Embed Size (px)
Citation preview
Research ArticleThe Effect of Hamatum Curvature Angle on Carpal TunnelVolumetry A Mathematical Simulation Model
Nazmi Bulent Alp 1 Tufan Kaleli1 Onur Can Kalay2 Fatih Karpat 2 Gokhan Akdag3
Aslı Ceren Macunluoglu 4 and Gamze Saygı Oral5
1Department of Orthopedics and Traumatology Bursa Uludag University School of Medicine Bursa Turkey2Department of Mechanical Engineering Bursa Uludag University Bursa Turkey3Istanbul Beylikduzu State Hospital Orthopedics and Traumatology Department Istanbul Turkey4Department of Biostatistics Uludag University Institute of Health Sciences Bursa Turkey5Independent Researcher Istanbul Turkey
Correspondence should be addressed to Nazmi Bulent Alp nazmibulentalphotmailcom
Received 3 July 2019 Accepted 19 December 2019 Published 10 March 2020
Academic Editor Michele Migliore
Copyright copy 2020 Nazmi Bulent Alp et al )is is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work isproperly cited
In carpal tunnel volume measurements the angle of the hamatum curvature is not considered a variable and its effect on carpaltunnel volume has not been investigatedWe hypothesize that a change in the anatomical angle of the hamatum curvature changesthe carpal tunnel volume To prove our hypothesis we used a mathematical simulation model considering the carpal tunnel as atruncated coneWe reviewed the wrist CTscans of 91 adults (gt18 years of age) including 51men and 40 womenWemeasured theangle of the hamatum curvature in the CTscans We measured cross-sectional areas at the outlet of the carpal tunnel at the level ofthe trapezium and hook of hamate (r1) and at the inlet at the level of the scaphoid and pisiform (r2) and the length (h) of the carpaltunnel We attempted to calculate the effect of 2 degree by 2-degree changes in the angle of the hamatum curvature between theangles of 98deg and 140deg on the carpal tunnel volume )e mean angle of the hook of hamatum of the subjects was 12255degplusmn 820deg(range 9720deg minus 13931deg) No suitable cutoff point was found for the angle values )ere was no difference between the gendergroups according to the angle value )e data clearly show that there is a high correlation between carpal tunnel volume and theangle of hamatum curvature )e results of our study emphasize the importance of taking into account the anatomical features ofthe hamatum bone especially the angle of curvature which may play a predisposing role in idiopathic carpal tunnel syndrome
1 Introduction
Carpal tunnel syndrome (CTS) is the most common pe-ripheral compression neuropathy syndrome in the USA [1]A carpal tunnel is a fibro-osseous tunnel where its innerboundaries are made up of soft tissues and carpal bones )etransverse carpal ligament (TCL) forms the volar margin ofthe tunnel Proximally the TCL attaches to the scaphoidtuberosity and pisiform distally it attaches to the hook ofhamate and the ridge of the trapezium )e hook of hamateis a reliable landmark [2 3] in hand surgery especially incarpal tunnel release [4 5 6] Some studies have reported asmall number of bipartite hypoplastic and aplastic hooks of
the hamate [2ndash12] In another study Huang et al measured2000 hamates and they classified 31 (622000) as hypo-plastic and aplastic )e volume of the carpal tunnel is onlyslightly less than the volume of the soft tissue content [13]therefore any process that reduces the volume of the carpaltunnel may cause compression of the median nerve Webelieve that anatomical changes in the hamate bone mayalter the volume of the carpal tunnel due to a change in theulnar border Various authors investigated the volume andcross-sectional areas of the carpal tunnel by computed to-mography magnetic resonance imaging silicon moldcasting and ultrasound [14ndash16] To the best of ourknowledge the relationship between the shape of the
HindawiComputational and Mathematical Methods in MedicineVolume 2020 Article ID 7582181 6 pageshttpsdoiorg10115520207582181
hamatum curvature or in other words the angle of thecurvature and its effects on carpal tunnel volume has neverbeen studied in the literature
)e aim of this study was two-fold (a) to study the angleof the hamatum curvature and whether there is any genderdifference and (b) to evaluate the relationship between theangle of the hamatum curvature and carpal tunnel volumeusing a mathematical simulation model
2 Materials and Methods
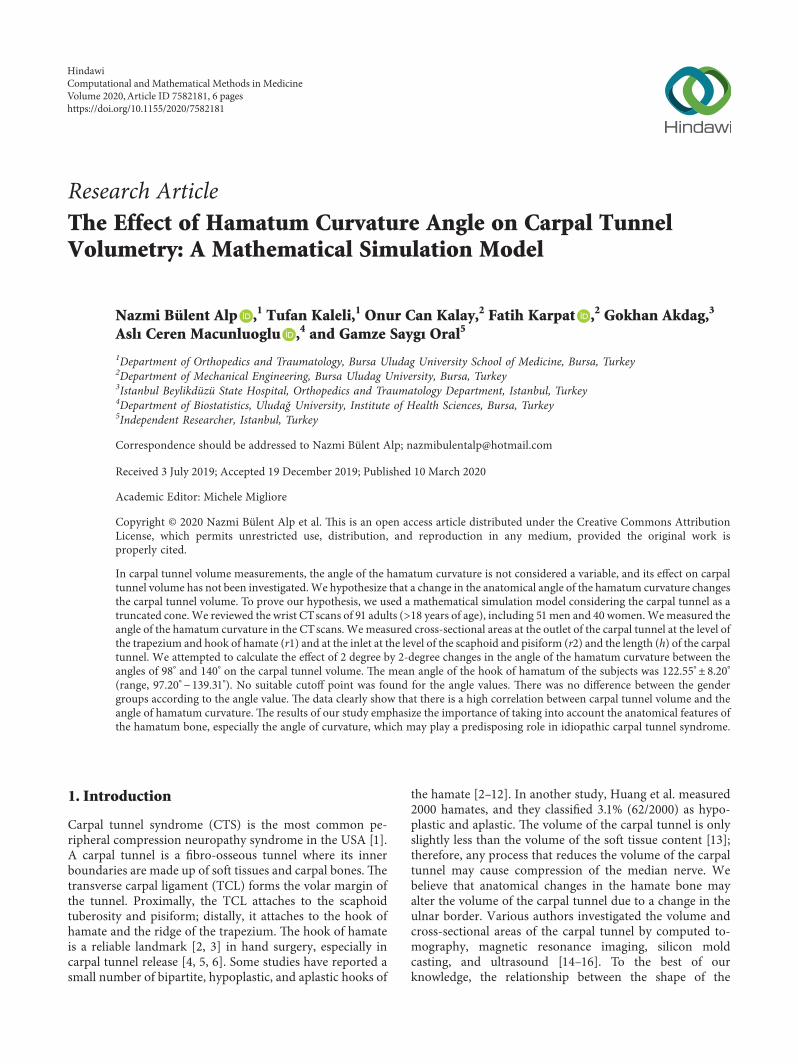
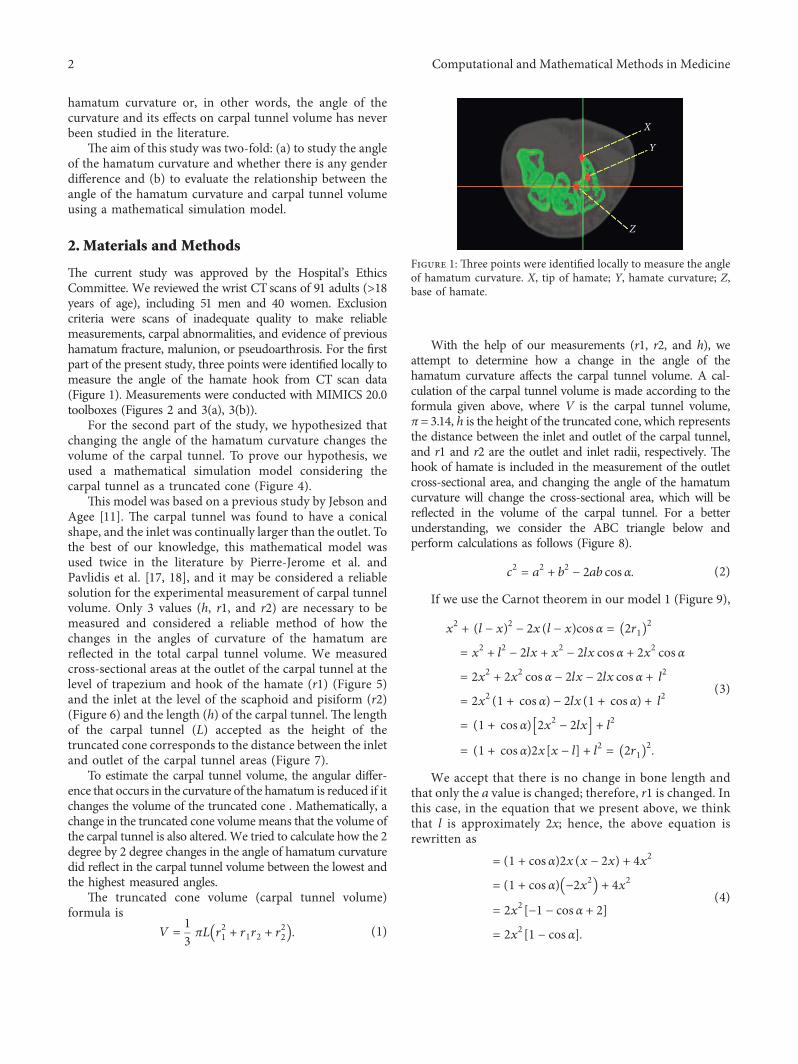
)e current study was approved by the Hospitalrsquos EthicsCommittee We reviewed the wrist CT scans of 91 adults (gt18years of age) including 51 men and 40 women Exclusioncriteria were scans of inadequate quality to make reliablemeasurements carpal abnormalities and evidence of previoushamatum fracture malunion or pseudoarthrosis For the firstpart of the present study three points were identified locally tomeasure the angle of the hamate hook from CT scan data(Figure 1) Measurements were conducted with MIMICS 200toolboxes (Figures 2 and 3(a) 3(b))
For the second part of the study we hypothesized thatchanging the angle of the hamatum curvature changes thevolume of the carpal tunnel To prove our hypothesis weused a mathematical simulation model considering thecarpal tunnel as a truncated cone (Figure 4)
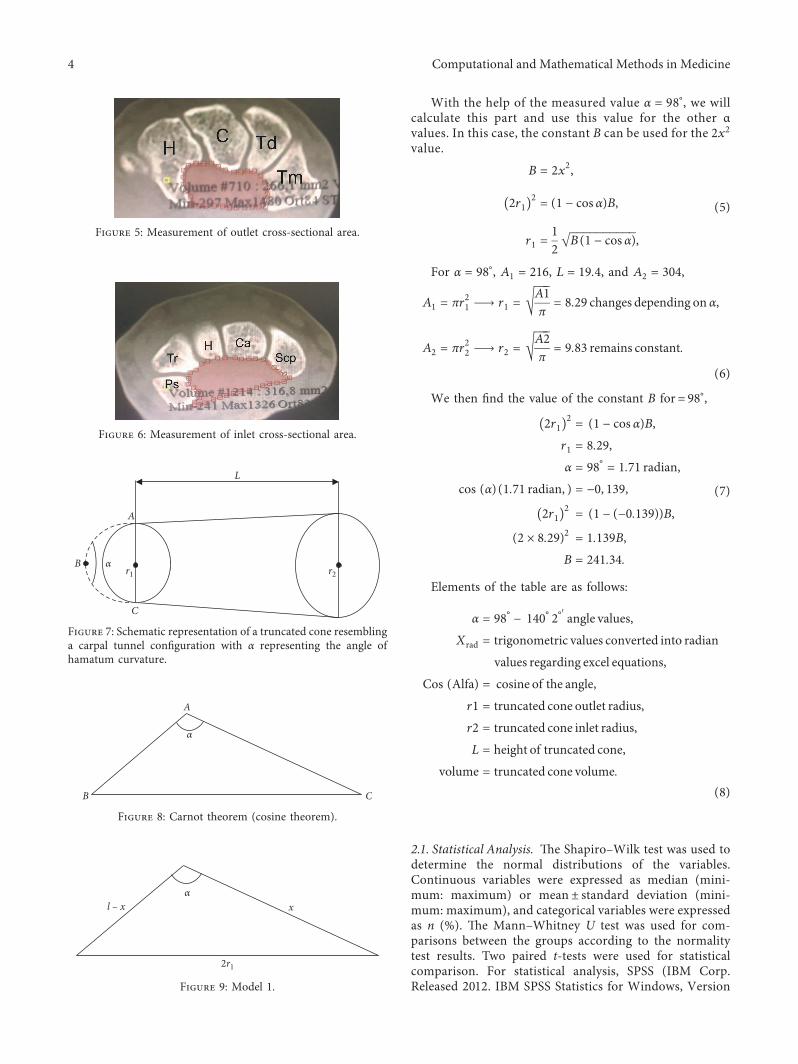
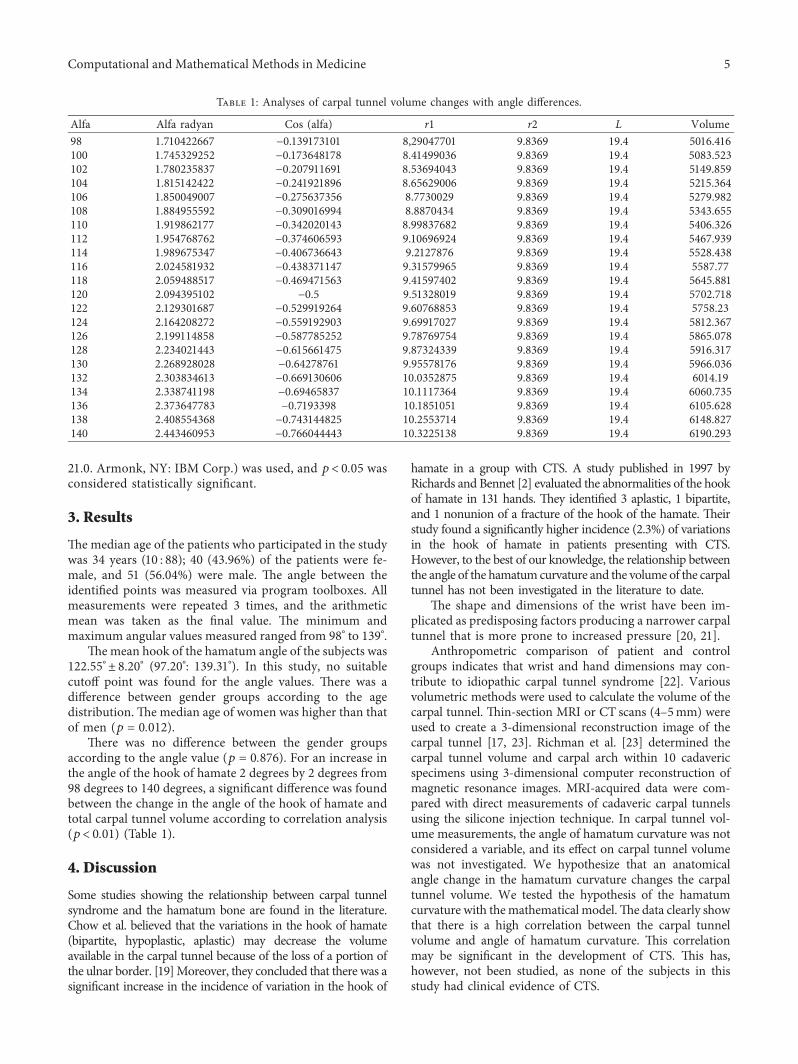
)is model was based on a previous study by Jebson andAgee [11] )e carpal tunnel was found to have a conicalshape and the inlet was continually larger than the outlet Tothe best of our knowledge this mathematical model wasused twice in the literature by Pierre-Jerome et al andPavlidis et al [17 18] and it may be considered a reliablesolution for the experimental measurement of carpal tunnelvolume Only 3 values (h r1 and r2) are necessary to bemeasured and considered a reliable method of how thechanges in the angles of curvature of the hamatum arereflected in the total carpal tunnel volume We measuredcross-sectional areas at the outlet of the carpal tunnel at thelevel of trapezium and hook of the hamate (r1) (Figure 5)and the inlet at the level of the scaphoid and pisiform (r2)(Figure 6) and the length (h) of the carpal tunnel )e lengthof the carpal tunnel (L) accepted as the height of thetruncated cone corresponds to the distance between the inletand outlet of the carpal tunnel areas (Figure 7)
To estimate the carpal tunnel volume the angular differ-ence that occurs in the curvature of the hamatum is reduced if itchanges the volume of the truncated cone Mathematically achange in the truncated cone volumemeans that the volume ofthe carpal tunnel is also alteredWe tried to calculate how the 2degree by 2 degree changes in the angle of hamatum curvaturedid reflect in the carpal tunnel volume between the lowest andthe highest measured angles
)e truncated cone volume (carpal tunnel volume)formula is
V 13πL r
21 + r1r2 + r
221113872 1113873 (1)
With the help of our measurements (r1 r2 and h) weattempt to determine how a change in the angle of thehamatum curvature affects the carpal tunnel volume A cal-culation of the carpal tunnel volume is made according to theformula given above where V is the carpal tunnel volumeπ 314 h is the height of the truncated cone which representsthe distance between the inlet and outlet of the carpal tunneland r1 and r2 are the outlet and inlet radii respectively )ehook of hamate is included in the measurement of the outletcross-sectional area and changing the angle of the hamatumcurvature will change the cross-sectional area which will bereflected in the volume of the carpal tunnel For a betterunderstanding we consider the ABC triangle below andperform calculations as follows (Figure 8)
c2
a2
+ b2
minus 2ab cos α (2)
If we use the Carnot theorem in our model 1 (Figure 9)
x2
+ (l minus x)2
minus 2x(l minus x)cos α 2r1( 11138572
x2
+ l2
minus 2lx + x2
minus 2lx cos α + 2x2 cos α
2x2
+ 2x2 cos α minus 2lx minus 2lx cos α + l
2
2x2(1 + cos α) minus 2lx(1 + cos α) + l
2
(1 + cos α) 2x2
minus 2lx1113960 1113961 + l2
(1 + cos α)2x[x minus l] + l2
2r1( 11138572
(3)
We accept that there is no change in bone length andthat only the a value is changed therefore r1 is changed Inthis case in the equation that we present above we thinkthat l is approximately 2x hence the above equation isrewritten as
(1 + cos α)2x(x minus 2x) + 4x2
(1 + cos α) minus 2x2
1113872 1113873 + 4x2
2x2[minus 1 minus cos α + 2]
2x2[1 minus cos α]
(4)
X
Y
Z
Figure 1 )ree points were identified locally to measure the angleof hamatum curvature X tip of hamate Y hamate curvature Zbase of hamate
2 Computational and Mathematical Methods in Medicine
Tip of hamate
12707degCurvature of
hamateBase of hamate
(a)
Tip of hamate
10527deg Curvature ofhamate
Base of hamate
(b)
Figure 3 Measurement of angle of hamatum curvature
Coronal view of computed tomography image of a wrist
Radius Ulna
(a)
Distal carpal row bones
AB C D
(b)
Sagittal view of a computed tomography image of a wrist
(c)
3D view of a computed tomography image of a wrist in supination
TrapeziumHamate
Carpal tunnel
UlnaRadius
(d)
Figure 2 Measurements were conducted with MIMICS 200 toolboxes (a) Coranal view of computed tomography image of a wrist(b) Distal carpal row bones (c) Sagittal view of a computed tomography image of a wrist (d) 3D view of a computed tomography image of awrist in supination
Figure 4 Schematic representation of a truncated cone
Computational and Mathematical Methods in Medicine 3
With the help of the measured value α 98deg we willcalculate this part and use this value for the other αvalues In this case the constant B can be used for the 2x2
value
B 2x2
2r1( 11138572
(1 minus cos α)B
r1 12
B(1 minus cos α)
1113968
(5)
For α 98deg A1 216 L 194 and A2 304
A1 πr21⟶ r1
A1π
1113970
829 changes depending on α
A2 πr22⟶ r2
A2π
1113970
983 remains constant
(6)
We then find the value of the constant B for = 98deg
2r1( 11138572
(1 minus cos α)B
r1 829
α 98deg 171 radian
cos (α)(171 radian ) minus 0 139
2r1( 11138572
(1 minus (minus 0139))B
(2 times 829)2
1139B
B 24134
(7)
Elements of the table are as follows
α 98deg minus 140deg 2degprime angle values
Xrad trigonometric values converted into radian
values regarding excel equations
Cos (Alfa) cosine of the angle
r1 truncated cone outlet radius
r2 truncated cone inlet radius
L height of truncated cone
volume truncated cone volume(8)
21 Statistical Analysis )e ShapirondashWilk test was used todetermine the normal distributions of the variablesContinuous variables were expressed as median (mini-mum maximum) or mean plusmn standard deviation (mini-mum maximum) and categorical variables were expressedas n () )e MannndashWhitney U test was used for com-parisons between the groups according to the normalitytest results Two paired t-tests were used for statisticalcomparison For statistical analysis SPSS (IBM CorpReleased 2012 IBM SPSS Statistics for Windows Version
xα
l ndash x
2r1
Figure 9 Model 1
L
A
B
C
r1 r2α
Figure 7 Schematic representation of a truncated cone resemblinga carpal tunnel configuration with α representing the angle ofhamatum curvature
Figure 6 Measurement of inlet cross-sectional area
Figure 5 Measurement of outlet cross-sectional area
A
B C
α
Figure 8 Carnot theorem (cosine theorem)
4 Computational and Mathematical Methods in Medicine
210 Armonk NY IBM Corp) was used and plt 005 wasconsidered statistically significant
3 Results
)emedian age of the patients who participated in the studywas 34 years (10 88) 40 (4396) of the patients were fe-male and 51 (5604) were male )e angle between theidentified points was measured via program toolboxes Allmeasurements were repeated 3 times and the arithmeticmean was taken as the final value )e minimum andmaximum angular values measured ranged from 98deg to 139deg
)emean hook of the hamatum angle of the subjects was12255degplusmn 820deg (9720deg 13931deg) In this study no suitablecutoff point was found for the angle values )ere was adifference between gender groups according to the agedistribution )e median age of women was higher than thatof men (p 0012)
)ere was no difference between the gender groupsaccording to the angle value (p 0876) For an increase inthe angle of the hook of hamate 2 degrees by 2 degrees from98 degrees to 140 degrees a significant difference was foundbetween the change in the angle of the hook of hamate andtotal carpal tunnel volume according to correlation analysis(plt 001) (Table 1)
4 Discussion
Some studies showing the relationship between carpal tunnelsyndrome and the hamatum bone are found in the literatureChow et al believed that the variations in the hook of hamate(bipartite hypoplastic aplastic) may decrease the volumeavailable in the carpal tunnel because of the loss of a portion ofthe ulnar border [19]Moreover they concluded that there was asignificant increase in the incidence of variation in the hook of
hamate in a group with CTS A study published in 1997 byRichards and Bennet [2] evaluated the abnormalities of the hookof hamate in 131 hands )ey identified 3 aplastic 1 bipartiteand 1 nonunion of a fracture of the hook of the hamate )eirstudy found a significantly higher incidence (23) of variationsin the hook of hamate in patients presenting with CTSHowever to the best of our knowledge the relationship betweenthe angle of the hamatumcurvature and the volume of the carpaltunnel has not been investigated in the literature to date
)e shape and dimensions of the wrist have been im-plicated as predisposing factors producing a narrower carpaltunnel that is more prone to increased pressure [20 21]
Anthropometric comparison of patient and controlgroups indicates that wrist and hand dimensions may con-tribute to idiopathic carpal tunnel syndrome [22] Variousvolumetric methods were used to calculate the volume of thecarpal tunnel )in-section MRI or CT scans (4ndash5mm) wereused to create a 3-dimensional reconstruction image of thecarpal tunnel [17 23] Richman et al [23] determined thecarpal tunnel volume and carpal arch within 10 cadavericspecimens using 3-dimensional computer reconstruction ofmagnetic resonance images MRI-acquired data were com-pared with direct measurements of cadaveric carpal tunnelsusing the silicone injection technique In carpal tunnel vol-ume measurements the angle of hamatum curvature was notconsidered a variable and its effect on carpal tunnel volumewas not investigated We hypothesize that an anatomicalangle change in the hamatum curvature changes the carpaltunnel volume We tested the hypothesis of the hamatumcurvature with themathematical model)e data clearly showthat there is a high correlation between the carpal tunnelvolume and angle of hamatum curvature )is correlationmay be significant in the development of CTS )is hashowever not been studied as none of the subjects in thisstudy had clinical evidence of CTS
Table 1 Analyses of carpal tunnel volume changes with angle differences
Alfa Alfa radyan Cos (alfa) r1 r2 L Volume98 1710422667 minus 0139173101 829047701 98369 194 5016416100 1745329252 minus 0173648178 841499036 98369 194 5083523102 1780235837 minus 0207911691 853694043 98369 194 5149859104 1815142422 minus 0241921896 865629006 98369 194 5215364106 1850049007 minus 0275637356 87730029 98369 194 5279982108 1884955592 minus 0309016994 88870434 98369 194 5343655110 1919862177 minus 0342020143 899837682 98369 194 5406326112 1954768762 minus 0374606593 910696924 98369 194 5467939114 1989675347 minus 0406736643 92127876 98369 194 5528438116 2024581932 minus 0438371147 931579965 98369 194 558777118 2059488517 minus 0469471563 941597402 98369 194 5645881120 2094395102 minus 05 951328019 98369 194 5702718122 2129301687 minus 0529919264 960768853 98369 194 575823124 2164208272 minus 0559192903 969917027 98369 194 5812367126 2199114858 minus 0587785252 978769754 98369 194 5865078128 2234021443 minus 0615661475 987324339 98369 194 5916317130 2268928028 minus 064278761 995578176 98369 194 5966036132 2303834613 minus 0669130606 100352875 98369 194 601419134 2338741198 minus 069465837 101117364 98369 194 6060735136 2373647783 minus 07193398 101851051 98369 194 6105628138 2408554368 minus 0743144825 102553714 98369 194 6148827140 2443460953 minus 0766044443 103225138 98369 194 6190293
Computational and Mathematical Methods in Medicine 5
)ere are weaknesses in this study Our measurementswere performed only in healthy subjects Because we did notknow whether the hamatum curvature angle influenced thevolume of the carpal tunnel before the study we did not havea computed tomography scan in patients with carpal tun-nels We know that computed tomography will create anunnecessary radiation burden on patients In our futurestudies we aim to compare the values of the hamatumcurvature angle of the healthy population with those ofpatients with a carpal tunnel diagnosis
Additionally it is evident that this mathematical modelcannot simulate every wrist at 100 In real-life cases inletand outlet areas are not perfect cones or circles however thismodel still provides valuable data for further clinical studies
)e results of our study will emphasize the importance oftaking into account the anatomical features of the hamatumbone especially the angle of curvature which may play apredisposing role in idiopathic carpal tunnel syndromeInvestigation of the correlation between the angle ofhamatum curvature and carpal tunnel volume requiresfurther clinical study
Data Availability
)e data used to support the findings of this study are in-cluded within the article (Table 1)
Ethical Approval
)is study was approved by the Research and EthicsCommittee of our hospital and was carried out according tothe principles of the Declaration of Helsinki
Conflicts of Interest
All authors declare that they have no conflicts of interest
References
[1] G D Papanicolaou S J McCabe and J Firrell ldquo)e prev-alence and characteristics of nerve compression symptoms inthe general populationrdquo4e Journal of Hand Surgery vol 26no 3 pp 460ndash466 2001
[2] R S Richards and J D Bennett ldquoAbnormalities of the hook ofthe hamate in patients with carpal tunnel syndromerdquo Annalsof Plastic Surgery vol 39 no 1 pp 44ndash46 1997
[3] F K Fuss and T F Wagner ldquoBiomechanical alterations in thecarpal arch and hand muscles after carpal tunnel release afurther approach toward understanding the function of theflexor retinaculum and the cause of postoperative gripweaknessrdquo Clinical Anatomy vol 9 no 2 pp 100ndash108 1996
[4] M B Rotman and J P Donovan ldquoPractical anatomy of thecarpal tunnelrdquoHand Clinics vol 18 no 2 pp 219ndash230 2002
[5] T K Cobb G A Knudson and W P Cooney ldquo)e use oftopographical landmarks to improve the outcome of Agee en-doscopic carpal tunnel releaserdquo Arthroscopy 4e Journal ofArthroscopic amp Related Surgery vol 11 no 2 pp 165ndash172 1995
[6] T K Cobb W P Cooney and K-N An ldquoClinical location ofhook of hamate a technical note for endoscopic carpal tunnelreleaserdquo 4e Journal of Hand Surgery vol 19 no 3pp 516ndash518 1994
[7] F B Bogart ldquoVariation of the bones of the wristrdquo AmericanJournal of Roentgenology vol 50 pp 638ndash646 1932
[8] C Pierre-Jerome S I Bekkelund G Husby S I MellgrenM Osteaux and R Nordstrom ldquoMRI of anatomical variantsof the wrist in womenrdquo Surgical and Radiologic Anatomyvol 18 no 1 pp 37ndash41 1996
[9] C Pierre-Jerome and I K Roug ldquoMRI of bilateral bipartitehamulus a case reportrdquo Surgical and Radiologic Anatomyvol 20 no 4 pp 299ndash302 1998
[10] M H Greene and A M Hadied ldquoBipartite hamulus withulnar tunnel syndrome-Case report and literature reviewrdquo4e Journal of Hand Surgery vol 6 no 6 pp 605ndash609 1981
[11] P J L Jebson and J M Agee ldquoCarpal tunnel syndromeunusual contraindications to endoscopic releaserdquo Arthros-copy 4e Journal of Arthroscopic amp Related Surgery vol 12no 6 pp 749ndash751 1996
[12] L L Seeger L W Bassett and R H Gold ldquoCase report 464rdquoSkeletal Radiology vol 17 no 1 pp 85-86 1988
[13] H K Watson and J Weinzweig 4e Wrist LippincottWilliams and Wilkins Philadelphia PA USA 2001
[14] M Skie J Zeiss N A Ebraheim and W )omas JacksonldquoCarpal tunnel changes and median nerve compression duringwrist flexion and extension seen bymagnetic resonance imagingrdquo4e Journal of Hand Surgery vol 15 no 6 pp 934ndash939 1990
[15] K H Allmann R Horch M Uhl et al ldquoMR imaging of thecarpal tunnelrdquo European Journal of Radiology vol 25 no 2pp 141ndash145 1997
[16] T K Cobb B K Dalley R H Posteraro and R C LewisldquoEstablishment of carpal contentscanal ratio by means ofmagnetic resonance imagingrdquo 4e Journal of Hand Surgeryvol 17 no 5 pp 843ndash849 1992
[17] C Pierre-Jerome S Bekkelund and R Nordstroslashm ldquoQuan-titative MRI analysis of anatomic dimensions of the carpaltunnel in womenrdquo Surgical and Radiologic Anatomy vol 19no 1 pp 31ndash34 1997
[18] L Pavlidis B E Chalidis E Demiri and C G Dimitriouldquo)e effect of transverse carpal ligament lengthening on carpaltunnel volumetry a comparison between four techniquesrdquoAnnals of Plastic Surgery vol 65 no 5 pp 480ndash484 2010
[19] J C Y Chow M A Weiss and Y Gu ldquoAnatomic variationsof the hook of hamate and the relationship to carpal tunnelsyndromerdquo 4e Journal of Hand Surgery vol 30 no 6pp 1242ndash1247 2005
[20] P G Lim S Tan and T S Ahmad ldquo)e role of wrist an-thropometric measurement in idiopathic carpal tunnel syn-dromerdquo Journal of Hand Surgery (European Volume) vol 33no 5 pp 645ndash647 2008
[21] J E Farmer and T R C Davis ldquoCarpal tunnel syndrome acase-control study evaluating its relationship with body massindex and hand and wrist measurementsrdquo Journal of HandSurgery (European Volume) vol 33 no 4 pp 445ndash448 2008
[22] J P M Mogk and P J Keir ldquoWrist and carpal tunnel size andshape measurements effects of posturerdquo Clinical Biome-chanics vol 23 no 9 pp 1112ndash1120 2008
[23] J A Richman R H Gelberman B L Rydevik V M Gylys-Morin P C Hajek and D J Sartoris ldquoCarpal tunnel volumedetermination by magnetic resonance imaging three-di-mensional reconstructionrdquo 4e Journal of Hand Surgeryvol 12 no 5 pp 712ndash717 1987
6 Computational and Mathematical Methods in Medicine
hamatum curvature or in other words the angle of thecurvature and its effects on carpal tunnel volume has neverbeen studied in the literature
)e aim of this study was two-fold (a) to study the angleof the hamatum curvature and whether there is any genderdifference and (b) to evaluate the relationship between theangle of the hamatum curvature and carpal tunnel volumeusing a mathematical simulation model
2 Materials and Methods
)e current study was approved by the Hospitalrsquos EthicsCommittee We reviewed the wrist CT scans of 91 adults (gt18years of age) including 51 men and 40 women Exclusioncriteria were scans of inadequate quality to make reliablemeasurements carpal abnormalities and evidence of previoushamatum fracture malunion or pseudoarthrosis For the firstpart of the present study three points were identified locally tomeasure the angle of the hamate hook from CT scan data(Figure 1) Measurements were conducted with MIMICS 200toolboxes (Figures 2 and 3(a) 3(b))
For the second part of the study we hypothesized thatchanging the angle of the hamatum curvature changes thevolume of the carpal tunnel To prove our hypothesis weused a mathematical simulation model considering thecarpal tunnel as a truncated cone (Figure 4)
)is model was based on a previous study by Jebson andAgee [11] )e carpal tunnel was found to have a conicalshape and the inlet was continually larger than the outlet Tothe best of our knowledge this mathematical model wasused twice in the literature by Pierre-Jerome et al andPavlidis et al [17 18] and it may be considered a reliablesolution for the experimental measurement of carpal tunnelvolume Only 3 values (h r1 and r2) are necessary to bemeasured and considered a reliable method of how thechanges in the angles of curvature of the hamatum arereflected in the total carpal tunnel volume We measuredcross-sectional areas at the outlet of the carpal tunnel at thelevel of trapezium and hook of the hamate (r1) (Figure 5)and the inlet at the level of the scaphoid and pisiform (r2)(Figure 6) and the length (h) of the carpal tunnel )e lengthof the carpal tunnel (L) accepted as the height of thetruncated cone corresponds to the distance between the inletand outlet of the carpal tunnel areas (Figure 7)
To estimate the carpal tunnel volume the angular differ-ence that occurs in the curvature of the hamatum is reduced if itchanges the volume of the truncated cone Mathematically achange in the truncated cone volumemeans that the volume ofthe carpal tunnel is also alteredWe tried to calculate how the 2degree by 2 degree changes in the angle of hamatum curvaturedid reflect in the carpal tunnel volume between the lowest andthe highest measured angles
)e truncated cone volume (carpal tunnel volume)formula is
V 13πL r
21 + r1r2 + r
221113872 1113873 (1)
With the help of our measurements (r1 r2 and h) weattempt to determine how a change in the angle of thehamatum curvature affects the carpal tunnel volume A cal-culation of the carpal tunnel volume is made according to theformula given above where V is the carpal tunnel volumeπ 314 h is the height of the truncated cone which representsthe distance between the inlet and outlet of the carpal tunneland r1 and r2 are the outlet and inlet radii respectively )ehook of hamate is included in the measurement of the outletcross-sectional area and changing the angle of the hamatumcurvature will change the cross-sectional area which will bereflected in the volume of the carpal tunnel For a betterunderstanding we consider the ABC triangle below andperform calculations as follows (Figure 8)
c2
a2
+ b2
minus 2ab cos α (2)
If we use the Carnot theorem in our model 1 (Figure 9)
x2
+ (l minus x)2
minus 2x(l minus x)cos α 2r1( 11138572
x2
+ l2
minus 2lx + x2
minus 2lx cos α + 2x2 cos α
2x2
+ 2x2 cos α minus 2lx minus 2lx cos α + l
2
2x2(1 + cos α) minus 2lx(1 + cos α) + l
2
(1 + cos α) 2x2
minus 2lx1113960 1113961 + l2
(1 + cos α)2x[x minus l] + l2
2r1( 11138572
(3)
We accept that there is no change in bone length andthat only the a value is changed therefore r1 is changed Inthis case in the equation that we present above we thinkthat l is approximately 2x hence the above equation isrewritten as
(1 + cos α)2x(x minus 2x) + 4x2
(1 + cos α) minus 2x2
1113872 1113873 + 4x2
2x2[minus 1 minus cos α + 2]
2x2[1 minus cos α]
(4)
X
Y
Z
Figure 1 )ree points were identified locally to measure the angleof hamatum curvature X tip of hamate Y hamate curvature Zbase of hamate
2 Computational and Mathematical Methods in Medicine
Tip of hamate
12707degCurvature of
hamateBase of hamate
(a)
Tip of hamate
10527deg Curvature ofhamate
Base of hamate
(b)
Figure 3 Measurement of angle of hamatum curvature
Coronal view of computed tomography image of a wrist
Radius Ulna
(a)
Distal carpal row bones
AB C D
(b)
Sagittal view of a computed tomography image of a wrist
(c)
3D view of a computed tomography image of a wrist in supination
TrapeziumHamate
Carpal tunnel
UlnaRadius
(d)
Figure 2 Measurements were conducted with MIMICS 200 toolboxes (a) Coranal view of computed tomography image of a wrist(b) Distal carpal row bones (c) Sagittal view of a computed tomography image of a wrist (d) 3D view of a computed tomography image of awrist in supination
Figure 4 Schematic representation of a truncated cone
Computational and Mathematical Methods in Medicine 3
With the help of the measured value α 98deg we willcalculate this part and use this value for the other αvalues In this case the constant B can be used for the 2x2
value
B 2x2
2r1( 11138572
(1 minus cos α)B
r1 12
B(1 minus cos α)
1113968
(5)
For α 98deg A1 216 L 194 and A2 304
A1 πr21⟶ r1
A1π
1113970
829 changes depending on α
A2 πr22⟶ r2
A2π
1113970
983 remains constant
(6)
We then find the value of the constant B for = 98deg
2r1( 11138572
(1 minus cos α)B
r1 829
α 98deg 171 radian
cos (α)(171 radian ) minus 0 139
2r1( 11138572
(1 minus (minus 0139))B
(2 times 829)2
1139B
B 24134
(7)
Elements of the table are as follows
α 98deg minus 140deg 2degprime angle values
Xrad trigonometric values converted into radian
values regarding excel equations
Cos (Alfa) cosine of the angle
r1 truncated cone outlet radius
r2 truncated cone inlet radius
L height of truncated cone
volume truncated cone volume(8)
21 Statistical Analysis )e ShapirondashWilk test was used todetermine the normal distributions of the variablesContinuous variables were expressed as median (mini-mum maximum) or mean plusmn standard deviation (mini-mum maximum) and categorical variables were expressedas n () )e MannndashWhitney U test was used for com-parisons between the groups according to the normalitytest results Two paired t-tests were used for statisticalcomparison For statistical analysis SPSS (IBM CorpReleased 2012 IBM SPSS Statistics for Windows Version
xα
l ndash x
2r1
Figure 9 Model 1
L
A
B
C
r1 r2α
Figure 7 Schematic representation of a truncated cone resemblinga carpal tunnel configuration with α representing the angle ofhamatum curvature
Figure 6 Measurement of inlet cross-sectional area
Figure 5 Measurement of outlet cross-sectional area
A
B C
α
Figure 8 Carnot theorem (cosine theorem)
4 Computational and Mathematical Methods in Medicine
210 Armonk NY IBM Corp) was used and plt 005 wasconsidered statistically significant
3 Results
)emedian age of the patients who participated in the studywas 34 years (10 88) 40 (4396) of the patients were fe-male and 51 (5604) were male )e angle between theidentified points was measured via program toolboxes Allmeasurements were repeated 3 times and the arithmeticmean was taken as the final value )e minimum andmaximum angular values measured ranged from 98deg to 139deg
)emean hook of the hamatum angle of the subjects was12255degplusmn 820deg (9720deg 13931deg) In this study no suitablecutoff point was found for the angle values )ere was adifference between gender groups according to the agedistribution )e median age of women was higher than thatof men (p 0012)
)ere was no difference between the gender groupsaccording to the angle value (p 0876) For an increase inthe angle of the hook of hamate 2 degrees by 2 degrees from98 degrees to 140 degrees a significant difference was foundbetween the change in the angle of the hook of hamate andtotal carpal tunnel volume according to correlation analysis(plt 001) (Table 1)
4 Discussion
Some studies showing the relationship between carpal tunnelsyndrome and the hamatum bone are found in the literatureChow et al believed that the variations in the hook of hamate(bipartite hypoplastic aplastic) may decrease the volumeavailable in the carpal tunnel because of the loss of a portion ofthe ulnar border [19]Moreover they concluded that there was asignificant increase in the incidence of variation in the hook of
hamate in a group with CTS A study published in 1997 byRichards and Bennet [2] evaluated the abnormalities of the hookof hamate in 131 hands )ey identified 3 aplastic 1 bipartiteand 1 nonunion of a fracture of the hook of the hamate )eirstudy found a significantly higher incidence (23) of variationsin the hook of hamate in patients presenting with CTSHowever to the best of our knowledge the relationship betweenthe angle of the hamatumcurvature and the volume of the carpaltunnel has not been investigated in the literature to date
)e shape and dimensions of the wrist have been im-plicated as predisposing factors producing a narrower carpaltunnel that is more prone to increased pressure [20 21]
Anthropometric comparison of patient and controlgroups indicates that wrist and hand dimensions may con-tribute to idiopathic carpal tunnel syndrome [22] Variousvolumetric methods were used to calculate the volume of thecarpal tunnel )in-section MRI or CT scans (4ndash5mm) wereused to create a 3-dimensional reconstruction image of thecarpal tunnel [17 23] Richman et al [23] determined thecarpal tunnel volume and carpal arch within 10 cadavericspecimens using 3-dimensional computer reconstruction ofmagnetic resonance images MRI-acquired data were com-pared with direct measurements of cadaveric carpal tunnelsusing the silicone injection technique In carpal tunnel vol-ume measurements the angle of hamatum curvature was notconsidered a variable and its effect on carpal tunnel volumewas not investigated We hypothesize that an anatomicalangle change in the hamatum curvature changes the carpaltunnel volume We tested the hypothesis of the hamatumcurvature with themathematical model)e data clearly showthat there is a high correlation between the carpal tunnelvolume and angle of hamatum curvature )is correlationmay be significant in the development of CTS )is hashowever not been studied as none of the subjects in thisstudy had clinical evidence of CTS
Table 1 Analyses of carpal tunnel volume changes with angle differences
Alfa Alfa radyan Cos (alfa) r1 r2 L Volume98 1710422667 minus 0139173101 829047701 98369 194 5016416100 1745329252 minus 0173648178 841499036 98369 194 5083523102 1780235837 minus 0207911691 853694043 98369 194 5149859104 1815142422 minus 0241921896 865629006 98369 194 5215364106 1850049007 minus 0275637356 87730029 98369 194 5279982108 1884955592 minus 0309016994 88870434 98369 194 5343655110 1919862177 minus 0342020143 899837682 98369 194 5406326112 1954768762 minus 0374606593 910696924 98369 194 5467939114 1989675347 minus 0406736643 92127876 98369 194 5528438116 2024581932 minus 0438371147 931579965 98369 194 558777118 2059488517 minus 0469471563 941597402 98369 194 5645881120 2094395102 minus 05 951328019 98369 194 5702718122 2129301687 minus 0529919264 960768853 98369 194 575823124 2164208272 minus 0559192903 969917027 98369 194 5812367126 2199114858 minus 0587785252 978769754 98369 194 5865078128 2234021443 minus 0615661475 987324339 98369 194 5916317130 2268928028 minus 064278761 995578176 98369 194 5966036132 2303834613 minus 0669130606 100352875 98369 194 601419134 2338741198 minus 069465837 101117364 98369 194 6060735136 2373647783 minus 07193398 101851051 98369 194 6105628138 2408554368 minus 0743144825 102553714 98369 194 6148827140 2443460953 minus 0766044443 103225138 98369 194 6190293
Computational and Mathematical Methods in Medicine 5
)ere are weaknesses in this study Our measurementswere performed only in healthy subjects Because we did notknow whether the hamatum curvature angle influenced thevolume of the carpal tunnel before the study we did not havea computed tomography scan in patients with carpal tun-nels We know that computed tomography will create anunnecessary radiation burden on patients In our futurestudies we aim to compare the values of the hamatumcurvature angle of the healthy population with those ofpatients with a carpal tunnel diagnosis
Additionally it is evident that this mathematical modelcannot simulate every wrist at 100 In real-life cases inletand outlet areas are not perfect cones or circles however thismodel still provides valuable data for further clinical studies
)e results of our study will emphasize the importance oftaking into account the anatomical features of the hamatumbone especially the angle of curvature which may play apredisposing role in idiopathic carpal tunnel syndromeInvestigation of the correlation between the angle ofhamatum curvature and carpal tunnel volume requiresfurther clinical study
Data Availability
)e data used to support the findings of this study are in-cluded within the article (Table 1)
Ethical Approval
)is study was approved by the Research and EthicsCommittee of our hospital and was carried out according tothe principles of the Declaration of Helsinki
Conflicts of Interest
All authors declare that they have no conflicts of interest
References
[1] G D Papanicolaou S J McCabe and J Firrell ldquo)e prev-alence and characteristics of nerve compression symptoms inthe general populationrdquo4e Journal of Hand Surgery vol 26no 3 pp 460ndash466 2001
[2] R S Richards and J D Bennett ldquoAbnormalities of the hook ofthe hamate in patients with carpal tunnel syndromerdquo Annalsof Plastic Surgery vol 39 no 1 pp 44ndash46 1997
[3] F K Fuss and T F Wagner ldquoBiomechanical alterations in thecarpal arch and hand muscles after carpal tunnel release afurther approach toward understanding the function of theflexor retinaculum and the cause of postoperative gripweaknessrdquo Clinical Anatomy vol 9 no 2 pp 100ndash108 1996
[4] M B Rotman and J P Donovan ldquoPractical anatomy of thecarpal tunnelrdquoHand Clinics vol 18 no 2 pp 219ndash230 2002
[5] T K Cobb G A Knudson and W P Cooney ldquo)e use oftopographical landmarks to improve the outcome of Agee en-doscopic carpal tunnel releaserdquo Arthroscopy 4e Journal ofArthroscopic amp Related Surgery vol 11 no 2 pp 165ndash172 1995
[6] T K Cobb W P Cooney and K-N An ldquoClinical location ofhook of hamate a technical note for endoscopic carpal tunnelreleaserdquo 4e Journal of Hand Surgery vol 19 no 3pp 516ndash518 1994
[7] F B Bogart ldquoVariation of the bones of the wristrdquo AmericanJournal of Roentgenology vol 50 pp 638ndash646 1932
[8] C Pierre-Jerome S I Bekkelund G Husby S I MellgrenM Osteaux and R Nordstrom ldquoMRI of anatomical variantsof the wrist in womenrdquo Surgical and Radiologic Anatomyvol 18 no 1 pp 37ndash41 1996
[9] C Pierre-Jerome and I K Roug ldquoMRI of bilateral bipartitehamulus a case reportrdquo Surgical and Radiologic Anatomyvol 20 no 4 pp 299ndash302 1998
[10] M H Greene and A M Hadied ldquoBipartite hamulus withulnar tunnel syndrome-Case report and literature reviewrdquo4e Journal of Hand Surgery vol 6 no 6 pp 605ndash609 1981
[11] P J L Jebson and J M Agee ldquoCarpal tunnel syndromeunusual contraindications to endoscopic releaserdquo Arthros-copy 4e Journal of Arthroscopic amp Related Surgery vol 12no 6 pp 749ndash751 1996
[12] L L Seeger L W Bassett and R H Gold ldquoCase report 464rdquoSkeletal Radiology vol 17 no 1 pp 85-86 1988
[13] H K Watson and J Weinzweig 4e Wrist LippincottWilliams and Wilkins Philadelphia PA USA 2001
[14] M Skie J Zeiss N A Ebraheim and W )omas JacksonldquoCarpal tunnel changes and median nerve compression duringwrist flexion and extension seen bymagnetic resonance imagingrdquo4e Journal of Hand Surgery vol 15 no 6 pp 934ndash939 1990
[15] K H Allmann R Horch M Uhl et al ldquoMR imaging of thecarpal tunnelrdquo European Journal of Radiology vol 25 no 2pp 141ndash145 1997
[16] T K Cobb B K Dalley R H Posteraro and R C LewisldquoEstablishment of carpal contentscanal ratio by means ofmagnetic resonance imagingrdquo 4e Journal of Hand Surgeryvol 17 no 5 pp 843ndash849 1992
[17] C Pierre-Jerome S Bekkelund and R Nordstroslashm ldquoQuan-titative MRI analysis of anatomic dimensions of the carpaltunnel in womenrdquo Surgical and Radiologic Anatomy vol 19no 1 pp 31ndash34 1997
[18] L Pavlidis B E Chalidis E Demiri and C G Dimitriouldquo)e effect of transverse carpal ligament lengthening on carpaltunnel volumetry a comparison between four techniquesrdquoAnnals of Plastic Surgery vol 65 no 5 pp 480ndash484 2010
[19] J C Y Chow M A Weiss and Y Gu ldquoAnatomic variationsof the hook of hamate and the relationship to carpal tunnelsyndromerdquo 4e Journal of Hand Surgery vol 30 no 6pp 1242ndash1247 2005
[20] P G Lim S Tan and T S Ahmad ldquo)e role of wrist an-thropometric measurement in idiopathic carpal tunnel syn-dromerdquo Journal of Hand Surgery (European Volume) vol 33no 5 pp 645ndash647 2008
[21] J E Farmer and T R C Davis ldquoCarpal tunnel syndrome acase-control study evaluating its relationship with body massindex and hand and wrist measurementsrdquo Journal of HandSurgery (European Volume) vol 33 no 4 pp 445ndash448 2008
[22] J P M Mogk and P J Keir ldquoWrist and carpal tunnel size andshape measurements effects of posturerdquo Clinical Biome-chanics vol 23 no 9 pp 1112ndash1120 2008
[23] J A Richman R H Gelberman B L Rydevik V M Gylys-Morin P C Hajek and D J Sartoris ldquoCarpal tunnel volumedetermination by magnetic resonance imaging three-di-mensional reconstructionrdquo 4e Journal of Hand Surgeryvol 12 no 5 pp 712ndash717 1987
6 Computational and Mathematical Methods in Medicine
Tip of hamate
12707degCurvature of
hamateBase of hamate
(a)
Tip of hamate
10527deg Curvature ofhamate
Base of hamate
(b)
Figure 3 Measurement of angle of hamatum curvature
Coronal view of computed tomography image of a wrist
Radius Ulna
(a)
Distal carpal row bones
AB C D
(b)
Sagittal view of a computed tomography image of a wrist
(c)
3D view of a computed tomography image of a wrist in supination
TrapeziumHamate
Carpal tunnel
UlnaRadius
(d)
Figure 2 Measurements were conducted with MIMICS 200 toolboxes (a) Coranal view of computed tomography image of a wrist(b) Distal carpal row bones (c) Sagittal view of a computed tomography image of a wrist (d) 3D view of a computed tomography image of awrist in supination
Figure 4 Schematic representation of a truncated cone
Computational and Mathematical Methods in Medicine 3
With the help of the measured value α 98deg we willcalculate this part and use this value for the other αvalues In this case the constant B can be used for the 2x2
value
B 2x2
2r1( 11138572
(1 minus cos α)B
r1 12
B(1 minus cos α)
1113968
(5)
For α 98deg A1 216 L 194 and A2 304
A1 πr21⟶ r1
A1π
1113970
829 changes depending on α
A2 πr22⟶ r2
A2π
1113970
983 remains constant
(6)
We then find the value of the constant B for = 98deg
2r1( 11138572
(1 minus cos α)B
r1 829
α 98deg 171 radian
cos (α)(171 radian ) minus 0 139
2r1( 11138572
(1 minus (minus 0139))B
(2 times 829)2
1139B
B 24134
(7)
Elements of the table are as follows
α 98deg minus 140deg 2degprime angle values
Xrad trigonometric values converted into radian
values regarding excel equations
Cos (Alfa) cosine of the angle
r1 truncated cone outlet radius
r2 truncated cone inlet radius
L height of truncated cone
volume truncated cone volume(8)
21 Statistical Analysis )e ShapirondashWilk test was used todetermine the normal distributions of the variablesContinuous variables were expressed as median (mini-mum maximum) or mean plusmn standard deviation (mini-mum maximum) and categorical variables were expressedas n () )e MannndashWhitney U test was used for com-parisons between the groups according to the normalitytest results Two paired t-tests were used for statisticalcomparison For statistical analysis SPSS (IBM CorpReleased 2012 IBM SPSS Statistics for Windows Version
xα
l ndash x
2r1
Figure 9 Model 1
L
A
B
C
r1 r2α
Figure 7 Schematic representation of a truncated cone resemblinga carpal tunnel configuration with α representing the angle ofhamatum curvature
Figure 6 Measurement of inlet cross-sectional area
Figure 5 Measurement of outlet cross-sectional area
A
B C
α
Figure 8 Carnot theorem (cosine theorem)
4 Computational and Mathematical Methods in Medicine
210 Armonk NY IBM Corp) was used and plt 005 wasconsidered statistically significant
3 Results
)emedian age of the patients who participated in the studywas 34 years (10 88) 40 (4396) of the patients were fe-male and 51 (5604) were male )e angle between theidentified points was measured via program toolboxes Allmeasurements were repeated 3 times and the arithmeticmean was taken as the final value )e minimum andmaximum angular values measured ranged from 98deg to 139deg
)emean hook of the hamatum angle of the subjects was12255degplusmn 820deg (9720deg 13931deg) In this study no suitablecutoff point was found for the angle values )ere was adifference between gender groups according to the agedistribution )e median age of women was higher than thatof men (p 0012)
)ere was no difference between the gender groupsaccording to the angle value (p 0876) For an increase inthe angle of the hook of hamate 2 degrees by 2 degrees from98 degrees to 140 degrees a significant difference was foundbetween the change in the angle of the hook of hamate andtotal carpal tunnel volume according to correlation analysis(plt 001) (Table 1)
4 Discussion
Some studies showing the relationship between carpal tunnelsyndrome and the hamatum bone are found in the literatureChow et al believed that the variations in the hook of hamate(bipartite hypoplastic aplastic) may decrease the volumeavailable in the carpal tunnel because of the loss of a portion ofthe ulnar border [19]Moreover they concluded that there was asignificant increase in the incidence of variation in the hook of
hamate in a group with CTS A study published in 1997 byRichards and Bennet [2] evaluated the abnormalities of the hookof hamate in 131 hands )ey identified 3 aplastic 1 bipartiteand 1 nonunion of a fracture of the hook of the hamate )eirstudy found a significantly higher incidence (23) of variationsin the hook of hamate in patients presenting with CTSHowever to the best of our knowledge the relationship betweenthe angle of the hamatumcurvature and the volume of the carpaltunnel has not been investigated in the literature to date
)e shape and dimensions of the wrist have been im-plicated as predisposing factors producing a narrower carpaltunnel that is more prone to increased pressure [20 21]
Anthropometric comparison of patient and controlgroups indicates that wrist and hand dimensions may con-tribute to idiopathic carpal tunnel syndrome [22] Variousvolumetric methods were used to calculate the volume of thecarpal tunnel )in-section MRI or CT scans (4ndash5mm) wereused to create a 3-dimensional reconstruction image of thecarpal tunnel [17 23] Richman et al [23] determined thecarpal tunnel volume and carpal arch within 10 cadavericspecimens using 3-dimensional computer reconstruction ofmagnetic resonance images MRI-acquired data were com-pared with direct measurements of cadaveric carpal tunnelsusing the silicone injection technique In carpal tunnel vol-ume measurements the angle of hamatum curvature was notconsidered a variable and its effect on carpal tunnel volumewas not investigated We hypothesize that an anatomicalangle change in the hamatum curvature changes the carpaltunnel volume We tested the hypothesis of the hamatumcurvature with themathematical model)e data clearly showthat there is a high correlation between the carpal tunnelvolume and angle of hamatum curvature )is correlationmay be significant in the development of CTS )is hashowever not been studied as none of the subjects in thisstudy had clinical evidence of CTS
Table 1 Analyses of carpal tunnel volume changes with angle differences
Alfa Alfa radyan Cos (alfa) r1 r2 L Volume98 1710422667 minus 0139173101 829047701 98369 194 5016416100 1745329252 minus 0173648178 841499036 98369 194 5083523102 1780235837 minus 0207911691 853694043 98369 194 5149859104 1815142422 minus 0241921896 865629006 98369 194 5215364106 1850049007 minus 0275637356 87730029 98369 194 5279982108 1884955592 minus 0309016994 88870434 98369 194 5343655110 1919862177 minus 0342020143 899837682 98369 194 5406326112 1954768762 minus 0374606593 910696924 98369 194 5467939114 1989675347 minus 0406736643 92127876 98369 194 5528438116 2024581932 minus 0438371147 931579965 98369 194 558777118 2059488517 minus 0469471563 941597402 98369 194 5645881120 2094395102 minus 05 951328019 98369 194 5702718122 2129301687 minus 0529919264 960768853 98369 194 575823124 2164208272 minus 0559192903 969917027 98369 194 5812367126 2199114858 minus 0587785252 978769754 98369 194 5865078128 2234021443 minus 0615661475 987324339 98369 194 5916317130 2268928028 minus 064278761 995578176 98369 194 5966036132 2303834613 minus 0669130606 100352875 98369 194 601419134 2338741198 minus 069465837 101117364 98369 194 6060735136 2373647783 minus 07193398 101851051 98369 194 6105628138 2408554368 minus 0743144825 102553714 98369 194 6148827140 2443460953 minus 0766044443 103225138 98369 194 6190293
Computational and Mathematical Methods in Medicine 5
)ere are weaknesses in this study Our measurementswere performed only in healthy subjects Because we did notknow whether the hamatum curvature angle influenced thevolume of the carpal tunnel before the study we did not havea computed tomography scan in patients with carpal tun-nels We know that computed tomography will create anunnecessary radiation burden on patients In our futurestudies we aim to compare the values of the hamatumcurvature angle of the healthy population with those ofpatients with a carpal tunnel diagnosis
Additionally it is evident that this mathematical modelcannot simulate every wrist at 100 In real-life cases inletand outlet areas are not perfect cones or circles however thismodel still provides valuable data for further clinical studies
)e results of our study will emphasize the importance oftaking into account the anatomical features of the hamatumbone especially the angle of curvature which may play apredisposing role in idiopathic carpal tunnel syndromeInvestigation of the correlation between the angle ofhamatum curvature and carpal tunnel volume requiresfurther clinical study
Data Availability
)e data used to support the findings of this study are in-cluded within the article (Table 1)
Ethical Approval
)is study was approved by the Research and EthicsCommittee of our hospital and was carried out according tothe principles of the Declaration of Helsinki
Conflicts of Interest
All authors declare that they have no conflicts of interest
References
[1] G D Papanicolaou S J McCabe and J Firrell ldquo)e prev-alence and characteristics of nerve compression symptoms inthe general populationrdquo4e Journal of Hand Surgery vol 26no 3 pp 460ndash466 2001
[2] R S Richards and J D Bennett ldquoAbnormalities of the hook ofthe hamate in patients with carpal tunnel syndromerdquo Annalsof Plastic Surgery vol 39 no 1 pp 44ndash46 1997
[3] F K Fuss and T F Wagner ldquoBiomechanical alterations in thecarpal arch and hand muscles after carpal tunnel release afurther approach toward understanding the function of theflexor retinaculum and the cause of postoperative gripweaknessrdquo Clinical Anatomy vol 9 no 2 pp 100ndash108 1996
[4] M B Rotman and J P Donovan ldquoPractical anatomy of thecarpal tunnelrdquoHand Clinics vol 18 no 2 pp 219ndash230 2002
[5] T K Cobb G A Knudson and W P Cooney ldquo)e use oftopographical landmarks to improve the outcome of Agee en-doscopic carpal tunnel releaserdquo Arthroscopy 4e Journal ofArthroscopic amp Related Surgery vol 11 no 2 pp 165ndash172 1995
[6] T K Cobb W P Cooney and K-N An ldquoClinical location ofhook of hamate a technical note for endoscopic carpal tunnelreleaserdquo 4e Journal of Hand Surgery vol 19 no 3pp 516ndash518 1994
[7] F B Bogart ldquoVariation of the bones of the wristrdquo AmericanJournal of Roentgenology vol 50 pp 638ndash646 1932
[8] C Pierre-Jerome S I Bekkelund G Husby S I MellgrenM Osteaux and R Nordstrom ldquoMRI of anatomical variantsof the wrist in womenrdquo Surgical and Radiologic Anatomyvol 18 no 1 pp 37ndash41 1996
[9] C Pierre-Jerome and I K Roug ldquoMRI of bilateral bipartitehamulus a case reportrdquo Surgical and Radiologic Anatomyvol 20 no 4 pp 299ndash302 1998
[10] M H Greene and A M Hadied ldquoBipartite hamulus withulnar tunnel syndrome-Case report and literature reviewrdquo4e Journal of Hand Surgery vol 6 no 6 pp 605ndash609 1981
[11] P J L Jebson and J M Agee ldquoCarpal tunnel syndromeunusual contraindications to endoscopic releaserdquo Arthros-copy 4e Journal of Arthroscopic amp Related Surgery vol 12no 6 pp 749ndash751 1996
[12] L L Seeger L W Bassett and R H Gold ldquoCase report 464rdquoSkeletal Radiology vol 17 no 1 pp 85-86 1988
[13] H K Watson and J Weinzweig 4e Wrist LippincottWilliams and Wilkins Philadelphia PA USA 2001
[14] M Skie J Zeiss N A Ebraheim and W )omas JacksonldquoCarpal tunnel changes and median nerve compression duringwrist flexion and extension seen bymagnetic resonance imagingrdquo4e Journal of Hand Surgery vol 15 no 6 pp 934ndash939 1990
[15] K H Allmann R Horch M Uhl et al ldquoMR imaging of thecarpal tunnelrdquo European Journal of Radiology vol 25 no 2pp 141ndash145 1997
[16] T K Cobb B K Dalley R H Posteraro and R C LewisldquoEstablishment of carpal contentscanal ratio by means ofmagnetic resonance imagingrdquo 4e Journal of Hand Surgeryvol 17 no 5 pp 843ndash849 1992
[17] C Pierre-Jerome S Bekkelund and R Nordstroslashm ldquoQuan-titative MRI analysis of anatomic dimensions of the carpaltunnel in womenrdquo Surgical and Radiologic Anatomy vol 19no 1 pp 31ndash34 1997
[18] L Pavlidis B E Chalidis E Demiri and C G Dimitriouldquo)e effect of transverse carpal ligament lengthening on carpaltunnel volumetry a comparison between four techniquesrdquoAnnals of Plastic Surgery vol 65 no 5 pp 480ndash484 2010
[19] J C Y Chow M A Weiss and Y Gu ldquoAnatomic variationsof the hook of hamate and the relationship to carpal tunnelsyndromerdquo 4e Journal of Hand Surgery vol 30 no 6pp 1242ndash1247 2005
[20] P G Lim S Tan and T S Ahmad ldquo)e role of wrist an-thropometric measurement in idiopathic carpal tunnel syn-dromerdquo Journal of Hand Surgery (European Volume) vol 33no 5 pp 645ndash647 2008
[21] J E Farmer and T R C Davis ldquoCarpal tunnel syndrome acase-control study evaluating its relationship with body massindex and hand and wrist measurementsrdquo Journal of HandSurgery (European Volume) vol 33 no 4 pp 445ndash448 2008
[22] J P M Mogk and P J Keir ldquoWrist and carpal tunnel size andshape measurements effects of posturerdquo Clinical Biome-chanics vol 23 no 9 pp 1112ndash1120 2008
[23] J A Richman R H Gelberman B L Rydevik V M Gylys-Morin P C Hajek and D J Sartoris ldquoCarpal tunnel volumedetermination by magnetic resonance imaging three-di-mensional reconstructionrdquo 4e Journal of Hand Surgeryvol 12 no 5 pp 712ndash717 1987
6 Computational and Mathematical Methods in Medicine
With the help of the measured value α 98deg we willcalculate this part and use this value for the other αvalues In this case the constant B can be used for the 2x2
value
B 2x2
2r1( 11138572
(1 minus cos α)B
r1 12
B(1 minus cos α)
1113968
(5)
For α 98deg A1 216 L 194 and A2 304
A1 πr21⟶ r1
A1π
1113970
829 changes depending on α
A2 πr22⟶ r2
A2π
1113970
983 remains constant
(6)
We then find the value of the constant B for = 98deg
2r1( 11138572
(1 minus cos α)B
r1 829
α 98deg 171 radian
cos (α)(171 radian ) minus 0 139
2r1( 11138572
(1 minus (minus 0139))B
(2 times 829)2
1139B
B 24134
(7)
Elements of the table are as follows
α 98deg minus 140deg 2degprime angle values
Xrad trigonometric values converted into radian
values regarding excel equations
Cos (Alfa) cosine of the angle
r1 truncated cone outlet radius
r2 truncated cone inlet radius
L height of truncated cone
volume truncated cone volume(8)
21 Statistical Analysis )e ShapirondashWilk test was used todetermine the normal distributions of the variablesContinuous variables were expressed as median (mini-mum maximum) or mean plusmn standard deviation (mini-mum maximum) and categorical variables were expressedas n () )e MannndashWhitney U test was used for com-parisons between the groups according to the normalitytest results Two paired t-tests were used for statisticalcomparison For statistical analysis SPSS (IBM CorpReleased 2012 IBM SPSS Statistics for Windows Version
xα
l ndash x
2r1
Figure 9 Model 1
L
A
B
C
r1 r2α
Figure 7 Schematic representation of a truncated cone resemblinga carpal tunnel configuration with α representing the angle ofhamatum curvature
Figure 6 Measurement of inlet cross-sectional area
Figure 5 Measurement of outlet cross-sectional area
A
B C
α
Figure 8 Carnot theorem (cosine theorem)
4 Computational and Mathematical Methods in Medicine
210 Armonk NY IBM Corp) was used and plt 005 wasconsidered statistically significant
3 Results
)emedian age of the patients who participated in the studywas 34 years (10 88) 40 (4396) of the patients were fe-male and 51 (5604) were male )e angle between theidentified points was measured via program toolboxes Allmeasurements were repeated 3 times and the arithmeticmean was taken as the final value )e minimum andmaximum angular values measured ranged from 98deg to 139deg
)emean hook of the hamatum angle of the subjects was12255degplusmn 820deg (9720deg 13931deg) In this study no suitablecutoff point was found for the angle values )ere was adifference between gender groups according to the agedistribution )e median age of women was higher than thatof men (p 0012)
)ere was no difference between the gender groupsaccording to the angle value (p 0876) For an increase inthe angle of the hook of hamate 2 degrees by 2 degrees from98 degrees to 140 degrees a significant difference was foundbetween the change in the angle of the hook of hamate andtotal carpal tunnel volume according to correlation analysis(plt 001) (Table 1)
4 Discussion
Some studies showing the relationship between carpal tunnelsyndrome and the hamatum bone are found in the literatureChow et al believed that the variations in the hook of hamate(bipartite hypoplastic aplastic) may decrease the volumeavailable in the carpal tunnel because of the loss of a portion ofthe ulnar border [19]Moreover they concluded that there was asignificant increase in the incidence of variation in the hook of
hamate in a group with CTS A study published in 1997 byRichards and Bennet [2] evaluated the abnormalities of the hookof hamate in 131 hands )ey identified 3 aplastic 1 bipartiteand 1 nonunion of a fracture of the hook of the hamate )eirstudy found a significantly higher incidence (23) of variationsin the hook of hamate in patients presenting with CTSHowever to the best of our knowledge the relationship betweenthe angle of the hamatumcurvature and the volume of the carpaltunnel has not been investigated in the literature to date
)e shape and dimensions of the wrist have been im-plicated as predisposing factors producing a narrower carpaltunnel that is more prone to increased pressure [20 21]
Anthropometric comparison of patient and controlgroups indicates that wrist and hand dimensions may con-tribute to idiopathic carpal tunnel syndrome [22] Variousvolumetric methods were used to calculate the volume of thecarpal tunnel )in-section MRI or CT scans (4ndash5mm) wereused to create a 3-dimensional reconstruction image of thecarpal tunnel [17 23] Richman et al [23] determined thecarpal tunnel volume and carpal arch within 10 cadavericspecimens using 3-dimensional computer reconstruction ofmagnetic resonance images MRI-acquired data were com-pared with direct measurements of cadaveric carpal tunnelsusing the silicone injection technique In carpal tunnel vol-ume measurements the angle of hamatum curvature was notconsidered a variable and its effect on carpal tunnel volumewas not investigated We hypothesize that an anatomicalangle change in the hamatum curvature changes the carpaltunnel volume We tested the hypothesis of the hamatumcurvature with themathematical model)e data clearly showthat there is a high correlation between the carpal tunnelvolume and angle of hamatum curvature )is correlationmay be significant in the development of CTS )is hashowever not been studied as none of the subjects in thisstudy had clinical evidence of CTS
Table 1 Analyses of carpal tunnel volume changes with angle differences
Alfa Alfa radyan Cos (alfa) r1 r2 L Volume98 1710422667 minus 0139173101 829047701 98369 194 5016416100 1745329252 minus 0173648178 841499036 98369 194 5083523102 1780235837 minus 0207911691 853694043 98369 194 5149859104 1815142422 minus 0241921896 865629006 98369 194 5215364106 1850049007 minus 0275637356 87730029 98369 194 5279982108 1884955592 minus 0309016994 88870434 98369 194 5343655110 1919862177 minus 0342020143 899837682 98369 194 5406326112 1954768762 minus 0374606593 910696924 98369 194 5467939114 1989675347 minus 0406736643 92127876 98369 194 5528438116 2024581932 minus 0438371147 931579965 98369 194 558777118 2059488517 minus 0469471563 941597402 98369 194 5645881120 2094395102 minus 05 951328019 98369 194 5702718122 2129301687 minus 0529919264 960768853 98369 194 575823124 2164208272 minus 0559192903 969917027 98369 194 5812367126 2199114858 minus 0587785252 978769754 98369 194 5865078128 2234021443 minus 0615661475 987324339 98369 194 5916317130 2268928028 minus 064278761 995578176 98369 194 5966036132 2303834613 minus 0669130606 100352875 98369 194 601419134 2338741198 minus 069465837 101117364 98369 194 6060735136 2373647783 minus 07193398 101851051 98369 194 6105628138 2408554368 minus 0743144825 102553714 98369 194 6148827140 2443460953 minus 0766044443 103225138 98369 194 6190293
Computational and Mathematical Methods in Medicine 5
)ere are weaknesses in this study Our measurementswere performed only in healthy subjects Because we did notknow whether the hamatum curvature angle influenced thevolume of the carpal tunnel before the study we did not havea computed tomography scan in patients with carpal tun-nels We know that computed tomography will create anunnecessary radiation burden on patients In our futurestudies we aim to compare the values of the hamatumcurvature angle of the healthy population with those ofpatients with a carpal tunnel diagnosis
Additionally it is evident that this mathematical modelcannot simulate every wrist at 100 In real-life cases inletand outlet areas are not perfect cones or circles however thismodel still provides valuable data for further clinical studies
)e results of our study will emphasize the importance oftaking into account the anatomical features of the hamatumbone especially the angle of curvature which may play apredisposing role in idiopathic carpal tunnel syndromeInvestigation of the correlation between the angle ofhamatum curvature and carpal tunnel volume requiresfurther clinical study
Data Availability
)e data used to support the findings of this study are in-cluded within the article (Table 1)
Ethical Approval
)is study was approved by the Research and EthicsCommittee of our hospital and was carried out according tothe principles of the Declaration of Helsinki
Conflicts of Interest
All authors declare that they have no conflicts of interest
References
[1] G D Papanicolaou S J McCabe and J Firrell ldquo)e prev-alence and characteristics of nerve compression symptoms inthe general populationrdquo4e Journal of Hand Surgery vol 26no 3 pp 460ndash466 2001
[2] R S Richards and J D Bennett ldquoAbnormalities of the hook ofthe hamate in patients with carpal tunnel syndromerdquo Annalsof Plastic Surgery vol 39 no 1 pp 44ndash46 1997
[3] F K Fuss and T F Wagner ldquoBiomechanical alterations in thecarpal arch and hand muscles after carpal tunnel release afurther approach toward understanding the function of theflexor retinaculum and the cause of postoperative gripweaknessrdquo Clinical Anatomy vol 9 no 2 pp 100ndash108 1996
[4] M B Rotman and J P Donovan ldquoPractical anatomy of thecarpal tunnelrdquoHand Clinics vol 18 no 2 pp 219ndash230 2002
[5] T K Cobb G A Knudson and W P Cooney ldquo)e use oftopographical landmarks to improve the outcome of Agee en-doscopic carpal tunnel releaserdquo Arthroscopy 4e Journal ofArthroscopic amp Related Surgery vol 11 no 2 pp 165ndash172 1995
[6] T K Cobb W P Cooney and K-N An ldquoClinical location ofhook of hamate a technical note for endoscopic carpal tunnelreleaserdquo 4e Journal of Hand Surgery vol 19 no 3pp 516ndash518 1994
[7] F B Bogart ldquoVariation of the bones of the wristrdquo AmericanJournal of Roentgenology vol 50 pp 638ndash646 1932
[8] C Pierre-Jerome S I Bekkelund G Husby S I MellgrenM Osteaux and R Nordstrom ldquoMRI of anatomical variantsof the wrist in womenrdquo Surgical and Radiologic Anatomyvol 18 no 1 pp 37ndash41 1996
[9] C Pierre-Jerome and I K Roug ldquoMRI of bilateral bipartitehamulus a case reportrdquo Surgical and Radiologic Anatomyvol 20 no 4 pp 299ndash302 1998
[10] M H Greene and A M Hadied ldquoBipartite hamulus withulnar tunnel syndrome-Case report and literature reviewrdquo4e Journal of Hand Surgery vol 6 no 6 pp 605ndash609 1981
[11] P J L Jebson and J M Agee ldquoCarpal tunnel syndromeunusual contraindications to endoscopic releaserdquo Arthros-copy 4e Journal of Arthroscopic amp Related Surgery vol 12no 6 pp 749ndash751 1996
[12] L L Seeger L W Bassett and R H Gold ldquoCase report 464rdquoSkeletal Radiology vol 17 no 1 pp 85-86 1988
[13] H K Watson and J Weinzweig 4e Wrist LippincottWilliams and Wilkins Philadelphia PA USA 2001
[14] M Skie J Zeiss N A Ebraheim and W )omas JacksonldquoCarpal tunnel changes and median nerve compression duringwrist flexion and extension seen bymagnetic resonance imagingrdquo4e Journal of Hand Surgery vol 15 no 6 pp 934ndash939 1990
[15] K H Allmann R Horch M Uhl et al ldquoMR imaging of thecarpal tunnelrdquo European Journal of Radiology vol 25 no 2pp 141ndash145 1997
[16] T K Cobb B K Dalley R H Posteraro and R C LewisldquoEstablishment of carpal contentscanal ratio by means ofmagnetic resonance imagingrdquo 4e Journal of Hand Surgeryvol 17 no 5 pp 843ndash849 1992
[17] C Pierre-Jerome S Bekkelund and R Nordstroslashm ldquoQuan-titative MRI analysis of anatomic dimensions of the carpaltunnel in womenrdquo Surgical and Radiologic Anatomy vol 19no 1 pp 31ndash34 1997
[18] L Pavlidis B E Chalidis E Demiri and C G Dimitriouldquo)e effect of transverse carpal ligament lengthening on carpaltunnel volumetry a comparison between four techniquesrdquoAnnals of Plastic Surgery vol 65 no 5 pp 480ndash484 2010
[19] J C Y Chow M A Weiss and Y Gu ldquoAnatomic variationsof the hook of hamate and the relationship to carpal tunnelsyndromerdquo 4e Journal of Hand Surgery vol 30 no 6pp 1242ndash1247 2005
[20] P G Lim S Tan and T S Ahmad ldquo)e role of wrist an-thropometric measurement in idiopathic carpal tunnel syn-dromerdquo Journal of Hand Surgery (European Volume) vol 33no 5 pp 645ndash647 2008
[21] J E Farmer and T R C Davis ldquoCarpal tunnel syndrome acase-control study evaluating its relationship with body massindex and hand and wrist measurementsrdquo Journal of HandSurgery (European Volume) vol 33 no 4 pp 445ndash448 2008
[22] J P M Mogk and P J Keir ldquoWrist and carpal tunnel size andshape measurements effects of posturerdquo Clinical Biome-chanics vol 23 no 9 pp 1112ndash1120 2008
[23] J A Richman R H Gelberman B L Rydevik V M Gylys-Morin P C Hajek and D J Sartoris ldquoCarpal tunnel volumedetermination by magnetic resonance imaging three-di-mensional reconstructionrdquo 4e Journal of Hand Surgeryvol 12 no 5 pp 712ndash717 1987
6 Computational and Mathematical Methods in Medicine
210 Armonk NY IBM Corp) was used and plt 005 wasconsidered statistically significant
3 Results
)emedian age of the patients who participated in the studywas 34 years (10 88) 40 (4396) of the patients were fe-male and 51 (5604) were male )e angle between theidentified points was measured via program toolboxes Allmeasurements were repeated 3 times and the arithmeticmean was taken as the final value )e minimum andmaximum angular values measured ranged from 98deg to 139deg
)emean hook of the hamatum angle of the subjects was12255degplusmn 820deg (9720deg 13931deg) In this study no suitablecutoff point was found for the angle values )ere was adifference between gender groups according to the agedistribution )e median age of women was higher than thatof men (p 0012)
)ere was no difference between the gender groupsaccording to the angle value (p 0876) For an increase inthe angle of the hook of hamate 2 degrees by 2 degrees from98 degrees to 140 degrees a significant difference was foundbetween the change in the angle of the hook of hamate andtotal carpal tunnel volume according to correlation analysis(plt 001) (Table 1)
4 Discussion
Some studies showing the relationship between carpal tunnelsyndrome and the hamatum bone are found in the literatureChow et al believed that the variations in the hook of hamate(bipartite hypoplastic aplastic) may decrease the volumeavailable in the carpal tunnel because of the loss of a portion ofthe ulnar border [19]Moreover they concluded that there was asignificant increase in the incidence of variation in the hook of
hamate in a group with CTS A study published in 1997 byRichards and Bennet [2] evaluated the abnormalities of the hookof hamate in 131 hands )ey identified 3 aplastic 1 bipartiteand 1 nonunion of a fracture of the hook of the hamate )eirstudy found a significantly higher incidence (23) of variationsin the hook of hamate in patients presenting with CTSHowever to the best of our knowledge the relationship betweenthe angle of the hamatumcurvature and the volume of the carpaltunnel has not been investigated in the literature to date
)e shape and dimensions of the wrist have been im-plicated as predisposing factors producing a narrower carpaltunnel that is more prone to increased pressure [20 21]
Anthropometric comparison of patient and controlgroups indicates that wrist and hand dimensions may con-tribute to idiopathic carpal tunnel syndrome [22] Variousvolumetric methods were used to calculate the volume of thecarpal tunnel )in-section MRI or CT scans (4ndash5mm) wereused to create a 3-dimensional reconstruction image of thecarpal tunnel [17 23] Richman et al [23] determined thecarpal tunnel volume and carpal arch within 10 cadavericspecimens using 3-dimensional computer reconstruction ofmagnetic resonance images MRI-acquired data were com-pared with direct measurements of cadaveric carpal tunnelsusing the silicone injection technique In carpal tunnel vol-ume measurements the angle of hamatum curvature was notconsidered a variable and its effect on carpal tunnel volumewas not investigated We hypothesize that an anatomicalangle change in the hamatum curvature changes the carpaltunnel volume We tested the hypothesis of the hamatumcurvature with themathematical model)e data clearly showthat there is a high correlation between the carpal tunnelvolume and angle of hamatum curvature )is correlationmay be significant in the development of CTS )is hashowever not been studied as none of the subjects in thisstudy had clinical evidence of CTS
Table 1 Analyses of carpal tunnel volume changes with angle differences
Alfa Alfa radyan Cos (alfa) r1 r2 L Volume98 1710422667 minus 0139173101 829047701 98369 194 5016416100 1745329252 minus 0173648178 841499036 98369 194 5083523102 1780235837 minus 0207911691 853694043 98369 194 5149859104 1815142422 minus 0241921896 865629006 98369 194 5215364106 1850049007 minus 0275637356 87730029 98369 194 5279982108 1884955592 minus 0309016994 88870434 98369 194 5343655110 1919862177 minus 0342020143 899837682 98369 194 5406326112 1954768762 minus 0374606593 910696924 98369 194 5467939114 1989675347 minus 0406736643 92127876 98369 194 5528438116 2024581932 minus 0438371147 931579965 98369 194 558777118 2059488517 minus 0469471563 941597402 98369 194 5645881120 2094395102 minus 05 951328019 98369 194 5702718122 2129301687 minus 0529919264 960768853 98369 194 575823124 2164208272 minus 0559192903 969917027 98369 194 5812367126 2199114858 minus 0587785252 978769754 98369 194 5865078128 2234021443 minus 0615661475 987324339 98369 194 5916317130 2268928028 minus 064278761 995578176 98369 194 5966036132 2303834613 minus 0669130606 100352875 98369 194 601419134 2338741198 minus 069465837 101117364 98369 194 6060735136 2373647783 minus 07193398 101851051 98369 194 6105628138 2408554368 minus 0743144825 102553714 98369 194 6148827140 2443460953 minus 0766044443 103225138 98369 194 6190293
Computational and Mathematical Methods in Medicine 5
)ere are weaknesses in this study Our measurementswere performed only in healthy subjects Because we did notknow whether the hamatum curvature angle influenced thevolume of the carpal tunnel before the study we did not havea computed tomography scan in patients with carpal tun-nels We know that computed tomography will create anunnecessary radiation burden on patients In our futurestudies we aim to compare the values of the hamatumcurvature angle of the healthy population with those ofpatients with a carpal tunnel diagnosis
Additionally it is evident that this mathematical modelcannot simulate every wrist at 100 In real-life cases inletand outlet areas are not perfect cones or circles however thismodel still provides valuable data for further clinical studies
)e results of our study will emphasize the importance oftaking into account the anatomical features of the hamatumbone especially the angle of curvature which may play apredisposing role in idiopathic carpal tunnel syndromeInvestigation of the correlation between the angle ofhamatum curvature and carpal tunnel volume requiresfurther clinical study
Data Availability
)e data used to support the findings of this study are in-cluded within the article (Table 1)
Ethical Approval
)is study was approved by the Research and EthicsCommittee of our hospital and was carried out according tothe principles of the Declaration of Helsinki
Conflicts of Interest
All authors declare that they have no conflicts of interest
References
[1] G D Papanicolaou S J McCabe and J Firrell ldquo)e prev-alence and characteristics of nerve compression symptoms inthe general populationrdquo4e Journal of Hand Surgery vol 26no 3 pp 460ndash466 2001
[2] R S Richards and J D Bennett ldquoAbnormalities of the hook ofthe hamate in patients with carpal tunnel syndromerdquo Annalsof Plastic Surgery vol 39 no 1 pp 44ndash46 1997
[3] F K Fuss and T F Wagner ldquoBiomechanical alterations in thecarpal arch and hand muscles after carpal tunnel release afurther approach toward understanding the function of theflexor retinaculum and the cause of postoperative gripweaknessrdquo Clinical Anatomy vol 9 no 2 pp 100ndash108 1996
[4] M B Rotman and J P Donovan ldquoPractical anatomy of thecarpal tunnelrdquoHand Clinics vol 18 no 2 pp 219ndash230 2002
[5] T K Cobb G A Knudson and W P Cooney ldquo)e use oftopographical landmarks to improve the outcome of Agee en-doscopic carpal tunnel releaserdquo Arthroscopy 4e Journal ofArthroscopic amp Related Surgery vol 11 no 2 pp 165ndash172 1995
[6] T K Cobb W P Cooney and K-N An ldquoClinical location ofhook of hamate a technical note for endoscopic carpal tunnelreleaserdquo 4e Journal of Hand Surgery vol 19 no 3pp 516ndash518 1994
[7] F B Bogart ldquoVariation of the bones of the wristrdquo AmericanJournal of Roentgenology vol 50 pp 638ndash646 1932
[8] C Pierre-Jerome S I Bekkelund G Husby S I MellgrenM Osteaux and R Nordstrom ldquoMRI of anatomical variantsof the wrist in womenrdquo Surgical and Radiologic Anatomyvol 18 no 1 pp 37ndash41 1996
[9] C Pierre-Jerome and I K Roug ldquoMRI of bilateral bipartitehamulus a case reportrdquo Surgical and Radiologic Anatomyvol 20 no 4 pp 299ndash302 1998
[10] M H Greene and A M Hadied ldquoBipartite hamulus withulnar tunnel syndrome-Case report and literature reviewrdquo4e Journal of Hand Surgery vol 6 no 6 pp 605ndash609 1981
[11] P J L Jebson and J M Agee ldquoCarpal tunnel syndromeunusual contraindications to endoscopic releaserdquo Arthros-copy 4e Journal of Arthroscopic amp Related Surgery vol 12no 6 pp 749ndash751 1996
[12] L L Seeger L W Bassett and R H Gold ldquoCase report 464rdquoSkeletal Radiology vol 17 no 1 pp 85-86 1988
[13] H K Watson and J Weinzweig 4e Wrist LippincottWilliams and Wilkins Philadelphia PA USA 2001
[14] M Skie J Zeiss N A Ebraheim and W )omas JacksonldquoCarpal tunnel changes and median nerve compression duringwrist flexion and extension seen bymagnetic resonance imagingrdquo4e Journal of Hand Surgery vol 15 no 6 pp 934ndash939 1990
[15] K H Allmann R Horch M Uhl et al ldquoMR imaging of thecarpal tunnelrdquo European Journal of Radiology vol 25 no 2pp 141ndash145 1997
[16] T K Cobb B K Dalley R H Posteraro and R C LewisldquoEstablishment of carpal contentscanal ratio by means ofmagnetic resonance imagingrdquo 4e Journal of Hand Surgeryvol 17 no 5 pp 843ndash849 1992
[17] C Pierre-Jerome S Bekkelund and R Nordstroslashm ldquoQuan-titative MRI analysis of anatomic dimensions of the carpaltunnel in womenrdquo Surgical and Radiologic Anatomy vol 19no 1 pp 31ndash34 1997
[18] L Pavlidis B E Chalidis E Demiri and C G Dimitriouldquo)e effect of transverse carpal ligament lengthening on carpaltunnel volumetry a comparison between four techniquesrdquoAnnals of Plastic Surgery vol 65 no 5 pp 480ndash484 2010
[19] J C Y Chow M A Weiss and Y Gu ldquoAnatomic variationsof the hook of hamate and the relationship to carpal tunnelsyndromerdquo 4e Journal of Hand Surgery vol 30 no 6pp 1242ndash1247 2005
[20] P G Lim S Tan and T S Ahmad ldquo)e role of wrist an-thropometric measurement in idiopathic carpal tunnel syn-dromerdquo Journal of Hand Surgery (European Volume) vol 33no 5 pp 645ndash647 2008
[21] J E Farmer and T R C Davis ldquoCarpal tunnel syndrome acase-control study evaluating its relationship with body massindex and hand and wrist measurementsrdquo Journal of HandSurgery (European Volume) vol 33 no 4 pp 445ndash448 2008
[22] J P M Mogk and P J Keir ldquoWrist and carpal tunnel size andshape measurements effects of posturerdquo Clinical Biome-chanics vol 23 no 9 pp 1112ndash1120 2008
[23] J A Richman R H Gelberman B L Rydevik V M Gylys-Morin P C Hajek and D J Sartoris ldquoCarpal tunnel volumedetermination by magnetic resonance imaging three-di-mensional reconstructionrdquo 4e Journal of Hand Surgeryvol 12 no 5 pp 712ndash717 1987
6 Computational and Mathematical Methods in Medicine

)ere are weaknesses in this study Our measurementswere performed only in healthy subjects Because we did notknow whether the hamatum curvature angle influenced thevolume of the carpal tunnel before the study we did not havea computed tomography scan in patients with carpal tun-nels We know that computed tomography will create anunnecessary radiation burden on patients In our futurestudies we aim to compare the values of the hamatumcurvature angle of the healthy population with those ofpatients with a carpal tunnel diagnosis
Additionally it is evident that this mathematical modelcannot simulate every wrist at 100 In real-life cases inletand outlet areas are not perfect cones or circles however thismodel still provides valuable data for further clinical studies
)e results of our study will emphasize the importance oftaking into account the anatomical features of the hamatumbone especially the angle of curvature which may play apredisposing role in idiopathic carpal tunnel syndromeInvestigation of the correlation between the angle ofhamatum curvature and carpal tunnel volume requiresfurther clinical study
Data Availability
)e data used to support the findings of this study are in-cluded within the article (Table 1)
Ethical Approval
)is study was approved by the Research and EthicsCommittee of our hospital and was carried out according tothe principles of the Declaration of Helsinki
Conflicts of Interest
All authors declare that they have no conflicts of interest
References
[1] G D Papanicolaou S J McCabe and J Firrell ldquo)e prev-alence and characteristics of nerve compression symptoms inthe general populationrdquo4e Journal of Hand Surgery vol 26no 3 pp 460ndash466 2001
[2] R S Richards and J D Bennett ldquoAbnormalities of the hook ofthe hamate in patients with carpal tunnel syndromerdquo Annalsof Plastic Surgery vol 39 no 1 pp 44ndash46 1997
[3] F K Fuss and T F Wagner ldquoBiomechanical alterations in thecarpal arch and hand muscles after carpal tunnel release afurther approach toward understanding the function of theflexor retinaculum and the cause of postoperative gripweaknessrdquo Clinical Anatomy vol 9 no 2 pp 100ndash108 1996
[4] M B Rotman and J P Donovan ldquoPractical anatomy of thecarpal tunnelrdquoHand Clinics vol 18 no 2 pp 219ndash230 2002
[5] T K Cobb G A Knudson and W P Cooney ldquo)e use oftopographical landmarks to improve the outcome of Agee en-doscopic carpal tunnel releaserdquo Arthroscopy 4e Journal ofArthroscopic amp Related Surgery vol 11 no 2 pp 165ndash172 1995
[6] T K Cobb W P Cooney and K-N An ldquoClinical location ofhook of hamate a technical note for endoscopic carpal tunnelreleaserdquo 4e Journal of Hand Surgery vol 19 no 3pp 516ndash518 1994
[7] F B Bogart ldquoVariation of the bones of the wristrdquo AmericanJournal of Roentgenology vol 50 pp 638ndash646 1932
[8] C Pierre-Jerome S I Bekkelund G Husby S I MellgrenM Osteaux and R Nordstrom ldquoMRI of anatomical variantsof the wrist in womenrdquo Surgical and Radiologic Anatomyvol 18 no 1 pp 37ndash41 1996
[9] C Pierre-Jerome and I K Roug ldquoMRI of bilateral bipartitehamulus a case reportrdquo Surgical and Radiologic Anatomyvol 20 no 4 pp 299ndash302 1998
[10] M H Greene and A M Hadied ldquoBipartite hamulus withulnar tunnel syndrome-Case report and literature reviewrdquo4e Journal of Hand Surgery vol 6 no 6 pp 605ndash609 1981
[11] P J L Jebson and J M Agee ldquoCarpal tunnel syndromeunusual contraindications to endoscopic releaserdquo Arthros-copy 4e Journal of Arthroscopic amp Related Surgery vol 12no 6 pp 749ndash751 1996
[12] L L Seeger L W Bassett and R H Gold ldquoCase report 464rdquoSkeletal Radiology vol 17 no 1 pp 85-86 1988
[13] H K Watson and J Weinzweig 4e Wrist LippincottWilliams and Wilkins Philadelphia PA USA 2001
[14] M Skie J Zeiss N A Ebraheim and W )omas JacksonldquoCarpal tunnel changes and median nerve compression duringwrist flexion and extension seen bymagnetic resonance imagingrdquo4e Journal of Hand Surgery vol 15 no 6 pp 934ndash939 1990
[15] K H Allmann R Horch M Uhl et al ldquoMR imaging of thecarpal tunnelrdquo European Journal of Radiology vol 25 no 2pp 141ndash145 1997
[16] T K Cobb B K Dalley R H Posteraro and R C LewisldquoEstablishment of carpal contentscanal ratio by means ofmagnetic resonance imagingrdquo 4e Journal of Hand Surgeryvol 17 no 5 pp 843ndash849 1992
[17] C Pierre-Jerome S Bekkelund and R Nordstroslashm ldquoQuan-titative MRI analysis of anatomic dimensions of the carpaltunnel in womenrdquo Surgical and Radiologic Anatomy vol 19no 1 pp 31ndash34 1997
[18] L Pavlidis B E Chalidis E Demiri and C G Dimitriouldquo)e effect of transverse carpal ligament lengthening on carpaltunnel volumetry a comparison between four techniquesrdquoAnnals of Plastic Surgery vol 65 no 5 pp 480ndash484 2010
[19] J C Y Chow M A Weiss and Y Gu ldquoAnatomic variationsof the hook of hamate and the relationship to carpal tunnelsyndromerdquo 4e Journal of Hand Surgery vol 30 no 6pp 1242ndash1247 2005
[20] P G Lim S Tan and T S Ahmad ldquo)e role of wrist an-thropometric measurement in idiopathic carpal tunnel syn-dromerdquo Journal of Hand Surgery (European Volume) vol 33no 5 pp 645ndash647 2008
[21] J E Farmer and T R C Davis ldquoCarpal tunnel syndrome acase-control study evaluating its relationship with body massindex and hand and wrist measurementsrdquo Journal of HandSurgery (European Volume) vol 33 no 4 pp 445ndash448 2008
[22] J P M Mogk and P J Keir ldquoWrist and carpal tunnel size andshape measurements effects of posturerdquo Clinical Biome-chanics vol 23 no 9 pp 1112ndash1120 2008
[23] J A Richman R H Gelberman B L Rydevik V M Gylys-Morin P C Hajek and D J Sartoris ldquoCarpal tunnel volumedetermination by magnetic resonance imaging three-di-mensional reconstructionrdquo 4e Journal of Hand Surgeryvol 12 no 5 pp 712ndash717 1987
6 Computational and Mathematical Methods in Medicine











![[18'] Carpal](https://img.pdfslide.net/doc/110x75/577d20351a28ab4e1e924083/18-carpal.jpg)