Embed Size (px)
Citation preview

Med. J. Cairo Univ., Vol. 83, No. 2, December: 37-44, 2015
www.medicaljournalofcairouniversity.net
The Effect of Kinesio Taping on Seated Postural Control in
Spastic Diplegic Cerebral Palsy Children
WANEES M. BADAWY, Ph.D.*; MOHAMED B. IBRAHEM, Ph.D.** and KHALED M. SHAWKY, M.D.***
The Departments of Physical Therapy for Neuromuscular Disorder & Its Surgery* and Physical Therapy for Growth & Development Disorders in Children and Its Surgery**, Faculty of Physical Therapy, Cairo University** and
The Department of Radiology, Faculty of Medicine, Zagazig University***, Egypt
Abstract
Background: Children with spastic diplegic Cerebral Palsy (CP) often show the difficulty to achieve well-balanced sitting
posture and display the poor sitting posture such as flexed
trunk with kyphotic curvature of the spine and asymmetry of
trunk.
Aim of the Study: The present study was designed to determine the effectiveness of kinesio taping over the paraspi-nal muscles in improving sitting balance in young children with Spastic Diplegic (CP) who displayed poor trunk control.
Material and Methods: Thirty children with Spastic Diplegic (CP) of both sexes with age ranged between 10-16
months were included in this study. Children were randomly
assigned to two equal groups (Group I and Group II). The study group (Group I) was treated by kinesio taping which was applied over the paraspinal region for 12 successive weeks in addition to a designed physical therapy program.
The control group (Group II) was treated by the designed
physical therapy program only. The children were evaluated by sitting score of Gross Motor Function Measure (GMFM)
and radiographic studies (Kyphotic and Cobb's angles) were
carried out on the whole spine while the children were sitting
before and after treatment.
Results: There was a statistically significant improvement
in the measured parameters in both groups when comparing
their pre and post treatment mean values. However, significant
difference was recorded between the two groups after treatment
in favor of the study group.
Conclusion: The obtained results suggest that the appli-cation of kinesio taping over the trunk become a beneficial
therapeutic technique in improving the sitting posture and
trunk control in children with Spastic Diplegic (CP) when
adjunct to a physical therapy program.
Key Words: Cerebral palsy – Spastic diplegia – Trunk control – Kinesio taping – Dynamic splint.
Introduction
CEREBRAL Palsy (CP) describes a group of
disorders of the development of movement and
posture causing activity limitations that are attrib-
Correspondence to: Dr. Wanees M.A. Badawy, E-mail: [email protected]
uted to non progressive disturbances that occurred
in the developing fetus or infant brain [1] . Cerebral palsy is the major developmental disability affecting
function in children. It is characterized by the
inability to normally control motor functions and
it has the potential to have an effect on the overall
development of a child [2] .
Most children with spastic diplegia have some motor impairment in their upper extremities milder
than lower ones. The primary functional problems include difficulty with mobility and posture. Other
problems include postural deviations, inability to
sit without support, inability to stand and difficulty
in movement transitions [3] .
Sitting is an important step for child to achieve
the upright posture against gravity and also an essential activity to provide the postural background
tone required for the functional movement of upper
extremity. However, the children with CP often
show the difficulty to achieve well-balanced sitting
posture and display the poor sitting posture such as flexed trunk with kyphotic curvature of the spine and asymmetry of trunk [4] .
Therapeutic interventions for seated postural
dyscontrol typically are directed at improving the
quality of information feedback, as well as stabi-lizing the body for functional control. This can
theoretically be achieved by improving postural alignment and gravitational forces concerning the body via which best possible muscle length and
normalization of recruitment and timing patterns
of muscles might be executed. These interventions might enable control to be gained over the entire
vertically oriented column of segments [5] .
The application of thermoplastic orthotic de-vices may allow the child to gain such control. The rigidity of this type of orthotic intervention
37

38 The Effect of Kinesio Taping on Seated Postural Control
theoretically acts through biomechanical principles
to reduce the degrees of freedom at which learning
must simultaneously take place, to control postural
alignment, to prevent deformity and to improve
function [6] . While the thermoplastic orthotic in-tervention can be used for seated postural control,
it is at the sacrifice of the child's ability to move
freely and limits the child's sensorimotor experi-ences for motor learning. Dynamic bracing offers
an alternative approach. Such braces are generally
fabricated from lycra material and have been re-ferred to as dynamic lycra pressure orthoses, lycra
garment or lycra splints. The inbuilt flexibility of
these orthoses allows movement freedom whilst
ensuring close skin contact with dynamic corrective
forces; therefore the child experiences more normal
movement patterns, these preferred movements
could be learned [7] .
Results from previous intervention studies on children with CP suggest that improvements in sitting control can be achieved through the facili-tation of sensorimotor systems, improvement of
postural alignment and dynamic splinting usage [8] . Although dynamic splinting is certainly avail-able as an intervention choice for poor postural
control, the used brace can be: (1) Meet the an
individual child needs, (2) Expensive, (3) Seemed
to be unsuitable and not used friendly, (4) Hot,
and (5) Not accommodative to the child growth
[7] .
As an alternative to lycra garments, therapeutic
taping may afford similar advantages for controlling
the seated posture in children with CP. It is antic-ipated that therapeutic taping would offer the
establishment for improved functional sitting abil-ities by: (1) Increasing proprioceptive and tactile
facilitation, (2) Controlling trunk movement in the
frontal and sagittal planes, (3) Restoring optimal
muscle length to provide a foundation for normal firing and recruitment patterns, (4) Orienting the
muscle force along more normal vectors, (5) As-sisting with static and dynamic balance and (6)
Optimizing gravitational forces about the column
of segments by improving body alignment [9] .
A very useful physiotherapeutic modality if
applied properly is the kinesio tape, which is a
valuable adjunct to therapeutic rehabilitation. It is
a specialized tape which is thin, elastic and can be stretched up to 120-140% of its original length
making it quite elastic, compared with the conven-tional taping. It allows a partial to full range of motion for the applied muscles and joints with
different pulling forces to the skin [9] . It is a tech-nique that allows a therapist to work on more
purposeful activities through improved proper
alignment but with the tape acting as an extra hand
[10] .
Therefore, this study was designed to determine
the effect of using kinesio taping over paraspinal
musculature on functional sitting control in children
with spastic CP.
Patients and Methods
Thirty CP children aged from 10-16 months were enrolled in this study as subjects. Children were selected from the outpatient clinic of the
Faculty of Physcial Therapy, Cairo University in the period from January 2015 to June 2015. Sub-jects were divided randomly into two equal groups. The first group (Group I) was treated by kinesio
taping which was applied over the paraspinal region
in addition to a designed physical therapy program.
The second group (Group II) received the same designed physical therapy program only.
The patients were diagnosed as having CP with
spastic diplegia based on careful clinical assessment by a neuropediatrican and magnetic resonance
imaging of the brain. The subjects' parents signed
a written consent forms approved by the Ethics
Committee of the Faculty of Physical Therapy,
Cairo University.
Study design: This was a randomized controlled trail.
Inclusion criteria were children who have had CP since birth. Patients displayed abnormal neuro-logic signs such as hypertonia in both lower limbs, ankle clonus, hyperactive deep tendon reflexes and
delayed motor development. The muscle tone of
the lower limbs ranged from 1+ to 2 according to Modified Asworth Scale (MAS) for muscle tone grading [11] . Patients were unable to sit alone
according to Gross motor function measure scale
[12] .
Exclusion criteria include patients who had
fixed skeletal hip deformities, structural scoliosis,
history of surgical interference, seizures or allergic
reactions to the adhesive kinesio tape or any other
materials used in this study.
Instrumentation: - Modified Ashworth Scale for assessment of mus-
cle tone.
- The sitting section of the Gross Motor Function
Measure (GMFM-88) was used to evaluate the functional sitting abilities of the subjects. The
GMFM-88 is an observational measurement tool

Wanees M. Badawy, et al. 39
that incorporates 88 items that address five gross
motor function domains: (A) Lying and rolling, (B) Sitting, (C) Crawling and kneeling, (D) Stand-ing, (E) Walking, running and jumping [12] .
- Plain anterior-posterior and lateral radiographs
of the whole spine. Radiographs were taken while the child was sitting on chair without arm rest
with 90º of knee flexion and neutral ankle posi-tion. The upper extremities of the child were
positioned at their sides.
In this study, the kyphotic angle might represent
the magnitude of round back and the Cobb's angle
might represent the magnitude of functional trunk
asymmetry of the spine. The kyphotic angle was
measured as usual method; first both ends of ver-tebrae of kyphotic curve were identified on the
lateral whole spine film and then a line along the upper end plate of upper end vertebrae and the other line along the lower end plate of the lower
vertebrae were drawn. At last the angle formed by these two lines was measured. The Cobb's angle
was measured by finding the upper and lower limits
of the primary curve by drawing tangents to the
vertebral bodies then draw erect perpendiculars
from the vertebrae which form the limits of the
curve. The angle formed between the erect inter-secting perpendicular lines and facing the parallel
lines (tangents) is the Cobb's angle [13] .
- Kinesio® Tex Classic tape.
- 2 inches width.
- Physical therapy tools of different shapes in the
form of: Mats, wedge, rolls and medical balls.
A- Evaluation session: Assessment of spinal curvatures (kyphotic and
Cobb's angles) using the Radiographs and were conducted at the Radiology Department, Faculty
of Medicine, Cairo University. Also, assessment
of the functional sitting abilities was done using
the sitting section of the Gross Motor Function
Measure (GMFM-88). These tests were done pre-and post treatment.
B- Training Session: In the study group (GI) before using kinesio
taping a skin sensitivity test was done by applying a square piece of kinesio tape (5 X 2.5cm) over
the back and kept for 48 hours then removed and
the skin was observed for a reaction to the tape.
Since no reaction was detected, the tape was applied
for 3 days as the elastic qualities of the kinesio
tape are effective for 3-5 days before the elastic
polymer diminishes. The kinesio taping was applied
as the protocol followed by Footer [5] :
1- The subjects were positioned in a supported
upright sitting position.
2- Prior to kinesio tape application, the therapist
used medical cotton damped with alcohol to
clean the skin over the paraspinal musculature
from the first thoracic vertebra (T 1) to the level
between the third and fourth lumbar vertebrae
(L3-4) as well as over the lower trapezius muscle
from the twelfth thoracic vertebra (T12) ob-liquely to the acromion process.
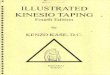
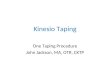
3- The kinesio tape was applied bilaterally in the following manner: Two strips were placed im-mediately lateral to the vertebral spinous pro-cesses in a caudal-cephalo direction from L3- 4 to T1 Fig. (1A) and two other strips were
placed along the course of the lower portion of
the trapezius muscle in a lateral to medial di-rection from the acromion process obliquely to
T12 Fig. (1B).
Fig. (1): Kinesio tape placements: (A) Vertical paraspinal
strips and (B) Oblique strips.
4- The tape was applied for 3 days then removed
for 24 hours to allow skin perspiration and then a new one was reapplied again [5] and the pro-cedure was repeated throughout the whole study
(12 successive weeks).
All patients in both groups (GI and GII) received
the designed physical therapy program for one and half hour, 3 times per week, day after day for 12
successive weeks. The program was based on Neurodevelopmental Technique (NDT) which di-rected towards inhibiting abnormal muscle tone
and abnormal reflexes and facilitation of normal

Kyp
hotic
ang
le 0
40
20
50
30
10
0
44.64 44.38
18.09
35.26
40 The Effect of Kinesio Taping on Seated Postural Control
movement patterns of postural control through reflex inhibiting positions using proximal and distal key points of control [14] .
- Facilitation of rolling from lower limbs.
- Exercises to facilitate static sitting and dynamic sitting.
- Facilitation of different sitting positions (e.g. side
sitting, ring sitting, half-ring sitting, crossed
sitting).
- Positioning to improve sitting posture (e.g. sitting
in adaptive seating chair, sitting in corner).
- Exercises to facilitate active trunk extension to
improve trunk control and sitting balance (e.g.
prone on wedge, sitting on edge of roll, perform-ing stooping and recovery).
- Facilitation of righting and equilibrium reactions to improve postural mechanism via variety of
exercises applied on ball from different positions in forward, backward and sideways.
- Approximation as a proprioceptive training ap-plied in a slow and rhythmic manner for upper limbs, lower limbs and trunk to control spasticity and stimulate the joint mechanoreceptors from
semi reclined and quadruped positions.
- Hand weight bearing exercises from different
sitting positions and from quadruped position.
- Facilitation of hand functions from sitting posi-tions (e.g. reaching, grasping, release, transferring objects) according to the child abilities.
Statistical analysis: GraphPad Prism 5 (Graph Pad Software Inc.,
La Jolla, CA, USA) was used for data analysis.
Data were presented as mean ± standard deviation of the mean (SD). In comparing the improvement
after the intervention in each group, paired t-test was used and for the difference between the two
groups; independent t-test was used. A (p) value of less than 0.05 was considered to represent a
statistically significant difference.
Results
Demographic and clinical characteristics of
the patients in both groups: There was no statistically significant difference
between both groups regarding mean age, kyphotic angle, Cobb's angle and GMFM-Sitting domain
pre treatment (p>0.05) (Table 1). GI included 9 boys and 6 girls while GII included 10 boys and 5 girls.
I- Comparison of kyphotic angle, Cobb's angle and GMFM-Sitting scores within groups:
Group (I):
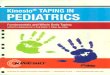
There was a statistically significant decrease in kyphotic angle and Cobb's angle values post treatment in GI (p<0.05). The mean value of ky-photic angle was 44.64 ° pre treatment and 18.09 ° post treatment. While the mean value of Cobb's
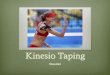
angle was 14.33 ° pre treatment and 5 ° post treat-ment. Also, there was a statistically significant
increase in GMFM-Sitting values post treatment
in GI (p<0.05). The mean value of GMFM-Sitting score was 29.76% pre treatment and 69.87% post
treatment [(Table 2), Figs. (2-4)].
Group (II):
There was a statistically significant decrease in kyphotic angle and Cobb's angle values post treatment in GII (p<0.05). The mean value of kyphotic angle was 44.38 ° pre treatment and 35.26 ° post treatment. While the mean value of Cobb's
angle was 14.75 ° pre treatment and 9.28 ° post treatment. Also, there was a statistically significant
increase in GMFM-Sitting values post treatment
in GII (p<0.05). The mean value of GMFM-Sitting
score was 29.85% pre treatment and 45.37% post
treatment [(Table 2), Figs. (2-4)].
II- Comparison between both groups as regards
kyphotic angle, Cobb's angle and GMFM-Sitting
scores post treatment:
Data presented in (Table 3) showed that there
were statistically significant difference between
both groups in their post treatment mean values of
kyphotic angle, Cobb's angle and GMFM-Sitting scores in favor of the study group (GI) (p<0.05).
GI GII
Pre treatment
Post treatment
Fig. (2): Comparison between pre and post treatment mean
values of kyphotic angle in degrees in both groups.

Cob
b's
angl
e (°
)
16
14
12
10
8
6
4
2
0
14.33 14.75
5.00
9.28
GM
FM-s
ittin
g (%
)
70
60
50
40
30
20
10
0
29.76
69.87
29.85
45.37
Wanees M. Badawy, et al. 41
GI GII
Pre treatment
Post treatment
Fig. (3): Comparison between pre and post treatment mean
values of Cobb's angle in degrees in both groups.
GI GII
Pre treatment
Post treatment
Fig. (4): Comparison between pre and post treatment mean
values of GMFM-Sitting scores in percentage in
both groups.
Table (1): Demographic and clinical characteristics of the patients in both groups (GI & GII).
Demographic and clinical characteristics
GI GII Comparison S
Mean SD Mean SD t-value p-value
Age (months) Kyphotic angle (º) Cobb’s angle (º) GMFM-sitting (%)
12.7 44.64 14.33 29.76
1.46 1.88 1.3 3.4
12.6 44.38 14.75 29.85
1.3 1.24 1.7 3.5
0.084 0.327 0.355 0.076
<0.05 <0.05 <0.05 <0.05
NS NS NS NS
GMFM
: Gross Motor Function Measure. S
: Significance. SD : Standard deviation. NS
: Non-significant. p : Probability.
Table (2): Comparison between pre and post treatment mean values of kyphotic angle, Cobb's angle
and GMFM-Sitting scores in both groups.
Variables Pre-treatment Mean ± SD
Post-treatment Mean ± SD
Mean difference
t- value
p - value
Significance
Kyphotic angle (º): GI 44.64± 1.88 18.09±0.87 26.55 33.47 <0.05 S GII 44.38± 1.24 35.26± 1.54 9.12 11.49 <0.05 S
Cobb’s angle (º): GI 14.33± 1.3 5.00±0.66 9.33 11.76 <0.05 S GII 14.75± 1.7 9.28±0.98 5.47 6.89 <0.05 S
GMFM-sitting (%): GI 29.76±3.4 69.87±4.1 40.11 50.57 <0.05 S GII 29.85±3.5 45.37±3.2 15.52 19.56 <0.05 S
GMFM
: Gross Motor Function Measure. p : Significance. SD : Standard deviation. S : Probability.
Table (3): Comparison of the mean values of kyphotic angle, Cobb's angle and GMFM-Sitting
scores between both groups post treatment.
Independent t-test
Kyphotic angle (º) Cobb’s angle (º) GMFM-sitting (%)
GI GII GI GII GI GII
Mean 18.09 35.26 5.00 9.28 69.87 45.37 SD 0.87 1.54 0.66 0.98 4.1 3.2 Mean difference 17.17 4.28 24.5 t-value 21.64 5.39 30.89 p-value <0.05 <0.05 <0.05 Significance S S S
GMFM
: Gross Motor Function Measure. p : Significance. SD : Standard deviation. S : Probability.

42 The Effect of Kinesio Taping on Seated Postural Control
Discussion
To verify the effect of kinesio taping on the trunk control, sitting posture and sitting balance were evaluated. Our concern was how to evaluate those quantitatively in very young children. The
cerebral palsied children with poor trunk control
show rounded back and trunk asymmetry while
they are sitting. From the perspective of this point,
we postulated that the kyphotic and Cobb's angles
in sitting posture be able to represent the functional
kyphosis and trunk asymmetry respectively.
The present study included spastic diplegic
type of CP, which constitutes a major classification
among spastic types. This finding was reported by Damiano [15] who reported that spastic diplegic
patients basically had better trunk control and more
potential of functional reorganization than spastic quadriplegic patients. It was suggested that the
children with spastic diplegic CP show better response to treatment than the children with spastic
quadriplegic CP. The functional skill of sitting is
required for many activities that children encounter
in their daily lives. In typical development, the
maturation of a child's postural control system
generally ensures task-specific stability and orien-tation to support the primary movements required for functional activities [16] .
The pre treatment results of the two groups
indicated that those children often show the diffi-culty to achieve well-balanced sitting posture and
display poor trunk control. This agrees with Shum-way-Cook and Woolacott [16] who revealed that children with CP often rely upon inappropriate
control strategies and faulty feedback mechanisms
when learning to maintain both static and dynamic sitting postures, which predictably leads to postural
dyscontrol and functional dependency. In other
words, the postural control system cannot effec-tively control the body's position and motion in
space because it lacks the ability to generate ap-propriate muscular force and to coordinate and
integrate the sensory information received from
various receptors throughout the body.
Statistical analysis of the post treatment results
of the two groups revealed significant improvement
in postural stability and functional ability which
is represented by keeping the body segments prop-erly aligned in upright sitting posture. Improvement
fulfilled in the control group might be attributed
to the effect of the therapeutic exercise program
which emphasized on a group of exercises for
facilitation of normal erect posture, this comes in agreement with Kern et al., [17] who established
that methods of physical therapy treatment for
children with CP focus on the attainment of se-quential developmental milestones and facilitation
of normal movement patterns.
The significant improvement in the post treat-ment results in the control group also comes in
agreement with Sterba et al., [18] who recommended strengthening of the trunk and core muscles, pro-motion of postural and equilibrium reactions and focus on postural alignment in sitting, standing and walking considered as components of physical
therapy treatment plans for pediatric therapists
who rehabilitate children with neurological condi-tions.
In respect to the study group who received kinesio taping which applied over the paraspinal
region in addition to the designed therapeutic exercise program, there was significant improve-ment in the sitting posture and trunk control in young children with spastic diplegic CP. This comes
in consistent with Hsu et al., [19] who reported that kinesio tape as an adjunct to the therapeutic pro-cedures can improve strength, functional activities, proprioception, control and positioning.
In addition this comes in agreement with Miller et al., [20] who conducted a study to examine the effect of kinesio taping on hypotonia. Four special
needs children were selected to participate in the
study. Kinesio taping was applied to the internal
and external oblique muscles once a week for four
consecutive weeks. They concluded that kinesio taping may be an effective tool for children with
hypotonia to improve core stability, attention to
task, sitting posture and fine motor skills.
Another study was performed by Yasukawa et
al., [21] to investigate the effects of kinesio taping
in an acute pediatric rehabilitation setting, they
used the kinesio taping for the upper extremity in enhancing functional motor skills of children. They
concluded that kinesio taping may be associated
with improvement in upper extremity control and
function in the acute pediatric rehabilitation setting.
In the current study, kinesio taping was applied
on the paraspinal muscles from origin to insertion.
In the context, Vithoulk et al., [22] stated that application of the tape from muscle origin to in-sertion is supportive, improves contraction and increases muscle strength. The wrinkles of the skin
formed after the application of kinesio taping in combination with the direction of the tape pulls the insertion of the muscle towards the direction
of the contraction and increases the muscle tone.

Wanees M. Badawy, et al. 43
Kinesio tape improves proprioception by pro-viding constant cutaneous afferent stimulation of
the skin. This activity improves joint function,
stimulates sensory mechanisms, decreases pain as
a result of a reduction in neurological activation, enhances blood and lymph circulation to the local
area by lifting fascia and soft tissue, realigns fascia
tissue function through normalizing muscle tension,
and improves muscle function. Conducted studies
which examined the effects of kinesio taping on
cutaneous mechanoreceptors have reported that,
kinesio taping application on selected muscles and
joints may improve muscle excitability [23-26] . On the other hand, Slupik et al., [27] proved that kinesio taping showed a significant increase in the bioelec-trical activity of the vastus medialis muscle after
24 hours of kinesio taping application and that
effect was maintained for another 48 hours after
removal of the tape.
The improvement observed in the study group comes in agreement with Simsek et al., [28] and Kaya Kara et al., [29] who concluded that kinesio taping was valuable when adjunct to an exercise
or manual therapy programs to achieve the required
goals and maximize functional independence and
there are no absolute contraindications to the use
of kinesio taping as a part of comprehensive phys-iotherapeutic management.
Conclusion: The children with spastic diplegic CP showed
better response to given treatment. Therefore,
kinesio taping applied over back muscles might
be a useful therapeutic tool and can be added with
the physical therapy as an additional modality to
improve sitting control in diplegic children.
References
1- BAX M., GOLDSTEIN M., ROSENBAUM P., GOLD-STEIN M., ROSENBAUM P., LEVITON A., PANETH N., DAN B., JACOBSSON B. and DAMIANO D.: Exec-utive Committee for the Definition of Cerebral Palsy:
Proposed definition and classification of cerebral palsy.
Dev. Med. Child Neurol., Aug., 47 (8): 571-6, 2005.
2- JONES M.W., MORGAN E., SHELTON J.E. and THOROGOOD C.: Cerebral palsy: Introduction and diagnosis (Part I). J. Pediatr. Health Care, May-Jun., 21
(3): 146-52, 2007.
3- ROSENBAUM P.L., PALISANO R.J., BARTLETT D.J., GALUPPI B.E. and RUSSELL D.J.: Development of the Gross Motor Function Classification System for cerebral
palsy. Dev. Med. Child Neurol., 50: 249-53, 2008.
4- VAN DER HEIDE J.C., OTTEN B., VAN EYKERN L.A. and HADDERS-ALGRA M.: Development of postural
adjustments during reaching in sitting children. Exp. Brain
Res., Jul., 151 (1): 32-45, 2003.
5- FOOTER C.B.: The Effects of Therapeutic Taping on
Gross Motor Function in Children with Cerebral Palsy.
Pediatr. Phys. Ther., 18: 245-52, 2006.
6- TERJESEN T., LANGE J.E. and STEEN H.: Treatment
of scoliosis with spinal bracing in quadriplegic cerebral palsy. Dev. Med. Child Neurol., 42: 448-54, 2000.
7- KNOX V.: The use of lycra garments in children with
cerebral palsy: A report of a descriptive clinical trial. Br.
J. Occupa. Ther., 68: 71-7, 2003.
8- ATTARD J. and RITHALIA S.: A review of the use of
Lycra pressure orthoses for children with cerebral palsy.
Int. J. Ther. Rehabil., 11: 120-5, 2004.
9- CHEN P.L., HONG W.H., LIN C.H. and CHEN W.C.: Biomechanics effects of kinesio taping for persons with
patellofemoral pain syndrome during stair climbing. In
4th Kuala Lumpur International Conference on Biomedical
Engineering, pp. 395-7, Springer Berlin Heidelberg, 2008.
10- GRISHAM S.R. and DEMING L.M.: Pediatric life care
planning and case management, Vol. 180, 2nd ed. Taylor & Francis Group, p. 520-1, 2011.
11-BOHANNON R.W. and SMITH M.B.: Inter-rater reliability
of a modified Ashworth scale of muscle spasticity. Phys.
Ther., 67: 206-7, 1987.
12- KO J. and KIM M.: Reliability and responsiveness of the
gross motor function measure-88 in children with cerebral palsy. Phys. Ther., 93 (3): 393-400, 2013.
13- GSTOETTNER M., SEKYRA K., WALOCHNIK N., WINTER P., WACHTER R. and BACH C.M.: Inter-and
intra-observer reliability assessment of the Cobb angle:
Manual versus digital measurement tools. Eur. Spine J.,
Oct., 16 (10): 1587-92, 2007.
14- LEVITTE S.: Treatment of cerebral palsy and motor delay.
5 th ed, Wiley-Blackwell, London, 2010.
15- DAMIANO D.L.: Rehabilitative Therapies in Cerebral
Palsy: The Good, the Not As Good, and the Possible. J. Child Neurol. Sep., 24 (9): 1200-4, 2009.
16- SHUMWAY-COOK A. and WOOLLACOTT M.H.: Motor Control: Theory and Practical Applications. 2 nd edition, Lippincott Williams and Wilkins, 2000.
17- KERN H., HORAK F. and NASHNER L.: Cerebral palsy. In: Campbell S.K., editor. Decision making in pediatric neurologic physical therapy. Phil: Churchill Livingstone,
pp. 317-22, 2000.
18- STERBA J., ROGERS B., FRANCE A. and VOKES D.:
Horseback riding in children with cerebral palsy: Effect
on gross motor function. Dev. Med. Child Neurol., 44 (5): 301-8, 2002.
19- HSU Y.H., CHEN W.Y., LIN H.C., WANG W.T. and SHIH Y.F.: The effects of taping on scapular kinematics and
muscle performance in baseball players with shoulder
impingement syndrome. J. Electromyogr. Kinesiol. Dec., 19 (6): 1092-9, 2009.
20- MILLER C.M., GREENWOOD S., MICHAEL GLEESON M., NARDONE F. and FAIGLE K.: Kiensio taping and
hypotonia. The International Organisation of Physical
Therapists in Paediatrics, Vol. 5, pp. 10, 2010.

44 The Effect of Kinesio Taping on Seated Postural Control
21- YASUKAWA A., PATEL P. and SISUNG C.: Pilot study:
Investigating the effects of Kinesio Taping in an acute
pediatric rehabilitation setting. Am. J. Occup. Ther. Jan.- Feb., 60 (1): 104-10, 2006.
22- VITHOULK I., BENEKA A., MALLIOU P., AGGELOU-SIS N., KARATSOLIS K. and DIAMANTOPOULOS K.:
The effects of Kinesio-Tapings on quadriceps strength during isokinetic exercise in healthy non athlete women;
Isokineti. Exerc. Sci., 18 (1): 1-6, 2010.
23- KASE K., WALLIS J., KASE T. and KINESIO TAPING
ASSOCIATION.: Clinical Therapeutic Applications of
the Kinesio Taping Methods. Tokyo, cccxxx m Japan:
Ken Ikai Co Ltd., 2003.
24- LEMOS T.V., PEREIRA K.C., PROTÁSSIO C.C., LUCAS L.B. and MATHEUS J.P.: The effect of Kinesio Taping
on handgrip strength. J. Phys. Ther. Sci., Mar., 27 (3):
567-70, 2015.
25- MOHAMMADI H.K, KALANTARI K.K., NAEIMI S.S., POURETEZAD M., SHOKRI E., TAFAZOLI M., DASTJERDI M. and KARDOONI L.: Immediate and Delayed Effects of Forearm Kinesio Taping on Grip
Strength; Iran Red. Crescent. Med. J. August, 16 (8):
e 19797, 2014.
26- HALSETH T., MCCHESNEY J.W., DEBELISO M., VAUGHN R. and LIEN J.: The Effects of KinesioTM
Taping on Proprioception at the Ankle; J. Sports Sci. Med., 3 (1): 1-7, 2004.
27- S´LUPIK A., DWORNIK M., BIA´LOSZEWSKI D. and ZYCH E.: Effects of kinesio tape on bioelectrical activity
of the vastus medialis muscle. Preliminary report. Ortop.
Traumatol. Rehabil., 9 (6): 644-51, 2007.
28- S IMS EK T.T., TÜRKÜCÜOG˘
LU B., ÇOKAL N., ÜSTÜNBAS G. and S IMS EK
.
I.E.: The effects of Kinesio® taping on sitting posture, functional indepen-dence and gross motor function in children with cerebral
palsy. Disabil. Rehabil., 33 (21-22): 2058-63, 2011.
29- KAYA KARA O., ATASAVUN UYSAL S., TURKER D., KARAYAZGAN S., GUNEL M.K. and BALTACI G.: The effects of Kinesio Taping on body functions and activity in unilateral spastic cerebral palsy: A single-blind
randomized controlled trial. Dev. Med. Child Neurol. Jan., 57 (1): 81-8, 2015.