Embed Size (px)
Citation preview

Actn Medicn Scnndinnvicn. Vol. CXXXV, fnsc. I, 1949.
From the Seventh Department, Kommrinehospitalet, Copenhagen. (Chief: Tage Bjering, N. I).)
The Elimination of Iodophtlzalein in Normnl and Icteric Sub j ccts.1
BY H. 0. B A N G 2 and JOHAN GEORG.
(Submitted for publication October 29, 1948.)
Introduced by the now classical paper of Abel and Rowntree: ))On the Pharma- cological Action of Some Phthaleins and Their Derivatives, with Especial Reference to Their Behavior as Purgatives)) (1909), the halogen-substituted phenolphthaleins rapidly gained a firm place among the diagnostic adjuvants of clinical medicine. Being excreted almost electively with the bile, this group of substances offer the possibility of an insight into the liver function through a study of their excretion. Rowntree et al. (1913) and Whipple et al. (1913) employed phenoltetrachlorphtha- lein for this purpose; later Rosenthal and White (1924-25, 1925) introduced a sulphonated compound phenoltetrabromphthalein sodium sulphonate, which, under the name of bromsulphalein, has been widely used for liver-function tests.
Graham and Cole (1924) employed the phenolphthalein derivatives as contrast media for X-ray examination of the gall bladder. I n this connexion iodophthalein (sodium tetraiodophenolphthaleinate) proved to be the most suitable.
The question of combining cholecystography and liver-function tests with these substances was taken up for discussion very soon (Graham et al. 1926)) but certain practical difficulties appeared. I n the performance of liver-function tests the indicator properties of the phenolphthalein derivatives were utilized in their quantitative estimation, these substances in a basic environment forming coloured compounds that are suitable for colorimetric determination. However, the chlorine and bromine compounds develop a more intense colour than do the iodine com- pounds. Moreover, of the isomer compounds, with halogen substitution either in the phthalic acid ring or in the phenol rings, the former have much more pro- nounced indicator properties than the latter. Thus it was a substance of the first
1 The work was supported by Miss P. A. Brandt’s E’und. a Kildeskovsvej 52, Urntofte (Denmark).
THE ELIMINATION OF IODOPHTIIALEIN IN NORMAL AND ICTERIC SUBJECTS. 69
group (i. e. the type: phenoltetrahalogenphthalein) that was adopted for the func- tion tests; but it was one of the substances of the other group: tetraiodophenol- phthalein (in the form of the sodium salt: iodophthalein) that proved the best for cholec ystography.
Nevertheless, there have been a few colorimetric determinations of the ex- cretion of iodophthalein in patients with liver affections. Behrend and Heesch (1926) observed that in the case of liver affections this substance is excreted for a
I 2 3 4 5 6 7 8 9 10 /I l 2 0 A f i
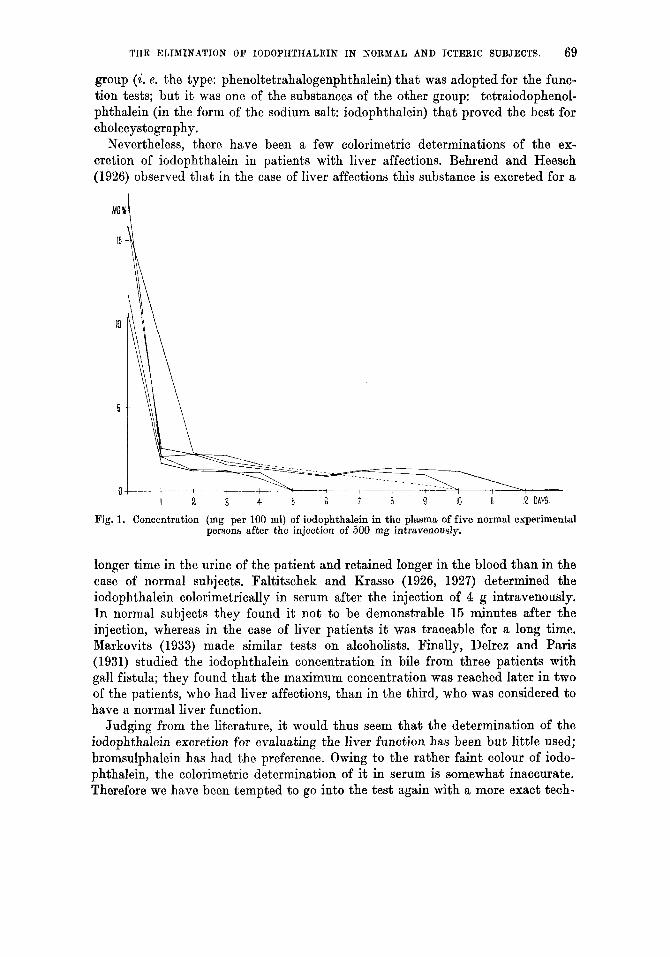
Fig. 1. Concentration (mg per 100 ml) of iodophthalein in the plasma of five normal experimental persons after the injection of 500 mg intravenously.
longer time in the urine of the patient and retained longer in the blood than in the case of normal subjects. Faltitschek and Krasso (1926, 1927) determined the iodophthalein colorimetrically in serum after the injection of 4 g intravenously. I n normal subjects they found i t not to be demonstrable 15 minutes after the injection, whereas in the case of liver patients i t was traceable for a long time. Markovits (1933) made similar tests on alcoholists. Finally, Dehez and Paris (1931) studied the iodophthalein concentration in bile from three patients with gall fistula; they found that the maximum concentration was reached later in two of the patients, who had liver affections, than in the third, who was considered to have a normal liver function.
Judging from the literature, it would thus seem that the determination of the iodophthalein excretion for evaluating the liver function has been but little used; bromsulphalein has had the preference. Owing to the rather faint colour of iodo- phthalein, the colorimetric determination of it in serum is somewhat inaccurate. Therefore we have been tempted to go into the test again with a more exact tech-
70 11. 0. BANQ AND JOHAN QEORQ.
nique. The point is that the iodine compounds, as distinct from the others, provide a possibility of exact quantitative determination by means of an iodometric titra- tion, following the complete destruction of the substance with liberation of iodine. A method for this has been worked out, and published in an earlier paper (Bang and Georg, 1948). I n the following an account will be given of the iodophthalein excretion of 12 patients with affections of the liver or bile-ducts, together with a brief recapitulation of the iodophthalein excretion in normal subjects (cf. Bang and Georg, 1. c.).
After the injection pf 500 mg iodophthalein intravenously the substance is demonstrable in serum up to ten or twelve days (fig. 1). (The slight sensibility of the colorimetric determination of this substance may be seen from this, for, as already stated, Paltitschek and Krasso found that iodophthalein had disappeared from the serum of normals 15 minutes after the intravenous injection of 4 g.) In the urine iodophthalein is excreted in very small quantities for one or two days, whereas much the greater part is excreted with faeces, in which it can be traced for ten days or more after the injection.
Material and Results.
The principal data of the twelve patients with liver or bile-duct affections, on whom the present investigation was made, will be found summarized in Table I. Numbers 1 to 9 are patients with acute hepatitis, enumerated according to the duration of the jaundice a t the time of the iodophthalein injection. Thus the lower numbers represent the early stages of hepatitis, the higher numbers later stages. Patient No. 10 had chronic hepatitis (hepatic cirrhosis), and Nos. 11 and 12 had obstructive jaundice as a consequence of pancreatic carcinoma (though both had some secondary liver affection, verified a t neoropsy). For the patients first tested the dose of iodophthalein was 500 mg, later a dose of 10 mg per kg body weight was used.
I n these tests the principal interest was directed against the determination of iodophthalein in serum. The patients were observed by means of daily blood samples during the first eight t o fourteen days after the injection -in some instances longer. The quantity of iodophthalein excreted in the urine does not seem to be of much interest in conjunction with liver affections; no definite difference was found between normal subjects and pathological cases. Excretion with faeces was not followed; this determination is somewhat difficult and time-consuming and does not seem to present any advantage over the blood analyses.
The table shows the iodophthalein concentration in plasma taken on the fourth, eighth and twelfth day after the injection. Our results on five normal experimental persons may be given here for purpose of comparison (cf. fig. 1): Iodophthalein was traceable in all five on the fourth day after the injection, in three on the eighth day, and in none on the twelfth day.
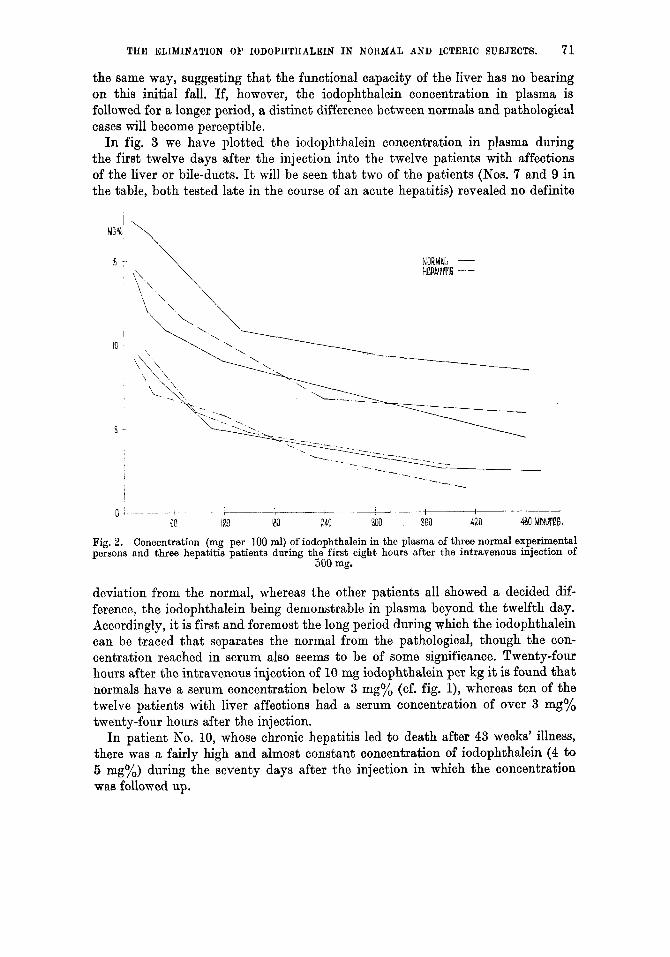
The plasma concentration during the first eight hours after the injection of iodophthalein is compared in fig. 2 between three normals and three patients with hepatitis. In all cases the decrease of the concentration seems to proceed in exactly
THE ELIMINATION OF IODOPHTHALEIN IN NORMAL A N D ICTERIC SUBJECTS. 71
the same way, suggesting that the functional capacity of the liver has no bearing on this initial fall. If, however, the iodophthalein concentration in plasma is followed for a longer period, a distinct difference between normals and pathological cases will become perceptible.
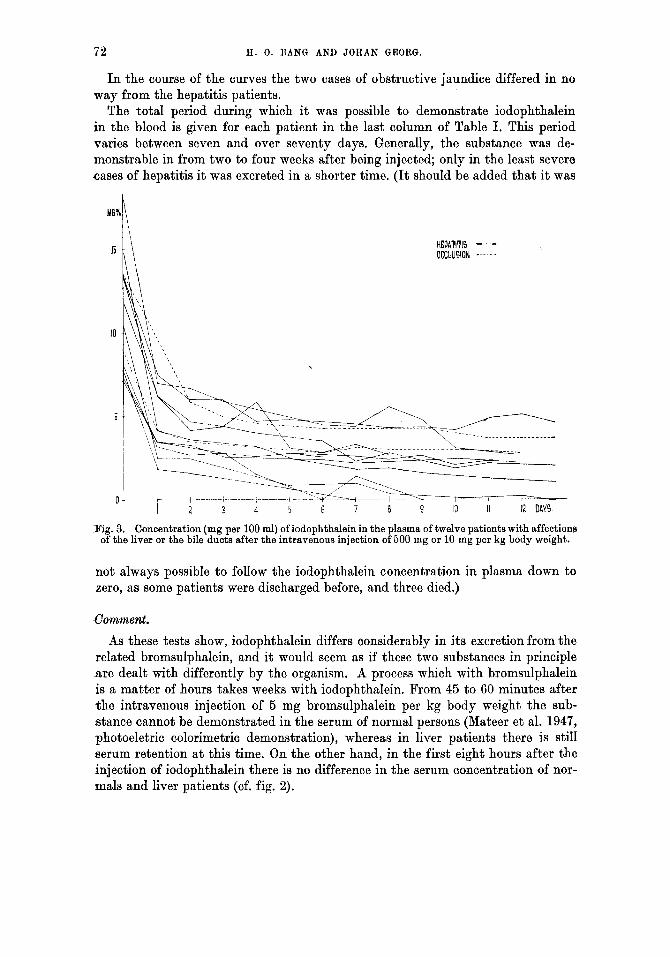
In fig. 3 we have plotted the iodophthalein concentration in plasma during the first twelve days after the injection into the twelve patients with affections of the liver or bile-ducts. It will be seen that two of the patients (Nos. 7 and 9 in the table, both tested late in the course of an acute hepatitis) revealed no definite
NORMAL - HEPATITIS - -
- -.-._
, . . . I
0 , ____ I-- - ,v-- I t' 60 ID iB0 240 "500 3BO 420 490 MINUTEG.
Fig. 2. Concentration (mg per 100 ml) of iodophthalein in the plasma of three normal experimental persons and three hepatitis patients during th,B first eight hours after the intravenous injection of
900 mg.
deviation from the normal, whereas the other patients all showed a decided dif- ference, the iodophthalein being demonstrable in plasma beyond the twelfth day. Accordingly, it is first and foremost the long period during which the iodophthalein can be traced that separates the normal from the pathological, though the con- centration reached in serum also seems to be of some significance. Twenty-four hours after the intravenous injection of 10 mg iodophthalein per kg it is found that normals have a serum concentration below 3 mg% (cf. fig. l), whereas ten of the twelve patients with liver affections had a serum concentration of over 3 mg% twenty-four hours after the injection.
In patient No. 10, whose chronic hepatitis led to death after 43 weeks' illness, there was a fairly high and almost constant concentration of iodophthalein (4 to 6 mg%) during the seventy days after the injection in which the concentration waa followed up.
72 H. 0. BANQ AND JOHAN GEORQ.
I n the course of the curves the two cases of obstructive jaundice differed in no way from the hepatitis patients.
The total period during which i t was possible to demonstrate iodophthalein in the blood is given for each patient in the last column of Table I. This period varies between seven and over seventy days. Generally, the substance was de- monstrable in from two to four weeks after being injected; only in the least severe cases of hepatitis i t was excreted in a shorter time. ( I t should be added that it was
15 HEPATIT14 - OCC~IUSION ------
Fig. 3. Concentration (mg per 100 ml) of iodophthalein in the plasma of twelve patients with affections of the liver or the bile ducts after the intravenous injection of 500 mg or 10 mg per kg body weight.
not always possible t o follow the iodophthalein concentration in plasma down to zero, as some patients were discharged before, and three died.)
Comment.
As these tests show, iodophthalein differs considerably in its excretion from the related bromsulphalein, and i t would seem as if these two substances in principle a re dealt with differently by the organism. A process which with bromsulphalein is a matter of hours takes weeks with iodophthalein. Prom 45 to 60 minutes after the intravenous injection of 5 mg bromsulphalein per kg body weight the sub- .stance cannot be demonstrated in the serum of normal persons (Mateer et al. 1947, photoeletric colorimetric demonstration), whereas in liver patients there is still serum retention at this time. On the other hand, in the first eight hours after the injection of iodophthalein there is no difference in the serum concentration of nor- mals and liver patients (cf. fig. 2).

THE ELIMINATION OF IODOPHTIIALEIN IN NORMAL AND ICTERIC SUBJECTS. 73
~
1 (ac. hepatitis) . . . . . . . . . . 2 ( 1) D ) . . . . . . . . . . 3 ( )) 1) ) . . . . . . . . . . 4 ( 0 1) ) . . . . . . . . . . 5 ( )) 1) ) . ......... 6 ( u 1) ) . . . . . . . . . 7 ( )) 1) ) . . . . . . . . . . 8 ( 1) 1) ) . . . . . . . . . . 9 ( 0 )> ) . . . . . . . . . .
10 (chr. heoatitis) . . . . . . . . .
Table I.
Data of Patient Material
63 210
. . . . . . . . . . . 11 (obstruction) 7; 12 ( )) ) . . . . . . . . . . .
1- 4 700
- 6 600 - 9 500
5-6 I 700
- 11-12 560 11 500
- 13 500 10 a00
._ 14 600
__ 7 1 700
t++ 43 600
++ 1 7 i 600
-
-
__
4.0 5.9 2.6 5.4 3.2 2.6 1.3 1. L 1 .o 4.7 3.2 4.ri
2.8 2.7 2.4 5.G 1.9 2.9 0.7 0.4 0
4.3 3.0 4.3
2.1 I 2 1 - .:. 8 2.2 22 2.7 -.15 i . 2 16 2.2 32 0 9
0.3 14 0 7
5.1 >70 2.s -.15 3.7 j -19
In plasma, iodophthalein is present in a colourless, undialysable form, presumably as a fine colloidal suspension, whereas the sulphonated compounds are soluble (Ilosenthal and White, 1924-25). Both iodophthalein and bromsulphalein can be demonstrated in the bile five to ten minutes after the injection. This means that the excretion of both begins a t once, but the excretion of iodophthalein continues over a much longer period. Presumably the cause of this is either a different re- absorption from the in t e she , or a different behaviour toward the reticuloendothe- lial system: the colloidally suspended compounds should mainly be absorbed by the reticuloendothelial system whereas the soluble sulphonated compounds are not affected by it. It was in conformity with this idea when Rosenthal and Lillie (1931) showed that the blocking of the reticuloendothelial system with Indian ink does not affect the excretion of bromsulphalein. However, Klein and Levinson (1933) arrived a t exactly the opposite result, and for the present the question must be regarded as still open.
To summarize, i t may be said that the estimation of the iodophthalein elimina- tion in patients with liver diseases provides an expression of the degree of liver affection, whereby i t acquires a certain prognostic interest. Like the related tests, principally the bromsulphalein test, i t is of no assistance in the differential dia- gnosis between parenchymatous jaundice and obstructive jaundice. The deter- mination of the iodophthalein concentration can be made with much greater accuracy than that of the bromsulphalein concentration, but i t is a considerable drawback that the result of the test is not available before the lapse of several weeks. If the excretion of iodophthalein is to become of any utility as a liver func- tion test the most reasonable course will be to follow the concentration in serum once a week, a t the same time as blood is taken for other liver-function tests.
74 H. 0. BANQ AND JOHAN QEORG.
Summary.
An account is given of the excretion of iodophthalein by twelve patients with affections of the liver or bile-ducts, tested after the intravenous injection of 500- 700 mg iodophthalein. The substance is usually traceable in serum during two to four weeks after the injection, and was in one case demonstrable for more than seventy days. The excretion curves are identical for patients with obstructive and with parenchymatous jaundice. I n the first eight hours after the injection the fall in iodophthalein-concentration is the same for normal subjects and for liver patients, but in normals the iodophthalein concentration in plasma reaches zero after six to twelve days.
Referenaes.
Abel, J. J. and L. G. Rowntree: J. Pharm. Exp. Ther. 1909, I , 231. - Bang, H. 0. and J. Georg: Acta pharmacol. 1948,4,87. - Behrend, C. M. and 0. Heesch: Med. Klinik 1926, 22, 767. - Delrez, L. M. and M. Paris: Presse m6d. 1931, 39, 97. - Paltitschek, P. and H. Krasso: Wien. klin. Wochenschr. 1926, 39, 387; ibid. 1927, 40, 386. - Graham, E. A. and W. H. Cole: J. A. M. A. 1924, 82, 613. - Graham, E. A., W. H. Cole, G. H. Copher and S. Moore: ibid. 1926, 86, 46. - Klein, R. I. and S. A. Levinson: Proc. SOC. Exp. Biol. Med. 1933, 31,179. - Markovits, G.: Monatschr. Psych. Neurol. 1933,815, 101. - Mateer, J. G., J. I. Baltz, P. D. Commanduras, H. H. Steele and S. W. Brouwer: Gastro- enterology 1947, 8, 52. - Rosenthal, S. M.: Bull. Johns Hopkins Hosp. 1922, 33, 432. - Rosenthal, S. M.: J. Pharm. Exp. Ther. 1922, 19, 385. - Rosenthal, S. M. and E. C. White: ibid. 1924-25, 24, 265. - Rosenthal, S. M. and E. C. White: J. A. M. A. 1925, 84,1112. - Rosenthal, S. M. and R. D. Lillie: Am. J. Physiol. 1931,97,131. - Rowntree, L. G., S. H. Hurwitz and A. L. Bloomfield: Bull. Johns Hopkins Hosp. 1913,24, 327. - Whipple, G. H., V. R. Mason and T. C. Peightal: ibid. 1913, 24, 207. - Whipple, G. H., T. C. Peightal and A. H. Clark: ibid. 1913,24, 343.