Embed Size (px)
Citation preview

Original research article
The effect of low-dose combined oral contraceptive pills versusinjectable contraceptive (Depot Provera) on liver function tests of
women with compensated bilharzial liver fibrosis
A.H.E.I. Tagy, M.E. Saker, A.A. Moussa*, A. KolgahDepartment of Obstetrics and Gynecology, Al-Azhar School of Medicine, 28 Kabal St., Nasr City, 11371 Cairo, Egypt
Abstract
This was an open comparative trial of two types of hormonal contraceptives, a low-dose combined oral contraceptive and the injectabledepot-medroxyprogerone acetate, with a control group using an intrauterine device (copper T-380). Clients were recruited from bilharzialpatients attending the maternal-child health and family centers affiliated with the National Liver Institute. Clients with compensatedbilharzial liver disease were chosen and were divided into three subgroups according to their own preference for the method ofcontraception. Baseline, 2-, and 4-months liver function tests were compared, and abdominal ultrasound scanning of the liver was done.There was a nonsignificant change in liver function tests, and the portal vein diameter measured by ultrasound scanning was not changedwith steroidal contraceptives. The use of combined oral contraceptive containing low-dose estrogen or using depot medroxyprogertone acetateinjectables are safe and can be prescribed in cases with compensated bilharzial hepatic fibrosis with normal function. © 2001 Elsevier Science Inc.All rights reserved.
Keywords: Injectable contraceptive; Oral contraceptive pills; Liver function tests; Bilharizal liver fibrosis; IUD
1. Introduction
Bilharziasis is a major, global public health problem. It isan endemic disease in rural Egypt and, along with viralhepatitis, is the main cause of liver diseases in the popula-tion as a whole, including women of reproductive age.
The liver is the main site of the metabolism of steroidhormones including sex hormones. Disturbance of liverfunction has been considered as a possible contraindica-tion for the use of hormonal contraception. Some studiesargue that previous infection of the liver by viruses orparasites in patients with normal liver function should notbe considered as a contraindication for hormonal contra-ceptive use. The impact of this argument is especiallyimportant in a country such as Egypt, which has 6 millionindividuals suffering from bilharziasis and where around10% of contraceptive users prefer oral contraceptives(OCs) [1].
Shaaban et al. at Assuit Medical School [2] showed thata standard dose combined OC pill (Ovral) did not affect he-
patic function in bilharzial patients who had normal liver func-tions and with no clinical evidence of hepatic involvement.
In 1995, a group from Utah University [3] reported thatNorplant and Depot Provera did not change the lipid profileor some liver functions after 1 year of use. In 1998, the TaskForce on Long-acting Systemic Agents for Fertility Regu-lation [4] reported a minor change in liver function andglucose metabolism in a comparative study of the effects oftwo once-a-month injectable steroidal contraceptives(Mesigyna and Cyclofem).
The aim of the present study was to evaluate the effectof combined low-dose OCs versus an injectable contra-ceptive (medroxyprogesterone acetate) on liver functionswhen prescribed to women with compensated bilharzial liverfibrosis.
2. Methods
This was an open comparative trial. It included 156 caseswith bilharzial liver disease with or without spleenomegalyand with normal liver function tests.
* Corresponding author. Tel.: �20-2-270-0517; fax: �20-2-273-8343.E-mail address: [email protected] (A.A. Moussa).
Contraception 64 (2001) 173–176
0010-7824/01/$ – see front matter © 2001 Elsevier Science Inc. All rights reserved.PII: S0010-7824(01)00248-7
2.1. Duration of the study
The study was carried out from July 1, 1997 to June23,1998.
2.2. Site and location
Cases were recruited from maternal-child health andfamily planning centers affiliated with the National LiverInstitute, Shebeen El-Kom, El-Menoufia governorate (1 hby car northwest of Cairo).
2.3. Inclusion criteria
1. Married, fertile women, aged between 20 and 35years, and with history of bilharzial infestation orwith anti-bilharzial treatment.
2. Liver disease was pure bilharzial periportal fibrosiswith a normal appearance of liver parenchyma onultrasound scanning of the liver. (See section 2.5.)
3. Normal liver function tests before the start of the trial.(See section 2.6.)
4. No history of hormonal medication for at least 6months before the start of the trial.
5. Free from other endemic diseases (such as malaria,sickle cell anemia) that could affect the liver.
2.4. Exclusion criteria
1. A past history of hepatitis B or C.2. Manifestations of malnutrition (weight-to-height less
than 20% of the standard).3. Advanced cases of bilharzial liver disease as mani-
fested on ultrasound scanning of the liver or withelevated liver enzymes.
4. The presence of other endemic diseases, anemia (he-moglobin less than 11 g), or blood clotting disorders.
5. Hormonal medication during the 6 months prior to thestudy.
6. Absolute contraindications for intrauterine device(IUD) insertion or hormonal contraceptive, such asacute or chronic cholestatic liver disease [5].
2.5. Ultrasound criteria for inclusion
1. The liver was free of focal lesion.2. The liver was free of any coarseness or bright texture.3. Main finding of periportal fibrosis.4. Portal vein diameters not to exceed 12 mm.5. Only early cases of bilharzial liver affection with a
periportal thickening less than 7 mm.
2.6. The normal values of liver enzymes
Y SGOT 15–35 IU/IY SGPT 30–65 IU/IY Alkaline phosphatase (AP) 50–136 Armstrong unitsY Total bilirubin 0.2–1.2 mg/dL
It was decided to include cases with normally accepted1.5-fold increase above normal values.
3. Results
In this nonrandomized, controlled clinical trial, 228 caseswere originally interviewed. Seventy-two cases were ex-cluded from the screened cases because they did not fulfillthe criteria for selection; this left us with 156 participants.These were divided into three subgroups according to thecontraceptive method used: pill users, 38 cases; the inject-able users, 53 cases; and the IUD users, considered as thecontrol group, 65 cases.
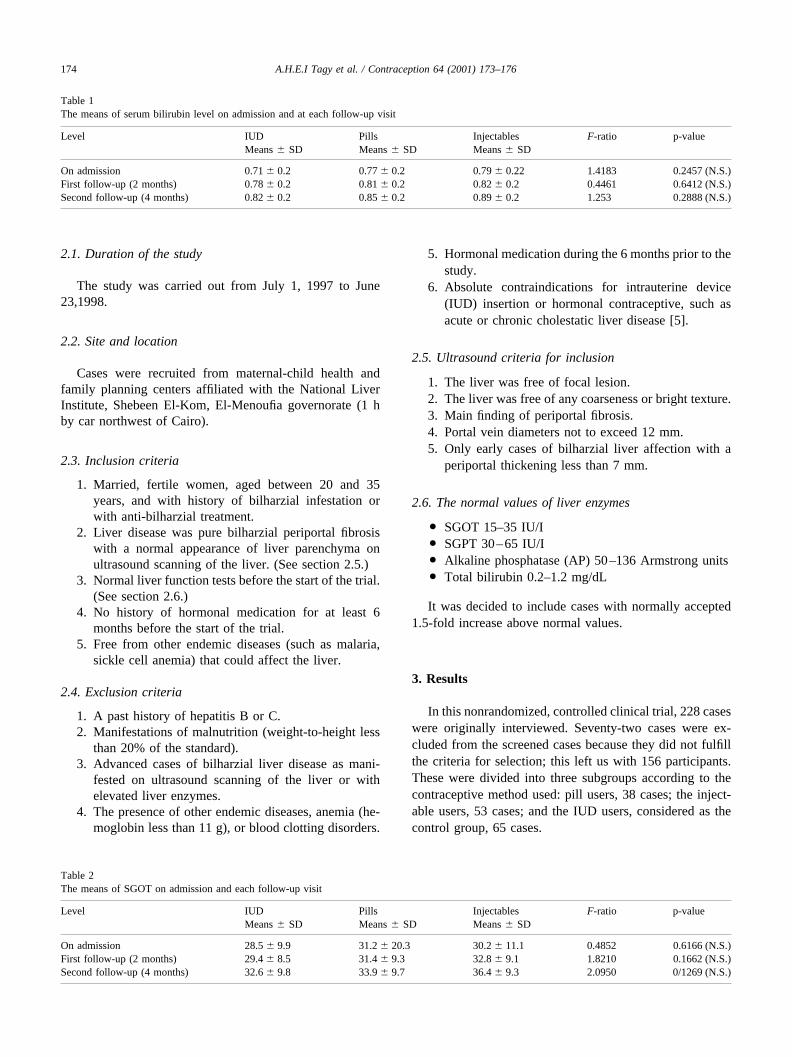
Table 1The means of serum bilirubin level on admission and at each follow-up visit
Level IUDMeans � SD
PillsMeans � SD
InjectablesMeans � SD
F-ratio p-value
On admission 0.71 � 0.2 0.77 � 0.2 0.79 � 0.22 1.4183 0.2457 (N.S.)First follow-up (2 months) 0.78 � 0.2 0.81 � 0.2 0.82 � 0.2 0.4461 0.6412 (N.S.)Second follow-up (4 months) 0.82 � 0.2 0.85 � 0.2 0.89 � 0.2 1.253 0.2888 (N.S.)
Table 2The means of SGOT on admission and each follow-up visit
Level IUDMeans � SD
PillsMeans � SD
InjectablesMeans � SD
F-ratio p-value
On admission 28.5 � 9.9 31.2 � 20.3 30.2 � 11.1 0.4852 0.6166 (N.S.)First follow-up (2 months) 29.4 � 8.5 31.4 � 9.3 32.8 � 9.1 1.8210 0.1662 (N.S.)Second follow-up (4 months) 32.6 � 9.8 33.9 � 9.7 36.4 � 9.3 2.0950 0/1269 (N.S.)
174 A.H.E.I Tagy et al. / Contraception 64 (2001) 173–176

3.1. Liver enzymes
Tables 1, 2, 3, and 4 present the serum levels of bilirubinand liver enzymes in the pill and injectable groups com-pared to the control group.
3.2. Serum bilirubin level
The average serum bilirubin level at admission was 0.71for the IUD group, 0.77 for the pill group, and 0.79 for theinjectable group.
Table 1 presents the mean � SD of serum bilirubin levelon admission and at 2- and 4-months follow-up visits. TheF-test indicated that there was no significant differencebetween the bilirubin levels of the control group and othergroups at baseline, the first follow-up, or the second fol-low-up visit.
3.3. Serum glutamic-oxaloacetic trasaminase level
The average serum level of glutamic-oxaloacetic trasami-nase (SGOT) at admission was 28.5 for the IUD group, 31.2for the pill group, and 30.2 for the injectable group.
Table 2 compares the mean SGOT on admission and at2 and 4 months from the start of the trial. There were nosignificant differences between the SGOT levels of thecontrol group and other groups at either baseline or thefollow-up visits.
3.4. Serum glutamic-pyruvic trasaminase level
The average serum level of glutamic-pyruvic trasami-nase (SGPT) on admission was 31.9 for the IUD group, 37.3for the pill group, and 33.8 for the injectable group.
Table 3 compares the mean SGPT at admission and at 2and 4 months from the start of the trial. There were nosignificant differences between the SGPT levels of the con-
trol group and other groups at either baseline, the firstfollow-up, or the second follow-up visits.
3.5. Serum AP level
The average serum AP level at admission was 86.9 forthe IUD group, 72.8 for the pill group, and 78.6 for theinjectable group. Table 4 compares the mean AP on admis-sion and at 2 and 4 months from the start of the trial. Therewere no significant differences between the AP levels of thecontrol group and the other groups, except at baseline whichwas in the normal range.
The above mentioned results indicate that there was nosignificant change in all liver enzymes measured at eitherthe first or the second follow-up visits when compared to thecontrol group.
A nonsignificant difference in the portal vein diameterwas found among the three groups (Table 5).
4. Discussion
Although some information is available about the risk ofliver tumors associated with combined OC use, little isknown about the relationship with other hepatic problems[6]. The studies done by Shaaban et al. [2] as well as Sy etal. [7] documented no statistical changes in liver functiontests with an OC containing 50 ug and 35 ug estradiol,respectively. These results are similar to the present studyand also correlate with the Royal College of General Prac-titioners’ study [6]. The current study also showed nochange in the portal vein diameter measured by ultrasound.On admission to the study and with subsequent follow-upvisits, no change was observed in the three groups and, tothe best of our knowledge, no other studies used this parameterin evaluating the effect of hormonal steroids on the liver.
In 1998, the Task Force on Long-acting Systemic Agentsfor Fertility Regulation [4] showed that liver function and
Table 3The means of SGPT on admission and at each follow-up visit
Level IUDMeans � SD
PillsMeans � SD
InjectablesMeans � SD
F-ratio p-value
On admission 31.9 � 10.0 37.3 � 24.2 33.8 � 16.9 1.0973 0.3367 (N.S.)First follow-up (2 months) 35.2 � 8.9 35.6 � 9.9 38.8 � 11.7 1.7110 0.1850 (N.S.)Second follow-up (4 months) 39.3 � 16.0 41.5 � 14.4 41.8 � 12.9 0.4988 0.6083 (N.S.)
Table 4Mean alkaline phosphatase on admission and at each follow-up visit
Level IUDMeans � SD
PillsMeans � SD
InjectablesMeans � SD
F-ratio p-value
On admission 86.9 � 19.2 72.8 � 13.5 78.6 � 25.1 5.3351 0.0059First follow-up (2 months) 84.1 � 18.3 79.8 � 9.4 83.3 � 13.6 0.7681 0.4661 (N.S.)Second follow-up (4 months) 84.3 � 14.6 81.4 � 21.3 84.0 � 13.4 0.5597 0.9623 (N.S.)
175A.H.E.I Tagy et al. / Contraception 64 (2001) 173–176

glucose metabolism were not significantly changed with theuse of two once-a-month injectable steroidal contraceptives(Mesigna and Cyclofem).
The present 6 month follow-up study that examined a com-bined OC, containing low-dose estrogen and depot medroxypro-geterone acetate injectables, found both to be safe and that theycan be prescribed to cases with compensated bilharzial hepaticfibrosis with normal liver function. Ultrasound scanning, as anoninvasive tool that is available in most health facilities, provedto be helpful and could be used in monitoring clients on steroidalcontraceptives along with other laboratory investigations.
References
[1] Egypt Demographic and Health Survey, El Tawila S. Perspective onfertility, and family planning in Egypt: results of further analysis ofthe 1992 Egypt Demographic Health Survey. National PopulationCouncil, 1995.
[2] Shaaban MM, Ghaneimah SA, Mohamed MA, Abdel-Ghani S,Mostafa S. Effect of oral contraceptives on serum bile acids. InternatJ Obstetr Gynecol 1984;22:111–5.
[3] Mainwaring R, Hales HA, Stevenson K, et al. Metabolic parameter,bleeding, and weight changes in U.S. women using progestin onlycontraceptives. Contraception 1995;51:149–53.
[4] Task Force on Long Acting Systemic Agents for Fertility Regulation.Comparative study of the effects of two once-a-month injectablesteroidal contraceptives (Mesigna, and Cyclofem) on glucose metab-olism and liver function. Contraception 1998;57:71–81.
[5] Speroff L, Glass R, Kase N. In: Clinical Gynecologic Endrocinology,and Infertility. 5th ed. Baltimore, Maryland: Williams and Wilkins,1994. p. 475–83.
[6] Hannaford PC, Kay CR, Vessey MP, Painter R, Mant J. Combinedoral contraceptives and liver disease. Contraception 1997;55:145–51.
[7] Sy FS, Osteria TS, OpinianoV, Gler S. Effects of oral contraceptiveson liver function tests of women with schistosomiasis in the Philip-pines. Contraception 1986;34:283–94.
Table 5Portal vein diameter in the studied groups
IUDMeans � SD
PillMeans � SD
InjectableMeans � SD
On admission 11.0 � 1.3 11.1 � 1.5 11.3 � 1.2First follow-up
(2 months)11.0 � 1.3 11.1 � 1.5 11.3 � 1.2
Second follow-up(4 months)
11.1 � 1.25 11.2 � 1.6 11.4 � 1.1
176 A.H.E.I Tagy et al. / Contraception 64 (2001) 173–176