to ED crowdingand education (Figure 1). For all three scenarios, a cer-tain degree of exposure to patient volume, illness acu-ity, and complexity of care is necessary to achieveeducational goals and produce autonomously function-ing and experienced medical practitioners. This is dem-onstrated in the initial upslope of each curve (Point A).If achieving competence in emergency care is at all
linked to the number of ill patients that a learner caresfor, increased patient volume and acuity will increasethe pace at which that goal is obtained.
In Scenario B of Figure 1, crowding could continuallyprovide educational opportunities and experiencesdespite deteriorating ED operational processes. In Sce-nario C, the quality of education could plateau to a the-oretical steady-state level, where the benefits fromincreased patient volume and acuity are offset by thelimited resources and educational time. In Scenario D,crowding may outstrip the resources and time availablefor educational opportunities. In the same way thatpatient safety and quality of care suffer, so may thequality of medical education. There may be a theoreticaloptimal crowding capacity to best achieve educationalgoals.
The different possible models on this education–crowding curve are not necessarily mutually exclusive.The effect of crowding on education can be learner-,teacher-, and institution-dependent. A less crowded EDcan afford the opportunity for longer, more in-depthdiscussion of case management, for instance. This set-ting would attract both faculty and learners for whomthat is a good learning style. A more crowded ED maypresent less time for discussion, but more opportunityto hone communication and decision-making skills,resource utilization, and leadership ability and therebybenefit a different set of teachers and learners. EMtraining programs clearly differentiate themselves bytheir clinical settings, and both EM faculty and resi-dents can select a practice environment that suits theirindividual teaching or learning style. This would miti-gate potential disadvantages and heighten advantagesof more or less crowded EDs. For those medical stu-dents and residents who are unable to select their EDlearning environment, however, the potential disadvan-tages may be more pronounced because of less com-patible learning styles.
Stated in the framework of the core competencies,less crowded EDs may offer learners in-depth opportu-nities to focus on medical knowledge and individualpatient care competencies, while more crowded EDs
Figure 1. Possible effects of crowding on quality of EDeducation.
78 Shayne et al. • ED CROWDING AND EDUCATION

may offer learners in-depth opportunities to focus onmultitasking, patient care skills, communication skills,professionalism, and system-based practice competen-cies. If this is true, emergency medical education bene-fits from a diversity of settings and experience that maysuit different types of learners.
As outlined in the previous section, there are insuffi-cient data to support any of these models. To develop aresearch agenda to elicit the real-world effect of crowd-ing on education, it is necessary to understand the fac-tors in which the training environment can promote orcompromise medical education. Competence in EM isdifficult to measure, but we can view it through theprism of the ACGME outcome project28 as comprisingpatient care, medical knowledge, practice-based learn-ing and improvement, interpersonal and communica-tion skills, professionalism and system-based practice.Table 1 summarizes the potential positive and negativeimpact of crowding on EM education by the ACGMEcore competencies, which are discussed in depthbelow.
Patient CareThe path toward competency in patient care is clearlyenhanced during the early upstroke in ED crowdingfactors. More patients bring greater exposure to a widevariety of clinical pathology and create more opportuni-ties for clinical learning and teaching. Cognitive psy-chologists discuss ‘‘illness scripts’’ as chunks ofinformation that physicians can quickly move betweenshort and long-term memory.29 Development of exper-tise is based on a large and elaborate number of illnessscripts that physicians can draw upon. More patientsprovide more opportunities for decision-making, auton-omous responsibilities, and developing these illnessscripts.
A greater number of acutely ill patients translate intomore opportunities to perform procedures and conductresuscitations. Boarding allows for the opportunity tofollow the longitudinal course of the critically ill andinjured and to observe the effects of therapy. These fac-tors can enhance the knowledge base of ED residentsand students. Crowding allows faculty to serve as rolemodels in multitasking and prioritization—skills thatlearners will need to master to succeed in clinicalpractice.
Potential disadvantages to ED crowding include apossible decrease in new patient census as morepatients are boarded in the ED and more ambulancesare diverted. Crowding can make it difficult to providemedical care in a safe and timely manner, according toaccepted clinical standards. Also, there is the potentialfor decreased attention to patient education, risk reduc-tion, and patient counseling as ED crowding worsens.Inappropriate modeling of medical care provision hasthe potential for devastating effects on the training ofmedical students and residents. Less faculty time maybe available to observe and offer feedback to learners.This lack of feedback diminishes the faculties’ ability toproperly mold the learner. Finally, as pressures ofpatient care mount in combination with research andteaching requirements, more faculty members mayleave for community practice—the loss of a valuableeducational resource.
Medical KnowledgeMedical knowledge is enhanced by increased patientvolume and corresponding patient variety. In theapprentice model of education, knowledge is solidifiedthrough direct contact with a patient with the diseaseprocesses. If ED crowding causes a decrease in thenew patient census, ED faculty and learners have more
Table 1Potential Consequences of ED Crowding on Education by ACGME Core Competency
PC MK PBLI ICS Pr SBP
Positive effectsBroader exposure to clinical presentations X X X X X XBroader exposure to patient diversity X X XMore opportunities for decision-making X X XMore autonomy in decision-making X X XMore procedures and resuscitations X X X XBoarding allows learner to follow time course of disease X X XIncreased multitasking required X X XFace adverse circumstances similar to potential future practice X X XIncreased emphasis on efficiency and patient flow X X X
Negative effectsDecrease in new patient volume X X XLess time to spend per patient and reflect on lessons X X X X XLess time counseling and educating patients X X XProviders became taxed, exhausted X X X X X X’’Normalization’’ of decreased expectations for patient care and privacy X X X X XLess faculty supervision of learners leading to increased errors and decreased patient safety X X X XLess time for faculty to observe and provide learner feedback X X X X X XLess time for learners to observe faculty demonstrating professionalism skills X X
ACGME = Accreditation Council for Graduate Medical Education; ED = emergency department; ICS = interpersonal and commu-nication skills; MK = medical knowledge; PBLI = problem-based learning and improvement; PC = patient care; Pr = professional-ism; SBP = systems-based practices.
ACAD EMERG MED • January 2009, Vol. 16, No. 1 • www.aemj.org 79

time to spend discussing the patients seen. In contrast,if crowding spreads the supervision thin, it can nega-tively impact the amount of time that is available forfaculty contact and teaching opportunities.
Practice-based Learning and ImprovementPractice-based learning can be improved as crowdingforces academic centers to address barriers to provid-ing efficient and timely patient care. Application of sci-entific evidence can improve patient flow and can alsospur further scientific inquiry. ED crowding is often amanifestation of hospital crowding and requires a hos-pitalwide and health care systemwide solution. Alter-nately, the factors that cause crowding can disrupt thetime needed to reflect and learn from current practice.
Interpersonal and Communication SkillsEffective, caring interpersonal and communication skillswhile taking care of multiple patients is a key require-ment of emergency physicians (EPs). Interpersonal andcommunication skills are critical in being able to obtainpatient histories in a timely and efficient manner, buildtrust and rapport quickly with patients and families,interact with colleagues, and develop a comprehensiveplan of care compassionately with patients. Crowdingcan enhance the acquisition and practice of theseimportant skills both by increased practice and the needto make each contact meaningful. However, when EDproviders become taxed, humanistic priorities may besubsumed by pragmatic needs. Faculty have feweropportunities to model appropriate communicationskills and frustrated and exhausted physicians may haveless capacity for modeling compassion and concern.
ProfessionalismThe development of professionalism requires a varietyof exposures to clinical situations. A high ED censusimproves exposure to a diverse patient population andincreases the opportunity for observation, modeling,and attainment of ethical professional practice stan-dards. However, the physical plant limitations in acrowded ED can compromise patient privacy. Forinstance, sensitive information may be discussed withthe patient while the patient is in the hallway. Further-more, the presence of family members may be curtailedin the patient care areas due to crowded conditions.This has the potential to compromise the perceived eth-ical norms and produce a culture of reduced expecta-tions in the eyes of the impressionable learner.
Systems-based PracticeEmergency department crowding offers a direct insightinto societal decisions on health care and disease. Thissystems-based knowledge can be used by an EP to actas an agent for change within the health care arena onbehalf of patients and learners in the ED. Finding solu-tions to ED and hospital crowding can provide uniqueopportunities for learners and other interested individu-als to get involved at the hospital level and beyond.Certainly the experience of performing in a crowdedED is the best preparation for a practice in similar con-ditions. However, systems-based problems can limit theprovision of clinical care at acceptable clinical stan-
dards due to lack of resources at ED, inpatient, and out-patient settings. Learners may not develop a commandof state of the art care and instead develop decreasedexpectations. This has grave implications when trainingthe next generation of physicians, physicians’ assistants,nurse practitioners, nurses, paramedics, and emergencymedical technicians.
In summary, the effects of crowding have the poten-tial to affect all facets of competency training in the ED.Increased volume, LOS, acuity, and simulation of ‘‘real-world’’ or community experiences have the potential tobe both positive and negative factors in medical train-ing. A diversity of clinical training environments allowsfor faculty and learners to gravitate toward a settingthat best suits their learning style. While we can theo-rize a potential detriment to education at either low orhigh extremes of the crowding spectrum, there is insuf-ficient literature to support either conclusion.
RESEARCH AGENDA
As Heins et al. noted in 2005,19 many opportunitiesexist for future research on the effect of crowding oneducation that remain uninvestigated. They commentthat ‘‘[t]he optimal method to study the effect of EDcrowding on education would be an extensive, multi-center study using validated measures of crowding,clinical teaching effectiveness, and learners’ educationaloutcomes.’’ As of 2008, we have seen little progress.The difficulty in measuring education and learningobjectively contributes to this slow progress. Nonethe-less, the question of crowding’s impact on educationneeds to be answered.
One approach to evaluating education in the settingof a crowded ED is to apply Kirkpatrick’s four-tieredhierarchy in training evaluation (Figure 2). On the low-est end of the hierarchical approach and as the easiesttool to implement, one can evaluate the learner’s reac-tion to the training or learning environment. This wasthe approach taken by the two ED-based studies evalu-ating learners’ assessment of faculty teaching withrespect to crowding.25,26 Next, the hierarchy progressesto an evaluation of learning using a validated instru-ment in both a less crowded and more crowded ED set-ting. The third level in the hierarchy is an evaluation ofbehavior, assessing whether the knowledge learnedtransferred to measurable behavioral actions in both aless crowed and more crowded ED setting. Finally, thefourth level is an evaluation of results, assessed byobjective patient care indicators.30
Another area for research includes assessing whetherthe crowded ED work environment influences a medi-cal student’s decision to select EM as a career choice.The quality of education and educators in the medicalspecialty may be directly linked to recruiting the mostcompetitive medical students into that field.31
SUMMARY
Emergency department crowding presents both oppor-tunities for and challenges to education. Although littleevidence currently exists to quantify the risks and bene-fits to education, we can hypothesize a variety of effects
80 Shayne et al. • ED CROWDING AND EDUCATION

across the entire spectrum of student and residenttraining, based on our theoretical crowding–educationmodel. Academic institutions need to be aware of thebenefits and downsides of their particular point on thecrowding curve to both select the best learners for theirenvironment and to actively mitigate negative factors.Regulatory bodies need to be careful to make balanced,evidenced-based decisions on guidelines involvingcrowding parameters to allow for a diversity of trainingenvironments. Validated measures of both crowdingand education will facilitate future research effects ofcrowding on student and resident education in the ED.
References
1. Burt CW, McCaig LF. Trends in hospital emergencydepartment utilization: United States, 1992–99. Vital& Health Statistics - Series 13: National HealthSurvey. 2001; (150):1–34.
2. McCaig LF, Burt CW. National Hospital AmbulatoryMedical Care Survey: 2003 emergency departmentsummary. Adv Data. 2005; (358):1–38.
3. American College of Emergency Physicians. Emer-gency Medicine Statistical Profile. Available from:http://www.acep.org/. Accessed Jul 18, 2008.
4. Asplin BR, Magid DJ, Rhodes KV, Solberg LI,Lurie N, Camargo CA Jr. A conceptual model ofemergency department crowding. Ann Emerg Med.2003; 42:173–80.
5. American College of Emergency Physicians.Crowding. Ann Emerg Med. 2006; 47:585.
6. General Accounting Office. Hospital EmergencyDepartments: Crowded Conditions Vary amongHospitals and Communities. Washington, DC: Uni-ted States General Accounting Office, 2003, p 1–70.
7. Derlet R, Richards J, Kravitz R. Frequent over-crowding in U.S. emergency departments. AcadEmerg Med. 2001; 8:151–5.
8. Nutter D, Whitcomb M. The AAMC Project on theClinical Education of Medical Students. Availableat: http://www.aamc.org/meded/clinicalskills/start.htm. Accessed Jul 18, 2008.
9. Aldeen AZ, Gisondi MA. Bedside teaching in theemergency department. Acad Emerg Med. 2006;13:860–6.
10. Ismach RB. Teaching evidence-based medicine tomedical students. Acad Emerg Med. 2004; 11:e6–10.
11. Kaji A, Moorhead JC. Residents as teachers in theemergency department. Ann Emerg Med. 2002;39:316–8.
12. Penciner R. Clinical teaching in a busy emergencydepartment: strategies for success. Can J EmergMed. 2002; 4:286–8.
13. Coates WC. An educator’s guide to teaching emer-gency medicine to medical students. Acad EmergMed. 2004; 11:300–6.
14. Moorhead R, Maguire P, Thoo SL. Giving feedbackto learners in the practice. Austr Fam Phys. 2004;33:691–5.
15. Paukert JL, Richards ML, Olney C. An encountercard system for increasing feedback to students.Am J Surg. 2002; 183:300–4.
16. Richardson BK. Feedback. Acad Emerg Med. 2004;11:e1–5.
17. King RW, Schiavone F, Counselman FL, Panacek EA.Patient care competency in emergency medicinegraduate medical education: results of a consensusgroup on patient care. Acad Emerg Med. 2002;9:1227–35.
18. Jagsi R, Shapiro J, Weissman JS, Dorer DJ,Weinstein DF. The educational impact of ACGMElimits on resident and fellow duty hours: a pre-postsurvey study. Acad Med. 2006; 81:1059–68.
19. Heins A, Farley H, Maddow C, Williams A. AResearch Agenda for Studying the Effect of Emer-gency Department Crowding on Clinical Education.Acad Emerg Med. 2005; 12:529–31.
20. Belamarich PF, Skae CC, Ozuah PO. Resident edu-cation and clinic efficiency. Med Educ. 2007;41:1100–1.
21. Davis EA, Escobar A, Ehrenwerth J, et al. Residentteaching versus the operating room schedule: anindependent observer-based study of 1558 cases.Anesth Analg. 2006; 103:932–7.
22. Pines JM, Hollander JE. Emergency departmentcrowding is associated with poor care for patientswith severe pain. Ann Emerg Med. 2008; 51:1–5.
23. Pines JM, Localio AR, Hollander JE, et al. Theimpact of emergency department crowding mea-sures on time to antibiotics for patients with com-munity-acquired pneumonia. Ann Emerg Med.2007; 50:510–6.
24. Schull MJ, Vermeulen M, Slaughter G, Morrison L,Daly P. Emergency department crowding andthrombolysis delays in acute myocardial infarction.Ann Emerg Med. 2004; 44:577–85.
25. Kelly S, Shapiro N, Woodruff M, Corrigan K,Sanchez LD, Wolfe RE. The effects of clinical work-load on teaching in the emergency department.Acad Emerg Med. 2007; 14:526–31.
Figure 2. Kirkpatrick’s Hierarchy of Learning. Evaluation ofreaction (satisfaction or happiness). Donald Kirkpatrick’s four-level measurement model has been widely published in manyarticles and its terminology is well-known to most trainingprofessionals. The original model was published in Trainingand Development Handbook. Craig RL (ed.). New York, NY:McGraw-Hill, 1967.
ACAD EMERG MED • January 2009, Vol. 16, No. 1 • www.aemj.org 81

26. Berger T, Ander DS, Terrell ML, Berle DC. Theimpact of the demand for clinical productivity onstudent teaching in academic emergency depart-ments. Acad Emerg Med. 2004; 11:1364–7.
27. Liaison Committee on Medical Education. Functionsand Structure of a Medical School. Available at:http://www.lcme.org/. Accessed Jul 18, 2008.
28. Accreditation Council for Graduate Medical Educa-tion. ACGME Outcome Project. Available at: http://www.acgme.org/outcome/. Accessed Jul 18, 2008.
29. Kuhn GJ. Diagnostic errors. Acad Emerg Med.2002; 9:740–50.
30. Hutchinson L. Evaluating and researching the effec-tiveness of educational interventions. Br Med J.1999; 318:1267–9.
31. Griffith CH III, Georgesen JC, Wilson JF. Specialtychoices of students who actually have choices: theinfluence of excellent clinical teachers. Acad Med.2000; 75:278–82.
Hillside offertory for the God Apollo in Delphi, Greece
Many Have Sought the Future at Delphi
>Her folks confirmed the pork chops were appeasingYet the drool they’d witnessed wasn’t gustatory.Previously healthy, their 9-year-old had seized.August 4th, 2008, 8PM in my weekly offertory;I knew my time, place, person, et cetera.So did she, but to my cognitive address,‘‘Who’s president?,’’ she firmly replied, ‘‘Obama.’’Do I consider this as clouded consciousnessOr prudence, and abandon scanning an oracle?
Jonathan Singer, MD
([email protected])Department of Emergency Medicine
Wright State UniversityDayton, OH
doi: 10.1111/j.1553-2712.2008.00286.x
REFLECTIONS
82 Shayne et al. • ED CROWDING AND EDUCATION