Embed Size (px)
Citation preview
ARTICLE IN PRESS
0003-6870/$ - se
doi:10.1016/j.ap
�CorrespondE-mail addr
bente.moen@is
Applied Ergonomics 37 (2006) 775–783
www.elsevier.com/locate/apergo
The effects of occupational health and safety management on workenvironment and health: A prospective study
S. Torpa,�, B.E. Moenb
aFaculty of Health Science, Centre for Health Promotion in Settings, Vestfold University College, P.O. Box 2243, N-3103 Tønsberg, NorwaybDepartment of Public Health and Primary Health Care, Section for Occupational Medicine, University of Bergen, Kalfarvn. 31, 5018 Bergen, Norway
Received 13 January 2005; accepted 1 November 2005
Abstract
According to Norway’s Internal Control Regulation, all companies are required to have an occupational health and safety (H&S)
management system. This study investigated the effects of implementing or improving occupational H&S management on the work
environment, H&S-related behaviour and musculoskeletal health of workers in small and medium-sized companies. A one-year
prospective cohort study, using self-administered questionnaires, was performed among the managers and blue-collar workers in 226
motor vehicle repair garages. Out of 1559 workers that responded at baseline 721 workers could be identified at follow-up. These 721
workers were included in the study. The workers in companies with improved H&S management from baseline to follow-up reported
increased satisfaction with the H&S activities at the garage; improved support from management and colleagues; improved health-related
support and control; and increased participation in H&S activities.
r 2005 Elsevier Ltd. All rights reserved.
Keywords: Health and safety management; Work environment; Musculoskeletal; Prospective
1. Introduction
Total quality management (Pfau, 1989; Kim, 1994) hasbeen one of the leading management strategies forenhancing the productivity of companies in industrializedcountries in recent decades. The principles of this manage-ment philosophy have been used in managing health andsafety (H&S) in the offshore oil industry in Norway formany years. Based on the positive results of this work, theInternal Control Regulation (Ministry of Labour andGovernment Administration, 1997; Ministry of LocalGovernment, 1991) on occupational H&S managementcame into force in Norway in 1992. As total qualitymanagement focuses on products and services fulfillingcertain specifications and customer expectations, internalcontrol embraces the domain of health, environment andsafety.
e front matter r 2005 Elsevier Ltd. All rights reserved.
ergo.2005.11.005
ing author. Tel.: +4733031277; fax: +4733031290.
esses: [email protected] (S. Torp),
f.uib.no (B.E. Moen).
According to the Internal Control Regulation, all privateand public companies in Norway, regardless of trade andthe number of employees, are required to act systematicallyto ensure health, environment and safety activities. TheInternal Control Regulation (Ministry of Labour andGovernment Administration, 1997) defines internal controlas systematic action (at management level) to ensure anddocument that the activities of health, environment andsafety control are performed in accordance with require-ments specified in acts or regulations (such as the WorkEnvironment Act (Friberg, 1990)). The systematic actionmust be described as administrative procedures. Further,the Regulation’s requirements can be grouped into thethree following main categories (Gaupseth, 2000):
�
Clarifying the aims, responsibilities and tasks for theH&S activities; � Identifying and assessing the risks and problems anddrawing up agendas with measures; and
� Systematically monitor that the company’s activitiesare in accordance with the aims determined by thecompany.

ARTICLE IN PRESSS. Torp, B.E. Moen / Applied Ergonomics 37 (2006) 775–783776
This includes both content claims, such as technical andadministrative standards that can be documented inhandbooks, and process claims such as assessments,meetings and H&S training. The employer is responsiblefor the company’s H&S activities, and each company mustadjust its H&S management system to its needs and specialrisk factors. In line with the Scandinavian tradition ofdemocratization of work and empowerment (Gustavsenand Hunnius, 1981; Elden, 1986), the Regulation alsoemphasizes that both employers and workers shouldparticipate in constructing the H&S routines and partici-pate in the H&S activities.
Most countries have legislation protecting workers fromhazards at work. Norway and Sweden also have regula-tions requiring all employers to implement a specifiedoccupational H&S management system. In its earliestform, the systematic regulation of occupational H&Smanagement in Norway’s offshore oil industry influencedEuropean Union directive 89/391/EEC on the introductionof measures to encourage improvements in the safety andhealth of workers at work (Frick et al., 2000; Walters andJensen, 2000).
Several studies have evaluated the internal controlreform (Gaupseth, 2000; Hovden, 1998; Saksvik andNytro, 1996; Nytro et al., 1998; Kjellen et al., 1997; Torpet al., 2000; Saksvik et al., 2003). These studies show thatlarge companies, companies highly competent in H&Sactivities and companies with external agents requestingH&S results from the company (such as customers,insurance companies and regional labour inspectorates)have been most successful in implementing internalcontrol. Internal control has proved to be successful inreducing occupational accidents and continuous pollution(Hovden, 1998), and companies report that the newregulations have increased awareness of H&S, made clearthe lines of responsibility and improved the risk assessmentand documentation of H&S activities (Saksvik and Nytro,1996). These evaluations have mainly assessed factorsaffecting the implementation of internal control and theeffects of internal control measured at an organizationallevel. One cross-sectional study (Torp et al., 2000) showedthat the implementation status of internal control corre-lated positively with how workers regard their workenvironment and health and how they participate in H&Sactivities. Researchers have sought prospective studiesshowing more detailed effects of implementing or improv-ing occupational H&S management according to theInternal Control Regulation (Gaupseth, 2000; Saksviket al., 2003).
The Norwegian Labour Directorate has put considerableeffort into motivating and helping small and medium-sized companies to implement internal control, but theyhave still had difficulty in fulfilling the requirementsof the Regulation. A debated issue has therefore beenwhether internal control should apply only to largecompanies (Gaupseth, 2000; Johansson and Johansson,1993).
The aim of this prospective study was to investigate theeffects of implementing or improving occupational H&Smanagement in small and medium-sized companies asdescribed by the Internal Control Regulation. The effectswere measured by workers’ own evaluation of their workenvironment, their participation in H&S activities at thework site and their musculoskeletal health.
2. Material and methods
2.1. Population study and data collection
A 1-year prospective study was performed among all themanagers and garage workers (excluding warehouse andoffice workers) at 226 motor vehicle repair garages inNorway. A total of 292 motor vehicle repair garages wereasked to participate in the study. All the garages weremembers of the Norwegian Association of MotorcarDealers and Service Organization. At baseline, themanagers of the 292 garages were asked to fill out aquestionnaire about the size of the company and to whatdegree the garage’s H&S management system fulfilled theInternal Control Regulation. A total of 250 managers(86%) answered the questionnaire, and 237 consented todistribute a questionnaire to the workers of their company.An identical questionnaire was sent to these 237 managers1 year later. A total of 11 companies were excluded in thisfollow-up survey because the company no longer had anyemployees or no longer was a member of the MotorcarDealers and Service Association or because the managerdid not return the questionnaire. At baseline, the 226participating companies had a mean of 19 employees(median ¼ 13, range ¼ 2–140), of which 10 were garageworkers (median ¼ 6, range ¼ 2–70). Forty-three percentof the garages had less than 10 employees, 40% had 10–30employees and 16% had more than 30 employees. Thesefigures were very similar 1 year later.The motor vehicle repair workers answered a self-
administered questionnaire on work environment, H&S-related behaviour and musculoskeletal health. The ques-tionnaire was sent to the garages’ safety delegate or asupervisor who distributed the questionnaires to all thegarage workers. A total of 2070 questionnaires weredistributed at the start of the study, and 1964 question-naires were distributed at the follow-up 1 year later. Theparticipation rate was 75% (n ¼ 1559) at baseline and 70%(n ¼ 1370) at follow-up. The questionnaires were answeredanonymously, but the questionnaires collected at baselinewere matched to the questionnaires at follow-up by use of apersonal code. A total of 721 workers could be identified bythe code in both surveys. The average age of the 721workers at baseline was 34 years (SD ¼ 10, range 18–64),the mean period of employment in the current occupationwas 13 years (SD ¼ 10, range 0–46) and 98% were men. Atotal of 83% worked as mechanics, panel beaters orsprayers, 17% were supervisors or foremen and 10% hadother work tasks such as vulcanization or auto electricity

ARTICLE IN PRESSS. Torp, B.E. Moen / Applied Ergonomics 37 (2006) 775–783 777
work. Some respondents reported more than one occupa-tion. The workers included in this study (those whoresponded to the questionnaire both at baseline and atfollow-up) and those who responded to the first question-naire only did not differ significantly in demographiccharacteristics or responses to the individual variables atbaseline. Other publications describe the study populationand data collection in more detail (Torp et al., 2000, 2001a).
2.2. Measures
The status of internal control was measured by anoverall question on how the manager subjectively rated thestatus of the implementation of internal control at thegarage. This question had a 5-point scale with the follow-ing response alternatives: ‘‘do not know what internalcontrol is’’ ( ¼ 1), ‘‘not started’’ ( ¼ 2), ‘‘under way’’( ¼ 3), ‘‘almost finished’’ ( ¼ 4) and ‘‘implemented internalcontrol’’ ( ¼ 5). The managers also reported how manyworkers who were employed in the garage.
Table 1 presents all the outcome variables and thenumber of items and the internal reliability (Cronbach’s a)of the indices, which are described elsewhere in furtherdetail (Torp et al., 2001b). The outcome variables werebased on each worker’s responses to the questionnaire. Theresponses on the work environment and coping withmusculoskeletal symptoms measures were all graded onscales ranging from 1 to 7. The questions regard-ing satisfaction with H&S activities and the physical andpsychosocial work environment included responses rangingfrom ‘‘poor’’ ( ¼ 1) to ‘‘very good’’ ( ¼ 7). All itemsincluded in the work environment indices were phrasedas statements and ranged from ‘‘do not agree’’ ( ¼ 1) to‘‘agree’’ ( ¼ 7). The coping index ranged from ‘‘never’’( ¼ 1) to ‘‘often’’ ( ¼ 7). The scores of the indices werecalculated by summing the scores of the single items. Ahigher total score indicates a higher level of psychologicaldemands, decision authority, social support, H&S-related
Table 1
The indices’ number of items and internal reliability (Cronbach’s a values), an
No. of items
Satisfaction with H&S activities at garage 1
Physical work environment 1
Psychosocial work environment 1
Psychological job demands 2
Decision authority 2
Social support 6
H&S-related management support 9
Health-related support and control 3
Workers’ participation in H&S activities 2
Coping with musculoskeletal symptoms at work 10
Musculoskeletal symptoms in the past 30 days 7
Sick leave in the past 30 days (no/yes) 1
aThe changes were calculated by subtracting the variables’ score at baseline
management support, health-related support and control,workers’ participation in H&S activities and coping withmusculoskeletal symptoms.Satisfaction with H&S activities was measured by the
question ‘‘How do you regard the H&S activities at thegarage?’’Satisfaction with the physical working environment was
measured by the question ‘‘How good do you think thephysical work environment (such as noise, lighting,ergonomics and chemical products) is at the garage?’’Satisfaction with the psychosocial work environment
was measured by the question ‘‘How good do you think thepsychosocial work environment (such as cooperation,stress and job satisfaction) is at the garage?’’Psychological job demands were measured by two
questions regarding the time allowed to perform tasksand excessive work.Decision authority was measured by two items measur-
ing the workers’ opportunities to decide what work shouldbe done and how.Social support was measured by six items on team spirit
and support from colleagues and supervisor. The questionsmeasuring social support, psychological job demands anddecision authority were taken from the Job Demands—Control—Support Questionnaire (Theorell et al., 1993;Toomingas et al., 1997; Karasek et al., 1998) and modifiedfor this study.The index for H&S-related management support con-
tained nine items on how the workers regarded thecommitment to and participation of management in H&Sactivities. Examples are ‘‘The management keeps itspromises regarding H&S improvements’’ and ‘‘The man-ager takes the workers’ opinions on H&S seriously’’.Health-related support and control was measured
with an index containing three items measuring theopportunities to take breaks and to get help fromthe supervisor and colleagues when experiencing healthproblems.
d the variables’ mean change in scores from baseline to follow-upa
Internal
reliability
Mean (SD)
(worker level)
Mean (SD)
(garage level)
NA 0.04 (1.26) 0.04 (0.26)
NA 0.19 (1.47) 0.22 (1.20)
NA �0.10 (1.53) �0.13 (1.13)
0.32 �0.31 (2.65) �0.26 (1.92)
0.77 0.14 (3.00) �0.05 (1.97)
0.72 �0.81 (5.75) �0.83 (4.48)
0.74 �0.44 (9.60) �0.52 (8.66)
0.81 �0.10 (4.11) �0.13 (2.90)
0.65 �0.06 (2.51) �0.01 (1.68)
0.78 1.90 (9.87) 1.56 (8.20)
0.69 0.36 (2.83) 0.27 (1.91)
NA 0.03 (0.54) 0.20 (0.34)
from the score at follow-up one year later.

ARTICLE IN PRESSS. Torp, B.E. Moen / Applied Ergonomics 37 (2006) 775–783778
Workers’ participation in H&S activities was measuredby two statements on how well the workers complied withthe H&S routines adopted and to what degree they usedprotective equipment.
Coping with musculoskeletal symptoms was measuredby an index of 10 items. We asked the workers what theydid when they experienced bodily pain or stiffness thattroubled them at work for days or weeks. The workers whoreported that they had bodily pain or stiffness at work wereasked whether they used any of 10 different copingstrategies, including ‘‘Change working technique’’, ‘‘Useequipment to reduce physical strain’’ and ‘‘Ask colleaguesfor help with strenuous tasks’’.
Musculoskeletal pain was chosen as the measure forworkers’ subjective health because such symptoms arecommon among this group of workers (Torp et al., 2001a,1996) and because they often are related to both physicaland psychosocial work environment. Musculoskeletal painwere measured by six of the questions in the SubjectiveHealth Complaints Questionnaire (Eriksen et al., 1999).The respondents were asked whether they had experiencedpain within the past 30 days from the head, neck, upperback, lower back, shoulders and arms. In addition, aquestion regarding pain in the knees was added. Theseverity of musculoskeletal pain was rated on a four-pointscale (0 ¼ ‘‘none’’, 1 ¼ ‘‘some’’, 2 ¼ ‘‘much’’ and 3 ¼ ‘‘se-vere’’). The scores of the seven body parts were summed,and a higher total score indicates a higher level of severity.
Sick leave was measured by asking the respondentswhether they had been away from work within the last 30days because of illness or health problems (1 ¼ ‘‘yes’’ or2 ¼ ‘‘no’’).
The participants were also asked about age, gender,profession, and years of employment in their currentprofession.
2.3. Statistics
In occupational epidemiology and stress research ana-lyses on relationships between social and organizationalfactors (i.e., higher-order level) and workers’ health andhealth-related behavior have mostly been performed withdata measured at an individual level. This has been done toavoid making the ‘‘aggregation bias’’ that occurs ifaggregated data are used to make inferences at theindividual level (Robinson, 1950). This tradition hasrecently been criticized since it is equally erroneous tomake group or organizational inferences based on indivi-dual level data. In addition, since outcomes amongindividuals nested within groups may be influenced byorganizational factors the assumption of independence forindividual level analyzes is violated (Diez-Roux, 1998;Bliese and Jex, 1999). Therefore, it has been argued thatanalyses based on both individual self-rated data andaggregated data should be performed (Bliese and Jex, 1999;Kristensen, 1995). As this study intended to investigate theeffects of developing a H&S management system (at the
organizational level) on individual’s work environment,behaviour and health the average score for all the variableswere calculated for each garage, and the relationshipsbetween H&S management and the outcome variables wereanalyzed at the garage level, as well as at the individuallevel by using the individuals’ subjective data. In theindividual level analyzes the answers given by the managerson internal control status were used as scores for eachindividual at the corresponding garage.Cronbach’s a values were calculated to test the internal
reliability of each index. Partial parametric correlationanalyses were performed to test correlations betweenchange in internal control status and change in thedependent variables from baseline to follow-up. In theseanalyses it was controlled for the effects of age, gender andyears in the current occupation. For comparison, bothbivariate Pearson’s correlation analysis and Spearman’snon-parametric analysis were performed. Change in theinternal control status and change in the dependentvariables were calculated by subtracting the score atbaseline from the score at follow-up. To investigatewhether implementing or improving internal control haddifferent effects in the smallest and largest companies inthis study the same analyses were performed separately ingarages with less than 10 employees, with 10–29 employeesand with 30 or more employees. The residual effect of thesize of the company was adjusted for by entering thisvariable as independent variable.In the analyses presented in Tables 1 and 2 the n varies
considerably for the different measures. This is becauseparticipants who reported no musculoskeletal symptomswere not supposed to respond to the coping withmusculoskeletal symptoms measure, and because theindices with many items had a lower n because respondentswere not included in the analysis if one item (or more) wasmissing.The level of significance was set at 0.05. The analyses
were performed using the SPSS 11.0 computer package(SPSS, 2001).
3. Results
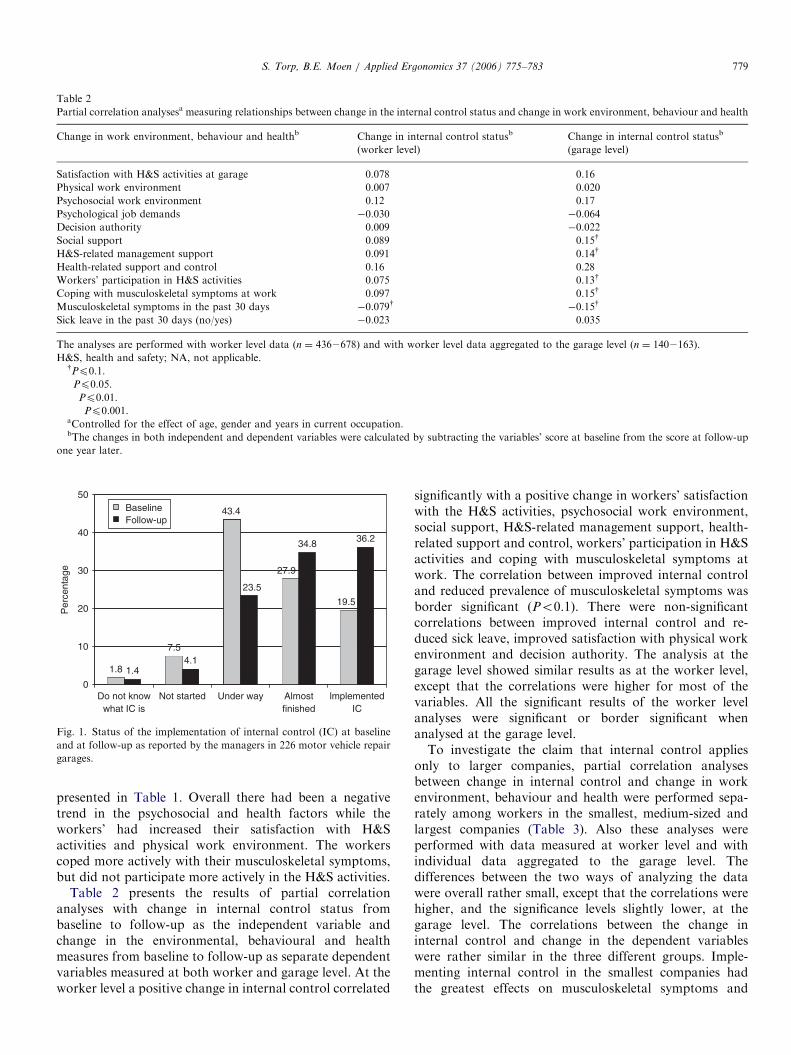
Fig. 1 shows the managers’ subjective ratings of theinternal control status at the garage in both years. About50% of the managers reported that the garage hadimplemented or almost implemented internal control atbaseline versus about 70% 1 year later. The garages withmost employees had to a larger extent implementedinternal control compared with garages with fewer employ-ees (Pearson’s correlation ¼ 0.27, Po0.001) (n ¼ 226garages).At baseline, 82.5% of the workers reported musculoske-
letal symptoms in one or more body parts within the past30 days, and 22.7% had been absent from work within thepast 30 days because of illness or health problems.The dependent variables’ mean change in scores from
baseline to follow-up at both the worker and garage level is
ARTICLE IN PRESS
Table 2
Partial correlation analysesa measuring relationships between change in the internal control status and change in work environment, behaviour and health
Change in work environment, behaviour and healthb Change in internal control statusb
(worker level)
Change in internal control statusb
(garage level)
Satisfaction with H&S activities at garage 0.078� 0.16�
Physical work environment 0.007 0.020
Psychosocial work environment 0.12�� 0.17�
Psychological job demands �0.030 �0.064
Decision authority 0.009 �0.022
Social support 0.089� 0.15y
H&S-related management support 0.091� 0.14y
Health-related support and control 0.16��� 0.28���
Workers’ participation in H&S activities 0.075� 0.13y
Coping with musculoskeletal symptoms at work 0.097� 0.15y
Musculoskeletal symptoms in the past 30 days �0.079y �0.15y
Sick leave in the past 30 days (no/yes) �0.023 0.035
The analyses are performed with worker level data (n ¼ 4362678) and with worker level data aggregated to the garage level (n ¼ 1402163).
H&S, health and safety; NA, not applicable.yPp0.1.�Pp0.05.��Pp0.01.���Pp0.001.aControlled for the effect of age, gender and years in current occupation.bThe changes in both independent and dependent variables were calculated by subtracting the variables’ score at baseline from the score at follow-up
one year later.
1.8
7.5
43.4
27.9
19.5
1.44.1
23.5
34.8 36.2
0
10
20
30
40
50BaselineFollow-up
Per
cent
age
Do not knowwhat IC is
Not started Under way Almostfinished
lmplementedIC
Fig. 1. Status of the implementation of internal control (IC) at baseline
and at follow-up as reported by the managers in 226 motor vehicle repair
garages.
S. Torp, B.E. Moen / Applied Ergonomics 37 (2006) 775–783 779
presented in Table 1. Overall there had been a negativetrend in the psychosocial and health factors while theworkers’ had increased their satisfaction with H&Sactivities and physical work environment. The workerscoped more actively with their musculoskeletal symptoms,but did not participate more actively in the H&S activities.
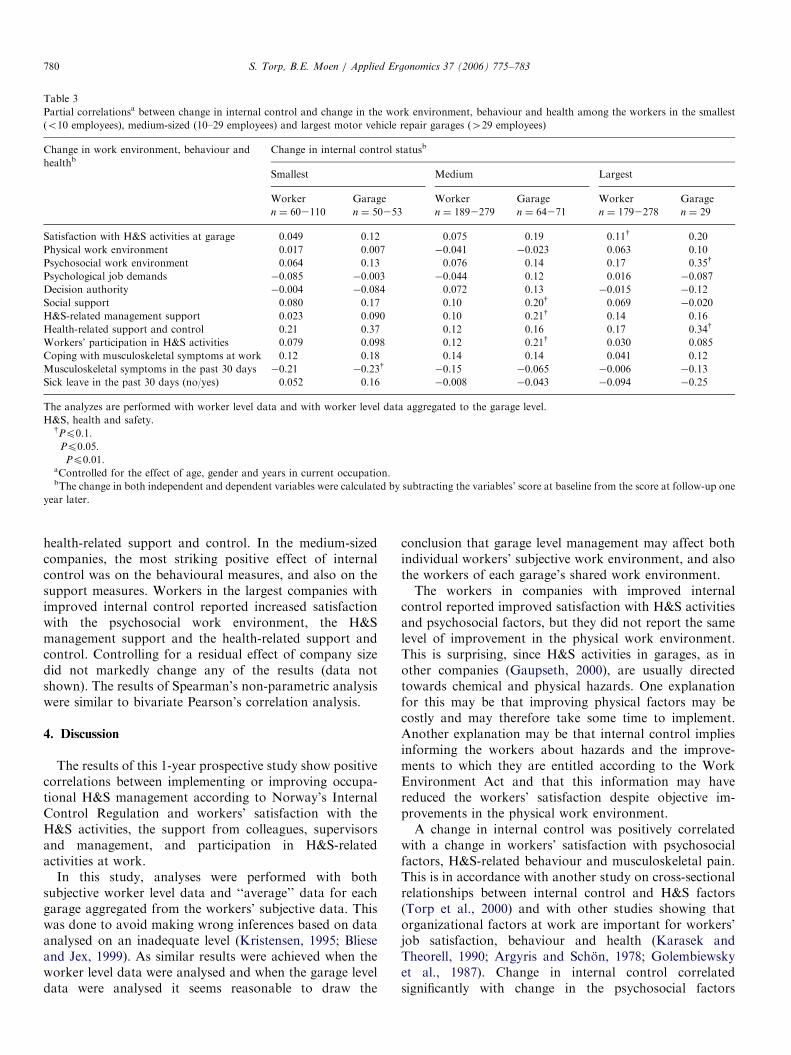
Table 2 presents the results of partial correlationanalyses with change in internal control status frombaseline to follow-up as the independent variable andchange in the environmental, behavioural and healthmeasures from baseline to follow-up as separate dependentvariables measured at both worker and garage level. At theworker level a positive change in internal control correlated
significantly with a positive change in workers’ satisfactionwith the H&S activities, psychosocial work environment,social support, H&S-related management support, health-related support and control, workers’ participation in H&Sactivities and coping with musculoskeletal symptoms atwork. The correlation between improved internal controland reduced prevalence of musculoskeletal symptoms wasborder significant (Po0.1). There were non-significantcorrelations between improved internal control and re-duced sick leave, improved satisfaction with physical workenvironment and decision authority. The analysis at thegarage level showed similar results as at the worker level,except that the correlations were higher for most of thevariables. All the significant results of the worker levelanalyses were significant or border significant whenanalysed at the garage level.To investigate the claim that internal control applies
only to larger companies, partial correlation analysesbetween change in internal control and change in workenvironment, behaviour and health were performed sepa-rately among workers in the smallest, medium-sized andlargest companies (Table 3). Also these analyses wereperformed with data measured at worker level and withindividual data aggregated to the garage level. Thedifferences between the two ways of analyzing the datawere overall rather small, except that the correlations werehigher, and the significance levels slightly lower, at thegarage level. The correlations between the change ininternal control and change in the dependent variableswere rather similar in the three different groups. Imple-menting internal control in the smallest companies hadthe greatest effects on musculoskeletal symptoms and
ARTICLE IN PRESS
Table 3
Partial correlationsa between change in internal control and change in the work environment, behaviour and health among the workers in the smallest
(o10 employees), medium-sized (10–29 employees) and largest motor vehicle repair garages (429 employees)
Change in work environment, behaviour and
healthbChange in internal control statusb
Smallest Medium Largest
Worker
n ¼ 602110
Garage
n ¼ 50253
Worker
n ¼ 1892279
Garage
n ¼ 64271
Worker
n ¼ 1792278
Garage
n ¼ 29
Satisfaction with H&S activities at garage 0.049 0.12 0.075 0.19 0.11y 0.20
Physical work environment 0.017 0.007 �0.041 �0.023 0.063 0.10
Psychosocial work environment 0.064 0.13 0.076 0.14 0.17�� 0.35y
Psychological job demands �0.085 �0.003 �0.044 0.12 0.016 �0.087
Decision authority �0.004 �0.084 0.072 0.13 �0.015 �0.12
Social support 0.080 0.17 0.10 0.20y 0.069 �0.020
H&S-related management support 0.023 0.090 0.10 0.21y 0.14� 0.16
Health-related support and control 0.21� 0.37�� 0.12� 0.16 0.17�� 0.34y
Workers’ participation in H&S activities 0.079 0.098 0.12� 0.21y 0.030 0.085
Coping with musculoskeletal symptoms at work 0.12 0.18 0.14 0.14 0.041 0.12
Musculoskeletal symptoms in the past 30 days �0.21� �0.23y �0.15 �0.065 �0.006 �0.13
Sick leave in the past 30 days (no/yes) 0.052 0.16 �0.008 �0.043 �0.094 �0.25
The analyzes are performed with worker level data and with worker level data aggregated to the garage level.
H&S, health and safety.yPp0.1.�Pp0.05.��Pp0.01.aControlled for the effect of age, gender and years in current occupation.bThe change in both independent and dependent variables were calculated by subtracting the variables’ score at baseline from the score at follow-up one
year later.
S. Torp, B.E. Moen / Applied Ergonomics 37 (2006) 775–783780
health-related support and control. In the medium-sizedcompanies, the most striking positive effect of internalcontrol was on the behavioural measures, and also on thesupport measures. Workers in the largest companies withimproved internal control reported increased satisfactionwith the psychosocial work environment, the H&Smanagement support and the health-related support andcontrol. Controlling for a residual effect of company sizedid not markedly change any of the results (data notshown). The results of Spearman’s non-parametric analysiswere similar to bivariate Pearson’s correlation analysis.
4. Discussion
The results of this 1-year prospective study show positivecorrelations between implementing or improving occupa-tional H&S management according to Norway’s InternalControl Regulation and workers’ satisfaction with theH&S activities, the support from colleagues, supervisorsand management, and participation in H&S-relatedactivities at work.
In this study, analyses were performed with bothsubjective worker level data and ‘‘average’’ data for eachgarage aggregated from the workers’ subjective data. Thiswas done to avoid making wrong inferences based on dataanalysed on an inadequate level (Kristensen, 1995; Blieseand Jex, 1999). As similar results were achieved when theworker level data were analysed and when the garage leveldata were analysed it seems reasonable to draw the
conclusion that garage level management may affect bothindividual workers’ subjective work environment, and alsothe workers of each garage’s shared work environment.The workers in companies with improved internal
control reported improved satisfaction with H&S activitiesand psychosocial factors, but they did not report the samelevel of improvement in the physical work environment.This is surprising, since H&S activities in garages, as inother companies (Gaupseth, 2000), are usually directedtowards chemical and physical hazards. One explanationfor this may be that improving physical factors may becostly and may therefore take some time to implement.Another explanation may be that internal control impliesinforming the workers about hazards and the improve-ments to which they are entitled according to the WorkEnvironment Act and that this information may havereduced the workers’ satisfaction despite objective im-provements in the physical work environment.A change in internal control was positively correlated
with a change in workers’ satisfaction with psychosocialfactors, H&S-related behaviour and musculoskeletal pain.This is in accordance with another study on cross-sectionalrelationships between internal control and H&S factors(Torp et al., 2000) and with other studies showing thatorganizational factors at work are important for workers’job satisfaction, behaviour and health (Karasek andTheorell, 1990; Argyris and Schon, 1978; Golembiewskyet al., 1987). Change in internal control correlatedsignificantly with change in the psychosocial factors

ARTICLE IN PRESSS. Torp, B.E. Moen / Applied Ergonomics 37 (2006) 775–783 781
associated with support from colleagues or management,but not with change in psychological job demands anddecision authority. The reason for this may be that theworkers’ experience of support is relatively easy to improvethrough such measures as meetings, discussions andparticipatory assessment of the work environment (Elden,1986), whereas psychological job demands and decisionauthority are more difficult to influence since they arerelated to how the work is organized, how the company isstaffed and the finances of the company.
One of the main aims of internal control is to encourageworkers to participate in H&S activities and to change theirhealth-related behaviour. The results of this study showedincreased participation in H&S activities (that is, use ofpersonal protective equipment and compliance with H&Sroutines adopted) and coping with musculoskeletal symp-toms among workers in garages with improved internalcontrol. This is in accordance with learning and organiza-tional theories (Karasek and Theorell, 1990; Argyris andSchon, 1978; Bandura, 1986) that claim that managementand other organizational factors are important for work-ers’ behaviour, and this also includes their H&S-relatedbehaviour.
As studies have shown that smaller companies have notimplemented internal control to the same degree as largercompanies (Gaupseth, 2000; Saksvik and Nytro, 1996), thismay support the claim that internal control applies best inlarger companies (Gaupseth, 2000; Johansson and Johans-son, 1993). Nytro et al. (1998) also found that the size ofthe company correlated with the implementation ofinternal control, but this correlation did not remain whencontrolled for H&S competency and external push-and-pull factors. Strictly speaking, all the companies included inthe present study were so-called ‘‘small and medium-sized’’companies. Still, in line with the results of other studieswith a greater range in size of the included companies, thelargest companies included in our material had a moredeveloped internal control system than the smallest. Theresults indicate however that the effect of developing theinternal control system is about as positive in the smallest(less than 10 workers) as in the medium-sized (10–29workers) and the largest (429 workers) companiesincluded in this study. Thus, it may seem that the smallestcompanies are more reluctant to implement internalcontrol, perhaps because of reduced competence andmotivation, but the companies that actually implementinternal control seem to benefit from this.
The Regulation states that the occupational H&Smanagement system should be adapted to the size andneeds of the company. This means that the system shouldbe less comprehensive in smaller than in larger companies,because the smaller companies have less complex organiza-tional structures. In these companies, process factors suchas assessments and meetings should be emphasized morerather than the content factors such as written documenta-tion (Antonsson et al., 1998). Compared with largercompanies, smaller companies may benefit from other
H&S factors when implementing internal control. In thisstudy, for example, the correlations between change ininternal control and change in the factors related tomusculoskeletal symptoms were higher in the smallestcompanies than in the larger ones.The results of this study should be interpreted cautiously
since the significant relationships between a positive changein internal control and positive changes in work environ-ment, behaviour and health may be explained by changesin some external factors affecting the included variablesdirectly or indirectly, and since the managers might have atendency to overestimate the progress in implementinginternal control. In addition, the significant correlationswere rather low with explained variances (R2) betweenapproximately 1% and 14%. Nevertheless, the shownrelationships in this prospective study must be regarded asstronger indicators of causal relationships than similarrelations shown in a cross-sectional study, and the validityof the results is strengthened by the fact that they are inaccordance with theory and other studies on organizationalchange (Pfau, 1989; Frick et al., 2000; Karasek andTheorell, 1990). According to Tones and Tilford (2001)one cannot expect strong effects on specific outcomemeasures when developing ‘‘horizontal’’ health promotingprograms (such as management systems) and not ‘‘ver-tical’’ disease-centred interventions. According to theseauthors such a program may still have important effects asit often will have positive effects on the whole organiza-tional culture and thereby on several different outcomemeasures. This may be the case in the present study. Inaddition, it has been shown that up to 5 years must passbefore positive results are obtained on objective measuresof a written safety policy (Hoonaker et al., 2005).This study used questionnaires to collect information.
The response rate was relatively high, as 80% of themanagers and 75% of the workers responded in the firstsurvey versus 95% and 70% in the second survey. Despitethese relatively high response rates only 721 workersparticipated in both surveys. This may be a threat to theexternal validity of the results. The low rate of workersparticipating at both years can be explained by the fact thatthere is a high turn-over among garage workers (Moen andTorp, 2000), and that some of the questionnaires at the firstand second survey were impossible to match because therespondents’ personal codes were filled out incompletely.Since the demographic characteristics and independentvariables did not differ between the workers respondingtwice and those responding to the first questionnaire only,we believe that the 721 respondents included in the studyare relatively representative for workers at the garages.The internal reliability (Cronbach’s a) of the indices was
satisfactory for all indices (a values between 0.66 and 0.90),except for the two-item index of psychological job demands(Nunnally and Bernstein, 1994). Studies have found thatmanagers’ subjective evaluations of the company’s imple-mentation status of internal control correlate highly withmore objective measures of internal control (Gaupseth,

ARTICLE IN PRESSS. Torp, B.E. Moen / Applied Ergonomics 37 (2006) 775–783782
2000; Torp et al., 2000; Torvatn, 1997). In addition,managers’ subjective evaluations of the implementationstatus of internal control correspond with those of safetydelegates (Gaupseth, 2000). Therefore, we believe that theinternal control status’ measured in our study are reliable.
The companies included in this study were not a randomsample of garages in Norway. They were all members ofthe Norwegian Association of Motorcar Dealers andService Organization, and they all had received informa-tion about the Regulation from the Association. Thecompanies that had improved their internal control haddone this voluntarily. As H&S competence is important forimplementing internal control (Hovden, 1998; Nytro et al.,1998), unorganized companies with less H&S competenceand motivation for implementing internal control mightbenefit less than the companies that improved their internalcontrol in this study. We believe the results are relevant toother small and medium-sized organized companies withblue-collar workers.
The results indicate that positively changing the occupa-tional H&S management (that is, internal control) in smalland medium-sized companies may positively change work-ers’ satisfaction with the H&S activities, psychosocial workenvironment, and health-related behaviour. More researchis especially needed on long-term effects and on whichcontent and process factors in occupational H&S manage-ment are most important for improving H&S at theindividual level. Such research is important, since severalother countries use Norway’s model to pattern their ownregulatory strategy on occupational H&S management(Gaupseth, 2000).
Acknowledgements
This project was supported by the Confederation ofBusiness and Industry, the Norwegian Association ofMotorcar Dealers and Service Organization, the Norwe-gian United Federation of Trade Unions and VestaInsurance Company.
References
Antonsson, A., Hansen, O., Nilsson, M., 1998. Internkontroll i sma
foretag. Verklighet och visioner. (Internal Control in Small Enter-
prises). Institutet for Vatten- och Luftvardsforskning, Stockholm.
Argyris, C., Schon, D., 1978. Organizational Learning: A Theory of
Action Perspective. Addison-Wesley, London.
Bandura, A., 1986. Social Foundation of Thought and Action. A Social
Cognitive Theory. Prentice-Hall Inc., Englewood Cliffs, NJ.
Bliese, P.D., Jex, S.M., 1999. Incorporating multiple levels of analysis into
occupational stress research. Work Stress 13, 1–6.
Diez-Roux, A.V., 1998. Bringing context back into epidemiology:
variables and fallacies in multilevel analysis. Am. J. Public Health
88, 216–222.
Elden, M., 1986. Sociotechnical systems ideas as public policy in Norway:
empowering participation through worker-managed change. J. Appl.
Behav. Sci. 22, 239–255.
Eriksen, H.R., Ihlebæk, C., Ursin, H., 1999. A scoring system of subjective
health complaints. Scand. J. Public Health 27, 63–72.
Friberg, O., 1990. Arbeidsmiljøloven (The work environment act). Tano,
Oslo.
Frick, K., Jensen, P.L., Quinland, M., Wilthagen, T., 2000. Systematic
occupational health and safety management—an introduction to a new
strategy for occupational safety, health and well-being. In: Frick, K.,
Jensen, P.L., Quinland, M., Wilthagen, T. (Eds.), Systematic Occupa-
tional Health and Safety Management. Perspectives on an Interna-
tional Development. Pergamon, Oxford, pp. 1–14.
Gaupseth, S., 2000. The Norwegian internal control reform—an
unrealized potential. In: Frick, K., Jensen, P.L., Quinland, M.,
Wilthagen, T. (Eds.), Systematic Occupational Health and Safety
Management. Perspectives on an International Development. Perga-
mon, Oxford, pp. 329–348.
Golembiewsky, R.T., Hilles, R., Daly, R., 1987. Some effects of multiple
OD interventions on burnout and work site features. J. Appl. Behav.
Sci. 23, 295–313.
Gustavsen, B., Hunnius, G., 1981. New Patterns of Work Reform—The
Case of Norway. University Press, Oslo.
Hoonaker, P., Loushine, T., Carayon, P., Kallman, J., Kapp, A., Smith,
M.J., 2005. The effect of safety initiatives on safety performance: a
longitudinal study. Appl. Ergon. 36, 461–469.
Hovden, J., 1998. The ambiguity of contents and results in the Norwegian
internal control of safety, health and environment reform. Reliab.
Engin. Syst. Safety 60, 133–141.
Johansson, J., Johansson, B., 1993. Smaforetag och internkontroll. (Small
enterprises and internal control). Arbete, Manniska och Miljø 4,
282–285.
Karasek, R., Theorell, T., 1990. Healthy Work. Stress, Productivity and
the Reconstruction of Working Life. Basic Books, New York.
Karasek, R., Brisson, C., Kawakami, N., Houtman, I., Bongers, P.,
Amick, B., 1998. The Job Content Questionnaire (JCQ): an instrument
for internationally comparative assessments of psychosocial job
characteristics. J. Occup. Health. Psychol. 3, 322–355.
Kim, D., 1994. TQM and systems thinking as theory building tools. Syst.
Thinker 5, 1–4.
Kjellen, U., Boe, K., Hagen, L., 1997. Economical effects of implementing
internal control of health, Safety and environment: a retrospective case
study of an aluminium plant. Safety Sci. 27, 99–114.
Kristensen, T.S., 1995. The demand-control-support model: methodolo-
gical challenges for future research. Stress Med. 11, 17–26.
Ministry of Labour and Government Administration, 1997. Regulation
concerning systematic health, environment and safety work in
enterprises (the internal control regulation). Oslo. (Available at
http://www.arbeidstilsynet.no/regelverk/forsokrifter/full544a.html,
accessed December 2004).
Ministry of Local Government, 1991. Internkontroll. Forskrift med
veiledning. (The internal control regulation). Oslo.
Moen, B.E., Torp, S., 2000. Den eldre arbeidstaker i bilbransjen: Hvor
blir det av utdannede bilmekanikere? (The senior worker in the
motorcar trade: where do the trained car mechanics go?) (Rep. No. 2/
2000). Section for Occupational Medicine, University of Bergen,
Bergen.
Nunnally, J.C., Bernstein, I.H., 1994. Psychometric Theory, third ed.
McGraw-Hill, New York.
Nytro, K., Saksvik, P.O., Torvatn, H., 1998. Organizational prerequisites
for the implementation of systematic health, environment and safety
work in enterprises. Safety Sci. 30, 297–307.
Pfau, L.D., 1989. Total quality management gives companies a way to
enhance position in global market. Ind. Eng. 21, 17–21.
Robinson, W.S., 1950. Ecological correlations and the behvior of
individuals. Am. Sociol. Rev. 15, 351–357.
Saksvik, P.O., Nytro, K., 1996. Implementation of internal control (IC) of
health, environment and safety (HES) in Norwegian enterprises. Safety
Sci. 23, 55–61.
Saksvik, P.O., Torvatn, H., Nytro, K., 2003. Systematic occupational
health and safety work in Norway: a decade of implementation. Safety
Sci. 41, 721–738.
SPSS Base 11.0, 2001. User’s Guide. SPSS Inc., Chicago.

ARTICLE IN PRESSS. Torp, B.E. Moen / Applied Ergonomics 37 (2006) 775–783 783
Theorell, T., Michelsen, H., Nordemar, R., Music 1 Study Group, 1993.
Validitetsprovning av psykososiala indexbildningar. (Validity testing
of psychosocial indices). In: Hagberg, M., Hogstedt, C. (Eds.),
Stockholmsundersokningen 1 (The Stockholm Study 1). Music Books,
Stockholm, pp. 163–177.
Tones, K., Tilford, S., 2001. Health Promotion. Effictiveness, Efficiency
and Equity. Nelson Thornes Ltd, Cheltonham.
Toomingas, A., Theorell, T., Michelsen, H., Nordemar, R., 1997. Associa-
tions between self-rated psychosocial work conditions and musculoske-
letal symptoms and signs. Scand. J. Work Environ. Health 23, 130–139.
Torp, S., Riise, T., Moen, B.E., 1996. Work-related musculoskeletal
symptoms among car mechanics: a descriptive study. Occup. Med.
(Lond.) 46, 407–413.
Torp, S., Riise, T., Moen, B.E., 2000. Systematic health, environment and
safety activities: do they influence occupational environment, beha-
viour and health? Occup. Med. (London) 50, 326–333.
Torp, S., Riise, T., Moen, B.E., 2001a. The impact of psychosocial work
factors on musculoskeletal pain: a prospective study. J. Occup.
Environ. Med. 43, 120–126.
Torp, S., Riise, T., Moen, B.E., 2001b. The impact of social and
organizational factors on workers coping with musculoskeletal
symptoms. Phys. Ther. 81, 1328–1338.
Torvatn, H., 1997. Faktorer som fremmer eller hindrer innføring av IK-
systemer i mindre bedrifter. En reanalyse av to spørreskjemaundersø-
kelser. (Factors influencing implementation of internal control
systems in small enterprises) (Rep. No. STF38 A97521). SINTEF,
Trondheim.
Walters, D., Jensen, P.L., 2000. The Discourses and purposes behind the
development of the EU Framework Directive 89/391. In: Frick, K.,
Jensen, P.L., Quinland, M., Wilthagen, T. (Eds.), Systematic Occupa-
tional Health and Safety Management. Perspectives on an Interna-
tional Development. Pergamon, Oxford, pp. 87–98.