Embed Size (px)
Citation preview

Schizophrenia Research 138 (2012) 274–279
Contents lists available at SciVerse ScienceDirect
Schizophrenia Research
j ourna l homepage: www.e lsev ie r .com/ locate /schres
The Experience of Caregiving Inventory for first-episode psychosis caregivers:Validation of the Brazilian version
Rita de Cássia Ferreira de Araújo Jorge, Ana Cristina Chaves ⁎First Episode Psychosis Program, Psychiatry Department, Federal University of São Paulo (UNIFESP-EPM), BrazilRua Borges Lagoa, 570, 6° andar, CEP 04032-900, São Paulo, SP, Brazil
⁎ Corresponding author at: Federal University of SãoProgram, Rua Borges Lagoa, 570, 6° andar, CEP 04032-90011 5576 4160; fax: +55 11 5571 7524.
E-mail addresses: [email protected] (R.C.F.A. Jorge(A.C. Chaves).
0920-9964/$ – see front matter © 2012 Elsevier B.V. Alldoi:10.1016/j.schres.2012.03.014
a b s t r a c t
a r t i c l e i n f oArticle history:Received 23 October 2011Received in revised form 5 March 2012Accepted 7 March 2012Available online 2 April 2012
Keywords:First-episode psychosis (FEP)CaregiversExperience of Caregiving InventorySRQ-20SF-36Translation studyValidation study
Family members of first-episode psychosis (FEP) patients are regarded as key components of the patient'sevaluation, recovery and treatment. This paper aimed to investigate 75 FEP caregivers' appraisal, psycholog-ical morbidity and quality of life in the initial phase of treatment in a specialized FEP outpatient program inSão Paulo, Brazil, and evaluate the validation of the Brazilian version of the Experience of Caregiving Inventory(ECI). Caregivers were also scored through Self Report Questionnaire-20 and Short Form-36. It was found that29% of them might be a case for minor psychiatric disorder, that the worst domains of quality of life concernedemotional aspects, vitality and bodily pain, and that they were particularly affected by patients' negativesymptoms, dependency and difficult behaviors. Additionally, internal consistency of ECI was very satisfac-tory (Cronbach's alpha=0.95) with subscales ranging from 0.57 (stigma) to 0.94 (total negative score). TheBrazilian version of the ECI is not only a facile, reliable and valid instrument to describe the experience ofcaring for a relative with serious mental illness. It offers mental health professionals an opportunity to ac-cess caregivers' global experience and their evaluation of a severe mental disease, as well as to predict theirpsychological suffering, which is harmful to both patient and caregiver.
© 2012 Elsevier B.V. All rights reserved.
1. Introduction
Family members of first-episode psychosis (FEP) patients areregarded as fundamental components of the patient's evaluation, recov-ery and treatment. However, this is not an easy task. Family membersusually face difficulties, feel distressed and hopelessness. Furthermore,insofar as this new situation may disrupt the family system, mentalhealth professionals should recognize it and be able to help familymem-bers deal and understand the nature of the patients' symptoms. Studiesconducted with FEP patients showed that caregivers' perceptions of thepatients' behavior were more important than their actual behavior,symptoms or functional impairment (Martens and Addington, 2001).To address all these concerns, FEP programs should develop models offamily intervention to ameliorate caregivers' distress and to help themto cope with this role (Bertolote and McGorry, 2005).
In the last ten years the Brazilian mental health system has em-braced the worldwide emphasis on community treatment for severemental disorders. As a consequence, patient's relatives became themain caregivers of these individuals, making a great effort to maintainthe family unit, understand what has happened and help the affected
Paulo, First Episode Psychosis, São Paulo, SP, Brazil. Tel.: +55
rights reserved.
member. A survey conducted in a FEP program in São Paulo, Brazilshowed that their needs and understanding about the illness are similarto FEP family members from other countries. They reported that theyknow little about the disease, have difficulty identifying the psychoticsymptoms and want to be knowledgeable about treating the patient.They stressed that talking about their feelings, such as guilt or anger,and struggling to understand the patient's behavior were their mainneeds (Cabral and Chaves, 2005). A further survey evaluatingmulti-family intervention delivered by this same FEP programshowed that caregivers found the intervention helpful regardingknowledge acquisition about the illness, but emphasized that thenon-specific aspects of the intervention were very useful for them(Cabral and Chaves, 2010).
The Experience of Caregiving Inventory (ECI) is an instrument de-veloped into a “stress-coping” model, whose concept is based on thecarer's appraise of the impact of the illness. It is a self-reportedmeasure,providing a comprehensive description of the caregiving experiencewith a relative with serious mental illness. ECI presents a new attitudeof caregiving, which rejects viewing burden as the only measure oftheir experience. The scale authors pointed that the term ‘burden’ isnegative and damaging, refuting any positive or rewarding aspect ofcare. The inventory assesses both positive and negative aspects of care-giving, and its negative scale is considered the strongest predictor ofcarers' psychological well-being (Szmukler et al., 1996; Addington etal., 2003). According to Joyce et al. (2000), carers' appraise their situa-tion not only according to the degree of demands or stressors on

275R.C.F.A. Jorge, A.C. Chaves / Schizophrenia Research 138 (2012) 274–279
them, but also mediating environmental factors such as social support,family relationships and service inputs. ECI was used to assess carersin several clinical situations (McCleery et al., 2007; Grover et al., 2011;Sepulveda et al., 2011). It was also adapted and validated in differentcultures (Tarricone et al., 2006; Lau and Pang, 2007). In addition, ECIis a good instrument to be used as anoutcomemeasure to evaluate fam-ily interventions aimed to decrease carers' distress.
There are few studies investigating the experience of FEP caregivingin South American countries. We consider very important to increasethe knowledge in this area for the Latin cultures and enlarge measuresto assess caregivers distress and experience. This paper has the purposeto assess FEP caregivers' appraisal, psychological morbidity and qualityof life in the initial phase of treatment and to evaluate the validation ofthe Brazilian version of ECI.
2. Methods
2.1. Setting
This studywas conducted in the FEP Programof the Federal Universityof São Paulo (UNIFESP-EPM), in São Paulo, Brazil, an outpatient service of-fering a comprehensive treatment program. To be enrolled in the service,the patients should be between15 and 35 years old, be experiencing theirfirst episode of psychosis (Keshavan and Schooler, 1992) and must nothave received more than 3 months of adequate previous treatment.Most patients are referred from the psychiatry emergency service of alarge public university hospital that primarily provides care to alow-income population. The data presented in this paper is part ofa follow-up study which received approval from the local ethicscommittee (no 0738/08).
2.2. Sample
From January of 2009 to July of 2011, seventy-five patientsand their caregivers were invited to participate in the study. To beconsidered a caregiver the individual (a) had to be over 18 yearsold, (b) should live with the patient in the same home or have atleast one contact per week in order to help him directly, (c) shouldnot be paid for the assistance and (d) agreed to participate in thestudy by signing the written consent form.
2.3. Translation
The translation of the Portuguese-Brazilian ECI version was autho-rized by the scale author and the process followed Guillemin's (1995)recommendations for this procedure. First, the scale was translatedfrom English into Brazilian-Portuguese by four independent translators.In this phase, translations divergences between themwere detected anddiscussed to reach a consensus. This edition was back-translated intoEnglish by two English native speakers, their versions being comparedwith the original English version to detect inaccuracies. An Englishfluent board comprising three psychiatrist and three psychologistsevaluated each scale item and scored it as adequate or not in relationto semantic, content, criteria and conceptual similarity. This first ver-sion received 84% of approval by the judges. Minor discrepancieswere revaluated by a new panel consisting of a psychiatrist, a psychol-ogist and a social worker, all with sound experience in FEP, and a finalversion was accomplished taking into account their suggestions. Wecarried out a pilot study with five caregivers and no problem wasdetected in the performance of the final scale version.
2.4. Measures and procedure
Patients' and caregivers' socio-demographic characteristics wererecorded using an ad hoc structured questionnaire. Patients werediagnosed according to DSM-IV criteria using the Structural Clinical
Interview (SCID-I) (First et al., 1995) and their symptoms wereassessed with the Positive and Negative Syndrome Scale for Schizo-phrenia (PANSS) (Kay et al., 1987; Vessoni, 1993). The scales ECI,SF-36 and SRQ-20 were designed to be self reported, however we de-cided to interview the caregivers because of the low educational levelof our sample, in order to avoid misclassification bias. An individualtrained by the first author, blind to patient's assessments performedthe caregivers' evaluation orally using the following instruments:
2.4.1. Experience of Caregiving Inventory (ECI) — Portuguese-Brazilianversion
Instrument developed into a “stress-coping” model, conceptualizedbased on carer's appraise of the impact of the illness. It is a scaledesigned to measure both negative and positive aspects of caregivingexperience as perceived by a person responsible for the care of a personwith a serious mental illness. Sixty-six items are comprised in ten sub-scales, eight negative (difficult behaviors, negative symptoms, stigma,problems with services, effects on family, need to provide backup, de-pendence and loss) and two positive (rewarding personal experiencesand good aspects of relationship with the patient) (Szmukler et al.,1996). The ECI negative scale is considered the strongest predictor ofcarer's psychological well-being (Addington et al., 2003).
2.4.2. Short-Form-36 (SF-36)Scale constructed to survey the health status in the Medical
Outcomes Study, was designed for use in clinical practice and research,health policy evaluations and general population surveys. It is a genericoutcomemeasure designed to examine a person's perceived health sta-tus and one of the most instruments used in health research, which in-cludes one multi-item scale measuring each of the following eighthealth concepts: physical functioning; role limitations because of phys-ical health problems; bodily pain; general health perceptions; Vitality(energy/fatigue); social functioning; role limitations because of emo-tional problems; and general mental health (Ware and Shelbourne,1992; Ciconelli et al., 1999). A recent study showed that the Brazilianversion of SF-36 is a reliable and validmeasure of health related to qual-ity of life among the general population in Brazil (LaGuardia et al.,2011).
2.4.3. Self-Report Questionnaire (SRQ-20)Screening instrumentwas developed by theWorldHealth Organiza-
tion as a screening instrument andwas designed to identify minor non-psychotic psychiatric disturbance in primary care settings and in thecommunity. In this study we used the full version, which contains 24items, 20 to screen for non-psychotic morbidity and 4 items intendedto detect psychotic symptoms (Harding et al., 1980). The validity coeffi-cients of the Brazilian version were evaluated at primary care servicesand the recommended cut-off point was 7 for man and 8 for woman(Mari and Williams, 1986).
2.5. Statistical analysis
Data were expressed as proportion or mean and standard devia-tion. Cronbach's alpha was used for reliability (internal consistency)of the Brazilian version of the ECI. The external validity level wasevaluated by correlations between ECI scores×caregivers' psycho-logical morbidity and quality of life measured by SRQ-20 and SF-36,respectively. Associations between variables were compared usingPearson's correlation and mean comparisons between subgroupswere performed using Student's T-test when the variable had a normaldistribution. For both ECI×SRQ-20 and ECI×SF-36 comparisons wechose to use non-parametric statistical tests, (Mann–WhitneyU compar-ison between mean scores for ECI/SRQ-20 data and Spearman correla-tions for the ECI/SF-36 data) because it was not possible to establish anormal distribution of data. We also ran parametric tests that showedidentical results. Descriptive and statistical tests (T-Test)were performed
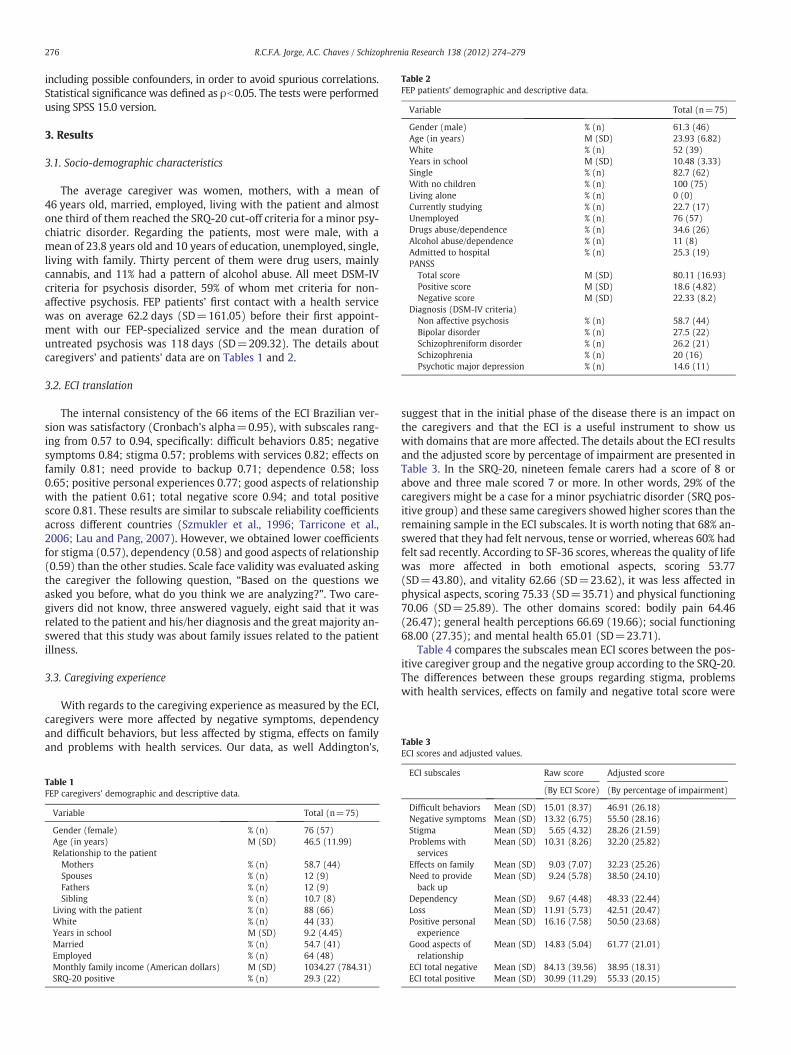
Table 2FEP patients' demographic and descriptive data.
Variable Total (n=75)
Gender (male) % (n) 61.3 (46)Age (in years) M (SD) 23.93 (6.82)White % (n) 52 (39)Years in school M (SD) 10.48 (3.33)Single % (n) 82.7 (62)With no children % (n) 100 (75)Living alone % (n) 0 (0)Currently studying % (n) 22.7 (17)Unemployed % (n) 76 (57)Drugs abuse/dependence % (n) 34.6 (26)Alcohol abuse/dependence % (n) 11 (8)Admitted to hospital % (n) 25.3 (19)PANSS
Total score M (SD) 80.11 (16.93)Positive score M (SD) 18.6 (4.82)Negative score M (SD) 22.33 (8.2)
Diagnosis (DSM-IV criteria)Non affective psychosis % (n) 58.7 (44)Bipolar disorder % (n) 27.5 (22)Schizophreniform disorder % (n) 26.2 (21)Schizophrenia % (n) 20 (16)Psychotic major depression % (n) 14.6 (11)
Table 3ECI scores and adjusted values.
276 R.C.F.A. Jorge, A.C. Chaves / Schizophrenia Research 138 (2012) 274–279
including possible confounders, in order to avoid spurious correlations.Statistical significance was defined as ρb0.05. The tests were performedusing SPSS 15.0 version.
3. Results
3.1. Socio-demographic characteristics
The average caregiver was women, mothers, with a mean of46 years old, married, employed, living with the patient and almostone third of them reached the SRQ-20 cut-off criteria for a minor psy-chiatric disorder. Regarding the patients, most were male, with amean of 23.8 years old and 10 years of education, unemployed, single,living with family. Thirty percent of them were drug users, mainlycannabis, and 11% had a pattern of alcohol abuse. All meet DSM-IVcriteria for psychosis disorder, 59% of whom met criteria for non-affective psychosis. FEP patients' first contact with a health servicewas on average 62.2 days (SD=161.05) before their first appoint-ment with our FEP-specialized service and the mean duration ofuntreated psychosis was 118 days (SD=209.32). The details aboutcaregivers' and patients' data are on Tables 1 and 2.
3.2. ECI translation
The internal consistency of the 66 items of the ECI Brazilian ver-sion was satisfactory (Cronbach's alpha=0.95), with subscales rang-ing from 0.57 to 0.94, specifically: difficult behaviors 0.85; negativesymptoms 0.84; stigma 0.57; problems with services 0.82; effects onfamily 0.81; need provide to backup 0.71; dependence 0.58; loss0.65; positive personal experiences 0.77; good aspects of relationshipwith the patient 0.61; total negative score 0.94; and total positivescore 0.81. These results are similar to subscale reliability coefficientsacross different countries (Szmukler et al., 1996; Tarricone et al.,2006; Lau and Pang, 2007). However, we obtained lower coefficientsfor stigma (0.57), dependency (0.58) and good aspects of relationship(0.59) than the other studies. Scale face validity was evaluated askingthe caregiver the following question, “Based on the questions weasked you before, what do you think we are analyzing?”. Two care-givers did not know, three answered vaguely, eight said that it wasrelated to the patient and his/her diagnosis and the great majority an-swered that this study was about family issues related to the patientillness.
3.3. Caregiving experience
With regards to the caregiving experience as measured by the ECI,caregivers were more affected by negative symptoms, dependencyand difficult behaviors, but less affected by stigma, effects on familyand problems with health services. Our data, as well Addington's,
Table 1FEP caregivers' demographic and descriptive data.
Variable Total (n=75)
Gender (female) % (n) 76 (57)Age (in years) M (SD) 46.5 (11.99)Relationship to the patient
Mothers % (n) 58.7 (44)Spouses % (n) 12 (9)Fathers % (n) 12 (9)Sibling % (n) 10.7 (8)
Living with the patient % (n) 88 (66)White % (n) 44 (33)Years in school M (SD) 9.2 (4.45)Married % (n) 54.7 (41)Employed % (n) 64 (48)Monthly family income (American dollars) M (SD) 1034.27 (784.31)SRQ-20 positive % (n) 29.3 (22)
suggest that in the initial phase of the disease there is an impact onthe caregivers and that the ECI is a useful instrument to show uswith domains that are more affected. The details about the ECI resultsand the adjusted score by percentage of impairment are presented inTable 3. In the SRQ-20, nineteen female carers had a score of 8 orabove and three male scored 7 or more. In other words, 29% of thecaregivers might be a case for a minor psychiatric disorder (SRQ pos-itive group) and these same caregivers showed higher scores than theremaining sample in the ECI subscales. It is worth noting that 68% an-swered that they had felt nervous, tense or worried, whereas 60% hadfelt sad recently. According to SF-36 scores, whereas the quality of lifewas more affected in both emotional aspects, scoring 53.77(SD=43.80), and vitality 62.66 (SD=23.62), it was less affected inphysical aspects, scoring 75.33 (SD=35.71) and physical functioning70.06 (SD=25.89). The other domains scored: bodily pain 64.46(26.47); general health perceptions 66.69 (19.66); social functioning68.00 (27.35); and mental health 65.01 (SD=23.71).
Table 4 compares the subscales mean ECI scores between the pos-itive caregiver group and the negative group according to the SRQ-20.The differences between these groups regarding stigma, problemswith health services, effects on family and negative total score were
ECI subscales Raw score Adjusted score
(By ECI Score) (By percentage of impairment)
Difficult behaviors Mean (SD) 15.01 (8.37) 46.91 (26.18)Negative symptoms Mean (SD) 13.32 (6.75) 55.50 (28.16)Stigma Mean (SD) 5.65 (4.32) 28.26 (21.59)Problems withservices
Mean (SD) 10.31 (8.26) 32.20 (25.82)
Effects on family Mean (SD) 9.03 (7.07) 32.23 (25.26)Need to provideback up
Mean (SD) 9.24 (5.78) 38.50 (24.10)
Dependency Mean (SD) 9.67 (4.48) 48.33 (22.44)Loss Mean (SD) 11.91 (5.73) 42.51 (20.47)Positive personalexperience
Mean (SD) 16.16 (7.58) 50.50 (23.68)
Good aspects ofrelationship
Mean (SD) 14.83 (5.04) 61.77 (21.01)
ECI total negative Mean (SD) 84.13 (39.56) 38.95 (18.31)ECI total positive Mean (SD) 30.99 (11.29) 55.33 (20.15)

277R.C.F.A. Jorge, A.C. Chaves / Schizophrenia Research 138 (2012) 274–279
statistically significant (pb0.05). Table 5 shows the correlations betweenECI scores and SF-36 scores, results which corroborated the findingsabove. Moreover, caregivers' physical quality of life was significantlynegatively correlated with most of the ECI subscales, showing the mostnegative caregiving experience is associated with caregivers' physicalquality of life. The ECI subscale stigmawas the item that hadmore signif-icant correlations with SF-36 domains.
Descriptive methods and statistical tests (T-Test) were performedincluding the following variables, in order to avoid spurious correla-tions: age, gender, marital status, monthly family incoming, employ-ment and years in school. Our data indicated that worse formaleducation is associated with lower quality of life levels assessed bySF-36 in 5 of the 8 domains (physical functioning, physical aspects,bodily pain, general health and vitality) as well worse formal educa-tion is associated with worse experience assessed by IEC in 4 of 10subscales (stigma, problems with health services, effects on familyand total negative score). So “years in school” is presented as a possibleconfounder, but there was no regularity in the relation.
4. Discussion
4.1. The ECI around the world
This is a well-know instrument to assess carers' experience, whichhas been used in studies with chronic and recent-onset psychosis pa-tients. Findings of such studies have showed that negative caregiverexperiences were associated with their mental status, i.e., the morenegative their appraisal of the situation, the higher their chance to de-velop a psychiatric condition. In order to evaluate whether those find-ings are comparable in our setting, a Brazilian version of ECI wasvalidated in our service.
4.2. The process of validation of the instrument
The validation of an instrument from another culture involves amethodological procedure that is not only merely a translation. It re-quires a number of steps and its goal is to accomplish the original as-sumption, maintaining the same clinical and psychometric properties.This study showed that the ECI Brazilian version achieved good reli-ability, confirmed by alpha values of internal consistency comparableto those reported by the developers of the original English instru-ment. It is important to emphasize that our results showed lower re-liability coefficients for stigma, dependency and good aspects of
Table 4Mean ECI scores between caregivers with positive and negative SRQ-20.
ECI sub-scales PositiveSRQ-20
NegativeSRQ-20
Total SRQ-20 p-value
n=22 n=53 n=75
MEAN s.d. Mean s.d. Mean s.d.
Difficult behaviors 17.50 8.32 13.87 8.26 14.93 8.39 0.39Negative symptoms 13.77 6.06 12.94 7.13 13.19 6.80 0.98Stigma 7.36 4.58 5.06 4.10 5.73 4.34 0.022⁎⁎
Problems with services 15.27 9.11 8.45 7.06 10.45 8.27 0.034⁎⁎
Effects on family 12.59 7.61 7.38 6.23 8.91 7.03 0.023⁎⁎
Need to provide back up 10.59 5.76 8.49 5.81 9.11 5.83 0.082⁎
Dependency 11.32 4.46 8.94 4.32 9.64 4.50 0.18Loss 14.59 6.44 10.85 5.10 11.95 5.74 0.082⁎
Positive personalexperience
15.41 6.99 16.32 7.81 16.05 7.53 0.31
Good aspects ofrelationship
15.77 4.87 14.30 5.11 14.73 5.05 0.62
ECI total negative 103.00 42.73 75.98 35.68 86.91 39.57 0.044⁎⁎
ECI total positive 31.18 10.09 30.62 11.77 30.79 11.24 0.68
p-value: Mann–Whitney non-parametric test.⁎⁎ Correlation is significant at the 0.01 level.⁎ Correlation is significant at the 0,05 level.
relationship than those in other-language versions of ECI, but in thedata analysis of the subscales none of the items particularly contributedto the depressed value found. On the other hand, both Italian and Japa-nese versions have these same sub-scales among their worst results,which could indicate a weakness of these items when subjected to atranslation process. We also consider that, in a FEP, stigma issuescould be less harmful because there is no time for the family to feelthe weight of prejudice.
This same reason could explain the low good aspects of relation-ship of Cronbach's alpha, given that the acute episode could preventthe family from experiencing these positive aspects of caregiving.With respect to the dependence alpha, we consider that almost allthe patients in our sample were still living with the caregivers andunemployed, even before the crisis, so they were already dependent.Add to this the fact that it is culturally acceptable and reasonable thatthe sons and daughters remain at their parents' home for many years.It is possible that this kind of dependence is so expected in the Brazilianculture that it is not seem as a burden by the caregiver or amodifying ofthe previous situation. The external validity level was evaluated by cor-relations between ECI scores and caregivers' psychological morbidity,and quality of life measured by SRQ-20 and SF-36, respectively. The re-sults were similar to those in findings from studies conducted in othercountries, thereby showing a cross cultural consistency (Szmukler etal., 1996; Tarricone et al., 2006; Lau and Pang, 2007). Our data, as wellAddington's, suggests that in the initial phase of the disease there isan impact on the caregivers, even in different cultures. As shown inTable 6, the Brazilian version subscale mean scores were presentedside by side to Calgary study results in FEP patients (Addington et al.,2003) than to the London's (Szmukler et al., 1996), whose sample con-sisted of chronic patients with schizophrenia.
4.3. The FEP caregivers' experience
We support the idea that our data, as well Addington's, suggeststhat in the initial phase of the disease there is an impact on the care-givers and that the ECI is a useful instrument to show us with do-mains that are more affected. FEP caregivers were affected in theinitial phase of treatment, particularly in their emotional aspectsand vitality. They were particularly affected by patients' negativesymptoms and difficult behaviors. On the other hand, FEP caregiversshowed a high level of positive personal experience, with the percep-tion of having discovered strengths in themselves, becoming moreunderstanding of others with problems and having meted helpfulpeople. The caregivers related also good experiences of relationshipwith the patients, with the perception of having contributed to theirwellbeing, felt useful in the relationship with them and that theywere good company. Almost one-third of the family membersreached SRQ-20 criteria for minor non-psychotic psychiatric disorderand most of them felt nervous, tense, worried and sad in the last4 weeks. This specific group of caregivers had a worse caregiving ex-perience in the fields of stigma, problems with health services and ef-fects on family, and they had a closer follow-up to help them developstrategies to cope with their new condition. Our data also indicatedthat physical aspects of the caregivers are associated with a negativeappraisal of their role as carers, but because this was a cross-sectionalstudy, it was not possible to determine the effect direction (Table 5).However, this finding is congruent with a supposed “somatizingtrace” of Latin cultures, which may be linked to a cultural and linguisticexpression (Tofoli et al., 2011).
4.4. Limitations
The findings of this study need to be carefully assessed. In view ofthe sample size, the findings of validity and reliability of the translat-ed version may not be fully acceptable. The Italian version of the ECIused a sample size of 95 subjects and the Chinese version used 129.

Table 5Spearman test (non-parametric) between ECI and SF-36.
ECI subscales Physical functioning Physical aspects Bodily pain General health Physical vitality Social functioning Emotional aspects Mental health
Difficult behaviors 0.01 −0.31⁎⁎ −0.20 −0.10 −0.03 −0.13 −0.15 0.00Negative symptoms 0.08 −0.12 0.08 −0.03 0.06 −0.12 0.02 0.10Stigma −0.24⁎ −0.34⁎⁎ −0.20 −0.43⁎⁎ −0.16 −0.25⁎ −0.20 −0.20Problems with services −0.18 −0.40⁎⁎ −0.16 −0.22 −0.14 −0.22 −0.23 −0.20Effects on family −0.22 −0.42⁎⁎ −0.19 −0.17 −0.15 −0.19 −0.29⁎ −0.15Need to provide back up −0.05 −0.22 −0.30⁎⁎ −0.19 −0.14 −0.17 −0.26⁎ −0.15Dependency −0.10 −0.30⁎⁎ −0.05 0.00 −0.22 −0.22 −0.19 −0.13Loss −0.06 −0.24⁎ −0.13 −0.19 −0.12 −0.14 −0.12 −0.12Positive personal experience 0.26⁎ 0.04 0.21 0.22 0.07 0.01 −0.07 0.04Good aspects of relationship −0.04 −0.08 −0.08 0.05 0.00 0.00 −0.08 −0.07ECI total negative −0.14 −0.42⁎⁎ −0.14 −0.21 −0.13 −0.27⁎ −0.28⁎ −0.14ECI total positive 0.16 −0.01 0.12 0.18 0.04 0.01 −0.10 −0.02
p-value: Spearman non-parametric test.⁎⁎ Correlation is significant at the 0.01 level.⁎ Correlation is significant at the 0.05 level.
278 R.C.F.A. Jorge, A.C. Chaves / Schizophrenia Research 138 (2012) 274–279
We did not perform a formal test to determine the ideal sample sizeand we understand that it might be a methodological issue. On theother hand, other important Brazilian version scales were validatedwith modest sample size and they proved themselves useful in thepsychiatric practice, as SF-36 (50 subjects×36 items and 8 domains),Folkman e Lazarus's Ways of Coping Questionnaire (100 subjects×66items) Obsessive–Compulsive Inventory (15 subjects×42 items) andDissociative Experiences Scale (10 subjects×28 items) (Savoia et al.,1996; Ciconelli et al., 1999; Fiszman et al., 2004; Souza et al., 2008).We understand that the ECI is a useful instrument and that the valida-tion process for Portuguese-Brazilian is a contribution for severementalhealth services, their patients and caregivers in Brazil as well. For asmall service, assisting poor people within the Brazilian mental healthsystem, we felt as a great victory to reach this sample size.
Another limitation is that the SRQ-20 applied to caregivers is ascreening test and there was not a psychiatric assessment and a formaldiagnosis for them. These caregivers were followed with special atten-tion through a multi-family group intervention offered by the service,but there was no specific psychiatric evaluation in the first moment.Only if the impairment persisted in the second evaluation, caregiverswere referred for psychiatric evaluation and treatment. For this reason,thefindings of psychiatricmorbidity are limited and cannot be attributedonly to the caregiving experience. In fact, we found an association, butother factors may interfere in this equation.
4.5. Clinical implications
Caregivers are subject to several problems in a relative's FEPprocess. Broadening the availability of measures to assess caregiver
Table 6ECI mean scores: carers of FEP patients x carers of patients with chronic schizophrenia.
ECI sub-scales FEP FEP Chronic
Brazilianversion
Addingtonet al. (2003)
Szmukleret al. (1996)
Mean s.d. Mean s.d. Mean s.d.
Difficult behaviors 15.01 8.37 13.85 7.91 11.20 6.40Negative symptoms 13.32 6.75 13.45 6.20 10.60 5.60Stigma 5.65 4.32 6.32 4.75 5.50 4.40Problems with services 10.31 8.26 11.24 5.86 13.30 7.30Effects on family 9.03 7.07 9.36 5.86 10.40 6.3Need to provide back up 9.24 5.78 10.31 5.45 8.90 5.7Dependency 9.67 4.48 10.52 4.45 10.10 4.7Loss 11.91 5.73 12.53 5.56 12.50 6.9Positive personal experience 16.16 7.58 15.80 6.35 16.30 7.1Good aspects of relationship 14.83 5.04 14.05 4.32 12.80 4.4ECI total negative 84.13 39.56 87.58 33.64 82.5 n/a
n/a — not available.
distress is essential for identification of caregivers who may be at-risk for problematic or maladaptative interactions with FEP patients,as such negative interactions may contribute to exacerbation of symp-toms and poor patient outcome for the patient and the caregiver. The ECIis a useful instrument for identification of this specific caregiversand it has the advantage of assessing negative and positive aspects ofcaregiving. Brazilian psychiatry is poor in such instruments, so translateand validate the ECI for our language give to us an important weaponto identify the individuals who need help early in the treatment, and itprovides substrate for tailored strategies to the most affected caregivers,working on the most affected domains.
The final version of Brazilian ECI is available and can be requestedfor free. Our interest is to share the present instrument with the com-munity, in order to this paper provide a real benefit to FEP patients,caregivers and mental health services.
5. Conclusion
FEP caregivers are under stress in the beginning of the disease andshould receive special attention in a FEP program, so as to reduce theultimate severity of the illness. The Brazilian version of ECI is an easy,reliable and valid instrument to describe the experience of caring fora relative with serious mental illness. Moreover, it can detect earlydistress on these caregivers. It offers mental health professionals anopportunity not only to access caregivers' global experience andtheir evaluation of a severe mental disease, but also to predict theirpsychological suffering, which is harmful to both patient and caregiver.There is some support for specialized early intervention services inBrazil, but further trials would be desirable. To date, the study of thispopulation in our country has been rudimentary and these data arejust the preliminary results of a comprehensive research. We hopethat our findings can help to stimulate more studies in this area,providing amodest but solid contribution in bringing themental healthservice closer to the real needs of our patients and their relatives.
Role of funding sourceThis work was supported by a grant to FAPESP, a foundation that supports research
in the São Paulo state, Brazil. Process number: 2008/10635-5. The funding source hadno involvement in the decision to write the paper or in the decision to submit thepaper for publication.
ContributorsRita Jorge and Ana Cristina Chaves had contributed equally for the design of the
study, writing the protocol, managing and overseeing all of the data collection, statisticalanalysis, andwriting the first draft of the paper, although author Dr. Ana Cristina Chaves isthe chief of the research and approved the final manuscript.
Conflict of interestRita Jorge and Ana Cristina Chaves report no financial relationships with commercial
interests.

279R.C.F.A. Jorge, A.C. Chaves / Schizophrenia Research 138 (2012) 274–279
AcknowledgmentsWe would like to thank the staff of First-Episode Program of the UNIFESP.
References
Addington, J., Coldham, E.L., Jones, B., Ko, T., Addington, D., 2003. The first episode ofpsychosis: the experience of relatives. Acta Psychiatr. Scand. 108 (4), 285–289.
Bertolote, J., McGorry, P., 2005. Early intervention and recovery for young people withearly psychosis: consensus statement. Br. J. Psychiatry 187, 116–119.
Cabral, R.R.F., Chaves, A.C., 2005. Knowledge of the disease and treatment expectationsin relatives of patients with the first psychotic episode: a cross-sectional study.Rev. Psiquiatr. Rio Gd. Sul 27 (1), 32–38.
Cabral, R.R.F., Chaves, A.C., 2010. Multi-family group intervention in a programme forpatients with first-episode psychosis: a Brazilian experience. Int. J. Soc. Psychiatry56 (5), 527–532.
Ciconelli, R.M., Ferraz, M.B., Santos, W., 1999. Brazilian-Portuguese version of the SF-36. Areliable and valid quality of life outcome measure. Rev. Bras. Reumatol. 39, 143–150.
First, M.B., Spitzer, R.L., Williams, J.B.W., Gibbon, M., 1995. Structured clinical interviewfor DSM-IV axis I disorders (SCID-I), Handbook of Psychiatric Measures, first ed.American Psychiatric Association, Washington (DC), pp. 49–53.
Fiszman, A., Cabizuca, M., Lanfredi, C., Figueira, I., 2004. The cross-cultural adaptationto Portuguese of the dissociative experiences scale for screening and quantifyingdissociative phenomena. Rev. Bras. Psiquiatr. 26 (3), 164–173.
Guillemin, F., 1995. Cross-cultural adaptation and validation of health status measures.J. Rheumatol. 24, 61–63.
Harding, T.W., Arango, M.V., Baltazar, J., Climent, C.E., Ibrahim, H.H., Ladrido-Ignacio, L.,Murthy, R.S., Wig, N.N., 1980. Mental disorders in primary health care: a study oftheir frequency and diagnosis in four development countries. Psychol. Med. 10,231–241.
Joyce, J., Leese, M., Szmukler, G., 2000. The experience of caregiving inventory: furtherevidence. Soc. Psychiatry Psychiatr. Epidemiol. 35, 185–189.
Kay, S.R., Fiszbein, A., Opler, L.A., 1987. The Positive and Negative Syndrome Scale forschizophrenia. Schizophr. Bull. 13, 261–276.
Keshavan, M.S., Schooler, N.R., 1992. First-episode studies in schizophrenia: criteriaand characterization. Schizophr. Bull. 18, 491–513.
Lau, D.Y.K., Pang, A.H.T., 2007. Validation of the Chinese version of experience ofcaregiving inventory in caregivers of persons suffering from severe mentaldisorders. Hong Kong J. Psychiatry 17, 24–31.
Mari, J.J., Williams, P., 1986. A validity study of a psychiatric screening questionnaire(SQR-20) in primary care in the city of São Paulo. Br. J. Psychiatry 148, 23–26.
Martens, L., Addington, J., 2001. The psychological well-being of family members ofindividuals with schizophrenia. Soc. Psychiatry Psychiatr. Epidemiol. 36, 128–133.
McCleery, A., Addington, J., Addington, D., 2007. Family assessment in early psychosis.Psychiatry Res. 152 (2–3), 95–102.
Savoia, M.G., Santana, P.R., Mejias, N.P., 1996. Adaptação do inventário de estratégias decoping de Folkman e Lazarus para o português. Psicol. USP 7 (1–2), 183–201.
Sepulveda, A.R., Graell, M., Berbel, E., Anastasiadou, D., Botella, J., Carrobles, J.A.,Morandé, G., 2011. Factors associated with emotional well-being in primary andsecondary caregivers of patients with eating disorders. Eur. Eat. Disord. Rev. 20(1), e78–e84.
Souza, F.P., Foa, E.B., Meyer, E., Niederauer, K.G., Raffin, A.L., Cordioli, A.V., 2008.Obsessive-compulsive inventory and Obsessive-compulsive inventory-revisedscales: translation into Brazilian Portuguese and cross-cultural adaptation. Rev.Bras. Psiquiatr. 30 (1), 42–46.
Szmukler, G.I., Burgess, P., Herrman, H., Bloch, S., Benson, A., Colusa, S., 1996. Caring forrelatives with serious mental illness: the development of the Experience ofCaregiving Inventory. Soc. Psychiatry Psychiatr. Epidemiol. 31 (3–4), 137–148.
Tarricone, I., Leese, M., Szmukler, G.I., Bassi, M., Berardi, D., 2006. The experience ofcarers of patients with severe mental illness: a comparison between London andBologna. Eur. Psychiatry 21 (2), 93–101.
Tofoli, L.F., Andrade, L.H., Fortes, S., 2011. Somatization in Latin America: a review ofthe classification of somatoform disorders, functional syndromes and medicallyunexplained symptoms. Rev. Bras. Psiquiatr. 33 (1), 59–69.
Vessoni, A.L.N., 1993. Adaptação e Estudo da Confiabilidade da Escala de Avaliação dasSíndromes Positiva e Negativa para a Esquizofrenia no Brasil São Paulo, Tese demestrado Escola Paulista de Medicina.
Ware, J.E., Shelbourne, D., 1992. The MOS 36-item short-form health survey (SF-36).Med. Care 30, 473–481.
Web References
Grover, S., Chakrabarti, S., Aggarwal, M., Avasthi, A., Kulhara, P., Sharma, S., Khehra, N.,2011. Comparative study of the experience of caregiving in bipolar affectivedisorder and schizophrenia. Int. J. Soc. Psychiatry (Aug 25. Electronic publicationahead of print, http://www.ncbi.nlm.nih.gov/pubmed/21873293).
Laguardia, J., Campos, M.R., Travassos, C.M., Najar, A.L., Anjos, L.A., Vasconcellos, M.M.,2011. Psychometric evaluation of the SF-36 (v.2) questionnaire in a probabilitysample of Brazilian households: results of the survey Pesquisa Dimensões Sociaisdas Desigualdades (PDSD), 2008. Health Qual. Life Outcomes 9, 61 (August 3.http://www.hqlo.com/content/9/1/61).